")
Back to Journals » Patient Preference and Adherence » Volume 11
Sociodemographic profile and predictors of outpatient clinic attendance among HIV-positive patients initiating antiretroviral therapy in Selangor, Malaysia
Authors Abdulrahman SA , Rampal L, Othman N, Ibrahim F, Hayati KS, Radhakrishnan AP
Received 11 May 2017
Accepted for publication 20 June 2017
Published 27 July 2017 Volume 2017:11 Pages 1273—1284
DOI https://doi.org/10.2147/PPA.S141609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Surajudeen Abiola Abdulrahman,1,2 Lekhraj Rampal,1 Norlijah Othman,3 Faisal Ibrahim,1 Kadir Shahar Hayati,1 Anuradha P Radhakrishnan4
1Department of Community Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Selangor, 2Department of Public Health Medicine, Penang Medical College, George Town, Penang, 3Department of Paediatrics, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Selangor, 4Infectious Disease Clinic, Hospital Sungai Buloh, Sungai Buloh, Selangor, Malaysia
Background: Inconsistent literature evidence suggests that sociodemographic, economic, and system- and patient-related factors are associated with clinic attendance among the HIV-positive population receiving antiretroviral therapy (ART) around the world. We examined the factors that predict outpatient clinic attendance among a cohort of HIV-positive patients initiating ART in Selangor, Malaysia.
Patients and methods: This cross-sectional study analyzed secondary data on outpatient clinic attendance and sociodemographic, economic, psychosocial, and patient-related factors among 242 adult Malaysian patients initiating ART in Selangor, Malaysia. Study cohort was enrolled in a parent randomized controlled trial (RCT) in Hospital Sungai Buloh Malaysia between January and December 2014, during which peer counseling, medication, and clinic appointment reminders were provided to the intervention group through short message service (SMS) and telephone calls for 24 consecutive weeks. Data on outpatient clinic attendance were extracted from the hospital electronic medical records system, while other patient-level data were extracted from pre-validated Adult AIDS Clinical Trial Group (AACTG) adherence questionnaires in which primary data were collected. Outpatient clinic attendance was categorized into binary outcome – regular attendee and defaulter categories – based on the number of missed scheduled outpatient clinic appointments within a 6-month period. Multivariate regression models were fitted to examine predictors of outpatient clinic attendance using SPSS version 22 and R software.
Results: A total of 224 (93%) patients who completed 6-month assessment were included in the model. Out of those, 42 (18.7%) defaulted scheduled clinic attendance at least once. Missed appointments were significantly more prevalent among females (n=10, 37.0%), rural residents (n=10, 38.5%), and bisexual respondents (n=8, 47.1%). Multivariate binary logistic regression analysis showed that Indian ethnicity (adjusted odds ratio [AOR] =0.235; 95% CI [0.063–0.869]; P=0.030) and heterosexual orientation (AOR =4.199; 95% CI [1.040–16.957]; P=0.044) were significant predictors of outpatient clinic attendance among HIV-positive patients receiving ART in Malaysia.
Conclusion: Ethnicity and sexual orientation of Malaysian patients may play a significant role in their level of adherence to scheduled clinic appointments. These factors should be considered during collaborative adherence strategy planning at ART initiation.
Keywords: sociodemographic, predictors, HIV/AIDS, clinic attendance, behavior, antiretroviral therapy, ART
Introduction
Adherence to antiretroviral therapy (ART) is a holistic concept comprising two key components – strict medication adherence and adherence to scheduled outpatient clinic appointments.1 In the management of HIV/AIDS, like all other chronic diseases, regular clinic attendance for medication refill, laboratory investigations, and clinician assessments are critical to achieving treatment success and good clinical outcomes.2 The opportunity to quickly identify and address treatment failure is also lost when patients default scheduled outpatient clinic appointments. With set targets of ≥80% and ≥90%, respectively, on-time appointment keeping and on-time drug pickups are very important early warning indicators (EWIs) with which World Health Organization (WHO) monitors HIV drug resistance among patients attending ART clinics around the world.3
Although strict medication adherence is believed to be the single most important predictor of treatment outcome,4 many studies have also shown that missed clinic appointments are significantly associated with virologic failure,5–7 drug resistance,8–10 and occurrence of AIDS-defining illness or death.11,12 Other studies have also shown that there is a significant association between adherence to clinic appointments and medication adherence in patients with chronic illnesses.13
As with medication adherence, factors related to health care delivery systems, patient-related factors, sociodemographic, economic, and factors associated with provider–patient relationship have been found to be significantly but inconsistently associated with clinic attendance. For example, whereas sociodemographic and economic factors such as older age, non-African-American ethnicity, and higher income were reported to be associated with regular clinic attendance in the United States and Brazil,14–17 older age and female gender were found to be associated with higher likelihood of early missed visits in China.18 More often than not, system-level factors such as adherence counseling, hospital-based support group, and high family support have been more consistently associated with regular clinic attendance among HIV-positive patients receiving ART in Asia.19,20 Provider-level factors such as availability, attitude, and communication styles of HIV clinicians and other health care team members have also been reported to influence clinic attendance.21
Given that the most frequently cited reason for missing scheduled clinic appointments is that patient simply forgot that they had an appointment, recent innovations involving use of short message service (SMS) reminders have gained popularity due to their varying degrees of effectiveness in improving patient adherence to scheduled clinic appointments in medical outpatient clinics across the world,22 including the United Kingdom,23 Uganda,13 Australia,24,25 and Malaysia.26
The aim of this paper was to highlight the sociodemographic profile and predictors of outpatient clinic attendance among a cohort of Malaysian patients initiating ART, in a parent study whose overall objective was to determine whether the introduction of mobile phone reminders (SMS and telephone call reminders) and peer counseling can significantly improve adherence (medication adherence and clinic attendance) and treatment outcomes among HIV-positive patients on ART.
Patients and methods
Study location and context
The current study was conducted among patients (predominantly homosexuals) who were newly initiated on ART in Hospital Sungai Buloh – a government hospital and the largest infectious disease hospital in Malaysia. It has over 8,000 HIV-positive patients on treatment and care, accounting for 35%–40% of the 21,654 patients currently on highly active ART (HAART) in various centers across Malaysia, as at 2014. This center provides a wide range of HIV/AIDS prevention, care, and treatment services including diagnostics, drugs, and clinical and support services to an average of 1,000 newly diagnosed HIV-positive patients per year, out of whom an average of 400–500 patients are initiated on HAART yearly based on eligibility criteria.
Study design
This was a cross-sectional study in which statistical analysis of secondary data on regularity of scheduled outpatient clinic attendance and sociodemographic, economic, psychosocial, and patient-related characteristics of 242 adult Malaysian patients who were newly initiated on ART was conducted, using SPSS version 22 (IBM Corporation, Armonk, NY, USA) and R Software. Randomized study subjects were enrolled in a parent study (single-blinded randomized controlled trial [RCT]) in Hospital Sungai Buloh, Malaysia, between January and December 2014. A “reminder module” that included standardized weekly SMS medication reminders (sent at 9 am every Monday), SMS reminder 3 days prior to scheduled clinic appointments (individualized and sent at lunch time), and an average of 90-second lunch-hour telephone call reminders a day prior to scheduled clinic appointment (in addition to standard care, routine adherence counseling and paper-based appointment scheduling) was delivered consistently for 24 consecutive weeks (starting from the date of ART initiation and baseline data collection) to respondents in the intervention group by two trained people living with HIV/AIDS (PLHIV) (research assistants), while respondents in the control group received standard care only. Multivariate regression models were used to determine predictors of outpatient clinic attendance at trial end point (after 6-month follow-up period).
