")
Back to Journals » International Journal of Women's Health » Volume 10
Spotlight on the utility of the Oncotype DX® breast cancer assay
Authors Siow ZR, De Boer RH, Lindeman GJ , Mann GB
Received 14 September 2017
Accepted for publication 6 December 2017
Published 21 February 2018 Volume 2018:10 Pages 89—100
DOI https://doi.org/10.2147/IJWH.S124520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Zhen Rong Siow,1–3 Richard H De Boer,2,3 Geoffrey J Lindeman,1–4 G Bruce Mann2–4
1ACRF Stem Cells and Cancer Division, Walter and Eliza Hall Institute of Medical Research, 2Department of Medical Oncology, Peter MacCallum Cancer Centre, 3Familial Cancer Centre, The Royal Melbourne Hospital, 4Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Parkville, VIC, Australia
Abstract: The Oncotype DX® assay was developed to address the need for optimizing the selection of adjuvant systemic therapy for patients with estrogen receptor (ER)-positive, lymph node-negative breast cancer. It has ushered in the era of genomic-based personalized cancer care for ER-positive primary breast cancer and is now widely utilized in various parts of the world. Together with several other genomic assays, Oncotype DX has been incorporated into clinical practice guidelines on biomarker use to guide treatment decisions. The Oncotype DX result is presented as the recurrence score which is a continuous score that predicts the risk of distant disease recurrence. The assay, which provides information on clinicopathological factors, has been validated for use in the prognostication and prediction of degree of adjuvant chemotherapy benefit in both lymph node-positive and lymph node-negative early breast cancers. Clinical studies have consistently shown that the Oncotype DX has a significant impact on decision making in adjuvant therapy recommendations and appears to be cost-effective in diverse health care settings. In this article, we provide an overview of the validation and clinical impact studies for the Oncotype DX assay. We also discuss its potential use in the neoadjuvant setting, as well as the more recent prospective validation trials, and the economic and utility implications of studies that use a lower cutoff score to define low-risk disease.
Keywords: breast cancer, adjuvant, Oncotype DX®, recurrence score, utility
Background
Breast cancer is the most common malignancy in females worldwide.1 The widespread use of adjuvant chemotherapy in patients diagnosed with early-stage estrogen receptor (ER)-positive breast cancer has contributed to the reduction of breast cancer-related mortality,2,3 and the estimated absolute risk reduction is between 5 and 15%.2,3 However, not all patients benefit equally from adjuvant chemotherapy. The absolute risk reduction in ER-positive and lymph node-negative disease may be modest (~5%).4,5 Methods to identify and select patients who benefit most and those who benefit little from chemotherapy are important to reduce unnecessary exposure to cytotoxic therapies and their associated side effects.6 The decision to recommend adjuvant chemotherapy in ER-positive/human epidermal growth factor receptor 2 (HER2)-negative early breast cancer is complex and is conventionally based on clinicopathological factors of the tumor in conjunction with clinician and patient’s preference. Clinicopathological factors include the tumor size, nuclear grade, level of hormone receptor positivity, and Ki-67.7–9 Ki-67 is a protein used as a marker for cellular proliferation and has been shown to be an independent prognostic parameter in breast cancer. It is most commonly assessed via immunohistochemistry.10,11 In addition, population-based recurrence calculators (eg, Adjuvant! Online and PREDICT) are utilized to provide an estimate of the recurrence risk and the magnitude of benefit from the addition of chemotherapy to endocrine therapy.9,12,13 However, there exists a high degree of discordance in pathology report parameters, especially of nuclear grade5,14,15 and Ki-67 scores.16,17 Furthermore, standard clinicopathological features have suboptimal prognostic and predictive utilities in predicting chemotherapy benefit.18 Thus, a more precise method for stratifying poor versus good prognosis patients and for predicting responders versus nonresponders to therapy (including chemotherapy) remained an area of need.
One of the tools developed to enable this stratification was the multigene assay. This was developed to overcome some of the inconsistencies associated with routine pathology and to address the need for personalized prognostication and prediction of chemotherapy benefit. Soonmyung Paik, the pathologist who contributed to the development of Oncotype DX® (Genomic Health Inc., Redwood City, CA, USA), noted that he developed the multi-gene assay as a result of his frustration with the lack of reproducibility of histological grading and the apparent lack of reliability of community-based HER2 testing during the conduct of a multicenter clinical trial.19
Gene expression profiles
There are a number of other commercially available genomic assays including EndoPredict® (EP; Myriad Genetics, Salt Late City, UT, USA), Breast Cancer Index (BCI; Biotheranostics, San Diego, CA, USA), Predictor Analysis of Microarray 50 (PAM50; NanoString Technologies, Seattle, WA, USA), and MammaPrint® (Agendia, Amsterdam, the Netherlands). Although evidence suggests that these assays are all prognostic, each of the assays can potentially report discordant results for the same individual patient.20,21 Hence, only one genomic assay should be recommended for any one patient.
EP is an 11-gene RNA-based assay that can be performed in local laboratories. The EP classifies tumors into high- and low-risk categories and can also be combined with tumor size and nodal status to derive the EPclin.22 EPclin can potentially reduce the use of adjuvant chemotherapy by identifying patients with a good prognosis that would have been classified as intermediate- or high-risk based on clinicopathological criteria, and spares the use of chemotherapy in this group.23 The EPclin has been shown to be able to accurately prognosticate recurrence risk up to 10 years.24
The BCI combines two biomarkers (HOXB13:IL17BR ratio and Molecular Grade Index) to derive the BCI score. This assay is performed at a central laboratory. The BCI score has been validated to provide prognostic information in addition to Adjuvant! Online.25 The BCI linear (BCI-L) model was also found to be strongly prognostic of both early and late recurrences, and its strength may be the ability to identify patients at risk of late recurrence as candidates for extended endocrine therapy.26
PAM50 is a 50-gene test. As it is based on NanoString® messenger RNA (mRNA) expression, it can be performed in local laboratories. It reports the risk of recurrence score (ROR) that classifies tumors into high, medium, and low groups and provides prognostic information independent of traditional clinicopathological factors in node-negative disease27 and is approved for risk estimation of ER-positive stage I/II breast cancer (up to three nodes) in postmenopausal women treated with endocrine therapy.
The Amsterdam 70-gene profile (MammaPrint) is a test performed at a central laboratory. Originally designed for unfixed tissue, it has recently been adapted to formalin-fixed tissue. It classifies tumors into low- and high-risk categories. The Microarray in Node-Negative Disease May Avoid Chemotherapy (MINDACT) trial reported that women with a high-clinical-risk and low-risk MammaPrint result had a risk of distant metastases only 1.5% higher at 5 years without chemotherapy, suggesting that these patients can potentially forgo chemotherapy.28
Although all of the assays are prognostic, at this point, only the Oncotype DX has been directly validated as a tool to predict benefit from the addition of chemotherapy.
