")
Back to Journals » International Medical Case Reports Journal » Volume 9
Spontaneous uterine rupture in the 35th week of gestation after laparoscopic adenomyomectomy
Authors Nagao Y, Osato K, Kubo M, Kawamura T, Ikeda T, Yamawaki T
Received 13 August 2015
Accepted for publication 11 November 2015
Published 18 December 2015 Volume 2016:9 Pages 1—4
DOI https://doi.org/10.2147/IMCRJ.S94363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Yukari Nagao,1,2 Kazuhiro Osato,2,3 Michiko Kubo,2 Takuya Kawamura,2 Tomoaki Ikeda,3 Takaharu Yamawaki2
1Department of Obstetrics and Gynecology, Japanese Red Cross Nagoya Daiichi Hospital, Aichi, 2Department of Obstetrics and Gynecology, Japanese Red Cross Ise Hospital, Mie, 3Department of Obstetrics and Gynecology, School of Medicine, Mie University, Mie, Japan
Abstract: Uterine rupture rarely occurs during pregnancy, but it is a critical situation if so. It is already known that a history of uterine surgeries, such as cesarean section or myomectomy, is a risk factor for uterine rupture. Currently, the laparoscopic adenomyomectomy is a widely performed procedure, but associated risks have not been defined. We observed a case of spontaneous uterine rupture in a patient during the 35th week of gestation, after a laparoscopic adenomyomectomy. A 42-year-old, gravida 2, para 0 woman became pregnant after a laparoscopic adenomyomectomy and her pregnancy was conventional. At a scheduled date in the 35th week of gestation, after combined spinal epidural anesthesia and frequent uterine contractions, a weak pain suddenly ensued. After 13 minutes of uterine contractions, vaginal bleeding was evident. A cesarean section was performed, and the uterine rupture was found in the scar. After a laparoscopic adenomyomectomy, a pregnant uterus can easily rupture by rather weak and short uterine contractions, and is characterized by vaginal bleeding. When uterine bleeding is observed in pregnant women that have a history of adenomyomectomy, one should consider uterine rupture.
Keywords: uterine rupture, pregnancy, laparoscopic adenomyomectomy, uterine contraction, vaginal bleeding
Introduction
Uterine rupture rarely occurs during pregnancy, but it is a critical obstetric complication associated with maternal and fetal mortality and morbidity.1 It is known that the rate of uterine rupture increases in patients with a history of uterine surgery, such as cesarean section or myomectomy. Laparoscopic adenomyomectomies are widely performed to treat infertility or palliate symptoms of menstruation. It is however, not yet known what kinds of complications this procedure can cause in pregnant women. Here we report a case of spontaneous uterine rupture in the 35th week of gestation after a laparoscopic adenomyomectomy.
Case report
A 42-year-old, gravida 2, para 0 woman was referred to our hospital at the 11th week of gestation. Before she got pregnant, she had had sterility treatment, but it hadn’t been successful. She subsequently received a laparoscopic adenomyomectomy in another hospital 14 months before referral. The findings in the operation were as follows: The lesion of adenomyosis existed at the posterior wall of the uterus and the lesion and rectum adhered to each other firmly. A vertical incision was made in the middle of the posterior wall of the uterus, and the adenomyosis lesion was enucleated as much as possible (50 g in total). Finally, the uterine wall was repaired with a three-layer suture. One year after the operation, she conceived spontaneously.
The patient’s singleton pregnancy was uneventful and she was admitted at the 30th week of gestation for the purpose of bed rest. This was done because past reports suggest that uterine rupture after laparoscopic adenomyomectomy typically occurs around the 30th week of gestation. The patient’s hospital stay was incident-free, and a cesarean section was due to be performed at the 34th week of gestation to achieve optimal trade-off between fetal lung maturation and fetal prematurity. However, the patient’s cesarean section was moved to the 35th week of gestation due to her strong request. On the scheduled date, no notable events occurred until the patient went into the operating room. The patient had undergone combined spinal epidural anesthesia, and was experiencing frequent uterine contractions when a weak pain suddenly occurred. After 13 minutes of uterine contractions, vaginal bleeding was observed while sterilizing the vagina. Cesarean section was performed immediately and a female neonate, weighing 2,283 g, was delivered 31 minutes after uterine contractions had begun. The neonate’s Apgar scores were 7 and 8 at 1 and 5 minutes, respectively. Umbilical arterial gas analysis indicated no acidosis (pH 7.267, base excess -3.4).
