")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 13
Socioeconomic inequality in the use of prescription medications for smoking cessation among patients with COPD: a nationwide study
Authors Tøttenborg SS , Clark AJ , Thomsen RW , Johnsen SP, Lange P
Received 5 December 2017
Accepted for publication 4 March 2018
Published 29 May 2018 Volume 2018:13 Pages 1775—1781
DOI https://doi.org/10.2147/COPD.S158954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Sandra Søgaard Tøttenborg,1 Alice Jessie Clark,1 Reimar Wernich Thomsen,2 Søren Paaske Johnsen,2 Peter Lange1,3
1Department of Public Health, Section of Social Medicine, University of Copenhagen, Copenhagen, Denmark; 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 3Respiratory Section, Hvidovre Hospital, Hvidovre, Denmark
Background: Bupropion and varenicline can substantially improve the chances of smoking cessation in patients with COPD, but are unsubsidized and relatively costly. We examined overall use and socioeconomic patterns of use among patients with COPD.
Patients and methods: We identified 4,741 COPD patients reporting to be smokers at their first contact for COPD during 2008–2012 in the Danish register of COPD, which covers all pulmonary outpatient clinics in Denmark. Patients were followed for 6 months in the National Prescription Registry. Logistic regression analyses were used to calculate the ORs with corresponding 95% CI of redeeming a prescription for any of the smoking cessation medications in strata of baseline characteristics.
Results: During 6 months from first consultation, only 5% redeemed a prescription for bupropion or varenicline. Younger age, female sex, higher education, and higher income were associated with an increased likelihood, while non-Danish ethnicity, living alone, and very severe COPD were associated with a lower likelihood of redeeming bupropion or varenicline.
Conclusion: Despite their proven effectiveness, bupropion and varenicline are sparingly used among COPD patients followed in the hospital outpatient setting with the lowest use among the socioeconomically disadvantaged. This highlights a missed opportunity for intervention.
Keywords: bupropion, varenicline, smoking intervention, lung disease
Plain language summary
Smoking cessation is crucial for slowing the progression of COPD. Yet, a large proportion of patients with COPD continue to smoke with the lowest quit rates observed among socioeconomically disadvantaged groups. Prescription medications bupropion and varenicline are effective but expensive smoking cessation aids. We did this study to determine if COPD patients take advantage of this therapeutic option in their efforts to quit smoking and whether some subgroups are more or less likely to do so.
Using the Danish register for COPD and the National Prescription Registry, we followed 4,741 smokers with COPD for filling a prescription for bupropion or varenicline during six months from first outpatient clinic contact and calculated the odds according to socio-demographic patient characteristics.
We found that bupropion and varenicline are sparingly used among COPD patients followed in the hospital outpatient setting overall with the lowest use among the socioeconomically disadvantaged. This highlights a missed opportunity for intervention.
Background
Smoking cessation is the most effective strategy to reduce respiratory symptoms1,2 and slow the progression of COPD.2–7 Despite these clear benefits, multiple studies show that many COPD patients continue to smoke.8–11 In Denmark, a national audit indicated that more than 30% of all patients followed in Danish hospital-based pulmonary outpatient clinics are active smokers.12 Recently, we showed that the probability of quitting smoking among COPD outpatients is only 19% after 1 year and 45% after 5 years, respectively.13 Patients who continue to smoke despite symptomatic COPD may have higher nicotine dependence relative to smokers without COPD.14 Patients who do not succeed in quitting smoking are generally younger, have milder COPD, more often live alone, and have a lower income.13 This could be indicative of inadequate intervention for achieving tobacco abstinence related to socioeconomic inequalities.
Doctors at hospital-based pulmonary outpatient clinics are well-placed to support smokers in quitting by providing prescriptions for smoking cessation medications (SCMs). Both bupropion and varenicline have been shown in randomized controlled trials and in real-world observational studies to substantially improve the chances of long-term smoking cessation in the general population15 and in patients with COPD.16–18 However, these medications are expensive and unlike most drugs for chronic diseases, there is no general public reimbursement for them in most countries including Denmark, making these drugs out of reach for the financially less well-off patients. To our knowledge, no previous study has examined how widespread the use of these medications is among patients with COPD.