Ethical approval
The parent study was registered with ClinicalTrials.gov, NCT02677675. Written approval for conducting this study was obtained from Universiti Putra Malaysia (UPM) Ethics Committee for Human Research (UPM/TNCPI/RMC/1.4.18.1 (JKEUPM)/F1) and the Malaysian Ministry of Health’s Institutional Review and Ethics Committee (NMRR-13-882-17412), prior to the commencement of the study. Written informed consent was obtained from all individual participants included in the study.
Data collection and analysis
Data on regularity of respondents’ scheduled outpatient clinic attendance were obtained by two trained research assistants (for whom access was duly sought and provided by the hospital management) from the hospital’s electronic medical record system using standardized data extraction forms and corroborated with drug refill appointments from pharmacy records. Only attendance records for five consecutive scheduled outpatient clinic visits within the first 6 months of ART initiation were considered. Typically, as a standard best practice for all patients, these visits were scheduled by clinicians in the study setting at ART initiation (visit 1), 2 weeks after ART initiation (visit 2), 1 month (visit 3), 3 months (visit 4), and 6 months after ART initiation (visit 5). Within this period, every outpatient clinic attendance was planned such that patients are clinically assessed by a clinician, receive adherence counseling, perform or receive feedback on their laboratory investigation (if required), and pick up their antiretroviral medications. Except for visits to emergency room and inpatient ward admissions which overlapped with any of the abovementioned five visits, unscheduled, changed, or canceled outpatient clinic appointments were not considered in this study. Clinic attendance was considered valid irrespective of the time of visit on the scheduled appointment day. Where there were multiple scheduled appointments (eg, for review of drug reactions), we also considered as valid, any visit that closely approximated the standard schedule for all patients. In doing so, we considered all visits made within a window of 24–48 hours prior to the “original” scheduled appointment.
Data on sociodemographic (age, gender, ethnicity, education level, residential location), economic (monthly income, employment status), psychosocial (availability and satisfaction with social support), treatment (type of ART regimen, intervention vs control group classification), and patient-related (sexual orientation, recreational/illicit drug use) characteristics of respondents were retrieved and extracted onto standardized data extraction sheets from a modified, pre-validated, self-administered Adult AIDS Clinical Trial Group (AACTG) adherence questionnaires that were used to collect the primary data at baseline and 6-month follow-up period. Only 224 patients who completed 6-month follow-up assessment out of the 242 enrolled at study commencement were included in the final analysis. A total of 18 patients had dropped out during the course of the trial (two lost to follow-up and three transferred out in the intervention group; 12 lost to follow-up, and one transferred out in the control group). Data extraction forms were reviewed periodically for completeness, correctness, and accuracy by the site study coordinator.
Regularity of scheduled outpatient clinic attendance – the outcome of interest in this study – was measured based on the number of outpatient clinic appointments attended on-schedule and the number of missed appointments. Regularity of scheduled outpatient clinic attendance was then categorized into two levels, which included the following: 1) regular attendee – a person who has never missed any scheduled clinic appointment; 2) defaulter – a person who has missed one or more scheduled clinic appointment, for any reason(s). We assessed the availability and level of satisfaction of respondents with psychosocial support received from friends and family members using the following questions: 1) To what extent do your friends or family members help you remember your appointment or to take your medications? This was rated on a 4-point Likert-like response scale: “not at all,” “sometimes,” “most times,” and “not applicable.” 2) In general, how satisfied are you with the overall support you get from your friends and family members? This was rated on a 4-point Likert-like response scale: “very dissatisfied,” “somewhat dissatisfied,” “somewhat satisfied,” and “very satisfied.” For ease of analysis, we combined and recoded these responses into three broad categories, including “not available,” “available and satisfied,” and “available and dissatisfied.” We assessed participants’ status on the use of recreational/illicit drugs (ever used and usage in the last 6 months) using a self-reported dichotomous response scale of “yes” and “no.”
Multivariate binary regression models were used to examine the relationship between regularity of scheduled outpatient clinic attendance, the independent predictor variables, and their interaction terms using SPSS version 22 and R software. Statistical significance was set at P<0.05.
Results
Distribution of respondents by economic and sociodemographic characteristics and regularity of outpatient clinic attendance
Of the 224 patients in this study, 197 (87.9%) were males and 27 (12.1%) were females (Table 1). Three-quarters (75.4%) of respondents were below 40 years of age. Majority (n=104, 46.4%) were Malays, private organization employees (n=137, 61.2%), with lower education (n=157, 70.1%) and monthly income of <Ringgit Malaysia (RM) 3,499 (n=163, 72.7%). Slightly over half of the study participants resided in urban locations (n=115, 51.3%; Table 1).
