")
Back to Journals » Journal of Pain Research » Volume 14
Spreading of Pain in Patients with Chronic Pain is Related to Pain Duration and Clinical Presentation and Weakly Associated with Outcomes of Interdisciplinary Pain Rehabilitation: A Cohort Study from the Swedish Quality Registry for Pain Rehabilitation (SQRP)
Authors Gerdle B , Rivano Fischer M, Cervin M, Ringqvist Å
Received 24 October 2020
Accepted for publication 4 December 2020
Published 28 January 2021 Volume 2021:14 Pages 173—187
DOI https://doi.org/10.2147/JPR.S288638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Björn Gerdle,1 Marcelo Rivano Fischer,2,3 Matti Cervin,4 Åsa Ringqvist2
1Pain and Rehabilitation Centre, Department of Health, Medicine and Caring Sciences, Linköping University, Linköping SE-58185, Sweden; 2Department of Neurosurgery and Pain Rehabilitation, Skåne University Hospital, Lund SE-22185, Sweden; 3Research Group Rehabilitation Medicine,Dept of Health Sciences, Lund University, Lund, Sweden; 4Department of Clinical Sciences Lund, Faculty of Medicine, Lund University, Lund SE-22100, Sweden
Correspondence: Björn Gerdle
Pain and Rehabilitation Centre, Department of Health, Medicine and Caring Sciences, Linköping University, Linköping SE-581 85, Sweden
Tel +46763927191
Email [email protected]
Introduction: The extent to which pain is distributed across the body (spreading of pain) differs largely among patients with chronic pain conditions and widespread pain has been linked to poor quality of life and work disability. A longer duration of pain is expected to be associated with more widespread pain, but studies are surprisingly scarce. Whether spreading of pain is associated with clinical presentation and treatment outcome in patients seen in interdisciplinary multimodal pain rehabilitation programs (IMMRPs) is unclear. The association between spreading of pain and (1) pain duration (2) clinical presentation (eg, pain intensity, pain-related cognitions, psychological distress, activity/participation aspects and quality of life) and (3) treatment outcome were examined.
Methods: Data from patients included in the Swedish Quality Registry for Pain Rehabilitation were used (n=39,916). A subset of patients that participated in IMMRPs (n=14,666) was used to examine whether spreading of pain at baseline predicted treatment outcome. Spreading of pain was registered using 36 predefined anatomical areas which were summarized and divided into four categories: 1– 6 regions with pain (20.6% of patients), 7– 12 regions (26.8%), 13– 18 regions (22.0%) and 19– 36 regions (30.6%).
Results: More widespread pain was associated with a longer pain duration and a more severe clinical picture at baseline with the strongest associations emerging in relation to health and pain aspects (pain intensity, pain interference and pain duration). Widespread pain was associated with a poorer overall treatment outcome following IMMRPs at both posttreatment and at a 12-month follow-up, but effect sizes were small.
Discussion: Spreading of pain is an indicator of the duration and severity of chronic pain and to a limited extent to outcomes of IMMRP. Longer pain duration in those with more widespread pain supports the concept of early intervention as clinically important and implies a need to develop and improve rehabilitation for patients with chronic widespread pain.
Keywords: chronic pain, interdisciplinary, outcome, pain spreading, rehabilitation, spatial distribution
Introduction
Interdisciplinary multimodal pain rehabilitation programs (IMMRPs) are based on a biopsychosocial model of chronic pain. The core goals of these programs are broad and multifactorial and include individualized goals of the patients.1,2 IMMRPs are psychologicallybased interventions, cognitive behavioral therapy (CBT) and/or acceptance commitment therapy (ACT), which also include chronic pain education, supervised physical activity, and work and activity training. IMMRP interventions are generally delivered in a group-treatment format by an interdisciplinary team and administered over several weeks to a few months.3–6 Systematic reviews suggest that IMMRPs are more effective than single treatment or treatment-as-usual programs.4,6–13 For complex interventions such as IMMRPs, it is important to include a broad range of outcomes. However, most systematic reviews of the effects of IMMRPs have traditionally evaluated the outcomes as independent from each other;1,2,14,15 a questionable strategy both from clinical and statistical standpoints.
Few studies have investigated outcomes of IMMRPs in large, nationwide cohorts of chronic pain patients. Exceptions are recent studies from the Swedish Quality Registry for Pain Rehabilitation (SQRP) project that have found that patients with the most severe pain experience the largest improvements following IMMRP.16–18 A study that examined changes in the 22 mandatory outcome variables in SQRP found that changes in 18 of the 22 variables were markedly intercorrelated.18 A multivariate improvement score (MIS) based on these variables was therefore defined as an overall outcome measure of IMMRPs in SQRP. Another recent study from the SQRP project found that patients born outside of Europe (including both men and women with different education levels) had the most severe clinical presentation at baseline while European women with a university education had the least severe clinical presentations at baseline.19 Moreover, using the MIS outcome, it was found that IMMRPs benefited the latter more than the former subgroup.19
The spatial distribution of pain (ie the spreading of pain over the body) differs among chronic pain patients. Chronic pain has been considered a continuum with widespread pain (WSP, including fibromyalgia) as one of the extremes which is associated with a more severe clinical picture and a worse prognosis. WSP is prevalent in the general population (9.6–10.6%) and more prevalent in women than in men.20,21 It is associated with a poor resolution prognosis, poor health related quality of life, work disability and a higher proportion of disability pensions.22,23 Cross-sectional population studies have reported that spreading of pain is significantly associated with pain intensity, depressive disorders and poor health.24,25
Prospective studies in the general population have shown that localized pain (LP) can transition into WSP over time and vice versa, with men being less prone to develop persistent WSP.26,27 In specialist settings (representing a selection of the most severe cases), smaller cohorts of chronic pain patients have been studied and WSP has been shown to be associated with a longer duration of pain.28 To the best of our knowledge, no studies have investigated spreading of pain in large cohort studies in specialist settings. Moreover, of importance for clinical assessments and designs of IMMRPs, it remains to be studied whether spreading of pain is associated with outcomes following IMMRPs.
The aim of this study was to address the above described knowledge gaps concerning possible associations between spreading of pain and (1) pain duration, (2) clinical picture, and (3) overall treatment outcomes in chronic pain patients referred to specialist clinics. SQRP offers a unique opportunity to investigate real-life chronic pain patients since most specialist care units in Sweden deliver data to the registry.29
Materials and Methods
The instruments used in this study and the included cohort of patients have been described in detail elsewhere and below we only give brief descriptions of SQRP and the variables analyzed in the present study.16,18
The Swedish Quality Registry for Pain Rehabilitation (SQRP)
The SQRP receives data from a vast majority of specialist units in Sweden.29 The SQRP is largely based on self-reported data, ie patient reported outcome measures (PROM). These capture a patient’s background, pain intensity, pain-related cognitions, and psychological distress symptoms as well as activity/participation aspects and health-related quality of life variables. Patients complete the questionnaires on up to three occasions: (1) before assessment on their first visit (baseline) and for patients participating in IMMRP also (2) immediately after discharge (post-IMMRPs); and (3) at a 12-month follow-up after discharge (12-month follow-up). Not all assessed patients will participate in IMMRPs; some may need further investigation, some receive a unimodal treatment, and some may, for different reasons, not participate in the IMMRPs despite this being recommended at the baseline assessment.
Subjects
This study included SQRP data from patients ≥18 years old with complex chronic (≥3 months) nonmalignant pain who were referred to specialist care centers between 2008 and 2016. Strict criteria for inclusion are not available since SQRP is a clinical registry study of patients with complex chronic pain conditions. However, general inclusion criteria for IMMRPs were: (i) disabling nonmalignant chronic pain (on sick leave or experiencing major interference in daily life due to chronic pain); (ii) age 18 years and above; (iii) no further medical investigations needed; and (iv) written consent to participate and attend in IMMRPs. General exclusion criteria for IMMRPs were severe psychiatric comorbidity, abuse of alcohol and/or drugs, diseases that did not allow physical exercise, and specific pain conditions associated with red flags.