The Oncotype DX assay
The Oncotype DX assay was first described in 2004 and was introduced into clinical practice shortly after this. The assay was originally developed by selecting 250 promising candidate genes from the literature and quantifying their expression by reverse transcriptase polymerase chain reaction (RT-PCR), using mRNA extracted from formalin-fixed paraffin-embedded tumors of 447 patients from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-20 study.29 Sixteen cancer-related genes were selected based on their statistical association between gene expression and distant breast cancer recurrence. The selected genes reflect distinct biological activities that can be grouped into estrogen signaling, proliferation, HER2 amplification, invasion, tumor-associated macrophages (CD68), detoxification (GTSM1), and chaperone protein binding (BAG-1, a co-chaperone for HSP70 that also acts as a nucleotide-exchange factor and is linked to increased BCL-2 expression). The 16 genes were combined with five reference “house keeping” genes (Figure 1) and an algorithm to produce the recurrence score (RS). The RS ranges from 0–100, where higher scores indicate a higher probability of distant recurrence at 10 years in patients treated with adjuvant tamoxifen therapy alone.29 The cutoff points were prespecified into low-risk (<18), intermediate-risk (18–30), and high-risk (≥31). These score ranges were chosen based on the results of the NSABP B-20 study.29
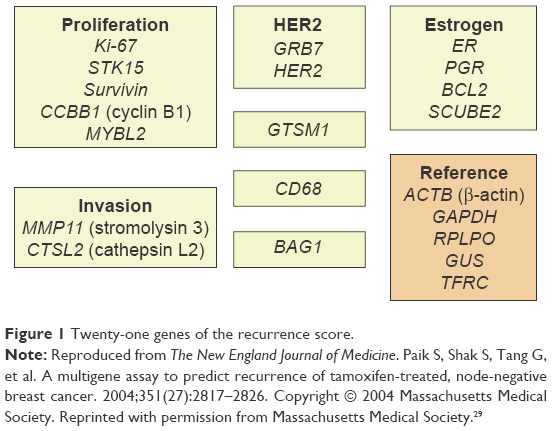 | Figure 1 Twenty-one genes of the recurrence score. |
Since being introduced into clinical practice, major oncology societies and entities including the American Society of Clinical Oncology (ASCO®), the National Comprehensive Cancer Network (NCCN®), the European Society for Medical Oncology (ESMO), the National Institute for Health and Care Excellence, and the St Gallen Consensus Conference have included Oncotype DX into their breast cancer guidelines.30–34 While initially validated in ER-positive and node-negative breast cancer, the utility of Oncotype DX has since been explored in other cohorts, as described later.
Lymph node-negative early breast cancer
The majority of validation studies for Oncotype DX are retrospective in nature, in which archival tissue from patients who had participated in large prospective randomized adjuvant trials was analyzed to determine the RS and its correlation with known outcomes (Table 1).
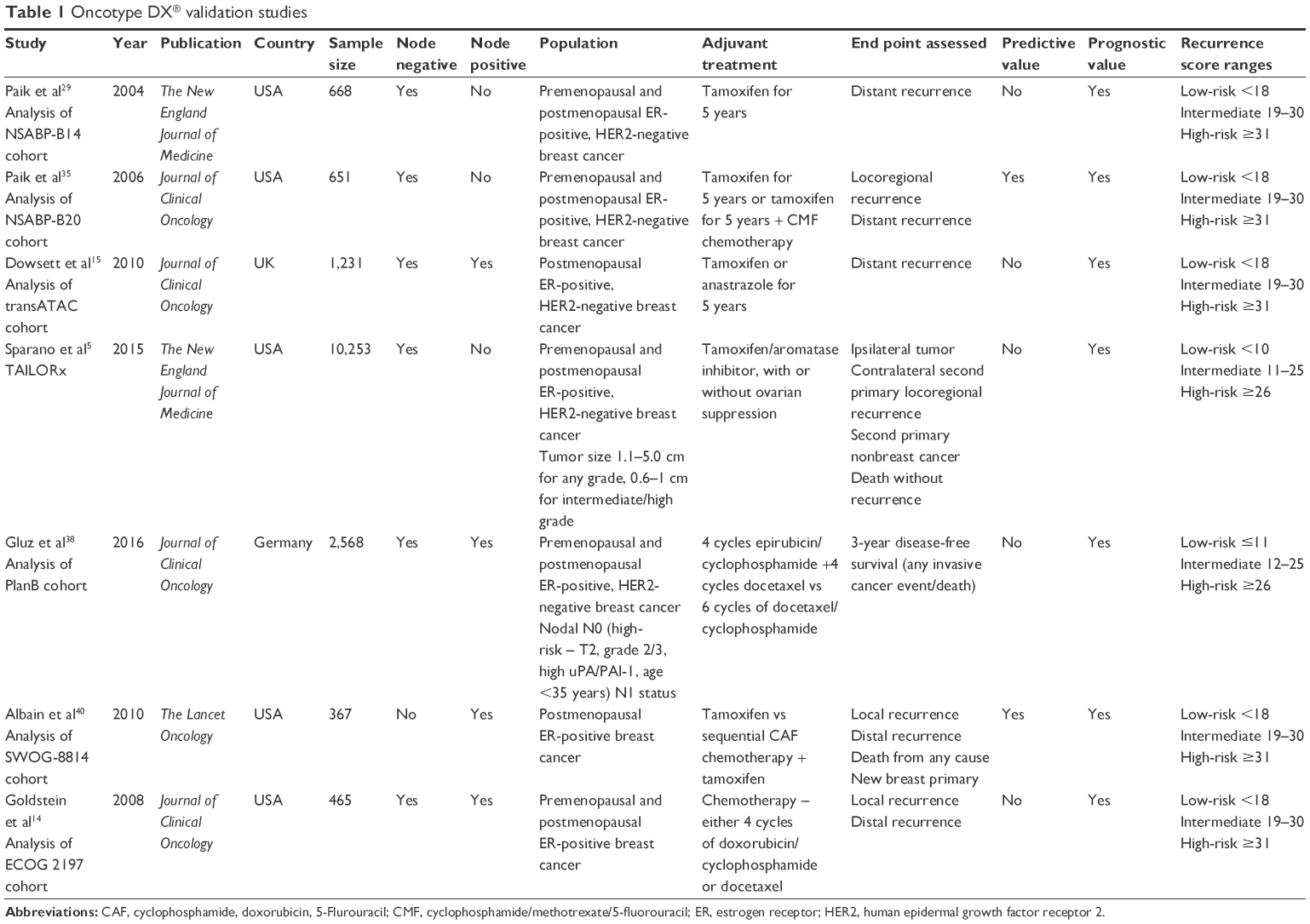 | Table 1 Oncotype DX® validation studies |
The RS is well validated in prognosticating the risk of distant recurrence at 10 years. Paik et al performed an analysis of a prospectively defined RS on archival cancer tissue samples of the NSABP B-14 trial participants. The NSABP B-14 study was originally designed to assess the effects of 5 years of adjuvant tamoxifen without chemotherapy in patients with resected node-negative, ER-positive breast cancer. The RS cutoff range was <18, 18–30, and ≥31 for low-risk, intermediate-risk, and high-risk, respectively. The primary objectives of the analysis were to determine whether the proportion of patients who were free of distant recurrence for >10 years was significantly greater in the low-risk group vs the high-risk group as defined by the RS, as well as to determine the relationship between the RS and the risk of distant recurrence. Secondary end points were relapse-free survival and 10-year all-cause mortality.29 A total of 668 tumor samples were successfully analyzed. Patients with low-risk RS had a significantly lower rate of distant recurrence at 10 years (6.8%) when compared with patients with intermediate-risk (14.3%) and high-risk (30.5%). These findings appeared to predict recurrence, independently of other factors, including age, tumor size, and grade. The analysis also demonstrated that the likelihood of distant recurrence at 10 years increased continuously as the RS increased. The RS was able to predict relapse-free survival and overall survival, although 50% of these deaths were not breast cancer related.29
The translational protocol of the Arimidex, Tamoxifen, alone, or in Combination (transATAC) trial further validated the prognostic value of the RS in patients who received adjuvant endocrine therapy. A high-risk RS was associated with a higher likelihood of disease relapse (for node negative – hazard ratio [HR] 5.2, 95% confidence interval [CI] 2.7–10.1; for node positive – HR 2.7, 95% CI 1.5–5.1). The 9-year distant relapse risk in node-negative patients for the low-risk, intermediate-risk and high-risk RS categories was 4, 12, and 25%, while the overall survival for the low-risk, intermediate-risk and high-risk RS categories in node-negative patients was 88, 84, and 73%, respectively.15
The RS is also validated to predict the magnitude of chemotherapy benefit,35 and from a clinical perspective, this may be its strongest benefit. The NSABP B-20 cohort comprised patients with node-negative and ER-positive breast cancer. A total of 227 of the 651 patients were treated with tamoxifen alone, while 424 patients received chemotherapy (cyclophosphamide/methotrexate/5-fluorouracil [CMF] or methotrexate/5-fluorouracil [MF] with tamoxifen). The Kaplan–Meier analysis showed benefit of including chemotherapy (distant recurrence-free survival 92.2 vs 87.8%; overall survival 89.5 vs 86.4%). However, if the outcomes were separated according to RS, patients did not benefit equally from chemotherapy. Patients with a high-risk RS (≥31) derived significant benefit, with their 10-year distant relapse-free survival improving from 60 to 88% (relative risk 0.26 [95% CI 0.13–0.53]). Patients with a low-risk RS (<18) did not derive benefit (relative risk 1.31 [95% CI 0.46–3.78]). For the intermediate group (18–30), the benefits of chemotherapy were less clear, although it appeared that they did not derive a significant benefit (relative risk 0.61 [95% CI 0.24–1.59]). A cutoff point at which there was a clear benefit of chemotherapy could not be accurately defined.35 Of note, CMF is no longer as commonly used as an adjuvant regimen. Third-generation anthracycline- and taxane-based chemotherapy regimens have been shown to provide more benefit and so have replaced it with the preferred regimen.36,37 It is likely that NSABP B-20 underestimates the benefit of third-generation chemotherapy regimens in patients with a high RS.