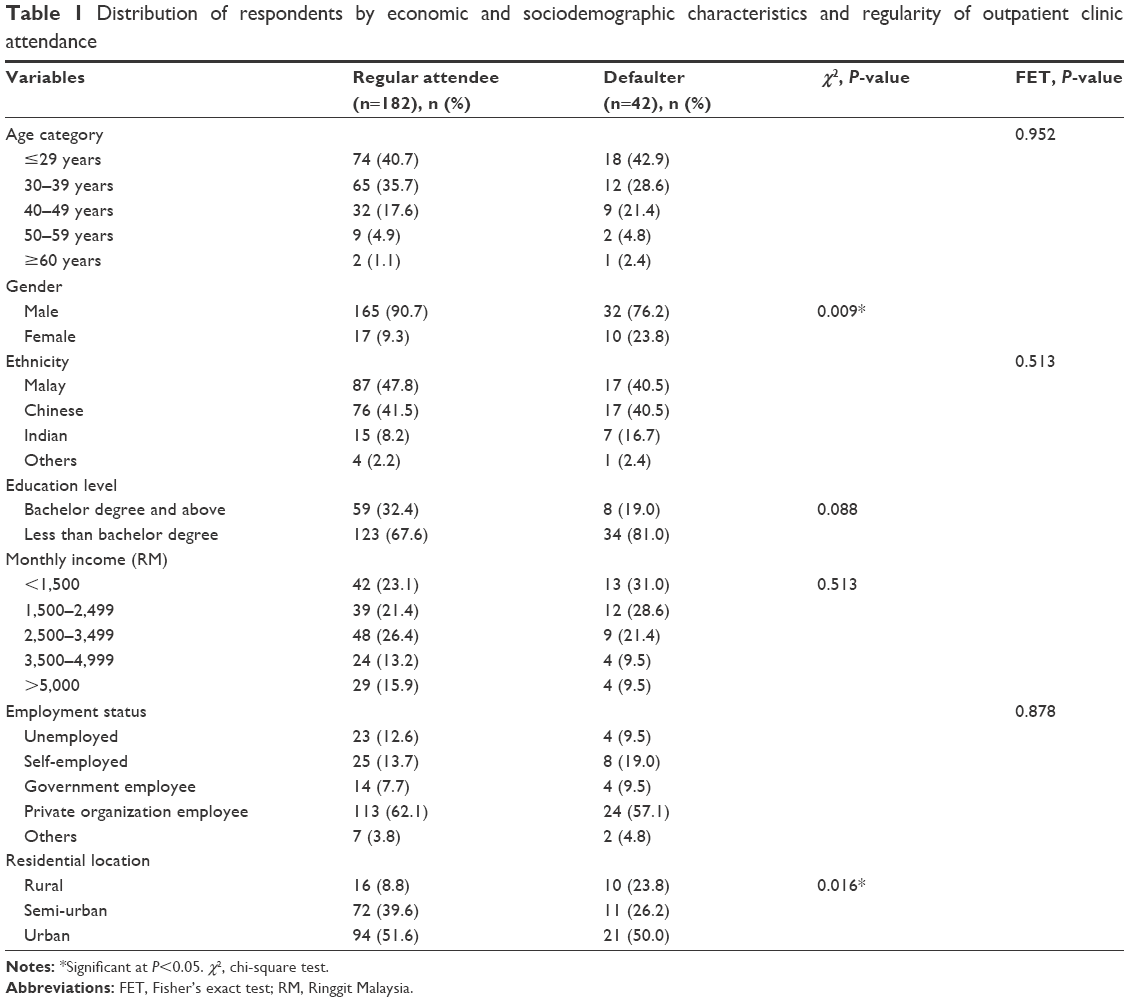 | Table 1 Distribution of respondents by economic and sociodemographic characteristics and regularity of outpatient clinic attendance |
All (100%) respondents (including the 18 dropouts) had a minimum of five scheduled visits, as per the standard mentioned earlier, within the first 6 months of ART initiation. A total of 182 (81.3%) attended all five scheduled visits and were considered regular attendees. Out of the 224 respondents in the sample, 42 (18.7%) defaulted scheduled clinic attendance at least once. Only one respondent missed more than three appointments within the study period. Majority of the defaulters were young (age ≤29 years; n=18, 42.9%), Malays (n=17, 40.5%), and Chinese (n=17, 40.5%), private organization employees (n=24, 57.1%), with lower income (<RM 2,500; n=25, 59.6%) and education (less than bachelor degree; n=34, 81.0%) level. A significantly higher prevalence of missed appointments was observed among females (n=10, 37.0%) than males (n=32, 16.2%; χ2 =6.739; df =1; P=0.009). Although prevalence of missed appointments was higher among rural residents (n=10, 38.5%), a significantly higher proportion of defaulters (n=21, 50%) resided in urban than semi-urban or rural location (χ2 =8.296; df =2; P=0.016; Table 1).
Like those included in this study, all of the 18 patients excluded from this analysis due to incomplete clinic attendance data were below 40 years of age, majority were Malays (n=13, 72.2%), private organization employees (n=13, 72.2%), with low income (n=12, 66.7%) and education level (n=14, 77.8%) and resided in urban locations (n=10, 55.6%).
Distribution of respondents by psychosocial, treatment, patient-related characteristics, and regularity of outpatient clinic attendance
Table 2 shows that the majority (n=124, 55.4%) of the respondents in the sample were homosexuals, never used any recreational drug before (n=210, 93.8%), and were satisfied with the social support they received from friends and family (n=188, 83.9%). A higher proportion (n=39, 92.9%) of the defaulters reported that they were satisfied with the social support they received, while an equal proportion of defaulters were observed among heterosexuals (n=17, 40.5%) and homosexuals (n=17, 40.5%). A significantly higher prevalence of missed appointments was observed among bisexual respondents (n=8, 47.1%; χ2 =11.174; df =2; P=0.004) than heterosexuals and homosexuals. Expectedly, a significantly lower proportion (n=12, 28.6%; χ2 =11.157; df =1; P=0.001) of respondents in the intervention group defaulted clinic attendance (Table 2).
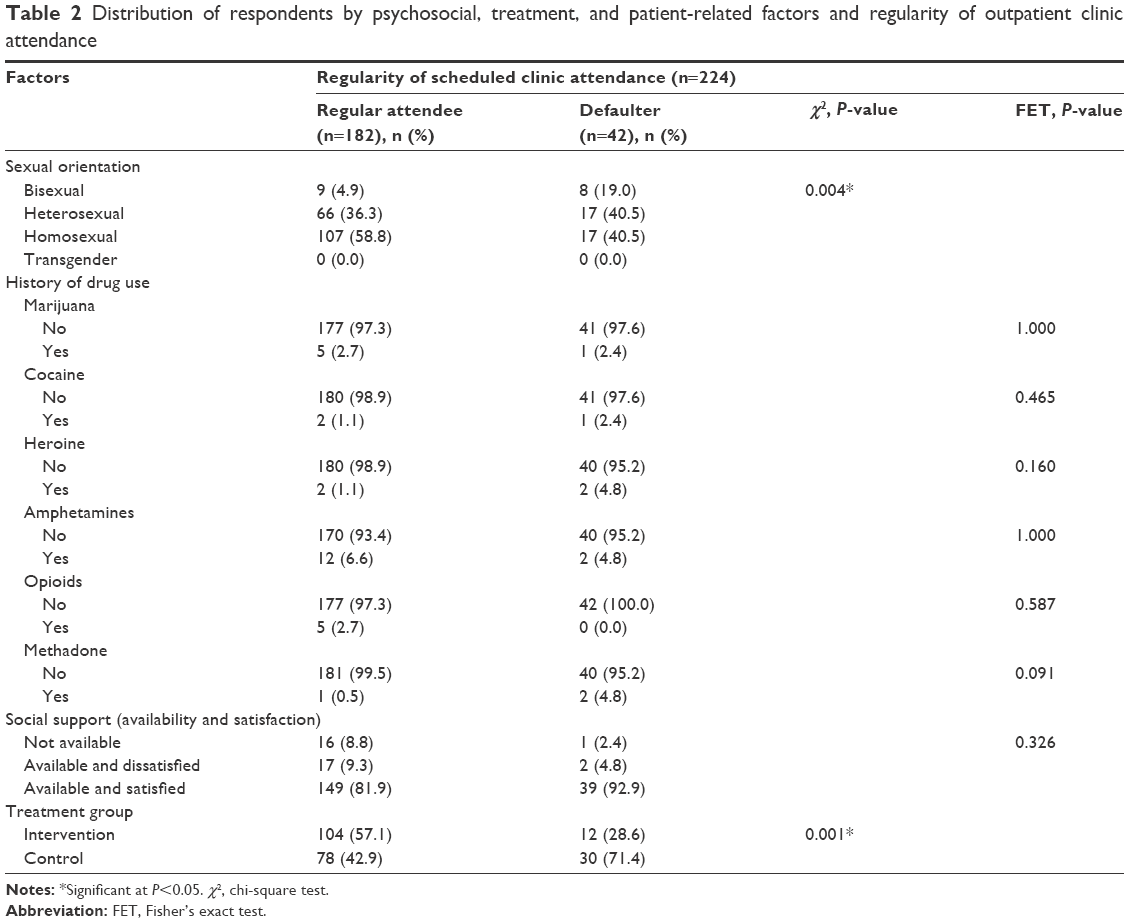 | Table 2 Distribution of respondents by psychosocial, treatment, and patient-related factors and regularity of outpatient clinic attendance |
Association of economic, sociodemographic, psychosocial, treatment, and patient-related factors with outpatient clinic attendance
We performed univariate and multivariate binary logistic regression analyses to test the association between independent predictor and outcome (regularity of scheduled outpatient clinic attendance) variables in this study. At univariate level, Table 3 shows that male respondents had three times higher odds of regular outpatient clinic attendance compared to females (odds ratio [OR] =3.033; 95% CI [1.273–7.225]; P=0.012). The results also showed that the odds of regular outpatient clinic attendance was four times higher among semi-urban residents (OR =4.091; 95% CI [1.485–11.269]; P=0.006) compared to rural residents. Similarly, the odds of regular outpatient clinic attendance was 2.7 times higher among urban residents (OR =2.798; 95% CI [1.114–7.026]; P=0.029) than rural dwellers. Although respondents who attained bachelor degree and above were observed to have twice higher odds of regular outpatient clinic attendance (OR =2.039; 95% CI [0.889–4.677]) than those with lower education levels (less than bachelor degree), this relationship did not reach statistical significance (P=0.093).
