")
Back to Journals » OncoTargets and Therapy » Volume 12
Spotlight on liposomal irinotecan for metastatic pancreatic cancer: patient selection and perspectives
Authors Woo W , Carey ET, Choi M
Received 6 November 2018
Accepted for publication 15 January 2019
Published 21 February 2019 Volume 2019:12 Pages 1455—1463
DOI https://doi.org/10.2147/OTT.S167590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Carlos E Vigil
Wonhee Woo, Edward T Carey, Minsig Choi
Division of Hematology/Oncology, Department of Medicine, Stony Brook University, Stony Brook, NY, USA
Abstract: Pancreatic cancer is a highly lethal disease, where the mortality closely matches increasing incidence. Pancreatic ductal adenocarcinoma (PDAC) is the most common histologic type that tends to metastasize early in tumor progression. For metastatic PDAC, gemcitabine had been the mainstay treatment for the past three decades. The treatment landscape has changed since 2010, and current first-line chemotherapy includes triplet drugs like FOLFIRINOX (folinic acid, 5-fluorouracil, irinotecan, and oxaliplatin), and doublet agents like nab-paclitaxel and gemcitabine. Nanoliposomal encapsulated irinotecan (nal-IRI) was developed as a novel formulation to improve drug delivery, effectiveness, and limit toxicities. Nal-IRI, in combination with leucovorin-modulated fluorouracil (5-FU/LV), was found in a large randomized phase III clinical trial (NAPOLI-1) to significantly improve overall survival in patients who progressed on gemcitabine-based therapy. This review will focus on the value of using nal-IRI, toxicities, recent clinical experiences, and tools to improve patient outcomes in this setting.
Keywords: liposomal irinotecan, nal-IRI, pancreatic cancer, pancreatic ductal adenocarcinoma, refractory cancer
Introduction
Pancreatic cancer, often referred to pancreatic ductal adenocarcinoma (PDAC), is the fourth most common cause of cancer death in the USA. In 2018, it was estimated that 55,440 cases were diagnosed and 44,330 patients died.1 Total deaths from pancreatic cancer are increasing and are expected to be the second leading cause of cancer death in the USA by 2030.2 This is due to many factors, including limited screening tests, limited efficacy of currently approved chemotherapeutic treatment, and because pancreatic cancer is often diagnosed at late stages, leading to poor outcomes.
There has been a substantial increase in knowledge about underlying mechanisms and pathophysiology of pancreatic cancer. In agreement to its predilection for spreading, a preclinical study using transgenic mice suggested that pancreatic cancer is possibly a systemic disease even at its early stage.3 Studies have implicated alterations in tumor drivers, such as RAS, AKT, WNT, B catenin, and PI3K, as well as loss of function in tumor suppressors, such as P53, P16, Smad4/DPC4 and APC.4–6 Moffitt et al investigated the gene expression in primary and metastatic PDAC tissues by using the source separation technique called nonnegative matrix factorization (NMF). They classified PDAC into two subtypes, basal-like subtype and classical subtype tumors. Patients with basal-like subtype tumors have worse prognosis with an overall median survival of 11 months and 44% 1-year survival compared with 19 months and 70% 1-year survival for patients with classical subtype tumor. However, it was found that basal-like subtype tumors showed better responses to adjuvant therapy hazard ratio (HR) =0.38, compared with HR =0.76 for the classical subtype tumor. They also found that the KRAS G12D mutation was significantly overexpressed in the basal-like subtype while G12V was overexpressed in the classical subtype. Additional mutated genes, such as SMAD4, GATA6, and STK11, were further identified as important in PDAC pathology.7 Ying et al demonstrated how KRAS was critical for PDAC progression, and approximately 93% of PDAC specimens had KRAS mutations.8,9 Another study used KRAS2 mutations for the diagnosis of PDAC compared to chronic pancreatitis.10 Multiple preclinical and clinical attempts, and extensive research efforts have been made to inhibit KRAS and its effectors such as MEK 1–2, Erk 1–2, or Akt. However, despite the efforts, KRAS remains a difficult molecular target to treat and monitor, and efforts continue to translate research findings with potential into clinical trials.11
Surgery remains the only curative treatment in today’s paradigm, but only about 20% of patients diagnosed with pancreatic cancer are candidates for curative resection.12 Even after resection and adjuvant chemotherapy, most patients eventually relapse, and 5-year survival is still only about 15%–20% even for those who underwent tumor resection.13 Importantly, it has been shown that large volume centers have been associated with improved prognosis and outcomes after curative pancreatic cancer resection, as perioperative mortality and complications are closely associated with the complexity of the surgery itself.14
Overall 5-year survival for pancreatic cancer is about 6% in the USA, and in the metastatic setting, PDAC is almost always fatal.15 Ghosn et al have examined the many dilemmas for oncologists and patients regarding how to approach first-line regimens in PDAC. Clinical efficacy, toxicity, patient preferences, and tumor characteristics should be included in the decision-making process.16 National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) treatment guidelines recommend clinical trials as the preferred options, and FOLFIRINOX (folinic acid, 5-fluorouracil [5-FU], irinotecan, and oxaliplatin) or nab-paclitaxel (nanoparticle albumin-bound-paclitaxel) and gemcitabine combination therapy for patients with good performance status.17,18 Other treatment options include gemcitabine and erlotinib, gemcitabine and capecitabine, or gemcitabine monotherapy for patients with poor performance status. Best supportive care could also be an option for patients with a debilitating status or multiple medical comorbidities based on physician’s discretion.17 FOLFIRINOX, and nab-paclitaxel and gemcitabine combination therapy are the preferred first-line chemotherapeutic regimens for patients with good performance status. However, most patients with PDAC eventually relapse, leaving them with few options for later lines of therapy.
