")
Back to Journals » Patient Preference and Adherence » Volume 13
South Asians’ experience of managing hypertension: a grounded theory study
Authors King-Shier KM , Dhaliwal KK, Puri R, LeBlanc P , Johal J
Received 28 November 2018
Accepted for publication 18 January 2019
Published 20 February 2019 Volume 2019:13 Pages 321—329
DOI https://doi.org/10.2147/PPA.S196224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Kathryn M King-Shier,1,2 Kirnvir K Dhaliwal,1 Roshani Puri,1 Pamela LeBlanc,1 Jasmine Johal3
1Faculty of Nursing, University of Calgary, Calgary, AB, Canada; 2Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; 3Werklund School of Education, University of Calgary, Calgary, AB, Canada
Objective: We examined the process that South Asians undergo when managing their hypertension (HTN).
Method: Using grounded theory methods, 27 community-dwelling English-, Punjabi-, or Hindi-speaking South Asian participants (12 men and 15 women), who self-identified as having HTN were interviewed. Transcripts were analyzed using constant comparison.
Results: The core category was “fitting it in”. First, the participants assessed their diagnosis and treatment primarily in the context of their current family/social environment. Participants who paid attention to their diagnosis either fully or partly embraced activities and attitudes associated with successful management of hypertension. However, those who did not attend to their diagnosis, identified other familial/social factors, stress of immigration, and not having symptoms of their disease as barriers. The longer the time since diagnosis of HTN, the more participants came to appropriately manage their HTN.
Conclusion: Healthcare providers may use this information to enhance their cultural understanding of how and why South Asians manage their HTN.
Keywords: South Asian, hypertension, grounded theory, health management
Introduction
Hypertension (HTN) is a chronic illness that is responsible for the greatest amount of disability and death in the world.1–3 Though the prevalence of HTN is rising in developed countries, such as Canada,4 it is rising at higher rates in many developing regions, including South Asia.3 The reasons for this are not clear. Once diagnosed, HTN generally requires lifelong management. Hypertension Canada5 and the European Society of Cardiology6 guidelines (among others worldwide) identify that patients are diagnosed with HTN when their SBP and/or DBP exceeds 140 mmHG and 90 mmHG, respectively. Depending on the severity of HTN at diagnosis, the first-line treatment is often lifestyle modification.5,6 Indeed, eating a diet high in fat and low in protein, having a high sodium intake, engaging in inadequate physical activity, being obese, having a high alcohol consumption, smoking, and being stressed are known to contribute to the development of HTN.7–12 Medications are introduced to the treatment regime when lifestyle modifications do not sufficiently control the HTN.
South Asians (people or whose ancestors originate from India, Pakistan, Bangladesh, Sri Lanka, or Nepal) are one of Canada’s fastest growing ethnic groups.13 South Asians have a nearly three times greater chance of being hypertensive and at a younger age than European whites.14,15 A South Asian community-screening initiative for HTN in Calgary, Alberta, Canada (location in which this study was conducted), revealed 55% of those screened were hypertensive and of those, the “control rates were 50% lower than those reported in the general population”.16
Our work has revealed that South Asians may be less adherent to lifestyle recommendations focused on reducing cardiovascular disease (including HTN) risk.17–19 Studies have also revealed that South Asians are less adherent to their cardiac medications, in general, relative to European whites.20,21 Several research groups have reported that a significant proportion of hypertensive South Asian patients (33%–67.6%) remain non-adherent to their medications.22–29
Researchers who conducted two separate systematic reviews regarding cardiac medication adherence in South Asians have concluded that reasons for non-adherence are unclear and evidence-based interventions need to be developed to improve adherence in this group.30,31
Aim
Given the burden of HTN in South Asians and their vast migration outside of their home countries, and a dearth of understanding regarding their management choices, we aimed to develop an in-depth explanation of how and why South Asians manage (or not) their HTN.