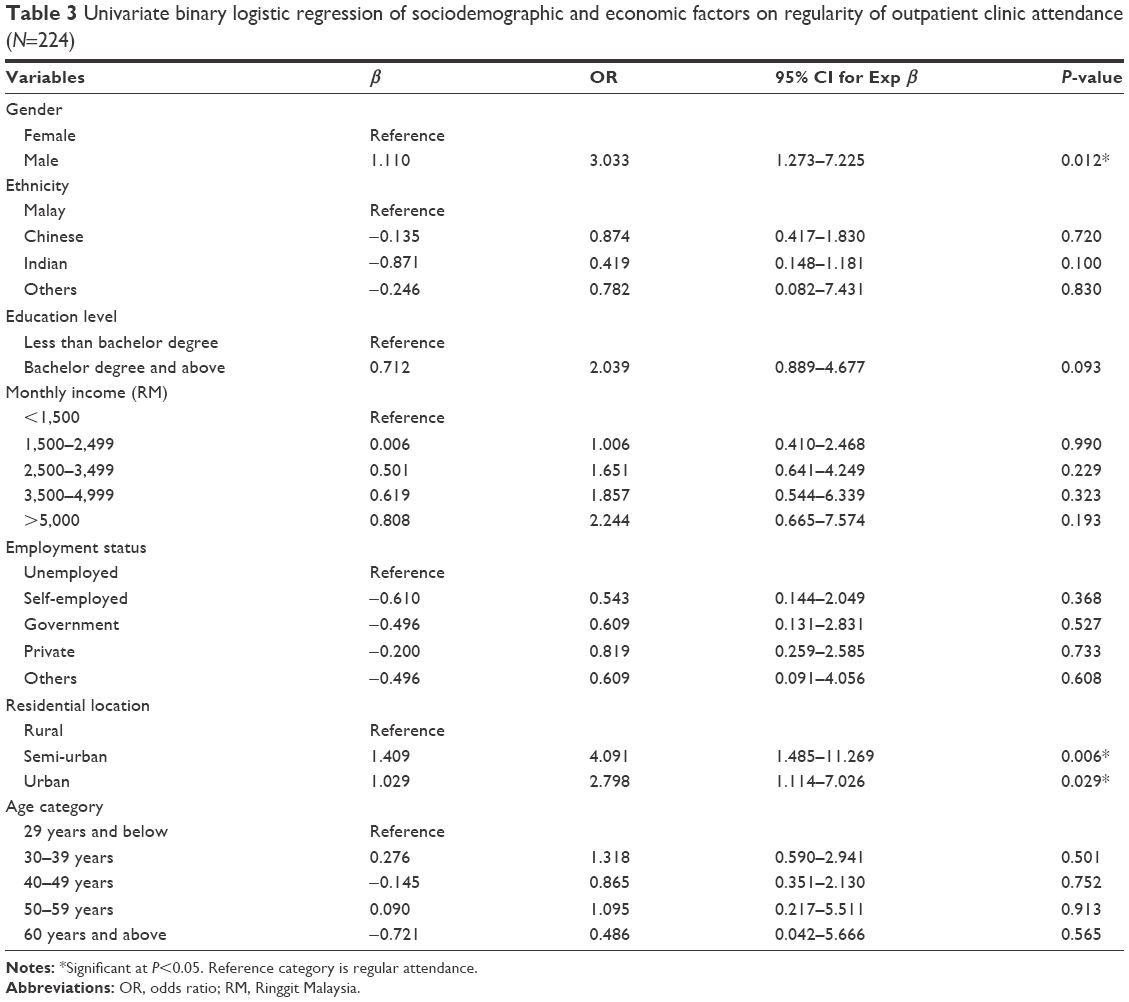 | Table 3 Univariate binary logistic regression of sociodemographic and economic factors on regularity of outpatient clinic attendance (N=224) |
Table 4 shows that the odds of regular outpatient clinic attendance was about 5.6 times higher among homosexuals (OR =5.595; 95% CI [1.898–16.494]; P=0.002) compared to bisexuals, whereas a 3.4 times higher odds of regular outpatient clinic attendance was observed among heterosexuals (OR =3.451; 95% CI [1.159–10.279]; P=0.026) compared to bisexuals. Expectedly, respondents in the intervention group had about 3.3 times higher odds of regular outpatient clinic attendance (OR =3.333; 95% CI [1.605–6.924]; P=0.001) compared to the control group respondents. Neither availability and satisfaction with social support nor history of drug use was significantly associated with outpatient clinic attendance.
