")
Back to Journals » International Journal of Women's Health » Volume 12
Socio-Demographic Determinants of Mortality from Chronic Noncommunicable Diseases in Women of Reproductive Age in the Republic of Georgia: Evidence from the National Reproductive Age Mortality Study (2014)
Authors Lomia N , Berdzuli N , Pestvenidze E , Sturua L, Sharashidze N , Kereselidze M, Topuridze M, Antelava T, Stray-Pedersen B , Stray-Pedersen A
Received 23 October 2019
Accepted for publication 27 January 2020
Published 27 February 2020 Volume 2020:12 Pages 89—105
DOI https://doi.org/10.2147/IJWH.S235755
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Nino Lomia,1 Nino Berdzuli,1 Ekaterine Pestvenidze,1 Lela Sturua,2 Nino Sharashidze,3 Maia Kereselidze,4 Marina Topuridze,5 Tamar Antelava,6 Babill Stray-Pedersen1,7,†, Arne Stray-Pedersen1,8
1Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway; 2Department of Noncommunicable Diseases, National Center for Disease Control and Public Health, Tbilisi, Georgia; 3Department of Clinical and Research Skills, Faculty of Medicine, Iv. Javakhishvili Tbilisi State University, Tbilisi, Georgia; 4Department of Medical Statistics, National Center for Disease Control and Public Health, Tbilisi, Georgia; 5Health Promotion Division, Department of Noncommunicable Diseases, National Center for Disease Control and Public Health, Tbilisi, Georgia; 6EVEX Medical Corporation, Tbilisi, Georgia; 7Department of Obstetrics and Gynecology, Rikshospitalet, Oslo University Hospital, Oslo, Norway; 8Department of Forensic Sciences, Oslo University Hospital, Oslo, Norway
†Dr Babill Stray-Pedersen passed away on 24 April, 2019
Correspondence: Nino Lomia Tel +995 595 197055
Email [email protected]
Purpose: Worldwide, noncommunicable diseases (NCDs) are the leading cause of premature death of women, taking the highest toll in developing countries. This study aimed to identify key socio-demographic determinants of NCD mortality in reproductive-aged women (15– 49 years) in Georgia.
Materials and Methods: The study employed the verbal autopsy data from the second National Reproductive Age Mortality Survey 2014. Univariate and multivariate logistic regression models were fitted to explore the association between each risk factor and NCD mortality, measured by crude and adjusted odds ratio (AOR) with respective 95% confidence intervals (95% CI).
Results: In the final sample of 843 women, 586 (69.5%) deaths were attributed to NCDs, the majority of which occurred outside a hospital (72.7%) and among women aged 45– 49 years (46.8%), ethnic Georgians (85.2%), urban residents (60.1%), those being married (60.6%), unemployed (75.1%) or having secondary and higher education (69.5%), but with nearly equal distribution across the wealth quintiles. After multivariate adjustment, the odds of dying from NCDs were significantly higher in women aged 45– 49 years (AOR=17.69, 95% CI= 9.35 to 33.50), those being least educated (AOR=1.55, 95% CI= 1.01 to 2.37) and unemployed (AOR=1.47, 95% CI= 1.01 to 2.14) compared, respectively, to their youngest (15– 24 years), more educated and employed counterparts. Strikingly, the adjusted odds were significantly lower in “other” ethnic minorities (AOR=0.29, 95% CI= 0.14 to 0.61) relative to ethnic Georgians. Contrariwise, there were no significant associations between NCD mortality and women’s marital or wealth status, place of residence (rural/urban) or place of death.
Conclusion: Age, ethnicity, education, and employment were found to be strong independent predictors of young women’s NCD mortality in Georgia. Further research on root causes of inequalities in mortality across the socioeconomic spectrum is warranted to inform equity- and life course-based multisectoral, integrated policy responses that would be conducive to enhancing women’s survival during and beyond reproduction.
Keywords: women’s health, mortality, noncommunicable diseases, socioeconomic factors, education, unemployment
Introduction
Worldwide, women, even during their fertile years, are increasingly facing the disproportionate, and often neglected, burden of chronic noncommunicable diseases (NCDs), collectively accounting for 65% (18 million) of all female deaths each year, and largely driven by the gains in life expectancy and population aging.1–4 Concurrently, the ongoing globalization processes, along with rapid urbanization, as a natural concomitant of industrialization and modernization, fuel the upsurge in four shared risk factors of NCDs, such as unhealthy diet, physical inactivity, smoking, and alcohol use, with girls and young adult women increasingly affected.4,5 Owing to this double-edged sword of progress, NCDs, once considered “diseases of affluence”, are now gradually replacing communicable diseases and playing an accelerating role in less developed economies, defined elsewhere as “a race against time”.3–5 This unhealthy trend in chronic diseases reflects the epidemiologic transition in low- and middle-income countries (LMICs), showing higher premature NCD mortality rates in those aged 15–59 years compared to high-income countries (HICs), while currently bearing 82% (4.7 million) of this burden among women aged 30–70 years.4–7 What is more, NCDs have progressively become the leading causes of mortality of reproductive-aged women (15–49 years) in most World Health Organization (WHO) regions, outnumbering deaths related to maternal conditions (44% vs 7%).8,9
There is a wide recognition, though, that the socioeconomic gradient of the risk and disease distribution also tracks with this shift. 10−11 Underlying macro-level socioeconomic and political factors, translated into social stratification based on education, occupation, income, gender and race/ethnicity, broadly known as social determinants, shape women’s exposure and vulnerability to risk behaviors and access to health services that influence their health outcomes and well-being.4,6,9,10−13 While inequalities in women’s health that are rooted in social determinants vary across and within countries, accumulated evidence base both in developed and developing settings consistently points to a clear gradient in women’s NCD-related mortality by educational attainment, employment and wealth status, along with age, ethnicity, marital status and place of residence.4–6,14–18 Responding to these challenges requires a holistic approach to women’s health across the life course, including understanding the socioeconomic patterns of the growing chronic disease burden, thus looking at the “cause of the cause” to identify actions outside health care systems and promote evidence-based equitable health.1,4,6,10−12 However, there continues to be a dearth of nationally representative data on the relationship between the multiple dimensions of young women’s social positioning and NCD mortality in LMICs. This particularly applies to the former Soviet Union (FSU) countries, like Georgia, which have been hit hardest by the transition from centralized to a market economy.17,18
Georgia is one of the most ethnically, culturally and religiously diverse countries in the Caucasus Region of Eurasia, with an estimated population of four million. Nearly half of the country population are represented by females (52.3%) and rural residents (48.0%).19,20 Currently, ethnic Georgians form 86.8% of the total population, while Azerbaijanis (6.3%) and Armenians (4.5%) constitute the largest ethnic minorities.20 The dominant religion is Georgian Orthodox Christianity (83.4%), with religious minorities headed by Muslims (10.7%).20 Since the breakup of the Soviet Union in 1991, Georgia has experienced the transition from a low-income- to a middle-income country owing to the continued rapid economic development. In 2013, the country ranked 79th on the Human Development Index, benefiting from the increase in life expectancy at birth up to 79 years for females and 70 years for males in 2012.20,21 However, as in the other FSU republics,18 economic and political uncertainties of the transition period, accompanied by the internal armed conflicts, have diminished the impact of economic growth by escalating unemployment, migration, divorce, impoverishment and wide income inequalities,21 provoking thereby, so-called, “four D’s” - “disruption”, “deprivation”, “disease” and “death”.22 Together with vanishing social welfare, a deficient health care system with subsequent mass privatization of health facilities and proliferation of direct out-of-pocket payments for health services and pharmaceuticals likely interacted with cultural and economic factors to magnify the effects of transition on mortality.23,24 In 2012, public spending on healthcare represented 1.7% of GDP, suggesting a significant mismatch between the very limited government resources devoted to health and existing needs.21 In the same year, only 8% of the population was insured in private insurance, while 36% were covered by state insurance and 56% were uninsured.21
The fundamental economic, social and cultural changes in the country have coincided with a pronounced shift in the burden of disease, with NCDs currently comprising 93% of total deaths, including 19% of female premature deaths.25 An alarming trend in underlying proximal risk factors such as physical inactivity (22.3%), overweight (54.2%) and obesity (28.5%) in adult Georgian women (≥18 years), alongside the growing smoking epidemic in younger urban educated females (<40 years), is the subject of increasing concern.26,27 This pattern is consistent with that in the other FSU countries, including Russia, where 46.8% of mortality in women aged 15–49 years is likely attributable to behavioral risk factors.28 Evidence from the two, 2008 and 2014 National Reproductive Age Mortality Surveys (RAMOS 2008 and RAMOS 2014) in Georgia indicated NCDs to be the greatest threat for women’s health during their fertile years, being responsible for over two-thirds of deaths in both 2006 and 2012, with cancer and cardiovascular diseases (CVD) taking a major tall.29,30 In fact, 7 of the 10 leading specific causes of death in 2012 were due to NCDs, dominated by breast and cervical cancers, followed by cerebrovascular diseases.30 However, these studies, focusing on mortality levels, cause-specific patterns and trends over time, have not examined to what extent underlying social determinants impact predominant NCD mortality in women during their child-bearing years.
Considering the profound shortage of such information in the country and overall in the region, the present study aimed to explore key demographic and socioeconomic determinants of NCD mortality in women of reproductive age (15–49 years) who died in Georgia in 2012, using the data from the second RAMOS 2014, conducted by the National Center for Disease Control and Public Health (NCDC&PH).
Materials and Methods
Study Population and Data Sources
The data for the repeat National RAMOS 2014 were collected from March to December 2014 through the verbal autopsy (VA) interviews with family members or other close caregivers of all deceased women aged 15–49 years, identified based on multiple sources of mortality data available in Georgia for the year 2012. Information on premortem illness signs and symptoms, as well as socio-demographic characteristics and place of death was obtained by skilled interviewers using the VA instrument developed for the first national RAMOS 2008.29,30 Of the 913 eligible deaths, 878 VAs were successfully completed, thus yielding a response rate of 96.2%.
Physician-certified VA (PCVA) approach was used to assign the most probable underlying cause to each death using the International Classification of Diseases, 10th revision (ICD-10).31 Based on the Global Burden of Disease (GBD) classification,2 VA-derived causes of death were then categorized into three broad groups: Communicable, maternal, neonatal, and nutritional disorders; NCDs; and Injuries. An additional fourth group of Undetermined causes incorporated all deaths assigned ill-defined and unknown codes. The detailed data collection and cause-of-death certification approaches for the RAMOS 2014 have been previously described elsewhere.30
Dependent Variable
The primary outcome was aggregated NCD mortality. This broad mortality group predominantly included deaths attributed to cancer, cardiovascular disorders, and chronic respiratory and digestive diseases, along with all other relatively less represented conditions. In the current study, NCD-related death is considered as the binary dependent variable, with two possible values coded as 1 (yes) and 0 (no).