In this nationwide population-based study, we examine the use of SCMs among outpatients with COPD who smoke and who were eligible for smoking cessation intervention. We also investigated clinical, demographic and socioeconomic predictors for the use of SCMs. Our hypothesis was that patients who are younger and have milder COPD are less likely to redeem a prescription for SCMs compared with their older, more severely ill, counterparts. Furthermore, we hypothesized that patients with lower disposable income and lower education are less likely to redeem a prescription for SCMs relative to their high-income and high-educated fellow smokers.
Patients and methods
Study population
In Denmark, stable, mild and moderate COPD is mainly managed by general practitioners (GPs). Patients with more severe COPD, those with frequent exacerbations or rapidly progressing disease are referred to pulmonary outpatient specialist clinics based in public hospitals. From 2008, the nationwide Danish Register of COPD (DrCOPD) has continuously monitored these outpatients in all of Denmark. Details of the DrCOPD have been described previously.12,19 Briefly, with the DrCOPD, all hospital-based outpatient clinics are committed to register and report a set of clinical variables including smoking status and pulmonary function (assessed as forced expiratory volume in 1 second [FEV1] % predicted) for each COPD patient who is followed at the clinic at least once a year. During 2008–2012, a total of 23,741 individuals with a first-ever outpatient contact for COPD were enrolled of which 4,741 reported to be current smokers and thus eligible for this study.
Prescription medications for smoking cessation
Use of SCMs was identified searching the Danish Prescription Registry (DPR) for filled prescriptions of bupropion (Anatomical Therapeutic Chemical [ATC] Classification code N06AX12) and varenicline (ATC code N07BA03) among smokers during 6 months from first outpatient visit in the DrCOPD. Patients who either died or migrated before the end of the observation period were excluded (N=796). The DPR holds complete information on all out-of-hospital dispensed prescriptions at pharmacies and nursing homes.20 Previous use of SCMs was identified searching for prescriptions filled in the year 2000, where bupropion was introduced to the Danish market and up to the date of first outpatient visit, and in 2006, where varenicline was introduced and first outpatient visit.
Clinical and sociodemographic variables
Statistics Denmark provided data on age (30–49, 50–69 and ≥70 years), sex (male and female) and cohabitation status (any other person who is not a dependent categorized as cohabiting and not cohabiting). Severity of airflow limitation was recorded as FEV1%pred from DrCOPD according to GOLD 1–4 staging.21 Educational attainment was categorized as primary/lower secondary (elementary school), upper secondary (high school) and tertiary (university). Family equalized disposable income (calculated as total income including estimated rental value before deduction of interest expenses minus total tax deductible interest expenses, including interest expenses in business minus total taxes including labor market contributions and special pension contributions minus paid tax deductible maintenance allowance minus reimbursed cash benefits taking into account the number and age of persons in the household) the year before baseline was divided into tertiles (low, medium and high).
Statistical analyses
As prescription data were only available until the end of 2012, 576 participants with a first outpatient visit later than June 30, 2012, were excluded due to follow-up shorter than the required 6 months. The 220 patients who died before the 6 months mark were included for analyses. Among the remaining 4,165 smokers with COPD, we calculated the proportion who claimed a prescription for bupropion and/or varenicline during the 6 months following first outpatient contact for the population as a whole, and in strata of baseline characteristics and previous use of SCMs. Multiple logistic regression analyses were used to calculate the OR with corresponding 95% CI of redeeming a prescription for any SCM. The identification of potential confounders was guided by previous knowledge and the methods of directed acyclic graphs.22 Analyses were performed using STATA-14 (StataCorp, College Station, TX, USA).
Ethical approval
The study was approved by the Danish Data Protection Agency (record 2012-41-0438), the Danish National Indicator Project, Danish Regions and the Danish Ministry of Health.