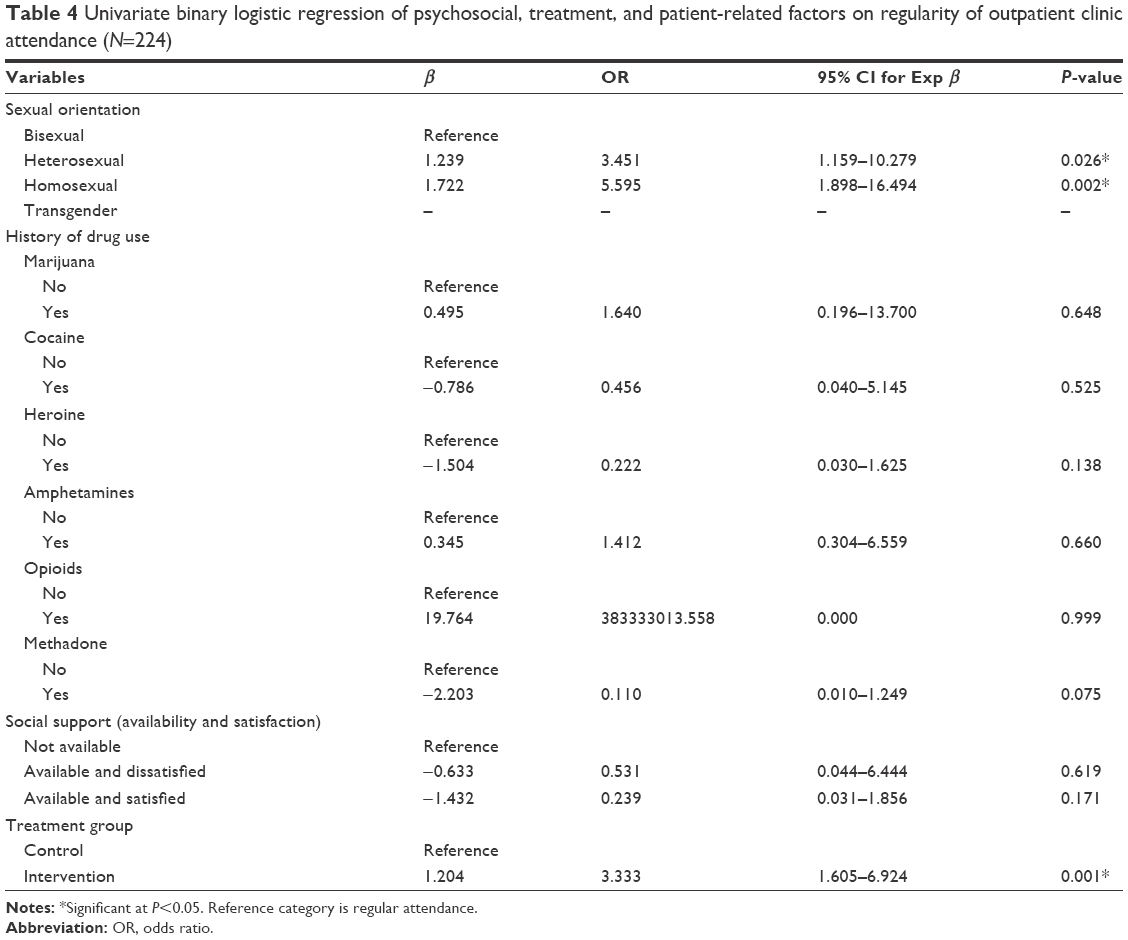 | Table 4 Univariate binary logistic regression of psychosocial, treatment, and patient-related factors on regularity of outpatient clinic attendance (N=224) |
To achieve a most parsimonious and robust multivariate regression model, variable selection process considered a significance value of <0.2527,28 at univariate analysis level, as well as biological plausibility criteria. Using the “enter method” of variable selection, all significant predictors at univariate level including age and treatment group were included in the model. After controlling for the effect of age and treatment group, a multivariate model was fitted to explore and isolate independent predictors of outpatient clinic attendance and possible interactions. The logistic regression model was statistically significant, χ2 (22) =41.159, P=0.008. The model explained 27.1% (Nagelkerke R2) of the variance in outpatient clinic attendance and correctly classified 83.0% of cases. Table 5 indicates that Indian respondents were about 24% or four times less likely to attend scheduled outpatient clinic appointments (OR =0.235; 95% CI [0.063–0.869]; P=0.030) compared to Malays. Conversely, the odds of regular outpatient clinic attendance were about 4.2 times higher among heterosexual respondents (OR =4.199; 95% CI [1.040–16.957]; P=0.044) as compared to bisexuals. No other economic, sociodemographic, psychosocial, treatment, patient-related variables, or the interaction terms examined in this model significantly predicted outpatient clinic attendance.
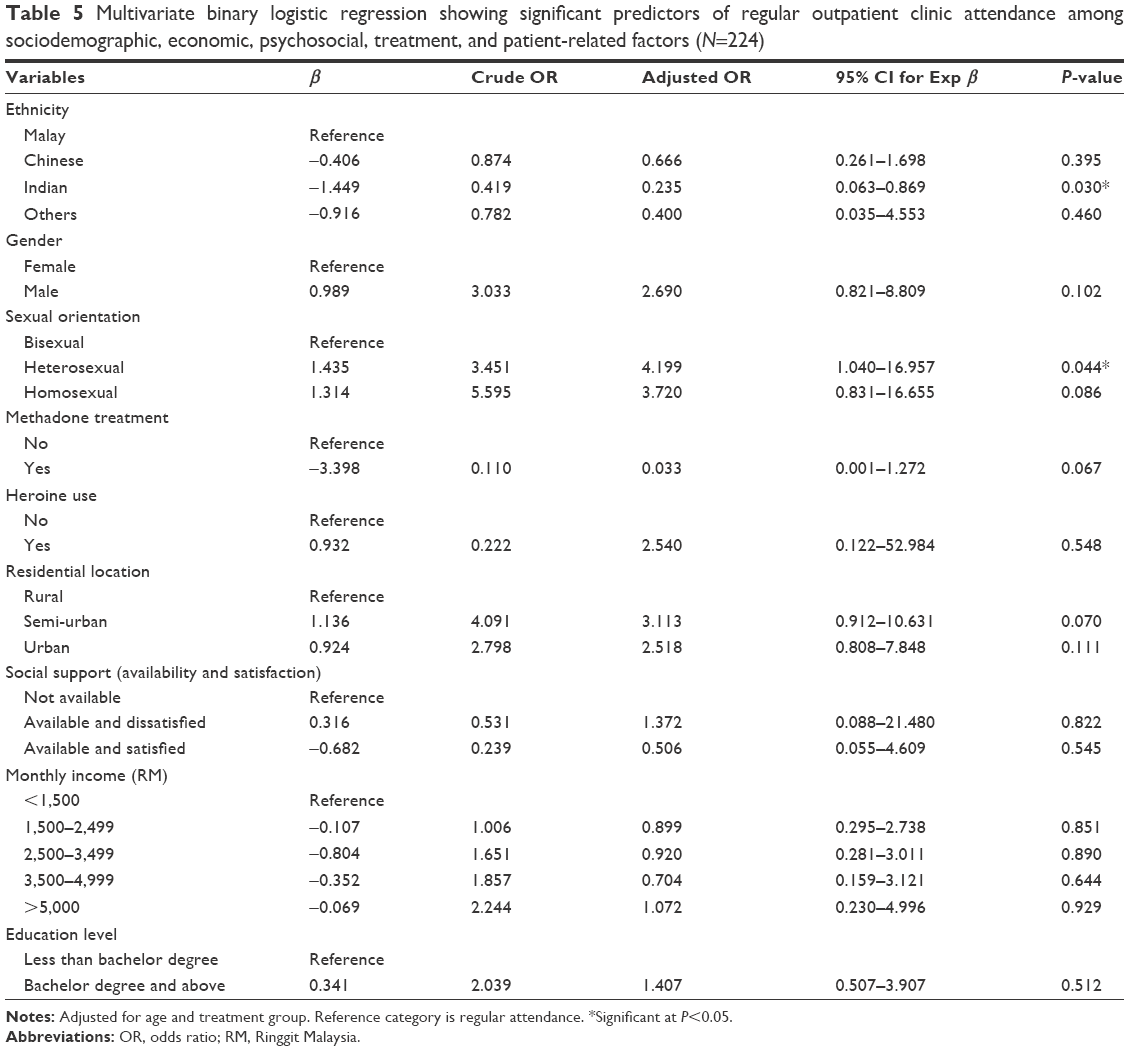 | Table 5 Multivariate binary logistic regression showing significant predictors of regular outpatient clinic attendance among sociodemographic, economic, psychosocial, treatment, and patient-related factors (N=224) |
Discussion
Study population
The age and gender characteristics of our study sample are similar to overall distribution among HIV-positive population in Malaysia.29–31 Albeit with a lower proportion compared to previous reports,32 Malays constituted the overall majority in the current study. We observed a higher income and education level among the study participants compared to previous reports elsewhere in Malaysia29,31 and Botswana.33 Four out of every five respondents in our study sample were employed compared to 64% and 75% reported in similar studies in Kelantan, Malaysia,29 and Botswana,33 respectively. Lower proportion of patients in our study resided in urban locations as compared to 81% reported in a similar study in Kenya.34
Summary of main findings
The prevalence of missed appointments among our study cohort was relatively high, particularly among females, bisexual respondents, and rural residents. We found in this study that heterosexual orientation and Indian race were significant predictors of outpatient clinic attendance. Heterosexual respondents had about 4.2 times higher odds of regular outpatient clinic attendance compared to bisexuals. Indian respondents were about four times less likely to attend scheduled outpatient clinic appointments than Malays.
