")
Back to Journals » Cancer Management and Research » Volume 10
Spotlight on dabrafenib/trametinib in the treatment of non-small-cell lung cancer: place in therapy
Authors Weart TC, Miller KD, Simone CB 2nd
Received 27 November 2017
Accepted for publication 20 February 2018
Published 3 April 2018 Volume 2018:10 Pages 647—652
DOI https://doi.org/10.2147/CMAR.S142269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Lu-Zhe Sun
Thomas C Weart, Kenneth D Miller, Charles B Simone II
Marlene and Stewart Greenebaum Comprehensive Cancer Center, University of Maryland Medical Center, Baltimore, MD, USA
Abstract: Advanced non-small-cell lung cancer (NSCLC) remains a challenging disease. The limited utility of chemotherapy indicates the need for additional therapeutic options. Targeted therapy continues to be an important tool in the treatment of NSCLC. Mutations within the RAS–RAF–MEK–MAPK pathway, specifically the BRAF V600E mutation, have become an important target for the subset of NSCLC patients with this mutation. This paper summarizes the clinical evidence that lead to the recent approval of the combination of dabrafenib and trametinib to treat patients with advanced NSCLC who harbor a BRAF V600E mutation.
Keywords: BRAF mutation, MEK, NSCLC, lung cancer, dabrafenib, trametinib
Introduction
Advanced non-small-cell lung cancer (NSCLC) continues to be a significant health burden worldwide. Over 85% of lung cancer cases are NSCLC,1 with 10%–30% of these cases occurring in nonsmokers.2 Lung cancer results in 1.6 million deaths annually worldwide and is projected to cause 155,000 deaths in the United States alone in 2017.3,4 While patients with early-stage disease hold the greatest chance for cure, approximately 70% of NSCLC patients present with advanced or metastatic disease at time of diagnosis.5 Traditional platinum-based combination chemotherapy results in response rates (RRs) of approximately 20%–40%.6–10 Unfortunately, durable long-term responses remain elusive, and the median survival for patients with advanced NSCLC remains at only 1 year from diagnosis.
The advent of targeted therapy offers the possibility of prolonged survival beyond the limited response seen with traditional cytotoxic chemotherapy. With the recent approval of dabrafenib and trametinib (TAFINLAR® and MEKINIST®, Novartis Pharmaceuticals Inc., Basel, Switzerland) in combination for advanced NSCLC in patients with a BRAF V600E mutation, we now have an additional tool to treat these patients.
BRAF mutation as a therapeutic target
The BRAF gene is a 2,949 base pair sequence of 18 exons found on chromosome 7q34, encoding a 766 amino acid peptide.11 The BRAF protein is a member of the Raf family of serine/threonine kinases. BRAF is a critical component of the RAS–RAF–MEK–MAPK pathway whereupon activated BRAF promotes increased cell proliferation and survival.
The normal cascade begins with GTP-bound RAS, which recruits inactive BRAF dimers to the cell membrane, whereupon BRAF is then phosphorylated.12 Activated cytosolic and membrane-bound BRAF then activate MEK1 and MEK2. The MEK proteins then phosphorylate and activate the MAPK/ERK proteins: ERK1 and ERK2.13 While these events occur within a complex composed of several scaffolding proteins, activated ERK proteins dissociate from the scaffolding proteins and the RAF/MEK/ERK complex to complete a series of downstream effects. Activated ERK1/2 targets include transcription factors, ribosomal proteins, and proteins of the cytoskeleton.14 These targets are critical to cell growth.
