")
Back to Journals » Clinical Interventions in Aging » Volume 15
Soluble Biomarkers of Osteoporosis and Osteoarthritis, from Pathway Mapping to Clinical Trials: An Update
Authors Nagy EE , Nagy-Finna C, Popoviciu H , Kovács B
Received 13 December 2019
Accepted for publication 2 March 2020
Published 8 April 2020 Volume 2020:15 Pages 501—518
DOI https://doi.org/10.2147/CIA.S242288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Előd Ernő Nagy,1 Csilla Nagy-Finna,1,2 Horațiu Popoviciu,2 Béla Kovács1
1Department of Biochemistry and Environmental Chemistry, George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș, Târgu Mureș, Romania; 2Department M4, George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș, Târgu Mureș, Romania; Rheumatology Clinic, Clinical Emergency Hospital, Târgu Mureș, Romania
Correspondence: Előd Ernő Nagy
Department of Biochemistry and Environmental Chemistry, George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș, Gheorghe Marinescu Street No. 38, Târgu Mureș 540139, Romania
Tel +40-265 215551 int. 187
Email [email protected]
Abstract: Serum biomarkers of osteoarticular diseases have been in the limelight of current clinical research trends. Laboratory validation of defined and candidate biomarkers for both osteoarthritis and osteoporosis is of key importance for future decisional algorithms in the diagnosis, monitoring, and prognosis of these diseases. The current guidelines recommend the use of collagen degradation remnants, eg, CTX-I and CTX-II, in the complementary diagnosis of both osteoporosis and osteoarthritis. Besides the collagen degradation markers, enzymes that regulate bone and articular metabolism are useful in the clinical evaluation of osteoarticular pathologies. Along these, several other recommended and new nominee molecules have been recently studied. Wnts and Wnt-related molecules have a cardinal role in the bone-joint homeostasis, making them a promising target not only for pharmaceutical modulation, but also to be considered as soluble biomarkers. Sclerostin and dickkopf, two inhibitor molecules of the Wnt/β-catenin signaling, might have a dual role in the assessment of the clinical manifestations of the osteoarticular unit. In osteoarthritis, besides fragments of collagen type II many pathway-related molecules have been studied and proposed for biomarker validation. The most serious limitation is that a significant proportion of studies lack statistical power due to the reduced number of cases enrolled. Serum biomarkers of bone and joint turnover markers represent an encouraging possibility for the diagnosis and prognosis of osteoarticular diseases, although further studies and laboratory validations should be carried out as to solely rely on them.
Keywords: osteoarthritis, osteoporosis, biomarkers
Introduction
According to the Biomarkers, EndpointS, and other Tools (BEST) Resource glossary, biomarkers are assigned as
A defined characteristic that is measured as an indicator of normal biological processes, pathogenic processes, or responses to an exposure or intervention, including therapeutic interventions.1
This document classifies biomarkers in seven groups, as follows: diagnostic, monitoring, pharmacodynamics/response, predictive, prognostic, safety, and surrogate biomarkers.
The Guidelines for Biomarkers Working Group of the Osteoarthritis Research Society International (OARSI), emitted in 2015 formulates recommendations based on current knowledge and putative, exploitable benefits.2 Biomarkers must be distinguished from clinical outcome assessment, they represent direct measures of feeling, function or survival of subjects supposed to a therapeutic intervention. The development of a soluble biomarker has three essential phases: analytical validation, qualification and practical application.3
Biomarkers can be applied at the preclinical level and in clinical studies, too. Their main goals are the establishment of diagnosis, disease staging, and monitoring, confirmation of pharmacological mechanism of action; demonstration of the biological mechanism of action; prediction of clinical outcome of the disease.4
Bone, although presenting as a passive tissue, is under a continuous, apprehensive metabolic equity, and its homeostasis relies on the harmonious interplay between the bone-forming and bone-disturbing events. In mammalian skeleton, proper bone turnover assures the repair of micro-architectural damage of the osseous tissue and simultaneously contributes to calcium homeostasis.5,6
Osteoporosis is a multifactorial, progressive skeletal disease, one of the most prevalent osteoarticular pathologies, with primary and secondary forms, having distinct etiologic backgrounds.7,8 Type 1 primary osteoporosis is related to postmenopausal women, where decreased estrogen levels are associated with increased pro-inflammatory cytokine levels, eg interleukins (IL-1, IL-6), which cause increased osteoclast activity and subsequent imbalance in bone metabolism shifting to bone loss. In contrast, type 2 primary osteoporosis has an incompletely elucidated pathologic mechanism, usually, bone atrophy that can occur regardless of sex.9 Secondary osteoporosis occurs as a comorbidity with various endocrine affections, like hyperthyroidism or Cushing’s syndrome.7
Osteoporosis has numerous etiologic backgrounds, amongst which age and related low estrogen levels in the postmenopausal period, fracture anamnesis, hyperthyroidism and use of oral corticosteroids are the most noteworthy.10 The main risk factor in osteoporosis is represented by fractures that appear in low-trauma situations. According to the current statistics published by the International Osteoporosis Foundation (IOF) around 200 million people are affected worldwide, mainly represented by the geriatric population and annually over 9 million fractures are reported. These numbers are predicted to arise in the future decades around 2.5–3 times in both the male and female populations, making not only osteoporosis but the musculoskeletal diseases an emerging global health and economic burden.11,12 According to a current experts’ point of view published by Kanis et al13 for the diagnosis of osteoporosis the measurement by dual X-ray absorptiometry (DXA) of bone mineral density (BMD) remains the golden standard. Bone turnover markers (BTMs) might have some prognostic value for the assessment of fragility fractures, when BMD measurements are unavailable.
In this view, the present article seeks to bring an updated overview on the management of both osteoporosis and osteoarthritis, by emphasizing the currently available data and future perspectives of soluble biomarkers, which might augment the diagnosis, monitoring, and prediction of these diseases.
BTMs – General Aspects and Classification in a Nutshell
BTMs are endogenously secreted proteins or derivatives thereof, that are synthesized by osteoblasts and osteoclasts during bone remodeling and offer information about bone physiology and patient’s response to various osteoporosis therapies.14,15 According to the consensus and based on the recent publications elaborated by the IOF and International Federation of Clinical Chemistry and Laboratory Medicine (IFCC), the current recommended reference BTMs for evaluating bone health are serum PINP (procollagen type I N propeptide), as bone formation marker and s-CTX (serum C-terminal telopeptide of type I collagen), as a bone resorption marker.16 BTMs can be enrolled in two major categories:17
- Bone resorption markers, wherein the collagen degradation markers dominate, like deoxypyridinoline (DPD), pyridinoline, (PYD), amino-terminal cross-linking telopeptide of type I collagen (NTX) and carboxy-terminal cross-linking telopeptide of type I collagen (CTX). Amongst the enzymes that regulate the bone formation, tartrate-resistant acid phosphatase (TRACP) possesses a marker role in bone turnover.
- Bone formation markers, wherein various matrix proteins, like osteocalcin (OC), procollagen type I C propeptide (PICP) and PINP are included. Enzymes, like alkaline phosphatase (ALP) and bone-specific alkaline phosphatase (BALP), might as well be considered as biomarkers of bone formation.
CTX-I is a metabolic remnant of type I collagen, being released under cathepsin K cleavage of intact bone collagen.18 Serum levels of CTX-I present a circadian variation and are slightly affected by various conditions (eg gender, age, menopausal status) with a maximum being observed at 05:00 in the morning and an afternoon minimum at 14:00.19
Adolescent boys achieving higher peak bone mass show significantly higher levels of OC, BALP and serum CTX-I (s-CTX-I) than age-matched girls.20 A recent study performed on 205 Vietnamese men and 432 women highlighted an interesting switch in age/gender dependency of the β-isomerized form of CTX-I along PINP, which were more increased in <50–year-old men and in >50–year-old women than in their age-matched gender counterparts.21
Currently, several working groups are implied in the bio-analytical validation of these molecules aiming to standardize methods for the use of CTX-I and PINP as BTMs.22–25 Szulc et al24 recently have elaborated a paper focusing on the pre-analytical variability of CTX-I and PINP measurements. These variables include both controllable (circadian variation, food intake, and lifestyle factors) and uncontrollable factors (age, gender, etc.), accelerator conditions of bone turnover (hyperparathyroidism, immobility), or diseases lowering (hypothyroidism), or dissociating (rheumatoid arthritis, multiple myeloma) bone turnover. According to the formulated recommendations based on the extensive literature review, the determination of BTMs should be carried out concerning their circadian rhythm and taking into consideration the variability of the uncontrollable aspects.
Complementary or Contradictory Clinical Aspects of BTMs in Osteoporosis?
Currently, the diagnosis of osteoporosis is generally made using DXA investigations. For bone turnover assessment the gold standard technique is the analysis of bone histomorphometry and BTMs are often measured as auxiliary or complementary diagnostic information.26 In a large cohort study realized by Chavassieux et al27 on 370 patients with postmenopausal women, concluded that there is only a weak correlation between bone formation (PINP and BALP), bone resorption (s-CTX-I) BTMs and corresponding bone histomorphometry results. Although, this correlation pitfall might be due to the different data carrying of BTMs vs bone histomorphometry. Whereas BTMs show the metabolic shifts and turnover of the whole skeleton, bone histomorphometry offers a precise assessment of one part of the investigated bone site and due to this limitation, bone histomorphometry cannot serve as an indicator of the integrity of the whole skeleton. Park et al28 have evaluated bone turnover in the postmenopausal period (PMOP) of Korean women by assessing s-CTX-I, serum OC, urinary DPD and BMD. Amongst the quantified BTMs only s-CTX-I showed a statistically greater level in the group of osteoporosis patients (0–6 years of onset) when compared to the non-osteoporosis group and this tendency was similar up to 10 years of PMOP. In a review article, Krege et al29 summarized the clinical significance of osteoblast-derived protein PINP, in patients receiving anabolic therapy with teriparatide. PINP showed a significant increase as soon as 3 months after therapy initiation, showing good correlation with the bone histomorphometric parameters. In this view, BTMs might have prognostic potential in the evaluation of osteoporosis, but a synchronous measurement of BTMs and BMD is deemed for a proper evaluation of PMOP.
Besides the well-established BTMs by IOF and IFCC, recent publications aim to compare the levels of circulating pro- and anti-resorptive cytokines in impaired bone metabolism. Azizieh et al30 evaluated the circulatory levels of selected cytokines (pro-resorptive: TNFα – tumor necrosis factor, IL-1β, IL-6, IL-8, IL-12, IL-17 and anti-resorptive: IFN-γ – interferon, IL-4, IL-10, IL-13, TGF-β – transforming growth factor beta), adipokines (eg adiponectin), BTMs (PINP, CTX) in postmenopausal women with normal and low BMD. Although, the CTX-I levels did not indicate a significant change in serum concentration levels, PINP and PINP/CTX ratio were significantly lower in patients with low BMD compared to the normal BMD PMOP patients. The patterns of the circulatory cytokine network remained similar between groups, except for TGF-β, which was significantly greater in patients with osteopenia, compared to the osteoporosis group.