Methods
Design
We took an inductive qualitative approach, grounded theory,32 to develop an in-depth explanation of the process that South Asians undergo when managing their HTN. Unlike other qualitative approaches, such as phenomenology or ethnography where the subjective reality or the cultural understanding of a phenomenon are explored,33,34 grounded theory is best used to examine processes of human behavior “from many different angles – thus developing comprehensive explanations”.32
Sampling and participant recruitment
Community-dwelling South Asian men and women; >18 years of age; who self-identified having a diagnosis of HTN (ie, a physician had told them that they were hypertensive); and who spoke English, Punjabi, or Hindi (the most common South Asian languages spoken in Canada) were eligible to participate in the study. A recruitment flyer was posted or distributed at a primary care network, local Gurdwara (Sikh place of worship), and community center in a community where the majority of the city’s South Asians reside. Potential participants either called into a research office or were screened and recruited in person. Thirty-one people were screened for participation in this study and 27 met the inclusion/exclusion criteria. In keeping with our standard practices, all study materials were rigorously translated into the languages of interest.35
Sampling in grounded theory studies is purposive.32 Initial participants were those who volunteered. As the study proceeded, we engaged in theoretical sampling. In other words, participants were screened based on: 1) additional criteria to ensure adequate reflection of the group being studied (eg, sex, age, language, and time since immigration); and 2) emergence of the theory and core category. Sampling continued until theoretical saturation occurred (eg, no new data were revealed).36
Ethical considerations
This study protocol received approval from the Conjoint Health Research Ethics Board of the University of Calgary and was undertaken in accordance with the Helsinki Declaration of 1964. All participants signed an informed consent in the language of their choice (which included information about the researcher, purpose of the study, and expectations of the participant) before data collection began, and were encouraged to ask questions about the study throughout the process.
Data collection
Data were collected between February 2017 and May 2018. Demographic data were collected to enable characterization of the study sample and assist with the sampling process. Each participant engaged in one audio-recorded semi-structured interview undertaken either over the telephone or in their home, as they preferred.37 As is typical in our experience, family members were usually present during the interviews and were occasionally engaged in the process. The general questions asked at the beginning were similar (eg, I’m interested in learning about what you thought and did when you first learned that you had high BP? Tell me about making changes to your lifestyle for your high BP). As the concurrent data analysis unfolded, questions evolved to be more specific (eg, sometimes people struggle when taking medicines. Has that been the case for you?). Interviews generally lasted 30–45 minutes. Data were collected until saturation (eg, no new information was being gleaned) occurred.
Research assistants of South Asian descent, who spoke either Punjabi or Hindi (KD, RP, JJ), assisted with data collection. All were highly experienced in undertaking interviews, and were asked to consider both “translational elements” (accurate literal translation) as well as “conceptual equivalence” (the culture-bound meaning) during the interview sessions.35,38–40 When translation was required, some interviews (n=12) were led by a more senior researcher (anonymized) with research assistant’s translation, while other interviews (n=7) were undertaken independently by the research assistants who spoke the same language as the participant.
All English-language elements of interviews were transcribed verbatim.
Interviews undertaken in Punjabi/Hindi were translated and transcribed into English by the research assistant who undertook the interview. To ensure accuracy of the translated data, audio-recordings of non-English interviews were later audited by a different research assistant to ensure accurate translation and cultural understanding. There were very few discrepancies (which were considered minor) between both the original research assistants and auditors.
Data analyses
Demographic data were entered into IBM SPSS Statistics 23 and descriptive analyses (eg, proportions and means) were performed. Analysis of these data began immediately after the first interview using constant comparative methods.32,41 This involved literally making continual comparisons between the data, as well as the codes and categories that were generated. This process guided theoretical sampling and evolving questions asked of participants.32
Straussian grounded theory analysis was followed.32,36 Open coding involved line-by-line reading and analysis of the transcribed interviews. Elements of the text that represented common concepts were identified and then given a label or code. Axial and selective coding were then performed. These involved condensing of open codes to form a more broad category. Each category was given a label or name and mutually exclusive rules for inclusion were generated. Linkages or relationships between categories were constantly examined to develop a “story line”, which helped to identify a core category around which the theory was developed. Though an eight-level conditional matrix to integrate the coding is advocated, we focused on the more microlevel elements in the interviews and analysis as follows: “action pertaining to the phenomenon”, “interaction”, and “group, individual, and collective” elements. Regular team meetings were held throughout the process to discuss the ongoing analysis and reflect on memos (which included notes regarding potential biases). Any discordance in the coding was resolved through discussion.