Nanoliposomal irinotecan (nal-IRI) has been developed as a formulation to improve drug delivery and reduce side effects. Combined with fluorouracil and leucovorin (5-FU/LV), nal-IRI has shown significant benefit compared to 5-FU/LV alone in terms of overall survival and progression-free survival (PFS) in patients who progressed on prior gemcitabine-based therapy.19 In this review, we will briefly examine traditional systemic therapy options, and further explore the novel approaches to metastatic pancreatic cancer, including nal-IRI. We will discuss the value of using this drug, associated toxicities, and clinical outcomes.
Current frontline systemic treatment options and limitation
Gemcitabine has been the mainstay of chemotherapy for metastatic PDAC for the past three decades, since Moore et al demonstrated that gemcitabine is superior to 5-fluorouracil (5-FU) in terms of quality of life and overall improvement in survival from 4.41 months to 5.56 months, compared to 5-FU.20 Since 2010, two combination therapies, FOLFIRINOX (a combination of oxaliplatin, irinotecan, folinic acid, and fluorouracil), and nab-paclitaxel and gemcitabine have been widely accepted as frontline systemic treatments. In a phase III randomized clinical trial, FOLFIRINOX has been shown to prolong overall median survival to 11.1 months compared to 6.8 months in a group treated with gemcitabine alone. However, this combination should be used in selected patients, such as younger (age <65) patients with limited comorbidities and those with good performance status.21 Another new combination, nab-paclitaxel and gemcitabine, improved median overall survival, from 6.6 to 8.7 months, compared to gemcitabine monotherapy alone. Furthermore, this combination has been widely used with manageable adverse effects and is currently the standard of care in most community practices.22
Refractory pancreatic cancer
Despite new chemotherapeutic regimens, in many patients with metastatic pancreatic cancer, unfortunately chemotherapy fails and there is disease progression. Nagrial et al demonstrated through a meta-analysis of PDAC trials that approximately 43% of patients who progressed on first-line therapy went on to second-line treatment.23 This number has increased in recent years due to availability of newer therapeutic options and improved supportive care for advanced pancreatic cancer patients.24 Therefore, research into defining and improving the sequence of optimal therapy remains an important consideration for patients with good performance status and who are motivated to pursue additional therapy to control their disease.
Results from a randomized phase III trial for second-line treatment of PDAC (CONKO-003), suggested that the use of a weekly regimen called OFF, a combination of oxaliplatin and 5-FU/LV, could be beneficial in PDAC patients refractory to gemcitabine. When compared to 5-FU/LV alone, OFF extended the duration of OS from 3.3 months to 5.9 months and PFS from 2.0 months to 2.9 months. OFF was found to be associated with significantly increased neurotoxicity and myelosuppression.25 However, a recent randomized phase III study (PANCREOX) failed to prove the benefit of 5-FU and oxaliplatin over 5-FU/LV alone. In this study, median OS and PFS for FOLFOX (folinic acid, 5-FU and oxaliplatin) was 6.1 and 3.1 months compared with 9.9 months and 2.9 months for 5-FU alone. Furthermore, the overall incidence of grade 3 or 4 adverse events was significantly higher in the FOLFOX arm at 63% compared to 11% in the control arm without additional clinical benefit. The most common adverse effects were hematological toxicities including neutropenia and thrombocytopenia, followed by paresthesia and peripheral neuropathy.26
A single institute retrospective study was conducted to test the efficacy of gemcitabine and nab-paclitaxel after FOLFIRINOX failure in 12 enrolled patients with metastatic pancreatic adenocarcinoma. The overall response rate was 30% and disease control rate was 60%. The gemcitabine and nab-paclitaxel combination therapy after FOLFIRINOX failure were later further investigated in other studies which showed inconsistent results. The efficacy of the gemcitabine and nab-paclitaxel combination therapy after FOLFIRINOX needs to be further evaluated in larger studies.27
Irinotecan is a prodrug, metabolized primarily in liver and colon tissue to the active form, SN-38.28 Yoo et al did a randomized phase II trial comparing oxaliplatin and 5-FU/LV (FOLFOX) with free irinotecan and 5-FU/LV (FOLFIRI) in PDAC patients. Median overall survival only marginally increased to 3.9 months with FOLFIRI, from 3.5 months with FOLFOX.29 Multiple prospective and retrospective studies of using FOLFIRI-based regimens were subsequently performed but they are all limited in terms of small sample sizes and were of single-arm design; therefore, the potential benefit of FOLFIRI is still unclear in refractory pancreatic cancer.29–34
Liposomal carriers are widely utilized in cancer therapy to enhance anticancer activity of drugs.35 The liposomal formulation shelters the drug from unwanted early metabolism, keeping it in plasma circulation and in tissues longer and increasing delivery into tumors. Therefore, this prolongs intratumoral levels of the drug, and theoretically increases antineoplastic activity.36 In preclinical settings, the nanoliposomal formulation of irinotecan, has been shown to have advantageous pharmacokinetics and roughly 5–6-fold higher level of its active metabolite, SN-38 in tumors, when compared with the free, traditional form of the drug.37 Ideally, this allows for increased active drug delivery to the tumor and increased antitumor effects and efficacy. Furthermore, irinotecan works by inhibiting topoisomerase activity in tumors, and subsequently halting rapid cell division.38
A phase II trial with PDAC patients showed nal-IRI produced median overall and median PFS rates of 5.2 and 2.4 months, respectively.39 These findings led to a large randomized, phase III clinical trial called NAPOLI-1. This study involved 417 patients at 76 sites in 14 countries. Wang-Gillan et al demonstrated that nal-IRI, when paired with 5-FU/LV, improved overall survival in patients who progressed on prior gemcitabine-based treatment.19 They compared three patient groups, nal-IRI +5-FU/LV, nal-IRI monotherapy, and 5-FU/LV as a control. It was shown that median OS was significantly increased in patients receiving nal-IRI +5-FU/LV compared with 5-FU/LV alone (6.6 months vs 4.0 months). Median overall survival did not differ between nal-IRI monotherapy and 5-FU/LV. In addition, PFS increased to 3.1 months in patients receiving nal-IRI +5-FU/LV from 1.5 months with 5-FU/LV alone. Nal-IRI with 5-FU/LV improved objective tumor response, time to treatment failure, and CA 19–9 tumor marker response showing its activities against pancreatic cancer.19 Detailed descriptions of patient characteristics and survival are summarized in Table 1.