BTMs and Their Clinical Significance Under Osteoporosis Treatment
Pharmacologic medication in osteoporosis aims the diminution of fracture risk in patients suffering from impaired bone formation. As a classification the therapeutic possibilities can be divided into two major groups: a) antiresorptive drugs – bisphosphonates, selective estrogen receptor modulators, receptor activator of nuclear factor κB (RANK) inhibitors, calcitonin, calcium, vitamin D, and phytoestrogens; b) bone remodeling drug – strontium ranelate as a dual-acting bone agent, and parathormone and Wnt signaling inhibitors as anabolic agents.31,32
The variations in BTMs under pharmacologic anti-osteoporotic intervention has been evaluated since the last decades of the past millennium. In an early study published by Bettica et al33 a rapid and significant reduction of bone-remodeling markers (CTX, NTX, DPD) was shown under alendronate and etidronate treatment, reaching a reduction plateau around 2–4 weeks after the beginning of the treatment. OC and BALP also presented reduced levels, at 56 and 84 days, respectively. The study included 74 women with PMOP, being divided into four subgroups with the following treatment allocated: calcium carbonate (50 mg/day), alendronate in 5 mg/day and 10 mg/day dosage, and cyclical etidronate. In a pilot study on ibandronate, serum and urinary CTX-I (u-CTX-I) levels were evaluated under medication of 50, 100, 150 mg of ibandronate administrated monthly to PMOP women. The results presented by Reginster et al34 showed an effectively decreased bone turnover for both s-CTX-I and u-CTX-I in a dose-response dependent manner. A similar study conducted by Binkley et al35 enrolled 67 women patients of which 47 received anti-resorptive medication, 150 mg ibandronate monthly. The measurements of s-CTX-I showed a marked reduction after 3 days of therapy initiation and remained suppressed over six months, showing a regular monthly fluctuation. Similar long-term inhibitory effects of bisphosphonates on BTMs were described in a prospective study by Borba et al.36 In their study, patients receiving a single dose of 4 mg of injectable zoledronic acid presented under baseline levels of both CTX-I and BALP even after 18 months of follow-up. Concurrently with these findings, after 18 months gain in BMD was also observed.
Serum markers of bone turnover, namely BALP and s-CTX were measured by Kaufman et al37 in men with primary osteoporosis. Patients received 2 g/day strontium ranelate for two years and both BALP and s-CTX were assessed at 3, 6, 9, 12, 18 and 24 months. s-CTX levels were significantly reduced in the strontium ranelate treated group in comparison to placebo peers throughout the testing period. In a large cohort study published by Bruyère et al38 and including 2373 women the bone resorption marker s-CTX was decreased by 5.9%, whereas BALP and PICP, as bone-forming markers were elevated by 9.6% and 9.9%, respectively. Moreover, an association between the BTMs and BMD was found, indicating the clinical importance of these soluble markers along with BMD measurements for the monitoring of strontium ranelate therapy.
Clinical effects of 2 g/day strontium ranelate (SrR) vs 70 mg/week alendronate therapy were evaluated and compared by Rizzoli et al,39 enrolling Caucasian PMOP women in a randomized 2-year-long trial. Medical treatment was supplemented with a daily intake of 500 mg calcium and 400 IU of vitamin D. s-CTX levels were significantly reduced, while BALP levels presented a significant increase after 3 and 18 months of treatment with SrR, respectively, compared to placebo. This tendency was not characteristic for alendronate, as BALP levels remained under borderline throughout the testing period.
Predictive Roles of BTMs in Osteoporosis-Related Pathologies
Obesity is one of the increasing global epidemic concerns, alarmingly affecting the younger population.40 Although conventionally considered as a promoter of bone formation through a greater mechanical loading of bone, obesity is unquestionably a prominent risk factor for various chronic diseases.41 In this perspective, the increased mass of adipose tissue, as an outcome of adipocyte-directional differentiation of mesenchymal stem cells, may result in an adipocyte loading of skeletal tissue cavities, instead of trabecular bone formation. Complementarily, low grade inflammation related to obesity promotes adipogenesis in the detriment of osteoblastogenesis and calcium absorption, increasing the risk of fractures and osteoporosis.42–44 In a study presented by Ambroszkiewicz et al45 higher CTX-I levels indicated a defective bone formation in thin children, compared to normal-weight peers. Moreover, the ratio of the carboxylated OC/undercarboxylated OC, as well as the BMD were significantly lower in thin children when compared to the normal-weight group.
A meta-analysis published (2016) by Starup-Linde et al46 summarizes the contradictory information that BTMs provide in diabetic (DM) patients. Comparing and stratifying the BTM levels in type I diabetes mellitus (T1DM) and type II diabetes mellitus (T2DM) it has been outlined that OC levels decrease in T1DM, but show only a borderline decline in T2DM. Further studies included have also pointed out the conflicting evidence regarding BTMs in DM. Pater et al47 found that both OC and CTX-I levels were decreased at the onset of T1DM in children, and after 3 months returned to their normal levels. TRACP5b showed a gradual increase in 12 months, becoming significantly higher at this time point when compared to the onset of T1DM. Other studies have found that besides CTX, OC, P1NP, TRACP also showed a decrease in T2DM, along with sclerostin, PTH and BALP.46,48 In a recent study, Liu et al49 presented an association between s-CTX and dysglycaemia. They proposed that bone, as an endocrine organ might contribute to glucose homeostasis, by increasing osteoclast activity in the early stages of DM, thus exhausting the bone metabolism, which results in impaired osteoclast activity, resulting in disturbances in both bone and glucose homeostasis. The former observation might be due to the formation of glycated s-CTX, as an advanced glycated end product. As both glycated s-CTX, and non-glycated s-CTX, derive from type I collagen, the assumption that the glycated s-CTX is already present in diabetic patients promotes glycated s-CTX to a promising BTM.
Wnts and Wnt-Pathway Related Molecules as Putative Future Biomarkers of Bone Metabolism?
Amongst the broad intracellular and intercellular molecular pathways, which regulate bone metabolism, Wnt signaling occupies a prominent spot in the nebulous world of these communication systems. In recent years, emerging evidence has been reported describing the crucial roles of Wnt proteins in bone homeostasis. In a review published by Canalis E,50 the altered biological activity of Wnt1 due to WNT1 mutations has been summarized. These impaired biological events are responsible for the early onset of an autosomal recessive form of osteogenesis imperfecta, leading to osteoporosis in children. Supportive evidence was disclosed by Mäkitie et al51 having found that skeletal changes and impaired bone mass due to mutations in WNT1, affecting Wnt1 protein activity can be observed even from the pubertal years. Recent studies categorize Wnt1 as a bone-anabolic Wnt ligand. The data presented by Luther et al52 characterized Wnt1 as a major bone-anabolic juxtacrine mediator of the osteoblastic lineage.
Non-canonical Wnt modulators also have noticeable effects on the metabolic equilibrium of the osseous tissue. Okamoto et al53 followed the mechanism of osteoblastogenesis in Wnt5a− deficient mice. Their findings indicate that Wnt5a-deficient signaling is strongly correlated with impaired bone formation and concurrent adipocyte differentiation. They also investigated the effect of exogenous Wnt5 on the Wnt5a− rodent calvarial cells. Interestingly, Wnt5a increased the expression of LRP5/6 (lipoprotein receptor-related proteins), indicating that Wnt5a does not grant the activation of Wnt/β-catenin signaling to a direct activation, but more likely by enhanced expression of the receptors involved in the activation of the canonical β-catenin pathway.
Recent studies bring further insights into the potential biomarker role of Wnt signaling related molecules. Endogenous Wnt signaling inhibitors such as Sclerostin (WISE, SOST) and Dickkopfs (DKKs) have been in the limelight of contemporary research advances. Numerous studies focusing on sclerostin has been reviewed by Garnero et al,54 having shown that serum sclerostin levels are increased in patients with a high risk of osteoporosis. Tian et al55 found a significant increase in serum DKK-1 levels in patients with postmenopausal osteoporosis in comparison with the age-paired control group. Intriguing insights into bone remodeling processes during osteoporosis have been disclosed by Ueland et al.56 According to their findings, both sclerostin and DKK-1 are incorporated in the bone mass under normal Wnt signaling; during menopausal imbalance, these proteins are unsynchronized released in the bone matrix further promoting bone resorption. Corrado et al57 described increased secretion of DKK-1 from primary human osteoblasts compared to the healthy, in contrast with osteoarthritic osteoblasts. In severe osteoporosis related to spinal cord injury, DKK-1 was not associated with bone mineral content or density.58 However, in a 4-year follow-up study, performed on 238 geriatric patients, DKK-1 proved to be a strong predictor of mortality at patients experiencing hip fracture.59
Currently available biomarkers of osteoporosis are shown on Figure 1 and their potential applications are encountered in Table 1.
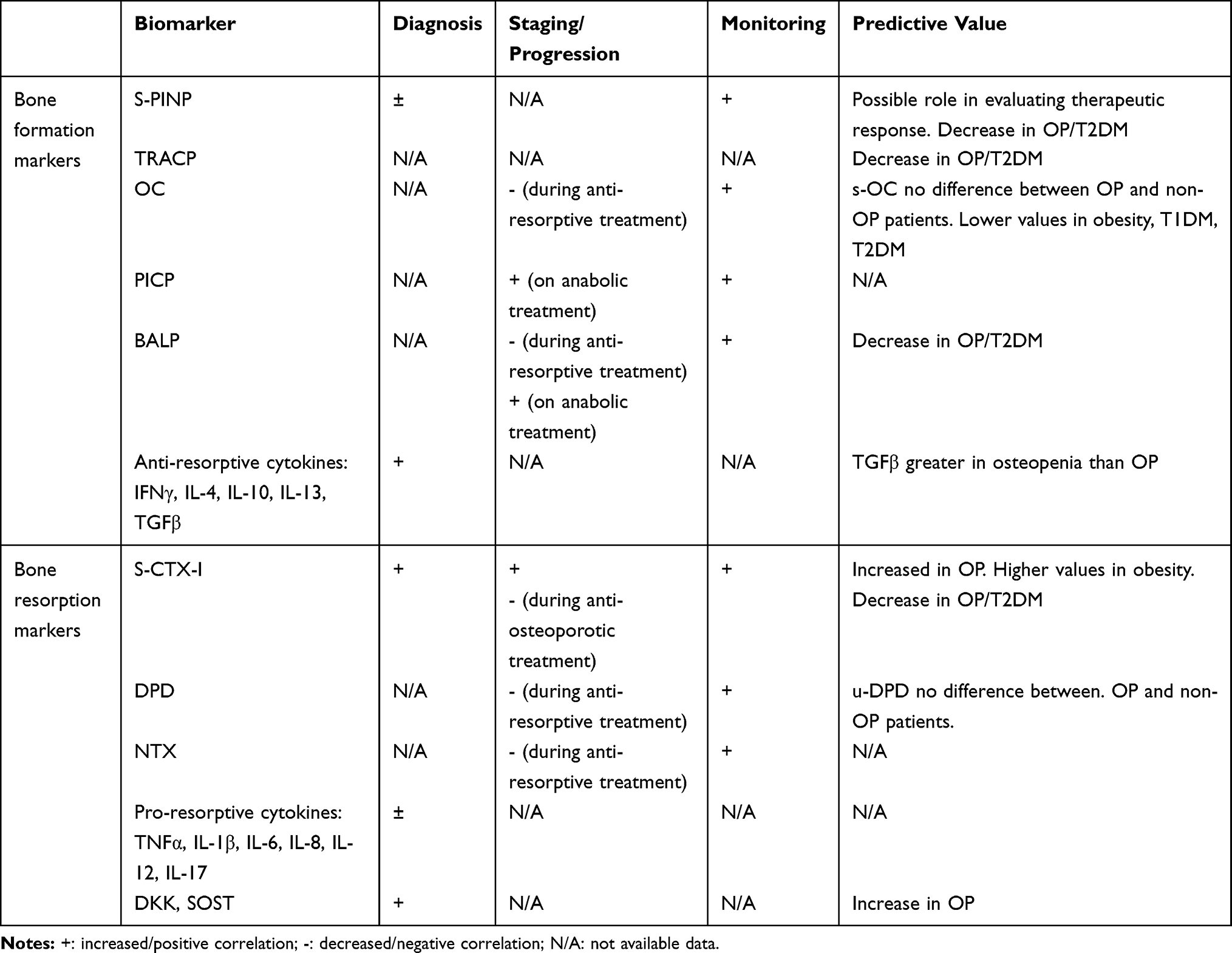 |
Table 1 Currently Available Data on Osteoporosis Serum Biomarkers and Their Applicability in the Diagnosis, Progression and Monitoring of Osteoporosis |
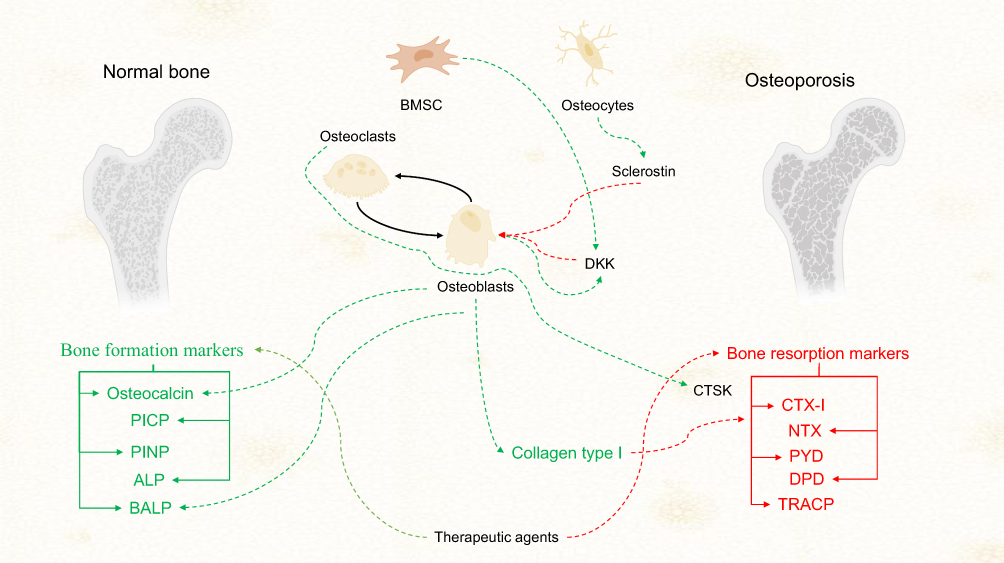 |