The study was conducted in accordance with the Helsinki Declaration and Good Clinical Practice and approved by the Ethical Review Board in Linköping, Sweden (Dnr: 2015/108-31). All participants received written information about the study and gave their written consent.
Variables
The variables and instruments used in this study are mandatory for the clinical specialist departments registering their data with the SQRP.
Spreading of Pain (Spatial Extent of Pain)
Spreading of pain was registered using 36 predefined anatomical areas (18 on the front and 18 on the back of the body) and patients reported about pain in the following areas: (1) head/face, (2) neck, (3) shoulder, (4) upper arm, (5) elbow, (6) forearm, (7) hand, (8) anterior aspect of chest, (9) lateral aspect of chest, (10) belly, (11) sexual organs, (12) upper back, (13) low back, (14) hip/gluteal area, (15) thigh, (16) knee, (17) shank, and (18) foot. The number of areas with pain (range: 1–36) were summarized and the obtained variable was denoted as pain region index (PRI). This variable was divided into roughly equal categories: 1–6 regions with pain (20.6% of patients), 7–12 regions (26.8%), 13–18 regions (22.0%) and 19–36 regions (30.6%).
Background Data
The following background data were extracted from SQRP: gender (man or woman); education level (university, upper secondary school, elementary school; this variable was dichotomized and denoted as university vs no university); country of birth, (Sweden; other Nordic countries, ie, Denmark, Finland, Iceland, and Norway); Europe except the Nordic countries; outside Europe; this variable was dichotomized as from Europe vs outside of Europe). Data for age (years), self-reported days with no work or studies and self-reported pain duration (days) were also extracted. Health-care seeking was indicated using an item indicating number of visits to a physician during the last 12 months (categories: 0–1 times, 2–3 times, and ≥4 times); the category ≥4 times was used to indicate high health-care consumption.
Mandatory Outcome Variables
The following 22 mandatory outcome variables are registered on up to three occasions (baseline, post-IMMRP and at the 12-month follow-up) in SQRP. Swedish language versions of all outcome measures were used and detailed reports of their psychometric properties have been provided elsewhere.16,18,30–32 In the present study, these 22 variables together with background variables were used as indicators of clinical presentation at baseline.
Pain Intensity
Average pain intensity during the previous seven days was registered using a 11-graded numeric rating scale (NRS; 0=no pain to 10=worst possible pain). This variable was denoted as NRS-7days.
The Multidimensional Pain Inventory (MPI)
This multidimensional pain inventory (MPI) consists of three parts.33,34 Part one has five scales: pain severity—measuring several aspects of the pain experience (MPI-pain-severity); pain-related interference in everyday life (MPI-pain-interfer); perceived life control (MPI-lifecon); affective distress (MPI-distress); and social support—perceived support from a spouse or significant other (MPI-socsupp). Part two assesses the perception of responses to displays of pain and suffering from significant others: punishing responses (MPI-punish); protecting responses (MPI-protect); and distracting responses (MPI-distract). Part three covers the participation in various activities using four scales, which in the Swedish version are combined into a general activity index (MPI-GAI).35
Psychological Distress Variables
The Hospital Anxiety and Depression Scale (HADS) consists of two subscales: depression (HADS-D) and anxiety (HADS-A) and scores on both subscales range from 0 to 21.36,37
The Short Form Health Survey (Sf36)
The short form health survey (sf36) addresses multidimensional health aspects.38 It consists of eight aspects, each graded from 0 to 100, with higher scores indicating a better perception of health: (1) physical functioning (sf36-pf); (2) role limitations due to physical functioning (sf36-rp); (3) bodily pain (sf36-bp); (4) general health (sf36-gh); (5) vitality (sf36-vt); (6) social functioning (sf36-sf); (7) role limitations due to emotional problems (sf36-re); and (8) mental health (sf36-mh).
The European Quality of Life Instrument (EQ-5D)
The European Quality of Life (EQ-5D) instrument captures the perceived state of health.39–41 Five dimensions (three alternatives for each dimension) are used to obtain an index: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. A measure of today’s health according to a scale, a thermometer-like 100-point scale (EQ-VAS) with defined end points (high values indicate good health and low values indicate poor health), is also part of EQ-5D.
General Overall Outcomes of IMMRPs in SQRP
Three overall outcome measures which were analyzed post-IMMRP and at the 12-month follow-up were used and are described below.
Multivariate Improvement Score (MIS)
Changes in the 22 mandatory outcome variables have been used to create a broad overall outcome measure.18 As described in the introduction, changes in 18 of the 22 mandatory are markedly intercorrelated.18 To synthesize information from these outcome variables, the t-score of the first component (labelled MIS) of a principal component analysis conducted at post-IMMRP and at the 12-month follow-up was used as a comprehensive measure of change in these 18 outcomes. As recently reported, the goodness of fit R2 (ie the fraction of sum of squares of all the variables explained by a principal component) was 0.31 post IMMRP and 0.36 at the 12-month follow-up; the goodness of prediction Q2 (ie the fraction of the total variation of the variables that could be predicted using principal component cross validation methods) was 0.25 and 0.31 at post-IMMRP and at the 12-month follow-up, respectively.18 Thus, MIS is a broad outcome measure of IMMRP and higher MIS indicates a larger overall improvement.18 The following MIS values were obtained for patients undergoing IMMRPs in the present study:
MIS post IMMRP:mean: −0.011±2.59, 95%CI: −0.053 to 0.030, n=14,666.
MIS 12-month follow-up:mean: −0.011±2.80, 95%CI: −0.069 to 0.048, n=8851.
In a recent study, conducted to explore the clinical importance of MIS, we identified three subgroups based on MIS data.18 At the 12-month follow-up, subgroup one had the highest MIS (5.01±1.78, 95%CI: 4.90 to 5.11), subgroup two had the second highest MIS (0.78±1.35; 95%CI: 0.74 to 0.82), and subgroup three had the lowest MIS (−2.43±1.39, 95%CI: −2.47 to −2.38).18 When scrutinizing the 22 mandatory outcomes, it was obvious that subgroup 1 generally showed clear improvements, subgroup two generally showed slight improvements, and subgroup three showed no changes or deteriorations. MIS data at post IMMRP and at the 12-month follow-up were used in the present study.
Changes in Pain and Life Situation Following IMMRPs
At post-IMMRPs and at the 12-month follow-up, patients estimated the degree of positive change in pain (Change-pain) and in the ability to handle life situations in general (Change-life situation). Both items were rated on five-point Likert scales: Change-pain—markedly increased pain (0) to markedly decreased pain (4) and Change-life situation—markedly worsened (0) to markedly improved (4). The two variables were trichotomized (Change-pain: increased pain, no change, diminished pain; Change-life situation: worsened, no change, improved).
