")
Back to Journals » Clinical Ophthalmology » Volume 10
Spectral domain optical coherence tomography imaging of subretinal bands associated with chronic retinal detachments
Authors Kothari N, Kuriyan A, Flynn Jr. H
Received 3 November 2015
Accepted for publication 9 December 2015
Published 30 March 2016 Volume 2016:10 Pages 467—470
DOI https://doi.org/10.2147/OPTH.S99754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nikisha Kothari, Ajay E Kuriyan, Harry W Flynn Jr
Department of Ophthalmology, Bascom Palmer Eye Institute, Miller School of Medicine, University of Miami, Miami, FL, USA
Abstract: We report three patients with subretinal bands associated with retinal detachment in chronic retinal detachments who underwent successful retinal reattachment. Subretinal bands before and after surgery can be identified on clinical examination and spectral domain optical coherence tomography. Removal of subretinal bands is not mandatory to achieve retinal reattachment.
Keywords: subretinal bands, retinal detachment, optical coherence tomography
Introduction
Proliferative vitreoretinopathy (PVR) occurs in 5%–10% of patients and is the most common cause of failure of retinal detachment (RD) surgery. The Silicone Study further classified PVR into focal or diffuse posterior PVR, subretinal PVR, and anterior PVR.1 Subretinal fibrosis is reported to occur in up to 15% of rhegmatogenous RDs.2–4 Retinal pigment epithelial cells may migrate on the detached outer retinal surface, proliferate, and differentiate into mesenchymal cells.5,6
The advent of spectral domain optical coherence tomography (SD-OCT) enables imaging of hyperreflective subretinal fibrotic bands in chronic RDs. To our knowledge, this is the first report of using SD-OCT to document subretinal bands associated with chronic RD. We did not have approval from our institutional review board as it is not required at our institution (University of Miami- Miller School of Medicine) for up to 3 patients. All procedures were performed in accordance with the Declaration of Helsinki.
Case 1