Figure 1 Metabolic imbalance is the source of biomarkers in osteoporosis In osteoporosis, a balanced activity between osteoblasts and osteoclasts is of utmost importance. An imbalance between the bone-forming and disturbing activities on the hand of the latter results in altered bone formation and eventually osteoporosis. Bone turnover biomarkers are promising candidates to monitor these molecular changes in this microcosm. Collagen type I produced by osteoblasts is of key importance in bone integrity and homeostasis. Under proteolytic activity promoted by osteoclast derived CTSK, collagen type I is degraded into several remnants, like CTX-I, NTX, PYD, and DPD. These collagen degradation products are candidate molecules for laboratory diagnosis of osteoporosis from biological fluids (patients’ sera and urine), CTX-I being currently the most widely accepted BTM for this clinical purposes. On the other hand, procollagens and osteocalcin are key participants in bone metabolism. According to the current guidelines PINP is considered the clinical counterpart of CTX-I, as a BTM of osteoporosis. Wnt signal molecules have a cardinal role in the interplay of cellular participants in bone tissues. Osteocyte derived sclerostin and DKKs secreted by BMSCs and osteoblasts, as inhibitors of the Wnt pathways and subsequently bone formation are two nominee molecules for future perspectives. Arrows in green represent activation or secretory mechanisms. Arrows in red indicate inhibition or degradation mechanisms. Abbreviations: DPD, deoxypyridinoline; PYD, pyridinoline; NTX, amino-terminal cross-linking telopeptide of type I collagen; CTSK, cathepsin K; CTX, carboxy-terminal cross-linking telopeptide of type I collagen; TRACP, tartrate-resistant acid phosphatase; OC, osteocalcin ; PICP, procollagen type I C propeptide; PINP, procollagen type I N propeptide ; ALP, alkaline phosphatase; BALP, bone-specific alkaline phosphatase. |
Trends and Limitations for Biomarker Research in Osteoarthritis
Osteoarthritis (OA) is the most common chronic musculoskeletal disorder, with complex and yet incompletely known etiopathogenic pathways. According to the white paper of OARSI, an estimated 242 million people live with symptomatic OA of the hip or knee.60 Clinically it appears with articular pain, stiffness which then progresses to deformities and altered quality of life. At the tissue level, progressive deterioration and low-grade inflammation of the cartilage, synovitis with inflammatory cell infiltration and subchondral bone remodeling are the most characteristic changes.61 There are many candidate diagnostic, monitoring and prognostic biomarkers that were reported to have relationships with the mainstream pathogenic processes of OA.62 At their individual level, these markers show variable sensitivity and specificity. This is the reason for which in the past years more effort has been taken to apply complex analytical approaches to enlarge the panel of discoveries. Proteomic studies were initiated to explore the sera, synovial fluid, the cartilage and chondrocyte secretome of OA patients, for a better understanding of disease mechanisms and definition of diagnostic and prognostic biomarker panels.63,64 Clinical OA biomarker studies, in general, suffer from a lack of proper experimental design, generating insufficient data to achieve adequate statistical power at the individual stages of the biomarker pipeline.2 In the proteomic approach, a consensus is needed to set statistical criteria for clinical relevance and to calculate the appropriate sample size. In the past two decades, for the coverage of the pathway streamline of OA, biochemical markers of the entire joint, including bone turnover – CTX-I, PINP, OC –, cartilage turnover – C2M (MMP-derived degradation of type II collagen), PIIANP (serum N-propeptide of collagen IIA), and COMP (cartilage oligomeric matrix protein) –, inflammation – a hsCRP (high sensitive C-reactive protein), IL-6 –, and connective tissue biochemical turnover – C3M (MMP-derived degradation of type III collagen), C1M (MMP-derived degradation of type I collagen), ICTP (serum cross-linking C-terminal telopeptide), and matrix metalloproteinase (MMP) 9 –, as well as bone-related Wnt signaling antagonists – sclerostin and DKK-1 – were analyzed in diverse studies.65
Genetic screening also can help in the identification of differentially expressed members of the chondrocyte, synovial cell or osteoblast transcriptome in various clinical stages of the disease.
In a recent study, Soul et al66 described 2980 differentially expressed genes in OA versus non-OA individuals, and additional 2122 distinctive genes when patients were divided into groups according to disease activity. The first patient group showed up-regulated chemokine signaling, inflammasome activity, Toll-receptor activation along with changes in glycosaminoglycan synthesis, presenting also increased expression of collagen type II, V, IX, XI, but decreased expression of collagen type I. The second group had characteristic changes in complement cascade regulation, Wnt system and eicosanoid receptor signaling, and pericellular matrix interactions, with reduced expression of Sox-9, SIRT-1, collagen type IX, and higher expression of collagen type I, VI, laminin, perlecan, and RUNX2 (runt-related transcription factor). Out of these factors, 478 differentially expressed proteins were secreted in the synovial fluid. These are important findings that may guide many future studies in the research endeavor.
Proinflammatory Cytokines and Chemokines
OA is characterized by low-grade inflammation of the cartilage, subchondral bone marrow, and cartilage-bone transition zone. CD86+/iNOS+ (inducible nitric oxide synthase) M1-type macrophages and a subset of osteoblasts are important sources of pro-inflammatory cytokines in the joint tissue.67,68 We demonstrated in an experimental model, that cyclooxygenase-2 expression is detectable at the bone-cartilage interface, in subchondral bone and bone marrow, but is abolished by long-term meloxicam treatment.69
Many results support the important pathogenic role of several proinflammatory cytokines, especially IL-1β and TNFα, but also IL-6, IL-15, IL-17 in the progressive degeneration of the cartilage.70 However, clinical studies could not reveal an unambiguous biomarker role for the majority of these factors. Imamura et al71 found in 53 female patients, aged 71±7 years, significant elevations of IL-6 and IL-10, but not IL-8 or TNFα. Radojcic et al72 described that synovial IL-6, but not plasma IL-6, are associated with magnetic resonance imaging signs of parapatellar synovitis, pain and the WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) score. A nutrition study highlighted that on 99, mainly female volunteers aged 31–90 a 16 weeks Mediterranean type diet decreases serum IL-1β with 47%, and serum COMP with 8%.73 Shan et al measured higher serum levels of proinflammatory cytokines IL-21, IL-17A and IFN-γ at 40 individuals recently diagnosed with OA.74
In animal models, synovial levels of pro-inflammatory cytokines can be used to monitor moderate physical activity.75 Oxidative stress is an important trigger in the pathogenesis of OA; age-related NADPH oxidase, an enzyme involved in reactive oxygen species neutralization, presents increased activity in advanced-stage OA.76 HIF-1α (hypoxia inducible factor), a transcription factor induced in hypoxic chondrocytes is present in about four-fold levels in the synovial fluid of OA patients. In the study of Chu et al,77 performed on 278 patients and 203 controls, HIF-1α slightly increased in parallel with the Kellgren-Lawrence score (K-L). However, it seems that HIF-1α has mainly protective actions inducing Sox-9, and, HIF-2α is responsible for the up-regulation of the pro-inflammatory environment in the joint.78
A chemokine promoting macrophage migration, CCL3 (Chemokine C-C motif ligand 3) was proposed to be used as a marker of early cartilage degeneration. In the study of Zhao et al,79 this reached a sensitivity of 70% with a specificity of 96% in distinguishing pre-X ray defined knee degeneration patients (with alterations diagnosed with magnetic resonance imaging or arthroscopy) from controls. It is to mention that there was a significant difference in the two groups’ age (early OA: n=47, 29 ±8 years, controls n=75, 43 ± years), however, plasma CCL3 could distinguish also between the K-L I–IV groups of X-ray defined knee OA patients (n=50, age 61 ± 13 years). TGF-β, an anti-inflammatory and pro-regenerative cytokine, proved a modest efficiency for the diagnosis of OA in the study of He et al80 on 160 knee OA cases compared to 80 healthy controls (aged 66 ± 10 and 66 ± 8 years, respectively). Serum levels of the molecule were associated with the K-L scores, qualifying TGF-β a putative biomarker of established OA severity. Adropin, a 76-aminoacid small protein, coded by the energy-homeostasis related gene (Enho), regulates energy status and storage and body mass. OA patients have significantly lower levels of adropin compared to healthy controls even in the lowest K-L grade 1 and significant differences between the highest grade 4 versus the other grades. Adropin correlates negatively with serum TNFα and the body mass index (BMI).81
Collagen Type II Degradation Products and COMP as Biomarkers of OA
Loss of proteoglycan matrix and type II collagen are hallmarks of the osteoarthritic cartilage. Carboxy-terminal cross-linking telopeptide of type II collagen (CTX-II) is released in circulation due to the activity of Cathepsin B, MMP-1,-3,-7,-9,-13 and is filtrated in urine.82
Exploring 615 healthy men and women, aged 20–87 years, Mouritzen et al83 stated that urinary CTX-II (u-CTX-II) depends on gender, age, body-mass-index, it is higher in postmenopausal women than in their age-matched premenopausal counterparts and is suppressed by hormone replacement therapy. Bihlet et al84 confirmed the gender dependency, reporting significantly elevated u-CTX-II values (along with u-CTX-I and OC) especially in women with bilateral OA and high K-L scores of 2/4 or 3/4. Reijman et al85 performed a large-scale investigation on 1235 men and women enrolled in the Rotterdam Study, aged ≥55 years and proved that u-CTX-II in the highest quartile confers a 4.2-fold risk for the presence of knee/hip OA, a 6.0-fold risk for knee OA progression, and an 8.4-fold risk for hip OA progression. Lehman and colleagues86 reported that high-dose anti-resorptive treatment (at least 3 years with 20 mg alendronate, or at least 1 year with 2.5–5 mg ibandronate) decreases u-CTX-II with about 50%, and this down-regulation is maintained even 1–3 years after cessation of pharmacotherapy.