Statistics
All statistics were performed using the statistical packages IBM SPSS Statistics (version 24.0; IBM Corporation, Armonk, New York, USA) and SIMCA-P+ (version 15.0; Sartorius Stedim Biotech, Umeå, Sweden). A probability of <0.001 (two-tailed) was accepted as the criteria for statistical significance due to the large number of subjects. Text and tables report the mean value ±one standard deviation (±1 SD) of continuous variables. Percentages (%) are reported for categorical variables. SQRP uses predetermined rules when handling single missing items of a scale or a subscale; details are reported elsewhere.42 To compare groups, we used Student’s t-test for independent samples, ANOVA; (Bonferroni post hoc test if significant difference), and chi-squared test. Effect sizes (ES; Cohen’s d) for within group analyses were computed using a calculator when appropriate (https://webpower.psychstat.org/models/means01/effectsize.php). Hedges’ g—a measure of effect size weighted according to the relative size of each sample was used for between group ES using a calculator (https://www.socscistatistics.com/effectsize/default3.aspx). The absolute effect size was considered clinically insignificant for <0.20, small for 0.20–0.49, moderate for 0.50–0.79, large for 0.80–1.29, and very large for ≥1.3.43 For traditional correlation analysis we used Pearson's correlation (correlation coefficient r and p-value are reported). A detailed statistical description of how MIS was obtained is given elsewhere.18
Using SIMCA-P+, we applied advanced principal component analysis (PCA) for the check of multivariate outliers (none found) and orthogonal partial least square regressions (OPLS) for the investigations of multivariate associations. These advanced multivariate techniques do not require normal distributions of the included variables and take advantage of multicollinearity among regressors.44 SIMCA-P+ uses the nonlinear iterative partial least squares (NIPALS) algorithm to handle missing data: max 50% missing data for variables/scales and max 50% missing data for subjects. OPLS was used for the multivariate regression analyses of number of anatomical regions with pain (ie PRI) using background variables and the 22 mandatory variables at baseline as regressors. The variable influence on projection (VIPpred) indicates the relevance of each X–variable pooled over all dimensions and Y-variables—the group of variables that best explain Y.45 VIP >1.0 was considered significant if VIP had 95% jackknife uncertainty confidence interval non-equal to zero. P(corr) was used to note the direction of the relationship (positive or negative). This is the loading of each variable scaled as a correlation coefficient and thus having a value of −1 to +1.44 The variable p(corr) is stable during iterative variable selection and comparable between models. An absolute p(corr) of ≥0.40 was considered significant.44 Thus, a variable/regressor was considered significant when VIP >1.0 and absolute p(corr) ≥0.40. A regression model will be obtained—including one or several components (the first is always the predictive component)—if certain predefined criteria are met. The validity of the model is estimated using cross validation. R2 describes the goodness of fit—the fraction of sum of squares of all the variables explained by a principal component.45 Q2 describes the goodness of prediction—the fraction of the total variation of the variables that can be predicted using principal component cross validation methods.45 Hence, for each regression, we report R2, Q2, and the p-value of a cross-validated analysis of variance (CV-ANOVA).
Results
Spreading of Pain and Clinical Presentation at Baseline
The number of pain regions (ie, spreading of pain) was statistically significantly higher in women than in men (15.8±8.7 vs 11.1±7.3; p<0.001) and this difference was associated with a moderate ES. Hence, more women than men reported widespread pain (Table 1). The categorial analyses showed that the patient group with most widespread pain had a lower proportion of men, a lower proportion of patients with university education, a higher proportion of patients born outside of Europe and high health-care seeking while the inverse was found for the group with the least spreading of pain (Table 1). The mean age in the group with most widespread pain was higher than in the group with least widespread pain, but the difference was small (Table 2). Pain duration as well as number of days with no work/education were significantly higher in the group with more widespread pain compared to the group with least spreading of pain (Table 2), with the ES for pain duration being in the moderate range (Table 2).
 |
Table 1 Gender, Born Outside Europe, University Education and High Health-care Seeking by Pain Spreading in Four Categories. Furthest to the Right is Shown Statistics (Chi-squared Test) |
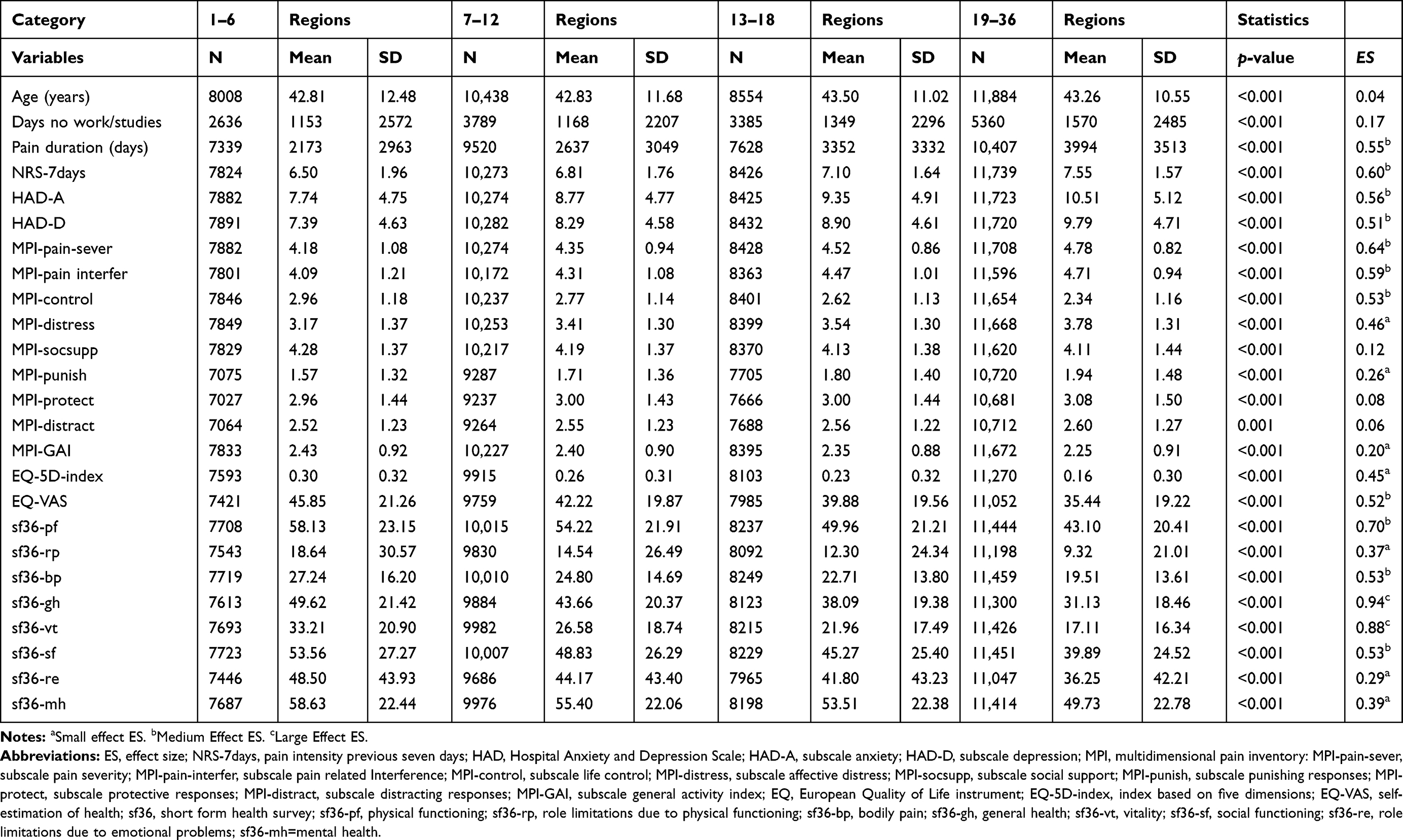 |
Table 2 Age, Duration of Period Without Work/Studies, Pain Duration and the 22 Mandatory Outcome Variables at Baseline (Mean, SD and n) by the Four Pain Categories Based on Pain Spreading. Group Comparison (ANOVA, p-value) and Effect Size (Hedges’ g) for the Pairwise Comparison 1–6 Regions vs 19–36 Regions are to the Far Right |
Baseline scores on 21 of the 22 outcome variables (lower part of Table 2) showed significant differences across groups; those with more widespread pain (19–36 regions) had significantly more severe scores on all variables compared with those with more localized pain (1–6 regions) (Table 2). These results were confirmed according to post-hoc tests for all variables (results not shown). The ESs were at least moderate for pain duration, pain intensity aspects, pain interference/physical function, psychological distress and health aspects including vitality (Table 2). Social support and responses from significant others were exceptions with ESs in the insignificant range (Table 2).
The variable containing the number of pain regions (PRI; 1–36) was regressed using the background variables and the 22 variables at baseline as regressors (Table 3). This significant analysis (one predictive component and two orthogonal components) confirmed the ES results presented in Table 2, namely that health aspects (sf-36-gh, sf36-vt, and EQ-VAS) were negatively and strongly associated with PRI. Pain intensity aspects (MPI-pain-sever, NRS-7d and sf36-bp), pain duration and interference in daily life (sf36-pf and MPI-pain-interfer), and female gender were also relatively strongly associated with PRI. Psychological distress variables (HAD-D, HAD-A, sf36-mh and MPI-distress) were less strongly associated with PRI in this multivariate context.