A 20-year-old female with high myopia presented with diminished peripheral vision in her right eye. Her best-corrected visual acuity (BCVA) was 20/25 oculus dexter (OD) and 20/20 oculus sinister (OS). Dilated fundus examination revealed a nasal shallow RD, lattice degeneration with multiple breaks superonasally, and a subretinal band inferiorly (Figure 1A). SD-OCT demonstrated a band of subretinal fibrosis along with subretinal fluid (Figure 1B). After lengthy discussion of management options, the patient elected for observation. However, 1 month later her BCVA diminished from 20/25 to 20/40 OD, which corresponded to progression of her detachment into the macula. The patient underwent a scleral buckling procedure and external drainage of subretinal fluid. Her BCVA improved to 20/25 and her retina remained attached with a persistent subretinal fibrotic band (Figure 1C) at her 3-year follow-up. SD-OCT confirmed the presence of persistent subretinal bands and resolution of subretinal fluid (Figure 1D).
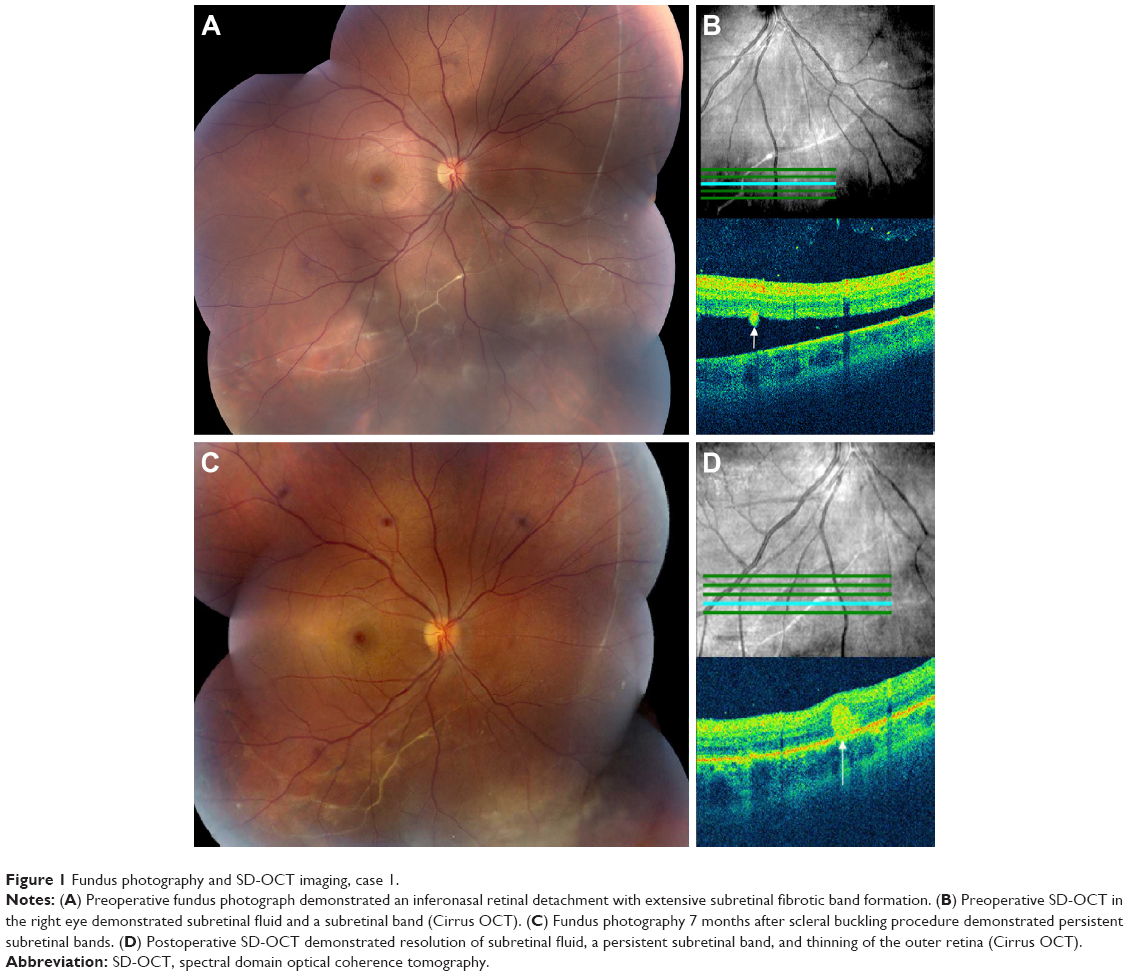 | Figure 1 Fundus photography and SD-OCT imaging, case 1. |
Case 2
A 24-year-old male presented with no light perception vision in the right eye due to previous trauma and an RD in his left eye related to toxoplasmosis. He initially underwent a scleral buckling procedure and received treatment for toxoplasmosis. The patient underwent three subsequent operations for recurrent RD including: 1) revision of the scleral buckle, 2) pars plana vitrectomy, sulfur hexafluoride (SF6) gas injection, and repeat revision of the scleral buckle 1 month later, and 3) a pars plana vitrectomy, fluid–air exchange, membrane peel, endolaser, and perfluoropropane (C3F8) gas injection 9 years later. His BCVA has remained 20/50 OS, and the posterior segment examination revealed an encircling scleral buckle, peripheral laser scars, subretinal bands, and no recurrence of active toxoplasmosis was observed during his follow-up visit 37 years later (Figure 2A). SD-OCT demonstrated a hyperreflective subretinal band corresponding to the subretinal fibrosis (Figure 2B).