It was suggested that CTX-II levels reflect spinal vertebral radiological findings and BMD, which are possibly related also to the bone turnover in men with ankylosing spondylitis.87 However, Catterall et al88 proved that CTX-II is not released when bone tissue is treated with cathepsin K, MMPs or activated osteoclasts. In the Genetics, Arthrosis, and Progression (GARP) Study, in 302 sibling pairs suffering from multiplex OA, Meulenbelt et al89 found that u-CTX-II was related to the radiological signs of the knees, hips, hands, and vertebral joints. CTX-II detection is possible not only in the urine but also in serum by various methods, like enzyme immunoassays or fluorescent beads-based chip techniques.90 In a chemically generated rat OA model, we observed that s-CTX-II is suppressed significantly by meloxicam treatment even 4 weeks after stopping the therapy.91 Luo et al argue for the non-comparable value of the two markers: examining 227 participants of the C4Pain Study they observed that only u-CTX-II could be significantly correlated to the WOMAC scores.92 Also, the group of Luo elaborated an electrochemiluminescent immunoassay named hs-PROC2 that measures the splice-variant of the N-terminal propeptide of collagen type II (PIIBNP). This fragment indicates the intensity of collagen synthesis, increases upon growth-factor triggering of human cartilage explants, and was significantly higher in K-L score 0–1 patients than in advanced disease.93
Another collagen II degradation product is Coll2-1 (108HRGYPGLDG116), located in the triple helix of the molecule. In 60 OA patients aged 62–67 years, this marker showed the difference between K-L grade <3 and K-L grade ≥3 patients, being reduced along with the improvement of the WOMAC score of patients receiving a single intra-articular platelet-rich plasma injection.94
C2M is a degradation product of collagen type II, with the sequence RDGAAG released from position 1053.95 Helix-II, another type II collagen fragment is measurable from synovial fluid and was reported to show good correlations with the severely damaged cartilage and also elevated in early OA disease but without the relevance for disease staging.96
COMP is an extracellular matrix protein with five identical glycoprotein subunits, that binds to collagens and is a reliable marker of cartilage turnover; Verma et al96 in a case-control study conducted on 100 OA patients described more than a three-fold elevation of this molecule compared to controls. COMP serum concentrations were negatively correlated with disease duration, and positively associated with age, physical and sports activities.96,97 Bai et al98 induced OA in rabbits by anterior crucial ligament transsection and monitored the evolution of s-CTX-II and COMP at baseline and weeks 2, 4, 6, 8, 10, and 12 after the intervention. The CTX-II and COMP concentrations increased gradually to week 12, in parallel with the disease severity index Mankin score. Histological findings confirmed a slow, but progressive cartilage deterioration.98,99 In such a design, the CTX-II/COMP combination may be a marker for early diagnosis, evolution, and disease severity. In the study of Riegger et al,100 conducted on 754 subjects who underwent total joint replacement, serum COMP levels positively correlated with markers of renal (cystatin C, creatinine, estimated glomerular filtration rate-eGFR) and cardiac (N-terminal propeptide of brain natriuretic peptide) function. After adjustment for eGFR, COMP levels were still associated with WOMAC scale and sub-scales, 6 months after surgery.
Matrix Metalloproteinases, Other Collagen Degradation Products, and Biomarker Combinations
MMP-13 is by far the most investigated metalloproteinase in cartilage pathology.101 Ruan et al102 performed a cross-sectional study on 149 subjects with established OA. They found that serum MMP-13 was negatively correlated with cartilage volume, but positively associated with infrapatellar fat pad MRI signal alternation, and K-L radiological grades. Moreover, MMP-13 showed significant positive correlations with pro-inflammatory cytokines IL-1β, IL-18, and TNFα along with an inverse relationship with adiponectin. Synovial MMP-3 levels were higher in operated knee joints of 22 OA patients than in their contralateral knee, even with decades after meniscectomy, and correlated with the radiographic scores, predicting life quality in a regression model, together with glycosaminoglycan levels. Serum MMP-3 correlated significantly with synovial MMP-3 of the operated knee, thus it had been proposed as a surrogate marker for diagnosis and staging of OA.103
Collagen type II is the most abundant species in cartilage, but collagen type I and III are also present in the subchondral bone and synovial membrane. Dedifferentiated chondrocytes also produce collagen I and III.104 Metalloproteinases generate neoepitopes by the degradation of collagen I, II and III. MMP-2,-9 and −13 form the fragment C1M from the mature collagen type I with the sequence GSPGKDGVRG.105 C3M is a 12-mer peptide (GGPGQPGTEGNK), cleaved by MMP-9 from mature collagen type III.106
The use of complex biomarker combinations proved to be useful in the prediction of surgical solutions. In a Phase III trial investigating the need for total joint replacement in OA patients treated with anti-nerve growth factor, tanezumab, Arends et al107 identified combinations of biomarkers which could predict with 77% certainty total joint replacement, in the six months of follow-up. Their combinations comprised molecules reflecting cartilage and bone turnover, inflammatory mediators and effector MMPs, along with Wnt inhibitors DKK-1 and sclerostin. In the OA group naïve for NSAID-treatment, C3M, C2M, the CTX-I/OC I ratio, PIIANP, hsCRP, and IL-6 treatment were predictive. In patients receiving NSAIDs only in the screening period, classification by IL-6 level proved to be useful, in combination with COMP, C3M, and ICTP. In those who were treated with NSAIDs throughout the study, six markers: C3M, PIIANP, COMP, MMP-9, the CTX-I/OC ratio, and DKK-1 could be applied.
In a large-scale meta-analysis, Valdes et al108 compared CTX-II, COMP, and C2M at 3582 participants of the Rotterdam, GARP, Chingford, and TwinsUK studies. COMP was associated with hip and knee OA incidence, C2M predicted knee OA incidence and progression; CTX-II proved to be the most versatile as it predicted the risk for hand, knee, hip OA, and indicated incidence along with progression. Collagen X overexpression indicates altered chondrocyte metabolism and hypertrophy; He et al measured the degradation products of collagen type X and found that OA patients with K-L scores ≥ 2have significantly higher levels of the molecule. He et al109 also performed investigations on patients of the C4pain Study (n=253), and a cohort of the NYU OA Progression Study (n=146) and found that a cathepsin K-generated fragment of collagen type X, Col10neo, measured from urine is significantly higher in the OA group than in controls and RA subjects, and it is associated to the K-L scores.
MicroRNA as OA Biomarkers
MicroRNA (miR) may be regulatory from secreted exosomes or microvesicles. Profiling the exosome cargo will help to highlight the role of this micro-compartment.110
miR expression profile varies in different forms of OA. In the study of Wan et al,111 miR-136, an effector of IL-17 degradation, proved to be negatively correlated to circulating IL-17 levels and disease severity. Zeng et al112 reported characteristically elevated miR-98 plasma levels, along with collagen type III degradation product CTX-III (20 patients vs 20 controls). Li et al99 described several sets of mRNA and miR differentially regulated in arthritic mice joint samples. Among these, there were mRNAs of chemokine CCL2 (Chemokine C-C motif ligand 2), responsible for the attraction of inflammatory cells, arginase 1, an enzyme characteristic for M2-type macrophages, miR-7, miR-150, and miR200b. In a six-week follow-up study of Celecoxib treatment, Dong et al113 showed ten down-regulated miR species: miR-675-5p, miR-126-5p, miR-155-5p, miR-320a, miR-210, miR-3197, miR-17-3p, miR-146a-5p, miR-4796, and miR-92a-3p. Among these miR-155-5p is known to trigger the key pro-inflammatory cytokines IL-1β, IL-6, IL-8, and TNFα.
Other Degradation Products of the Extracellular Matrix
Fibulin-3 is an extracellular matrix protein controlling the differentiation of chondrocytes and inhibits angiogenesis. In an experimental rat grove model, the Fibulin-3-3 peptide increased about 30% in sera of animals with cartilage damage induced on a high-fat diet background.114 In a 30 months duration human survey, Fibulin-3 degradation peptides proved to prognostic for OA on 241 women with slightly elevated BMI, initially free of disease.115
De Seny et al116 analyzed 284 serum samples from knee OA cases of the Bristol OA 500 cohort and the Bristol Validation Study with K-L scores 0–4, along with healthy controls and rheumatoid arthritis patients. Applying the SELDI-TOF MS proteomics approach, they identified four novel biomarkers in sera of OA patients: V65, C3f, the 3762 protein, and CTAPIII (Connective tissue-activating peptide III). The C-terminal end-product of vitronectin, V65, showed elevated levels in MS spectra in all K-L grades, but not in controls or rheumatoid arthritis cases. These findings emphasize its specificity for OA. Moreover, V65 correlated positively with CTX-II, an established marker of cartilage degradation. Vitronectin is a ligand for the αVβ3 integrin receptor, being degraded by several metalloproteinases, like MMP-1,-2,-3,-7 and −9.117 Vitronectin is a cell-adhesion and spreading factor, and bone-resorbing osteoclasts intensely express αVβ3. The C3f peptide is highly expressed especially in advanced cases (K-L 3 and 4), it is present also in the synovial fluid, and it correlates significantly with V65. The strongly hydrophobic 3762 protein was also elevated only in OA subjects, and it correlated with MMP-3, PYD, and DPD levels. Meanwhile, CTAPIII found to be decreased in OA cases and especially in groups K-L 3 and 4 seemed to be produced outside of the joint since it cannot be detected in the synovial fluid.
Recently, two immunoassays have been built for the measurement of C3f and V65 from patients’ sera, but these yet lack the necessary diagnostic sensitivity for OA.118
Kraus et al119 selected 129 controls from 2722 African-American and Caucasian participants of the Foundation for the National Institutes of Health (FNIH) OA Biomarkers Consortium Project to determine the gender-based reference values for u-CTX-II, s-MMP-3, uNitrated type II collagen degradation fragment (uCol2-1 NO2) and hyaluronan and based on race for u-CTX-II, sCOMP, s-CTX-I and uCol2-1 NO2.
Wnt Signaling Molecules and Antagonists as Biomarkers of OA
The Wnt signaling system, at the basic level of activity, is homeostatic for the cartilage. However, its activation triggers hypertrophic degeneration of chondrocytes, MMP cleavage and loss of proteoglycan matrix. Some checkpoints of the Wnt signaling are promising therapeutic targets in OA.78 Weng et al120 studied in rats the component of a plant used in traditional Chinese medicine for the treatment of OA, called Achyranthes bidentata polysaccharides (ABPS) and demonstrated activation of Wnt/β catenin pathway, they also used Western blot for Wnt4, Frizzled 2, β catenin. ABPS seems to have beneficial effects in patients with OA by inducing proliferation of chondrocytes120 Cassuto et al followed proinflammatory cytokines, anabolic and catabolic pathways in patients following hip arthroplasty. They found increased levels of the anabolic molecules, including Wnt/β catenin, and transient and remodeling activities for Wnt inhibitor molecules (ex. DKK-1, sFRP – soluble Frizzled receptor related protein) - calling their action as “fine-tuning”.121
Theologis et al122 investigated the Wnt inhibitors DKK-1 and sclerostin levels both in serum and synovial fluid of 40 patients with knee OA, as well as 20 control patients, by correlating his result to the radiographic stage of the disease. He found that DKK-1 in synovial fluid was higher than in healthy subjects, and correlating especially with patients having grade 4 (K-L) OA. On the other hand, they did not find any significant difference between serum DKK-1, and neither serum or synovial fluid sclerostin and radiographic progression of the disease. In equine OA Mills et al123 found a higher DKK-1 level in low motion joint, but no significant difference was observed with radiographic progression.