Independent Variables
The independent variables have been chosen on the basis of existing literature and availability of data. Key demographic and socioeconomic variables, considered in the analysis, were either based on the original coding or aggregated into broader categories to increase the power for the study. Factors examined included women’s age (15–24, 25–34, 35–44, and 45–49 years), ethnicity (Georgian, Azerbaijani, Armenian, and other), marital status (never married, currently married, and formerly married, including divorced, separated and widowed), educational attainment (incomplete secondary, and complete secondary or higher, including technical college and university), as well as the current employment status (employed and unemployed). The composite wealth index, developed based on the ownership of household durable assets, housing characteristics and services (TV, refrigerator, landline and mobile telephone, video player, car, vacation home, housing tenure, room number, roofing materials, cooking fuel, electricity, water supply, and sanitation facilities), served as a proxy for wealth status (poorest, poorer, middle, richer and richest). In addition, place of death (hospital or any other place, but mostly home) was also used in the analysis as a proxy for access to health care during the terminal illness.
Statistical Analysis
Principal component analysis (PCA), specifically the first principal component, was employed to construct first separate urban, rural and common household proxy wealth indices using the dichotomized area-specific and common material circumstances.32 Area-specific wealth indices were then regressed on a common index and combined to generate a single composite wealth index for each household, which were finally ranked into wealth quintiles, as: poorest, poorer, middle, richer and richest.32,33
Descriptive statistics were used to summarize the findings for selected variables (all categorical), expressed as the absolute numbers and percentages. Records with missing data were removed from the analysis (n= 35, <5%). Proportions were compared using the Pearson’s chi-square test or Fisher’s exact test, as appropriate. Univariate and multivariate binary logistic regression models were then fitted to explore the association between each risk factor and NCD mortality. All explanatory variables were simultaneously included in the multivariate regression model. A likelihood ratio test was then employed to check all biologically plausible interaction terms, with none emerged to be statistically significant (data not shown). The goodness-of-fit of the final main effect model was confirmed by the Hosmer–Lemeshow test.34 The results were reported as crude and adjusted odds ratios with corresponding 95% confidence intervals (COR and AOR, 95% CI). A two-tailed p-value of <0.05 was considered statistically significant. All the analyses were performed using SPSS version 21.0 (IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.)35 and Stata version 14.2 (StataCorp LP, College Station, TX, USA).36
Ethical Consideration
Ethical clearance for this study was received from the Institutional Review Board of the NCDC&PH and the Regional Committees for Medical and Health Research Ethics South East Norway. Written informed consent was obtained from all respondents prior to interviews. The study protocol and conduct adhered to the principles laid down in the Declaration of Helsinki.
Results
Characteristics of the Study Population
The final sample comprised 843 women of reproductive age (15–49 years), with complete data for each risk factor of interest (Table 1). The mean age at death was 39.35 ± 8.84 years. Overall, the majority were ethnic Georgians (83.2%), currently married (59.5%), and urban dwellers (59.2%). Nearly three-quarters (71.2%) of the deceased had at least a secondary level of education and were unemployed (74.1%). Only about one-third (27.1%) of deaths occurred in a hospital, in contrast to the overwhelmingly common other place of death (72.9%), yet with the highest share of home deaths (60.0%, data not shown).
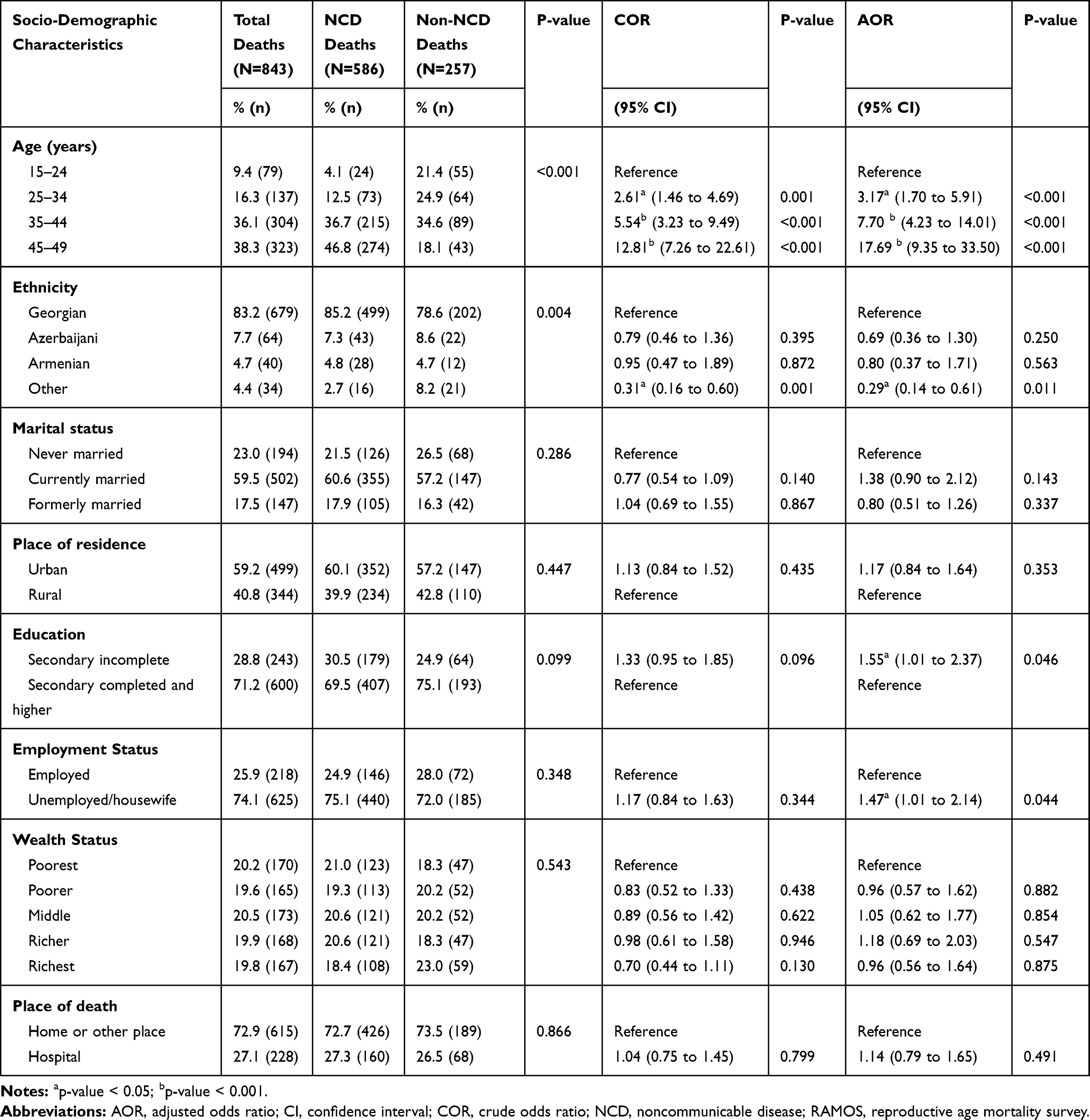 |
Table 1 Socio-Demographic Determinants of Noncommunicable Disease Mortality in Women of Reproductive Age Who Died in 2012: Georgia RAMOS 2014 |
Table 1 presents the socio-demographic characteristics of 586 (69.5%) women who died from NCDs. As indicated, women in the oldest age group (45–49 years) were at significantly higher risk (46.8%) of dying from chronic diseases than their younger counterparts. The same holds true for married women (60.6%) with respect to their single (21.5%) or formally married (17.9%) peers. The proportionate share of NCD mortality was far higher (85.2%) among ethnic Georgians than among the ethnic minority groups, ranging from 7.3% in Azerbaijanis to 4.8% in Armenians and 2.7% in other ethnic minorities. The likelihood of NCD death among urban women was remarkably higher (60.1%) than among rural dwellers (39.9%), as was among least literate (69.5%) and unemployed (75.1%) women compared to their more educated and employed counterparts. There was a relatively equal distribution of NCD-attributed deaths across wealth quintiles. Women with NCDs were much more likely to die notably at their own home (72.7%) than in a hospital (27.3%).
Predictors of NCD-Attributed Mortality
Table 1 summarizes the results of the univariate and multivariate regression, showing the crude and adjusted effects of each selected risk factor on the odds of NCD-attributed mortality. As can be seen from the final multivariate model, age, ethnicity, education, and employment status were significant independent predictors of women’s mortality due to NCDs during their reproductive years.
As expected, both the crude and adjusted odds of dying from NCDs tended to significantly increase with advance in age, peaking in the age range of 45–49 years and yielding 17.69 (95% CI=9.35 to 33.50, p<0.001) times higher than that in the youngest age group (15–24 years) in the final model. Compared to ethnic Georgians, all of the ethnic minority groups had the lower odds of NCD death. However, this effect was only statistically significant for other ethnic minorities, being slightly attenuated upon multivariate adjustment (AOR=0.29, 95% CI=0.14 to 0.61, p=0.011). Although the adjusted odds of NCD mortality, unlike unadjusted ones, were found to be greater in single women relative to their married counterparts, with the reverse being true for divorced and widowed women, none of these associations reached statistical significance in either model. The same holds true for place of residence, with urban women exhibiting the non-significant excess mortality due to NCDs both before and after mutual adjustment (Table 1).
Education and employment status both had an inverse effect on NCD mortality, which emerged to become statistically significant (p<0.05) after adjustment for other fitted variables. Namely, in the final model, women with incomplete secondary education were 1.55 times (95% CI=1.01 to 2.37, p=0.046) more likely to die from chronic diseases relative to their more literate counterparts. Likewise, unemployed women appeared to have 47% (AOR=1.47, 95% CI=1.01 to 2.14, p=0.044) greater odds of this fatal outcome as compared to their working peers. By contrast, there were no statistically significant discrepancies in NCD mortality across the wealth quintiles, although women from the “middle” and “richer” quintiles tended to have the slightly higher adjusted, but not unadjusted, odds of NCD death with respect to their poorest counterparts. Strikingly, both the univariate and multivariate analyses revealed that women with NCDs were more likely to seek care in a hospital during their terminal illness. However, this association appeared to be non-significant either before or after controlling for other variables (Table 1).
