")
Back to Journals » Vascular Health and Risk Management » Volume 18
Socio-Demographic Characteristics and Associated Factors of Morbidity in Patients with Venous Ulcers Treated in Two Institutions of Contributive and Subsidized Regime in Colombia: Retrospective, Multicenter, Observational Study
Authors Cacua Sanchez MT , Buenahora G
Received 21 October 2021
Accepted for publication 9 January 2022
Published 3 March 2022 Volume 2022:18 Pages 89—104
DOI https://doi.org/10.2147/VHRM.S345542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Maria Teresa Cacua Sanchez,1 Gustavo Buenahora2
1Vascular Surgery, Ambulatory Surgery Center, Vascular Laboratory Kennedy Hospital, Bogotá, Colombia; 2General Practitioners, Ambulatory Surgery Center, Bogotá, Colombia
Correspondence: Maria Teresa Cacua Sanchez, Tel +57-1-3057470125, Email [email protected]
Aim: Venous ulcers are the most serious complication of chronic venous insufficiency secondary to venous hypertension and represent between 80% and 90% of all ulcers vascular, having socioeconomic repercussions and on the patient’s quality of life.
Objective: To determine the factors associated and complications with the morbidity of patients with venous ulcers CEAP 6 in two health delivery systems in Colombia.
Methodology: Observational study retrospective multicenter carried out in two health centers, one under the subsidized scheme and the other under the contributory scheme in patients captured adults over 18 years of age during the years 2018 and 2019 with a diagnosis of chronic venous insufficiency CEAP 6 performing a review to the clinical history up to 4 years before the consultation for vascular surgery of ulcerative pathology.
Results: A total of 105 patients were evaluated 52% of the contributory regime and 48% patients of the subsidized regime. With 139 ulcers, 70% were women. The educational level of the population in 77% of the individuals had no schooling or only had primary education. The patients of the subsidized regime belonged to the low socioeconomic stratum vs the middle-class stratum in the contributory regime. 80.5% of the lesions are concentrated in groups less than 25 cm and 19.4% of the cases are located above 50 cm. Dressings and advanced technologies were used in 30.02% of the patients in the contributory scheme compared to 24.35% in the subsidized scheme. 37% of the subsidized scheme had contagion vs 28% of the contributory scheme. The epithelialization rates were 67.27% in the contributory regime compared to 26% in the subsidized regime.
Conclusion: The prognostic factors that favor wound epithelialization are related to ulcers smaller than 25 cm, lesion evolution time under 36 months, having been managed with dressings and other advanced technologies, and belonging to the contributory regime.
Keywords: venous ulcers, chronic venous insufficiency, subsidized, contributive
Introduction
The 1991 Political Constitution established the right of all Colombians to health care as a public service provided under the direction, coordination and control of the State with the participation of public and private agents.1
In 1993, the General Social Security Health System (SGSSS) was created, which is a health system of regulated competition, based on a public-private and market-regulation mix, whose main sources of financing are the contributions of employees and employers, which finance the CONTRIBUTIVE regime, and the fiscal resources obtained through general taxes, which finance the SUBSIDIZED regime.1
But although health is a universal right for Colombians, the existing gap between patients of the subsidized and contributive regime is still visible in terms of waiting times in their care, accessibility to advanced therapeutic options and efficiency in timely management of their pathologies, sometimes having a negative impact on those patients with chronic pathologies as is the case of patients with venous ulcers secondary to Chronic Venous Disease.
The prevalence of venous ulcers in the population worldwide is as high as 1.5% in adults and 4.5% in people over 65 years old.2 They frequently present difficult healing and have long periods of duration that vary from a few weeks to a period of more than 10 years, never healing in some patients.3
They usually appear in the internal supramalleolar region, although they can also appear in the external area or be slightly ascending at the calf level. Its size is variable.
The skin surrounding the ulcer normally shows all the signs of dermatosis of venous insufficiency, with ocher pigmentation, liposclerosis, cyanosis, induration, sometimes even ossification.4
The comprehensive classification (CEAP) has been approved worldwide and is now an accepted standard for classifying chronic venous disorders, with CEAP being 6 active ulcers.5
In Colombia, it is difficult to know the incidence and prevalence of venous problems, especially venous ulcers, due to the scarcity of population-based epidemiological studies and little information regarding ethnic differences.6
The burden of venous leg ulceration may be exacerbated by the presence of wound infection. The results of microbiological studies show that 80% to 100% of leg ulcers can be colonized by bacteria.7 Producing in some cases infection, which leads to a delay in the healing process, requiring the use of topical or systemic antibiotics, sometimes requiring in-hospital management, which is the first reason for admission of the patient with venous ulcer requiring hospitalization.7
The ultimate goal of venous ulcer management is its closure and prevention of recurrence. For this, multiple strategies have been used that aim to manage the underlying pathology to suppress the deleterious effects of venous hypertension and local wound treatment.
Compression therapy (bandages or stockings) is currently considered the mainstay of venous leg ulcer treatment and together with maintaining a moist wound bed environment and primary coverage (moist dressing) is considered conventional management, leading to the enhancement of the healing process.7
Currently, there is a wide range of dressings that provide options according to the characteristics of ulcers; it has also been a subject of research to determine the superiority of one dressing vs others; however, according to the literature there does not seem to be a significant difference between them.8
However, a variety of different interventions can be used concurrently with compression, including debridement agents (Davies 2005; Cardinal 2009), vasoactive drugs (Robson 2006), topical applications (Robson 2006),7 and the use of advanced therapies such as recombinant human epidermal growth factor (Cacua 2018) that can generate an epithelialization rate of over 80% and has been successfully used in those recalcitrant patients with longstanding venous ulcers that fail to close.9
There are very few national and regional quantitative studies that describe and quantify the complications and factors associated with morbidity in patients with this condition. For the General System of Social Security in Health in Colombia, these patients are not quantified, they are neglected or poorly attended and unknown in location, which also leads to untimely care and exacerbation of signs and symptoms of the disease.