The rectum and omentum adhered to the posterior uterine wall, where there was a scar from the previous adenomyomectomy. Bleeding was found in the adhered tissue and therefore we peeled off those adhesions. A 1.5 cm hole was found in the uterus (Figure 1). One area did not have a muscle layer and was covered with only uterine serosa adjacent to the ruptured area. This was repaired with a three-layer suture and total sutured length was 7–8 cm. The patient’s postoperative process proceeded without complications and the patient was discharged at a postoperative date of 12 days. Informed consent was obtained from the patient orally, in order to retain the anonymity of the patient. No ethics approval was required for this study.
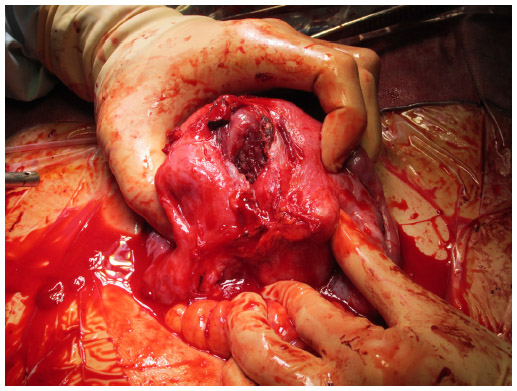 | Figure 1 Uterine rupture with a 1.5 cm hole. |
Discussion
Two important clinical issues were identified: 1) after a laparoscopic adenomyomectomy, a pregnant uterus might rupture easily by rather weak and short uterine contractions; 2) uterine contractions followed by uterine bleeding might be useful for the diagnosis of uterine rupture.
First, after laparoscopic adenomyomectomy, a pregnant uterus might rupture easily by rather weak and short uterine contractions. A recent review by Morimatsu et al showed that the rate of uterine rupture after adenomyomectomy during pregnancy is 6.0%2 in contrast to the entire rate of uterine rupture during pregnancy, which is 0.035%.3 This is much higher than the rate of complications after cesarean section (0.27%–0.7%)4,5 or myomectomy (2.45%).6,7 We determined some reasons why uterine rupture frequently occurs in pregnant women with prior laparoscopic adenomyomectomies. The boundary between the normal uterine muscle layer and the lesion is unclear. A lesion of adenomyosis tends to remain around the edges of excisions and the area to be sutured, which might lead to weak connections between sutured edges. If a lesion of adenomyosis is enucleated widely to eliminate the lesion, the uterus will be small and irregular in shape, which leads to a diminished capacity to expand.8 With a laparoscopic adenomyomectomy, it is particularly difficult to delineate the border of the lesion because of a lacking sense of touch and deep sensation.9
Only five publications have presented cases of uterine rupture during pregnancy in patients with prior histories of adenomyomectomy (laparoscopic 4, laparotomic 1) (Table 1).2,8,10,11 According to 96 reported cases (Table 2),2,8–16 the rate of uterine rupture during pregnancy was 6.25%; this is similar to the review reported by Morimatsu et al.2 It would appear that the frequency of uterine rupture after laparoscopic adenomyomectomy is higher than that of laparotomic adenomyomectomy (Tables 1 and 2), but there is no cohort study to compare these so far.