A pioneering study by Lu et al124 evaluated DKK-1 and sclerostin serum levels in OA patients who had total joint arthroplasty (TJA). They measured the levels 1 day before the TJA, as well as 1, 3 and 5 days after the TJA. The results are surprising because there is an opposite change in the level of these molecules, namely DKK-1 shows an increasing trend after TJA reaching its maximum after 5 days post-operation, while sclerostin has a lowering trend, reaching its minimum after 3 days post-operation. The study team has no explanation for these results, requiring further studies for elucidating the exact molecular mechanisms. Huang et al125 reported recently that synovial fluid s-FRP and DKK-1 correlate negatively with the cartilage deterioration scores, synovial NO (nitric oxide) and IL-1β. In their study performed on 132 subjects, the synovial and the serum levels of these molecules showed similar trends of variability.
Even if the most researched molecule from the DKK family is DKK-1, many studies demonstrated the role of the non-canonical member, DKK-3, in OA, but there is no consensus on the exact role of this mediator. Snelling et al126 evaluated DKK-3 in human OA patients’ cartilage and synovial tissue sample, as well as cell culture, cartilage expats, hip avulsion from mice and synovial fluid sampling for expression, immunohistochemistry and ELISA detection of DKK-3. They found that DKK-3 is up-regulated in OA, but decreased during chondrogenesis, thus concluding that in vitro DKK-3 has a protective role from cartilage destruction.
Current or candidate biomarkers of OA, and their metabolic relevance are shown in Figure 2 and their potential applications are summarized in Table 2.
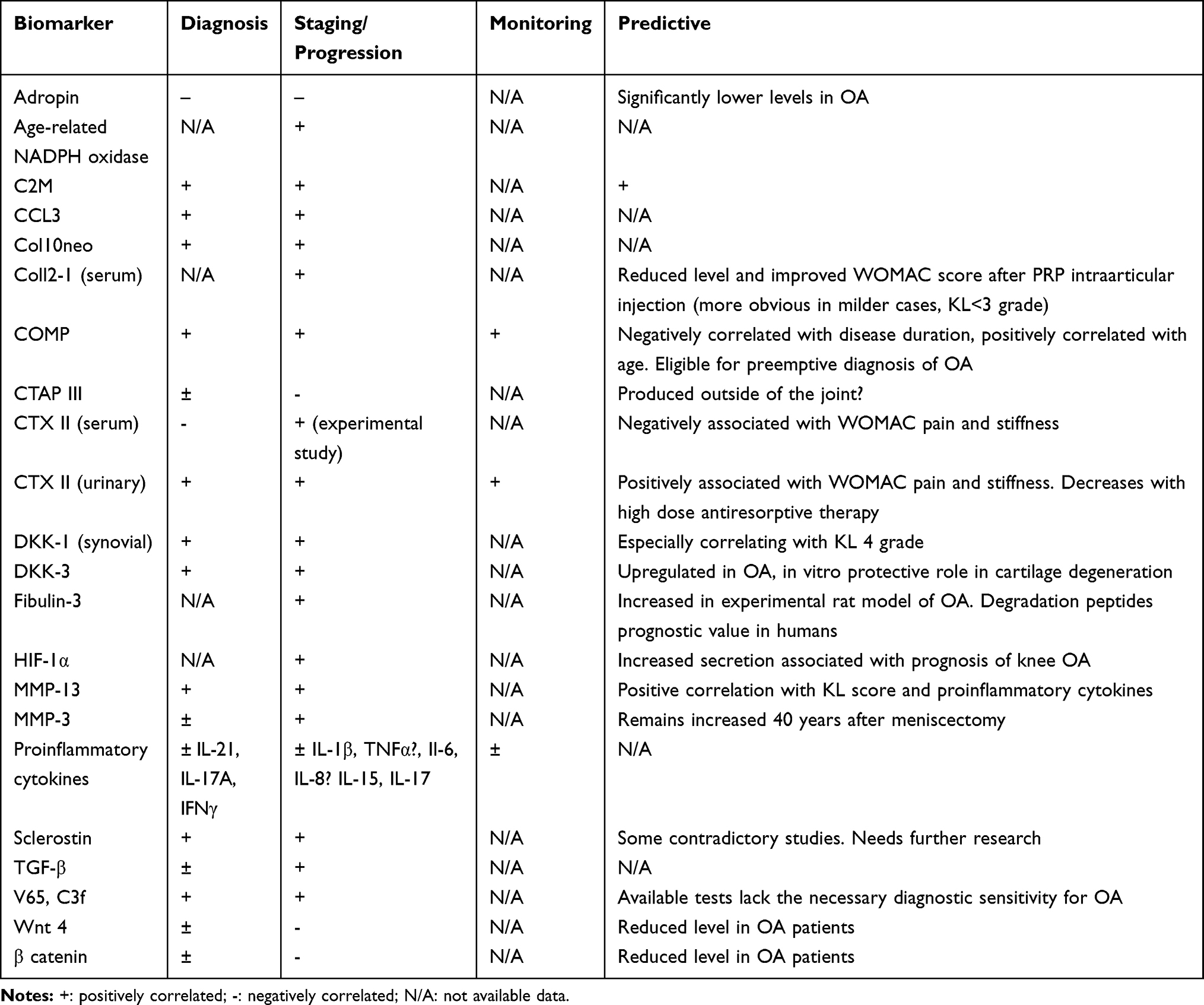 |
Table 2 Currently Available Evidence of Soluble Biomarkers for the Diagnosis, Staging and Monitoring of Osteoarthritis |
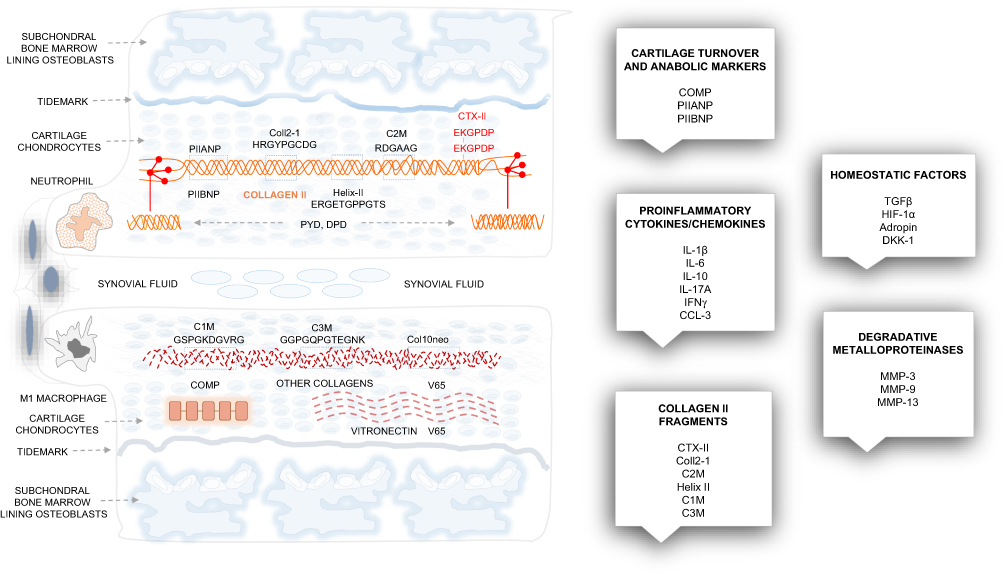 |
Figure 2 The basic structures of the cartilage, molecular sources and main groups of osteoarthritis biomarkers. Superficial and deep cartilage, synovial membrane and the subchondral bone marrow are all affected in osteoarthritis. Inflammatory cells invade the synovial membrane, the subchondral bone suffers intense remodeling, and the metabolic turnover of the extracellular matrix components is high. Collagen type II fragments: CTX-II, Coll2-1, Helix II, C2M are cleaved and released in the synovial fluid and the blood. Collagen I, III, vitronectin and proteoglycans are also excessively degraded, which results in the loss of matrix. The main groups of osteoarthritis biomarkers: cartilage turnover/anabolic markers, proinflammatory cytokines/chemokines, collagen II fragments, matrix metalloproteinases, and various homeostatic molecules are shown in boxes. Abbreviations: CTX-II, carboxy-terminal cross-linking telopeptide of type II collagen; Coll2-1, collagen type II degradation nonapeptide; C2M, collagen type II degradation hexapeptide. |
Conclusions
According to the IOF Datasheet, osteoporosis affects one in three women and one in five men over 50 years. Upon estimation, the incidence of the disease in Europe, India, Japan, and the US is about 125 million, and this number is quickly increasing due to the aging population and lifestyle change. The imbalance of bone remodeling in the favor of resorption is a hallmark of osteoporosis. IOF and IFCC recommend bone formation and bone resorption biomarkers for the evaluation of bone turnover. The bio-analytical validation of these markers in many cases is on ongoing process. For the bone turnover biomarkers, a desirable goal is to correlate with BMD results. Since the metabolic activity of bone synthesis and degradation is powerfully influenced by anti-resorptive or pro-anabolic therapies, these markers proved to be adequate in the evaluation of therapeutic efficiency. Currently, the most accepted anabolic marker PINP is suitable for monitoring teriparatide therapy. CTX-I, the C-terminal cross-linked telopeptide of collagen type I decreases in a dose-response manner during ibandronate administration and similar effects were seen with other bisphosphonates. CTX-I is also efficient in the evaluation of combined therapies, eg strontium ranelate, and bisphosphonates. Some members of the Wnt signaling family, like the pro-anabolic agonist Wnt1, are putative markers of bone formation, but yet do not have the necessary investigational background. Sclerostin and DKK-1 are Wnt inhibitors and promote bone catabolic processes, which are also candidates for osteoporosis diagnosis and monitoring.
OA is a complex disease with cartilage deterioration, low-grade inflammation, synovial infiltration of inflammatory cells and excessive subchondral bone remodeling. The global prevalence of the disease is almost 5%, presenting also an increasing rate. The application of biomarkers for diagnosis or monitoring treatment of OA is not so well established since the majority of studies were performed only on limited numbers of patients. Proinflammatory cytokines, with some exceptions, did not prove useful for diagnostic or prognostic purposes. Some molecules participating in the mainstream pathways of OA, like HIF-1α or CCL3 have been proposed as markers of chondrocyte homeostasis and early cartilage degeneration. CTX-II, the cross-linked telopeptide of collagen type II is formed due to cathepsin and metalloproteinase processing, and it is a parameter of cartilage turnover. CTX-II is suppressed by anti-inflammatory treatment; its urinary fraction being significantly associated with the WOMAC scores. The combination of CTX-II and COMP may be a marker of early diagnosis, evolution and disease severity. The cartilage degrading enzyme MMP-13 is a promising marker since negatively correlates with cartilage thickness, and positively with the K-L score. Complex combinations of biomarkers, among which collagen I, II, III neoepitopes, the CTX-I/OC ratio, PINP, COMP, IL-6, and other molecules were nominated are suitable to define patient subgroups who will undergo total joint replacement with 77% certainty. The vitronectin V65 degradation product and the C3f complement fragment are new candidates, which show elevated spectra in patients with high K-L scores, being present also in the synovial fluid. Wnt inhibitors, sclerostin and DKK-1 and DKK-3 presumably possess protective actions in the cartilage, but in the lack of sufficient data, there is no consensus concerning their use. Clinical studies with an appropriate design probably will validate new biomarkers and new applications in the near future.