The discovery of activating BRAF mutations within a variety of tumor types has established BRAF as a true protooncogene. Mutations in BRAF are present in as many as 7%–9% of all malignancies.15 Namely, BRAF mutations have been reported in as many as 97% of hairy cell leukemias,16 70% of melanomas,17 50% of papillary and anaplastic thyroid cancers,18 and 10% of colon cancers.19
Although many types of BRAF mutations have been observed within the kinase region, the V600 (T1799A) mutation at exon 15 is often seen.17 The V600E mutation is a single substitution of the T→A nucleotide transversion at codon 600, resulting in the amino acid valine rather than glutamate.20 This mutation disrupts the hydrophobic interactions between the activating region and the glycine-rich P loop within the BRAF kinase. While these hydrophobic interactions within wild-type BRAF maintain the kinase in an inactive state, the V600E mutation results in constitutive activation of the kinase.21
Within NSCLC, BRAF mutations are present in approximately 1.5%–4% of cases. Approximately 50% of BRAF mutations seen in NSCLC are the V600E mutation.17 A 2016 meta-analysis of 16 studies composed of 11,711 patients with NSCLC revealed a female-to-male predominance (62.5% vs 32.6%) to harbor the BRAF V600E mutation. Additionally, the V600E mutation was found more frequently in never smokers than current or former smokers. Patients with adenocarcinoma NSCLC were over 4.5 times more likely to harbor the V600E mutation when compared to nonadenocarcinoma NSCLC.22 In contrast, non-V600E BRAF mutations occur almost exclusively in current or former smokers. Notably, BRAF non-V600E mutations also tend to appear with concurrent KRAS mutations.23
Early clinical experience of dabrafenib: use as monotherapy and development of resistance
Dabrafenib is an inhibitor of multiple mutated forms of the BRAF kinase. In vitro testing of selectivity of dabrafenib to 270 kinases, including BRAF, showed a 400-fold selectivity of dabrafenib to BRAF in 91% of the kinases tested.24 In vitro models have demonstrated that dabrafenib significantly decreases ERK phosphorylation, resulting in cell arrest in G1 phase and subsequent cell death.25
In the treatment of metastatic melanoma, the phase III, open-label, BREAK-3 trial demonstrated superior efficacy of dabrafenib monotherapy over standard chemotherapy. Of the 733 Stage IV or unresectable Stage III melanoma patients screened for the trial, 250 patients were randomly assigned to receive dacarbazine chemotherapy (1,000 mg/m2 intravenously every 3 weeks) or oral dabrafenib monotherapy (150 mg twice daily). In total, 187 patients were assigned to the dabrafenib group and 63 patients were in the dacarbazine group. The median progression-free survival (PFS) for the dabrafenib group was 5.1 months compared to 2.7 months for the dacarbazine group with a hazard ratio of 0.30 (95% confidence interval [CI]: 01.8–0.51; p<0.0001).26 However, most patients in the dabrafenib group developed disease resistance within 1 year following initial disease response (Table 1).27
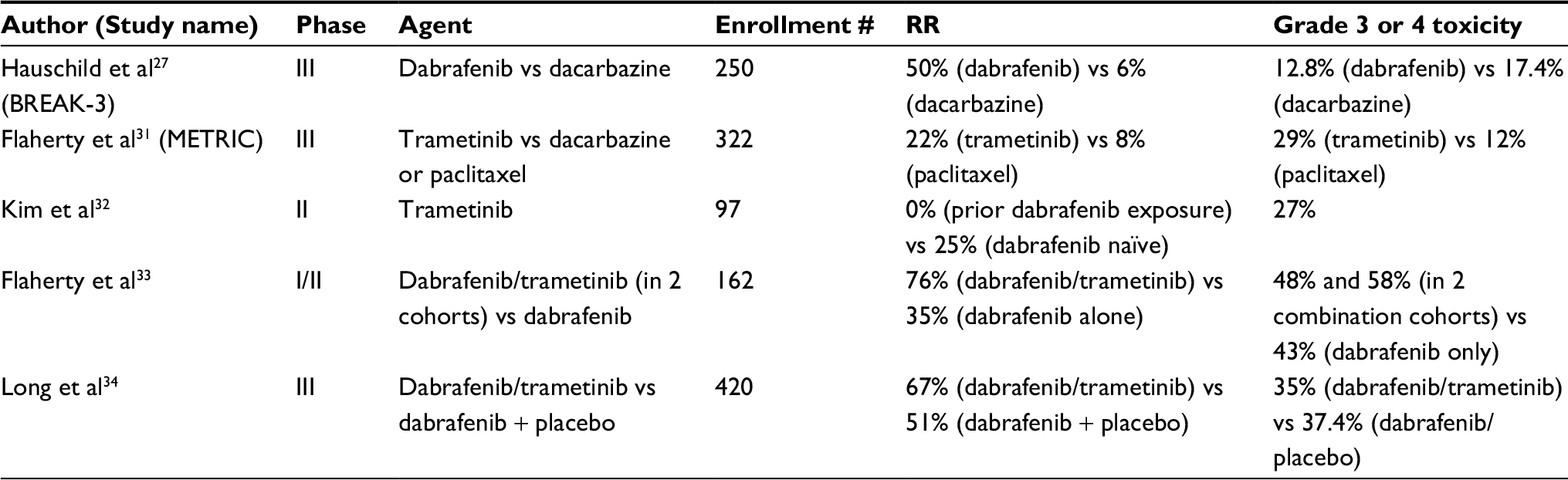 | Table 1 Melanoma phase II and III clinical trials using BRAF and MEK inhibition Abbreviation: RR, response rate. |
While inherent resistance to BRAF inhibition exists in melanoma, only approximately 10% of BRAF resistance in mutated-BRAF cases are reported to be inherent. The remaining 90% of BRAF inhibition-resistant melanoma cases are acquired.28 The development of BRAF inhibition resistance is further complicated by tumor heterogeneity and the development of multiple resistance pathways within the same tumor. Universally, all patients develop multiple mechanisms of resistance to BRAF inhibition. Known resistance pathways within melanoma include acquired reactivating mutations within MAPK (NRAS, KRAS, BRAF amplification, BRAF alternative splicing, MEK1/2, and CDKN2A) and alterations within the PI3K–PTEN–AKT pathway.29 This phenomenon of BRAF inhibitor resistance spurred the advent of targeted combination therapy.