In view of the lack of quantitative studies in Colombia regarding the possible complications that a patient with active venous ulcer may develop. This study becomes a contribution to the outcome of the pathology and epidemiology in our country as it aims to provide elements that promote statistical data on patients suffering from venous ulcers.
Purpose
Determine the complications and factors associated with the morbidity of patients with venous ulcers (CEAP 6) in two health-care systems in Colombia that represent the two regimes of the health-care system (subsidized and contributive).
Methodology
Observational, descriptive, retrospective, multicenter, retrospective study, where the medical records of patients with a diagnosis of chronic venous insufficiency CEAP 6, who consulted for vascular surgery at the Ambulatory Surgery Center, an institution of the contributive regime of health, were reviewed, and in the Hospital de Kennedy which is an institution of the subsidized health regime during 2018 and 2019, performing the systematic and complete review of the entire clinical history in each patient that preceded the time of consultation for vascular surgery of 4 previous years, looking for specific variables regarding the study pathology. This research was approved by the Ethics committee in Biomedical Research CEDIFF. Act 1008–2021.
Inclusion Criteria
- Adult patients over 18 years.
- Patients diagnosed with CEAP 6 venous insufficiency; the evaluation was performed by a specialist doctor (vascular surgeon).
- Patients who had a complete medical history of 4 years since the assessment by vascular surgery.
- Patients in whom the clinical history reported linear measurement of the ulcer in all consultations.
- Ankle-arm index greater than 0.8.
- Patients with a clinical history with complete information on each of the study variables.
Exclusion Criteria
- Patients who had an ankle brachial index with values below 0.8.
- Patients with diagnosed occlusive arterial disease.
- Arterial, mixed, neuropathic or diabetic foot ulcer diagnosed.
- Patients without a complete medical record from the last four years.
- Patients who did not record linear ulcer measurement.
- Patients with medical history that did not have complete information on the variables to be studied.
Variables
The variables taken into account were classified as follows: Demographic variables, variables regarding the characteristics of the ulcer, other variables involving wound complications and outcome variables such as epithelialization, epithelialization time and percentage of closure were also determined.
Collection Techniques and Instruments
The primary source of clinical information for each patient was the clinical history, a pre-established format was used in EXCEL and a search of the histories was carried out, looking for the appropriate period according to the inclusion criteria, the clinical histories that did not meet the criteria were discarded and those that met the inclusion criteria were reviewed, filling out a database in an EXCEL file with parameterized and adjusted records, then the data analysis was performed after adjusting the database, descriptively with EXCEL, for the analytical analysis, the Chi2 test was used, with Yates adjustment as appropriate, and to determine the association of dependent and independent variables, a logistic regression was performed with the SPSS program.
Outcomes
The study population is composed of 105 patients, captured in the vascular surgery consultation during the years 2018 and 2019 with a diagnosis of CEAP 6 venous ulcer, who underwent a retrospective review of the clinical history up to four years prior to the first assessment or vascular surgery.
Characterization of the Study Population
Table 1 shows the characteristics of the population corresponding to sex, age, marital status, educational level, socioeconomic status and work activity according to the social affiliation regime.
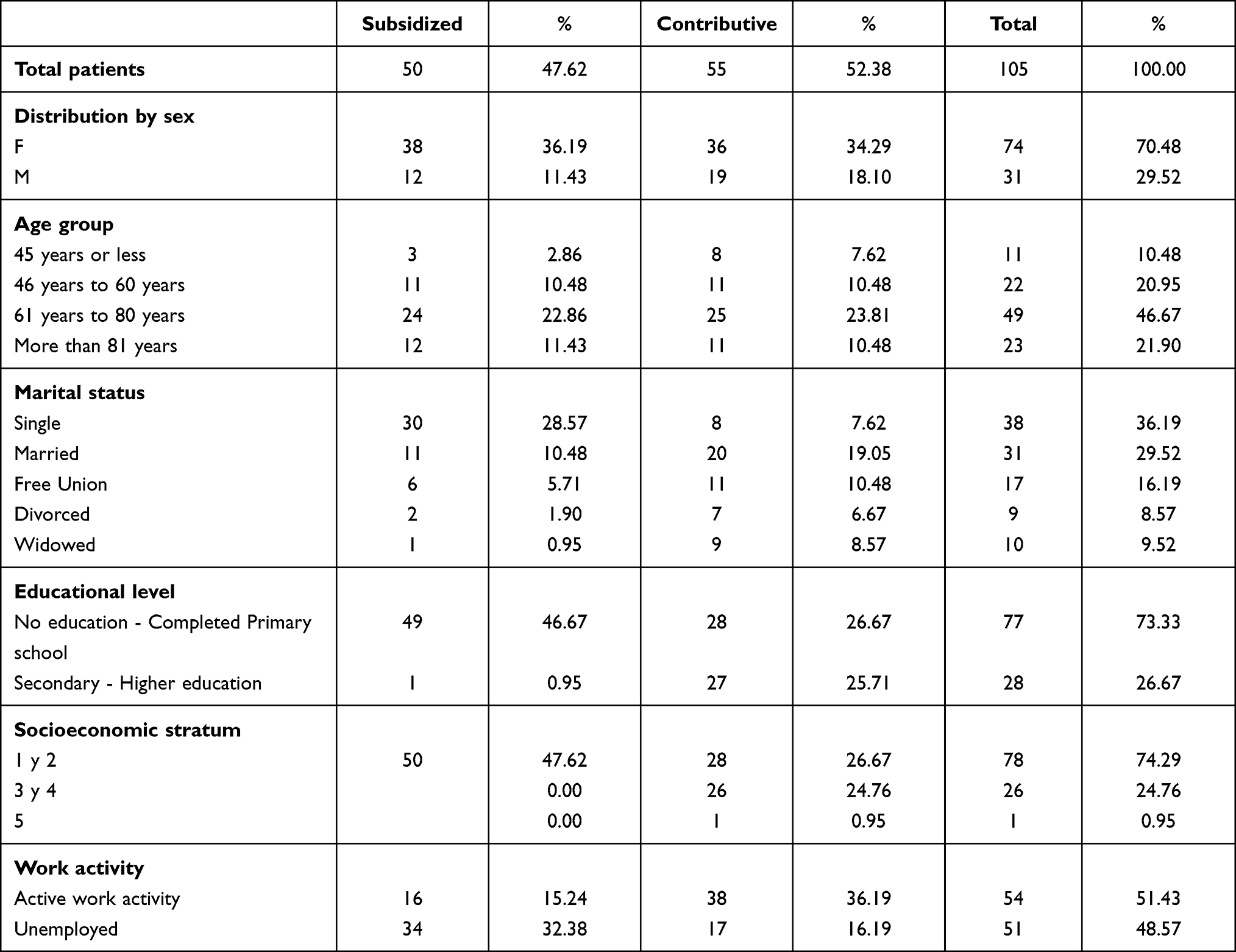 |
Table 1 Characterization of the Study Population |
Ulcers Characterization
The following is a description of the characteristics of the venous ulcers presented by the individuals under study. Table 2.