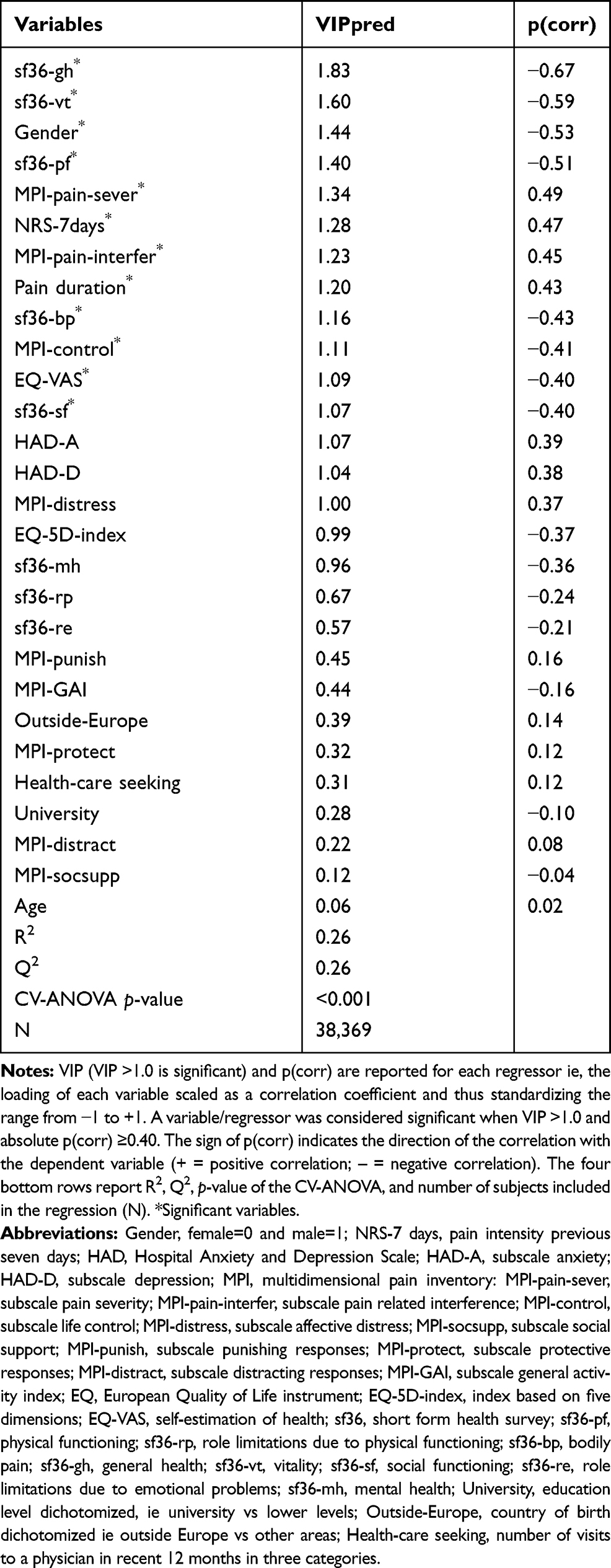 |
Table 3 OPLS Regression of Number of Pain Regions (1–36I) Using Background Variables and the 22 Mandatory Variables at Baseline as Regressors. Note that variable Days with no work or studies was not entered in the regression due to low N. |
Participation in and Outcomes of IMMRPs
Small significant differences (χ2=56.42, df=3, p<0.001) for participation rate in IMMRPs were found between the four pain groups: 1–6 regions: 34.6%; 7–12 regions: 39.6%; 13–18 regions: 38.5%; and 19–36 regions: 36.5%. The groups with least and most spreading of pain had the lowest participation rates.
Statistically significant but very weak correlations were found between number of pain regions (PRI) and MIS at post-IMMRP (r=−0.034, n=14,516 p<0.001) and at the 12-month follow-up (r=−0.078, n=8783, p<0.001), with more widespread pain at baseline being associated with worse treatment outcome.
Significant differences in MIS were also found across the four groups classified according to the extent of spreading of pain. Differences were present both at post-IMMRP and at the 12-month follow-up: post IMMRP: 1–6 regions: 0.15±2.74 (n=2769), 7–12 regions: 0.01±2.59 (n=4135), 13–18 regions: −0.03 ±2.55 (n=3294) and 19–36 regions: −0.12±2.51 (n=4318), p<0.001; 12-month follow-up: 1–6 regions: 0.36±2.99 (n=1714), 7–12 regions: 0.09±2.83 (n=2442), 13–18 regions: −0.08±2.78 (n=2038) and 19–36 regions −0.28± 2.63 (n=2589), p<0.001. The post hoc tests at post-IMMRP showed a significant difference between 1–6 vs 19–36 regions (p<0.001). At the 12-month follow-up, the post-hoc test showed that 1–6 regions differed significantly from the other groups (p<0.001–0.010) and that those with 7–12 regions differed from those with 19–36 regions (p<0.001). The pairwise effect sizes for 1–6 regions vs 19–36 were insignificant (ES=0.10) at post IMMRP and small at the 12-month follow-up (ES=0.23). To facilitate the interpretation of MIS, the changes in the 22 outcome variables across the four groups at the 12-month follow-up are presented in Table 4.
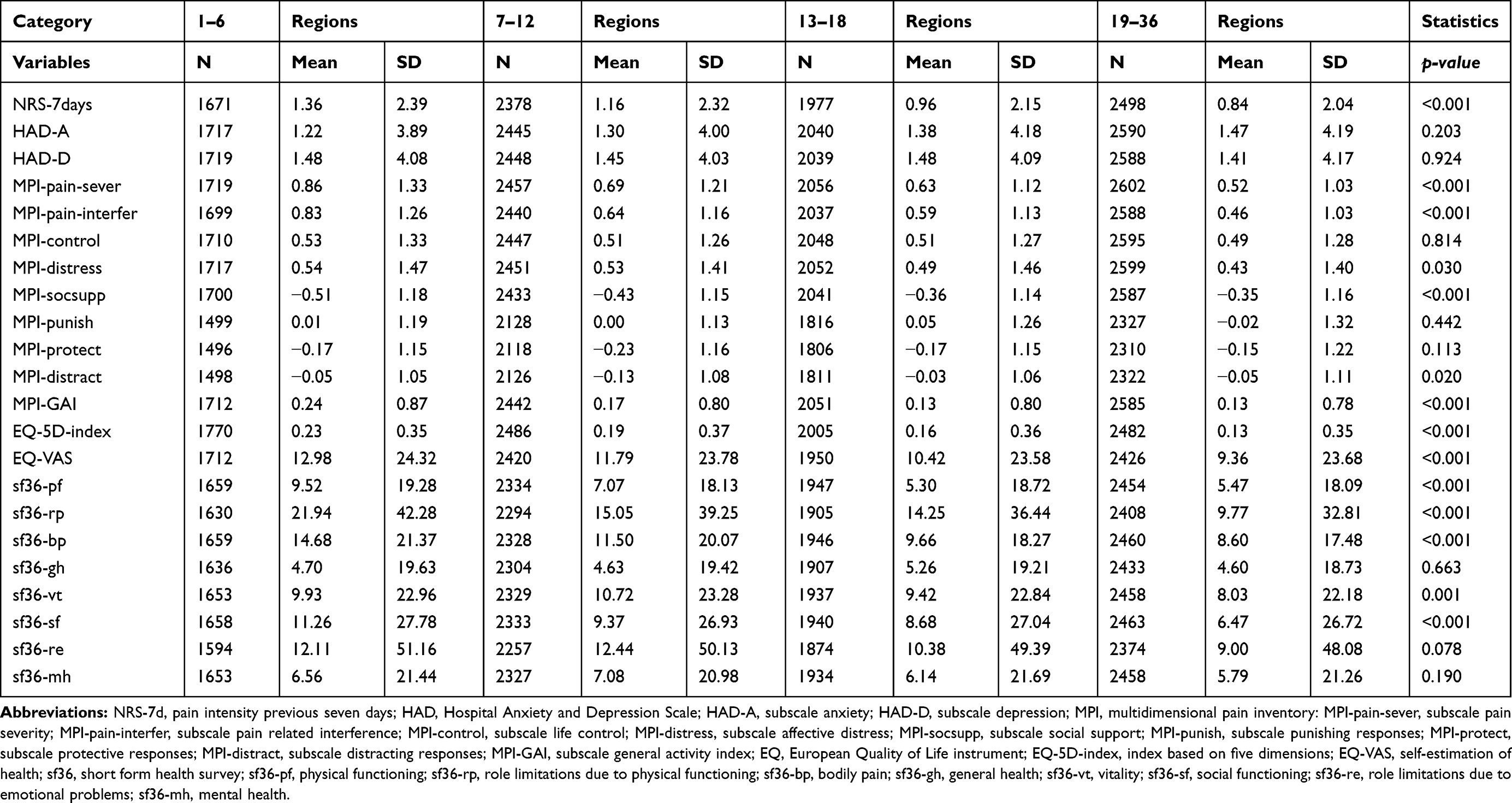 |
Table 4 Changes in the 22 Mandatory Outcome Variables Pre vs 12-month Follow-up (Mean and Standard Deviation; a Positive Value Indicates Improvement) by the Four Categories Based on Spreading of Pain. Group Comparison (ANOVA, p-value) are to the Far Right |
For the change-pain variable, significant differences across the four groups were found at post-IMMRP and at the 12-month follow-up. Fewest patients were classified as improved in the group with the most spreading of pain (post-IMMRP: 1–6 regions: 61.6% improved; 7–12 regions: 59.7% improved; 13–18 regions: 56.1% improved; and 19–36 regions: 51.4% improved; χ2=110.3, df=6, p<0.001; 12-month follow-up: 1–6 regions: 62.3%, 7–12 regions: 60.9%, 13–18 regions: 55.0% and 19–36 regions: 49.5%; χ2=99.6, df=6, p<0.001).