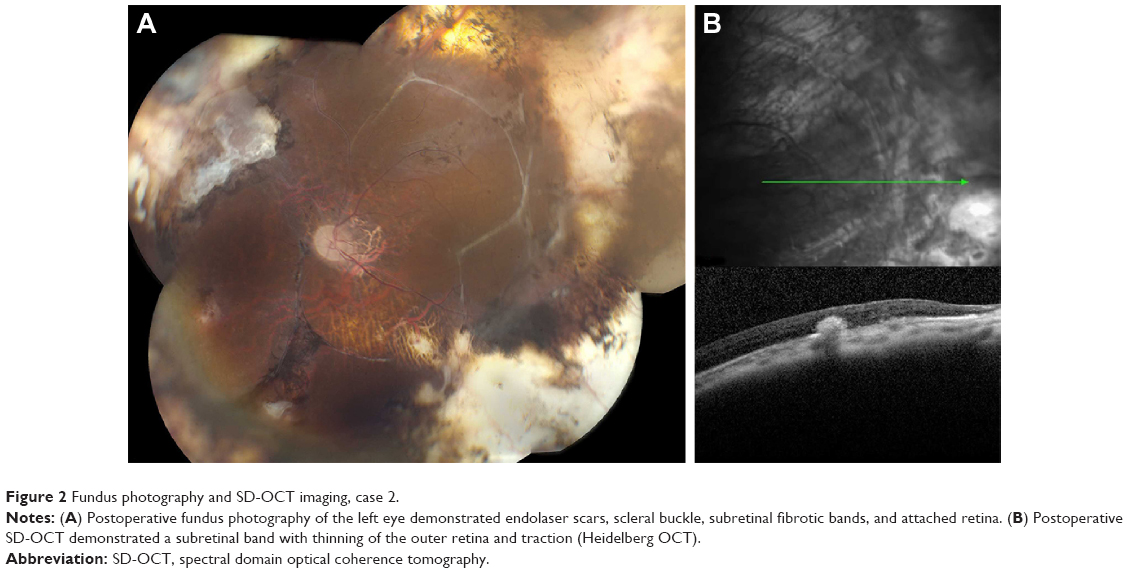 | Figure 2 Fundus photography and SD-OCT imaging, case 2. |
Case 3
A 43-year-old female with history of high myopia and LASIK (laser-assisted in situ keratomileusis) in both eyes presented after she noticed a visual field defect in her right eye. Her BCVA was 20/20 in both eyes. Dilated fundus examination revealed an RD with a subretinal band temporally associated with lattice and multiple holes in the right eye (Figure 3A). She underwent a scleral buckling procedure with successful reattachment of her retina (Figure 3C). Her BCVA was 20/20 OU (oculus uterque), and her examination by SD-OCT at the 2-year follow-up showed a stable subretinal band temporally (Figure 3D).
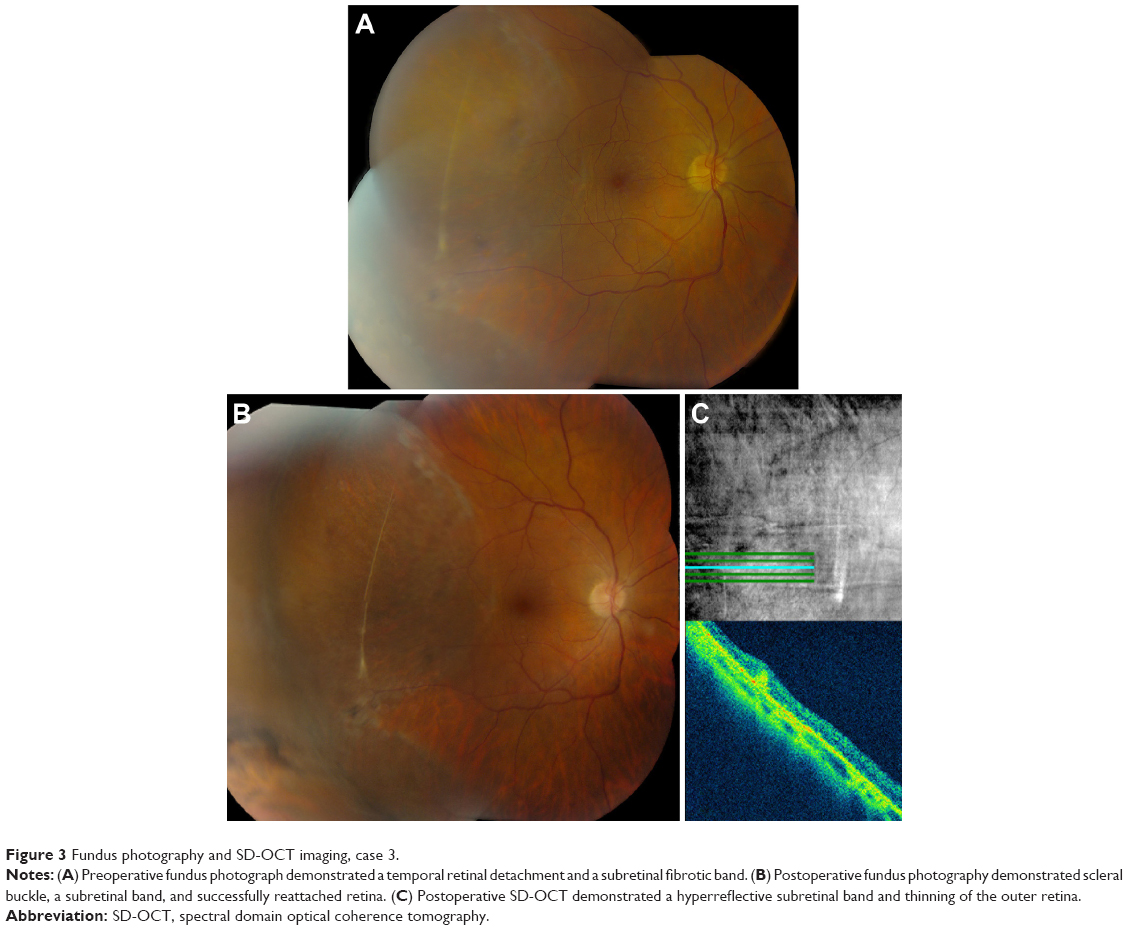 | Figure 3 Fundus photography and SD-OCT imaging, case 3. |
Discussion
RD with PVR may be associated with development of fibrotic bands possibly causing failure of RD repair. Based on the current classification scheme, subretinal bands are considered as part of more advanced PVR.7 However, successful reattachment after a single surgery for isolated subretinal PVR ranges from 89% to 95%.2,3,8,9 If removal of subretinal bands is required to achieve reattachment, the success rate decreases to 65% in one study.3 In addition, the presence of concomitant preretinal PVR alters management and reduces success rates.8
The current series demonstrates that successful retinal reattachment without removing subretinal bands can be accomplished by a scleral buckling procedure, with or without vitrectomy. However, subretinal bands causing a napkin-ring configuration are more likely to require pars plana vitrectomy, retinotomy, and excision of subretinal membranes.
In conclusion, we present SD-OCT findings of subretinal fibrotic bands in three patients who underwent successful anatomic reattachment without removal of the subretinal bands. In an era of multimodal imaging, OCT studies are useful in documenting the extent and location of subretinal bands and may guide preoperative surgical assessment.