Results
Among the 4,165 smokers with COPD, the vast majority was above 50 years of age (91%) and of Danish origin (96%). Sex, cohabitation status and disposable income were equally distributed and the majority of patients had COPD severity corresponding to GOLD 2 and 3 (46% and 35%, respectively). As expected for a relatively older population, elementary school was the highest attained education for 56% while 37% had finished high school.
During 6 months from first outpatient visit, only 5% redeemed any prescription for SCM, with 1% redeeming bupropion and 4% redeeming varenicline. We did not observe any temporal trends in the use of SCMs during the study period (results not shown).
Table 1 shows proportions as well as crude and confounder adjusted ORs with corresponding 95% CI of redeeming any SCM within 6 months from first outpatient visit according to baseline clinical and sociodemographic characteristics and previous use of SCMs.
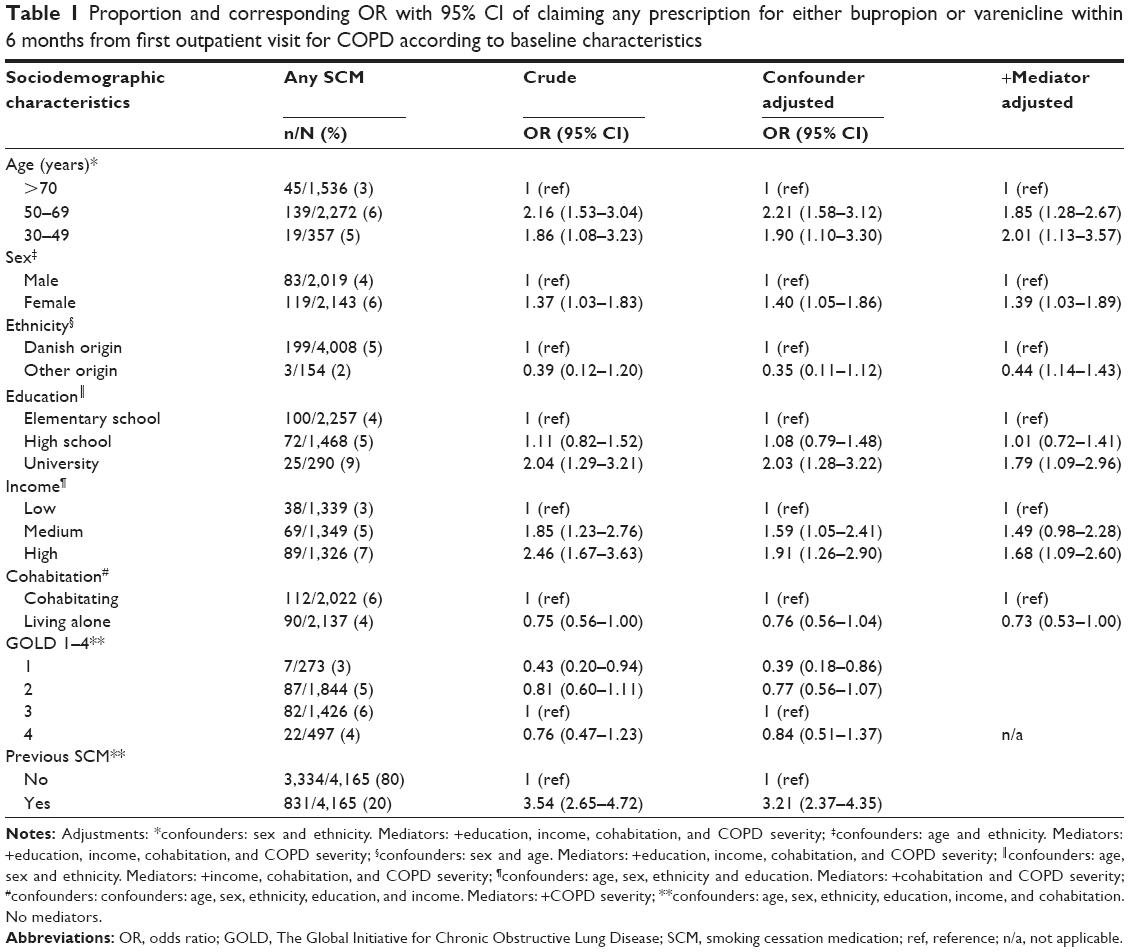 | Table 1 Proportion and corresponding OR with 95% CI of claiming any prescription for either bupropion or varenicline within 6 months from first outpatient visit for COPD according to baseline characteristics |
Confounder adjusted analyses showed that patients aged 30–49 (OR 1.90, 95% CI 1.10–3.30) and 50–69 (OR 2.21, 95% CI 1.58–3.12) years had an ~2-fold increased likelihood of redeeming an SCM compared with patients older than 70 years of age. The association persisted after excluding patients, who died within the follow-up period (data not shown). The observed age differences in the use of SCMs could neither be explained by education and income, which are generally higher among the younger age groups, nor by a higher degree of cohabiting and milder disease.