For the change-in-life situation variable, significant differences in the proportions classified as improved was found at the 12-month follow-up (but not post-IMMRP) with the smallest proportion in the group with most widespread pain at baseline: 1–6 regions: 77.3%, 7–12 regions: 79.7%, 13–18 regions: 76.4% and 19–36 regions: 73.2% (χ2=44.6, df=6, p<0.001).
Discussion
This study sought to examine whether spreading of pain was associated with clinical presentation and treatment outcome in patients with chronic pain conditions. The main findings of this large cohort study are:
- WSP is associated with a longer pain duration.
- WSP is associated with female gender and a more severe clinical presentation at baseline; the largest effects were found in relation to general health and vitality and moderate effects in relation to pain intensity, pain interference, pain duration, anxiety, depression, quality of life, physical performance, and social functioning.
- WSP is associated with worse outcome at post-IMMRPs and at a 12-month follow-up, but the effects are small, particularly at post-IMMRP.
A relatively high proportion (30.6%) of patients in this large chronic pain cohort reported a considerable spreading of pain (19–36 anatomical regions). At a group level, men reported less spreading of pain than women. This is in line with evidence showing that men seem to recover, ie transit from chronic widespread pain to less spatially distributed pain, to a greater extent than women according to a longitudinal study.26 The reasons for more WSP in women are unclear and multiple and possibly interacting factors (eg biological, psychosocial and cultural factors including gender roles) are probably involved.21,25 The present study also found that individuals with the most WSP were more frequently born outside of Europe, had lower education levels and more health-care seeking. These results align with other studies— both from pain cohorts and from the general population—reporting that spreading of pain is associated with female gender,20,21,24,46 lower education level47,48 and being an immigrant.48,49 Hypothetically, a lower education level may indicate occupational conditions with higher risks for developing pain conditions. This is in line with a population study that found a correlation between a high mechanical workload and job demands and number of pain regions two years later.50 It is possible that patients with low education levels might also apply less effective individual pain approaches that can result in an increased risk WSP.51
An interesting finding in the present study was the considerably longer pain duration in the group with 19–36 pain regions (moderate ES) compared to subjects with more localized pain (1–6 regions). Accordingly, pain duration was a significant regressor on number of anatomical regions with pain in the multivariate model and pain duration was approximately equally important as pain intensity. This finding is in line with cross-sectional studies based on considerably smaller samples.52,53 Results from longitudinal studies (also relatively small) are inconclusive with respect to pain duration as a risk factor for WPS conditions.54,55 There are several reports indicating that WSP develops from local or regional pain conditions;56–59 approximately one fifth of those with a regional pain condition will go on to develop a WSP condition.60 A wide variety of risk factors have been identified for WSP and fibromyalgia. Pain duration was not identified as a risk factor according to a very recent review, but can be “hidden” in other risk factors (eg, age and pre-existing medical conditions).61 The present results indicate that pain duration might be a risk factor for development of WSP, which in turn warrants large longitudinal studies both in pain cohorts and in the general population. If pain duration is confirmed as a risk factor it underscores the need for preventive strategies and interventions in the early chronic stage. The need to develop effective prevention is underlined by the 10–11% prevalence of WSP in the general population, which is associated with high socioeconomic costs.20,21 Some studies report a relatively low reduction of the spreading of pain over time,23,62 but there are also studies indicating a larger transition between different extents of spreading.47,63 The latter may indicate that widespread pain is not as static as previously assumed but instead can deteriorate or improve. The severity of WSP conditions is further underlined by evidence suggesting that fibromyalgia can lead to premature aging in brain areas.64 Moreover, WSP is associated with more somatic comorbidities (eg, cardiovascular diseases and diabetes) which probably contribute to the total burden of disease for patients.25,47,61 Increased mortality in malignancy, cardiovascular and respiratory diseases have also been found.65–67 A factor that might contribute to our results concerning spreading of pain and pain duration is the relation found between pain conditions and time waiting for care. Longer time before seeking care has been reported for patients with WSP conditions (ie, fibromyalgia) compared to other pain conditions,68 but it is currently not known whether this applies to patients registered in the SQRP.
The worst clinical situation at baseline (Table 2) was found in the group with the most WSP (16–19 regions), with a subsequent improved clinical situation correlating with decreased number of pain sites. The effect sizes when comparing the two extreme categories were at least medium for 12 out of the 22 variables. Large ESs were noted for health aspects (sf36-gh and sf36-vt). Moderate ESs were found for pain intensity aspects (NRS-7d, MPI-pain-sever and sf36-bp), psychological distress aspects (HAD-A and HAD-D), interference in daily life (MPI-interfere, MPI-control, sf36-pf) and other health aspects (EQ-VAS). Thus, patients referred to specialist clinics with more WSP can be expected to have a more severe clinical presentation. These results align with studies from pain cohorts and from the general population that report that spreading of pain is associated with higher pain intensity,24,43,69–71 psychological distress and insomnia,52,71 interference in daily life,52 health and quality of life aspects24,47,71 and health-care seeking.47,72
The regression analysis of PRI (ie number of regions with pain) mainly confirmed that a mix of factors were associated with spreading of pain at baseline. Specifically, findings showed that spreading of pain was significantly associated with perceived poor health, high pain intensity, female gender and pain interference. Psychological distress variables were less clearly associated with spreading of pain in this model which is in line with cross-sectional studies showing that psychological distress is more strongly associated with health aspects than with number of anatomical regions with pain.29,73
A recent study showed that a combination of background variables (sex, education level and country of birth) could be used to explain participation rates in IMMRPs in SQRP.19 Although there was a statistically significant difference indicating that patients with more widespread pain participated in IMMRPs less frequently, this difference was very small and was only present in comparison with the two intermediate number of pain sites groups. These findings contrast with findings from a smaller SQRP study that included patients from two clinical university hospital departments (n=1226) which showed that more spatial spreading of pain was positively associated with participation in IMMRPs.74 Reasons for whether patients enter IMMRPs may differ across contexts and this is an important area for future research to address as it could imply that different strategies (dependent upon the clinical setting and population) are needed to increase patient participation in treatment.
