")
Back to Journals » Clinical Interventions in Aging » Volume 16
Somatotype and Its Impact on Asymptomatic Target Organ Damage in the Elderly Chinese: The Northern Shanghai Study
Authors Xiong J, Qian Y, Yu S, Ji H, Teliewubai J, Chi C , Lu Y, Zhou Y, Fan X , Li J, Blacher J, Zhang Y , Xu Y
Received 21 January 2021
Accepted for publication 13 April 2021
Published 21 May 2021 Volume 2021:16 Pages 887—895
DOI https://doi.org/10.2147/CIA.S302468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Jing Xiong,1,* Yunyun Qian,1,* Shikai Yu,1 HongWei Ji,1 Jiadela Teliewubai,1 Chen Chi,1 YuYan Lu,1 YiWu Zhou,1 XiMin Fan,1 Jue Li,2 Jacques Blacher,3 Yi Zhang,1 YaWei Xu1
1Department of Cardiology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2The Research Institute of Clinical Epidemiology, Tongji University School of Medicine, Shanghai, People’s Republic of China; 3Paris Descartes University, AP-HP, Diagnosis and Therapeutic Center, Hôtel-Dieu, Paris, France
*These authors contributed equally to this work
Correspondence: Yi Zhang; Yawei Xu
Department of Cardiology, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, 301 Yanchang Road, Shanghai, 200072, China
Tel +86-21-66308182
Fax +86-21-66301051
Email [email protected]; [email protected]
Objective: To investigate the relationship between asymptomatic target organ damage (TOD) and different somatotypes in a population of elderly from Chinese community-dwelling.
Methods: A total of 2098 Chinese senior residents from northern Shanghai older than 65 years were recruited in the research. The following somatotype parameters were recorded and analyzed: body mass index, waist circumference, hip circumference, and waist-hip ratio were recorded and calculated. Asymptomatic TOD, including urine albumin/creatinine ratio, estimated glomerular filtration rate (eGFR), intima-media thickness (IMT), left ventricular mass index (LVMI), left ventricular diastolic function, and carotid-femoral pulse wave velocity (PWV) was recorded using the MyLab30 Gold CV system and SphygmoCor.
Results: Of all 2098 residents, 817 (38.9%) were overweight and 289 (13.8%) were obese. All somatotype measures were significantly correlated with TOD parameters (p< 0.05). After adjustment for age and male gender, in total population, LVMI (p< 0.001), cardiac diastolic function (E/Ea, p< 0.001), PWV (p< 0.001), eGFR (p=0.03), and urine albumin/creatinine ratio (p< 0.001) changed gradually and significantly correlated with increasing BMI values. Obesity and overweight were independently related to the incidence of LVH, LVDD, artery stiffness, carotid arterial plaque, and microalbuminuria.
Conclusion: The incidence of asymptomatic TOD was significantly correlated with overweight and obesity, especially in women, whereas the underweight may favor in the prevention of TOD.
Keywords: Chinese elderly cardiovascular risk
Introduction
Since 1990, cardiovascular (CV) disease is the leading cause of death in China.1 Meanwhile, widespread lifestyle changes increased the obesity in China.2 Several investigations indicated that the obese were prone to develop CV diseases.3–6 Since target organ damage (TOD) was widely recognized as the intermedium between CV risk factors and CV diseases, it is warranted to investigate the association of TOD with somatotype.
As result of prolonged life expectancy and reduced birth ratio, China is one of the countries experiencing the most rapid social aging. In 2015, 16.15% of the Chinese people were over 65 years old. In 2055, the proportion of the Chinese aging population will peak at 27.2%.7 Therefore, an increasing economic and medical burden, due to an increase in the elderly population, will be a serious problem for the government in next several decades.
Although there were several studies investigating the relationship between asymptomatic TOD and obesity.3,5,6,8,9 There were only few conducted in a geriatric population. Since social aging is a serious problem in China, we were aimed at investigating the relationship between asymptomatic target organ damage (TOD) and different somatotype in elderly population Chinese community-dwelling.
Methods
Study Design and Subject Inclusion Criteria
The present investigation is nested in the Northern Shanghai Study (ClinicalTrials.gov Identifier: NCT02368938). The northern Shanghai study is a community-based study in progress in order to establish a framework of CV risk assessments in the urban elderly residents. This study was approved by the Research Ethics Committee of Shanghai Tenth People’s Hospital.
All details of study design were already described in the protocol of Northern Shanghai Study published in the journal of BMJ open.10 By the end of June 30th, 2017, the northern Shanghai study enrolled 2098 participants.
Social, Clinical and Anthropometric Parameters
All details were already described in the previous protocol.10 Anthropometric parameters included body height, body weight, waist circumference, hip circumference. Social and clinical data were obtained through a questionnaire, including age, gender, disease history, and drug used. Obesity was defined by body mass index (BMI, the ratio of body weight [kilogram] and body height [meter] square), including the following categories: underweight (BMI<18.5 kg/m2), normal (18.5 ≤ BMI <24 kg/m2), overweight (24 ≤ BMI <28 kg/m2), and obese (BMI ≥28 kg/m2).11 Abdominal obesity was defined as waist circumference greater than 80 cm (women), and greater than 85 cm (men).