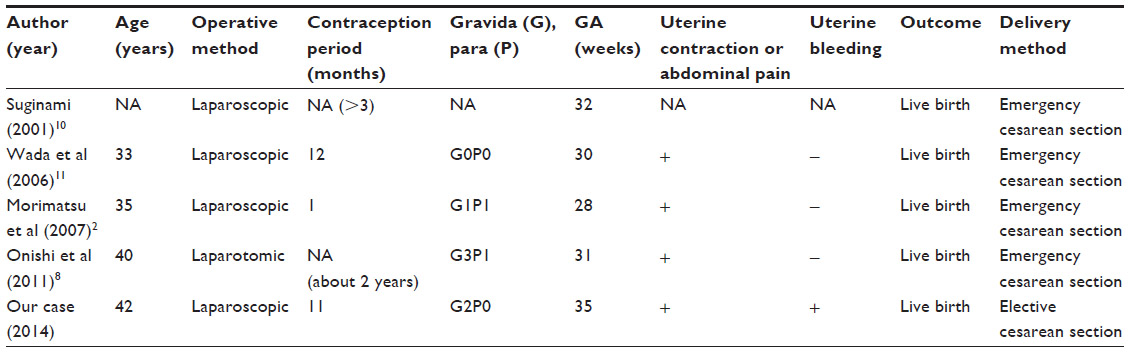 | Table 1 Characteristics in five cases of uterine rupture during pregnancy after adenomyomectomy |
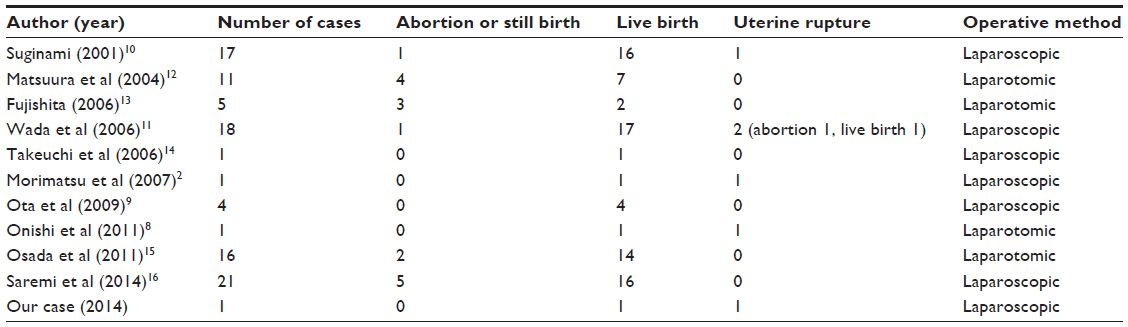 | Table 2 Pregnancy outcome in patients with prior history of adenomyomectomy |
Uterine rupture or dehiscence during pregnancy tends to occur more frequently after laparoscopic myomectomy than after laparotomic myomectomy. Specifically, the frequency of uterine dehiscence is 1.85–4.94% in laparoscopic6,7 and 0% in laparotomic (this finding is extremely limited because it depends on only 69 cases from two reports).6,7 We guess that uterine rupture or dehiscence is similarly more common in laparoscopic than in laparotomic adenomyomectomy cases.
Second, uterine contractions followed by uterine bleeding might be useful for the diagnosis of uterine rupture. Uterine rupture does not have any typical symptoms and is often asymptomatic.17,18 Classical symptoms and signs are abdominal pain, external bleeding, vital signs indicating shock, disappearance of labor pain, and signs of fetal distress etc. In this case, the patient experienced both abdominal pain and external bleeding.
Conclusion
A pregnant uterus after laparoscopic adenomyomectomy might rupture easily by rather weak and short uterine contractions. Furthermore, uterine contractions followed by uterine bleeding might be useful for the diagnosis of uterine rupture. When uterine contractions are followed by uterine bleeding in pregnant women that have had a prior adenomyomectomy, this must be considered a potential sign of uterine rupture. If physicians are planning to perform surgery for treating sterility and infertility, they should carefully choose the modality of surgery and get more detailed informed consent from patients with adenomyosis. Further reports should be accumulated to develop more reliable and safe operative techniques, and to establish guidelines for pregnancy after adenomyomectomy in women of reproductive age.
Disclosure
The authors report no conflicts of interest in this work.