Comparison with existing literature
Besides its important correlation with immune recovery2,9 and viral suppression,5–7 regular attendance of scheduled outpatient clinics also offers clinicians the opportunity to clinically assess patients on HAART for treatment progress as well as identify and address adherence and potential drug resistance problems early. Irrespective of the specific purpose of a scheduled outpatient clinic visit – be it for clinical evaluation, laboratory investigations, or drug refill – missed appointments often result in poor outcomes for patients receiving ART. In fact, poor adherence to drug refill or pickup has been proven to be a strong EWI of virologic and immunologic failure19,35 and predictor of medication adherence13 among HIV-positive patients on ART.
The problem of missed appointments among patients receiving ART appears to be a universal one, cutting across epidemic types (concentrated vs generalized) and economies (high, middle, and low). Nonattendance rates have been reported to range from 6% to 68.4%. With the exception of one study conducted in Uganda,13 studies conducted in United States, South America, Africa, and Asia among HIV-positive patients attending outpatient clinics have consistently reported prevalence rates of missed appointment above 20%.5,14,17,19,20,36 The lower prevalence (18.7%) reported in this study is probably partly due to the fact that half of the respondents in this study had received SMS and telephone call reminders for their scheduled clinic appointments throughout the study period. In addition, it is important to note that ours was a cohort initiating ART, and therefore has possibly higher than normal attendance rates. Whereas a similar rate of nonattendance was reported in a cross-sectional study among patients with chronic diseases attending an outpatient family practice clinic in Kuala Lumpur, Malaysia,37 this study reported a lower rate of missed appointments among intervention (10.3% vs 41.0%) than the control (27.8% vs 51.9%) group respondents when compared to a previous intervention study among primary care clinic attendees at seven primary care clinics in Malaysia.26 Differences in reasons for clinic attendance between these two intervention studies may probably explain these differences.
Despite being a largely male-dominated study, we found a higher prevalence of missed appointments among females in this study. This finding is in contrast with the result of a previous study among Malaysians with chronic diseases attending an outpatient family practice clinic in Kuala Lumpur, Malaysia.37 It is possible that the well-documented vulnerabilities, stigma, and discrimination often associated with HIV positivity status, particularly among females, might have influenced their clinic attendance behavior in this study. That said, our study provides further evidence to support previous reports16,17,19 that gender is not a significant predictor of outpatient clinic attendance among HIV-positive patients receiving ART. Of several similar studies conducted around the world in the past decade, only a Chinese national study of 27,504 patients receiving ART reported female gender as being significantly associated with higher likelihood of early missed visits.18
We observed that rural residents in this study had a higher prevalence of missed appointments. Given that the majority (95%) of respondents in this study resided within 100 km radius of the study location which is accessible by road and rail transport, with an average commute time of about 30 minutes to 1 hour, and an average transportation cost of RM 25–65 per visit, the argument that monthly income could have mediated this association may not be tenable among this cohort. Perhaps other psychosocial factors (such as stigma and discrimination and confidentiality concerns) and patient-level factors (such as forgetfulness and treatment fatigue) may explain these differences. It is instructive to mention that distance from clinic for rural residents not only is an issue because of travel costs but also increased time/inconvenience and associated potential loss of earnings compared to patients who live nearer. Income differentials may however be expected to play a role in the regularity of scheduled outpatient clinic attendance where additional clinic visits for special consultations/follow-up or drug pickups are required among low-income earners (<RM 1,500). It is also unclear whether commuting patterns (use of public vs private transportation) might have influenced outpatient clinic attendance among the study cohort, as it has been reported in other parts of the world.38,39
Sexual orientation of respondents in this study was associated with outpatient clinic attendance. In addition to a lower prevalence of missed appointments, heterosexual respondents in this study had significantly higher odds of regular outpatient clinic attendance than bisexual respondents. This finding is at variance with earlier reports from similar studies in the United States16,36 in which the authors reported that heterosexual orientation was associated with missing scheduled medical appointments. In other studies, reporting heterosexual and homosexual transmission as respondent’s HIV risk factor has been more commonly associated with missed appointments.40 Given the recent surge of heterosexual transmission of HIV among the Malaysian population, and the corresponding multi-sectoral efforts by the government and nongovernmental organizations (NGOs) to increase HIV awareness among most-at-risk populations (MARPs),30 it is possible that these efforts are beginning to translate to improved utilization of HIV care services by the population. Beyond the recent implementation of targeted awareness among the heterosexual-at-risk population, it remains to be seen what other factors might have led to the disproportionate level of outpatient clinic attendance between heterosexual and homosexual population in this study, the latter haven been beneficiaries of long-term prevention and control efforts and strong social support network.