Few studies have evaluated whether spreading of pain is associated with treatment outcome for chronic pain (eg, IMMRPs). The present study found that more widespread pain at baseline was related to poorer treatment outcomes at posttreatment and at a 12-month follow-up. Specifically, those with localized pain conditions (1–6 regions) had the best outcomes while those with the most WSP had the worst outcomes. However, ESs were very small at post-IMMRPs and in the small range at the 12-month follow-up. In a recent study from the SQRP, we reported that those with the worst clinical presentation at baseline (according to pain intensity and interference, psychological distress, and life control) benefitted most from IMMRPs.16 In future research, it is important to investigate how spreading of pain interacts with other clinical variables with respect to outcomes of IMMRPs. Worse results in those with the most WSP were also found for change in pain at both time points and for change in life situation at the 12-month follow-up. Taken together, our findings suggest that more research is needed on how to improve the content and duration of IMMRPs.
Most rehabilitation studies about WSP have focused on fibromyalgia, reporting a low to moderate strength of evidence for long-term improvements in this condition.5,75 However, the literature is inconclusive and the reported ES is small to moderate.76 It can be questioned whether the relatively small effects of IMMRPs, both for chronic pain patients and especially for those with widespread pain, are due to an insufficient targeting of neurobiological alterations and other factors such as insomnia and obesity (known risk factors for WSP).61 WSP has also been linked to pain hypersensitivity and in some studies to poor treatment outcomes (for references).77 In WSP, including fibromyalgia, neural alterations (eg, morphological changes in the brain, neuroinflammation, nociception-driven amplification of neural signalling), impaired top-down modulation as well as peripheral alterations (eg, systemic low grade inflammation and nociceptor/muscle alterations) have been reported.78–82 Chronic pain as well as obesity have been linked to systemic low-grade inflammation. Physical activity has anti-inflammatory and positive metabolic effects but may need optimization within IMMRPs.83,84 Understanding the complicated interactions between such neurobiological peripheral and central processes may be fundamental to develop more effective interventions including revised versions of IMMRPs. Undoubtedly, chronic pain, including WSP, is associated with psychological distress and as mentioned in the introduction, IMMRPs are generally based upon psychologicallybased interventions. Even though these and other components of IMMRPs are evidence-based, the summarized effect might not suffice for patients with severe chronic pain conditions. In this study, we show that spreading of pain is one factor to take into account when trying to develop more effective interventions for patients with chronic pain.
Strengths and Limitations
The spreading of pain variable was operationally designed to achieve approximately numerically equal categories. It can be argued that among those with least spreading of pain (1–6 regions), these regions can be distributed over different parts of the body. More fine-grained analyses may increase knowledge in this area and in ongoing research, we will analyze distribution patterns of pain and whether these patterns are linked to clinical presentation and treatment outcome. A strength of the present study is the large nationwide cohort which includes a non-selected flow of chronic patients in real-life settings at specialist clinics. However, the patients represent a selection of the most complex cases and the results cannot simply be generalized to primary care settings. A related limitation is that no rigorous criteria for inclusion in SQRP exist since it is a clinical registry. We used predetermined benchmarks for whether statistically significant differences were clinically important using ESs, which is a strength with respect to clinical interpretation. Although validated and well-known PROM instruments were used, these may be problematic from several points of view in repeated evaluations as discussed elsewhere.85,86,87,88 However, both MIS and the two retrospective overall outcomes (ie, change-pain and change-life situation) generally showed the same pattern. A biopsychosocial approach was used when designing SQRP and selecting the mandatory variables for outcomes, and the MIS variable extracts important information from changes in these outcomes, which is a strength. However, the 22 mandatory variables plus background data results in a large set of variables which complicates inference. In future studies, baseline variables carrying the most information need to be identified to increase interpretation and clinical translation and such work is ongoing in our group.
Conclusions and Clinical Implications
Spreading of pain was clearly associated with a longer pain duration and a more severe clinical presentation at baseline. It was also associated with poorer outcomes of treatment, but the effects were in the small range. We have previously reported that the combination of gender, education level and country of birth are important for clinical presentation and treatment outcome.19 Here we show that spreading of pain, used as a background variable in SQRP, is also important for understanding chronic pain, most clearly as an indicator of severity but also to some extent as a predictor of poor outcome of IMMRPs. The association between WSP and pain duration supports the concept of early intervention as clinically important and an opportunity to possibly change prognosis with conceivable gains for the individual and society. Our results further indicate the need to develop and improve rehabilitation for patients with widespread chronic pain.
Abbreviations
ACT, acceptance commitment therapy; CBT, cognitive behavioral therapy; Change-pain, positive change in pain; Change-life situation, change in ability to handle life situations in general; ES, effect size; EQ-5D, European Quality of Life instrument; EQ-5D-index, index of EQ-5D based on five items; EQ-VAS, health scale of EQ-5D; HADS, Hospital Anxiety and Depression Scale; HADS-A, Hospital Anxiety and Depression Scale—anxiety subscale; HADS-D, Hospital Anxiety and Depression Scale—depression subscale; IASP, the International Association for the Study of Pain; IMMRP, interdisciplinary multimodal pain rehabilitation program; LP, localized pain; MPI, multidimensional pain inventory; MPI-pain-sever, MPI subscale concerning pain severity; MPI-pain-interfer. MPI subscale concerning painrelated interference; MPI-distress, MPI subscale concerning affective distress; MPI-lifecon, MPI subscale concerning life control; MPI-socsupp, MPI subscale concerning social support; MPI-punish, MPI subscale concerning punishing responses; MPI-solict, MPI subscale concerning solicitous responses; MPI-distract, MPI subscale concerning distracting responses; MPI-GAI, MPI subscale general activity index; NRS, numeric rating scale; NRS-7days, average pain intensity the last week; OPLS, orthogonal partial least square regression; Outside-Europe, born outside Europe; PCA, principal component analysis; PRI, pain region index ie, the number of areas with pain (range: 1–36); PROM, patient reported outcome measures; RCT, randomized controlled trial; SQRP, Swedish Quality Registry for Pain Rehabilitation; sf36, short form health survey; sf36-pf, sf36 subscale concerning physical functioning; sf36-rp, sf36 subscale concerning role limitations due to physical functioning; sf36-bp, sf36 subscale concerning bodily pain; sf36-gh, sf36 subscale concerning general health; sf36-vt, sf36 subscale concerning vitality; sf36-sf, sf36 subscale concerning social functioning; sf36-re, sf36 subscale concerning role limitations due to emotional problems; sf36-mh, sf36 subscale concerning mental health; SR, systematic review; University, university education; WSP, widespread pain.
Data Sharing Statement
The datasets generated and analyzed in this study are not publicly available as the Ethical Review Board has not approved the public availability of these data.
Acknowledgment
This study was supported by grants from the Swedish Research Council (2018-02470) and County Council of Östergötland (Research-ALF; LIO-608021). The sponsors had no role in study design, data collection, data analysis, data interpretation, writing of the report, or the decision to submit for publication. The authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Björn Gerdle reports grants from Swedish Research Council and from County Council of Östergötland (Research-ALF), during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. doi:10.1016/j.pain.2003.08.001
2. Kaiser U, Kopkow C, Deckert S, et al. Developing a core outcome-domain set to assessing effectiveness of interdisciplinary multimodal pain therapy: the VAPAIN consensus statement on core outcome-domains. Pain. 2018;159(4):673–683.
3. Bennett M, Closs S. Methodological issues in nonpharmacological trials for chronic pain. Pain Clinical Updates. 2010;18(2):1–6.
4. SBU. Methods for Treatment of Chronic Pain a Systematic Review of the Literature (In Swedish: Metoder För Behandling Av Långvarig Smärta: En Systematisk Litteraturöversikt). Vol. 177. Stockholm: SBU – Swedish Council on Health Technology Assessment; 2006:1–2.
5. SBU. Rehabilitation of Chronic Pain [In Swedish: Rehabilitering Vid Långvarig Smärta. En Systematisk Litteraturöversikt]. Stockholm: SBU – Swedish Council on Health Technology Assessment; 2010.
6. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology. 2008;47(5):670–678.
7. Weiner SS, Nordin M. Prevention and management of chronic back pain. Best Pract Res Clin Rheumatol. 2010;24(2):267–279.
8. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: cochrane systematic review and meta-analysis. BMJ. 2015;350:h444.