Rigor
Rigor or trustworthiness42 of the study process and findings were enhanced through a number of activities. The credibility (gaining the real essence of the phenomenon under study) rests greatly on the researchers’ ability to engage participants such that they are willing and able to genuinely articulate their experience. The study participants were interested in sharing their thoughts and experiences of having HTN and taking medications. Indeed, enabling participants to engage with research assistants of the same ethnicity and their language of choice35,38–40 also contributed to the rigor of this work. Credibility of the study process and findings was enhanced by engaging in theoretical sampling and ensuring data accuracy. Theoretical sampling rendered a group of participants who were representatives of South Asian people who had HTN and who could describe the experience and its nuances. Data accuracy was assured by rigorously scrutinizing the transcriptions of interviews.35,38–40 We were able to develop rich descriptions of the management of HTN in this group, thus enhancing transferability (ability of others to see utility of the results in other contexts). This was achieved through careful sampling (eg, ensuring the sample was representative and the participants were able and enabled to describe their thoughts and feelings), rigorous data analysis procedures (eg, team approach and consensus building), and achieving data saturation. Documentation (or creation of audit trails) of the details of these processes and including consensus building as part of the data analytic process enhanced dependability and confirmability of the findings and process.
Results
Participants ranging in age from 24 to 76 years participated in this study. More than half (63%) of the interviews were conducted in Punjabi or Hindi. The majority of participants were of the Sikh religion (74%) and had immigrated from India (85%). More than one-third (37%) of the participants had immigrated to Canada <5 years ago. The time from HTN diagnosis ranged from 3 months to >30 years. Most participants were married (78%) and residing with their children (56%). The majority (70%) had a high school (equivalent) or greater education and 78% were unemployed or retired (Table 1).
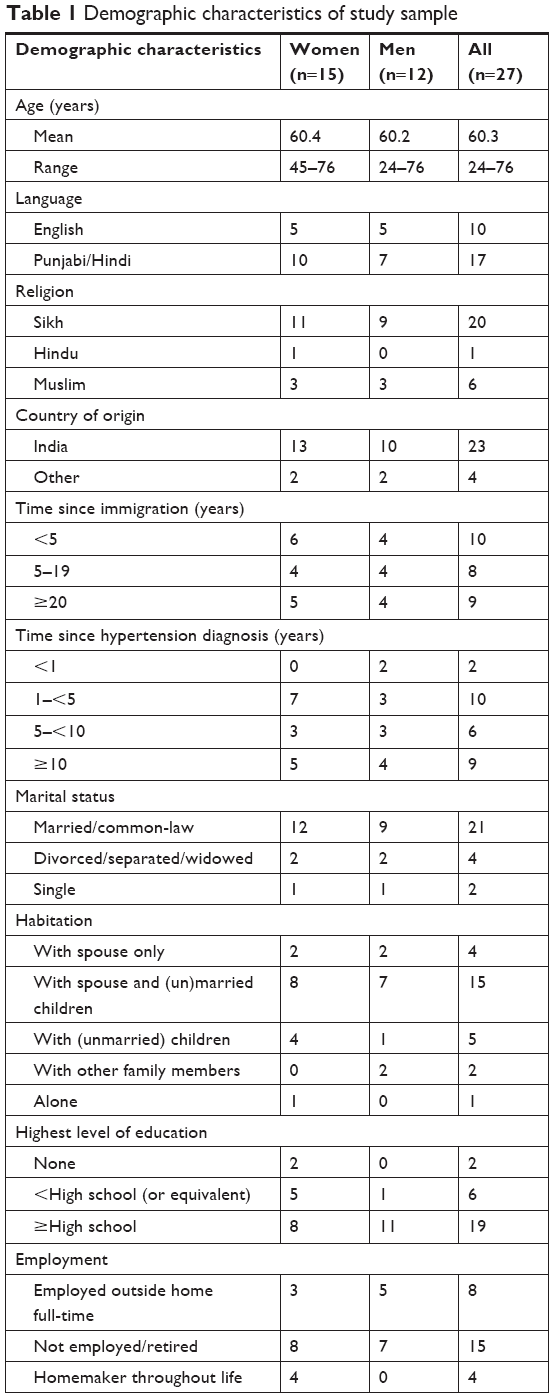 | Table 1 Demographic characteristics of study sample |
Participants initially assessed the HTN diagnosis in a variety of contexts. Thereafter, two key elements characterized the process in which the participants engaged when managing their HTN. The first element was the level of initial acceptance. Some participants fully or partly accepted the HTN diagnosis and the recommended treatment, while others were resistant to the diagnosis and recommended treatment and were thus not accepting. The second element was the influence of time. Those participants who were less than fully accepting of the HTN diagnosis and recommended treatment became more accepting over time, and often reflected and wished they had behaved differently. Overall, the participants found a path to fitting HTN into their lives (core category; Figure 1).