The association between race/ethnicity and outpatient clinic attendance has been widely documented in the literature. In both resource-rich and resource-limited settings across the world, previous studies have established that black, African American, and non-white race/ethnicity were significantly associated with higher likelihood of missed appointments.14,16,36,41,42 Unlike in other parts of the world, race/ethnicity has been rarely associated with outpatient clinic attendance behavior among Asians.19,20 We found a significant association between Indian race and likelihood of missed outpatient clinic appointments among our study cohort. This finding is consistent with a previous report among Malaysians with chronic diseases attending an outpatient family practice clinic in Kuala Lumpur, Malaysia.37 Compared to Chinese and Malays, Indians generally constitute a small proportion of the HIV-positive population in Malaysia. This apparently low prevalence, and consequent low-risk perception, inadequate social support networks, religious coping and apparent stigma, and discrimination within the racial circle, may partly explain why the Indian HIV-positive subpopulation are at higher odds of missed outpatient clinic appointments. This is further supported by the fact that the relationship between ethnicity and outpatient clinic attendance observed in this study does not appear to have been mediated by low income, employment status, or availability and satisfaction with social support, all of which were not independently associated with outpatient clinic attendance in this study. Further follow-up studies are required to unearth the specific explanations behind this relationship.
Given the widely documented inconsistent association between respondents’ age and outpatient clinic attendance in the literature, it is not surprising that our study failed to identify any positive relationship between these variables among the study cohort. Whereas some studies reported older age18 as a significant predictor of missed appointment, others have reported the contrary.15–17,41,43–45 In most Asian studies, the relationship between age and outpatient clinic attendance has not been well established.
Unlike previous reports of similar studies among respondents in Nepal and Cambodia,19,20 this study agreed with reports by Bodenlos et al46 in failing to establish an association between outpatient clinic attendance and availability and satisfaction with social support that respondents received from their family and friends. This is probably not surprising owing to the widely available social support network provided by hospital and community-based NGOs across Malaysia, in addition to support received from close family members. To the extent that a higher proportion of defaulters in this study reported availability and satisfaction with the level of social support they received from family and friends, it would appear that other patient-level factors such as busy work schedule, treatment fatigue, low perception of ill-health, and the importance of regular clinic visits may partly explain the observed pattern.
Despite the flurry of literature evidence suggesting that sociodemographic, economic, and cultural characteristics of patients may influence their attendance of clinic appointments, these findings have not been consistently demonstrated over time and among different populations.
We believe that other behavioral (eg, alcohol use, non-HIV disclosure, stigma, and depression), patient-related (eg, self-rated perception of ill health and religious coping) and treatment-related factors (eg, side effects, comorbidities, CD4 count, and viral load), beyond the sociodemographic (ethnicity) and psychosocial (sexual orientation) factors identified in this study, may explain some of the variance in outpatient clinic attendance behavior among this study cohort. The findings from this study could be particularly useful in informing targeted interventions to address the increasingly prevalent problem of missed outpatient clinic appointments among heterosexuals and Indian HIV-positive subpopulation in Malaysia.
Limitations
This study has a number of important limitations. First, the predictors explored in this study were limited largely to economic and psychosocial factors without cognizance to other patient-related (such as beliefs, depression, perceived improvement in health status, disclosure status, personal circumstances, forgetfulness, and fasting), and system/provider-related factors that could potentially affect outpatient clinic attendance. Other treatment-related factors such as the presence of other comorbidities, baseline CD4 count, and viral load were also not considered in this analysis. Second, a qualitative explanatory study would have provided further and deeper insights into these relationships, but this was not considered as it was beyond the scope of this study.
Conclusion
Although inconsistencies in the association between sociodemographic and other predictors of outpatient clinic attendance have been documented in the literature over the years, the findings from this study provide additional support to the growing body of evidence on the potential relationship between outpatient clinic attendance and sexual orientation of respondents, particularly in concentrated epidemics and low-to-middle-income economies. To the best of our knowledge, this study is the first to establish the association between race/ethnicity and outpatient clinic attendance among HIV-positive population receiving ART in Malaysia. At the level of individual patient care, this information becomes very valuable to the pretreatment, collaborative adherence strategy planning between the patient and provider, if successful treatment outcomes are to be achieved. At program level, our finding underscores the importance of stronger intersectoral collaboration toward community system strengthening in the areas of psychosocial and economic empowerment to the success of health programs.
Acknowledgments
The authors wish to thank all the participants of this study and also acknowledge the critical role and contribution of Mrs Jayanthi Arumugam and the entire health care team of Infectious Disease Clinic, Hospital Sungai Buloh, to the successful conduct of this research. The authors received no specific funding for this research.
Author contributions
Conceived and designed the experiment: SAA, LR, FI, KSH, and APR. Performed the experiment: SAA and APR. Analyzed the data: SAA, LR, and HK. Wrote the paper: SAA. Reviewed the manuscript: SAA, LR, KSH, and NO. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Adherence to Long Term Therapies – Evidence for Action; 2003; (WHO/MNC/03.01). Available from: http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf. Accessed June 22, 2017. | ||
Anoje C, Agu KA, Oladele EA, et al. Adherence to on-time ART drug pick-up and its association with CD4 changes and clinical outcomes amongst HIV infected adults on first-line antiretroviral therapy in Nigerian hospitals. AIDS Behav. 2017;21(2):386–392. | ||
Bennett DE, Jordan MR, Bertagnolio S, et al. HIV drug resistance early warning indicators in cohorts of individuals starting antiretroviral therapy between 2004 and 2009: World Health Organization global report from 50 countries. Clin Infect Dis. 2012;54(suppl 4):S280–S289. | ||
Nachega JB, Hislop M, Dowdy DW, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann Intern Med. 2007;146(8):564–573. | ||
Brennan AT, Maskew M, Sanne I, Fox MP. The importance of clinic attendance in the first six months on antiretroviral treatment: a retrospective analysis at a large public sector HIV clinic in South Africa. J Int AIDS Soc. 2010;13(1):1. | ||