9. Norlund A, Ropponen A, Alexanderson K. Multidisciplinary interventions: review of studies of return to work after rehabilitation for low back pain. J Rehabil Med. 2009;41(3):115–121.
10. Busch H, Bodin L, Bergstrom G, Jensen IB. Patterns of sickness absence a decade after pain-related multidisciplinary rehabilitation. Pain. 2011;152(8):1727–1733. doi:10.1016/j.pain.2011.02.004
11. Jensen IB, Busch H, Bodin L, Hagberg J, Nygren Å, Bergstrom G. Cost effectiveness of two rehabilitation programmes for neck and back pain patients: A seven year follow-up. Pain. 2009;142(3):202–208. doi:10.1016/j.pain.2008.12.015
12. Salathe CR, Melloh M, Crawford R, Scherrer S, Boos N, Elfering A. Treatment efficacy, clinical utility, and cost-effectiveness of multidisciplinary biopsychosocial rehabilitation treatments for persistent low back pain: a systematic review. Global Spine j. 2018;8(8):872–886. doi:10.1177/2192568218765483
13. Casey MB, Smart KM, Segurado R. Multidisciplinary-based Rehabilitation (MBR) compared with active physical interventions for pain and disability in adults with chronic pain: a systematic review and meta-analysis. Clin J Pain. 2020;36(11):874–886.
14. Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ. 2008;336(7656):1281–1283.
15. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. BMJ. 2008;337:a1655.
16. Gerdle B, Akerblom S, Brodda Jansen G, et al. Who benefits from multimodal rehabilitation - an exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish quality registry for pain rehabilitation. J Pain Res. 2019;12:891–908.
17. Gerdle B, Åkerblom S, Stålnacke B-M, et al. The importance of emotional distress, cognitive behavioural factors and pain for life impact at baseline and for outcomes after rehabilitation – a SQRP study of more than 20 000 chronic pain patients. Scand J Pain. 2019;19(4):693–711.
18. Ringqvist Å, Dragioti E, Björk M, Larsson B, Gerdle B. Moderate and stable pain reductions as a result of Interdisciplinary Pain Rehabilitation – a cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J Clin Med. 2019;8:905.
19. Gerdle B, Boersma K, Asenlof P, Stalnacke BM, Larsson B, Ringqvist A. Influences of sex, education, and country of birth on clinical presentations and overall outcomes of interdisciplinary pain rehabilitation in chronic pain patients: a cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J Clin Med. 2020;9(8):2374.
20. Mansfield KE, Sim J, Jordan JL, Jordan KP. A systematic review and meta-analysis of the prevalence of chronic widespread pain in the general population. Pain. 2016;157(1):55–64.
21. Andrews P, Steultjens M, Riskowski J. Chronic widespread pain prevalence in the general population: A systematic review. Eur J Pain. 2018;22(1):5–18.
22. Wang M, Ropponen A, Narusyte J, et al. Adverse outcomes of chronic widespread pain and common mental disorders in individuals with sickness absence - a prospective study of Swedish twins. BMC Public Health. 2020;20(1):1301.
23. Andersson HI. The course of non-malignant chronic pain: a 12-year follow-up of a cohort from the general population. Eur J Pain. 2004;8(1):47–53.
24. Dragioti E, Larsson B, Bernfort L, Levin LA, Gerdle B. A cross-sectional study of factors associated with the number of anatomical pain sites in an actual elderly general population: results from the PainS65+ cohort. J Pain Res. 2017;(10):2009–2019.
25. Dragioti E, Larsson B, Bernfort L, Levin LA, Gerdle B. Prevalence of different pain categories based on pain spreading on the bodies of older adults in Sweden: a descriptive-level and multilevel association with demographics, comorbidities, medications, and certain lifestyle factors (PainS65+). J Pain Res. 2016;9:1131–1141.
26. Sylwander C, Larsson I, Andersson M, Bergman S. The impact of chronic widespread pain on health status and long-term health predictors: a general population cohort study. BMC Musculoskelet Disord. 2020;21(1):36.
27. Mundal I, Grawe RW, Bjorngaard JH, Linaker OM, Fors EA. Prevalence and long-term predictors of persistent chronic widespread pain in the general population in an 11-year prospective study: the HUNT study. BMC Musculoskelet Disord. 2014;15:213.
28. Krause SJ, Tait RC, Margolis RB. Pain distribution, intensity, and duration in patients with chronic pain. J Pain Symptom Manage. 1989;4(2):67–71.
29. Bromley Milton M, Borsbo B, Rovner G, Lundgren-Nilsson A, Stibrant-Sunnerhagen K, Gerdle B. Is pain intensity really that important to assess in chronic pain patients? A study based on the Swedish Quality Registry for Pain Rehabilitation (SQRP). PLoS One. 2013;8(6):e65483.
30. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19.
31. Rovner GS, Sunnerhagen KS, Bjorkdahl A, et al. Chronic pain and sex-differences; women accept and move, while men feel blue. PLoS One. 2017;12(4):e0175737.
32. Bernfort L, Gerdle B, Husberg M, Levin LA. People in states worse than dead according to the EQ-5D UK value set: would they rather be dead? Qual Life Res. 2018;27(7):1827–1833.
33. Turk DC, Rudy TE. Toward an empirically derived taxonomy of chronic pain patients: integration of psychological assessment data. J Consult Clin Psychol. 1988;56(2):233–238.
34. Turk DC, Rudy TE. Towards a comprehensive assessment of chronic pain patients. Behav Res Ther. 1987;25(4):237–249.
35. Bergström G, Jensen IB, Bodin L, Linton SJ, Nygren AL, Carlsson SG. Reliability and factor structure of the multidimensional pain inventory–swedish language version (MPI-S). Pain. 1998;75(1):101–110.
36. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370.
37. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77.
38. Sullivan M, Karlsson J, Ware J. The Swedish 36 Health survey. Evaluation of data quality, scaling assumption, reliability and construct validity across general populations in Sweden. Soc Sci Med. 1995;41:1349–1358.
39. EuroQol. EuroQol: a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199–208.
40. Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72.
41. Dolan P, Sutton M. Mapping visual analogue scale health state valuations onto standard gamble and time trade-off values. Soc Sci Med. 1997;44(10):1519–1530.
42. Gerdle B, Molander P, Stenberg G, Stalnacke BM, Enthoven P. Weak outcome predictors of multimodal rehabilitation at one-year follow-up in patients with chronic pain-a practice based evidence study from two SQRP centres. BMC Musculoskelet Disord. 2016;17(1):490.
43. Backryd E, Persson EB, Larsson AI, Fischer MR, Gerdle B. Chronic pain patients can be classified into four groups: clustering-based discriminant analysis of psychometric data from 4665 patients referred to a multidisciplinary pain centre (a SQRP study). PLoS One. 2018;13(2):e0192623.
44. Wheelock AM, Wheelock CE. Trials and tribulations of ‘omics data analysis: assessing quality of SIMCA-based multivariate models using examples from pulmonary medicine. Mol Biosyst. 2013;9(11):2589–2596.
45. Eriksson L, Byrne T, Johansson E, Trygg J, Vikström C Multi- and Megavariate Data Analysis: Basic Principles and Applications.
46. Westergren H, Larsson J, Freeman M, Carlsson A, Joud A, Malmstrom EM. Sex-based differences in pain distribution in a cohort of patients with persistent post-traumatic neck pain. Disabil Rehabil. 2018;40(9):1085–1091.
47. Grimby-Ekman A, Gerdle B, Bjork J, Larsson B. Comorbidities, intensity, frequency and duration of pain, daily functioning and health care seeking in local, regional, and widespread pain - a descriptive population-based survey (SwePain). BMC Musculoskelet Disord. 2015;16:165.
48. Larsson B, Dragioti E, Grimby-Ekman A, Gerdle B, Bjork J. Predictors of chronic pain intensity, spread, and sensitivity in the general population: A two-year follow-up study from the SWEPAIN cohort. J Rehabil Med. 2019;51(3):183–192.
49. Bergman S, Herrstrom P, Hogstrom K, Petersson IF, Svensson B, Jacobsson LT. Chronic musculoskeletal pain, prevalence rates, and sociodemographic associations in a Swedish population study. J Rheumatol. 2001;28(6):1369–1377.