In age- and ethnicity-adjusted analyses, females were more likely to redeem an SCM prescription (OR 1.40, 95% CI 1.10–3.30) compared with males. The association persisted after additional inclusion of potential mediating factors as education, income, cohabitation and COPD severity.
Confounder adjusted analyses suggested that smokers of non-Danish origin have substantially lower odds of redeeming an SCM (OR 0.35, 95% CI 0.11–1.12) compared with native Danes. Further adjustment for education and income, which is generally lower among non-Danes, attenuated this association slightly.
Smokers with the highest education were more than twice as likely to redeem an SCM prescription (OR 2.03, 95% CI 1.28–3.22) relative to patients with the lowest education when adjusting for confounders. A generally higher income, higher likelihood of cohabiting and lower COPD severity among patients with a university degree explained about a one-fourth of the increased likelihood.
A gradient in the use of SCMs was observed for income, with patients belonging to the middle and highest income groups having ORs of redeeming an SCM of 1.59 (95% CI 1.05–2.41) and 1.91 (95% CI 1.26–2.90), respectively, when compared with patients in the lowest income group. A generally higher proportion cohabiting and milder COPD severity explained some, but not all of the increased likelihood.
Patients who lived alone were less likely to redeem an SCM prescription (OR 0.76, 95% CI 0.56–1.04) compared with patients who cohabited. Differences in COPD severity could not explain the observed difference.
Mild COPD corresponding to GOLD 1 was associated with lower odds of redeeming an SCM prescription (OR 0.39, 95% CI 0.18–0.86) when compared with severe COPD (GOLD 3), which was the most common severity level in the population. Although not materially different from patients in GOLD group 3, patients with GOLD 4 were less likely to redeem an SCM; this association was not explained by higher 6-month mortality in the more severe COPD group (results not shown).
Discussion
Despite the well-documented effectiveness of bupropion and varenicline for smoking cessation among persistent smokers with COPD,16–18 studies on the use of these medications among patients initiating specialized outpatient care are virtually nonexisting. This exact time in the patient’s history of disease is a relevant point of intervention as patients who continue to smoke despite the progression of their disease likely have special needs in order to quit.
Our study shows that the use of prescription medications for smoking cessation among persistent smokers with COPD is low, with only 5% redeeming a prescription within 6 months of first outpatient visit. The study further shows substantial clinical and sociodemographic inequalities in the use of SCMs with a higher chance of redeeming SCM in younger individuals, women, those with Danish origin, highest income and education, those living with a partner and those with either mildest or most severe COPD.
Smoking cessation is beneficial in COPD patients of all ages, and to our knowledge, SCMs have not been shown less efficacious in older compared with younger smokers. It is possible that conscious or subconscious ageism by physicians may explain the lower SMC prescription rate among older patients. It is well-known that older people with chronic conditions tend to have a lower use of statins and a lower use of newer antidiabetic drugs23 and receive less aggressive medical cancer treatments than younger patients.24 Alternatively, patient preferences or higher price sensitivity in regard to smoking cessation aids among older individuals might explain the lower use of SMCs.