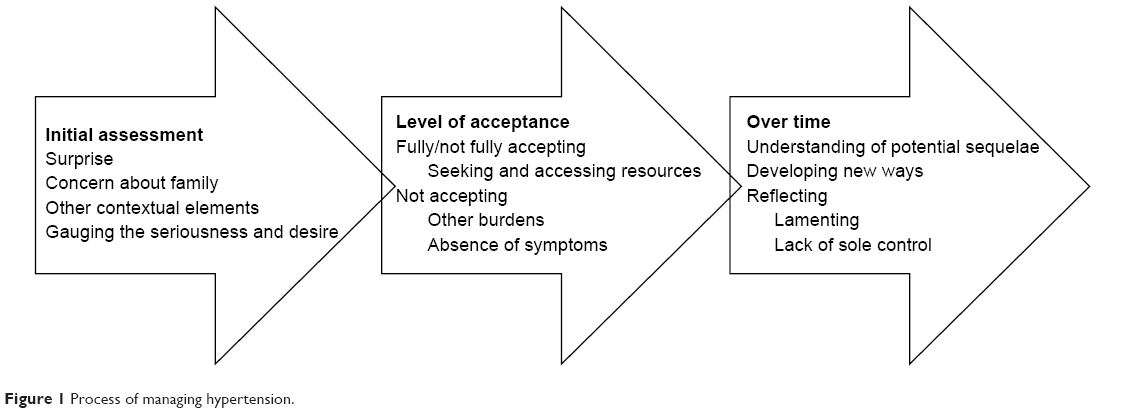 | Figure 1 Process of managing hypertension. |
Initial assessment
There were varying contexts in which participants’ HTN diagnosis was made, including diagnosis at a sudden hospital admission or medical event, a series of doctor visits due to ongoing symptoms, or a routine check-up. Regardless, it seemed to come as a surprise.
I had no idea it could happen to me. I exercised. Walking a lot, and not eating extra food. I found out when I was hospitalized … It should have not happened. (man)
There were also immediate concerns about how the family was managing the diagnosis and the need to take medication.
I feel sad. If I don’t take my medication, it causes tension in the family. They say “You don’t take your medication … do you want to die? Take your medication.” I don’t want them worrying about me. (woman)
Finally, there was acknowledgment by many of the additional stress that this diagnosis could add to the family.
Well at that time (of the diagnosis), we had other family problems. We were new in this country and we had to work very hard and we had other problems like we had to support our family members back home and so all that was dominating my thought process and I got this. (man)
Some participants cited other recent contextual elements that may have had an influence on developing HTN.
The doctor has said it may be just because of the change in weather, the travel, coming here from India 6 weeks ago. We will wait and see if I still have it 3 months from now. (man)
Participants also realized the seriousness of their condition, as well as their desire or capacity to focus on managing it. Some listened to others’ advice.
My brother, who is a doctor, said it has to be controlled and if you can’t control, it will affect the organs. I listened to him. (man)
However, some were more fatalistic.
Why should I worry? When God asks me to come, he will. He has that control … But, who wants to leave the world? (woman)
The outcome of these (conscious or unconscious) deliberations determined the extent to which participants would accept or dismiss the diagnosis and recommended treatment.
Level of acceptance
(Not) fully accepting
When the HTN diagnosis was made at the time of a medical event, having trust in the physician led to acceptance.
… we must listen to our medical doctor. His education and scientific background are the only guidelines for decisions about our health. (woman)
Also, if the participant had observed relatives’ experiences with HTN or thought it was God’s will, they identified that the HTN required attention.