Abbreviations
ABPS, Achyrantes bidentata polysaccharides; ALP, alkaline phosphatase; BALP, bone-specific alkaline phosphatase; BEST, Biomarkers, EndpointS, and other Tools Resource glossary; BMD, bone mineral density; BMI, body mass index; BTM, bone turnover marker; C1M, MMP-derived degradation of type I collagen; C2M, MMP-derived degradation of type II collagen; C3M, MMP-derived degradation of type III collagen; CCL2, Chemokine (C-C motif) ligand 2; CCL3, Chemokine (C-C motif) ligand 3; COMP, cartilage oligomeric matrix protein; CTAPIII, Connective tissue-activating peptide III; CTX-I, carboxy-terminal cross-linking telopeptide of type I collagen; CTX-II, carboxy-terminal cross-linking telopeptide of type II collagen; CTX-III, carboxy-terminal cross-linking telopeptide of type III collagen; DKK, dickkopf; DM, diabetes mellitus; DPD, deoxypyridinoline; DXA, dual X-ray absorptiometry; Enho, energy-homeostasis related gene; FNIH, Foundation for the National Institutes of Health; GARP, Genetics, Arthrosis, and Progression Study; HIF, hypoxia inducible factor; hsCRP, high-sensitive C-reactive protein; ICTP, serum cross-linking C-terminal telopeptide; IFCC, International Federation of Clinical Chemistry and Laboratory Medicine; IFN, interferon; IL, interleukin; iNOS, inducible nitric oxide synthase; IOF, International Osteoporosis Foundation; IU, international units; K-L, Kellgren-Lawrence score; LRP, lipoprotein receptor-related proteins; miR, microRNA; MMP, matrix metalloproteinase; NADPH, Nicotinamide adenine dinucleotide phosphate; NO, nitric oxide; NSAID, non-steroid anti-inflammatory drug; NTX, amino-terminal cross-linking telopeptide of type I collagen; OA, osteoarthritis; OARSI, Osteoarthritis Research Society International; OC, osteocalcin; PICP, procollagen type I C propeptide; PIIANP, serum N-propeptide of collagen IIA; PIIBNP, N-terminal propeptide of collagen type II; PINP, procollagen type I N propeptide; PMOP, postmenopausal period osteoporosis; PYD, pyridinoline; RANK, receptor activator of nuclear factor κB; RUNX, runt-related transcription factor; s-CTX-I, serum carboxy-terminal cross-linking telopeptide of type I collagen; sFRP, soluble Frizzled receptor related proteins; SIRT, sirutin; SOST, sclerostin gene; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; TGF, transforming growth factor; TJA, total joint arthroplasty; TNF, tumor necrosis factor; TRACP, tartrate-resistant acid phosphatase; uCol2-1 NO2 - urinary nitrated type II collagen degradation fragment; u-CTX-I, urinary carboxy-terminal cross-linking telopeptide of type I collagen; u-CTX-II, urinary C-terminal cross-linked telopeptide of type II collagen; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Funding
This research was partially funded by an external grant of the University of Pécs, Hungary, grant number 48101-1/2018.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Group F-NBW. BEST (Biomarkers, Endpoints, and Other Tools) Resource; 2016.
2. Kraus VB, Blanco FJ, Englund M, et al. OARSI clinical trials recommendations: soluble biomarker assessments in clinical trials in osteoarthritis. Osteoarthr Cartil. 2015;23(5):686–697. doi:10.1016/j.joca.2015.03.002
3. Micheel CM, Ball JR. Evaluation of biomarkers and surrogate endpoints in chronic disease. 2010. doi:10.17226/12869
4. Floyd E, McShane TM. Development and use of biomarkers in oncology drug development. Toxicol Pathol. 2004;32(SUPPL. 1):106–115. doi:10.1080/01926230490425021
5. Burch J, Rice S, Yang H, et al. Systematic review of the use of bone turnover markers for monitoring the response to osteoporosis treatment: the secondary prevention of fractures, and primary prevention of fractures in high-risk groups. Health Technol Assess (Rockv). 2014;18(11):1–180. doi:10.3310/hta18110
6. Zhou H, Lu SS, Dempster DW. Bone remodeling: cellular activities in bone. Osteoporosis in Men. 2010;15–24. doi:10.1016/B978-0-12-374602-3.00002-X
7. Mulder JE, Moreira Kulak CA, Shane E. Secondary osteoporosis. Dynam Bone Carti Metabol. 2006;717–737. doi:10.1016/B978-012088562-6/50044-3
8. Hendrickx G, Boudin E, Van Hul W. A look behind the scenes: the risk and pathogenesis of primary osteoporosis. Nat Rev Rheumatol. 2015;11(8):462–474. doi:10.1038/nrrheum.2015.48
9. Damjanov I. Bones and joints. Pathol Secrets. 2009;409–433. doi:10.1016/B978-0-323-05594-9.00020-9
10. Unnanuntana A, Gladnick BP, Donnelly E, Lane JM. The assessment of fracture risk. J Bone Jt Surg - Ser A. 2010;92(3):743–753. doi:10.2106/JBJS.I.00919
11. IOF. Osteoporosis - Facts and statistics. Available from: https://www.iofbonehealth.org/facts-statistics. Accessed December 12, 2019.
12. Kanis JA, Harvey NC, McCloskey E, et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos Int. 2019. doi:10.1007/s00198-019-05176-3
13. Kanis JA, Cooper C, Rizzoli R, Reginster JY. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019;30(1):3–44. doi:10.1007/s00198-018-4704-5
14. Greenblatt MB, Tsai JN, Wein MN. Bone turnover markers in the diagnosis and monitoring of metabolic bone disease. Clin Chem. 2017;63(2):464–474. doi:10.1373/clinchem.2016.259085
15. Bauer DC. Clinical use of bone turnover markers. JAMA - J Am Med Assoc. 2019. doi:10.1001/jama.2019.9372
16. Vasikaran S, Eastell R, Bruyère O, et al. Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: a need for international reference standards. Osteoporos Int. 2011;22(2):391–420. doi:10.1007/s00198-010-1501-1
17. Shetty S, Kapoor N, Bondu J, Thomas N, Paul T. Bone turnover markers: emerging tool in the management of osteoporosis. Indian J Endocrinol Metab. 2016;20(6):846–852. doi:10.4103/2230-8210.192914
18. Cremers S, Garnero P, Seibel MJ. Biochemical markers of bone metabolism. Principles of Bone Biol. 2008;2:1857–1881. doi:10.1016/B978-0-12-373884-4.00020-3
19. Qvist P, Christgau S, Pedersen BJ, Schlemmer A, Christiansen C. Circadian variation in the serum concentration of C-terminal telopeptide of type I collagen (serum CTx): effects of gender, age, menopausal status, posture, daylight, serum cortisol, and fasting. Bone. 2002;31(1):57–61. doi:10.1016/S8756-3282(02)00791-3
20. Fares JE, Choucair M, Nabulsi M, Salamoun M, Shahine CH, Fuleihan GEH. Effect of gender, puberty, and vitamin D status on biochemical markers of bone remodedeling. Bone. 2003;33(2):242–247. doi:10.1016/S8756-3282(03)00160-1
21. Nguyen LT, Nguyen UDT, Nguyen TDT, Ho-Pham LT, Nguyen TV. Contribution of bone turnover markers to the variation in bone mineral density: a study in Vietnamese men and women. Osteoporos Int. 2018;29(12):2739–2744. doi:10.1007/s00198-018-4700-9
22. Wu C-H, Chang Y-F, Chen C-H, et al. Consensus statement on the use of bone turnover markers for short-term monitoring of osteoporosis treatment in the Asia-Pacific region. J Clin Densitom. 2019. doi:10.1016/j.jocd.2019.03.004
23. Lorentzon M, Branco J, Brandi ML, et al. Algorithm for the use of biochemical markers of bone turnover in the diagnosis, assessment and follow-up of treatment for osteoporosis. Adv Ther. 2019;36(10):2811–2824. doi:10.1007/s12325-019-01063-9
24. Szulc P, Naylor K, Hoyle NR, Eastell R, Leary ET. Use of CTX-I and PINP as bone turnover markers: national Bone Health Alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Osteoporos Int. 2017;28(9):2541–2556. doi:10.1007/s00198-017-4082-4
25. Bhattoa HP. Laboratory aspects and clinical utility of bone turnover markers. Electron J Int Fed Clin Chem Lab Med. 2018;29(2):117–128.
26. Eastell R, Szulc P. Use of bone turnover markers in postmenopausal osteoporosis. Lancet Diabetes Endocrinol. 2017;5(11):908–923. doi:10.1016/S2213-8587(17)30184-5
27. Chavassieux P, Portero-Muzy N, Roux JP, Garnero P, Chapurlat R. Are biochemical markers of bone turnover representative of bone histomorphometry in 370 postmenopausal women? J Clin Endocrinol Metab. 2015;100(12):4662–4668. doi:10.1210/jc.2015-2957
28. Park SG, Jeong SU, Lee JH, et al. The changes of CTX, DPD, osteocalcin, and bone mineral density during the postmenopausal period. Ann Rehabil Med. 2018;42(3):441–448. doi:10.5535/arm.2018.42.3.441
29. Krege JH, Lane NE, Harris JM, Miller PD. PINP as a biological response marker during teriparatide treatment for osteoporosis. Osteoporos Int. 2014;25(9):2159–2171. doi:10.1007/s00198-014-2646-0
30. Azizieh FY, Shehab D, Jarallah Al K, Mojiminiyi O, Gupta R, Raghupathy R. Circulatory pattern of cytokines, adipokines and bone markers in postmenopausal women with low BMD. J Inflamm Res. 2019;12:99–108. doi:10.2147/JIR.S203590
31. Ivanova S, Vasileva L, Ivanova S, Peikova L, Obreshkova D. Osteoporosis: therapeutic options. Folia Med (Plovdiv). 2015. doi:10.1515/folmed-2015-0037
32. Dominguez LJ, Scalisi R, Barbagallo M. Therapeutic options in osteoporosis. Acta Biomed. 2010;81(SUPPL. 1):55–65.
33. Bettica P, Bevilacqua M, Vago T, Masino M, Cucinotta E, Norbiato G. Short-term variations in bone remodeling biochemical markers: cyclical etidronate and alendronate effects compared. J Clin Endocrinol Metab. 1997;82(9):3034–3039. doi:10.1210/jcem.82.9.4193
34. Reginster JY, Wilson KM, Dumont E, Bonvoisin B, Barrett J. Monthly oral ibandronate is well tolerated and efficacious in postmenopausal women: results from the Monthly Oral Pilot Study. J Clin Endocrinol Metab. 2005;90(9):5018–5024. doi:10.1210/jc.2004-1750
35. Binkley N, Silverman SL, Simonelli C, et al. Monthly ibandronate suppresses serum CTX-I within 3 days and maintains a monthly fluctuating pattern of suppression. Osteoporos Int. 2009;20(9):1595–1601. doi:10.1007/s00198-008-0827-4
36. Borba VZC, Paz-Filho G, Kulak CAM, Seibel MJ, Bilezikian JP. Bone turnover 18 months after a single intravenous dose of zoledronic acid. Int J Clin Pract. 2007;61(6):1058–1062. doi:10.1111/j.1742-1241.2007.01392.x
37. Kaufman J-M, Audran M, Bianchi G, et al. Efficacy and safety of strontium ranelate in the treatment of osteoporosis in men. J Clin Endocrinol Metab. 2013;98(2):592–601. doi:10.1210/jc.2012-3048
38. Bruyère O, Collette J, Rizzoli R, et al. Relationship between 3-month changes in biochemical markers of bone remodelling and changes in bone mineral density and fracture incidence in patients treated with strontium ranelate for 3 years. Osteoporos Int. 2010;21(6):1031–1036. doi:10.1007/s00198-009-1078-8
39. Rizzoli R, Chapurlat RD, Laroche J-M, et al. Effects of strontium ranelate and alendronate on bone microstructure in women with osteoporosis results of a 2-year study. Osteoporos Int. 2012;23(1):305–315. doi:10.1007/s00198-011-1758-z
40. Savvidis C, Tournis S, Dede AD. Obesity and bone metabolism. Hormones. 2018;17(2):205–217. doi:10.1007/s42000-018-0018-4
41. Cao JJ. Effects of obesity on bone metabolism. J Orthop Surg Res. 2011;6(1):1. doi:10.1186/1749-799X-6-30
42. Zhao LJ, Liu YJ, Liu PY, Hamilton J, Recker RR, Deng HW. Relationship of obesity with osteoporosis. J Clin Endocrinol Metab. 2007;92(5):1640–1646. doi:10.1210/jc.2006-0572
43. Sharma S, Tandon V, Mahajan S, Mahajan V, Mahajan A. Obesity: friend or foe for osteoporosis. J Midlife Health. 2014;5(1):6. doi:10.4103/0976-7800.127782
44. Faienza MF, D’Amato G, Chiarito M, et al. Mechanisms involved in childhood obesity-related bone fragility. Front Endocrinol (Lausanne). 2019:10. doi:10.3389/fendo.2019.00269.