Measurement of Asymptomatic TOD
Echocardiography parameters and intima-media thickness (IMT) were measured by the MyLab 30 Gold Cardiovascular System (Esaote SEpA, Genoa, Italy) as previously described.10 Echocardiography parameters were measured under the American Society of Echocardiography (ASE) recommendations, including left ventricular end-diastolic diameter and septal and posterior wall thickness, left atrial parameters (long axis, four chambers), peak E (Early diastolic), A (late diastolic) velocities, and primary Early diastolic velocity (Ea). Left atrial volume was estimated by using the ellipse model formula,12 and standardized for the body surface area as left atrial volume index (LAVI). Left ventricular mass index (LVMI) was calculated using the ASE-recommended formula,13 and standardized to body size. Left ventricular diastolic dysfunction (LVDD) was defined according to the ASE recommendation.14,15 If E/Ea ≥ 15, the subject was considered as LVDD. If 8 < E/Ea < 15, LVDD was defined by the presence of any of the following evidences of abnormal left ventricular function: (1) LAVI > 40mL/m2; (2) LVMI > 149g/m2 for male or LVMI > 122g/m2 for female. Left ventricular hypertrophy (LVH) was defined as LVMI > 115g/m2 for male or LVMI > 95g/m2 for female.
Carotid-femoral pulse wave velocity (cf-PWV) was measured with applanation tonometry (SphygmoCor, AtCor Medical, Sydney, Australia) on the basis of the European Expert Consensus on Arterial Stiffness.16,17 Arterial stiffness was defined as cf-PWV>10m/s.
The urine albumin to creatinine ratio was obtained from a urine sample test. Calculating the estimated glomerular filtration rate (eGFR) used the original CKD-EPI equation.18
Statistical Analysis
Participant characteristics were presented as mean ± standard deviation (SD) for continuous variables and as proportion (percentage) for categorical variables. Correlation between different anthropometric parameters and CV parameters was determined using univariate regression analysis. General linear model tests and DUNCAN’s multiple range test were applied for the comparisons of characteristics of asymptomatic TOD among different somatotypes. Multivariate logistics regression was performed to analyze the specific relationship between different somatotype and asymptomatic TOD. Statistical analyses were performed using the SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA). Statistically significant difference was set at p<0.05.
Results
Characteristics of the Participants
By the end of July, 2017, 2285 subjects were initially invited to participate in the study, of whom 2098 (92.9%) were enrolled and examined. The final sample was 2098 participants, which met the inclusion criteria and related CV parameters. Table 1 summarizes population characteristics. The mean age of the total population was 71.3±6.12 years, with 955 (46%) men. The total mean BMI was 23.9. Among the elderly community, 817 (38.9%) were overweight, 289 (13.8%) were obese, and 100 (4.8%) were underweight. In addition, almost all the overweight (749/817, 91.6%) and obesity (286/289, 99.0%) had abdominal obesity. This is the reason why we did not include an abdominal obesity subgroup analysis.
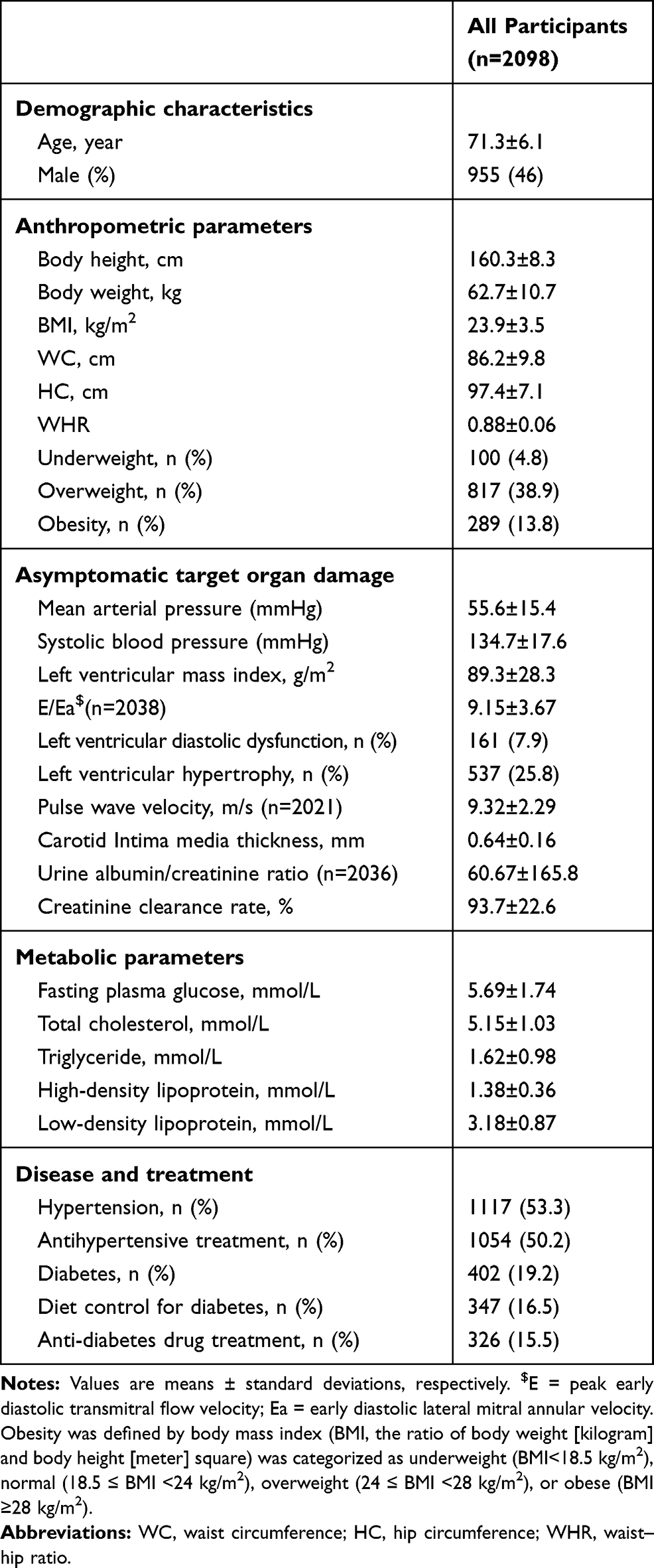 |
Table 1 Participants’ Characteristics |
Table 1 shows the disease prevalence and TOD parameters of all participants. More than half of population had hypertension (1117 (53.3%)), and the majority of patients with hypertension took antihypertensive agents (1054 (50.2%)). Left ventricular diastolic dysfunction (LVDD) was exist in 161 (7.90%) of the patients, and a quarter of patients (537 (25.8%)) had left ventricular hypertrophy (LVH).