Actually, my mother had high blood pressure … and had a lot of problems, her heart enlarged. And later, after kidney problems, she died very early. I didn’t know the exact reason but I knew I shouldn’t eat a lot of salt. I learned from this. (woman)
If God has put me on these medications, I just take them. (woman)
Some of those who did not fully accept their diagnosis and recommendations went through a process of exploring alternatives to taking medications (eg, homeopathy and enhanced lifestyle changes) as the solution to their HTN.
I didn’t want to take medication. I tried homeopathy for a bit. Then once it (HTN) increased so much that I had to get admitted (to hospital) once or twice. I did a bit of naturopathy as well … curry leaves … holy basil … with black pepper. (It) helped only for a bit. (woman)
Those who were accepting or not fully accepting also went through a process of finding resources and support. Having the desire and ability to access resources and support were important factors in their success.
Through an interpreter: They want to take care of their health, and she said that she is very engaged with their doctor and the dietitians … She follows their advice very strictly too … even at the Gurudwara, she won’t eat the food that is given there because her dietitian said to make it a specific way. (woman)
I’ll try and reduce the blood pressure by taking whatever actions I have to take, rather than take medications. I’m already taking medication for diabetes and for high cholesterol. I don’t think I need any more medication. (man)
Furthermore, accessibility in terms of location and language were also key to using resources.
We’re very lucky that it’s (health programs) very close to our, my residence. (man)
Through an interpreter: He appreciates that their doctor speaks Punjabi. It makes it much easier for him to understand what he needs to and why. The doctor also understands our culture. (man)
Not accepting
Some participants were too occupied with other matters to allocate the time to accept their HTN diagnosis and treatment (eg, burden of housework, recent immigration, and lack of symptoms).
The doctor told me to exercise. Neither have I done it nor can I do it. I sweep and mop the house, make food 3 or 4 times each day, make sabji (food), do dishes, washing clothes, just this … it is all I can do. (woman)
My primary (focus) was to get established, to get a foot firm in this country, make an income. We have different types of problems like getting established. (man)
Other participants’ perceptions and beliefs made them more likely to dismiss their HTN diagnosis, and less likely to engage in the recommended health behaviors.
Actually, I didn’t take any action because I thought I had no problem with my health. I thought I was healthy enough … I thought I was fit. I wasn’t in any pain or anything so I thought why should I take medication? (man)
Over time
Time since diagnosis was a key factor in how participants managed their HTN. The longer the time from diagnosis, the more likely it was that participants appropriately managed their health. Some participants came to understand more about potential sequelae of HTN, and realized the need to attend to it.
Now, I get scared that high blood pressure might affect my eyes or paralyze (me). People get paralyzed from that. Their face gets droopy, one eye might close. Now I realize how harmful it is. (woman)
Also, over time, most participants arrived at their own ways of incorporating at least some activities and attitudes associated with successful management of HTN into their lives.
Now, (taking medications) has become a habit. I don’t feel like any of it is hard, like before. I need to do this for my family. (man)
Reflection. Some participants looked back over their life and wondered if their current health state might have been better had they been more attentive to the diagnosis.
I didn’t follow the advice my doctor’s advice back then (30 years ago). My pressure would have been under control, and the heart wouldn’t have to work that hard and, I wouldn’t have had to go to the hospital for (heart) surgery. That I regret. (man)
Others, especially those who were older continued to believe that ultimately, they were not solely in control of this disease process.
When we have done what we can do, God has the ultimate control. (woman)
Core category: Fitting it in
The South Asian participants in this study consistently spoke about how to “fit” HTN into their already challenging lives. Even those who quickly accepted the diagnosis had to find ways to “fit in” exercise, a change in diet, and regularly taking medications.
I accept that I have high blood pressure, but when life is busy due to travel back home, and take care of my family, my exercise routine does suffer. I have to get back to it, but it is difficult. (woman)
Another participant spoke about the challenges of keeping the taste in food.
We have our usual ways of cooking, and we do not want to compromise with the taste we are accustomed to. But we must try new ways (of cooking) to stay healthy. (man)
Finally, another participant offered insights about taking medications.
Yeah, even though I know my dad had it (HTN) and its inherited, sometimes I forget to take my medication in the morning. It’s just tough to remember every day, but I must keep trying and make it a habit. (man)
Discussion
South Asians live longer with HTN as they develop the disease ~10 years younger relative to white European.15 Thus, it is imperative to understand the complexities of how they choose to manage this condition. We have identified that there are specific contexts and elements faced by South Asian people when “fitting” HTN and its treatment into their lives. These include primarily family and social contexts, cultural and religious beliefs, as well as access to healthcare resources.