This study showed a higher likelihood in female than in male smokers to initiate SCM when starting in COPD outpatient care. In a recent study by McKee et al, women reported greater perceived benefits of smoking cessation compared with men, and that perceived benefits were associated with a motivation to quit.25 Simultaneously, women reported lower self-efficacy in their ability to resist smoking in situations involving negative affect,26 and have been found to more accurately remember past withdrawal, while men tend to minimize symptoms.27 On the basis of these studies, one could hypothesize that women are more motivated to quit, but to a lesser extent rely on their own willpower in smoking cessation attempts, consequently being more proactive and/or open to trying SCMs. An alternative explanation may be that men to a larger extent prefer other therapeutic options such as nicotine replacement therapy.
Smokers of non-Danish origin were less likely than native Danes to redeem an SCM. In a recent study, we found that patients of non-Danish origin were considerably less likely to use any inhaled maintenance medication compared with ethnic Danes.28 In both the previous and the current studies, the association between ethnicity and medicine use was adjusted for a range of potential explanatory factors including education and income. Although these are generally lower among non-Danish patients, this did not explain the association. An explanation for the lower SCM initiation may be cultural and language barriers as well as different health belief models, which could affect the patient’s understanding and willingness in taking SCMs.
In this study addressing socioeconomic difference in SCM use among COPD patients who smoke, having a higher education and higher income nearly doubled the likelihood of redeeming an SCM. Given the relatively high cost of these medications, this socioeconomic skew comes as no surprise. In Denmark in 2016, the recommended 12-week treatment with varenicline sold as Champix® (Pfizer, New York, NY, USA) is 316 Euros, while the shortest recommended treatment course of 7 weeks with bupropion sold as Zyban® (GSK Pharma, Brentford, UK) is 124 Euros. In contrast to the majority of medications for chronic conditions in Denmark, SCMs are not subsidized, which could explain why the use is so much higher among the more well-off patients, which, in turn, could help to explain the higher quit rates observed among more affluent smokers with COPD.13 A 2012 Cochrane systematic review concluded that financial interventions directed at smokers when compared with no financial interventions increase the proportion of smokers who attempt to quit, use smoking cessation treatments and succeed in quitting.29 Such a strategy could be particularly beneficial for low SES patients who to a larger extent report financial motivations for wanting to quit30 as they would experience a more immediate financial upside by quitting instead of merely replacing tobacco expenses with expenses for SMCs in the first critical phase of quitting.
The present study also showed that living alone is associated with lower SCM use and that this was independent of age, sex, ethnicity, education and income. We speculate that motivation from a partner may play a role in explaining the higher likelihood of SCM use among cohabiting COPD patients.
We observed an association between GOLD stage and use of SMC. In a previous study using data from the DrCOPD, we found an association between lower COPD severity and chance of quitting13 and another study observed activity limitation due to pulmonary symptoms to be associated with smoking cessation.31 Hence, patients who have milder COPD may feel less motivated to quit or may prefer and agree with the managing physician to try quitting unassisted, which could explain the lower use of SCM in this group. Furthermore, we wonder if the seemingly lower chance of redeeming an SMC among the very severely ill patients could be due to the physician “giving up” on these particularly persistent smokers. This notion is supported by a recent multinational qualitative study, where Eerd et al found that doctors’ frustrations and negative attitudes toward COPD patients who continued to smoke contributed to poor cessation management and treatment inequalities in some cases. Many doctors also cited a lack of experience with smoking cessation techniques alongside time and money issues as to effective treatment.32
Finally, the study showed that the previous use of SCM was a strong predictor for repeated use. This could be reflective of a higher motivation for stopping and implicitly COPD patients more proactive and receptive to using cessation aids. However, it could also reflect a degree of continuous use instead of the recommended treatment course of up to 12 weeks.