Correlation Between TOD Parameters and Different Anthropometric Parameters
Univariate correlation analyses were utilized to investigate the association of TOD with anthropometric parameters (Table 2). All anthropometric measures, including body mass index (BMI), waist circumference (WC), hip circumference (HC), and waist-hip ratio (WHR), were significantly correlated with cardiac, vascular and renal TOD parameters (p<0.05). Only E/Ea and WHR were not significantly correlated, except for the association between E/Ea and WHR (p=0.06).
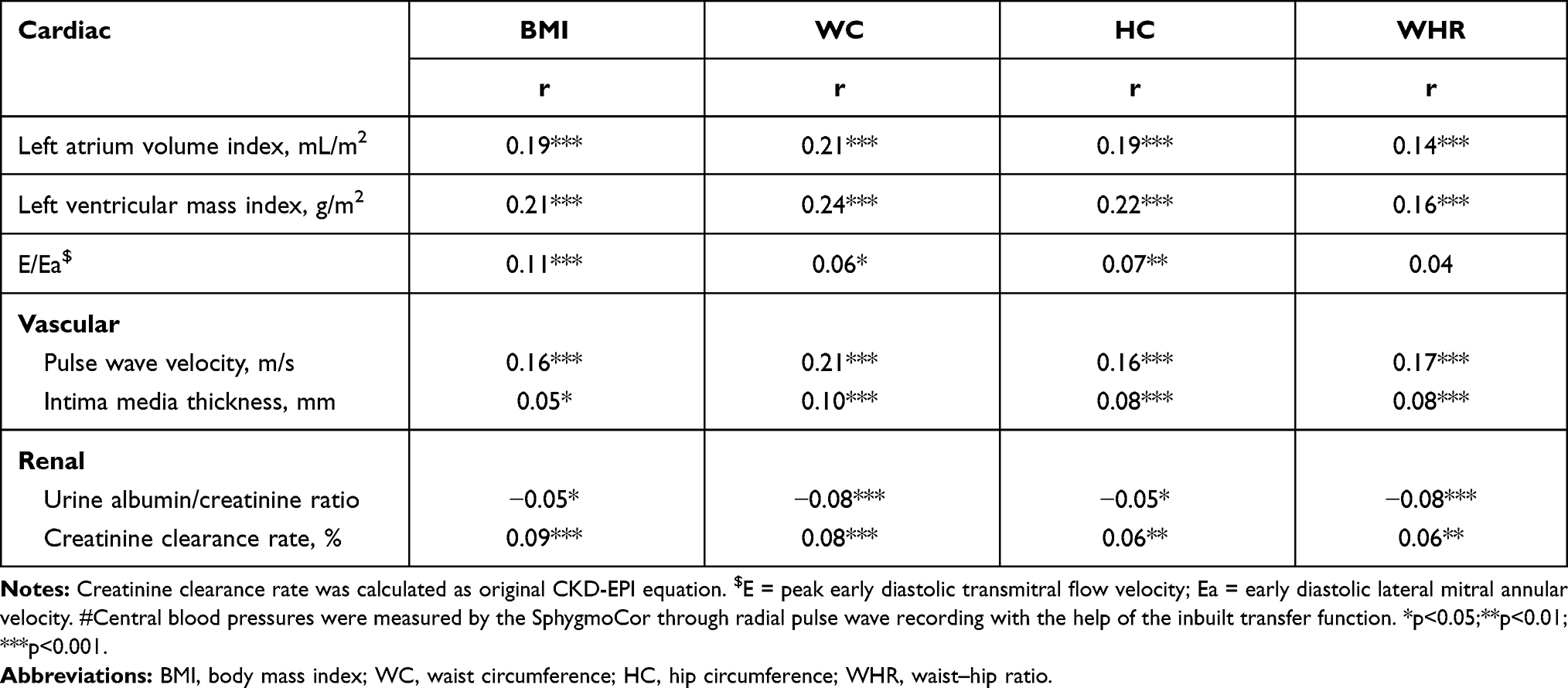 |
Table 2 The Correlation Between Different Anthropometric Parameters and Target Organ Damage Parameters |
TOD According to the Participants’ Somatotype
With increasing BMI values, categorized as four grades: underweight (BMI<18.5 kg/m2), normal (18.5≤BMI<24 kg/m2), overweight (24≤ BMI<28 kg/m2), or obese (BMI≥28 kg/m2), as depicted in Table 3, LVMI (p<0.001), diastolic function (E/Ea, p<0.001), PWV (p<0.001), and urine albumin/creatinine ratio (p<0.001) increased significantly and gradually, whereas eGFR (p=0.03) decreased. With similar adjustments, in the further interclass comparison, taking normal status as reference, LVMI, PWV, and the urine albumin/creatinine ratio were significantly greater in obese, while LVMI and PWV were significantly lower in underweight participants. As shown in Figure 1, the significant increasing trend was observed for the incidence of LVH (p<0.001), LVDD (p=0.04) and artery stiffness (p=0.007), along with the increasing BMI.