The Trial Assigning Individualized Options for Treatment (TAILORx) aims to validate the RS prospectively.5 This study recruited 10,273 node-negative patients with hormone receptor-positive and HER2-negative breast cancer. The RS determined the recommended adjuvant therapy. Of note, cutoff scores for the respective risk groups were different from earlier studies (low-risk ≤10, intermediate 11–25, and high-risk ≥26). This decision to change the cutoff scores was based on clinical consensus. The primary end point was disease-free survival (DFS). Only the intermediate-risk patients underwent randomization of treatment. Low-risk patients were recommended endocrine therapy alone, while high-risk patients were recommended chemotherapy in combination with endocrine therapy. Results for the low-risk RS has been reported, while the data for the intermediate- and high-risk RS cohorts are awaited. A total of 1,629 patients (15.9% of the trial population) had a low-risk RS. This group had an excellent 5-year overall survival (98.0%, 95% CI 97.1–98.6) and freedom from recurrence (98.7%, 95% CI 97.9%–99.2%) on endocrine therapy alone.5 Importantly, 31% of these patients had primary tumors >2 cm and 7% were high grade. The TAILORx trial provides prospective evidence to support omitting chemotherapy in patients with low-risk RS. However, the selected cutoff of the RS (≤10) was different to that of the original studies (<18).5 In addition, the 5-year follow-up period is currently shorter than earlier analyses (NSABP B-14, B-20). The majority of patients enrolled in the study had an intermediate-risk score, and outcomes for the intermediate- and high-risk RS groups are eagerly awaited.
PlanB originally compared anthracycline-containing and anthracycline-free chemotherapy regimens (4 cycles of epirubicin/cyclophosphamide [EC] followed by 4 cycles of docetaxel vs 6 cycles of docetaxel/cyclophosphamide [TC]) in patients clearly “requiring” chemotherapy. Shortly after recruitment, an amendment recommended the omission of chemotherapy for patients with a low RS (≤11). This amendment resulted in PlanB being the first reported prospective chemotherapy trial where patients were treated according to the RS. The choice of a lower RS cutoff score was similar to TAILORx. The primary objective of the translational component of this study was to compare the independent prospective central pathology review and assessment of immunohistochemistry markers with RS and local pathology. The RS was available for 2,568 hormone receptor-positive patients. In 348 patients (14%) with RS ≤11, chemotherapy was omitted. Despite this group containing patients with adverse clinicopathological risk factors including node-positive disease (31.4%) and grade 3 tumors (20%), patients with RS ≤11 had an excellent 3-year DFS (98%) without chemotherapy. As expected, the 3-year DFS was substantially poorer for patients with RS >25. This study highlights the high discordance rate between clinicopathological parameters between different pathologists (nuclear grade discordance of 44%) and emphasized that RS can serve to standardize assessment information and improve treatment consistency.38 Although PlanB provides important prospective validation of the RS (including in node-positive disease), the current short follow-up limits the ability to draw concrete conclusions. Updated results showing a 5-year DFS of 94% for both the low-risk group treated with endocrine therapy alone and the intermediate-risk group treated with endocrine therapy and adjuvant chemotherapy were subsequently presented at the European Breast Cancer Conference.39 Unlike TAILORx, PlanB did not randomize the cohort of intermediate-risk patients to endocrine therapy alone vs endocrine with chemotherapy. Creating the randomized cohort would have been complex, given that the RS was introduced after the trial started recruiting. Thus, there remains the ongoing uncertainty on the optimal treatment for patients with an intermediate RS, which will hopefully be addressed by TAILORx.
Lymph node-positive early breast cancer
Evidence for the utility of the RS in node-positive disease is less robust than in the node-negative population. Data to guide clinical use of the RS in this population are mostly derived from retrospective analysis of node-positive patient subgroups from larger trials. As a result, recommendations by major cancer associations currently differ with ASCO recommending Oncotype DX for node-negative patients only,30 while NCCN recommends Oncotype DX for patients with limited node positivity (1–3 involved nodes).31
A total of 25% of the transATAC study’s population (306) had node-positive disease. Of these, 79% had 1–3 positive nodes.15 Overall, for the node-positive cohort, the rate of disease recurrence at 9 years was 17, 28 and 49% for RS <18, RS 18–30, and RS ≥31, respectively. In all groups, the RS had a continuous relationship with the risk of relapse. Although the group with 1–3 positive lymph nodes had a higher risk of recurrence compared to the node-negative group, the group with ≥4 positive lymph nodes had a markedly elevated risk of recurrence, even if the RS was classified as low-risk (~50% 9-year risk of distal recurrence at an RS score of 18).15 This supports the consensus that RS testing is not of value in patients with >3 positive axillary lymph nodes.