Melanoma and trametinib: the development of combination RAS–RAF–MEK–MAPK pathway targeted therapy
Trametinib is a MAPK kinase/MEK inhibitor. As BRAF is directly upstream from the MEK kinase, activating mutations in BRAF result in constitutively activated MEK with subsequent activation of the MAPK/ERK pathway.30
As monotherapy, trametinib was found to be highly active in metastatic melanoma with the results of the multicenter, phase III, open-label, METRIC Study. In that trial, 322 patients with metastatic melanoma with either V600E or V600K BRAF mutations were randomized to receive either trametinib (2 mg orally) once daily or dacarbazine (1,000 mg/m2) IV or paclitaxel (175 mg/m2) every 3 weeks. The median PFS (4.8 months vs 1.5 months, p<0.001) and overall survival (OS) rate at 6 months (81% vs 67%, p=0.01) were improved in patients receiving trametinib compared with chemotherapy (Table 1).31
Additionally, a phase III trial evaluated trametinib monotherapy in metastatic melanoma patients with known BRAF V600E or V600K mutations previously treated with or without a BRAF inhibitor. Of the 40 patients who previously received a BRAF inhibitor, there were no confirmed treatment responses, although 28% maintained stable disease (SD), and the PFS was 1.8 months. In the BRAF inhibitor-naïve group (57 patients), there was one (2%) complete response (CR), 13 (23%) partial responses (PRs), and 29 patients (51%) with SD, for an overall confirmed RR of 25%, and a median PFS of 4.0 months (Table 1).32 Theses data lead to United States Food and Drug Administration (FDA) approval of trametinib as monotherapy for BRAF inhibitor-naïve metastatic melanoma patients.
BRAF and MEK inhibition combination therapy was first analyzed by Flaherty et al33 in an open-label, phase I/II study of 247 patients with metastatic melanoma and BRAF V600 mutations. The phase I portion verified safety of oral dabrafenib (75 or 150 mg twice daily) and trametinib (1, 1.5, or 2 mg daily) in 85 patients. Subsequently, 162 patients were randomized to receive combination therapy with dabrafenib (150 mg) plus trametinib (1 or 2 mg) or dabrafenib monotherapy. Combination therapy allowed for an improved median PFS (9.4 months vs 5.8 months, p<0.001) and a higher CR or PR rate (76% vs 54%, p=0.03) (Table 1).33
In a randomized phase III trial, Long et al34 randomly assigned 423 previously untreated stage IIIC or stage IV melanoma patients with a BRAF V600E or V600K mutation to receive a combination of dabrafenib (150 mg orally twice daily) and trametinib (2 mg orally once daily) or dabrafenib and placebo. The median PFS was 9.3 months in the combination group vs 8.8 months in the dabrafenib-only group (p=0.03). The overall RR was 67% in the dabrafenib/trametinib group and 51% in the dabrafenib-only group (p=0.002). The 6-month OS was 93% with dabrafenib/trametinib and 85% with dabrafenib alone (p=0.02) (Table 1).34 These collective results demonstrated the utility of BRAF/MEK inhibition combination therapy in melanoma. However, as compared to Flaherty’s phase II study, Long’s phase III study indicates that while the benefit of combination therapy over dabrafenib monotherapy is clinically and statistically significant, a smaller benefit was seen with a larger study population.