45. Ambroszkiewicz J, Gajewska J, Rowicka G, Klemarczyk W, Chelchowska M. Assessment of biochemical bone turnover markers and bone mineral density in thin and normal-weight children. Cartilage. 2018;9(3):255–262. doi:10.1177/1947603516686145
46. Starup-Linde J, Vestergaard P. Biochemical bone turnover markers in diabetes mellitus - A systematic review. Bone. 2016;82:69–78. doi:10.1016/j.bone.2015.02.019
47. Pater A, Sypniewska G, Pilecki O. Biochemical markers of bone cell activity in children with Type 1 diabetes mellitus. J Pediatr Endocrinol Metab. 2010;23(1–2):81–86. doi:10.1515/JPEM.2010.23.1-2.81
48. Starup-Linde J, Westberg-Rasmussen S, Lykkeboe S, Vestergaard P. Effects of glucose on bone markers: overview of current knowledge with focus on diabetes, glucose, and bone markers. Biomark Bone Dis. 2017:1105–1128. doi:10.1007/978-94-007-7693-7_15
49. Liu TT, Liu DM, Xuan Y, et al. The association between the baseline bone resorption marker CTX and incident dysglycemia after 4 years. Bone Res. 2017:5. doi:10.1038/boneres.2017.20.
50. Canalis E. Wnt signalling in osteoporosis: mechanisms and novel therapeutic approaches. Nat Rev Endocrinol. 2013;9(10):575–583. doi:10.1038/nrendo.2013.154
51. Mäkitie RE, Haanpää M, Valta H, et al. Skeletal characteristics of WNT1 osteoporosis in children and young adults. J Bone Miner Res. 2016;31(9):1734–1742. doi:10.1002/jbmr.2841
52. Luther J, Yorgan TA, Rolvien T, et al. Wnt1 is an Lrp5-independent bone-anabolic Wnt ligand. Sci Transl Med. 2018;10(466):466. doi:10.1126/scitranslmed.aau7137
53. Okamoto M, Udagawa N, Uehara S, et al. Noncanonical Wnt5a enhances Wnt/β-catenin signaling during osteoblastogenesis. Sci Rep. 2014:4. doi:10.1038/srep04493.
54. Garnero P. New developments in biological markers of bone metabolism in osteoporosis. Bone. 2014;66:46–55. doi:10.1016/j.bone.2014.05.016
55. Tian J, Xu XJ, Shen L, et al. Association of serum Dkk-1 levels with β-catenin in patients with postmenopausal osteoporosis. J Huazhong Univ Sci Technol - Med Sci. 2015;35(2):212–218. doi:10.1007/s11596-015-1413-6
56. Ueland T, Stilgren L, Bollerslev J. Bone matrix levels of dickkopf and sclerostin are positively correlated with bone mass and strength in postmenopausal osteoporosis. Int J Mol Sci. 2019;20(12):12. doi:10.3390/ijms20122896
57. Corrado A, Neve A, Macchiarola A, Gaudio A, Marucci A, Cantatore FP. RANKL/OPG ratio and DKK-1 expression in primary osteoblastic cultures from osteoarthritic and osteoporotic subjects. J Rheumatol. 2013;40(5):684–694. doi:10.3899/jrheum.120845
58. Morse LR, Sudhakar S, Lazzari AA, et al. Sclerostin: a candidate biomarker of SCI-induced osteoporosis. Osteoporos Int. 2013;24(3):961–968. doi:10.1007/s00198-012-2072-0
59. Dovjak P, Heinze G, Rainer A, Sipos W, Pietschmann P. Serum levels of Dickkopf-1 are a potential negative biomarker of survival in geriatric patients. Exp Gerontol. 2017;96:104–109. doi:10.1016/j.exger.2017.06.002
60. OARSI. Osteoarthritis: a Serious Disease, Submitted to the U.S. Food and Drug Administration. Available from: https://www.oarsi.org/sites/default/files/library/2018/pdf/oarsi_white_paper_oa_serious_disease121416_1.pdf. 2016.
61. Berenbaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr Cartil. 2013;21(1):16–21. doi:10.1016/j.joca.2012.11.012
62. Watt FE. Osteoarthritis biomarkers: year in review. Osteoarthr Cartil. 2018;26(3):312–318. doi:10.1016/j.joca.2017.10.016
63. Fernández-Puente P, Calamia V, González-Rodríguez L, et al. Multiplexed mass spectrometry monitoring of biomarker candidates for osteoarthritis. J Proteomics. 2017;152:216–225. doi:10.1016/j.jprot.2016.11.012
64. Haraden CA, Huebner JL, Hsueh MF, Li YJ, Kraus VB. Synovial fluid biomarkers associated with osteoarthritis severity reflect macrophage and neutrophil related inflammation. Arthritis Res Ther. 2019;21(1):1. doi:10.1186/s13075-019-1923-x
65. Bay-Jensen AC, Hoegh-Madsen S, Dam E, et al. Which elements are involved in reversible and irreversible cartilage degradation in osteoarthritis? Rheumatol Int. 2010;30(4):435–442. doi:10.1007/s00296-009-1183-1
66. Soul J, Dunn SL, Anand S, et al. Stratification of knee osteoarthritis: two major patient subgroups identified by genome-wide expression analysis of articular cartilage. Ann Rheum Dis. 2018;77(3):423. doi:10.1136/annrheumdis-2017-212603
67. Massicotte F, Lajeunesse D, Benderdour M, et al. Can altered production of interleukin-1β, interleukin-6, transforming growth factor-β and prostaglandin E2 by isolated human subchondral osteoblasts identity two subgroups of osteoarthritic patients. Osteoarthr Cartil. 2002;10(6):491–500. doi:10.1053/joca.2002.0528
68. Liu B, Zhang M, Zhao J, Zheng M, Yang H. Imbalance of M1/M2 macrophages is linked to severity level of knee osteoarthritis. Exp Ther Med. 2018;16(6):5009–5014. doi:10.3892/etm.2018.6852
69. Nagy E, Vajda E, Vari C, Sipka S, Fárr A-M, Horváth E. Meloxicam ameliorates the cartilage and subchondral bone deterioration in monoiodoacetate-induced rat osteoarthritis. PeerJ. 2017;5:e3185. doi:10.7717/peerj.3185
70. Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 2011;7(1):33–42. doi:10.1038/nrrheum.2010.196
71. Imamura M, Ezquerro F, Marcon Alfieri F, et al. Serum levels of proinflammatory cytokines in painful knee osteoarthritis and sensitization. Int J Inflam. 2015:2015. doi:10.1155/2015/329792.
72. Radojčić MR, Thudium CS, Henriksen K, et al. Biomarker of extracellular matrix remodelling C1M and proinflammatory cytokine interleukin 6 are related to synovitis and pain in end-stage knee osteoarthritis patients. Pain. 2017;158(7):1254–1263. doi:10.1097/j.pain.0000000000000908
73. Dyer J, Davison G, Marcora SM, Mauger AR. Effect of a Mediterranean type diet on inflammatory and cartilage degradation biomarkers in patients with osteoarthritis. J Nutr Heal Aging. 2017;21(5):562–566. doi:10.1007/s12603-016-0806-y
74. Shan Y, Qi C, Liu Y, Gao H, Zhao D, Jiang Y. Increased frequency of peripheral blood follicular helper T cells and elevated serum IL-21 levels in patients with knee osteoarthritis. Mol Med Rep. 2017;15(3):1095–1102. doi:10.3892/mmr.2017.6132
75. Castrogiovanni P, Di Rosa M, Ravalli S, et al. Moderate physical activity as a prevention method for knee osteoarthritis and the role of synoviocytes as biological key. Int J Mol Sci. 2019;20(3):3. doi:10.3390/ijms20030511
76. Munjal A, Bapat S, Hubbard D, Hunter M, Kolhe R, Fulzele S. Advances in molecular biomarker for early diagnosis of osteoarthritis. Biomol Concepts. 2019;10(1):111–119. doi:10.1515/bmc-2019-0014
77. Chu H, Xu ZM, Yu H, Zhu KJ, Huang H. Association between hypoxia-inducible factor-1a levels in serum and synovial fluid with the radiographic severity of knee osteoarthritis. Genet Mol Res. 2014;13(4):10529–10536. doi:10.4238/2014.December.12.15
78. Kovács B, Vajda E, Nagy EE. Regulatory effects and interactions of the Wnt and OPG-RANKL-RANK signaling at the bone-cartilage interface in osteoarthritis. Int J Mol Sci. 2019;20(18):18. doi:10.3390/ijms20184653
79. Zhao XY, Yang ZB, Zhang ZJ, et al. CCL3 serves as a potential plasma biomarker in knee degeneration (osteoarthritis). Osteoarthr Cartil. 2015;23(8):1405–1411. doi:10.1016/j.joca.2015.04.002
80. He J, Cao W, Azeem I, Zhao Q, Shao Z. Transforming growth factor Beta1 being considered a novel biomarker in knee osteoarthritis. Clin Chim Acta. 2017;472:96–101. doi:10.1016/j.cca.2017.07.021
81. Gundogdu G, Gundogdu K. A novel biomarker in patients with knee osteoarthritis: adropin. Clin Rheumatol. 2018;37(8):2179–2186. doi:10.1007/s10067-018-4052-z
82. Charni-Ben Tabassi N, Desmarais S, Bay-Jensen AC, Delaissé JM, Percival MD, Garnero P. The type II collagen fragments Helix-II and CTX-II reveal different enzymatic pathways of human cartilage collagen degradation. Osteoarthr Cartil. 2008;16(10):1183–1191. doi:10.1016/j.joca.2008.02.008
83. Mouritzen U, Christgau S, Lehmann HJ, Tankó LB, Christiansen C. Cartilage turnover assessed with a newly developed assay measuring collagen type II degradation products: influence of age, sex, menopause, hormone replacement therapy, and body mass index. Ann Rheum Dis. 2003;62(4):332–336. doi:10.1136/ard.62.4.332
84. Bihlet AR, Byrjalsen I, Bay-Jensen AC, et al. Associations between biomarkers of bone and cartilage turnover, gender, pain categories and radiographic severity in knee osteoarthritis. Arthritis Res Ther. 2019;21(1):1. doi:10.1186/s13075-019-1987-7
85. Reijman M, Hazes JMW, Bierma-Zeinstra SMA, et al. A new marker for osteoarthritis: cross-sectional and longitudinal approach. Arthritis Rheum. 2004;50(8):2471–2478. doi:10.1002/art.20332
86. Lehmann HJ, Mouritzen U, Christgau S, Cloos PAC, Christiansen C. Effect of bisphosphonates on cartilage turnover assessed with a newly developed assay for collagen type II degradation products. Ann Rheum Dis. 2002;61(6):530–533. doi:10.1136/ard.61.6.530
87. Park MC, Chung SJ, Park YB, Lee SK. Bone and cartilage turnover markers, bone mineral density, and radiographic damage in men with ankylosing spondylitis. Yonsei Med J. 2008;49(2):288–294. doi:10.3349/ymj.2008.49.2.288
88. Catterall J, Dewitt Parr S, Fagerlund K, Caterson B. CTX-II is a marker of cartilage degradation but not of bone turnover. Osteoarthr Cartil. 2013;21:S77. doi:10.1016/j.joca.2013.02.168
89. Meulenbelt I, Kloppenburg M, Kroon HM, et al. Urinary CTX-II levels are associated with radiographic subtypes of osteoarthritis in hip, knee, hand, and facet joints in subject with familial osteoarthritis at multiple sites: the GARP study. Ann Rheum Dis. 2006;65(3):360–365. doi:10.1136/ard.2005.040642
90. Park YM, Kim SJ, Lee KJ, Yang SS, Min BH, Yoon HC. Detection of CTX-II in serum and urine to diagnose osteoarthritis by using a fluoro-microbeads guiding chip. Biosens Bioelectron. 2015;67:192–199. doi:10.1016/j.bios.2014.08.016
91. Csifó (Vajda) E, Nagy EE, Horváth E, Fárr A-M, Muntean D-L. Mid-term effects of meloxicam on collagen type II degradation in a rat osteoarthritis model induced by iodoacetate. Farmacia. 2015;63(4):556–560.