50. Dragioti E, Gerdle B, Larsson B. Longitudinal associations between anatomical regions of pain and work conditions: A Study from The SwePain Cohort. Int J Environ Res Public Health. 2019;16(12):2167.
51. Cano A, Mayo A, Ventimiglia M. Coping, pain severity, interference, and disability: the potential mediating and moderating roles of race and education. j Pain. 2006;7(7):459–468.
52. Alfoldi P, Dragioti E, Wiklund T, Gerdle B. Spreading of pain and insomnia in patients with chronic pain: results from a national quality registry (SQRP). J Rehabil Med. 2017;49(1):63–70.
53. Viniol A, Jegan N, Leonhardt C, et al. Differences between patients with chronic widespread pain and local chronic low back pain in primary care–a comparative cross-sectional analysis. BMC Musculoskelet Disord. 2013;14:351.
54. Kindler LL, Jones KD, Perrin N, Bennett RM. Risk factors predicting the development of widespread pain from chronic back or neck pain. J Pain. 2010;11(12):1320–1328.
55. Forseth KO, Husby G, Gran JT, Forre O. Prognostic factors for the development of fibromyalgia in women with self-reported musculoskeletal pain. A prospective study. J Rheumatol. 1999;26(11):2458–2467.
56. Lapossy E, Maleitzke R, Hrycaj P, Mennet W, Muller W. The frequency of transition of chronic low back pain to fibromyalgia. Scand J Rheumatol. 1995;24(1):29–33.
57. Buskila D, Neumann L, Vaisberg G, Alkalay D, Wolfe F. Increased rates of fibromyalgia following cervical spine injury. A controlled study of 161 cases of traumatic injury. Arthritis Rheumatology. 1997;40((3)):446–452.
58. Larsson B, Balogh I. Is there a relationship between fibromyalgia syndrome and work conditions? J Musculoskelet Pain. 2005;13(4):5–14.
59. Bergman S, Thorstensson C, Andersson MLE. Chronic widespread pain and its associations with quality of life and function at a 20- year follow-up of individuals with chronic knee pain at inclusion. BMC Musculoskelet Disord. 2019;20(1):592.
60. Larsson B, Björk J, Börsbo B, Gerdle B. A systematic review of risk factors associated with transitioning from regional musculoskeletal pain to chronic widespread pain. European J Pain. 2012;16(8):1084–1093.
61. Creed F. A review of the incidence and risk factors for fibromyalgia and chronic widespread pain in population-based studies. Pain. 2020;161(6):1169–1176.
62. Mogard E, Lindqvist E, Bremander A, Bergman S. Risk factors for development and persistence of chronic widespread pain in spondyloarthritis: a population-based two-year follow-up study. Scand J Rheumatol. 2019;48(6):460–468.
63. Bergman S, Jacobsson LT, Herrstrom P, Petersson IF. Health status as measured by SF-36 reflects changes and predicts outcome in chronic musculoskeletal pain: a 3-year follow up study in the general population. Pain. 2004;108(1–2):115–123.
64. Villafaina S, Collado-Mateo D, Fuentes-Garcia JP, Dominguez-Munoz FJ, Gusi N. Duration of the symptoms and brain aging in women with fibromyalgia: a cross-sectional study. Appl Sci-Basel. 2019;9(10):2106.
65. McBeth J, Symmons DP, Silman AJ, et al. Musculoskeletal pain is associated with a long-term increased risk of cancer and cardiovascular-related mortality. Rheumatology. 2009;48(1):74–77.
66. Macfarlane GJ, Barnish MS, Jones GT. Persons with chronic widespread pain experience excess mortality: longitudinal results from UK Biobank and meta-analysis. Ann Rheum Dis. 2017;76(11):1815–1822.
67. Tesarz J, Eich W, Baumeister D, Kohlmann T, D’Agostino R, Schuster AK. Widespread pain is a risk factor for cardiovascular mortality: results from the Framingham Heart Study. Eur Heart J. 2019;40(20):1609–1617.
68. Deslauriers S, Roy JS, Bernatsky S, et al. Factors associated with waiting times for persons with rheumatic conditions in multidisciplinary pain treatment facilities. J Pain Res. 2019;12:2379–2390.
69. Lundberg G, Gerdle B. The relationships between pain, disability, and health-related quality of life: an 8-year follow-up study of female home care personnel. Disabil Rehabil. 2016;38(3):235–244.
70. Ektor-Andersen J, Isacsson SO, Lindgren A, Orbaek P. The experience of pain from the shoulder-neck area related to the total body pain, self-experienced health and mental distress. The Malmo Shoulder-Neck Study group. Pain. 1999;82(3):289–295.
71. Peolsson M, Borsbo B, Gerdle B. Generalized pain is associated with more negative consequences than local or regional pain: a study of chronic whiplash-associated disorders. J Rehabil Med. 2007;39(3):260–268.
72. Jordan KP, Kadam UT, Hayward R, Porcheret M, Young C, Croft P. Annual consultation prevalence of regional musculoskeletal problems in primary care: an observational study. BMC Musculoskelet Disord. 2010;11:144.
73. Molander P, Dong H-J, Äng B, Enthoven P, Gerdle B. The role of pain in chronic pain patients’ perception of health-related quality of life: a cross-sectional SQRP study of 40 000 patients. Scand J Pain. 2018;18(3):417–429.
74. Enthoven P, Molander P, Oberg B, Stalnacke BM, Stenberg G, Gerdle B. Do pain characteristics guide selection for multimodal pain rehabilitation? J Rehabil Med. 2017;49(2):161–169.
75. Skelly A, Chou R, Dettori J, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018.
76. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76(2):318–328.
77. Larsson B, Gerdle B, Bjork J, Grimby-Ekman A. Pain sensitivity and its relation to spreading on the body, intensity, frequency, and duration of pain: a cross-sectional population-based study (SwePain). Clin J Pain. 2017;33(7):579–587.
78. Albrecht DS, Forsberg A, Sandstrom A, et al. Brain glial activation in fibromyalgia - A multi-site positron emission tomography investigation. Brain Behav Immun. 2019;75:72–83.
79. Gerdle B, Larsson B. Muscle. In: Häuser W, Perrot S, editors. Fibromyalgia Syndrome and Widespread Pain – From Construction to Relevant Recognition. Wolters Kluwer, Philadelphia; 2018:215–231.
80. Jensen KB, Kosek E, Petzke F, et al. Evidence of dysfunctional pain inhibition in Fibromyalgia reflected in rACC during provoked pain. Pain. 2009;144(1–2):95–100.
81. Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience. 2016;338:114–129.
82. Üçeyler N, Sommer C. Small nerve fiber pathology. In: Häuser W, Perrot S, editors. Fibromyalgia Syndrome and Widespread Pain - from Construction to Relevant Recognition. Philadelphia: Wolters Kluwer; 2018:204–214.
83. Sharif K, Watad A, Bragazzi NL, Lichtbroun M, Amital H, Shoenfeld Y. Physical activity and autoimmune diseases: get moving and manage the disease. Autoimmun Rev. 2018;17(1):53–72.
84. Padrao AI, Ferreira R, Amado F, Vitorino R, Duarte JA. Uncovering the exercise-related proteome signature in skeletal muscle. Proteomics. 2016;16(5):816–830.
85. Westlander G. Refined use of standardized self-reporting in intervention studies (In swedish: förfinad användning av standardiserad självrapportering i interventionstudier). Socialvetenskaplig Tidskrift. 2004;(2):168–181.
86. Pina-Sánchez J, Koskinen J, Plewis I. Measurement Error in Retrospective Reports of Unemployment. Manchester, UK: The Cathie Marsh Centre for Census and Survey Research, University of Manchester; 2012.
87. Bernard H, Killworth P, Kronenfeld D, Sailer L. The problem of informant accuracy: the validity of retrospective data. Ann Rev Anthropol. 1984;13:495–517.
88. Van der Vaart W, Van der Zouwen J, Dijkstra W. Retrospective questions: data quality, task difficulty and the use of checklist. Qual Quant. 1995;29:299–315.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.