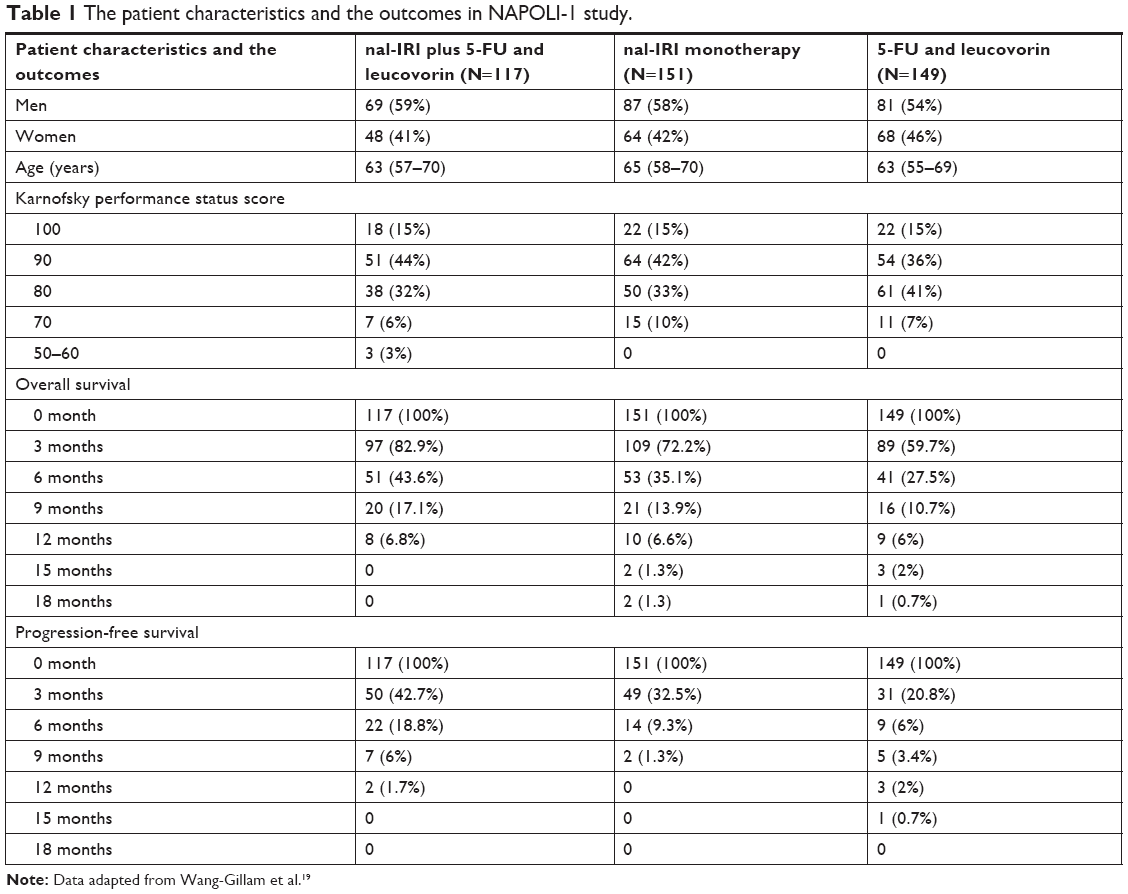 | Table 1 The patient characteristics and the outcomes in NAPOLI-1 study. |
Glassman et al at Memorial Sloan Kettering Cancer Center retrospectively examined their experiences with nal-IRI in 56 patients with advanced PDAC who received nal-IRI +5-FU/LV. The results showed median OS and PFS were 5.3 and 2.9 months, respectively. However, patients who progressed previously on irinotecan-based chemotherapy experienced worse outcomes on nal-IRI compared to those who were irinotecan naïve. Specifically, patients with prior irinotecan had median OS of 3.9 months, compared to 7.7 months in irinotecan naïve patients. PFS was also worse in patients with prior irinotecan, with PFS falling from 5.7 to 2.2 months.40 Petrelli et al did a meta-analysis comparing oxaliplatin and irinotecan therapies for PDAC treatment after administering gemcitabine. They found that second-line irinotecan-based regimens improved overall survival by 5.5 months, whereas patients who received oxaliplatin-based regimens improved OS by 5.3 months.41 These data suggest that additional cytotoxic agents might have a value in refractory pancreatic cancer patients.