Evidence of BRAF and MEK inhibitor monotherapy and in combination for NSCLC treatment
The success of BRAF and MEK inhibition using dabrafenib, trametinib, and other agents in the treatment of metastatic melanoma generated increased interest in a variety of other malignancies that also harbor BRAF mutations, particularly NSCLC.
Preclinical NSCLC cell line studies have shown that in tumor cells with BRAF V600E and non-V600E mutations, BRAF and MEK inhibitory agents as monotherapy and in combination are proapoptotic. However, BRAF and MEK inhibition in combination has been shown to cause increased apoptosis in V600E- and non-V600E-mutated NSCLC cell lines as compared to BRAF or MEK inhibitor monotherapy.35,36
The first case report in 2012 of BRAF inhibition in NSCLC (off-label) using vemurafenib (BRAF Inhibitor: ZELBORAF®, Genentech, Inc.©, San Francisco, CA, USA) showed a therapeutic response; however, these results were discovered at autopsy as the patient died from complications from heart failure 3 weeks after initiation of treatment (Table 2).37
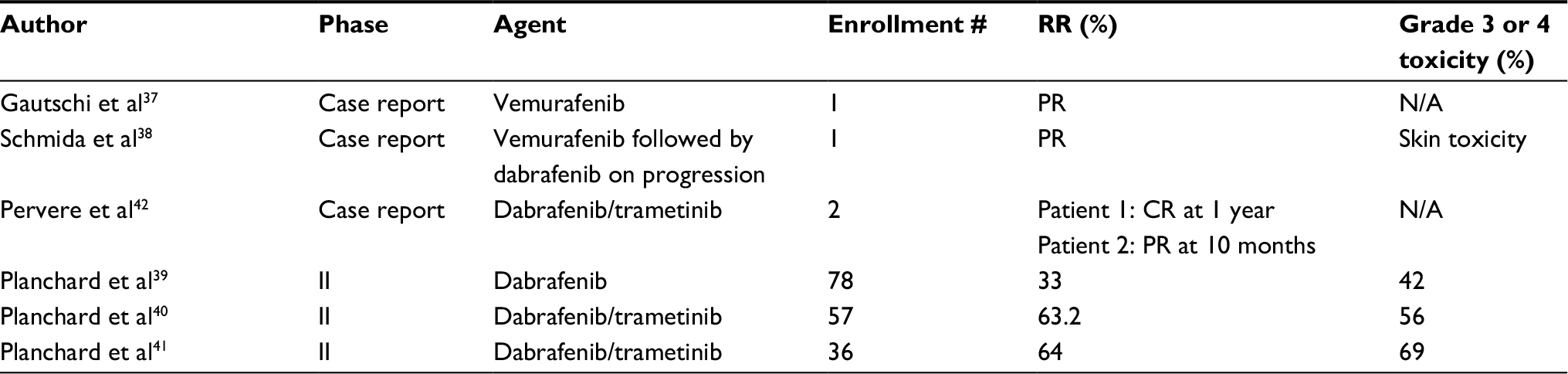 | Table 2 NSCLC case reports and clinical trials using BRAF and MEK inhibition Abbreviations: CR, complete response; NSCLC, non-small-cell lung cancer; PR, partial response; RR, response rate; N/A, not available. |
Additionally, a 2014 case report also revealed continued clinical benefit in a NSCLC patient with a BRAF V600E mutation who received second-line vemurafenib following standard chemotherapy. Upon progression, vemurafenib was discontinued, and the patient received docetaxel thereafter. However, upon the development of malignant ascites, the patient was switched to dabrafenib and had continued disease response for approximately 3 months before disease progression (Table 2).38
Within the context of a clinical trial, dabrafenib was first evaluated by Planchard et al39 in a multicenter, nonrandomized, open-label, phase II study published in 2016. The study enrolled 78 patients with Stage IV NSCLC who had already received first-line systemic chemotherapy. Patients received 150 mg orally of dabrafenib twice daily. The primary endpoint was overall response (PR or CR), and secondary endpoints were OS, PFS, duration of response, disease control for longer than 12 weeks, pharmacokinetics, and safety and tolerability of dabrafenib. At a median follow-up of 10.7 months, the median exposure to dabrafenib was 4.6 months. Overall response by investigator assessment was observed in 26 of 78 (33%; 95% CI: 23%–45%) previously treated patients, with each of these responses being PRs. However, 73% of responses were reported during the first assessment at 6 weeks. Median PFS was 5.5 months. Disease control was achieved in 58% of patients.