Family is foremost in the South Asian culture.43 Each member plays a certain role. Women can be caring for generations of family members, while men as head of the household are the key decision-makers. Once immigrated, both women and men may work outside the home. Yet, women will continue to have household responsibilities and will ultimately defer to the husband (as well as other senior family members) should lifestyle changes be suggested. It is not uncommon for women to make significant changes for the sake of their husbands, but not for themselves.44,45 A qualitative study revealed that South Asian women, and especially those who are older, felt that making time to address health needs (eg, exercise) is not culturally consistent with their primary role of dedicating themselves to the family.46 Ultimately, it is “almost expected (for both women and men) to sacrifice health … for one’s work and family … (because) they have sacrificed a great deal to leave their homelands and to provide better lives for their family and children”.43
Indeed, immigration itself is stressful as people work diligently to create a successful life in their new country. South Asians may feel that living and adjusting to life in a new country contributes to significant stress.47 A systematic review revealed that South Asians may “over-attribute the origin of their cardiovascular disease to stress and not to other modifiable lifestyle behaviors”.43
Immigrants bring unique culture and religious beliefs and practices to their new community, which can be a great source of pride.48 Reconciling health behavior recommendations with cultural practices, particularly associated with food and how it is shared, can be very challenging.43 Our group has found that South Asians do not readily accept the concept of having a chronic illness17–19 and acquiring illness is often perceived as outside of one’s control. Thus, health behavior change for future benefit is not seen as a priority in their already demanding lives.21,43 A recent study suggested that present-fatalistic orientation to time (eg, “living in the moment” with a belief that what one does today will not have any real influence – good or bad – in the future; apathetic49 is associated with certain subgroups of the South Asians (older, women) (unpublished data).
Study participants also appreciated being able to access healthcare resources that are culturally and linguistically compatible. A systematic review50 revealed that effective communication with healthcare providers is central to South Asian patients’ adherence. South Asians tend to have a great respect for physicians and other healthcare providers and their advice. However, if there is discordance in communication, adherence is reduced significantly. Other qualitative work51,52 has revealed that relationships with healthcare professionals, and physicians in particular, are central to adherence and that South Asian patients take medication with the hope of being able to reduce or quit taking medications in the future.
Strengths and limitations
There were several important strengths to this study. The participants in this study were representative of those South Asians currently residing in Canada (ie, higher education and variability in time since immigration)13 as well as those who have HTN (ie, broad range of age groups).15 There was also representation of people who spoke the two most common South Asian languages13 while rigorous translation processes were used.19 The team of researchers also included members of the South Asian community who could offer important insights and context to the data analysis. There were some limitations to this work. The majority of participants were of the Sikh religion and had immigrated from India. It is possible that had there been a more diverse representation of religion and place of origin, additional insights would have been offered.
Conclusion
There were different approaches to accepting and managing HTN in this sample of South Asians. Those who were resistant, dismissive of, or refused to acknowledge the diagnosis, tended to position social/family responsibilities ahead of their own health. It is important for healthcare providers to consider these culturally based barriers in their health counseling.
Acknowledgment
Kathryn M King-Shier was funded by the Guru Nanak Dev Ji DIL Research Chair, a partnership between the DIL Walk Foundation and the University of Calgary. The sponsor had no involvement in this project.
Author contributions
All authors contributed toward data analysis, drafting, and critically revising the paper, and agree to be accountable for all aspects of the work. All the authors have reviewed and approved the final version.