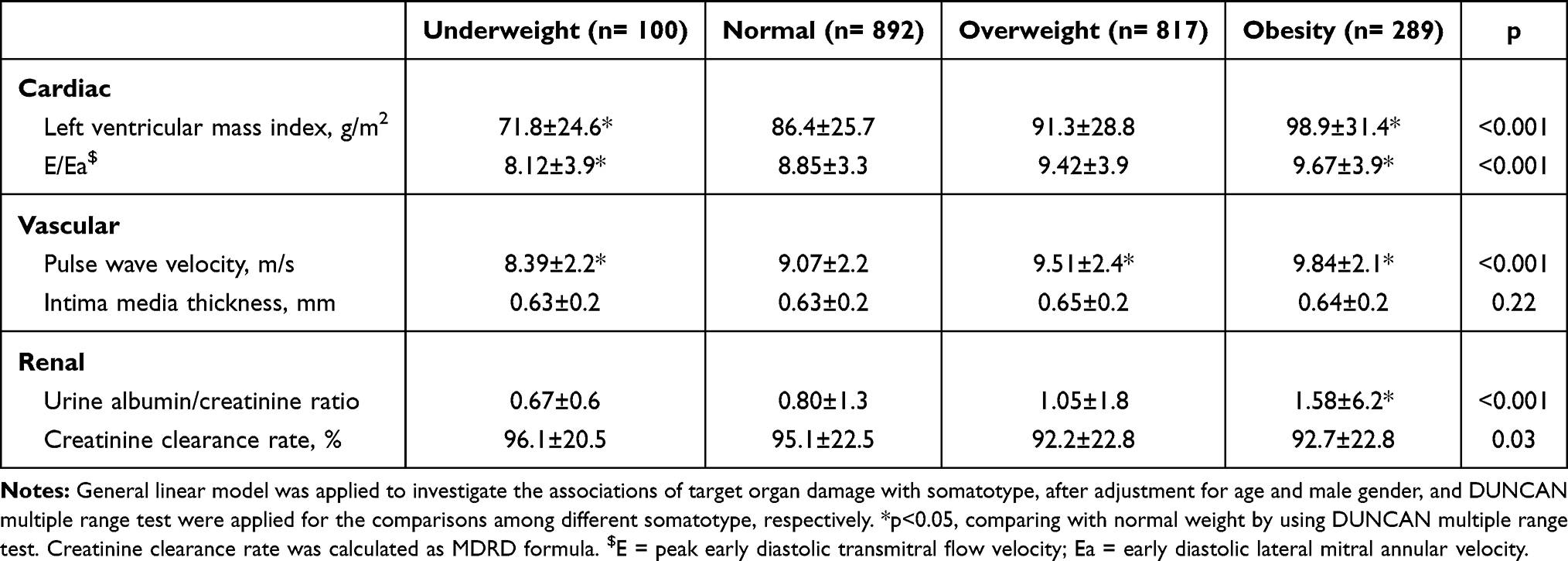 |
Table 3 Target Organ Damage According to Participants’ Somatotype |
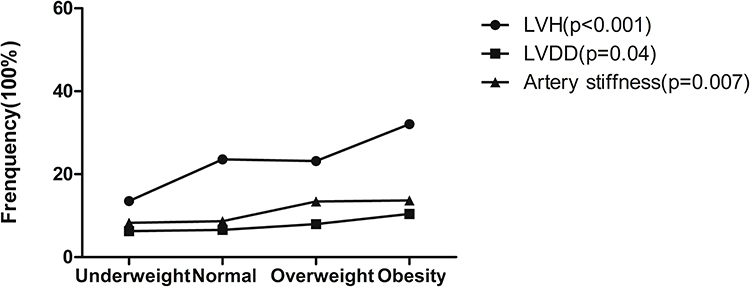 |
Figure 1 Incidence of LVH, LVDD, artery stiffness in different somatotype. Abbreviations: LVH, left ventricular hypertrophy; LVDD, left ventricular diastolic dysfunction. |
Relation Between Asymptomatic TOD and Different Somatotypes
As Table 4 shows, BMI was independently related to the LVH, LVDD, artery stiffness, carotid arterial plaque, and microalbuminuria after adjustments for age and male gender, mean arterial pressure, fasting plasma glucose, low-density lipoprotein cholesterol, glomerular filtration rate. Compared to the normal somatotype, the odds ratio (OR) of LVDD was 1.78 for overweight (95% confidence interval [CI]: 1.20, 2.65, p=0.004) and 2.51 for obese participants (95% CI: 1.57, 4.02, p<0.001). The OR of artery stiffness was 1.65 for obese (95% CI: 1.20, 2.52, p=0.002). The OR of microalbuminuria was 1.31 for overweight (95% CI: 1.07, 1.60, p=0.007) 1.39 for obese (95% CI: 1.05, 1.84, p=0.02). The OR of LVH for obese compared with normal somatotype was 2.05 (95% CI: 1.52, 2.78, p<0.001). Of note, OR of LVH for underweight compared with normal somatotype was 0.47 (95% CI: 0.24, 0.90, p=0.03, Figure 2). The OR of carotid arterial plaque for underweight compared with normal somatotype was 0.60 (95% CI: 0.39, 0.94, p=0.02). The same result was found after adjustments for age and male gender, mean arterial pressure, hypertension, diabetes, glomerular filtration rate (Supplemental Table 1).