Pelzer et al presented an interpretation of the NAPOLI-1 data for quality of life. Through statistical analysis of data, they presented Q-TWiST, which integrates quality and quantity of survival, by dividing periods into periods of treatment and toxicity (TOX). The authors evaluated treatment differences in quality-adjusted time without symptoms of disease progression or toxicity (Q-TWiST). This analysis also penalizes treatments with increased toxicities or shorter times to disease progression (REL) and rewarding those with lower TOX and longer PFS times. Q-TWiST data may help inform physicians in discussing quality of life issues in patients with pancreatic cancer when considering second-line chemotherapy. Patients with nal-IRI +5-FU/LV treatment had significantly more mean time in TWiST (3.4 vs 2.4) and TOX (1.0 vs 0.3), but similar REL (2.5 vs 2.7). Nal-IRI +5-FU/LV had 1.3 months greater Q-TWiST (5.1 vs 3.9). These data show that nal-IRI +5-FU/LV provided significantly greater quality-adjusted survival time compared to 5-FU/LV alone. In summary, treatment with nal-IRI with 5-FU/LV in patients refractory to gemcitabine would benefit regardless of their functional status, but the decision should be made individually based on physician’s discretion and shared decision-making.42 This study is particularly important, as quality of life decisions and data are particularly important since most of the patients are given cancer therapy to palliate their symptoms and to improve OS.
Nanoliposomal irinotecan: patient selection
Nanoliposomal irinotecan with 5-FU/LV (nal-IRI +5-FU/LV) has become accepted as a second-line treatment for PDAC after gemcitabine-based therapy. In NAPOLI-1, key inclusion criteria were good performance status and adequate hematological (absolute neutrophil counts >1.5×109 cells/L), hepatic (normal total bilirubin, and albumin levels ≥30 g/L), and renal function. Patient groups were further stratified by ethnicity, time since receiving most recent anticancer therapy, tumor stage at diagnosis, status of liver metastases, and baseline CA19-9. Adjusting for all these prognostic factors, nal-IRI +5-FU/LV showed an OS benefit in most of these patient populations. The only sub-groups favoring 5-FU/LV over nal-IRI +5-FU/LV were those treated on irinotecan previously, but definite conclusions cannot be made due to the small sample sizes of the subgroups. Since this study included few patients who were previously treated with irinotecan, the study concluded that the efficacy of nal-IRI after FOLFIRINOX is not clear. Also, it might be prudent not to offer systemic therapy in patients with poor performance status, as they were excluded from the study.19
Glassman et al demonstrated that the performance statuses of patients receiving nal-IRI are not significantly correlated with median OS and PFS. They enrolled 56 patients, and of those more than 20% had an ECOG (Eastern Cooperative Oncology Group) status of two or worse, compared with only 8.5% of patients who had a Karnofsky performance status of 70 or worse in NAPOLI-1 study. Median OS and PFS were not significantly different among different ECOG groups. However, it was reported that patients who previously progressed on previous irinotecan-based chemotherapy had significant short PFS and OS. They also compared the differences in median OS and PFS in treatment sequences. The OS seen across all sequences of treatments with FOLFIRINOX and/or nab-paclitaxel/gemcitabine prior to nal-IRI +5-FU/LV significantly increased with small differences in median OS. Median OS for patients with stage III or IV PDAC receiving nal-IR regardless of their first-line treatment since their first diagnosis was 24.2 months, ranging from 23 to 28 months. Also, it was shown that there is a trend that patients receiving nal-IRI +5-FU/LV in earlier lines of therapy had significant longer PFS and OS, although the sample size was very small.40 This is a potential source of future research, looking into other settings for nal-IRI usage in real-time practice experience.