Disclosure
The authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
References
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. | ||
Government of Canada [homepage on the Internet]. Hypertension facts and figures. Available from: https://www.canada.ca/en/public-health/services/chronic-diseases/cardiovascular-disease/hypertension-facts-figures.html. Accessed February 11, 2019. | ||
Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134(6):441–450. | ||
Padwal RS, Bienek A, McAlister FA, Campbell NR. Outcomes Research Task Force of the Canadian Hypertension Education Program. Epidemiology of hypertension in Canada: an update. Can J Cardiol. 2016;32(5):687–694. | ||
Leung AA, Daskalopoulou SS, Dasgupta K, et al. Hypertension Canada’s 2017 guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults. Can J Cardiol. 2017;33(5):557–576. | ||
Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension. J Hypertens. 2013;31(7):1281–1357. | ||
Nguyen T, Lau DC. The obesity epidemic and its impact on hypertension. Can J Cardiol. 2012;28(3):326–333. | ||
Primatesta P, Falaschetti E, Gupta S, Marmot MG, Poulter NR. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension. 2001;37(2):187–193. | ||
Rossi A, Dikareva A, Bacon SL, Daskalopoulou SS. The impact of physical activity on mortality in patients with high blood pressure: a systematic review. J Hypertens. 2012;30(7):1277–1288. | ||
Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. N Engl J Med Overseas Ed. 2001;344(1):3–10. | ||
Sparrenberger F, Cichelero FT, Ascoli AM, et al. Does psychosocial stress cause hypertension? A systematic review of observational studies. J Hum Hypertens. 2009;23(1):12–19. | ||
Yun M, Li S, Sun D, et al. Tobacco smoking strengthens the association of elevated blood pressure with arterial stiffness: the Bogalusa heart study. J Hypertens. 2015;33(2):266–274. | ||
Statistics Canada. Immigration and Ethnocultural diversity in Canada; 2011. Available from: http://www12.statcan.gc.ca/nhs-enm/2011/as-sa/99-010-x/99-010-x2011001-eng.cfm | ||
Anand SS, Yusuf S, Vuksan V, et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the study of health assessment and risk in ethnic groups (SHARE). Lancet. 2000;356(9226):279–284. | ||
Quan H, Chen G, Walker RL, et al. Incidence, cardiovascular complications and mortality of hypertension by sex and ethnicity. Heart. 2013;99(10):715–721. | ||
Jones CA, Mawani S, King KM, et al. Tackling health literacy: adaptation of public hypertension educational materials for an Indo-Asian population in Canada. BMC Public Health. 2011;11:24. | ||
Bedi H, Leblanc P, Mcgregor L, Mather C, King KM. Older immigrant Sikh men’s perspective of the challenges of managing coronary heart disease risk. J Mens Health. 2008;5(3):218–226. | ||
King KM, Mather CD, Sanguins J. Ethnocultural affiliation, gender, and cardiovascular disease risk management. Can J Cardiovasc Nurs. 2005;15(2):10–16. | ||
King KM, Leblanc P, Sanguins J, Mather C. Gender-based challenges faced by older Sikh women as immigrants: recognizing and acting on the risk of coronary artery disease. Can J Nurs Res. 2006;38(1):16–40. | ||
Chong E, Wang H, King-Shier KM, Quan H, Rabi DM, Khan NA. Prescribing and adherence in South Asian, Chinese and white adults with diabetes: a cohort study. Diabet Med. 2014;31(12):1586–1593. | ||
Khan NA, Grubisic M, Hemmelgarn B, et al. Outcomes after acute myocardial infarction in South Asian, Chinese, and white patients. Circulation. 2010;122(16):1570–1577. | ||
Almas A, Hameed A, Ahmed B, Islam M. Compliance to antihypertensive therapy. J Coll Physicians Surg Pak. 2006;16(1):23–26. | ||
Bharucha NE, Kuruvilla T. Hypertension in the Parsi community of Bombay: a study on prevalence, awareness and compliance to treatment. BMC Public Health. 2003;3:1. | ||
Dennis T, Meera NK, Binny K, Sekhar MS, Kishore G, Sasidharan S. Medication adherence and associated barriers in hypertension management in India. CVD Prev Control. 2011;6(1):9–13. | ||
Hashmi SK, Afridi MB, Abbas K, et al. Factors associated with adherence to anti-hypertensive treatment in Pakistan. PLoS One. 2007;2(3):e280. | ||
Joshi PP, Salkar RG, Heller RF. Determinants of poor blood pressure control in urban hypertensives of Central India. J Hum Hypertens. 1996;10(5):299–303. | ||