Strengths and limitations
Our study has several major strengths. The prospective design ensured the ability to assess the redemption of prescriptions in the months following the initiation of management in outpatient clinics, a critical moment to intensify efforts for the patient to achieve abstinence. Independently collected data on socioeconomic factors and COPD severity from high validity national registers were available on most subjects. The use of the extensive Danish prescription registry to account for patient use of SCMs was another major strength as it completely removes the biases due to recall. However, we are likely to have under-ascertained the prescription practices of the physicians, as pharmacy records only account for claimed medications. Therefore, we cannot be sure whether part of the non-use of SCM is due to the patient not claiming a prescription issued by the managing physicians. Indeed, medication nonadherence – not taking pharmacologic treatments according to agreed recommendations from a health care provider – is common in patients with COPD.33,34 If less affluent COPD patients are less likely to redeem an issued SCM prescription than their better-off counterparts, we may have accentuated the difference in prescription practices with the data available. Furthermore, the prescription registry does not hold information on nicotine replacement therapy, which is primarily sold over-the-counter and is cheaper than both varenicline and bupropion. Thus, patients who did not claim an SCM may be in treatment with nicotine replacement therapy, be participating in other smoking cessation interventions or have taken up electronic cigarettes as a means of risk reduction, although the latter were not widely used in Denmark during the study period. Regardless the possible use of alternative interventions for smoking cessation, our findings show a worryingly low use of documented effective SCMs among smokers with COPD followed in the outpatient setting.
Conclusion
Bupropion and varenicline for smoking cessation are being sparingly used in general and with significantly lower usage among socioeconomically disadvantaged patients and patients with less severe disease. These inequalities may contribute to the observed low quit rates in these patient groups. The vast importance of smoking cessation in slowing the progression of COPD and improving overall prognosis of this high-risk population calls for continuous efforts to ensure equal and timely access to effective cessation medications. It could be argued that individuals with COPD would benefit from reimbursed SCMs on similar principles as for other maintenance medications for COPD.
Disclosure
Dr Lange reports grants and personal fees from GSK, personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim and personal fees from Chiesi, outside the submitted work. The other authors report no conflicts of interest in this work.
References
Willemse BW, Postma DS, Timens W, ten Hacken NH. The impact of smoking cessation on respiratory symptoms, lung function, airway hyperresponsiveness and inflammation. Eur Respir J. 2004;23(3):464–476. | ||
Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999;106(4):410–416. | ||
Godtfredsen NS, Lam TH, Hansel TT, et al. COPD-related morbidity and mortality after smoking cessation: status of the evidence. Eur Respir J. 2008;32(4):844–853. | ||
Au DH, Bryson CL, Chien JW, et al. The effects of smoking cessation on the risk of chronic obstructive pulmonary disease exacerbations. J Gen Intern Med. 2009;24(4):457–463. | ||
Godtfredsen NS, Vestbo J, Osler M, Prescott E. Risk of hospital admission for COPD following smoking cessation and reduction: a Danish population study. Thorax. 2002;57(11):967–972. | ||
Kupiainen H, Kinnula VL, Lindqvist A, et al. Successful smoking cessation in COPD: association with comorbidities and mortality. Pulm Med. 2012;2012:725024. | ||
Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE; Lung Health Study Research Group. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142(4):233–239. | ||
Martinez FJ, Calverley PM, Goehring UM, Brose M, Fabbri LM, Rabe KF. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trial. Lancet. 2015;385(9971):857–866. | ||