Discussion
Drawing on the recommendations from the WHO Commission on Social Determinants of Health, understanding the underlying mechanisms and pathways linking women’s social determinants with avoidable NCD mortality is central to challenging the root causes of health inequities and inequalities.10–12 This, in turn, is a core to achieving one of the United Nations Sustainable Development Goals (SDG 3, target 3.4) by the year 2030,37 as well as the WHO “25 by 25” target by 2025.38
Our study, based on the second National RAMOS 2014 data, identified significant disparities in reproductive-aged women’s premature NCD mortality by age, ethnicity, education and employment status, though this was not true for the marital status, rural-urban place of residence, household wealth, and place of death. We notably found women’s advanced age, low level of educational attainment and unemployment to be predictive of a higher risk of NCD mortality, while being of “other” ethnic origin emerged as a strong protective factor against this fatal outcome.
As expected, age had a strong positive effect on NCD mortality, indicating that the older a woman, the more likely that she would die from chronic diseases. Age, as a marker of time, is consistently among the major precipitants of death due to NCDs,2,3,9,13 provided that it captures the duration of deleterious exposures and accumulation of various NCD risk factors over the lifespan.39,40 It has been widely acknowledged that effects of these factors start to exponentially increase in the fifth decade,39,40 thus in parallel to women’s reproductive aging (e.g. a marked decline in endogenous estrogen’s cardioprotective effect during the menopausal transition).41 Moreover, the most promising epigenetic biomarker of aging, known as the epigenetic clock, has permitted to detect “accelerated biological aging”, denoting substantial deviations from individuals’ actual chronological age that has been largely linked to unhealthy behaviors, cancer, diabetes, CVD, and mortality risk.12,42 This has been reaffirmed by the most recent research, proposing age-related global disease and death burden as a new metric of population aging and identifying 92 age-related GBD causes to be vastly dominated by NCDs (81), namely neoplasms (35) and CVD (13), albeit with wide variations in the levels, trends, and the onsets of this burden across countries.43 For example, adults in low Socio-demographic Index (SDI) countries, including Russia, were found to accrue age-related disease burden at earlier ages compared to those in high SDI countries, with Central and Eastern Europe, and Central Asia overall exhibiting the worst performance (56.6%).43 Hence, in common with these findings, the observed association in our study reinforces the well-established notion that chronic diseases evolve insidiously incorporating a complex confluence of multiple intertwined factors that vary in importance as adults age.44 Therefore, to ensure the women’s healthspan extension, it would be beneficial to mitigate an advancement or initiate the reversal of accelerated biological aging by targeting risk factors amenable to interventions.42 This, in turn, should be viewed through the life-course perspective that implicates understanding the age-specific priorities for women’s health and addressing NCD prevention and control in its earliest stages.1,4,45
The present study, however, provides striking evidence, showing the NCD mortality advantage of all the ethnic minority groups relative to native Georgians, though such a protective effect only reached statistical significance for women of “other” ethnic origin. While the ethnic composition of our study sample closely mirrors that of Georgia’s population in general,20 the observed trend is surprising given the social stratification patterns in the country, whereby ethnic minorities, often with little integration into the local society and language barriers, tend to lag behind their native compatriots in many respects as a legacy of the Soviet era.21 Still, several earlier epidemiological studies from the US and Europe have documented an analogous mortality paradox (“Hispanic paradox”, “Immigrant paradox”, “Muslim paradox”), although highlighting substantial heterogeneity by specific cause categories, not examined in our study.16,46–48 Likewise, previous research in the post-communist Central Asian countries identified the “Russian mortality paradox”, suggesting the excess all-cause, cancer and CVD mortality in more privileged ethnic Russian females (and males) aged 20–59 years relative to those from titular ethnic groups.49,50 Beyond long-standing concerns arising from data artefacts and mixed ancestry,16,46,49,50 one hypothesized explanation of this phenomenon lies in differential susceptibility to most common NCDs, reflecting the complex gene–environment interactions during the life course (including in utero and early childhood).12,51,52 Another explanatory hypothesis for such resilience invokes buffering effects of unique cultural, religious (e.g. Muslim identity) and linguistic factors, shaping the protective lifestyles (e.g. smoking and drinking norms), dietary habits (e.g. Mediterranean), and health (e.g. reproductive) and social support practices across generations.16,46–51 Alternatively, it has been suggested that differential exposure to and adoption of global and local cultural forces may affect the timing and patterning of acculturation and westernization of lifestyles and behaviors (nutrition transition, sedentariness, smoking and alcohol consumption, and reproductive factors) and thereby the pace of health transition with subsequent onset of adverse outcomes.46,50–53 Furthermore, the observed ethnic gradient may reflect the variations in vulnerability and coping responses to psychosocial stress experienced during the economic transition in the country, which has been amplified by unresolved internal conflicts with two separatist regions and the recent war with Russia (2008).18,21,54,55 Moreover, the resultant massive influx of internally displaced ethnic Georgians (260,000 as of 2014), and a large out-migration of ethnic minorities (>80% of Ukrainians, Russians, Jews, and Greeks) could have substantially contributed to a widening ethnic gap in women’s NCD mortality.21,56 Noticeably, Georgia holds the third place (after Albania and Kazakhstan) among the 25 East European and FSU nations in the share of the population lost to external migration (both forced and voluntary), facing the current wave of bidirectional “feminized” labor outflow (43% in 2012), largely driven by the exodus of young native Georgian women.21,56 This, in turn, may lend support to the plausible role of health-selective migration in ethnic divergence of mortality, inferring the greater likelihood of healthier individuals to migrate (“healthy migrant effect”) and those with poorer health to return (“salmon bias”).16,46–48,51,57 According to the recent survey among returned migrants in Georgia, 92% of respondents assessed their health status as good prior to emigration, but only 59% considered it as good after departure, 57% claimed health care abroad to be unaffordable, while some 44% rated their health as worse upon return.21 Taken together, our paradoxical observation warrants further research to elucidate multidimensional and likely mutable mediators of ethnic inequalities in women’s NCD mortality to inform health policy priorities in demographically and culturally changing Georgia.
By contrast, no consistent relation was found in our study between marital status and the likelihood of NCD mortality. This finding is in line with the pattern observed in the previous Russian prospective study among women (25–64 years) with respect to CVD mortality, but is at odds with the excess all-cause mortality in single women compared to their married peers,58 as supported by other works in Bulgaria,48 and for CVD mortality in Lithuania, albeit disproving such trend across other marital categories.59 In common with our finding, the most recent large prospective cohort study from Iran confirmed the absence of marital-related disparities in women’s all-cause mortality.60 Likewise, the earlier Japanese and Chinese longitudinal studies could not delineate all-cause, cancer and CVD mortality gradient across young women’s (40–64 years) marital categories, except for the significant all-cause and CVD mortality disadvantage of single Japanese women and a small cancer mortality disadvantage of Chinese widowed women relative to married ones.61,62 The recent meta-analytic reviews also highlighted the elevated risk of CVD and all-cause mortality among widowed and divorced women compared to those being married, with the younger cohorts exhibiting higher vulnerability to bereavement and marital dissolution soon after these life-changing events than their older counterparts.63,64 In general, there is remarkable heterogeneity among the published studies examining marital status and all-cause and NCD mortality that is largely influenced by cause-specific patterns and contextual factors. However, the available literature overwhelmingly supports the argument that married individuals have a reduced risk of mortality, with men gaining the greater health benefits than women.65–70 One potential mechanism behind this association lies on the "marriage selection hypothesis", implying that healthier individuals are more likely to marry or stay married than those with poorer health.61,71,72 Alternatively, the "marriage protection hypothesis" posits that a health-protective effect of marriage is conferred through social ties, social networks, social support, and economic security, translated into better access to preventive care (e.g. screening) and treatment uptake and adherence.71,72 The beneficial effect of marriage also applies to the promotion of healthy lifestyle and behavioral choices, encouraging married women to be less likely to engage in negative health behaviors than those being single, widowed or divorced.71,72 Furthermore, the buffering effect of marriage against psychological distress has been shown to mitigate the progression of several pathological processes such as atherosclerosis and cancer, mediated through allostatic processes involving cardiovascular reactivity, neuroendocrine and immune pathways.72 On the other hand, it has been documented elsewhere that experiencing more than one meaningful life event (severe and/or mild to moderate) is an independent risk factor of breast cancer among young females (<45 years), with married women worst affected.73 The longitudinal evidence further suggests that both highly strained and intense caregiving burden for ill spouses and related emotional and financial stress may markedly increase the risk of CVD and all-cause mortality among working-aged married women, especially those with a history of chronic diseases.74,75 The same holds true for poor marital quality, eroded by hostility and partner’s negative behavior as a predictor of women’s CVD and all-cause mortality, mediated by excessive wear and tear on the body (“allostatic load”).72,76,77 Such a positive link between marital functioning and health has been partially explained by the "subordinate-reactivity hypothesis", suggesting women’s greater physiological and psychological reactivity to marital discord given their relative subordinate (lower status and less powerful) social position both within society at large and marital relationships specifically.72 This is particularly relevant to less egalitarian, patriarchal societies, like Georgia, ranking 85th among 135 countries on the world’s Gender Gap Index (2012), where persistent gender-based violence is highly pervasive and reflects the imbalance of power relations in the household and society more generally.21 The most recent national research (2017) on domestic violence among a large sample of women aged 15–64 years found one in every eight women to be a victim of physical or sexual violence from their spouse or partner, an increase from one in every 11 women in 2009.78 Concerns arise also from Georgia’s one of the highest rates (17%) of teenage marriage (≤18 years) in Europe, along with Moldova (19%) and Turkey (14%),21 that has been documented to precipitate premature NCD mortality later in life (at ages 30–45), namely from all causes, CVD, cervical and lung cancers.62,79 The proposed underlying mechanisms have been largely connected to the teenage mothers’ higher risk of elevated parity, early parental responsibilities, psychological distress, social stigma, maladaptive behaviors, substandard care, lone motherhood, and welfare dependency, alongside the disruption of normative developmental trajectories (e.g. schooling).62,79 Based on these controversial and circumstantial findings, the observed marital gradient in this study may implicate a balanced power of the underlying social, behavioral and biological pathways. This deserves further research, especially in the face of the steep rise in divorce (44%) and a parallel decline in marriage rates (24%) since 2012,20 foreshadowing remarkable alterations in marital-related mortality inequalities in the country.