References
Yazawa H, Endo S, Hayashi S, Suzuki S, Ito A, Fujimori K. Spontaneous uterine rupture in the 33rd week of IVF pregnancy after laparoscopically assisted enucleation of uterine adenomatoid tumor. J Obstet Gynaecol Res. 2011;37(5):452–457. | |
Morimatsu Y, Matsubara S, Okuchi A, et al. Shikyusenkinsho kakushutsujutsu go no ninshin – Shikyu haretsu no literature review to sanka kanri ni tsuite – [Pregnancy after adenomyomectomy – literature review of uterine rupture and obstetrical management –]. Sanka to fujinka [Japanese Journal of Obstetrics and Gynaecology] 2007;74(9):1047–1053. Japanese. | |
Ofir K, Sheiner E, Levy A, Katz M, Mazor M. Uterine rupture: risk factors and pregnancy outcome. Am J Obstet Gynecol. 2003;189(4):1042–1046. | |
Guise JM, McDonagh MS, Osterweil P, Nygren P, Chan BK, Helfand M. Systematic review of the incidence and consequences of uterine rupture in women with previous caesarean section. BMJ. 2004;329(7456):19–25. | |
Landon MB, Hauth JC, Leveno KJ, et al; for National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med. 2004;351(25):2581–2589. | |
Kim MS, Uhm YK, Kim JY, Jee BC, Kim YB. Obstetric outcomes after uterine myomectomy: Laparoscopic versus laparotomic approach. Obstet Gynecol Sci. 2013;56(6):375–381. | |
Tian YC, Long TF, Dai YM. Pregnancy outcomes following different surgical approaches of myomectomy. J Obstet Gynaecol Res. 2015; 41(3):350–357. | |
Onishi K, Hiromura K, Miyazaki K, et al. Shikyusenkinsho setsujojutsu go ninshin ni okeru zenchi kannyu taiban, shikyu haretsu no ichi rei [A case of uterine rupture in a patient with placenta previa and accreta following adenomyomectomy]. Nihon shusanki shinseiji igakkai zasshi. [J Jpn Soc Perin Neon Med.] 2011;47(4):947–950. Japanese. | |
Ota Y, Hada T, Deura I, et al. Fukukukyo ka shikyusenkinsho setsujojutsu – byoso no keijo ni chumoku shita jutsushiki no tsukaiwake [Laparoscopic adenomyomectomy – the use of a method focusing attention on the shape of the lesion]. Sanka to fujinka [Japanese Journal of Obstetrics and Gynaecology] 2009;76(12):1547–1553. Japanese. | |
Suginami H. Shikyusenkinsho shujutsu deno ninyono onzon [Fertility preservation following an adenomyosis operation]. Sanka to fujinka [Japanese Journal of Obstetrics and Gynaecology] 2001; 68(8):1017–1022. Japanese. | |
Wada S, Kudo M, Minakami H. Spontaneous uterine rupture of a twin pregnancy after a laparoscopic adenomyomectomy: a case report. J Minim Invasive Gynecol. 2006;13(2):166–168. | |
Matsuura K, Honda R, Okamura H. Kaifuku ni yoru shikyusenkinsho kakushutsujutsu – kakyuteki byoso shukushojutsu kara mita chiryo seiseki – [Laparoscopic adenomyomectomy – the result of treatment following an operation that limits the size/ number of lesions]. Nihon Seishokugeka gakkai zasshi [Japanese Reproductive Surgery Society Magazine] 2004;17(1):9–13. Japanese. | |
Fujishita A. Shikyusenkinsho ni taisuru sikyu onzon shujutsu [Conservative surgery for adenomyosis]. Sanfujinka chiryo [Treatment of Obstetrics and Gynaecology] 2006;92(3):294–298. Japanese. | |
Takeuchi H, Kitade M, Kikuchi I, et al. Laparoscopic adenomyomectomy and hysteroplasty: a novel method. J Minim Invasive Gynecol. 2006;13(2):150–154. | |
Osada H, Silber S, Kakinuma T, Nagaishi M, Kato K, Kato O. Surgical procedure to conserve the uterus for future pregnancy in patients suffering from massive adenomyosis. Reprod Biomed Online. 2011; 22(1):94–99. | |
Saremi A, Bahrami H, Salehian P, Hakak N, Pooladi A. Treatment of adenomyomectomy in women with severe uterine adenomyosis using a novel technique. Reprod Biomed Online. 2014;28(6):753–760. | |
Guiliano M, Closset E, Therby D, LeGoueff F, Deruelle P, Subtil D. Signs, symptoms and complications of complete and partial uterine ruptures during pregnancy and delivery. Eur J Obstet Gynecol Reprod Biol. 2014;179:130–134. | |
Hashiguchi M. Shikyu haretsu [Uterine rupture]. Sanka to fujinka [Japanese Journal of Obstetrics and Gynaecology] 2012;79(5):573–581. Japanese. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.