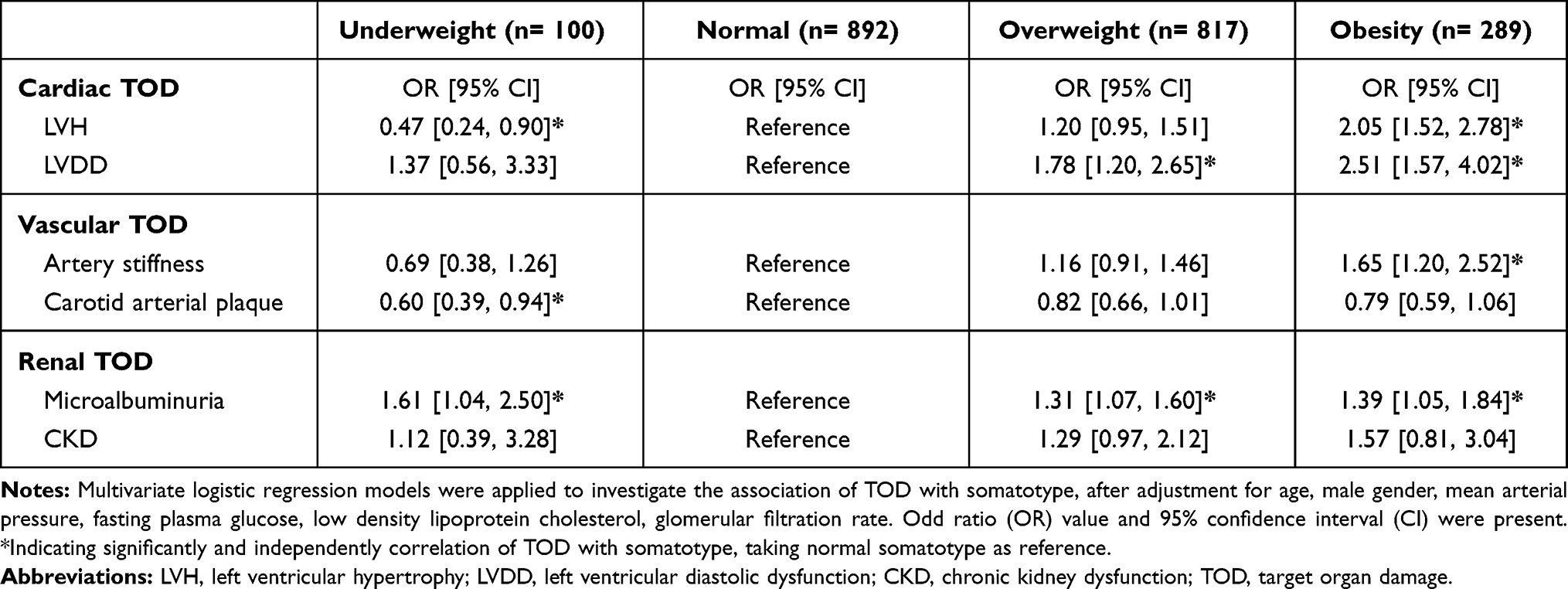 |
Table 4 Multivariate Logistic Regression Analysis on the Association of Target Organ Damage with Somatotype |
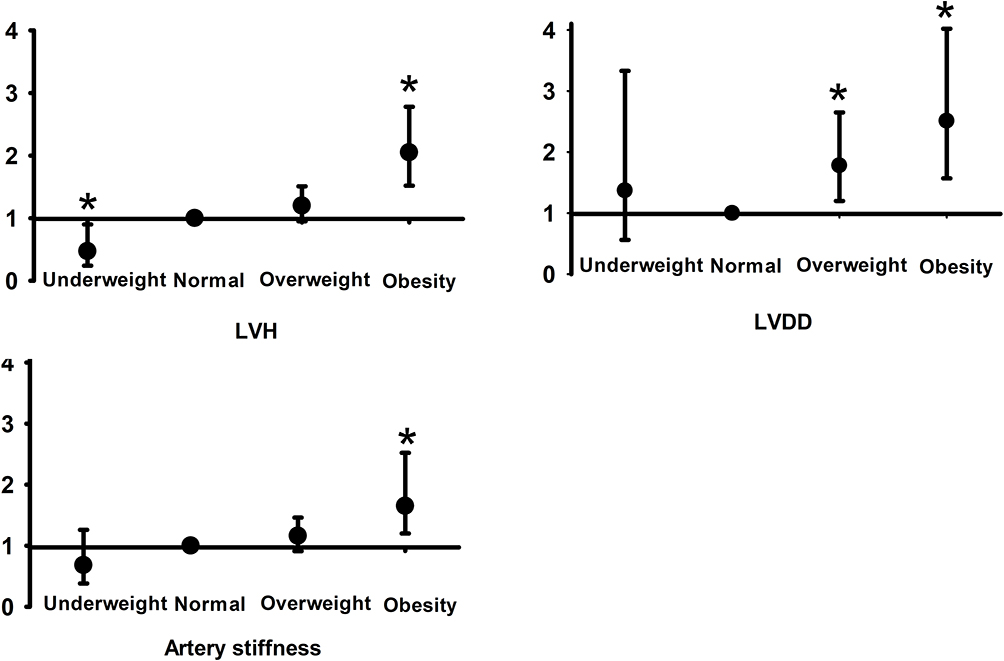 |
Figure 2 Multivariate logistic regression analysis on the association of target organ damage with somatotype (normal somatotype as reference); *p<0.05. Abbreviations: LVH, left ventricular hypertrophy; LVDD, left ventricular diastolic dysfunction. |
Sexual Differences in the Incidence of TOD of Different Somatotypes
Figure 3 shows the sexual subgroup analysis. The incidence of LVDD was 7.02%, 6.78%, 11.3% and 15.5% for female participants with underweight, normal, overweight and obese, respectively (p<0.001). Yet, there was no significant and gradual change with increasing BMI in male subjects (p=0.12). Meanwhile, the incidence of artery stiffness also increased gradually and