Likewise, our observation of the non-significant association between rural-urban place of residence and NCD mortality could be compositional in that this effect may be channeled through a myriad of offsetting mechanisms. As there is no universally used definition of “urban” or “rural”, much of the research investigating urban-rural inequalities in women’s NCD mortality presents mixed results, with substantial contrasting patterns in cause-specific mortality.80,81 For example, for women in Slovenia, the share of neoplasms was the highest in the most prosperous regions, while the share of the circulatory and digestive system diseases was higher in the stagnant regions and regions with poor socioeconomic conditions.69 Some studies, including those from Eastern Europe and Central Asia, report that compared to urban dwellers, rural women fare worse on many health dimensions, including NCD mortality.82–85 This likely reflects the imbalanced urban-rural economic development, lack of infrastructure, recourses, transportation, educational and employment opportunities, information and knowledge, as well as limited access to quality and timely health care in rural areas, which is compounded by traditional gender stereotypes.82–85 However, as documented in the 2010 Georgia Reproductive Health Survey (GERHS10),86 prior to the launch of the Universal Healthcare Program in 2013, and countrywide expansion of the National Reproductive Tract Cancers Prevention and Early Detection Program in 2011,21 the health insurance coverage and utilization of costly preventive, diagnostic, therapeutic and screening services in reproductive-aged women were equally trivial in both areas, as were health literacy and care-seeking practice, with the weak exception of the capital city Tbilisi. This pattern receives more support from previous studies in Georgia, identifying that over half (61%) of adults aged 18 and over, notably at ages 34–49, with long-term illnesses did not seek care when needed primarily owing to unaffordability (70%), but not geographical inaccessibility.23,24 There is also evidence that the share of households that incurred catastrophic out-of-pocket health expenditures, predominantly due to chronic diseases, increased from 2.8% to 11.7% during 2000–2007.87 Such a trend seems to be commonplace in the FSU,23 as in LMICs in general, bearing a disproportionate detrimental economic burden of NCDs, which in turn precipitates impoverishment and poorer care-seeking behavior.88 All the above may, in large part, explain the other noteworthy finding of our study regarding the absence of NCD mortality gradient by the place of death as a proxy of the access and utilization of care during the terminal illness. However, the widely embedded andronormativity and gender bias in health care (e.g. CVD-related stereotypes), the long trajectory of the disease and women’s documented preference for home death at the end of life could also be the relevant contributors.89–91 Current research further suggests that persistent social deprivation, apart from wars and conflicts, maybe a major push factor leading eventually to a surge in women’s rural-urban migration mainly for economic reasons, leaving the rural stayers likely affected by the healthy migrant effect.10,11,81,92–94 This holds true for Georgia as well, facing female-dominated relentless internal migration in search of employment, with a peak at ages 40–44.20,21 Available data for 2013 reveal that about 40% of women living in an urban location were born elsewhere, with Tbilisi experiencing the fastest population growth in the country, yet in parallel to the largest external migration.20,21 On the other hand, as urban areas are becoming home to the larger world’s (>50%) and European (70%) populations, more keenly felt in LMICs, emerging evidence demonstrates that urbanization may pose new environmental, social and cultural (assimilation, acculturation) challenges, known as the “urban health penalty”, which often overshadow the “urban advantage”, with an “ameliorative” impact on rural-urban mortality inequalities.5,80,81,84,92,93 In support of our finding, the absence of spatial gradient for major NCD causes of mortality has been previously documented in several European studies,95 including one from Greece,96 showing no rural-urban disparities in women’s overall and site-specific cancer mortality. The similar gradient in all-cause cancer mortality in Lithuania and China reflected, to varying degrees, the excess mortality from infection-related cancers (cervical, gastro-esophageal and liver) in rural women and that from “westernized lifestyle”-related cancers (breast and colorectal) in urban ones.97,98 The Chinese women’s rural-urban disparities in premature breast and cervical cancer deaths have been partially explained by urban women’s fewer childbearing, later ages at first full-term birth and less average duration of breastfeeding, among other reproductive factors,99 as also demonstrated by the GERHS10, with the widest rural-urban gap in total fertility rates (TFR).86 Although the literature remains contradictory as to the protective effect of parity on breast cancer given its dual effect on this risk,100 there is strong evidence from HICs and to a lesser extent, from LMICs, that more childbearing (greater TFR) and larger family size may contribute to developing cervical cancer, with the reverse being true for uterine and ovarian cancers.101 Furthermore, with widespread rapid and unplanned urbanization, current public health paradigm delineates the various environmental hazards of urbanicity as the key drivers of urban women’s excess NCD morbidity and mortality of premature onset from major causes (cancer, CVD, diabetes, and respiratory diseases).10,11 An increasing interest has recently gained the role of ambient air pollution and noise from mass motorization, heat islands from impervious surface areas and less open green spaces, light pollution by artificial light at night, and a broad suite of obesogenic factors such as urban sprawl, street connectivity and fast food outlet abundance, alongside other attributes of built and social (e.g. deprivation) neighborhood environments, operating via stress and risk-promoting westernized lifestyles and behaviors.10,11,102–113 Meanwhile, a growing body of evidence emphasizes that health disparities based on a simple and rigorous urban–rural dichotomy may not capture all of the intricacies of diversity at the local level and even more so the increased blurring between these residential distinctions, as seen in the uptrend of tobacco and processed food consumption in rural settings, suggesting progressive market penetration throughout LMICs.80,81,92 Interestingly, according to the GERHS10, although the female current smoking prevalence, along with alcohol use, is as yet traditionally low in Georgia even at fertile ages (9% in urban vs 2% in rural), nearly half of these young women in each area are likely equally exposed to secondhand smoking.86 Furthermore, challenging the current paradigm of urbanization as a key driver of the global epidemic of obesity, the latest review of the literature from LMICs emphasized the rising BMI at the same rate or faster in rural areas compared to urban, with rural women in MICs worst affected.114 Such convergence, largely driven by rapid economic development, has been acknowledged as a major contributor to the BMI rise in LMICs and globally over the last three decades.114 On the whole, the current wave of urbanization, projected to more severely and prematurely affect the relatively young and disadvantaged urbanizing populations in LMICs than in HICs,80 and concomitant “urbanization of rural life”115 substantiates the overriding need for the increased focus on the rural-urban context in the general endeavor of reducing health inequalities in Georgia. This would be conducive to deploying contextually sensitive policy interventions targeting at-risk women in each residential area and thereby curtail avoidable NCD mortality epidemic.
Contrariwise, we found that women with incomplete secondary education had a higher probability of NCD mortality compared to those with secondary education or higher, although this effect only became statistically significant when the other explanatory variables were taken into account. The observed inverse association between educational attainment and NCD mortality is concordant with wealth of evidence generated by previous cross-sectional and longitudinal investigations both in developed and developing countries, including in Europe, consistently highlighting the undereducated women’s NCD and all-cause mortality disadvantages, with important contributions of CVD and most but not all types of cancer.15,17,48,116–118 Consistent with our finding, several studies in FSU have also postulated lower educational qualification to be a strong independent predictor of women’s increased risk of avoidable NCD mortality.58,118,119 Our finding lends additional credence to the conjecture that as a proxy for a complex web of life experiences, opportunities and capabilities, education may have direct and indirect impact on health status by influencing information processing skills, adoption of health-promoting behavior and lifestyles, effective interaction with healthcare providers and compliance with medical recommendations, in parallel to future occupational opportunities and earning potential, implicating improvements in access to preventive and curative services and health care-seeking practices.10,120 Our finding further supports the existing evidence that, compared to men, women’s educational gradient in mortality tends to be less steep both for specific and broader cause categories, yet with some geographic pattern, as confirmed by the large multinational research in Europe.15,121 The dilution of women’s educational gradient for all-cause and NCD mortality could be partially accounted for the heterogeneity in the magnitude and direction of educational differentials by specific causes, as seen in several European studies, reporting the reverse educational gradient in breast cancer mortality, which likely offsets the inverse or “regular” gradient across other specific causes, notably for CVD.15,117,122–124 Likewise, the study in Slovenia identified the least educated women to be more likely to die from CVD, but not from neoplasms.69 It has been further proposed that less socially patterned lifestyle and behavioral factors or even their “reverse” relationship with education may also dampen or erase the health advantages conferred by education.15 As such, the findings from some FSU countries indicate that more educated women, particularly young, fare worse with regards to the common NCD risk factor prevalence (e.g. smoking, excessive alcohol consumption, physical activity, obesity), similar to those in the southern region of Europe, but in stark contrast to the northern, western, and continental regions.15,27,125–127 Particular concern should be also given to the role of healthcare system and diagnostic delays.15,23,116 Strikingly, one study in the FSU found that having greater than primary education and being aged 35–49 was associated with a lower probability to seek care when needed.23 Notwithstanding the observed small magnitude of educational inequalities in NCD mortality, our finding has considerable practical significance and indicates potential areas for policy intervention. Although Georgia, like other FSU countries, overall benefits from high enrolment rates in all levels of education, irrespective of gender, it faces the progressively higher female dropout rates in later stages of schooling (16% vs 10% in boys).21 This has been strongly linked to early marriages, particularly in rural areas, and suggested to be largely driven by patrilocal norms, attaching less value to girls’ education and their role in society.21,85,86 The factors that trigger child marriage, however, are not homogenous and vary according to the religious, ethnic, and regional context.21 Our observation, therefore, underscores that engaging in strategies to increase educational attainment in women, and policies focusing on equity-based and life-course approaches are important in redressing the social and economic inequalities that contribute to avoidable fatal outcomes of chronic diseases.