Goldstein et al (2008) performed an analysis of RS on tissue samples from the Eastern Cooperative Oncology Group (ECOG) 2197 cohort. This included both node-positive (limited to 1–3 nodes) and node-negative patients. A total of 16% of tumors were also HER-2 positive. The analysis sought to determine if the RS could more reliably predict outcomes at 5 years than standard clinicopathological factors. The RS was found to be a significant predictor of recurrence in both node-positive and node-negative groups. When compared with patients with node-negative disease, node-positive patients had an increased risk of recurrence. For patients with RS <18, the likelihood of recurrence at 5 years was 3.3% (0–1 node) and 7.9% (2–3 nodes). There was a progressive increase in recurrence risk observed as the RS risk-category increased regardless of nodal status, and there was a continuous correlation between RS and risk of recurrence, up to an RS of ~40. As patients in the analysis received chemotherapy, the lack of correlation above a score of 40 probably reflects on the high degree of chemotherapy benefit in reducing the risk of disease recurrence. However, as the study was restricted to patients who received chemotherapy, it was not possible to determine whether similarly favorable outcomes for the RS <18 group would have been achieved without chemotherapy.14
To date, Oncotype DX remains the only multigene assay validated to predict the likelihood of chemotherapy benefit for node-positive patients. A translational retrospective study on banked tissue of the Southwest Oncology Group (SWOG)-8814 trial was performed to analyze both the prognostic and predictive potential in this node-positive cohort. The RS was performed in patients receiving cyclophosphamide/doxorubicin/5-fluorouracil followed by tamoxifen (CAF-T) chemo-endocrine therapy as well as in the tamoxifen-only group. A small proportion of this group had HER2-positive tumors (11.7% overall for both cohorts). Patients with low-, intermediate-, and high-risk RS had a 10-year DFS of 60, 49, and 43% and a 10-year overall survival of 77, 68, and 51%, respectively. The RS was also a strong predictor of benefit from CAF chemotherapy, where patients with a low-risk (HR 1.02, 95% CI 0.54–1.93) or intermediate-risk (HR 0.72, 95% CI 0.39–1.31) RS did not have a significant benefit from adjuvant chemotherapy. However, in patients with a high-risk score (≥31), there was an improvement in the DFS with the addition of chemotherapy (HR 0.59, 95% CI 0.35–1.01, P=0.033).40 Consistent with the TransATAC results, patients with ≥4 positive lymph nodes had a markedly elevated risk of recurrence when compared with patients with 1–3 positive nodes.40
A total of 35.2% of the PlanB cohort had node-positive disease. A total of 35.2% of the population were pN1 and 4.6% were pN2. Nodal status was found to be prognostic for disease outcomes, but the RS was still able to identify patients who had a better prognosis within this subgroup. For patients with RS <11, the multivariate HR was 2.45 (95% CI 1.42–3.73) comparing groups pN1–3 to pN0; whereas in patients with RS ≥12, the multivariate HR was 2.89 (95% CI 1.59–5.58).24
RxPONDER (SWOG S1007) is a Phase III trial that seeks to determine whether chemotherapy benefits patients with a low-intermediate RS score and to determine whether there is a threshold RS above which patients may benefit from chemotherapy. Patients with hormone receptor-positive, HER2-negative breast cancer with 1–3 positive lymph nodes are being recruited. Patients with an RS of ≤25 will be randomized to chemotherapy (physician’s choice) plus endocrine therapy versus endocrine therapy alone. Patients with an RS of >25 will receive chemotherapy and endocrine therapy and not undergo randomization. Recruitment commenced in 2011 with 10,000 participants planned. The outcomes of this study will provide prospective data on the utility of RS in patients with limited node-positive disease.41
Integrating the RS and clinicopathological factors
Adjuvant! Online is a web-based risk assessment tool designed to provide prognostic estimates of the outcome with and without therapy, based on estimates of an individual patient’s prognosis and the efficacy of different adjuvant therapy options.12 It has been the tool most utilized by clinicians to help in adjuvant chemotherapy decisions and is validated to determine patient outcomes at 10 years based on clinicopathological features.14,42 The transATAC analysis assessed if the RS provided information in addition to Adjuvant! Online.15 Of note, only node-negative patients were included in this analysis. The correlation between distant recurrence risk as determined by RS and Adjuvant! Online was low (Spearman rank correlation =0.22, P<0.001), although both provided a comparable degree of mutually independent predictive information (Δχ2 21.9, P<0.001).15 Another analysis compared an integrator tool (modeled after Adjuvant! but adjusted to 5-year outcomes instead of 10-year outcomes) and the RS from 465 patients from the ECOG 2197 study. However, there was again poor overall concordance between the integrator and RS groups (38%, correlation coefficient 0.19) and the effect of the RS was largely independent of the risk estimated by the integrator. The area under the receiver operator characteristics (ROC) curve was 0.69 for RS and 0.61 for the integrator, suggesting that the RS provided the greater accuracy in predicting recurrence. In addition, the RS was shown to provide additional information on the relative risk of recurrence and provided the most additional discriminatory value in patients estimated to have low/intermediate-risk by the integrator.14
Efforts to integrate clinicopathological factors with the RS have the potential to further refine prediction algorithms for clinical relapse. Tang et al (2011) assessed formal integration of the RS with traditional pathology (age, tumor size, tumor grade, and adjuvant hormonal therapy) in 1,735 patients and assessed the difference between the RS pathology clinical (RSPC) model and RS alone. Compared to the RS alone, the RSPC classified fewer patients in the intermediate-risk group (17.8 vs 26.7%). However, the RSPC score did not show statistically significant interaction with treatment (P=0.10).43 This suggests that while including traditional pathological features in a model may improve the assay’s ability to prognosticate, it does not have a similar impact on the ability to predict response to chemotherapy. While the RSPC calculator is available through Oncotype DX tools on Genomic Health’s website https://online.genomichealth.com/Login.aspx (registration and password required), it has not been clinically validated.44
Taken together, current evidence supports the utility of Oncotype DX for selecting node-negative patients with ER-positive and HER2-negative breast cancer who may benefit from the addition of adjuvant chemotherapy to endocrine therapy and in which patients may omit chemotherapy. The Oncotype DX’s prognostication has not been validated >10 years. It remains difficult to assign a specific RS cutoff at which chemotherapy is deemed to provide meaningful benefit as different studies have utilized different definitions of low-risk, intermediate-risk, and high-risk diseases.5,15,29,35 Recent prospective studies (TAILORx and PlanB) have confirmed that the omission of chemotherapy in node-negative patients with RS <11 is safe,5 but these studies used a different cutoff from earlier studies, and indeed, Genomic Health continues to utilize <18 as the low-risk cutoff. Further data from the TAILORx study will be important in determining the optimal RS below which adjuvant chemotherapy can be safely omitted. Until then, a reasonable approach would be to omit chemotherapy in patients with an RS of <11 and strongly consider omitting chemotherapy in the RS range 11–18. For patients with an RS of 19–31, the decision to use chemotherapy continues to be determined by the choice of physicians and patients. The RSPC calculator may be used to refine the decision in some intermediate-risk patients. As the RS has a continuous relationship with the magnitude of chemotherapy benefit, another approach would be to predetermine a cutoff point in discussion with the patient, before undergoing the Oncotype DX test. As data for the intermediate- and high-risk groups for TAILORx are still unavailable, definition of “high-risk” should remain as RS ≥31 and patients with a score of this category should definitely be offered adjuvant chemotherapy.