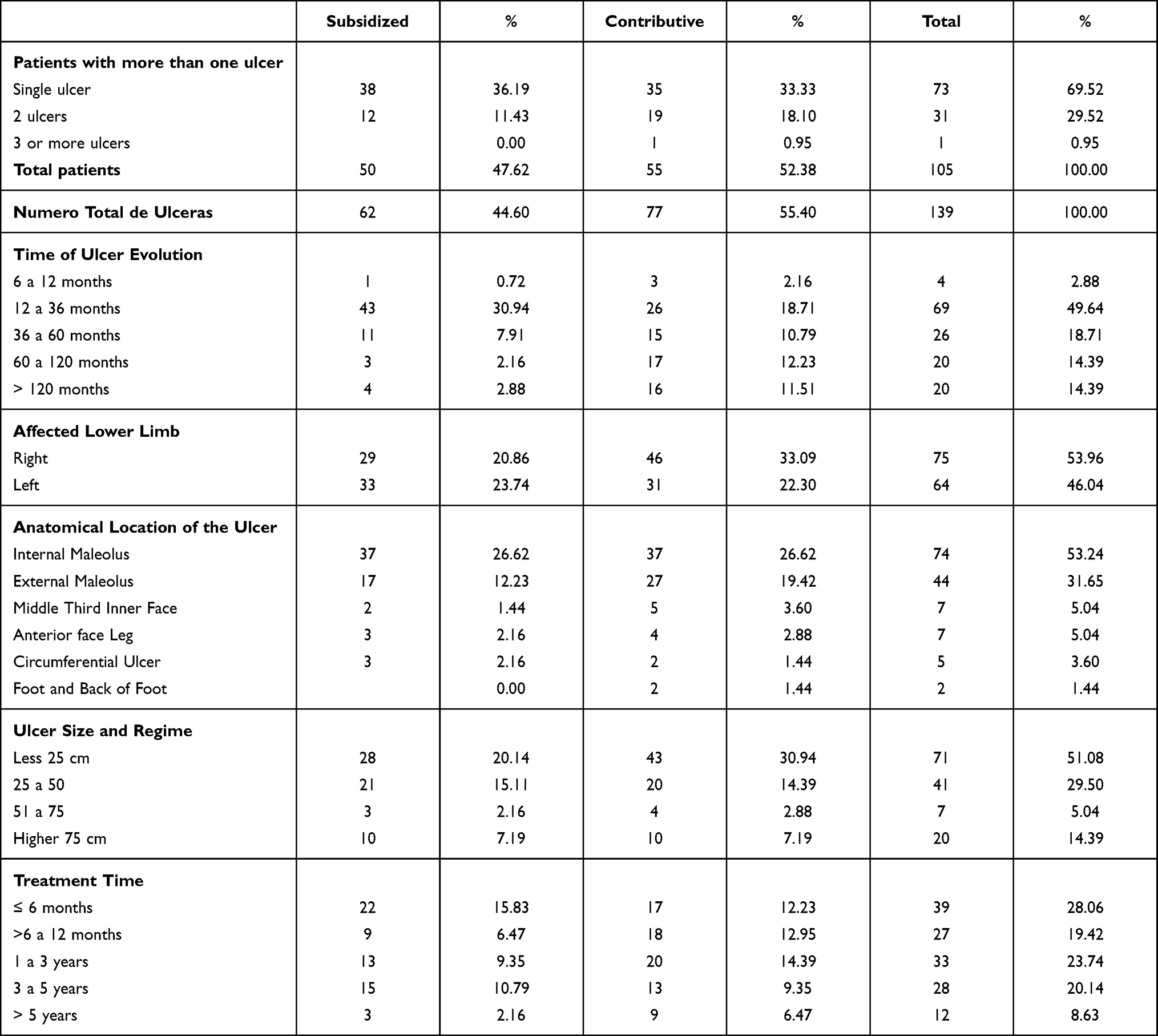 |
Table 2 Ulcers Characterization |
Type of Treatment
It was evidenced that, in the two affiliation regimes, there are wound clinic programs and that all patients were ordered and underwent healing and topical treatment in these clinics, which according to clinical history are carried out by nursing staff, however.
It was evidenced that the use of advanced technologies was requested by the specialist and that topical treatment other than advanced technology was carried out according to the protocols managed by each wound clinic.
The elastocompression was prescribed to 100% of the patients, and duplex to 83% of the patients, with the contributive regime predominating with 45%.
The infection was diagnosed by the treating physician based on the clinical signs that the patient presented in the venous ulcer, which were reported in the medical history as heat, redness, purulent discharge.
It was found that 69 patients presented at least one episode of infection, corresponding to 65% of the medical records reviewed, of which 30 patients corresponded to the contributory regimen with 28% and 39 patients to the subsidized regimen with 37%.