Nanoliposomal irinotecan: toxicities
Studies have also examined nanoliposomal irinotecan’s toxicities, and the NAPOLI-1 study showed that diarrhea, vomiting, and anorexia were some of the most common toxicities. The percentage of adverse effects among three groups, nal-IRI +5-FU/LV, nal-IRI monotherapy, and 5-FU/LV alone, were detailed in Table 2. Patients receiving nal-IRI with and without 5-FU/LV experienced higher rates of adverse effects compared with 5-FU/LV alone. The overall percentages of patients experiencing various adverse effects were similar between those two groups, but those receiving nal-IRI and 5-FU/LV had a significantly higher rate of neutropenia. Furthermore, a significant percentage of patients experiencing neutropenia had grade 3 or 4 toxicity (27%) compared to 15% of irinotecan monotherapy and 2 (1%) of 5-FU/LV group. Patients receiving nal-IRI had higher rates of gastrointestinal (GI) complications. Specifically, 14% of nal-IRI patients had vomiting, whereas 11% of patients receiving dual therapy and 4% of those receiving 5-FU/ LV had this side effect.19 A long acting 5HT3 antagonist, such as palonosetron, can help with the delayed nausea and vomiting of patients on chemotherapy, including those receiving nal-IRI.43 Since one of the adverse events of 5-HT3 antagonist is constipation, it might also help with the diarrhea associated with use of cytotoxic chemotherapeutic agents. Approximately one third of patients receiving nal-IRI, whether as mono or dual therapy, required dose reduction. It was shown that 70% of monotherapy with nal-IRI patients had diarrhea, whereas 59% of patients receiving dual nal-IRI/5-FU/LV and 26% of those who receiving 5-FU/LV had this side effect.19
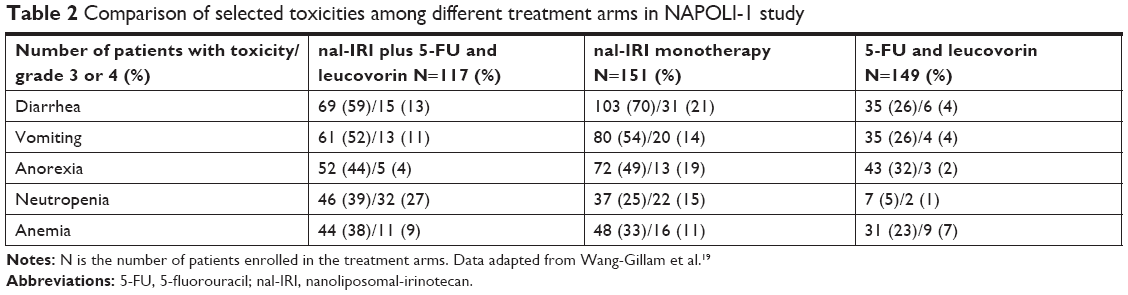 | Table 2 Comparison of selected toxicities among different treatment arms in NAPOLI-1 study |
These findings are similar to phase I and phase II trials of nal-IRI. In a study by Ko et al, which was a phase II trial, 75% of all patients had diarrhea. Fatigue was seen in 62% of patients and 20% had grade 3 or 4 toxicity in this regard.39 Forty percent of patients had neutropenia, and this was grade 3 or 4 in 30%. Chang et al (2015) detailed phase I findings, with high rates of patients with diarrhea and vomiting.44 Similar to later studies, neutropenia was common, with 33% experiencing this. Overall, the dose-limiting toxicities of nal-IRI seem to be myelosuppression and diarrhea. Kipps et al (2017) also reviewed the data on nal-IRI and offered interesting perspectives. They posit that a few different therapies can offer extended OS in the second-line setting, giving nal-IRI some value. However, they argue the strong rates of neutropenia and GI side effects are not insignificant in the palliative setting.45
Furthermore, the CONKO 003 study showed the benefit of aggressive second-line therapy in terms of OS in patients with metastatic PDAC. Specifically, they used oxaliplatin, 5-FU, and folinic acid. Although there is no clear comparison between that regimen and the 5-FU/ nal-IRI/ folinic acid used in the NAPOLI-1 trial, nal-IRI has the benefit of not being associated with paresthesia and neurotoxicity. Therefore, this helps to manage and maintain quality of life in patients with advanced malignancy and to offer a non-neurotoxic regimen since the majority of first-line chemotherapy causes neurotoxicity.25
The Memorial Sloan Kettering study experiences and outcomes with liposomal irinotecan toxicity were similar to prior studies – with nausea, vomiting, diarrhea, and neutropenia as common adverse events. The recommended dosage of nal-IRI is 70 mg/m2, but the median starting dose used in this study was 55 mg/m2, based on their physician’s preference.40 The effects of lower dose on percentage of adverse effects in the study cannot be completely excluded. They also described how dose reductions were most frequently due to fatigue and diarrhea. However, it is worth noting that dose reductions were not associated with worse outcomes. Overall, side effects were similar compared to the NAPOLI-1 trial, but lower rates of grade 3–4 toxicities may be due to the group’s lower starting doses. Common adverse events associated with liposomal irinotecan and 5-FU were anemia (89%), neutropenia (29%), diarrhea (63%), anorexia (57%), and vomiting (32%). Serious adverse events were less than 5% except for anemia 15%.40
The NAPOLI-1 trial did not compare nal-IRI with traditional irinotecan, either in outcomes or in toxicities. However, it is worthwhile to compare the two formulations of the drug, especially in terms of safety, and in a similar context. Neuzillet et al evaluated the regimen of folate, 5-FU, and irinotecan (FOLFIRI) in patients with PDAC who failed gemcitabine or platinum chemotherapy. They described approximately 57% of patients required a dose reduction. The investigators showed that hematologic and GI disturbances were common problems with patients receiving this regimen. They reported grade 3–4 hematologic toxicity in 17.5% of patients, and similar grade GI toxicity in 6.3% of patients.33
A recently presented poster from the ESMO conference also corroborated these findings. Ahn et al queried data from the Flatiron Health medical record database, which included over 2 million US cancer patients and 265 clinics. For similar dosages and lower mean performance status, in this real-world data, the authors found their cohort had fewer dose modifications than the NAPOLI-1 group. Overall, 27.2% of patients underwent a dose reduction. Progression was the most common cause for discontinuation, and overall, this study reported similar discontinuation rates compared to the NAPOLI-1 study.46
Overall, nal-IRI’s side effects and toxicities are similar to other cytotoxic chemotherapies. However, fewer toxicities were seen compared to traditional irinotecan. Furthermore, managing and preparing patients for these toxicities is where clinical experience is particularly useful. Although many patients experienced diarrhea, the drug’s stimulation of gut function can be a useful side effect in patients with metastatic PDAC who are on large doses of opiates, which can cause constipation and slowing of bowel function. However, in advanced pancreatic cancer patients who are not on opiate therapy, use of antimotility agents like loperamide and diphenoxylate-atropine (IMODIUM®) should be highly recommended. Irinotecan-based chemotherapy and chronic diarrhea also causes lactose intolerance, so it is advised for patient to avoid dairy products. Nausea and vomiting were also seen in high rates in patients receiving nal-IRI and is often seen in many patients on traditional irinotecan. Therefore, it is prudent to use long-acting anti-5-HT3 antagonists, such as palonosetron, to manage nausea and vomiting. It is important to treat these side effects preemptively rather than reactively. This is particularly important as a good way to encourage nutrition and maintain good quality of life while on treatment.