92. Luo Y, Bay-Jensen A, Karsdala M, Qvist P, He Y. Serum CTX-II does not measure the same as urinary CTX-II. Osteoarthr Cartil. 2018;26:S179. doi:10.1016/j.joca.2018.02.386
93. Fawzy RM, Hashaad NI, Mansour AI. Decrease of serum biomarker of type II Collagen degradation (Coll2-1) by intra-articular injection of an autologous plasma-rich-platelet in patients with unilateral primary knee osteoarthritis. Eur J Rheumatol. 2017;4(2):93–97. doi:10.5152/eurjrheum.2017.160076
94. Bay-Jensen AC, Liu Q, Byrjalsen I, et al. Enzyme-linked immunosorbent assay (ELISAs) for metalloproteinase derived type II collagen neoepitope, CIIM-Increased serum CIIM in subjects with severe radiographic osteoarthritis. Clin Biochem. 2011;44(5–6):423–429. doi:10.1016/j.clinbiochem.2011.01.001
95. Wei X, Yin K, Li P, et al. Type II collagen fragment HELIX-II is a marker for early cartilage lesions but does not predict the progression of cartilage destruction in human knee joint synovial fluid. Rheumatol Int. 2013;33(7):1895–1899. doi:10.1007/s00296-011-2309-9
96. Verma P, Dalal K. Serum cartilage oligomeric matrix protein (COMP) in knee osteoarthritis: a novel diagnostic and prognostic biomarker. J Orthop Res. 2013;31(7):999–1006. doi:10.1002/jor.22324
97. Hoch JM, Mattacola CG, Bush HM, Medina McKeon JM, Hewett TE, Lattermann C. Longitudinal documentation of serum cartilage oligomeric matrix protein and patient-reported outcomes in collegiate soccer athletes over the course of an athletic season. Am J Sports Med. 2012;40(11):2583–2589. doi:10.1177/0363546512458260
98. Bai B, Li Y. Combined detection of serum CTX-II and COMP concentrations in osteoarthritis model rabbits: an effective technique for early diagnosis and estimation of disease severity. J Orthop Surg Res. 2016;11:1. doi:10.1186/s13018-016-0483-x
99. Li H, Bai B, Wang J, Xu Z, Yan S, Liu G. Identification of key mRNAs and microRNAs in the pathogenesis and progression of osteoarthritis using microarray analysis. Mol Med Rep. 2017;16(4):5659–5666. doi:10.3892/mmr.2017.7251
100. Riegger J, Rehm M, Büchele G, et al. Serum cartilage oligomeric matrix protein in late-stage osteoarthritis: association with clinical features, renal function, and cardiovascular biomarkers. J Clin Med. 2020;9(1):268. doi:10.3390/jcm9010268
101. Rose BJ, Kooyman DL. A tale of two joints: the role of matrix metalloproteases in cartilage biology. Dis Markers. 2016;2016. doi:10.1155/2016/4895050
102. Ruan G, Xu J, Wang K, et al. Associations between knee structural measures, circulating inflammatory factors and MMP13 in patients with knee osteoarthritis. Osteoarthr Cartil. 2018;26(8):1063–1069. doi:10.1016/j.joca.2018.05.003
103. Pengas I, Eldridge S, Assiotis A, McNicholas M, Mendes JE, Laver L. MMP-3 in the peripheral serum as a biomarker of knee osteoarthritis, 40 years after open total knee meniscectomy. J Exp Orthop. 2018;5(1):1. doi:10.1186/s40634-018-0132-x
104. Charlier E, Deroyer C, Ciregia F, et al. Chondrocyte dedifferentiation and osteoarthritis (OA). Biochem Pharmacol. 2019;165:49–65. doi:10.1016/j.bcp.2019.02.036
105. Leeming DJ, He Y, Veidal SS, et al. A novel marker for assessment of liver matrix remodeling: an enzyme-linked immunosorbent assay (ELISA) detecting a MMP generated type I collagen neo-epitope (C1M). Biomarkers. 2011;16(7):616–628. doi:10.3109/1354750X.2011.620628
106. Barascuk N, Veidal SS, Larsen L, et al. A novel assay for extracellular matrix remodeling associated with liver fibrosis: an enzyme-linked immunosorbent assay (ELISA) for a MMP-9 proteolytically revealed neo-epitope of type III collagen. Clin Biochem. 2010;43(10–11):899–904. doi:10.1016/j.clinbiochem.2010.03.012
107. Arends RHGP, Karsdal MA, Verburg KM, West CR, Bay-Jensen AC, Keller DS. Identification of serological biomarker profiles associated with total joint replacement in osteoarthritis patients. Osteoarthr Cartil. 2017;25(6):866–877. doi:10.1016/j.joca.2017.01.006
108. Valdes AM, Meulenbelt I, Chassaing E, et al. Large scale meta-analysis of urinary C-terminal telopeptide, serum cartilage oligomeric protein and matrix metalloprotease degraded type II collagen and their role in prevalence, incidence and progression of osteoarthritis. Osteoarthr Cartil. 2014;22(5):683–689. doi:10.1016/j.joca.2014.02.007
109. He Y, Manon-Jensen T, Arendt-Nielsen L, et al. Potential diagnostic value of a type X collagen neo-epitope biomarker for knee osteoarthritis. Osteoarthr Cartil. 2019;27(4):611–620. doi:10.1016/j.joca.2019.01.001
110. Asghar S, Litherland GJ, Lockhart JC, Goodyear CS, Crilly A. Exosomes in intercellular communication and implications for osteoarthritis. Rheumatology. 2019. doi:10.1093/rheumatology/kez462
111. Wan L, Zhao Q, Niu G, Xiang T, Ding C, Wang S. Plasma miR-136 can be used to screen patients with knee osteoarthritis from healthy controls by targeting IL-17. Exp Ther Med. 2018;16(4):3419–3424. doi:10.3892/etm.2018.6625
112. Zheng WD, Zhou FL, Lin N, Liu J. Investigation for the role of CTX-III and microRNA-98 in diagnosis and treatment of osteoarthritis. Eur Rev Med Pharmacol Sci. 2018;22(17):5424–5428. doi:10.26355/eurrev_201809_15801
113. Dong Z, Jiang H, Jian X, Zhang W. Change of miRNA expression profiles in patients with knee osteoarthritis before and after celecoxib treatment. J Clin Lab Anal. 2019;33(1):1. doi:10.1002/jcla.22648
114. de Visser HM, Sanchez C, Mastbergen SC, Lafeber FPJG, Henrotin YE, Weinans H. Fib3-3 as a biomarker for osteoarthritis in a rat model with metabolic dysregulation. Cartilage. 2019;10(3):329–334. doi:10.1177/1947603518754629
115. Runhaar J, Sanchez C, Taralla S, Henrotin Y, Bierma-Zeinstra SMA. Fibulin-3 fragments are prognostic biomarkers of osteoarthritis incidence in overweight and obese women. Osteoarthr Cartil. 2016;24(4):672–678. doi:10.1016/j.joca.2015.10.013
116. De Seny D, Sharif M, Fillet M, et al. Discovery and biochemical characterisation of four novel biomarkers for osteoarthritis. Ann Rheum Dis. 2011;70(6):1144–1152. doi:10.1136/ard.2010.135541
117. Imai K, Shikata H, Okada Y. Degradation of vitronectin by matrix metalloproteinases-1, −2, −3, −7 and −9. FEBS Lett. 1995;369(2–3):249–251. doi:10.1016/0014-5793(95)00752-U
118. Ourradi K, Xu Y, De Seny D, Kirwan J, Blom A, Sharif M. Development and validation of novel biomarker assays for osteoarthritis. PLoS One. 2017;12(7):7. doi:10.1371/journal.pone.0181334
119. Kraus VB, Burnett B, Coindreau J, et al. Application of biomarkers in the development of drugs intended for the treatment of osteoarthritis. Osteoarthr Cartil. 2011;19(5):515–542. doi:10.1016/j.joca.2010.08.019
120. Weng X, Lin P, Liu F, et al. Achyranthes bidentata polysaccharides activate the Wnt/β -catenin signaling pathway to promote chondrocyte proliferation. Int J Mol Med. 2014:1045–1050. doi:10.3892/ijmm.2014.1869
121. Cassuto J, Folestad A, Göthlin J, Malchau H, Kärrholm J. The key role of proinflammatory cytokines, matrix proteins, RANKL/OPG and Wnt/β -catenin in bone healing of hip arthroplasty patients. Bone. 2018;107:66–77.
122. Theologis T, Efstathopoulos N, Nikolaou V, et al. Association between serum and synovial fluid Dickkopf-1 levels with radiographic severity in primary knee osteoarthritis patients. 2017:1865–1872. doi:10.1007/s10067-017-3640-7
123. Mills JS, Kinsley MA, Peters DF, Weber PSD, Shearer TR, Pease AP. Correlation of dickkopf-1 concentrations in plasma and synovial fluid to the severity of radiographic signs of equine osteoarthritis. Vet Comp Orthop Traumatol. 2017;30(05):311–317. doi:10.3415/VCOT-16-11-0157
124. Lu K, Li Y, Shi T, et al. Changes in expression of Wnt signaling pathway inhibitors dickkopf-1 and sclerostin before and after total joint arthroplasty. Medicine. 2017;96: 1–5.
125. Huang X, Post JN, Zhong L, et al. Dickkopf-related protein 1 and gremlin 1 show different response than frizzled-related protein in human synovial fluid following knee injury and in patients with osteoarthritis. Osteoarthr Cartil. 2018;26(6):834–843. doi:10.1016/j.joca.2018.02.904
126. Snelling SJB, Davidson RK, Swingler TE, et al. Dickkopf-3 is upregulated in osteoarthritis and has a chondroprotective role. Osteoarthritis Cartil. 2016;24:883–891. doi:10.1016/j.joca.2015.11.021
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.