Notably, 83 (99%) of 84 patients had at least one adverse event, while 45 (54%) of 84 patients experienced grade 2 or greater adverse events. The most common grade 3 adverse event was the development of cutaneous squamous cell carcinoma or basal cell carcinoma, which was seen in 12% and 5% of patients, respectively. Only 6% of patients had adverse events that resulted in the discontinuation of dabrafenib. The most common adverse events were grade 1–2 pyrexia (33% of patients) and hyperkeratosis (29% of patients).39
This study also evaluated the combination of dabrafenib and trametinib in BRAF V600E mutated NSCLC as two separate cohorts not included in the phase II dabrafenib monotherapy results. These patients were also evaluated within a phase II, multicenter, randomized, open-label study that enrolled 57 patients who received dabrafenib 150 mg twice daily (oral) and trametinib 2 mg daily (oral) in continuous 21 day cycles. As in the dabrafenib monotherapy study, the primary endpoint was overall response (PR or CR). Early results reported that 36 of 57 patients (63.2% [95% CI: 49.3–75.6]) achieved an investigator-assessed overall response. With 9 patients (16%) maintaining SD, the investigators found that 45 (78.9%) of enrolled patients maintained disease control (CR + PR + SD). PFS was 9.7 months (6.9–19.6), while the duration of response was 9.0 months (6.9–18.3). The most common adverse event, as in the dabrafenib monotherapy study, was grade 1–2 pyrexia (reported in 44% of patients). Serious adverse events were reported in 32 of 57 (56%) patients and included pyrexia (16%), anemia (5%), confusional state (4%), decreased appetite (4%), hemoptysis (4%), hypercalcemia (4%), nausea (4%), and cutaneous squamous cell carcinoma (4%). The most common grade 3–4 adverse events were neutropenia (9%), hyponatremia (7%), and anemia (5%).40
In the updated results published online ahead of print in September 2017, the investigators reported that of the 36 patients enrolled (median follow-up 15.9 months) and treated with first-line dabrafenib plus trametinib, an overall response was achieved in 23 patients (64%, 95% CI: 46–79), with two (6%) patients achieving a CR and 21 patients (58%) achieving a PR. All patients had one or more adverse event of any grade, and 25 (69%) had one or more grade 3 or 4 events. The most common grade 3 or 4 adverse event was pyrexia (11%). Serious adverse events occurring in more than two patients included alanine aminotransferase increase (14%), pyrexia (11%), aspartate aminotransferase increase (8%), and ejection fraction decrease (8%). One fatal serious adverse event deemed unrelated to study treatment was reported (cardiorespiratory arrest).41 The FDA-approved dabrafenib and trametinib in combination for metastatic NSCLC with a BRAF V600E mutation on June 22, 2017, based on these results under the Study designations of BRF113928 /CDRB436E2201/NCT01336634 (Table 2).
Limitations of this study discussed by the investigators include the following: small sample size, nonrandomization of the study, and lack of quality of life indicators within the study results. However, the investigators are reviewing the quality of life information of these patients, and it is expected that these findings will be reported in the future. Despite these limitations, the results from this trial demonstrate a clear benefit with the therapy combination of dabrafenib/trametinib in the treatment of BRAF V600E mutated NSCLC to warrant further investigation.
Future directions
Currently, the FDA approval of dabrafenib and trametinib in combination for BRAF V600E-mutated NSCLC patient is limited to patients with metastatic disease in first, second, or third line. However, the study that led to the current approval did not fully evaluate utility in the first-line setting. Additionally, the dabrafenib/trametinib combination has yet to be evaluated head-to-head with chemotherapy or other targeted therapies as first-line therapy. The role of this combination in the neoadjuvant or adjuvant settings remains unclear in early or locally advanced disease. No current clinical trials are underway evaluating the dabrafenib/trametinib combination, but further study is warranted to evaluate these current knowledge gaps. Similarly, the role of this targeted therapy used concurrently or sequentially with radiotherapy remains unknown.