Rastegar DA, Fingerhood MI, Jasinski DR. Highly active antiretroviral therapy outcomes in a primary care clinic. AIDS Care. 2003;15(2):231–237. | ||
Sethi AK, Celentano DD, Gange SJ, Moore RD, Gallant JE. Association between adherence to antiretroviral therapy and human immunodeficiency virus drug resistance. Clin Infect Dis. 2003;37(8):1112–1118. | ||
Bastard M, Pinoges L, Balkan S, Szumilin E, Ferreyra C, Pujades-Rodriguez M. Timeliness of clinic attendance is a good predictor of virological response and resistance to antiretroviral drugs in HIV-infected patients. PLoS One. 2012;7(11):e49091. | ||
Berg MB, Safren SA, Mimiaga MJ, Grasso C, Boswell S, Mayer KH. Nonadherence to medical appointments is associated with increased plasma HIV RNA and decreased CD4 cell counts in a community-based HIV primary care clinic. AIDS Care. 2015;17(7):902–907. | ||
Walburn A, Swindells S, Fisher C, High R, Islam KM. Missed visits and decline in CD4 cell count among HIV-infected patients: a mixed method study. Int J Infect Dis. 2012;16(11):e779–e785. | ||
Kimeu M, Burmen B, Audi B, et al. The relationship between adherence to clinic appointments and year-one mortality for newly enrolled HIV infected patients at a regional referral hospital in Western Kenya, January 2011–December 2012. AIDS Care. 2016;28(4):409–415. | ||
Park WB, Choe PG, Kim SH, et al. One-year adherence to clinic visits after highly active antiretroviral therapy: a predictor of clinical progress in HIV patients. J Intern Med. 2007;261(3):268–275. | ||
Kunutsor S, Walley J, Katabira E, et al. Clinic attendance for medication refills and medication adherence amongst an antiretroviral treatment cohort in Uganda: a prospective study. AIDS Res Treat. 2010;2010:872396. | ||
Bofill L, Waldrop-Valverde D, Metsch L, Pereyra M, Kolber MA. Demographic and psychosocial factors associated with appointment attendance among HIV-positive outpatients. AIDS Care. 2011;23(10):1219–1225. | ||
Catz SL, McClure JB, Jones GN, Brantley PJ. Predictors of outpatient medical appointment attendance among persons with HIV. AIDS Care. 1999;11(3):361–373. | ||
Israelski D, Gore-Felton C, Power R, Wood MJ, Koopman C. Sociodemographic characteristics associated with medical appointment adherence among HIV-seropositive patients seeking treatment in a county outpatient facility. Prev Med. 2001;33(5):470–475. | ||
Nagata D, Gutierrez EB. Characteristics of HIV patients who missed their scheduled appointments. Rev Saude Publica. 49. Epub 2015 Dec 31. | ||
Zhang Y, Dou Z, Sun K, et al. Association between missed early visits and mortality among patients of china national free antiretroviral treatment cohort. J Acquir Immune Defic Syndr. 2012;60(1):59–67. | ||
Ayer R, Kikuchi K, Ghimire M, et al. Clinic attendance for antiretroviral pills pick-up among HIV-positive people in Nepal: roles of perceived family support and associated factors. PLoS One. 2016;11(7):e0159382. | ||
Daigle GT, Jolly PE, Chamot EA, et al. System-level factors as predictors of adherence to clinical appointment schedules in antiretroviral therapy in Cambodia. AIDS Care. 2015;27(7):836–843. | ||
Lam Y, Westergaard R, Kirk G, et al. Provider-level and other health systems factors influencing engagement in HIV care: a qualitative study of a vulnerable population. PLoS One. 2016;11(7):e0158759. | ||
Gurol-Urganci I, de Jongh T, Vodopivec-Jamsek V, Atun R, Car J. Mobile phone messaging reminders for attendance at healthcare appointments. Cochrane Database Syst Rev. 2013;12:CD007458. | ||
Milne RG, Horne M, Torsney B. SMS reminders in the UK national health service: an evaluation of its impact on “no-shows” at hospital out-patient clinics. Health Care Manage Rev. 2006;31(2):130–136. | ||
Downer SR, Meara JG, Da Costa AC. Use of SMS text messaging to improve outpatient attendance. Med J Aust. 2005;183(7):366. | ||
Downer SR, Meara JG, Da Costa AC, Sethuraman K. SMS text messaging improves outpatient attendance. Aust Health Rev. 2006;30(3):389–396. | ||
Leong KC, Chen WS, Leong KW, et al. The use of text messaging to improve attendance in primary care: a randomized controlled trial. Fam Pract. 2006;23(6):699–705. | ||
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3(1):1. | ||
Hosmer DW Jr, Lemeshow S. Applied Logistic Regression. John Wiley & Sons, Hoboken, NJ, USA; 2005. | ||
Hasanah CI, Zaliha AR, Mahiran M. Factors influencing the quality of life in patients with HIV in Malaysia. Qual Life Res. 2011;20(1):91–100. | ||
Malaysia 2015: Global AIDS Response Country Progress Report. Putrajaya: Ministry of Health Malaysia; 2015. | ||
Yagoub U, Bulgiba A, Devi P, Ali M, Lee C, Zamri C. Factors affecting adherence level to HAART (Adherence predictors) in Kuala Lumpur, Malaysia. Life Sci J. 2012;9(4):3600–3603. | ||
Malaysia AIDS Council. Annual Report. 2013. Available from: http://www.mac.org.my/v3/wp-content/uploads/2014/05/Annual-Report-2013_A4_FA_22052013-web.pdf. Accessed July 3, 2017. | ||
Ndubuka NO, Ehlers VJ. Adult patients’ adherence to anti-retroviral treatment: a survey correlating pharmacy refill records and pill counts with immunological and virological indices. Int J Nurs Stud. 2011;48(11):1323–1329. | ||
Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–1845. | ||
El-Khatib Z, Katzenstein D, Marrone G, et al. Adherence to drug-refill is a useful early warning indicator of virologic and immunologic failure among HIV patients on first-line ART in South Africa. PLoS One. 2011;6(3):e17518. | ||
Mugavero MJ, Lin HY, Allison JJ, et al. Racial disparities in HIV virologic failure: do missed visits matter? J Acquir Immune Defic Syndr. 2009;50(1):100. | ||
Zailinawati AH, Ng CJ, Nik-Sherina H. Why do patients with chronic illnesses fail to keep their appointments? A telephone interview. Asia Pac J Public Health. 2005;18(1):10–15. | ||
Dasgupta S, Kramer MR, Rosenberg ES, Sanchez TH, Reed L, Sullivan PS. The effect of commuting patterns on HIV care attendance among men who have sex with men (MSM) in Atlanta, Georgia. JMIR Public Health Surveill. 2015;1(2):e10. | ||
Reif S, Golin CE, Smith SR. Barriers to accessing HIV/AIDS care in North Carolina: rural and urban differences. AIDS Care. 2005;17(5):558–565. | ||
Giordano TP, Hartman C, Gifford AL, Backus LI, Morgan RO. Predictors of retention in HIV care among a national cohort of US veterans. HIV Clin Trials. 2015;10(5):299–305. | ||
Mugavero MJ, Lin HY, Willig JH, et al. Missed visits and mortality in patients establishing initial outpatient HIV treatment. Clin Infect Dis. 2009;48(2):248–256. | ||
Traeger L, O’Cleirigh C, Skeer MR, Mayer KH, Safren SA. Risk factors for missed HIV primary care visits among men who have sex with men. J Behav Med. 2012;35(5):548–556. | ||
Howe CJ, Cole SR, Napravnik S, Eron JJ Jr. Enrollment, retention, and visit attendance in the University of North Carolina Center for AIDS Research HIV clinical cohort, 2001–2007. AIDS Res Hum Retroviruses. 2010;26(8):875–881. | ||
Krishnan S, Wu K, Smurzynski M, et al. Incidence rate of and factors associated with loss to follow-up in a longitudinal cohort of antiretroviral-treated HIV-infected persons: an AIDS Clinical Trials Group (ACTG) Longitudinal Linked Randomized Trials (ALLRT) analysis. HIV Clin Trials. 2011;12(4):190–200. | ||
Lee S, Lee SH, Lee SJ, et al. Predictors of poor retention in care of HIV-infected patients receiving antiretroviral therapy in Korea: five-year hospital-based retrospective cohort study. J Korean Med Sci. 2016;31(3):376–381. | ||
Bodenlos JS, Grothe KB, Whitehead D, Konkle-Parker DJ, Jones GN, Brantley PJ. Attitudes toward health care providers and appointment attendance in HIV/AIDS patients. J Assoc Nurses AIDS Care. 2007;18(3):65–73. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.