Acknowledgments
This study was supported by the NIH Center Core Grant P30EY014801, an unrestricted grant to the University of Miami from National Eye Institute, a grant from the Research to Prevent Blindness, New York, New York, USA, and also the Department of Defense grant (DOD-Grant# W81XWH-13-1-0048), an unrestricted grant to the University of Miami.
Disclosure
The authors report no conflicts of interest in this work.
References
Lean JS, Stern WH, Irvine AR, Azen SP. Classification of proliferative vitreoretinopathy used in the silicone study. The Silicone Study Group. Ophthalmology. 1989;96(6):765–771. | ||
Wallyn RH, Hilton GF. Subretinal fibrosis in retinal detachment. Arch Ophthalmol. 1979;97(11):2128–2129. | ||
Lewis H, Aaberg TM, Abrams GW, McDonald HR, Williams GA, Mieler WF. Subretinal membranes in proliferative vitreoretinopathy. Ophthalmology. 1989;96(9):1403–1414. | ||
Miura M, Ideta H. Factors related to subretinal proliferation in patients with primary rhegmatogenous retinal detachment. Retina. 2000;20(5):465–468. | ||
Tabandeh H, Callejo SA, Rosa RH Jr, Flynn HW Jr. Subretinal “napkin-ring” membrane in proliferative vitreoretinopathy. Arch Ophthalmol. 2000;118(9):1287–1289. | ||
Machemer R, Laqua H. Pigment epithelium proliferation in retinal detachment (massive periretinal proliferation). Am J Ophthalmol. 1975;80(1):1–23. | ||
Machemer R, Aaberg TM, Freeman HM, Irvine AR, Lean JS, Michels RM. An updated classification of retinal detachment with proliferative vitreoretinopathy. Am J Ophthalmol. 1991;112(2):159–165. | ||
Ghasemi Falavarjani K, Alemzadeh SA, Modarres M, et al. Scleral buckling surgery for rhegmatogenous retinal detachment with subretinal proliferation. Eye (Lond). 2015;29(4):509–514. | ||
Yao Y, Jiang L, Wang ZJ, Zhang MN. Scleral buckling procedures for longstanding or chronic rhegmatogenous retinal detachment with subretinal proliferation. Ophthalmology. 2006;113(5):821–825. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.