Clinical trials
The utilities of nal-IRI are being investigated in a number of clinical trials. In a few clinical trials including FUNGEMAX and FOOTPATH, the efficacy of nal-IRI/5-FU/LV is directly compared to gemcitabine and nab-paclitaxel as first-line therapy. Both of these trials are phase II. In another trial, nal-IRI is replacing traditional irinotecan as part of neoadjuvant FOLFIRINOX for patients who may undergo resection of pancreatic cancer. This is a single institution phase I trial seeking to recruit 30 patients. Another phase II trial is comparing nal-IRI with cabiralizumab and nivolumab immunotherapy and combinations of immunotherapy plus traditional chemotherapy. Another active, non-recruiting phase II trial is assessing the safety and efficacy of nal-IRI plus other therapies in previously untreated PDAC. This is a multi-site, combined phase I/II trial, with 56 actual participants, and is scheduled to be completed in 2020. Also, in the FOOTPATH trial, efforts are being made to find an optimized treatment sequence to ensure for maximal survival with more tolerable adverse effects. Examples of the ongoing clinical trials involving nal-IRI combination therapy are summarized in Table 3.47–52
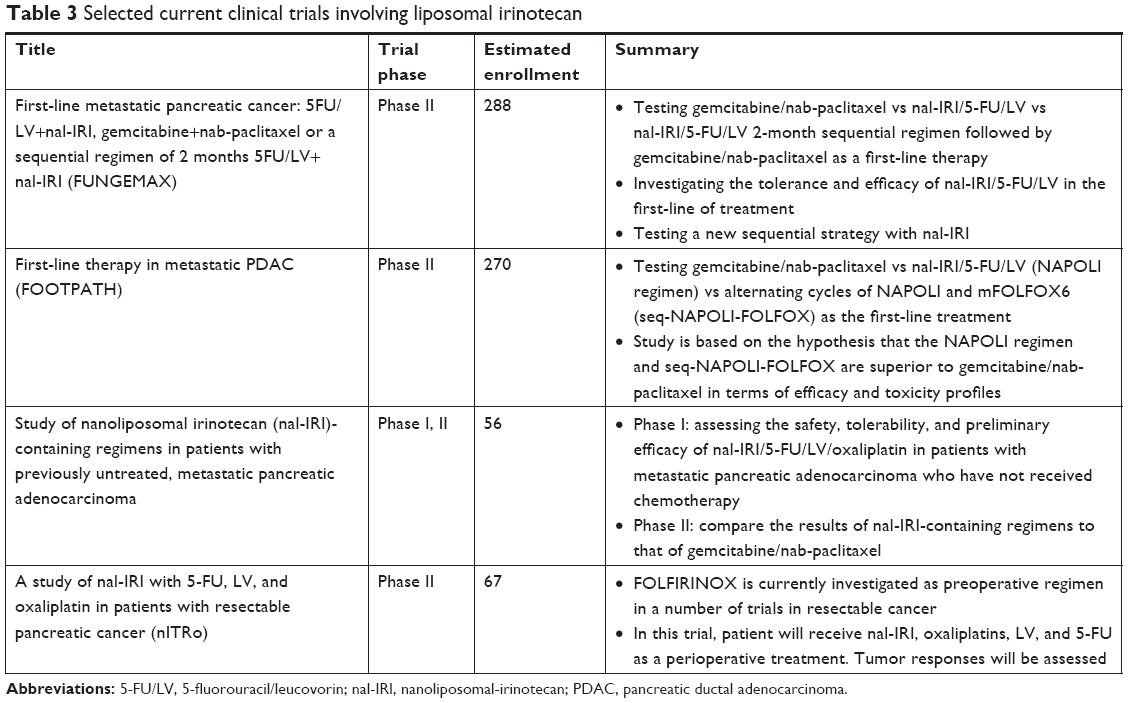 | Table 3 Selected current clinical trials involving liposomal irinotecan |
Conclusion
Pancreatic cancer is a highly lethal disease, with high rates of mortality. Extensive efforts have been made to advance therapy, but therapy options for patients who are refractory to first-line treatments are limited. Nanoliposomal irinotecan (nal-IRI) has been approved by the FDA and has been shown to improve overall median and PFS in NAPOLI-1, and subsequent real-life experience studies. Nal-IRI is associated with multiple adverse effects, most notably diarrhea, nausea, vomiting and myelosuppression, which are manageable in clinical practice. Recent data suggest that introducing nal-IRI early in the treatment paradigm significantly improved median OS and PFS. Multiple clinical trials are currently being conducted to use liposomal irinotecan in the early stage of pancreatic cancer and in other disease states.