Conclusion
The BRAF pathway has proven to be important in a variety of malignancies. The combination of dabrafenib and trametinib is now available for the treatment of metastatic NSCLC, with clear evidence of patient benefit. However, the role of this targeted therapy combination outside of the metastatic setting or with other treatment modalities remains unclear. Despite these unresolved issues, the dabrafenib/trametinib combination therapy has emerged as a viable tool to treat a carefully selected subset of NSCLC patients.
Disclosure
The authors report no conflicts of interest in this work.
References
Reck M, Popat S, Reinmuth N, et al. Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(Suppl 3):iii27–iii39. | ||
Wakelee HA, Chang ET, Gomez SL, et al. Lung cancer incidence in never smokers. J Clin Oncol. 2007;25(5):472–478. | ||
Stewart BW, Wild CP, editors. World Cancer Report 2014. Lyon, France: International Agency for Research on Cancer; 2014. | ||
SEER Research Data 1973–2014 – ASCII Text Data: Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) Research Data (1973–2014), National Cancer Institute, DCCPS, Surveillance Research Program, released April 2017, based on the November 2016 submission. | ||
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–594. | ||
Sandler AB, Nemunaitis J, Denham C, et al. Phase III trial of gemcitabine plus cisplatin vs cisplatin alone in patients with locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol. 2000;18(1):122–130. | ||
Gatzemeier U, von Pawel J, Gottfried M, et al. Phase III comparative study of high-dose cisplatin versus a combination of paclitaxel and cisplatin in patients with advanced non-small cell lung cancer. J Clin Oncol. 2000;18(19):3390–3399. | ||
Von Pawel J, von Roemeling R, Gatzemeier U, et al. Tirapazamine plus cisplatin versus cisplatin in advanced non-small-cell lung cancer: a report of the International CATAPULT 1 Study Group. Cisplatin and tirapazamine in subjects with advanced previously untreated non-small-cell lung tumors. J Clin Oncol. 2000;18(6):1351–1359. | ||
LeChevalier T, Brisgand D, Douillard JY, et al. Randomised study of vinorelbine and cisplatin versus vindesine and cisplatin versus vinorelbine alone in non-small-cell lung cancer. Results of an European multicenter trial including 612 patients. J Clin Oncol. 1994;12(2):360–367. | ||
Bonomi P, Kim K, Chang A, Johnson D. Phase III trial comparing etoposide/cisplatin versus taxol with cisplatin G-CSF versus taxol/cisplatin in advanced non-small cell lung cancer [abstract 1145]. Proc Am Soc Clin Oncol. 1996;15:382. | ||
Huang T, Karsy M, Zhuge J, Zhong M, Liu D. B-Raf and the inhibitors: from bench to bedside. J Hematol Oncol. 2013;6:30. | ||
Tuveson DA, Weber BL, Herlyn M. BRAF as a potential therapeutic target in melanoma andother malignancies. Cancer Cell. 2003;4(2):95–98. | ||
Chong H, Vikis HG, Guan KL. Mechanisms of regulating the Raf kinase family. Cell Signal. 2003;15(5):463–469. | ||
Schaeffer HJ, Weber MJ. Mitogen-activated protein kinases: specific messages from ubiquitous messengers. Mol Cell Biol. 1999;19(4):2435–2444. | ||
Nazarian R, Shi H, Wang Q, et al. Melanomas acquire resistance to B-RAF(V600E) inhibition by RTK or N-RAS upregulation. Nature. 2010;468(7326):973–977. | ||
Tiacci E, Trifonov V, Schiavoni G, et al. BRAF mutations in hairy-cell leukemia. N Engl J Med. 2011;364(24):2305–2315. | ||
Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417(6892):949–954. | ||
Fagin JA, Mitsiades N. Molecular pathology of thyroid cancer: diagnostic and clinical implications. Best Pract Res Clin Endocrinol Metab. 2008;22(6):955–969. | ||
Lin CC, Lin JK, Lin TC, et al. The prognostic role of microsatellite instability, codon-specific KRAS, and BRAF mutations in colon cancer. J Surg Oncol. 2014;110(4):451–457. | ||
Holderfield M, Deuker MM, McCormick F, McMahon M. Targeting RAF kinases for cancer therapy: BRAF-mutated melanoma and beyond. Nat Rev Cancer. 2014;14(7):455–467. | ||