The patients who required culture were those who presented systemic signs and not only local signs of infection using a sample obtained by swab. (Table 3)
The elements used in the treatment in the wound clinic are summarized in two groups; were grouped into dressings and other technologies and another group that includes gels, tinctures and creams. (Table 4)
Recombinant Human Epidermal Growth Factor (hrEGF)
Among the different treatments found in the present review, an important predominance was found in the use of Human Recombinant Epidermal Growth Factor (hRGF); therefore, and according to the frequency of use, it was decided to separate it into a separate group for the analysis (Figure 1).
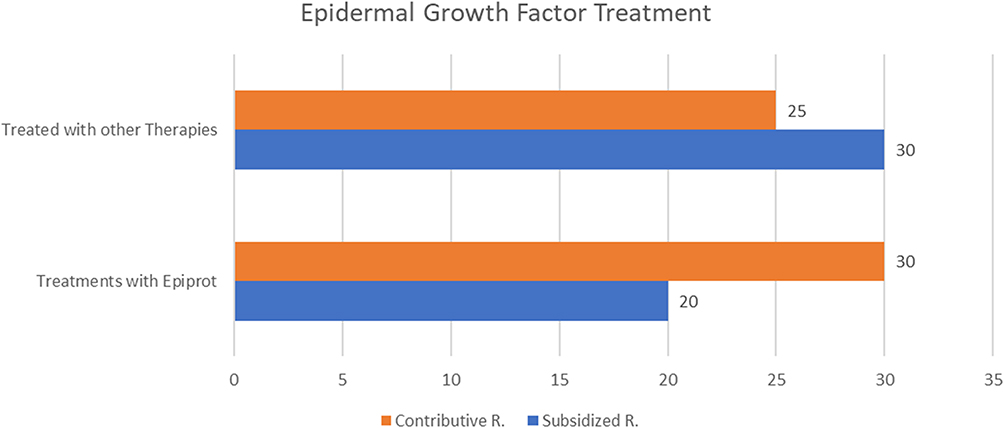 |
Figure 1 Patients with FCErh treatment, Contributive and Subsidized Regime. |
Antibiotics – Analgesic