Disclosure
Minsig Choi has served as consultant and speaker for Ipsen and Celgene. The authors report no other conflicts of interest in this work.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. | ||
Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. | ||
Rhim AD, Mirek ET, Aiello NM, et al. EMT and dissemination precede pancreatic tumor formation. Cell. 2012;148(1–2):349–361. | ||
Zavoral M, Minarikova P, Zavada F, Salek C, Minarik M. Molecular biology of pancreatic cancer. World J Gastroenterol. 2011;17(24):2897–2908. | ||
Morton JP, Timpson P, Karim SA, et al. Mutant p53 drives metastasis and overcomes growth arrest/senescence in pancreatic cancer. Proc Natl Acad Sci USA. 2010;107(1):246–251. | ||
Ahmed S, Bradshaw AD, Gera S, Dewan M, Xu R. The TGF-β/Smad4 signaling pathway in pancreatic carcinogenesis and its clinical significance. J Clin Med. 2017;6(1):5. | ||
Moffitt RA, Marayati R, Flate EL, et al. Virtual microdissection identifies distinct tumor- and stroma-specific subtypes of pancreatic ductal adenocarcinoma. Nat Genet. 2015;47(10):1168–1178. | ||
Ying H, Kimmelman AC, Lyssiotis CA, et al. Oncogenic KRAS maintains pancreatic tumors through regulation of anabolic glucose metabolism. Cell. 2012;149(3):656–670. | ||
Biankin AV, Waddell N, Kassahn KS, et al. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature. 2012;491(7424):399–405. | ||
Maire F, Micard S, Hammel P, et al. Differential diagnosis between chronic pancreatitis and pancreatic cancer: value of the detection of KRAS2 mutations in circulating DNA. Br J Cancer. 2002;87(5):551–554. | ||
Choi M, Bien H, Mofunanya A, Powers S. Challenges in Ras therapeutics in pancreatic cancer. Semin Cancer Biol. 2017;pii:S1044–579X(17):30235–30243. | ||
Vincent A, Herman J, Schulick R, Hruban RH, Goggins M. Pancreatic cancer. The Lancet. 2011;378(9791):607–620. | ||
Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297(3):267–277. | ||
Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361(14):1368–1375. | ||
Gillen S, Schuster T, Meyer Zum Büschenfelde C, Friess H, Kleeff J. Preoperative/neoadjuvant therapy in pancreatic cancer: a systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010;7(4):e1000267. | ||
Ghosn M, Ibrahim T, Assi T, El Rassy E, Kourie HR, Kattan J. Dilemma of first line regimens in metastatic pancreatic adenocarcinoma. World J Gastroenterol. 2016;22(46):10124–10130. | ||
National Comprehensive Cancer Network (NCCN). Pancreatic adenocarcinoma version 2; 2018. Available from: https://www.nccn.org/professionals/physician_gls/default.aspx. Accessed December 24, 2018. | ||
Ducreux M. Cancer of the pancreas: ESMO clinical practice guidelines. ESMO. 2015;26(5):56–68. | ||
Wang-Gillam A, Li CP, Bodoky G, et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. The Lancet. 2016;387(10018):545–557. | ||
Burris HA, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15(6):2403–2413. | ||
Conroy T, Desseigne F, Ychou M, for the Groupe Tumeurs Digestives of Unicancer and the PRODIGE Intergroup. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. | ||
Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. | ||
Nagrial AM, Chin VT, Sjoquist KM, et al. Second-line treatment in inoperable pancreatic adenocarcinoma: a systematic review and synthesis of all clinical trials. Crit Rev Oncol Hematol. 2015;96(3):483–497. | ||
Schrag D, Archer L, Wang X, Romanus D, Mulcahy M, Goldberg R, Kindler H. A patterns-of-care study of post-progression treatment (Rx) among patients (pts) with advanced pancreas cancer (APC) after gemcitabine therapy on Cancer and Leukemia Group B (CALGB) study #80303. J Clin Oncol. 2007;25(Suppl 18): Abstract 4524. | ||
Oettle H, Riess H, Stieler JM, et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: outcomes from the CONKO-003 trial. J Clin Oncol. 2014;32(23):2423–2429. | ||
Gill S, Ko YJ, Cripps C, et al. PANCREOX: a randomized phase III study of fluorouracil/leucovorin with or without oxaliplatin for second-line advanced pancreatic cancer in patients who have received gemcitabine-based chemotherapy. J Clin Oncol. 2016;34(32):3914–3920. | ||
El Rassy E, Assi T, El Karak F, Ghosn M, Kattan J. Could the combination of nab-paclitaxel plus gemcitabine salvage metastatic pancreatic adenocarcinoma after FOLFIRINOX failure? A single institutional retrospective analysis. Clin Res Hepatol Gastroenterol. 2017;41(2):e26–e28. | ||
Marsh S, Hoskins JM. Irinotecan pharmacogenomics. Pharmacogenomics. 2010;11(7):1003–1010. | ||
Yoo C, Hwang JY, Kim JE, et al. A randomised phase II study of modified FOLFIRI.3 vs modified FOLFOX as second-line therapy in patients with gemcitabine-refractory advanced pancreatic cancer. Br J Cancer. 2009;101(10):1658–1663. | ||
Gebbia V, Maiello E, Giuliani F, Borsellino N, Arcara C, Colucci G. Irinotecan plus bolus/infusional 5-fluorouracil and leucovorin in patients with pretreated advanced pancreatic carcinoma: a multicenter experience of the Gruppo Oncologico Italia Meridionale. Am J Clin Oncol. 2010;33(5):461–464. | ||