For node-positive disease, data from the SWOG-8814 cohort suggest that omitting chemotherapy for patients with limited node-positive disease (1–3 nodes) and a low RS (<18) could be considered. However, given the overall higher risk of recurrence, the decision to omit chemotherapy based on RS score alone would need to be fully discussed with patients to help inform their decision. The RS should not be recommended for patients with ≥4 lymph nodes, as the risk of relapse is substantial even when a low-risk RS is obtained.
Neoadjuvant therapy
Neoadjuvant chemotherapy is frequently prescribed for patients with locally advanced tumors and where breast conservation surgery is desired. Pathological factors associated with a good response to neoadjuvant treatment include lower hormone-receptor levels, HER2 positivity, and a higher tumor grade.45,46 A number of studies have explored the utility of the RS in selecting tumors that are more likely to respond to neoadjuvant chemotherapy.
Yardley et al recruited 168 patients who underwent neoadjuvant chemotherapy (6 cycles of ixabepilone/cyclophosphamide) for a study investigating the correlation between RS and rates of pathological complete response (pCR). In this cohort, 45% of patients had tumors with a triple-negative phenotype. The majority (161 of 168 recruited patients) underwent definitive surgery and 17% achieved pCR. The RS strongly correlated with pCR rates, and pCR only occurred in patients with a high baseline RS.47 However, the use of ixabepilone as neoadjuvant chemotherapy is not typical. The RS is also not validated or designed for ER-negative tumors. Higher levels of Ki-67 are known to be an independent predictive factor for the response to neoadjuvant chemotherapy.48 As Ki-67 is a major component of the RS, it is possible that using Ki-67 alone could have predicted the same outcomes in this cohort.49
Bear et al (2017) reported a pilot trial of 64 patients that used RS to select neoadjuvant treatment with either chemotherapy or endocrine therapy, based on the premise that tumors with low RS have a very low likelihood of achieving pathological complete response with neoadjuvant chemotherapy. The study population had hormone receptor-positive and HER2-negative breast cancer, up to cN2b nodal status. Patients with RS <11 received neoadjuvant hormonal therapy, while those with an RS of 11–25 were randomized to either neoadjuvant hormonal therapy or chemotherapy, and patients with an RS >25 received adjuvant chemotherapy. All the patients with a pCR had an RS of >25. In the group with RS <11, 83.3% of patients had a clinical response to neoadjuvant endocrine therapy alone (8.3% complete response) and 75% had successful breast conservation.50
Most studies of the use of Oncotype DX in selecting neoadjuvant treatment were limited by small sample sizes (mostly <100).51 Although the results of these studies are hypothesis generating, larger studies will be required to provide sufficient power to properly investigate the utility of RS in the neoadjuvant setting.
Health economics, clinical utility, and acceptability
The Oncotype DX currently costs USD$4,620 in the USA.52 Despite this high cost, multiple studies carried out in Europe, North America, Latin America, and Asia have supported the cost-effectiveness of utilizing the assay. For these studies, the cost of utilizing Oncotype DX was compared to the cost of chemotherapy, quality-adjusted life expectancy, as well as societal costs.53–56 Most of the cost-effectiveness appears to be primarily attributable to the cost of chemotherapy (typically at least twice the cost of the Oncotype DX) and life-years lost for patients with disease relapse.57 At this point in time, Oncotype DX is publicly funded in the UK, Ireland, Switzerland, Spain, Israel, Greece, and Canada.58–61 All major insurers in the USA also cover the cost of the Oncotype DX assay.62
A number of clinical impact studies have been performed looking at the utility of the RS in helping determine adjuvant treatment decisions. These studies have consistently shown that the RS changes adjuvant treatment recommendations (Table 2). The initial study by Lo et al (2010) was a multicenter study in the USA assessing if the RS influenced physician and patient treatment selection over and above standard prognostic factors. Adjuvant treatment recommendations were given before and after the RS results were made available. Eighty-nine patients with ER-positive and node-negative tumors were analyzed, and a small proportion (7%) also had HER2 positive tumors. The majority (65.2%) had intermediate grade tumors. Before the RS assay results were available, medical oncologists recommended chemotherapy and hormonal therapy (CHT) for 47% of patients and hormonal therapy alone (HT) for 51.7% of patients. After the RS results, the recommendation of CHT decreased to 25.8% and HT alone increased to 67.4%. All patients with a high-risk RS were recommended to undergo CHT. A lower proportion of the intermediate-risk (26.2%) and low-risk (7.9%) groups were recommended to have CHT. Overall, medical oncologists changed their recommendation in 31.5% of cases after the RS became available and the most significant change was from CHT to HT alone (22.5%). The RS also increased the oncologist’s confidence in their treatment recommendation in 76% of cases. A total of 83% of patients stated that the RS results influenced their adjuvant treatment decision making and almost all patients were glad they undertook the RS and understood how the assay worked and were able to understand the results.63
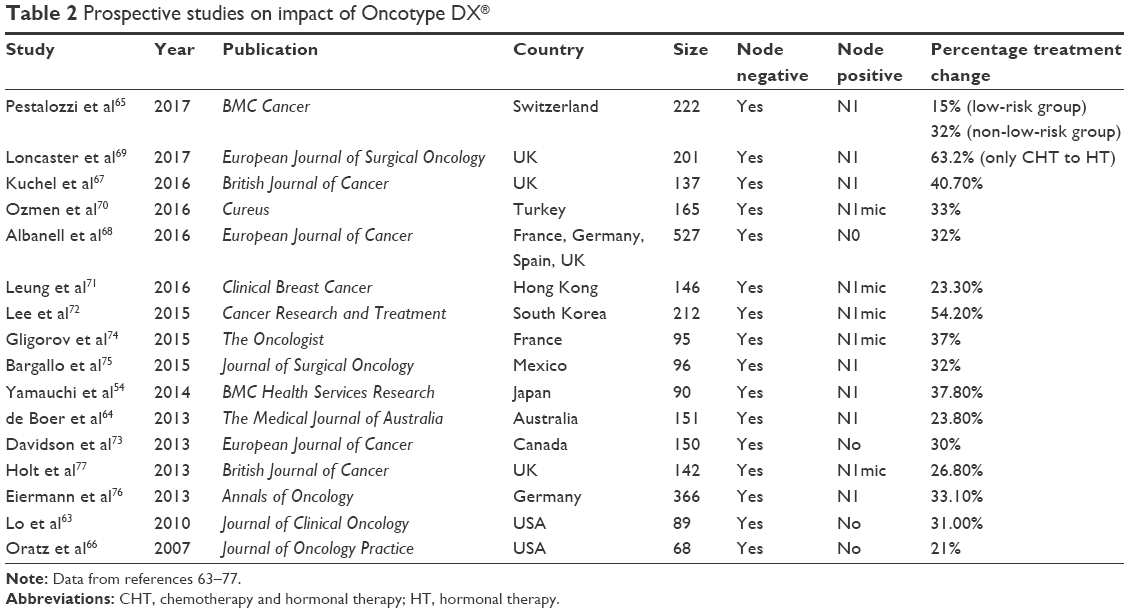 | Table 2 Prospective studies on impact of Oncotype DX® |
de Boer et al (2013) explored the effect of RS information on the treatment recommendation in the multidisciplinary meeting (MDM) setting in 151 patients with hormone receptor-positive and HER2-negative disease, involving 0–3 lymph nodes. The majority of patients had grade 2 tumors (56%) and <2 cm tumors (68%) and were lymph node negative (67%). Adjuvant treatment recommendation was given by the MDM before and after the RS. In the node-negative group (number [n] =101), 40% of patients initially recommended CHT had their recommendation changed to HT alone, while only 17% initially recommended HT alone had their recommendation changed to CHT. For the node-positive group, 24% of patients initially recommended CHT had their recommendation changed to HT, while only 2% had their recommendation changed from HT to CHT. Overall, the most significant treatment change was from CHT to HT and the RS assay had the largest impact in node-positive patients who were initially recommended CHT (a decrease from 74 to 52%). Change in treatment recommendations was made according to the RS categories, supporting that the assay had a strong impact on the final adjuvant treatment recommendation.64