Similarly, our study provides a strong insight into the inverse association between employment and NCD mortality, which only emerged to be significant after multivariate adjustment. Our observation is compatible with a plethora of scientific research, lending support to the excess premature CVD, cancer (amenable) and all-cause mortality among unemployed women relative to employed ones, especially for those in their early and middle careers, which has been well documented during economic recessions both in HICs and MICs.18,76,128–131 It also appears that while CVD and cancer mortality peaks with mid-levels of accumulated unemployment, women’s long-term unemployment is related to an elevated risk of all-cause mortality.129 The published literature clearly substantiates that labor force participation confers women’s autonomy, self-efficacy, and empowerment in the family and in the broader society mainly through social status and regular income, which in turn is conducive for their own health enhancement.11,131 Conversely, job instability or loss may immediately lead to identity and financial loss and thereby social exclusions, with devastating consequences for both physical and mental health, including early death.11,131 Researchers further argue that health behavior variables actually represent an important mediating mechanism through which unemployment is translated into mortality (i.e. the “coping hypothesis”), suggesting that individuals, particularly those with low socioeconomic status and younger persons, cope with unemployment stress by changing their consumption patterns in unhealthy ways.128 This has been extensively exemplified by the deleterious impact of mass privatization and ensuing involuntary unemployment on the unprecedented upsurge of all-cause and CVD mortality in the FSU (e.g. “mortality crisis” in Russia) during the economic transition, peaking at ages 35–44 and mediated by extremely elevated levels of psychosocial stress and risky behaviors.130,133 The same holds true for Georgia, currently ranking among the world’s top 25 countries with the highest unemployment rates (14.6% in 2013).21 Available data indicate that about 75% of the unemployed in Georgia have not had a job for at least a year, whereas new job creation has remained slow.21 Importantly, unemployed workforce incorporates the largest share of people with secondary or higher education (81%) and those aged 15–24 years (31.7%).21 Alarmingly, these young jobless individuals have been shown elsewhere to be at increased risk of mortality from all- and other causes, except for transport accidents and suicide, compared to their employed peers.134 Of special significance is gaining the high female unemployment rate (13.8% vs 16.1% for men in 2012), with much of the unemployment and under-employment likely hidden under the self-employment category.21 Of note, as the current global context of unregulated labor markets, industrial restructuring and downsizing, trade competition and technological change encourages the growth of “precarious” forms of work arrangements such as short-term, part‐time contracts, and low incomes,11,132 this type of temporary employment, yet to a lesser extent than unemployment, has been well documented to be associated with the elevated risk of women’s all-cause and cause specific mortality.130,135 This may partially explain the relatively weak employment-related mortality gradient in our study. Apart from the underlying upstream or macro-level factors, women’s labor force participation in Georgia is likely shaped by the deep-rooted gender stereotypes and patriarchal attitudes, with exceedingly polarized gender roles forcing women to bear brunt of traditional and unpaid domestic and caregiving workload, while also spurring occupational gender segregation and wage discrimination (35%), which substantially impedes women’s either entrance or stay in the labor market.21,85,86 Unequal power relations and gendered norms and values translate into differential access to and control over health resources, with a negative impact on women’s health.13,85,86 Indeed, women in Georgia tend to be overly represented in the informal sector or lower-paying part-time jobs (health care, education, and subsistence agriculture), or even withdraw earlier from the labor market often due to the work-family conflict, as evinced elsewhere.136 It is also important to note that accumulated evidence increasingly highlights the bidirectional association between health and employment, whereby unemployment may cause poor health (more favored “causation hypothesis”), while poor health may increase the probability of becoming unemployed or not entering the labor force in the first place (health selection or “reverse-causation hypothesis”).137 In support of this, the longitudinal study from Norway indicated that suffering from several NCD-related health impairments and behavioral problems significantly increases the risk of job loss, just as the risk of having longer unemployment spells, with young women (<50 years) worst affected.138 More worrisomely, while jobless women with disabilities may continue to deal with their heavy domestic commitments, incurring additional stress, they are more than likely to neglect their own health needs and therefore, not to seek health care (“inverse-care law”) in the face of extreme precipitation of adverse health outcomes with unfavorable prognosis.139 These findings could be of great relevance to transitional economies such as Georgia, especially given 27% of the population and 30% among the poorest (40%) live in the households headed by a woman, as a breadwinner in their families.20,21 Together, our finding calls both researchers and policymakers to draw an explicit attention on factors at the macro level, including the labor market regulations and gender-neutral employment initiatives and protections as an effective primary prevention efforts. Simultaneously, secondary and tertiary prevention of negative health consequences of unemployment, focusing particularly on screening activities, behavioral interventions and stress management, ought to be a top policy priority.
Another striking finding of our study pertains to the failure of the women’s wealth status to predict NCD mortality. This finding replicates the results from one comprehensive study in Russia, which did not reveal the strong association between women’s material disadvantage and all-cause mortality after controlling for education,119 unlike other investigations in Eastern Europe, including Russia.48,140 The recent reviews of the similar literature have also signified substantial heterogeneity among the empirical results examining the association between NCD mortality and accumulated wealth.17,121 Although the reason behind the observed wealth gradient in women’s NCD mortality is unclear, it could be partially attributed to the full state-subsidized targeted “Medical Insurance Program for Poor”, rolled out nationwide in 2008 and rendering some positive impact, albeit mostly non-significant, on health care utilization and expenditures of individuals with chronic illnesses.141 At the same time, as discussed earlier, compared to men, women overall tend to be relatively immune to the socioeconomic gradient in all but CVD outcomes.121 Moreover, a body of evidence shows that wealth-related mortality pattern is not uniform across disease categories, suggesting that causes of death may distort the anticipated socioeconomic gradient, narrowing a span between mortality of poorest and richest.121 For example, a large prospective study in Eastern Europe indicated material amenities to be a more sensitive socioeconomic predictor of women’s premature CVD mortality than education.18 Conversely, the reverse gradient for breast cancer, shown to follow the “greater wealth confers greater risk,” rather than “wealth means health” pattern, may offset the CVD-related gradient, thereby yielding the blunted wealth gradient for overall or NCD causes.112,124,142 Furthermore, the role of the competing benefit of higher wealth status and harm of prevalent risky behaviors could be another plausible consideration.121 In that sense, the World Health Survey (WHS) in 48 LMICs indicated Georgia to be among the top 4 out of 16 countries (mostly MICs), exhibiting pro-poor inequality patterns in the current adult female smoking by household wealth index,143 similar to another WHS, identifying the analogous reverse patterns for women’s physical inactivity in many LMICs.126 Likewise, evidence from 54 LMICs documented a positive correlation between BMI/overweight and household wealth among reproductive-aged women (15–49 years) in nearly all FSU countries.127 Moreover, one study from Serbia identified the highest prevalence of classical cardiovascular risk factors such as hyperlipidemia, hypertension and diabetes in the wealthiest women.144 Some researchers also suggest that the asset-based “proxy” wealth index, measuring the household’s long-run economic status, may mask or buffer the effects of short-term fluctuations in economic well-being or economic shocks.33 Others, however, argue that measures of household material circumstances are “poor” enough to unambiguously discriminate between economically well-off and worse-off individuals and therefore predict the adverse health outcomes.145 Given such heterogeneity in conclusions, it stands to reason that future disaggregated research incorporating various relevant and objective indicators will help to unveil a variety of nuanced pathways underpinning women’s perplexing resistance to their economic hardship or advantage, which in itself may capture the socioeconomic patterning of the current stage of the epidemiological transition in the country.
Limitations
This study has a number of limitations. One major limitation is its cross-sectional design, which precludes making causal inferences, therefore longitudinal evaluations remain necessary. Second, NCD mortality in our study was examined as an aggregate measure that could have masked the distinct inequality patterns according to specific cause categories, though disaggregated analysis was limited by relatively small sample sizes for many subgroups. Further, the possible contributions of lifestyles and other potentially relevant indicators could not be ruled out in our study. However, our choice of risk factors was confined to those available in the original data, primarily collected for different purposes and thereby overall suffering from high item non-response rates,120 except for a relatively small share (0%-4%) of missing data for the selected variables, suggesting no major bias. On the other hand, information on women’s socio-demographics in this study largely relies on respondents’ self-reports and may be a subject to social desirability and recall biases. As well as these, other potential biases in our study could be attributable to the well-established limitations inherent in the VA, including PCVA, method, largely stemming from the instrument design, selection of respondents, variability in interviewers’ skills, and physicians’ approaches to death certification and coding.146 Nonetheless, our findings, based on the nationally representative data, for the most part, corroborate and extend available global and regional evidence base, with clear implications for guiding more holistic future research and policy development addressing young adult women’s health inequities and inequalities in the context of transitional economies.
Conclusion
To the best of our knowledge, the present study is the first attempt to shed light on socio-demographic inequalities in NCD-attributed mortality among reproductive-aged women in Georgia, providing new insights into how age, ethnic background, level of education and employment status might be implicated in women’s health outcomes in the prime of life. Recognizing the women’s profound contribution to society in both their productive and reproductive roles and the devastating consequences of their premature deaths on families, societies, and economies,8 our findings call for the urgent need to adopt the life-coarse and equity-based approaches to curb the mounting NCD mortality epidemic and enhance women’s survival during and beyond reproduction. This will stand to benefit from multisectoral and evidence-informed policy and interventions targeting the most disadvantaged and focusing on the broader socioeconomic, geographical and ethno-cultural contexts in which health beliefs and behaviors of girls and young adult women are embedded. Considering as well the intersection between women’s reproductive health and NCDs, it gains particular importance to integrate these two global health agendas and approaches by using the available reproductive health services.8 As such, explicit attention should be given to culturally sensitive health promotion and disease prevention efforts across the socioeconomic spectrum and earlier in the life course, alongside the elimination of barriers to education, employment and career progression to enable all women to age successfully and fully realize their health and well-being potential in Georgia.
Acknowledgments
The authors thank the US International Development Agency (USAID) for funding this study and the Letten Foundation for providing financial support for this work. The authors would like to express their deepest gratitude and appreciation to the Late Professor Babill Stray-Pedersen, without whom this research work would not have been possible. The authors are also grateful to the NCDC&PH staff and all other contributors to this study. The funding agency had no role in the study design and data collection, data analysis, or preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bonita R, Beaglehole R. Women and NCDs: overcoming the neglect. Glob Health Action. 2014;7:23742. doi:10.3402/gha.v7.23742
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Raymond SU, Greenberg HM, Leeder SR. Beyond reproduction: women’s health in today’s developing world. Int J Epidemiol. 2005;34(5):1144–1148. doi:10.1093/ije/dyi121
4. Langer A, Meleis A, Knaul FM, et al. Women and health: the key for sustainable development. Lancet. 2015;386:1165–1210. doi:10.1016/S0140-6736(15)60497-4
5. Ezzati M, Vander Hoorn S, Lawes CMM, et al. Rethinking the “diseases of affluence” paradigm: global patterns of nutritional risks in relation to economic development. PLoS Med. 2005;2:e133.