significantly with increasing BMI in female (p<0.01) but not in male (p=0.73). LVH increased significantly and gradually from 0% to 23.1% (P<0.01) in men, and from 22.4% to 50.3% (P<0.001) in women.
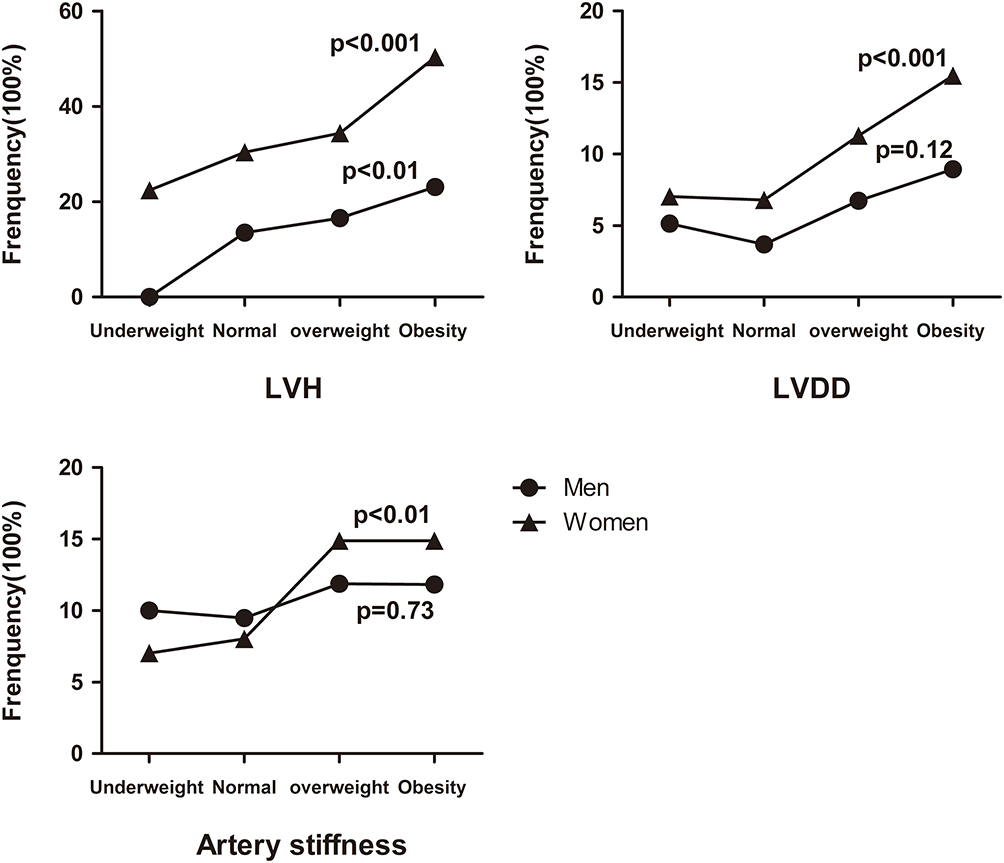 |
Figure 3 Sexual differently incidence of LVH, LVDD, artery stiffness in different somatotype. Abbreviations: LVH, left ventricular hypertrophy; LVDD, left ventricular diastolic dysfunction. |
Discussion
In the present study, there are two major findings. First, the presence of obesity in the old Chinese citizens was 13.8% with a BMI over 28 kg/m2, and the figure for the overweight was 38.9% with a BMI over 24 kg/m2. Second, all somatotype parameters and the status of obesity or overweight were significantly associated with asymptomatic TOD, whereas the underweight (BMI<19kg/m2) was reversely associated with LVH and carotid arterial plaque.