Regarding antibiotics, Table 5 shows the frequency of the different antibiotics and analgesics prescribed.
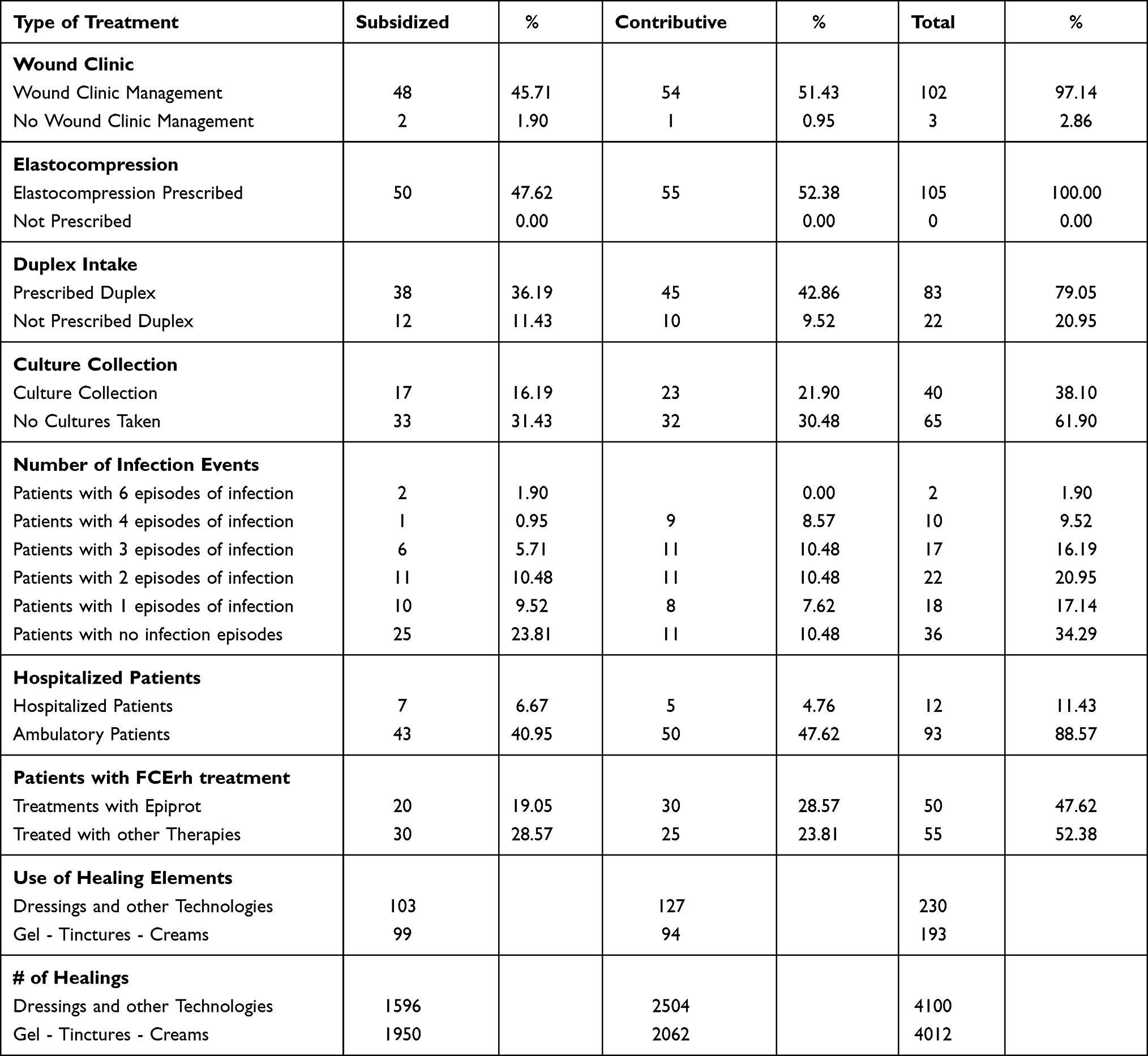 |
Table 3 Type of Treatment |
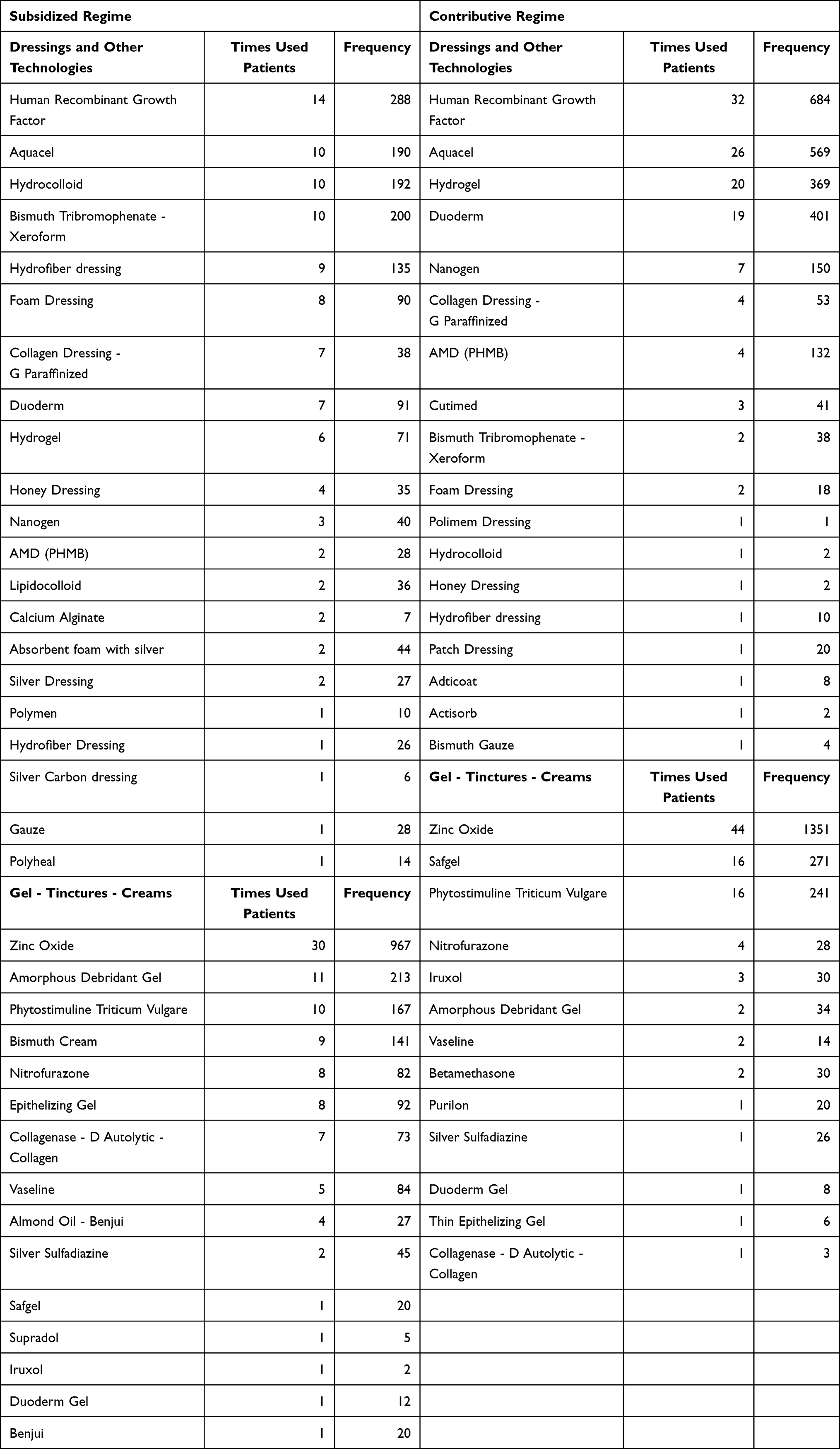 |
Table 4 Frequency of Dressings and Other Technologies/Gel - Dyes and Creams - Contributive and Subsidized Regime |
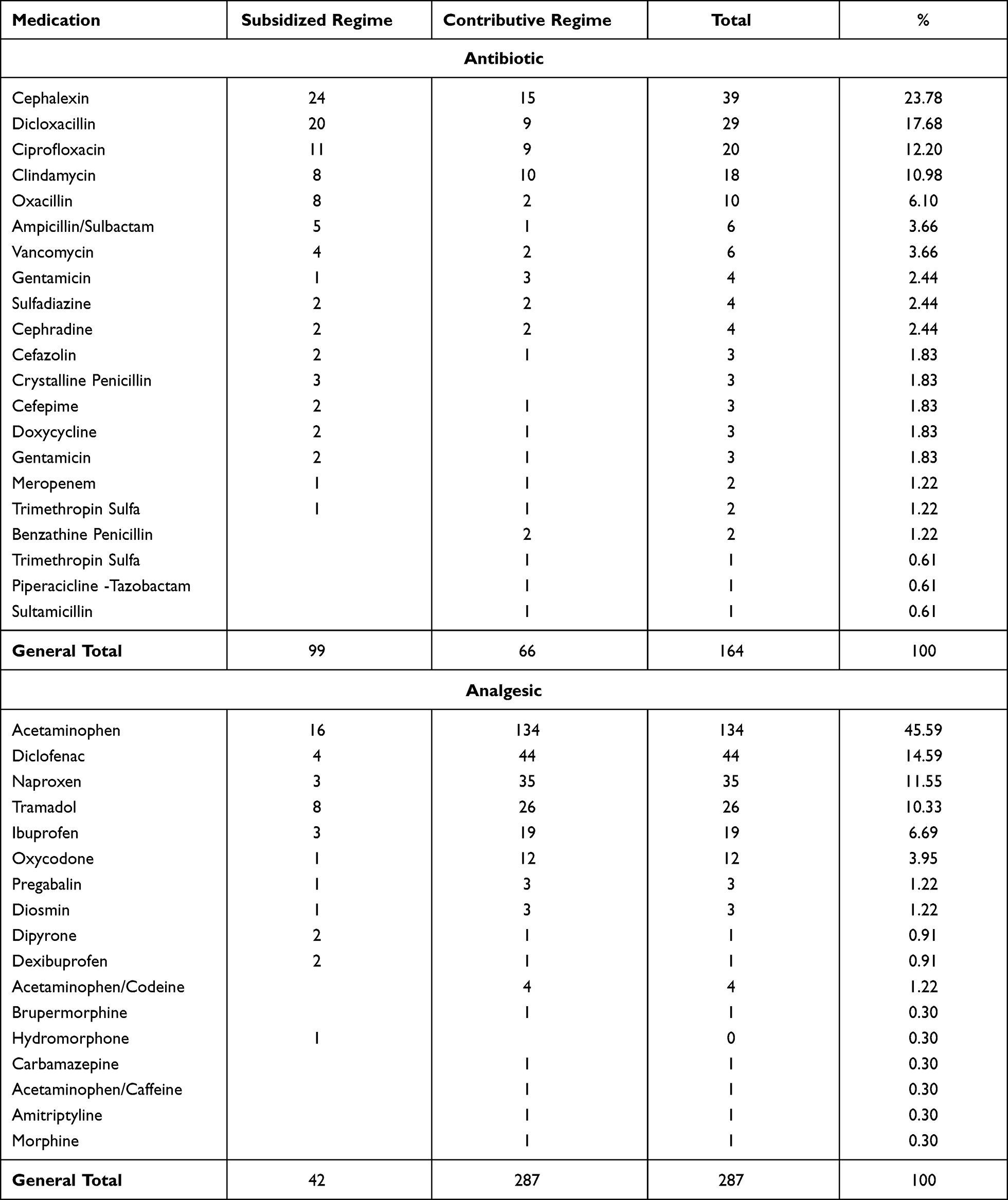 |
Table 5 Frequency of Antibiotic and Analgesics Prescriptions - Contributive and Subsidized Regime |
Observed Outcomes
The results were measured as follows:
Epithelialization
According to the information generated by the review of the medical records it was possible to determine the outcome of epithelialization, which we will analyze below:
In the contributory regimen, 67.27% of the patients had complete closure compared to 26% to the subsidized regimen.