6. Egger G, Dixon J. Beyond obesity and lifestyle: a review of 21st century chronic disease determinants. Biomed Res Int. 2014;2014:731685. doi:10.1155/2014/731685
7. Temmerman M, Khosla R, Laski L, Mathews Z, Say L. Women and health working group for the global strategy for women’s, children’s and adolescents’ health. Women’s health priorities and interventions. BMJ. 2015;351:h4147. doi:10.1136/bmj.h4147
8. Knaul FM, Langer A, Atun R, Rodin D, Frenk J, Bonita R. Rethinking maternal health. Lancet Glob Health. 2016;4:e227–e228. doi:10.1016/S2214-109X(16)00044-9
9. World Health Organization Regional Office for Europe. Beyond the Mortality Advantage: Investigating Women’s Health in Europe. Copenhagen, Denmark: WHO Regional Office for Europe; 2015. Available from: http://www.euro.who.int/en/health-topics/health-determinants/gender/publications/2015/beyond-the-mortality-advantage.-investigating-womens-health-in-europe.
10. Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva, Switzerland: World Health Organization; 2008. Available from: www.who.int/social_determinants/final_report/csdh_finalreport_2008.pdf.
11. Marmot M, Friel S, Bell R, et al. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372:1661–1669. doi:10.1016/S0140-6736(08)61690-6
12. Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129:19–31. doi:10.1177/00333549141291S206
13. AbouZahr C. Progress and challenges in women’s health: an analysis of levels and patterns of mortality and morbidity. Contraception. 2014;90(Suppl 6):S3–S13. doi:10.1016/j.contraception.2014.03.007
14. Di Cesare M, Khang Y-H, Asaria P, et al. Inequalities in non-communicable diseases and effective responses. Lancet. 2013;381:585–597. doi:10.1016/S0140-6736(12)61851-0
15. Mackenbach JP, Stirbu I, Roskam AJ, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. 2008;358(23):2468–2481. doi:10.1056/NEJMsa0707519
16. Ikram UZ, Mackenbach JP, Harding S, et al. All-cause and cause-specific mortality of different migrant populations in Europe. Eur J Epidemiol. 2016;31(7):655–665. doi:10.1007/s10654-015-0083-9
17. Williams J, Allen L, Wickramasinghe K, Mikkelsen B, Roberts N, Townsend N. A systematic review of associations between non-communicable diseases and socioeconomic status within low- and lower-middle-income countries. J Glob Health. 2018;8(2):020409. doi:10.7189/jogh.08.020409
18. Tillmann T, Pikhart H, Peasey A, et al. Psychosocial and socioeconomic determinants of cardiovascular mortality in Eastern Europe: a multicenter prospective cohort study. PLoS Med. 2017;14(12):e1002459. doi:10.1371/journal.pmed.1002459
19. The World Bank. Data: Georgia. Washington: The World Bank; 2017. Available from: https://data.worldbank.org/country/georgia.
20. National Statistics Office of Georgia. Available from: http://www.geostat.ge.
21. United Nations Population Fund. Population situation analysis (PSA). 2014: final report. Tbilisi, Georgia: United Nations Population Fund; 2014. Available from: https://georgia.unfpa.org/sites/default/files/pub-pdf/PSA%20_Final%20Print%20version_0.pdf.
22. Szreter S. Rapid economic growth and ‘the four Ds’ of disruption, deprivation, disease and death: public health lessons from nineteenth-century Britain for twenty-first-century China? Trop Med Int Health. 1999;4(2):146–152. doi:10.1046/j.1365-3156.1999.00369.x
23. Balabanova D, Roberts B, Richardson E, Haerpfer C, McKee M. Health care reform in the former Soviet Union: beyond the transition. Health Serv Res. 2012;47(2):840–864. doi:10.1111/j.1475-6773.2011.01323.x
24. Gotsadze G, Bennett S, Ranson K, Gzirishvili D. Health care seeking behavior and out-of-pocket payments in Tbilisi, Georgia: household survey findings. Health Policy Plan. 2005;20:232–242. doi:10.1093/heapol/czi029
25. World Health Organization. Noncommunicable Diseases (NCD) Country Profiles, 2014: Georgia. Geneva, Switzerland: World Health Organization; 2014. Available from: http://www.who.int/nmh/countries/geo_en.pdf.
26. World Health Organization. Georgia STEPS Survey 2010: Fact Sheet. Geneva, Switzerland: World Health Organization; 2010. Available from: http://www.who.int/chp/steps/Georgia_2010_Fact_Sheet.pdf.
27. Berg CJ, Aslanikashvili A, Djibuti M. A cross-sectional study examining youth smoking rates and correlates in Tbilisi, Georgia. Biomed Res Int. 2014;2014:476438. doi:10.1155/2014/476438
28. GBD. Russia Collaborators. The burden of disease in Russia from 1980 to 2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2016;2018(392):1138–1146.
29. Serbanescu F, Teft M, Shakhnazarova M, Williams D, Berdzuli N, Berg C. Reproductive Age Mortality Study, Georgia 2008 - Part II: Maternal Mortality. Atlanta, GA: Division of Reproductive Health, Centers for Disease Control and Prevention (DRH/CDC); 2009.
30. Lomia N, Berdzuli N, Sturua L, et al. Leading causes of death of women of reproductive age in the Republic of Georgia: findings from the National Reproductive Age Mortality Survey (2014). Int J Womens Health. 2018;10:437–452. doi:10.2147/IJWH
31. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision, Edition 2010. Geneva, Switzerland: World Health Organization; 2010. Available from: http://apps.who.int/classifications/icd10/browse/2010/en.
32. Rutstein SO. The DHS Wealth Index: Approaches for Rural and Urban Areas. Washington, DC: Macro International Inc; 2008.
33. Filmer D, Pritchett LH. Estimating wealth effects without expenditure data–or tears: an application to educational enrollments in states of India. Demography. 2001;38:115–132. doi:10.1353/dem.2001.0003
34. Hosmer JDW, Lemeshow S, Sturdivant RX. Applied Logistic Regression.
35. IBM. SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp; 2012.
36. StataCorp. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP; 2015.
37. United Nations. RES/70/1. Transforming our world: the 2030 Agenda for Sustainable Development; 2015.
38. World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. Geneva, Switzerland: World Health Organization; 2013.
39. White MC, Holman DM, Boehm JE, Peipins LA, Grossman M, Kenley J. Age and cancer risk. Am J Prev Med. 2014;46(3):S7–S15. doi:10.1016/j.amepre.2013.10.029
40. Hardy R, Lawlor DA, Kuh D. A life course approach to cardiovascular aging. Future Cardiol. 2015;11(1):101–113. doi:10.2217/fca.14.67
41. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ. 2017;8(1):33. doi:10.1186/s13293-017-0152-8
42. Fransquet PD, Wrigglesworth J, Woods RL, Ernst ME, Ryan J. The epigenetic clock as a predictor of disease and mortality risk: a systematic review and meta-analysis. Clin Epigenetics. 2019;11(1):62. doi:10.1186/s13148-019-0656-7
43. Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL. Measuring population ageing: an analysis of the Global Burden of Disease Study 2017. Lancet Public Health. 2019;4(3):e159–e167. (). doi:10.1016/S2468-2667(19)30019-2
44. Mehta NK, Zheng H, Myrskylä M. How do age and major risk factors for mortality interact over the life-course? Implications for health disparities research and public health policy. SSM Popul Health. 2019;8:100438. doi:10.1016/j.ssmph.2019.100438
45. Mikkelsen B, Williams J, Rakovac I, et al. Life course approach to prevention and control of non-communicable diseases. BMJ. 2019;364:l257. doi:10.1136/bmj.l257
46. Teruya SA, Bazargan-Hejazi S. The immigrant and hispanic paradoxes: a systematic review of their predictions and effects. Hisp J Behav Sci. 2013;35(4):486–509. doi:10.1177/0739986313499004
47. Vanthomme K, Vandenheede H. Migrant mortality differences in the 2000s in Belgium: interaction with gender and the role of socioeconomic position. Int J Equity Health. 2019;18(1):96. doi:10.1186/s12939-019-0983-5
48. Kohler IV, Preston SH. Ethnic and religious differentials in Bulgarian mortality, 1993–1998. Popul Stud (Camb). 2011;65(1):91–113. doi:10.1080/00324728.2010.535554
49. Guillot M, Gavrilova N, Pudrovska T. Understanding the “Russian mortality paradox” in Central Asia: evidence from Kyrgyzstan. Demography. 2011;48(3):1081–1104. doi:10.1007/s13524-011-0036-1
50. Sharygin EJ, Guillot M. Ethnicity, russification, and excess mortality in Kazakhstan. Vienna Yearb Popul Res. 2013;11:219–246. doi:10.1553/populationyearbook2013s219
51. Spallek J, Zeeb H, Razum O. What do we have to know from migrants’ past exposures to understand their health status? A life course approach. Emerg Themes Epidemiol. 2011;8(1):6. doi:10.1186/1742-7622-8-6
52. Porter P. Westernizing’ women’s risks? Breast cancer in lower income countries. NEJM. 2008;358(3):213–216. doi:10.1056/NEJMp0708307
53. Lara M, Gamboa C, Kahramanian MI, Morales LS, Bautista DE. Acculturation and Latino health in the United States: a review of the literature and its sociopolitical context. Annu Rev Public Health. 2005;26:367–397. doi:10.1146/annurev.publhealth.26.021304.144615
54. Duthé G, Guillot M, Meslé F, et al. Adult mortality patterns in the former Soviet Union’s southern tier: Armenia and Georgia in comparative perspective. Demogr Res. 2017;36:589–608. doi:10.4054/DemRes.2017.36.19
55. Cockerham WC. The intersection of life expectancy and gender in a transitional state: the case of Russia. Sociol Health Ill. 2012;34:943–957. doi:10.1111/j.1467-9566.2011.01454.x
56. Caucasus Research Resource Centers. Migration and Return in Georgia: Trends, Assessments, and Potential. Tbilisi, Georgia: Caucasus Research Resource Centers; 2008. Available from: http://crrc.ge/uploads/tinymce/documents/Completed-projects/CRRC_MigrationReport_FINAL_23JAN2008.pdf.