Cereda S, Reni M, Rognone A, et al. XELIRI or FOLFIRI as salvage therapy in advanced pancreatic cancer. Anticancer Res. 2010;30(11):4785–4790. | ||
Zaniboni A, Aitini E, Barni S, et al. FOLFIRI as second-line chemotherapy for advanced pancreatic cancer: A GISCAD multicenter phase II study. Cancer Chemother Pharmacol. 2012;69(6):1641–1645. | ||
Neuzillet C, Hentic O, Rousseau B, et al. FOLFIRI regimen in metastatic pancreatic adenocarcinoma resistant to gemcitabine and platinum-salts. World J Gastroenterol. 2012;18(33):4533–4541. | ||
Assaf E, Verlinde-Carvalho M, Delbaldo C, et al. 5-fluorouracil/leucovorin combined with irinotecan and oxaliplatin (FOLFIRINOX) as second-line chemotherapy in patients with metastatic pancreatic adenocarcinoma. Oncology. 2011;80(5–6):301–306. | ||
Drummond DC, Meyer O, Hong K, Kirpotin DB, Papahadjopoulos D. Optimizing liposomes for delivery of chemotherapeutic agents to solid tumors. Pharmacol Rev. 1999;51(4):691–744. | ||
Maeda H. Tumor-selective delivery of macromolecular drugs via the EPR effect: background and future prospects. Bioconjug Chem. 2010;21(5):797–802. | ||
Kalra AV, Kim J, Klinz SG, et al. Preclinical activity of nanoliposomal irinotecan is governed by tumor deposition and intratumor prodrug conversion. Cancer Res. 2014;74(23):7003–7013. | ||
Kim G, Kim GP. MD: role of liposomal in nanoliposomal irinotecan. Targeted Oncology. 2016. | ||
Ko AH, Tempero MA, Shan YS, et al. A multinational phase 2 study of nanoliposomal irinotecan sucrosofate (PEP02, MM-398) for patients with gemcitabine-refractory metastatic pancreatic cancer. Br J Cancer. 2013;109(4):920–925. | ||
Glassman DC, Palmaira RL, Covington CM, et al. Nanoliposomal irinotecan with fluorouracil for the treatment of advanced pancreatic cancer, a single institution experience. BMC Cancer. 2018;18(1):1–10. | ||
Petrelli F, Inno A, Ghidini A, et al. Second line with oxaliplatin- or irinotecan-based chemotherapy for gemcitabine-pretreated pancreatic cancer: a systematic review. Eur J Cancer. 2017;81:174–182. | ||
Pelzer U, Blanc JF, Melisi D, et al. Quality-adjusted survival with combination nal-IRI+5-FU/LV vs 5-FU/LV alone in metastatic pancreatic cancer patients previously treated with gemcitabine-based therapy: a Q-TWiST analysis. Br J Cancer. 2017;116(10):1247–1253. | ||
Rubenstein E. Palonosetron: a unique 5-HT3 receptor antagonist indicated for the prevention of acute and delayed chemotherapy-induced nausea and vomiting. Clin Adv Hematol Oncol. 2004;5:284–289. | ||
Chang TC, Shiah HS, Yang CH, et al. Phase I study of nanoliposomal irinotecan (PEP02) in advanced solid tumor patients. Cancer Chemother Pharmacol. 2015;75(3):579–586. | ||
Kipps E, Young K, Starling N. Liposomal irinotecan in gemcitabine-refractory metastatic pancreatic cancer: efficacy, safety and place in therapy. Ther Adv Med Oncol. 2017;9(3):159–170. | ||
Ahn D, Barzi A, Miksad R. Real-world dosing patterns of patients with metastatic pancreatic cancer (mPC) treated with liposomal irinotecan (nal-IRI) in US oncology clinics. Presented at European Society for medical oncology; 2018; Munich, Germany. | ||
Randomized phase II study comparing 5FU/LV+nal-IRI, gemcitabine+nab-paclitaxel or a sequential regimen of 2 months 5FU/LV+nal-IRI followed by two months of gemcitabine+nab-paclitaxel, in metastatic pancreatic cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT03693677. NLM identifier: NCT03693677. Accessed December 24, 2018. | ||
Second-line therapy with nal-IRI after failure gemcitabine/nab-paclitaxel in advanced pancreatic cancer – predictive role of 1st-line therapy. Available from: https://clinicaltrials.gov/ct2/show/NCT03468335. NLM identifier: NCT03468335. Accessed December 24, 2018. | ||
A study of Nal-IRI With 5-FU, Levofolinic Acid and Oxaliplatin in Patients with Resectable Pancreatic Cancer (nITRo). Available from: https://clinicaltrials.gov/ct2/show/NCT03528785. NLM identifier: NCT03528785. Accessed December 24, 2018. | ||
A randomized, open-label phase 2 study of nanoliposomal irinotecan (nal-IRI)-containing regimens versus nab-paclitaxel plus gemcitabine in patients with previously untreated, metastatic pancreatic adenocarcinoma. Available from: https://clinicaltrials.gov/ct2/show/NCT02551991. NLM identifier: NCT02551991. Accessed December 24, 2018. | ||
Alternating neoadjuvant gemcitabine-nab-paclitaxel and nanoliposomal irinotecan (nal-IRI) with 5-fluorouracil and folinic acid (leucovorin) regimens in resectable and borderline resectable pancreatic cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT03703063. NLM identifier: NCT03703063. Accessed December 24, 2018. | ||
A multicenter randomized phase II study to determine the optimal first-line chemotherapy regimen in patients with metastatic pancreatic cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT03487016. NLM identifier: NCT03487016. Accessed December 24, 2018. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.