Considering that there were several patients who presented more than one ulcer in their lower limbs, the following table shows the behavior of the 139 ulcers regarding epithelialization, shows that in the contributive regime 64.94% of the ulcers had complete closure against 35.06% of those that did not, regarding the subsidized regime 24.19% of the ulcers had complete closure against 75.81% that did not.
Table 6 shows the total percentage of epithelialization of the wounds and their epithelialization behavior, according to its initial size and the time of evolution of the wound.
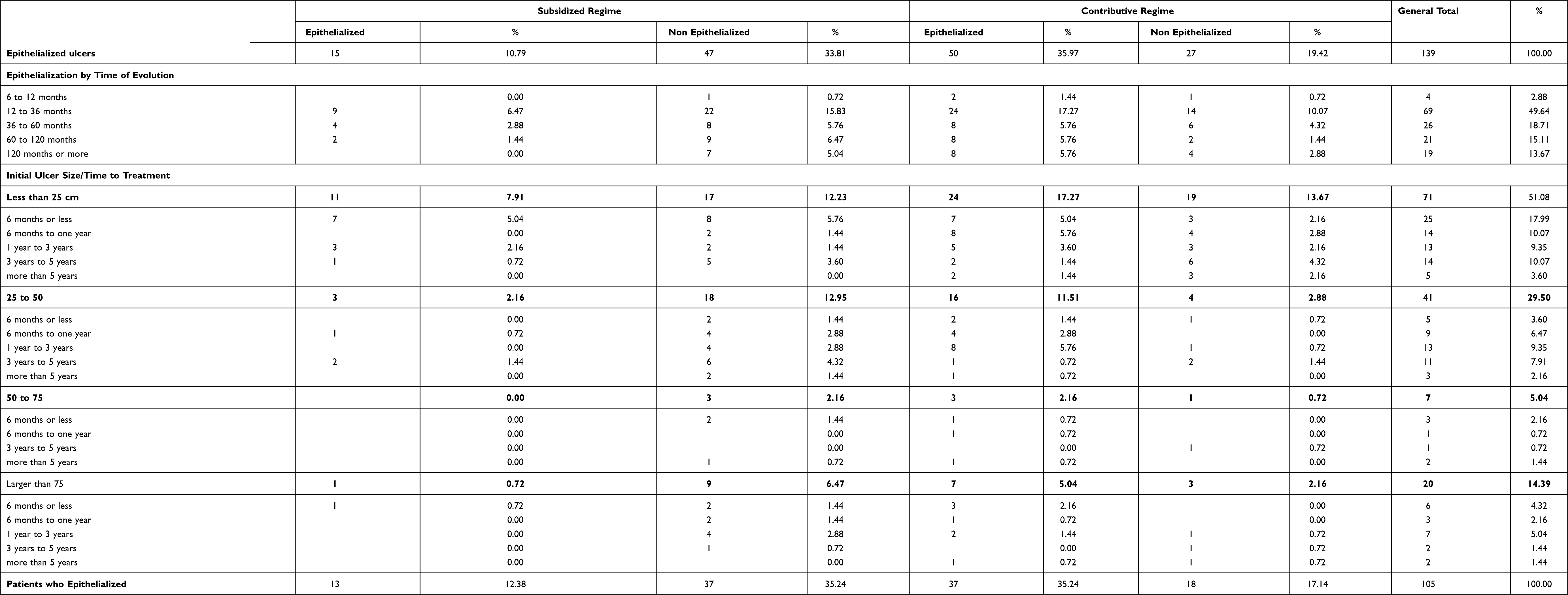 |
Table 6 Observed Outcomes |
Additionally, the relationship between epithelialization according to the initial size and the episodes of infection and which patients required disability is shown.