57. Norredam M, Hansen OH, Petersen JH, et al. Remigration of migrants with severe disease: myth or reality? - A register-based cohort study. Eur J Pub Health. 2015;25(1):84–89. doi:10.1093/eurpub/cku138
58. Malyutina S, Bobak M, Simonova G, Gafarov GV, Nikitin Y, Marmot M. Education, marital status, and total and cardiovascular mortality in Novosibirsk, Russia: a prospective cohort study. Ann Epidemiol. 2004;14:244–249. doi:10.1016/S1047-2797(03)00133-9
59. Kalediene R, Petrauskiene J, Starkuviene S. Inequalities in mortality by marital status during socio-economic transition in Lithuania. Public Health. 2007;121:385–392. doi:10.1016/j.puhe.2006.09.026
60. Ramezankhani A, Azizi F, Hadaegh F. Associations of marital status with diabetes, hypertension, cardiovascular disease and all-cause mortality: a long term follow-up study. PLoS One. 2019;14(4):e0215593. doi:10.1371/journal.pone.0215593
61. Ikeda A, Iso H, Toyoshima H, et al. Marital status and mortality among Japanese men and women: the Japan Collaborative Cohort Study. BMC Public Health. 2007;7:73. doi:10.1186/1471-2458-7-73
62. Va P, Yang WS, Nechuta S, et al. Marital status and mortality among middle age and elderly men and women in urban Shanghai. PLoS One. 2011;6(11):e26600. doi:10.1371/journal.pone.0026600
63. Shor E, Roelfs DJ, Bugyi P, Schwartz JE. Meta-analysis of marital dissolution and mortality: reevaluating the intersection of gender and age. Soc Sci Med. 2012;75(1):46–59. doi:10.1016/j.socscimed.2012.03.010
64. Shor E, Roelfs DJ, Curreli M, Clemow L, Burg MM, Schwartz JE. Widowhood and mortality: a meta-analysis and meta-regression. Demography. 2012;49(2):575–606. doi:10.1007/s13524-012-0096-x
65. Roelfs DJ, Shor E, Kalish R, Yogev T. The rising relative risk of mortality for singles: meta-analysis and meta-regression. Am J Epidemiol. 2011;174(4):379–389. doi:10.1093/aje/kwr111
66. Dhindsa DS, Khambhati J, Schultz WM, Tahhan AS, Quyyumi AA. Marital status and outcomes in patients with cardiovascular disease: a review. Trends Cardiovasc Med. 2019;S1050–1738(18):30181–30186.
67. Aizer AA, Chen MH, McCarthy EP, et al. Marital status and survival in patients with cancer. J Clin Oncol. 2013;31(31):3869–3876. doi:10.1200/JCO.2013.49.6489
68. Gomez SL, Hurley S, Canchola AJ, et al. Effects of marital status and economic resources on survival after cancer: a population-based study. Cancer. 2016;122(10):1618–1625. doi:10.1002/cncr.29885
69. Artnik B, Vidmar G, Javornik J, Laaser U. Premature mortality in Slovenia in relation to selected biological, socioeconomic, and geographical determinants. Croat Med J. 2006;47(1):103–113.
70. Hinyard L, Wirth LS, Clancy JM, Schwartz T. The effect of marital status on breast cancer‐related outcomes in women under 65: a SEER database analysis. Breast. 2017;32:
71. Robards J, Evandrou M, Falkingham J, Vlachantoni A. Marital status, health and mortality. Maturitas. 2012;73(4):295–299. doi:10.1016/j.maturitas.2012.08.007
72. Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: a meta-analytic review. Psychol Bull. 2014;140(1):140–187. doi:10.1037/a0031859
73. Peled R, Carmil D, Siboni-Samocha O, Shoham-Vardi I. Breast cancer, psychological distress and life events among young women. BMC Cancer. 2008;8:245. doi:10.1186/1471-2407-8-245
74. Lee S, Colditz GA, Berkman LF, Kawachi I. Caregiving and risk of coronary heart disease in U.S. women. Am J Prev Med. 2003;24:113–119. doi:10.1016/S0749-3797(02)00582-2
75. Perkins M, Howard VJ, Wadley VG, et al. Caregiving strain and all-cause mortality: evidence from the REGARDS study. J Gerontol B Psychol Sci Soc Sci. 2013;68(4):504–512. doi:10.1093/geronb/gbs084
76. Kriegbaum M, Lund R, Schmidt L, Rod NH, Christensen U. The joint effect of unemployment and cynical hostility on all-cause mortality: results from a prospective cohort study. BMC Public Health. 2019;19(1):203. doi:10.1186/s12889-019-6622-7
77. Robertson T, Beveridge G, Bromley C. Allostatic load as a predictor of all-cause and cause-specific mortality in the general population: evidence from the Scottish Health Survey. PLoS One. 2017;12(8):e0183297. doi:10.1371/journal.pone.0183297
78. UN Women. National Study on Violence Against Women. Tbilisi, Georgia: UN Women; 2018. Available from: https://www2.unwomen.org/-/media/field%20office%20georgia/attachments/publications/2018/national%20study%20on%20violence%20against%20women%202017.pdf?la=en&vs=2932.
79. Otterblad Olausson P, Haglund B, Ringbäck Weitoft G, Cnattingius S. Premature death among teenage mothers. BJOG Int J Obstet Gynaecol. 2004;111:793–799. doi:10.1111/j.1471-0528.2004.00248.x
80. Allender S, Foster C, Hutchinson L, Arambepola C. Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health. 2008;85(6):938–951. doi:10.1007/s11524-008-9325-4
81. Dahly DL, Adair LS. Quantifying the urban environment: a scale measure of urbanicity outperforms the urban-rural dichotomy. Soc Sci Med. 2007;64(7):1407–1419. doi:10.1016/j.socscimed.2006.11.019
82. Singh GK, Siahpush M. Widening rural-urban disparities in all-cause mortality and mortality from major causes of death in the USA, 1969-2009. J Urban Health. 2014;91(2):272–292. doi:10.1007/s11524-013-9847-2
83. Ke C, Gupta R, Xavier D, et al. Divergent trends in ischaemic heart disease and stroke mortality in India from 2000 to 2015: a nationally representative mortality study. Lancet Glob Health. 2018;6(8):e914–e923. doi:10.1016/S2214-109X(18)30242-0
84. Koster EM, de Gelder R, Di Nardo F, et al. Health status in Europe: comparison of 24 urban areas to the corresponding 10 countries (EURO-URHIS 2). Eur J Pub Health. 2017;27(Suppl 2):62–67. doi:10.1093/eurpub/ckw188
85. Food and Agriculture Organization of the United Nations. Gender and Rural Development in Eastern Europe and Central Asia: Key Issues. Rome, Italy: Food and Agriculture Organization; 2016. Available from: http://www.fao.org/3/a-i5497e.pdf.
86. Serbanescu F, Egnatashvili V, Ruiz A, Suchdev D, Goodwin M. Reproductive Health Survey, Georgia 2010: Summary Report. Atlanta, GA: Division of Reproductive Health, Centers for Disease Control and Prevention (DRH/CDC); 2011.
87. Gotsadze G, Zoidze A, Rukhadze N. Household catastrophic health expenditure: evidence from Georgia and its policy implications. BMC Health Serv Res. 2009;9:69. doi:10.1186/1472-6963-9-69
88. Kankeu HT, Saksena P, Xu K, Evans DB. The financial burden from non-communicable diseases in low- and middle-income countries: a literature review. Health Res Policy Syst. 2013;11:31. doi:10.1186/1478-4505-11-31
89. Ruiz-Cantero MT, Vives-Cases C, Artazcoz L, et al. A framework to analyse gender bias in epidemiological research. J Epidemiol Community Health. 2007;61(Suppl 2):ii46–ii53. doi:10.1136/jech.2007.062034
90. Samulowitz A, Gremyr I, Eriksson E, Hensing G. “Brave men” and “emotional women”: a theory-guided literature review on gender bias in health care and gendered norms towards patients with chronic pain. Pain Res Manag. 2018;2018:6358624.
91. Gomes B, Higginson IJ. Factors influencing death at home in terminally ill patients with cancer: systematic review [published correction appears in BMJ]. BMJ. 2006;332(7540):515–521. doi:10.1136/bmj.38740.614954.55
92. Oyebode O, Pape UJ, Laverty AA, Lee JT, Bhan N, Millett C. Rural, urban and migrant differences in non-communicable disease risk-factors in middle income countries: a cross-sectional study of WHO-SAGE data. PLoS One. 2015;10(4):e0122747. doi:10.1371/journal.pone.0122747
93. Hernández AV, Pasupuleti V, Deshpande A, Bernabé-Ortiz A, Miranda JJ. Effect of rural-to-urban within-country migration on cardiovascular risk-factors in low- and middle-income countries: a systematic review. Heart. 2012;98(3):185–194. doi:10.1136/heartjnl-2011-300599
94. Szklarska A, Lipowicz A, Lopuszanska M, Bielicki T, Koziel S. Biological condition of adult migrants and nonmigrants in Wroclaw, Poland. Am J Hum Bio. 2008;20:139–145. doi:10.1002/ajhb.20691
95. Gartner A, Farewell D, Dustan F, Gordon E. Differences in mortality between rural and urban areas in England and Wales, 2002–2004. Health Stat Q. 2008;39:6–13.
96. Nikolaidis C, Tentes I, Lialiaris T, Constantinidis TC, Kortsaris A. Regional disparities in cancer mortality across the rural-urban axis: a case study from north-eastern Greece. Rural Remote Health.2015;15:3013.
97. Li X, Deng Y, Tang W, et al. Urban-rural disparity in cancer incidence, mortality, and survivals in Shanghai, China, during 2002 and 2015. Front Oncol. 2018;8:579. doi:10.3389/fonc.2018.00579
98. Smailyte G, Kurtinaitis J. Cancer mortality differences among urban and rural residents in Lithuania. BMC Public Health. 2008;8:56. doi:10.1186/1471-2458-8-56
99. Lewington S, Li L, Murugasen S, et al. Temporal trends of main reproductive characteristics in ten urban and rural regions of China: the China Kadoorie biobank study of 3,00,000 women. Int J Epidemiol. 2014;43:1252–1262. doi:10.1093/ije/dyu035
100. Kobayashi S, Sugiura H, Ando Y, et al. Reproductive history and breast cancer risk. Breast Cancer. 2012;19(4):302–308. doi:10.1007/s12282-012-0384-8
101. You W, Rühli FJ, Henneberg RJ, Henneberg M. Greater family size is associated with less cancer risk: an ecological analysis of 178 countries. BMC Cancer. 2018;18(1):924. doi:10.1186/s12885-018-4837-0
102. Gambaryan MH, Shalnova SA, Deev AD, Drapkina OM. Chronic respiratory diseases in the regions of Northern Russia: epidemiological distinctions in the results of a National Population Study. Int J Environ Res Public Health. 2017;14(8):841. doi:10.3390/ijerph14080841
103. Dzhambov AM, Dimitrova DD. Exposures to road traffic, noise, and air pollution as risk factors for type 2 diabetes: a feasibility study in Bulgaria. Noise Health. 2016;18(82):133–142. doi:10.4103/1463-1741.181996
104. Newell K, Kartsonaki C, Lam KBH, Kurmi O. Cardiorespiratory health effects of gaseous ambient air pollution exposure in low and middle income countries: a systematic review and meta-analysis. Environ Health. 2018;17(1):41.