The prevalence of somatotypes on the health of the elderly is the focal point in many elderly studies. Although Jan-Magnus et al have reported that underweight individuals have higher mortality than overweight individuals because the former is susceptible to respiratory diseases in Norwegian geriatric population. And excluding respiratory diseases, overweight and obesity individuals also have increased mortality.19 The reason for the higher mortality rate of increasing BMI and obese elderly is still unknown. Obesity contributes to CV disease, which is multifactorial, including insulin resistance, hypertension, and dyslipidemia, cardiac remodeling including LVH and chamber enlargement, vascular endothelial dysfunction.20 There was increasing evidence from western countries suggested that obesity increased the incidence of coronary heart disease, even worsened heart failure prognosis, and increased CV mortality in adult.9,21,22 Teixeira et al also documented CV disease risk factor among obese children group.23 However, there are still no appropriate risk factors identified for asymptomatic TOD. The most important predictors are still the classic risk factors, especially blood pressure and age.24,25 In the present study, we focus obese Chinese geriatric population. We found that obesity was significantly associated with asymptomatic TOD.
Obesity and overweight were associated with heart remodeling, resembling the changes found in patients with hypertension.3,8,26 Lauer et al indicated that, in 3922 participants from the Framingham Heart Study, health obese population was likely to have greater LVMI.3 Bello et al indicated that, in 4343 senior residents (69–82 years old) from the Atherosclerosis Risk in Communities (ARIC) study also highlight the association of obesity and subclinical LV remodeling.8 The present study also showed the considerate increase of LVH in the obese Chinese elderly. From a pathological viewpoint, severe myocardial fibrosis, a typical signature of pathological cardiac hypertrophy, was found in ob/ob mice with leptin treatment, which was also common in the obese animals and human being.27
Despite cardiac structural remodeling consistently exist in the obese population and obese animals, obesity was not rarely associated with cardiac functional abnormalities, after adjustment for clinical covariates.28 Moreover, Bello et al found that, in 4343 large old individuals, obese women were prone to develop cardiac dysfunction, whereas men did not.8 We also found similar gender discrepancies in the present study. Obese women were prone to develop LVH and LVDD. On the contrast, obese men did not exhibit the increased incidence of LVDD. This gender discrepancy in response to the obesity, with the cardiac structural or functional change, need further investigations. In this respect, gender-specific analysis was warranted in this field in both population level and animal level. It is also noteworthy that, women, compared to men, with the similar somatotype, had significantly greater subcutaneous abdominal fat.
Although compared to the elderly from western countries, the aged Chinese may enjoy a “healthy” somatotype (obesity rate: China, 13.8%; United State, 33.9%, p<0.05).8 However, even in this relatively “lean” geriatric population, we also found that obesity plays a negative effect on the development of TOD. It reminded us a Chinese old proverb: billions cannot buy someone thin at his old age. Keeping fit is really necessary for the Chinese elderly. Given the gender differences in obesity-related TOD, female Chinese elderly should pay more attention to control their body weight.
Our community-based study contained the relatively large and centralized sample size, which gives us sufficient data with a variety of statistical methods for some subgroup analysis. However, our findings still have certain limitations to be interpreted. The first limitation is the fact that in cross-sectional analyses, the causal association between two related factors cannot be well established, but some prospective data would be available with our undergoing follow-up study. The second limitation is that the present study only focused on the traditional measures of obesity, which did not include several novel indexes, such as visceral fat. However, the obesity parameters in the present study are routinely used in clinical practice in China. The third limitation of this study is several new parameters of LVDD assessment recommended by the recent guidelines, including the early mitral flow deceleration and peak velocity of tricuspid regurgitation (peak-TR velocity), were not included in this study.29 The fourth limitation is the sample size which is not large enough to support the follow-up subgroup analysis for further discussion.
Conclusion
In Chinese community-dwelling elderly, the prevalence of obesity and overweight were 13.8% and 38.9%, respectively. The incidence of asymptomatic TOD was significantly associated with overweight and obesity, especially in women, whereas the underweight may favor in the prevention of TOD.
Data Sharing Statement
Research data are not shared.
Ethics Statement
This study was approved by the Research Ethics Committee of Shanghai Tenth People’s Hospital and was conducted in accordance with the Declaration of Helsinki. All participants signed the informed consent.
Acknowledgments
We would like to express our gratitude to all the participants and investigators of the Northern Shanghai Study. Jing Xiong and Yunyun Qian should be considered joint first author.
Funding
This study was financially supported by the National Key Research and Development Program (2016YFC1301202 from), and Clinical Research Plan of SHDC (No. SHDC2020CR1040B, SHDC2020CR5009, SHDC2020CR5015-002). Dr. Yi Zhang was supported by the National Nature Science Foundation of China (Grant ID. 81300239; 81670377). Dr. Xiong was financially supported by the National Nature Science Foundation of China (81900292) and Shanghai Sailing Program (19YF1438000).
Disclosure
The abstract of this paper was presented at the 2018 International Society of Hypertension Conference as a conference talk with interim findings. The poster’s abstract was published in “Poster Abstracts” in journal of hypertension: Hyperlink with DOI: 10.1097/01.hjh.0000548409.69528.da.
The authors report no conflicts of interest in this work.