Magnussen H, Disse B, Rodriguez-Roisin R, et al; WISDOM Investigators. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. | ||
Calverley PM, Anderson JA, Celli B, et al; TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. | ||
Tashkin DP, Celli B, Senn S, et al; UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. | ||
Tøttenborg SS, Thomsen RW, Nielsen H, Johnsen SP, Frausing Hansen E, Lange P. Improving quality of care among COPD outpatients in Denmark 2008–2011. Clin Respir J. 2013;7(4):319–327. | ||
Tøttenborg SS, Thomsen RW, Johnsen SP, Nielsen H, Lange P. Determinants of smoking cessation in COPD patients treated in the outpatient setting. Chest. 2016;150(3):554–562. | ||
Jimenez-Ruiz CA, Masa F, Miravitlles M, et al. Smoking characteristics: differences in attitudes and dependence between healthy smokers and smokers with COPD. Chest. 2001;119(5):1365–1370. | ||
Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. 2013;(5):CD009329. | ||
Tashkin D, Kanner R, Bailey W, et al. Smoking cessation in patients with chronic obstructive pulmonary disease: a double-blind, placebo-controlled, randomised trial. Lancet. 2001;357(9268):1571–1575. | ||
Wagena EJ, Knipschild PG, Huibers MJ, Wouters EF, van Schayck CP. Efficacy of bupropion and nortriptyline for smoking cessation among people at risk for or with chronic obstructive pulmonary disease. Arch Intern Med. 2005;165(19):2286–2292. | ||
Anthenelli RM, Benowitz NL, West R, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial. Lancet. 2016;387(10037):2507–2520. | ||
Lange P, Tøttenborg SS, Sorknes AD, et al. Danish register of chronic obstructive pulmondary disease. Clin Epidemiol. 2016;8:1–6. | ||
Kildemoes HW, Sorensen HT, Hallas J. The Danish national prescription registry. Scand J Public Health. 2011;39(7 Suppl):38–41. | ||
Lange P, Marott JL, Vestbo J, et al. Prediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general population. Am J Respir Crit Care Med. 2012;186(10):975–981. | ||
Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. 1999;10(1):37–48. | ||
Christensen DH, Rungby J, Thomsen RW. Nationwide trends in glucose-lowering drug use, Denmark, 1999–2014. Clin Epidemiol. 2016;8:381–387. | ||
Sogaard M, Thomsen RW, Bossen KS, Sorensen HT, Norgaard M. The impact of comorbidity on cancer survival: a review. Clin Epidemiol. 2013;5 (Suppl 1):3–29. | ||
McKee SA, O’Malley SS, Salovey P, Krishnan-Sarin S, Mazure CM. Perceived risks and benefits of smoking cessation: gender-specific predictors of motivation and treatment outcome. Addict Behav. 2005;30(3):423–435. | ||
Abrams DB, Monti PM, Pinto RP, Elder JP, Brown RA, Jacobus SI. Psychosocial stress and coping in smokers who relapse or quit. Health Psychol. 1987;6(4):289–303. | ||
Pomerleau CS. Smoking and nicotine replacement treatment issues specific to women. Am J Health Behav. 1996;20:291–299. | ||
Tøttenborg SS, Lange P, Johnsen SP, Nielsen H, Ingebrigtsen T, Thomsen RW. Socioeconomic inequalities in adherence to inhaled maintenance medications and clinical prognosis of COPD. Respir Med. 2016;119:160–167. | ||
Reda AA, Kotz D, Evers SM, van Schayck CP. Healthcare financing systems for increasing the use of tobacco dependence treatment. Cochrane Database Syst Rev. 2012;(6):CD004305. | ||
Pisinger C, Aadahl M, Toft U, Jorgensen T. Motives to quit smoking and reasons to relapse differ by socioeconomic status. Prev Med. 2011;52(1):48–52. | ||
Schiller JS, Ni H. Cigarette smoking and smoking cessation among persons with chronic obstructive pulmonary disease. Am J Health Promot. 2006;20(5):319–323. | ||
van Eerd EAM, Bech Risor M, Spigt M, et al. Why do physicians lack engagement with smoking cessation treatment in their COPD patients? A multinational qualitative study. NPJ Prim Care Respir Med. 2017;27(1):41. | ||
Blackstock FC, ZuWallack R, Nici L, Lareau SC. Why don’t our patients with chronic obstructive pulmonary disease listen to us? The enigma of nonadherence. Ann Am Thorac Soc. 2016;13(3):317–323. | ||
Tottenborg SS, Lange P, Johnsen SP, Nielsen H, Ingebrigtsen TS, Thomsen RW. Socioeconomic inequalities in adherence to inhaled maintenance medications and clinical prognosis of COPD. Respir Med. 2016;119:160–167. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.