According to the measurements of the ulcers registered in the clinical histories that registered a complete closure of the ulcer, 70% of the patients prescribed with rhEGF closed completely, compared to 30% of other therapies, as regards the ulcers that did not epithelialize the rhEGF, it has 30% regarding other treatments that have 69%, as it was specified from the data found another specific work will be carried out for the Recombinant Human Epidermal Growth Factor.
As well as the specialties that were consulted during the period reviewed, according to the regimen and the number of consultations registered by general medicine and vascular surgery during the time of the study. Table 7.
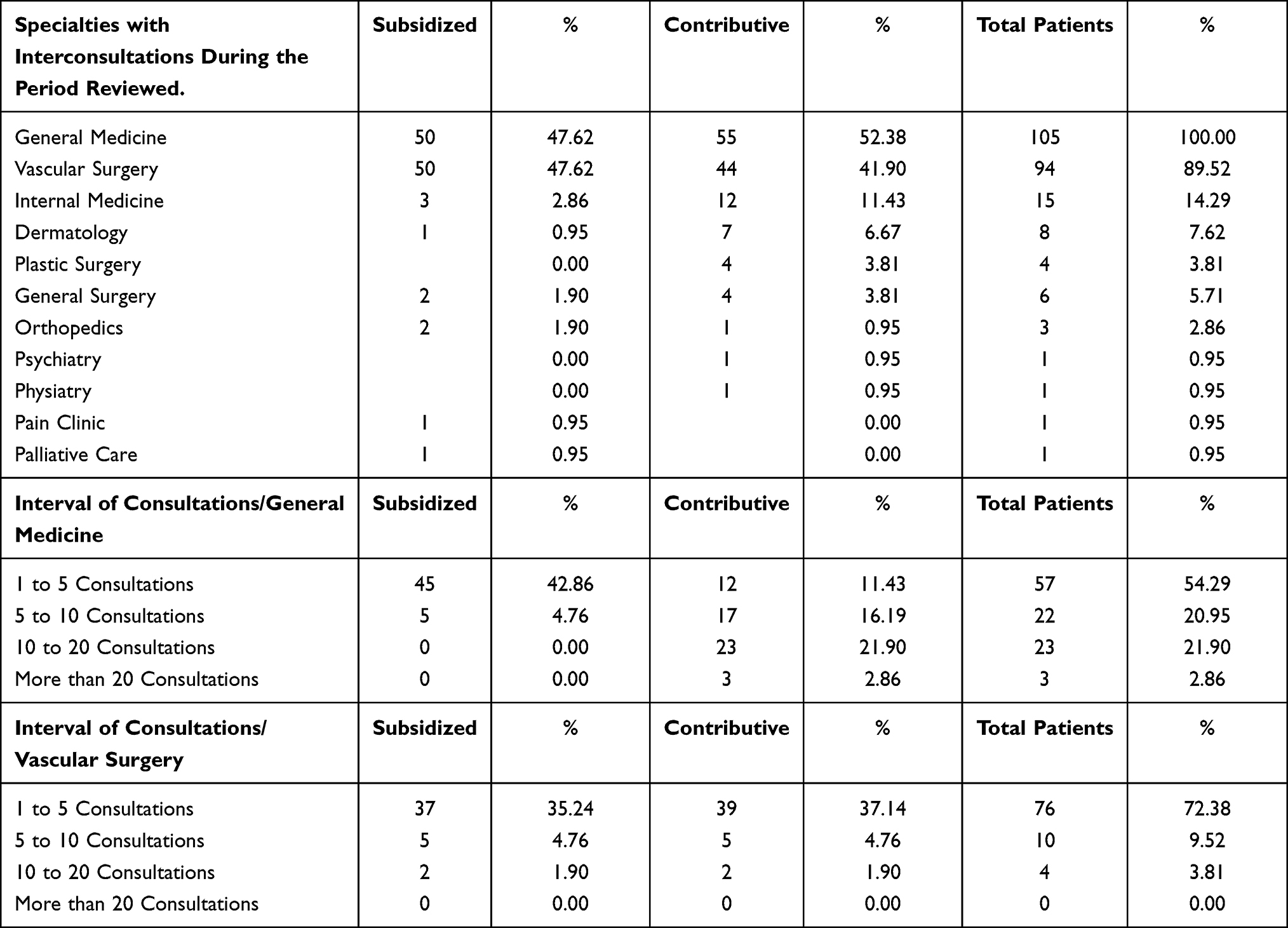 |
Table 7 Specialties with Interconsultations |
Regarding the association of epithelialization in the 139 ulcers between the contributive regimen and the subsidized regime, there is a 5.8 times more probability that ulcer epithelializes in the contributive regime than in the subsidized regime (p = 0.0000) (CI = 2.75–12.23), an association that varies according to the initial size of the ulcer. To determine the association between the variables regime and size of the ulcer with respect to the epithelialization descent, the logistic regression determined that there is a statistically significant association between the variable regime; Exp (B) 5.5 (p = 0.0000) (CI = 2.048–14.964) in contrast to the ulcer size variables that were not statistically significant Table 8.