105. Ishigami A, Hajat S, Kovats RS, et al. An ecological time-series study of heat-related mortality in three European cities. Environ Health. 2008;7:5. doi:10.1186/1476-069X-7-5
106. Lane KJ, Stokes EC, Seto KC, Thanikachalam S, Thanikachalam M, Bell ML. Associations between greenness, impervious surface area, and nighttime lights on biomarkers of vascular aging in Chennai, India. Environ Health Perspect. 2017;125(8):087003. doi:10.1289/EHP36
107. Keshet-Sitton A, Or-Chen K, Yitzhak S, Tzabary I, Haim A. Light and the city: breast cancer risk factors differ between urban and rural women in Israel. Integr Cancer Ther. 2017;16(2):176–187. doi:10.1177/1534735416660194
108. Mackenbach JD, Rutter H, Compernolle S, et al. Obesogenic environments: a systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health. 2014;14(1):233. doi:10.1186/1471-2458-14-233
109. Griffin BA, Eibner C, Bird CE, et al. The relationship between urban sprawl and coronary heart disease in women. Health Place. 2013;20:51–61. doi:10.1016/j.healthplace.2012.11.003
110. Tamosiunas A, Grazuleviciene R, Luksiene D, et al. Accessibility and use of urban green spaces, and cardiovascular health: findings from a Kaunas cohort study. Environ Health. 2014;13(1):20. doi:10.1186/1476-069X-13-20
111. Malambo P, Kengne AP, De Villiers A, Lambert EV, Puoane T. Built environment, selected risk factors and major cardiovascular disease outcomes: a systematic review. PLoS One. 2016;11(11):e0166846. doi:10.1371/journal.pone.0166846
112. Belon AP, Barros MB, Marín-León L. Mortality among adults: gender and socioeconomic differences in a Brazilian city. BMC Public Health. 2012;12:39. doi:10.1186/1471-2458-12-39
113. Movsisyan NK, Sochor O, Kralikova E, Cifkova R, Ross H, Lopez-Jimenez F. Current and past smoking patterns in a Central European urban population: a cross-sectional study in a high-burden country. BMC Public Health. 2016;16:571. doi:10.1186/s12889-016-3216-5
114. NCD Risk Factor Collaboration. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature. 2019;569(7755):260–264.
115. Stuckler D, Nestle M. Big food, food systems, and global health. PLoS Med. 2012;9:6. doi:10.1371/journal.pmed.1001242
116. Stirbu I, Kunst AE, Bopp M, et al. Educational inequalities in avoidable mortality in Europe. J Epidemiol Community Health. 2010;64:913–920. doi:10.1136/jech.2008.081737
117. Leinsalu M, Stirbu I, Vågerö D, et al. Educational inequalities in mortality in four eastern European countries: divergence in trends during the post-communist transition from 1990 to 2000. Int J Epidemiol. 2009;38:512–525. doi:10.1093/ije/dyn248
118. Pikala M, Burzyn Ska M, Pikala R, Bryła M, Maniecka-Bryła I. Educational inequalities in premature mortality in Poland, 2002–2011: a population-based cross-sectional study. BMJ Open. 2016;6(9):e011501. doi:10.1136/bmjopen-2016-011501
119. Perlman F, Bobak M. Socioeconomic and behavioral determinants of mortality in posttransition Russia: a prospective population study. Ann of Epidemiol. 2008;18(2):92–100. doi:10.1016/j.annepidem.2007.07.093
120. Shavers VL. Measurement of socioeconomic status in health disparities research. J Natl Med Assoc. 2007;99(9):1013–1023.
121. Phillips SP, Hamberg K. Women’s relative immunity to the socio-economic health gradient: artifact or real? Glob Health Action. 2015;8:27259. doi:10.3402/gha.v8.27259
122. Lundqvist A, Andersson E, Ahlberg I, Nilbert M, Gerdtham U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe - a systematic review and meta-analysis. Eur J Public Health. 2016;26(5):804–813. doi:10.1093/eurpub/ckw070
123. Strand BH, Tverdal A, Claussen B, Zahl PH. Is birth history the key to highly educated women’s higher breast cancer mortality? A follow-up study of 500,000 women aged 35–54. Int J Cancer. 2005;117:1002–1006. doi:10.1002/ijc.21239
124. Cabrera C, Helgesson O, Wedel H, Bjorkelund C, Bengtsson C, Lissner L. Socioeconomic status and mortality in Swedish women: opposing trends for cardiovascular disease and cancer. Epidemiology. 2001;12:532–536. doi:10.1097/00001648-200109000-00012
125. Pomerleau J, Gilmore A, McKee M, Rose R, Haerpfer CW. Determinants of smoking in eight countries of the former Soviet Unions: results from the living conditions, lifestyles and health study. Addiction. 2004;99(12):1577–1585. doi:10.1111/j.1360-0443.2004.00885.x
126. Hosseinpoor AR, Bergen N, Kunst A, et al. Socioeconomic inequalities in risk factors for non-communicable diseases in low-income and middle-income countries: results from the World Health Survey. BMC Public Health. 2012;12:912. doi:10.1186/1471-2458-12-912
127. Subramanian SV, Perkins JM, Ozaltin E, Davey SG. Weight of nations: a socioeconomic analysis of women in low- to middle-income countries. Am J Clin Nutr. 2011;93:413–421. doi:10.3945/ajcn.110.004820
128. Roelfs DJ, Shor E, Davidson KW, Schwartz JE. Losing life and livelihood: a systematic review and meta-analysis of unemployment and all-cause mortality. Soc Sci Med. 2011;72(6):840–854. doi:10.1016/j.socscimed.2011.01.005
129. Garcy AM, Vågerö D. The length of unemployment predicts mortality, differently in men and women, and by cause of death: a six year mortality follow-up of the Swedish 1992–1996 recession. Soc Sci Med. 2012;74:1911–1920. doi:10.1016/j.socscimed.2012.01.034
130. Perlman F, Bobak M. Assessing the contribution of unstable employment to mortality in posttransition Russia: prospective individual-level analyses from the Russian longitudinal monitoring survey. Am J Public Health. 2009;99(10):1818–1825. doi:10.2105/AJPH.2008.154815
131. Maruthappu M, Watkins J, Noor AM, et al. Economic downturns, universal health coverage, and cancer mortality in high‐income and middle‐income countries, 1990–2010: a longitudinal analysis. Lancet. 2016;388:684–695. doi:10.1016/S0140-6736(16)00577-8
132. Marmot M, Allen J, Bell R, Bloomer E, Goldblatt P. WHO European review of social determinants of health and the health divide. Lancet. 2012;380:1011–1029. doi:10.1016/S0140-6736(12)61228-8
133. Brainerd E, Cutler DM. Autopsy on an empire: understanding mortality in Russia and the Former Soviet Union. J Economic Perspectives. 2005;19(1):107–130. doi:10.1257/0895330053147921
134. Davila EP, Christ SL, Caban-Martinez AJ, et al. Young adults, mortality, and employment. J Occup Environ Med. 2010;52(5):501–504. doi:10.1097/JOM.0b013e3181d5e371
135. Virtanen M, Kivimäki M, Joensuu M, Virtanen P, Elovainio M, Vahtera J. Temporary employment and health: a review. Int J Epidemiol. 2005;34(3):610–622. doi:10.1093/ije/dyi024
136. Lilly MB, Laporte A, Coyte PC. Labor market work and home care’s unpaid caregivers: a systematic review of labor force participation rates, predictors of labor market withdrawal, and hours of work. Milbank Q. 2007;85(4):641–690. doi:10.1111/milq.2007.85.issue-4
137. Schuring M, Burdorf L, Kunst A, Mackenbach J. The effects of ill health on entering and maintaining paid employment: evidence in European countries. J Epidemiol Community Health. 2007;61(7):597–604. doi:10.1136/jech.2006.047456
138. Kaspersen SL, Pape K, GÅ V, et al. Health and unemployment: 14 years of follow-up on job loss in the Norwegian HUNT Study. Eur J Public Health. 2016;26(2):312–317. doi:10.1093/eurpub/ckv224
139. Voncina L, Pristas I, Mastilica M, Polasek O, Sosić Z, Stevanović R. Use of preventive health care services among the unemployed in Croatia. Croat Med J. 2007;48(5):667–674.
140. Vandenheede H, Vikhireva O, Pikhart H, et al. Socioeconomic inequalities in all-cause mortality in the Czech Republic, Russia, Poland and Lithuania in the 2000s: findings from the HAPIEE Study. J Epidemiol Community Health. 2014;68(4):297–303. doi:10.1136/jech-2013-203057
141. Gotsadze G, Murphy A, Shengelia N, Zoidze A. Healthcare utilization and expenditures for chronic and acute conditions in Georgia: does benefit package design matter? BMC Health Serv Res. 2015;15:88. doi:10.1186/s12913-015-0755-x
142. Lehrer S, Green S, Rosenzweig KE. Affluence and Breast Cancer. Breast J. 2016;22(5):564–567. doi:10.1111/tbj.2016.22.issue-5
143. Hosseinpoor AR, Parker LA, Tursan d’Espaignet E, Chatterji S. Socioeconomic inequality in smoking in low-income and middle-income countries: results from the World Health Survey. PLoS One. 2012;7(8):e42843. doi:10.1371/journal.pone.0042843
144. Vuković D, Bjegović V, Vuković G. Prevalence of chronic diseases according to socioeconomic status measured by wealth index: health survey in Serbia. Croat Med J. 2008;49(6):832–841. doi:10.3325/cmj.2008.49.832
145. Marmot M, Bobak M. International comparators and poverty and health in Europe. BMJ. 2000;321(7269):1124–1128. doi:10.1136/bmj.321.7269.1124
146. Lozano R, Lopez AD, Atkinson C, Naghavi M, Flaxman AD, Murray CJ. Population Health Metrics Research Consortium (PHMRC). Performance of physician-certified verbal autopsies: multisite validation study using clinical diagnostic gold standards. Popul Health Metr. 2011;9:32. doi:10.1186/1478-7954-9-32
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.