A more recent Swiss multicenter study by Pestalozzi et al (2017) assessed the impact of the RS on the treatment recommendations of Swiss multidisciplinary tumor boards. Patients were stratified into low- and non-low-risk groups based on nodal status and a number of other risk factors (ER/PR <50%, grade 3, tumor >5 cm, extensive lymphovascular invasion, and Ki-67 >30%). Patients were low-risk if they were node negative and had ≤1 risk factors or pN1a with none of the risk factors, and all other patients were classified as non-low-risk. Cases presented at the multidisciplinary board had adjuvant treatment recommendation issued before and after the RS. The majority of the 222 patients had grade 2 tumors (78%), were pN0 (76%), and were classified as low-risk (69%). Overall, pre- and post-RS recommendations differed by 20% and ranged from 15% (low-risk) and 32% (non-low-risk). Of note, for patients who were initially offered HT, the RS resulted in a decision change in only 4% of low-risk patients and 16% in the non-low-risk group. This potentially reflects a decreased utility of the value of the assay in this group, especially for those with low-risk disease. For the group initially recommended CHT, the post-RS recommendation change to HT alone was significant in both patients in low-risk (44%) and non-low-risk groups (40%).65 Overall, the RS had the most significant impact in the group of patients initially recommended CHT (especially those with limited node-positive disease), in which the proportion of patients who were recommended CHT decreased by ~20–30% after the RS results. A 20%–30% decrease in chemotherapy rates would have significant health and economic implications. Importantly, however, the prospective validation for this group is not yet available and awaits the results of RxPONDER trial.
Summary
Genomic assays such as Oncotype DX have changed the landscape for the treatment of ER-positive early breast cancer. In a USA-based study, there has been a 13% decline in the use of adjuvant chemotherapy in 2006–2008, which has been largely attributed to the introduction of the Oncotype DX in 2004.78 While the Oncotype DX is expensive, the potential cost savings from chemotherapy avoidance and reduced exposure to the side effects of cytotoxic therapy appear to be cost-effective in most jurisdictions. The development and eventual validation of other genomic assays could potentially reduce test costs. While Oncotype DX is currently well validated in the node-negative population, its optimal use remains to be defined for cohorts of patients with intermediate-risk RS, as well as for patients with lymph node-positive disease. Results from the prospective TAILORx and RxPONDER trials will help shed light on these questions.
Disclosure
The authors report no conflicts of interest in this work.
References
GLOBOCAN 2012 [webpage on the Internet]. Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012; 2012. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed May 31, 2017. | ||
Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353(17):1784–1792. | ||
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. | ||
Dignam JJ, Dukic VM, Anderson SJ, Mamounas EP, Wickerham DL, Wolmark N. Hazard of recurrence and adjuvant treatment effects over time in lymph node-negative breast cancer. Breast Cancer Res Treat. 2009;116(3):595–602. | ||
Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373(21):2005–2014. | ||
Harbeck N, Thomssen C. A new look at node-negative breast cancer. Oncologist. 2011;16(suppl 1):51–60. | ||
Griggs J, Hawley S, Graff J, et al. Factors associated with receipt of breast cancer adjuvant chemotherapy in a diverse population-based sample. J Clin Oncol. 2012;30(25):3058–3064. | ||
Gaß P, Fasching PA, Fehm T, et al. Factors influencing decision-making for or against adjuvant and neoadjuvant chemotherapy in postmenopausal hormone receptor-positive breast cancer patients in the Evaluate-TM study. Breast Care. 2016;11(5):315–322. | ||
Baum M, Ravdin PM. Decision-making in early breast cancer: guidelines and decision tools. Eur J Cancer. 2002;38(6):745–749. | ||
Scholzen T, Gerdes J. The Ki-67 protein: from the known and the unknown. J Cell Physiol. 2000;182(3):311–322. | ||
Inwald EC, Klinkhammer-Schalke M, Hofstädter F, et al. Ki-67 is a prognostic parameter in breast cancer patients: results of a large population-based cohort of a cancer registry. Breast Cancer Res Treat. 2013;139(2):539–552. | ||
Ravdin PM, Siminoff LA, Davis GJ, et al. Computer program to assist in making decisions about adjuvant therapy for women with early breast cancer. J Clin Oncol. 2001;19(4):980–991. | ||
Olivotto IA, Bajdik CD, Ravdin PM, et al. Population-based validation of the prognostic model ADJUVANT! for early breast cancer. J Clin Oncol. 2005;23(12):2716–2725. | ||
Goldstein LJ, Gray R, Badve S, et al. Prognostic utility of the 21-gene assay in hormone receptor–positive operable breast cancer compared with classical clinicopathologic features. J Clin Oncol. 2008;26(25):4063–4071. | ||
Dowsett M, Cuzick J, Wale C, et al. Prediction of risk of distant recurrence using the 21-gene recurrence score in node-negative and node-positive postmenopausal patients with breast cancer treated with anastrozole or tamoxifen: a TransATAC Study. J Clin Oncol. 2010;28(11):1829–1834. | ||
De Schutter H, Van Damme N, Colpaert C, et al. Quality of pathology reporting is crucial for cancer care and registration: a baseline assessment for breast cancers diagnosed in Belgium in 2008. Breast. 2015;24(2):143–152. | ||
Polley MY, Leung SC, McShane LM, et al. An international Ki67 reproducibility study. J Natl Cancer Inst. 2013;105(24):1897–1906. | ||
Albain KS, Paik S, van’t Veer L. Prediction of adjuvant chemotherapy benefit in endocrine responsive, early breast cancer using multigene assays. Breast. 2009;18:S141–S145. | ||
Paik S. Is gene array testing to be considered routine now? Breast. 2011;20(suppl 3):S87–S91. | ||