Palanisamy S, Sumathy A. Intervention to improve patient adherence with antihypertensive medications at a tertiary care teaching hospital. Int J Pharm Tech Res. 2009;1(2):369–374. | ||
Qureshi NN, Hatcher J, Chaturvedi N, Jafar TH, Hypertension Research Group. Effect of general practitioner education on adherence to antihypertensive drugs: cluster randomised controlled trial. BMJ. 2007;335(7628):1030. | ||
Saleem F, Hassali MA, Shafie AA, Awad AG, Bashir S. Association between knowledge and drug adherence in patients with hypertension in Quetta, Pakistan. Trop J Pharm Res. 2011;10(2):125–132. | ||
Ens TA, Seneviratne CC, Jones C, Green TL, King-Shier KM. South Asians’ cardiac medication adherence. Eur J Cardiovasc Nurs. 2014;13(4):357–368. | ||
Akeroyd JM, Chan WJ, Kamal AK, Palaniappan L, Virani SS. Adherence to cardiovascular medications in the South Asian population: a systematic review of current evidence and future directions. World J Cardiol. 2015;7(12):938–947. | ||
Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. 4th ed. Thousand Oaks, CA: Sage; 2015. | ||
Polit DF, Beck CT. Nursing Research: Principles and Methods. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2004. | ||
Hammersley M, Atkinson P. Ethnography. Principles in Practice. 3rd ed. Routledge, New York, NY; 2007. | ||
King KM, Khan N, Leblanc P, Quan H. Examining and establishing translational and conceptual equivalence of survey questionnaires for a multi-ethnic, multi-language study. J Adv Nurs. 2011;67(10):2267–2274. | ||
Kenny M, Fourie R. Contrasting classic, Straussian, and constructivist grounded theory: methodological and philosophical conflicts. Qual Report. 2015;20(9):1270–1298. | ||
Musselwhite K, Cuff L, Mcgregor L, King KM. The telephone interview is an effective method of data collection in clinical nursing research: a discussion paper. Int J Nurs Stud. 2007;44(6):1064–1070. | ||
Gerstein LH. Methodological issues in cross-cultural counseling research: equivalence, bias, and translations. J Couns Psychol. 2008;36(2):188–219. | ||
Larkin PJ, Dierckx de Casterlé B, Schotsmans P. Multilingual translation issues in qualitative research: reflections on a metaphorical process. Qual Health Res. 2007;17(4):468–476. | ||
Squires A. Methodological challenges in cross-language qualitative research: a research review. Int J Nurs Stud. 2009;46(2):277–287. | ||
Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago, IL: Aldine Publishing Co; 1967. | ||
Sandelowski M. The problem of rigor in qualitative research. Adv Nurs Sci. 1986;8(3):27–37. | ||
Patel M, Phillips-Caesar E, Boutin-Foster C. Barriers to lifestyle behavioral change in migrant South Asian populations. J Immigr Minor Health. 2012;14(5):774–785. | ||
Astin F, Atkin K, Darr A. Family support and cardiac rehabilitation: a comparative study of the experiences of South Asian and white European patients and their carer’s living in the United Kingdom. Eur J Cardiovasc Nurs. 2008;7(1):43–51. | ||
Mather CM, King KM, Leblanc P. Meanings of the heart among a group of older Sikh immigrant women with cardiovascular disease. Int J Mult Res Approaches. 2007;1(1):39–51. | ||
Kalra P, Srinivasan S, Ivey S, Greenlund K. Knowledge and practice: the risk of cardiovascular disease among Asian Indians. Results from focus groups conducted in Asian Indian communities in northern California. Ethnic Dis. 2004;14(4):497–504. | ||
Darr A, Astin F, Atkin K. Causal attributions, lifestyle change, and coronary heart disease: illness beliefs of patients of South Asian and European origin living in the United Kingdom. Heart Lung. 2008;37(2):91–104. | ||
Galanti GA. Caring for Patients from Different Cultures. Pensylvannia, PA: University of Pennsylvania Press; 2015. | ||
Zimbardo P, Boyd J. The Time Paradox. New York, NY: New York Free Press; 2008. | ||
Sohal T, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PLoS One. 2015;10(9):e0136202. | ||
Ens TA, Seneviratne CC, Jones C, King-Shier KM. Factors influencing medication adherence in South Asian people with cardiac disorders: an ethnographic study. Int J Nurs Stud. 2014;51(11):1472–1481. | ||
King-Shier KM, Singh S, Khan NA, et al. Ethno-cultural considerations in cardiac patients’ medication adherence. Clin Nurs Res. 2017;26(5):576–591. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.