References
1. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
2. Collaboration NCDRF. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet. 2017.
3. Lauer MS, Anderson KM, Kannel WB, Levy D. The impact of obesity on left ventricular mass and geometry. The Framingham heart study. JAMA. 1991;266(2):231–236. doi:10.1001/jama.1991.03470020057032
4. Lavie CJ, Alpert MA, Arena R, et al. Impact of obesity and the obesity paradox on prevalence and prognosis in heart failure. JACC Heart Fail. 2013;1(2):93–102. doi:10.1016/j.jchf.2013.01.006
5. Wong CY, O’Moore-Sullivan T, Leano R, et al. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004;110(19):3081–3087. doi:10.1161/01.CIR.0000147184.13872.0F
6. Wong CY, O’Moore-Sullivan T, Leano R, et al. Association of subclinical right ventricular dysfunction with obesity. J Am Coll Cardiol. 2006;47(3):611–616. doi:10.1016/j.jacc.2005.11.015
7. Keyong Dong YY. Annual report of the development of China’s aging finance (2016). In: Sun B, editor. Annual Report of the Development of China’s Aging Finance (2016). Literature of Social Science Press; 2016:5.
8. Bello NA, Cheng S, Claggett B, et al. Association of weight and body composition on cardiac structure and function in the ARIC study (atherosclerosis risk in communities). Circ Heart Fail. 2016;9(8):9. doi:10.1161/CIRCHEARTFAILURE.115.002978
9. Wilson PW, D’Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162(16):1867–1872. doi:10.1001/archinte.162.16.1867
10. Ji H, Xiong J, Yu S, et al. Northern Shanghai study: cardiovascular risk and its associated factors in the Chinese elderly-a study protocol of a prospective study design. BMJ Open. 2017;7(3):e013880. doi:10.1136/bmjopen-2016-013880
11. Chen C, Lu FC. Department of disease control ministry of health PRC. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed Environ Sci. 2004;17 Suppl:1–36.
12. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1–39):e14. doi:10.1016/j.echo.2014.10.003
13. Nunan D, Wassertheurer S, Lasserson D, et al. Assessment of central haemomodynamics from a brachial cuff in a community setting. BMC Cardiovasc Disord. 2012;12(1):48. doi:10.1186/1471-2261-12-48
14. Paulus WJ, Tschope C, Sanderson JE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the heart failure and echocardiography associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539–2550. doi:10.1093/eurheartj/ehm037
15. Nagueh SF, Appleton CP, Gillebert TC, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10(2):165–193. doi:10.1093/ejechocard/jep007
16. Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–2605. doi:10.1093/eurheartj/ehl254
17. Chirinos JA. Arterial stiffness: basic concepts and measurement techniques. J Cardiovasc Transl Res. 2012;5(3):243–255. doi:10.1007/s12265-012-9359-6
18. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
19. Kvamme J-M, Holmen J, Wilsgaard T, et al. Body mass index and mortality in elderly men and women: the Tromsø and HUNT studies. J Epidemiol Community Health. 2012;66(7):611–617. doi:10.1136/jech.2010.123232
20. Poirier P, Cornier MA, Mazzone T, et al. Bariatric surgery and cardiovascular risk factors: a scientific statement from the American Heart Association. Circulation. 2011;123(15):1683–1701. doi:10.1161/CIR.0b013e3182149099
21. Yusuf S, Hawken S, Ounpuu S, et al. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study. Lancet. 2005;366(9497):1640–1649. doi:10.1016/S0140-6736(05)67663-5
22. Canoy D, Boekholdt SM, Wareham N, et al. Body fat distribution and risk of coronary heart disease in men and women in the European prospective investigation into cancer and nutrition in norfolk cohort: a population-based prospective study. Circulation. 2007;116(25):2933–2943. doi:10.1161/CIRCULATIONAHA.106.673756
23. Teixeira PJ, Sardinha LB, Going SB, Lohman TG. Total and regional fat and serum cardiovascular disease risk factors in lean and obese children and adolescents. Obes Res. 2001;9(8):432–442. doi:10.1038/oby.2001.57
24. Alessandro M, Esmerilda Q, Lucia O, et al. Hyperuricemia prevalence in healthy subjects and its relationship with cardiovascular target organ damage. Nutr Metab Cardiovasc Dis; 2020.
25. Maloberti A, Farina F, Carbonaro M, et al. In healthy normotensive subjects age and blood pressure better predict subclinical vascular and cardiac organ damage than atherosclerosis biomarkers. Blood Press. 2018;27:1–9. doi:10.1080/08037051.2017.1407218
26. Dahlen EM, Tengblad A, Lanne T, et al. Abdominal obesity and low-grade systemic inflammation as markers of subclinical organ damage in type 2 diabetes. Diabetes Metab. 2014;40(1):76–81. doi:10.1016/j.diabet.2013.10.006
27. Zibadi S, Cordova F, Slack EH, Watson RR, Larson DF. Leptin’s regulation of obesity-induced cardiac extracellular matrix remodeling. Cardiovasc Toxicol. 2011;11(4):325–333. doi:10.1007/s12012-011-9124-0
28. Fischer M, Baessler A, Hense HW, et al. Prevalence of left ventricular diastolic dysfunction in the community. Results from a Doppler echocardiographic-based survey of a population sample. Eur Heart J. 2003;24(4):320–328. doi:10.1016/S0195-668X(02)00428-1
29. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016;17(12):1321–1360. doi:10.1093/ehjci/jew082
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.