Bartlett J, Bayani J, Marshall A, et al. Comparing breast cancer multiparameter tests in the OPTIMA prelim trial: no test is more equal than the others. J Natl Cancer Inst. 2016;108(9):djw050. | ||
Varga Z, Sinn P, Fritzsche F, et al. Comparison of EndoPredict and Oncotype DX Test results in hormone receptor positive invasive breast cancer. PLoS One. 2013;8(3):e58483. | ||
Filipits M, Rudas M, Jakesz R, et al; EP Investigators. A new molecular predictor of distant recurrence in ER-positive, HER2-negative breast cancer adds independent information to conventional clinical risk factors. Clin Cancer Res. 2011;17(18):6012–6020. | ||
Dubsky P, Filipits M, Jakesz R, et al; Austrian Breast and Colorectal Cancer Study Group (ABCSG). EndoPredict improves the prognostic classification derived from common clinical guidelines in ER-positive, HER2-negative early breast cancer. Ann Oncol. 2013;24(3):640–647. | ||
Buus R, Sestak I, Kronenwett R, et al. Comparison of EndoPredict and EPclin with Oncotype DX Recurrence Score for prediction of risk of distant recurrence after endocrine therapy. J Natl Cancer Inst. 2016;108(11):djw149. | ||
Jankowitz RC, Cooper K, Erlander MG, et al. Prognostic utility of the breast cancer index and comparison to Adjuvant! Online in a clinical case series of early breast cancer. Breast Cancer Res. 2011;13(5):R98. | ||
Sgroi DC, Sestak I, Cuzick J, et al. Prediction of late distant recurrence in patients with oestrogen-receptor-positive breast cancer: a prospective comparison of the breast-cancer index (BCI) assay, 21-gene recurrence score, and IHC4 in the TransATAC study population. Lancet Oncol. 2013;14(11):1067–1076. | ||
Parker JS, Mullins M, Cheang MCU, et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol. 2009;27(8):1160–1167. | ||
Cardoso F, van’t Veer LJ, Bogaerts J, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375(8):717–729. | ||
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–2826. | ||
Harris LN, Ismaila N, McShane LM, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2016;34(10):1134–1150. | ||
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) – Breast Cancer, Version 2.2017; 2017. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed July 4, 2017. | ||
Senkus E, Kyriakides S, Ohno S, et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(suppl_5):v8–v30. | ||
Gnant M, Harbeck N, Thomssen C. St. Gallen/Vienna 2017: a brief summary of the consensus discussion about escalation and de-escalation of primary breast cancer treatment. Breast Care (Basel). 2017;12(2):102–107. | ||
NICE [webpage on the Internet]. Gene Expression Profiling and Expanded Immunohistochemistry Tests for Guiding Adjuvant Chemotherapy Decisions in Early Breast Cancer Management: MammaPrint, Oncotype DX, IHC4 and Mammostrat; 2013. Available from: https://www.nice.org.uk/guidance/dg10. Accessed July 4, 2017. | ||
Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor–positive breast cancer. J Clin Oncol. 2006;24(23):3726–3734. | ||
Mamounas EP, Bryant J, Lembersky B, et al. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: results from NSABP B-28. J Clin Oncol. 2005;23(16):3686–3696. | ||
Fisher B, Brown AM, Dimitrov NV, et al. Two months of doxorubicin-cyclophosphamide with and without interval reinduction therapy compared with 6 months of cyclophosphamide, methotrexate, and fluorouracil in positive-node breast cancer patients with tamoxifen-nonresponsive tumors: results from the National Surgical Adjuvant Breast and Bowel Project B-15. J Clin Oncol. 1990;8(9):1483–1496. | ||
Gluz O, Nitz UA, Christgen M, et al. West German Study Group Phase III PlanB Trial: first prospective outcome data for the 21-gene recurrence score assay and concordance of prognostic markers by central and local pathology assessment. J Clin Oncol. 2016;34(20):2341–2349. | ||
European Cancer Organisation [webpage on the Internet]. EBCC-10 NEWS: Five-Year Result Show 21-Gene Test Successfully Identifies Early Breast Cancer Patients Who Can Be Spared Chemotherapy; 2017. Available from: http://www.ecco-org.eu/Global/News/EBCC/EBCC10-PR/2016/03/Five-year-results-identifies-early-breast-cancer-patients-who-can-be-spared-chemo. Accessed June 9, 2017. | ||
Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55–65. | ||
Kalinsky K. Tamoxifen citrate, letrozole, anastrozole, or exemestane with or without chemotherapy in treating patients with invasive RxPONDER breast cancer; 2017. Available from: https://clinicaltrials.gov/ct2/show/NCT01272037. NLM identifier: NCT01272037. Accessed July 5, 2017. | ||
Shachar SS, Muss HB. Internet tools to enhance breast cancer care. NPJ Breast Cancer. 2016;2:16011. | ||
Tang G, Cuzick J, Costantino JP, et al. Risk of recurrence and chemotherapy benefit for patients with node-negative, estrogen receptor–positive breast cancer: recurrence score alone and integrated with pathologic and clinical factors. J Clin Oncol. 2011;29(33):4365–4372. | ||
Oncotype DX tools. Oncotype DX tools® User Guide; 2013. Available from: http://www.genomichealth.com/-/media/ODX-Breast/Files/Downloads/GHI10203_0313_Oncotype_DX_tools_Guide.pdf. Accessed July 4, 2017. | ||
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. | ||
Guarneri V, Broglio K, Kau SW, et al. Prognostic value of pathologic complete response after primary chemotherapy in relation to hormone receptor status and other factors. J Clin Oncol. 2006;24(7):1037–1044. | ||
Yardley DA, Peacock NW, Shastry M, et al. A phase II trial of ixabepilone and cyclophosphamide as neoadjuvant therapy for patients with HER2-negative breast cancer: correlation of pathologic complete response with the 21-gene recurrence score. Breast Cancer Res Treat. 2015;154(2):299–308. | ||
Brown JR, DiGiovanna MP, Killelea B, Lannin DR, Rimm DL. Quantitative assessment Ki-67 score for prediction of response to neoadjuvant chemotherapy in breast cancer. Lab Invest. 2014;94(1):98–106. | ||
Sahebjam S, Aloyz R, Pilavdzic D, et al. Ki 67 is a major, but not the sole determinant of Oncotype Dx Recurrence Score. Br J Cancer. 2011;105(9):1342–1345. | ||
Bear HD, Wan W, Robidoux A, et al. Using the 21-gene assay from core needle biopsies to choose neoadjuvant therapy for breast cancer: a multicenter trial. J Surg Oncol. 2017;115(8):917–923. | ||
Robidoux A, McCullough D, Lau A, Stöppler M, Chao C. Use of the 21-gene Oncotype DX® Breast Recurrence Score™ (RS) assay in the neoadjuvant treatment setting. Breast. 2017;32(suppl 1):S80. | ||