Fiskus W, Mitsiades N. B-Raf inhibition in the clinic: present and future. Annu Rev Med. 2016;67:29–43. | ||
Cui G, Liu D. A meta-analysis of the association between BRAF mutation and nonsmall cell lung cancer. Medicine. 2017;96(14):e6552. | ||
Tissot C, Couraud S, Tanguy R, Bringuier PP, Girard N, Souquet PJ. Clinical characteristics and outcome of patients with lung cancer harboring BRAF mutations. Lung Cancer. 2016;91:23–28. | ||
Ballantyne AD, Garnock-Jones KP. Dabrafenib: first global approval. Drugs. 2013;73(12):1367–1376. | ||
Laquerre S, Arnone M, Moss K, et al. Abstract B88: a selective Raf kinase inhibitor induces cell death and tumor regression of human cancer cell lines encoding B-Raf V600E mutation. Mol Cancer Ther. 2009;8(12 Suppl):B88. | ||
Hauschild A, Grob JJ, Demidov LV, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2012;380(9839):358–365. | ||
Hauschild A, Grob JJ, Demidov LV, et al. An update on BREAK-3, a phase III, randomized trial: dabrafenib (DAB) versus dacarbazine (DTIC) in patients with BRAF V600E-positive mutation metastatic melanoma (MM). J Clin Oncol. 2013;31(15 Suppl):9013–9013. | ||
Chan M, Haydu L, Menzies AM, et al. Clinical characteristics and survival of BRAF-mutant (BRAF plus) metastatic melanoma patients (pts) treated with BRAF inhibitor (BRAFi) dabrafenib or vemurafenib beyond disease progression (PD). J Clin Oncol. 2013;31(15 Suppl):9062–9062. | ||
Shi H, Hugo W, Kong X, et al. Acquired resistance and clonal evolution in melanoma during BRAF inhibitor therapy. Cancer Discov. 2014;4(1):80–93. | ||
Wright CJ, McCormack PL. Trametinib: first global approval. Drugs. 2013;73(11):1245–1254. | ||
Flaherty KT, Robert C, Hersey P, et al. Improved survival with MEK inhibition in BRAF-mutated melanoma. N Engl J Med. 2012;367(2):107–114. | ||
Kim K, Kefford R, Pavlick AC, et al. Phase II study of the MEK1/MEK2 inhibitor trametinib in patients with metastatic BRAF-mutant cutaneous melanoma previously treated with or without a BRAF inhibitor. J Clin Oncol. 2013;31(4):482–489. | ||
Flaherty KT, Infante JR, Daud A, et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. N Engl J Med. 2012;367(18):1694–1703. | ||
Long GV, Stroyakovskiy D, Gogas H, et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N Engl J Med. 2014;371(20):1877–1888. | ||
Pratilas CA, Hanrahan AJ, Halilovic E, et al. Genetic predictors of MEK dependence in non-small cell lung cancer. Cancer Res. 2008;68(22):9375–9383. | ||
Joshi M, Rice SJ, Liu X, Miller B, Belani CP. Trametinib with or without vemurafenib in BRAF mutated non-small cell lung cancer. PLoS One. 2015;10(2):e0118210. | ||
Gautschi O, Pauli C, Strobel K, et al. A patient with BRAF V600E lung adenocarcinoma responding to vemurafenib. J Thorac Oncol. 2012;7(10): e23–e24. | ||
Schmida S, Sianoa M, Joerger M, Rodriguez R, Müller J, Früh M. Case report: response to dabrafenib after progression on vemurafenib in a patient with advanced BRAF V600E-mutant bronchial adenocarcinoma. Lung Cancer. 2015;87(1):85–87. | ||
Planchard D, Kim TM, Mazieres J, et al. Dabrafenib in patients with BRAFV600E-positive advanced non-small-cell lung cancer: a single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016;17(5):642–650. | ||
Planchard D, Besse B, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously treated BRAFV600E-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Lancet Oncol. 2016;17(7):984–993. | ||
Planchard D, Smit E, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: an open-label, phase 2 trial. Lancet Oncol. 2017;18(10):1307–1316. | ||
Pervere LM, Rakshit S, Schrock AB, Miller VA, Ali SM, Velcheti V. Durable response to combination of dabrafenib and trametinib in BRAF V600E-mutated non-small-cell lung cancer. Clin Lung Cancer. 2017;18(3):e211–e213. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.