[webpage on the Internet]. 10-K: Genomic Health; 2017. Available from: http://www.marketwatch.com/story/10-k-genomic-health-inc-2017-03-15. Accessed June 1, 2017. | ||
Lamond NW, Skedgel C, Rayson D, Lethbridge L, Younis T. Cost-utility of the 21-gene recurrence score assay in node-negative and node-positive breast cancer. Breast Cancer Res Treat. 2012;133(3):1115–1123. | ||
Yamauchi H, Nakagawa C, Yamashige S, et al. Societal cost-effectiveness analysis of the 21-gene assay in estrogen-receptor-positive, lymph-node-negative early-stage breast cancer in Japan. BMC Health Serv Res. 2014;5(14):372. | ||
Bargallo-Rocha JE, Lara-Medina F, Perez-Sanchez V, et al. Cost-effectiveness of the 21-gene breast cancer assay in Mexico. Adv Ther. 2015;32(3):239–253. | ||
Katz G, Romano O, Foa C, et al. Economic impact of gene expression profiling in patients with early-stage breast cancer in France. PLoS One. 2015;10(6):e0128880. | ||
Tsoi DT, Inoue M, Kelly CM, Verma S, Pritchard KI. Cost-effectiveness analysis of recurrence score-guided treatment using a 21-gene assay in early breast cancer. Oncologist. 2010;15(5):457–465. | ||
MSAC Public Summary Document. Application No. 1342.1 – Gene Expression Profiling of 21 genEs in Breast Cancer to Quantify the Risk of Disease Recurrence and Predict Adjuvant Chemotherapy Benefit; 2014. Available from: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/D4EF97AE878785FDCA25801000123BEE/$File/1342.1-PSD-MSACPSD-OncotypeDX(D14-1184441).PDF. Accessed July 4, 2017. | ||
Specialised Therapeutics [webpage on the Internet]. Press Release – Cutting Edge Breast Cancer Test ‘Should be Reimbursed’ – Medical Experts; 2015. Available from: https://www.stabiopharma.com/index.php?q=cutting-edge-breast-cancer-test-should-be-reimbursed-medical-experts.html. Accessed June 1, 2017. | ||
Genomic Health [webpage on the Internet]. Following NICE’s Exclusive Recommendation, NHS England Agrees to Access Program for Oncotype DX® Breast Cancer Test; 2015. Available from: http://investor.genomichealth.com/releasedetail.cfm?releaseid=894895. Accessed June 1, 2017. | ||
Genomic Health. Oncotype DX® Breast Cancer Test Achieves Positive Reimbursement in Switzerland; 2014. Available from: https://www.bioalps.org/data/documents/suggesteventsnews/genomic-health-breast-cancer-test-obtains-1426.pdf. Accessed July 4, 2017. | ||
Genomic Health [webpage on the Internet]. Oncotype DX for Breast Cancer – Tailoring Treatment for Individual Patients with Early-Stage Breast Cancer; 2017. Available from: http://www.genomichealth.com/en-US/oncotype_iq_products/oncotype_dx/oncotype_dx_breast_cancer. Accessed June 1, 2017. | ||
Lo SS, Mumby P, Norton J, et al. Prospective multicenter study of the impact of the 21-gene recurrence score assay on medical oncologist and patient adjuvant breast cancer treatment selection. J Clin Oncol. 2010;28(10):1671–1676. | ||
de Boer R, Baker C, Speakman D, Chao C, Yoshizawa C, Mann GB. The impact of a genomic assay (Oncotype DX) on adjuvant treatment recommendations in early breast cancer. Med J Aust. 2013;199(3):205–208. | ||
Pestalozzi BC, Tausch C, Dedes KJ, et al. Adjuvant treatment recommendations for patients with ER-positive/HER2-negative early breast cancer by Swiss tumor boards using the 21-gene recurrence score (SAKK 26/10). BMC Cancer. 2017;17(1):265. | ||
Oratz R, Paul D, Cohn AL, Sedlacek SM. Impact of a commercial reference laboratory test recurrence score on decision making in early-stage breast cancer. J Oncol Pract. 2007;3(4):182–186. | ||
Kuchel A, Robinson T, Comins C, et al. The impact of the 21-gene assay on adjuvant treatment decisions in oestrogen receptor-positive early breast cancer: a prospective study. Br J Cancer. 2016;114(7):731–736. | ||
Albanell J, Svedman C, Gligorov J, et al. Pooled analysis of prospective European studies assessing the impact of using the 21-gene recurrence score assay on clinical decision making in women with oestrogen receptor-positive, human epidermal growth factor receptor 2-negative early-stage breast cancer. Eur J Cancer. 1990;2016(66):104–113. | ||
Loncaster J, Armstrong A, Howell S, et al. Impact of Oncotype DX breast Recurrence Score testing on adjuvant chemotherapy use in early breast cancer: real world experience in Greater Manchester, UK. Eur J Surg Oncol. 2017;43(5):931–937. | ||
Ozmen V, Atasoy A, Gokmen E, et al. Impact of Oncotype DX Recurrence Score on treatment decisions: results of a prospective multicenter study in Turkey. Cureus. 2016;8(3):e522. | ||
Leung RC, Yau TC, Chan MC, et al. The impact of the Oncotype DX breast cancer assay on treatment decisions for women with estrogen receptor-positive, node-negative breast carcinoma in Hong Kong. Clin Breast Cancer. 2016;16(5):372–378. | ||
Lee MH, Han W, Lee JE, et al. The clinical impact of 21-gene recurrence score on treatment decisions for patients with hormone receptor-positive early breast cancer in Korea. Cancer Res Treat. 2015;47(2):208–214. | ||
Davidson JA, Cromwell I, Ellard SL, et al. A prospective clinical utility and pharmacoeconomic study of the impact of the 21-gene Recurrence Score® assay in oestrogen receptor positive node negative breast cancer. Eur J Cancer. 2013;49(11):2469–2475. | ||
Gligorov J, Pivot XB, Jacot W, et al. Prospective clinical utility study of the use of the 21-Gene assay in adjuvant clinical decision making in women with estrogen receptor-positive early invasive breast cancer: results from the SWITCH Study. Oncologist. 2015;20(8):873–879. | ||
Bargallo JE, Lara F, Shaw-Dulin R, et al. A study of the impact of the 21-gene breast cancer assay on the use of adjuvant chemotherapy in women with breast cancer in a Mexican public hospital. J Surg Oncol. 2015;111(2):203–207. | ||
Eiermann W, Rezai M, Kümmel S, et al. The 21-gene recurrence score assay impacts adjuvant therapy recommendations for ER-positive, node-negative and node-positive early breast cancer resulting in a risk-adapted change in chemotherapy use. Ann Oncol. 2013;24(3):618–624. | ||
Holt S, Bertelli G, Humphreys I, et al. A decision impact, decision conflict and economic assessment of routine Oncotype DX testing of 146 women with node-negative or pNImi, ER-positive breast cancer in the UK. Br J Cancer. 2013;108(11):2250–2258. | ||
Hassett MJ, Silver S, Hughes M, et al. Adoption of gene expression profile testing and association with use of chemotherapy among women with breast cancer. J Clin Oncol. 2012;30(18):2218–2226. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.