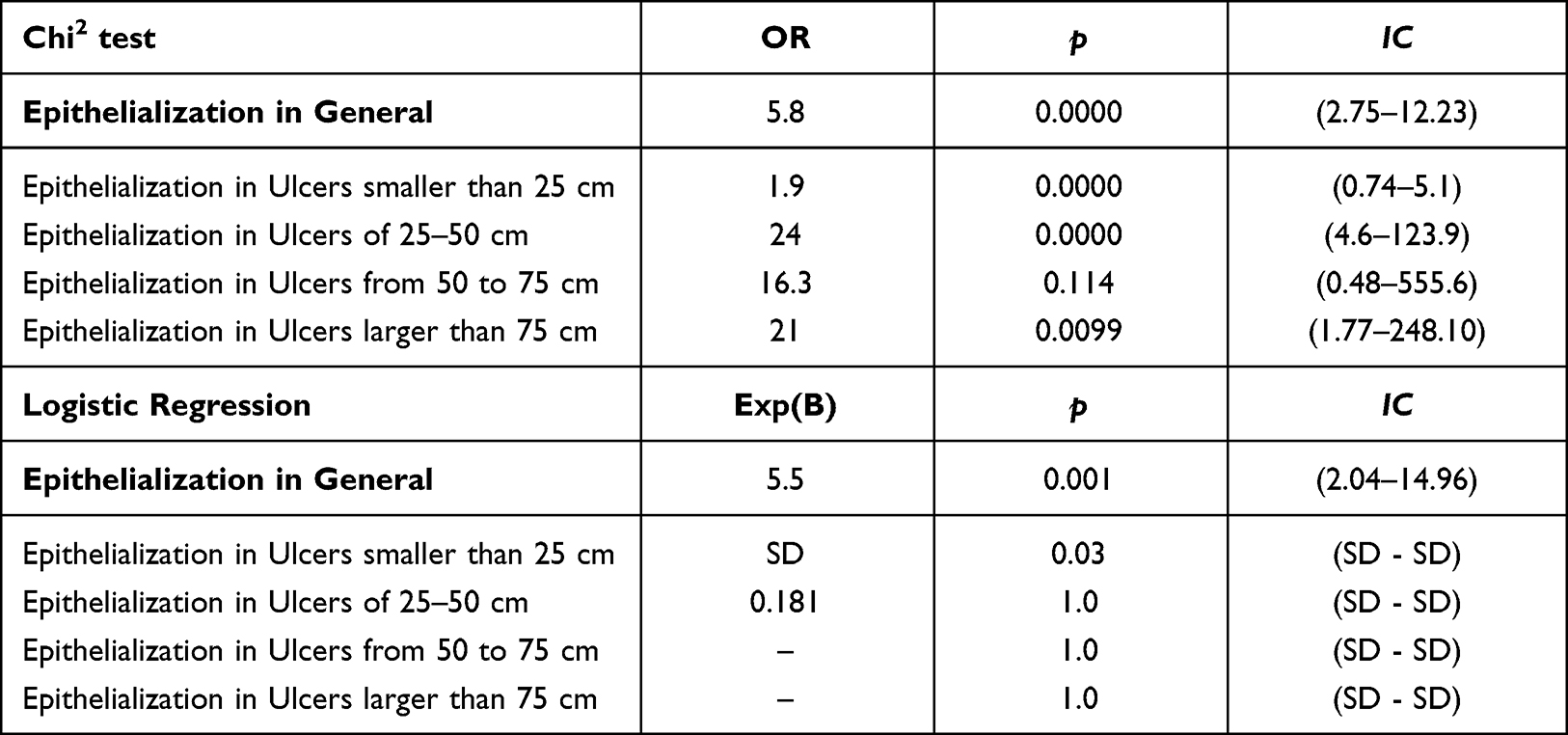 |
Table 8 Association Between Epithelialization vs Regimen Contributive and Subsidized/Ulcer Size at the Start of Treatment; Chi2 Test and Logistic Regression |
Discussion
In Colombia, there are few records on the epidemiology of this pathology and little information on ethnic differences and other population characteristics, however, it has been estimated worldwide that the frequency of this type of lesions affects about 1–2% of the population. In addition, the ratio of women to men is 3:1, which coincides with our study in terms of age group and predominant gender.10
Regarding the socioeconomic group and educational level, we found in this study, a predominance of socioeconomic stratum 1 and 2 (low) with a lower educational level, which correlates with the Latin American literature since Marques in his research conducted in Brazil reports a higher prevalence of venous ulcers in individuals of low socioeconomic stratum, low income and low educational level.11
The studies such as Vasconcelos’s report the predominance of these patients without formal work, retired or who are unemployed at the time the ulceration occurs.4 In our study, this situation was related to the level of social security that the patient had. In the subsidized regime most of the patients were unemployed while in the contributory regime they had a current work activity.12
We already know that venous ulcers are a type of wound that can take a long time to heal, it is reported in the literature that 50% of venous ulcers need more than a year to heal and 10% can take up to 5 years. Therefore, the time of evolution of these ulcers can be quite insidious, which was found in our study in which the largest number of patients had more than 12 months of evolution of this lesion.13 Associated with this, the most frequent site reported in the literature of occurrence of these wounds is predominantly in the internal and external malleoli, a confirmed finding in our study.14
The literature reports that delayed closure, disproportionate pain, abnormal odor, friable granulation tissue should lead to suspect of an infected ulcer. The percentages of infection reported in the literature range from 30% according to the study conducted in London in 2017 by Guest,15 to 60% according to the study published in Chile,5 thus finding higher percentage at the Latin American level. In our study, it was found that the infection rate was 60%, taking into account the clinical signs reported in the clinical history that justified the use of antibiotic therapy in the patient.
Our study showed that 65.71% of the patients presented at least one episode of infection, being first-generation cephalosporins, penicillins and fluoroquinolones the most used, however, only 38.1% of these patients required culture taking.
Venous ulcers are associated with significant levels of pain, their prevalence rate for this symptom according to the literature ranges from 48% to 81% and moderate to severe levels of pain are reported in 19–46% of patients.16
The study carried out in Chile in 2006 by Dr. Arbuto and Dr. Salas reported that 97% of patients with venous ulcer were consuming analgesics (NSAIDs, opioids or others), for our study the use of analgesics was required, predominantly acetaminophen and secondly naproxen, also tramadol and other NSAIDs.
Regarding the number of hospitalizations in the study conducted by Sosa and Chirino, it was reported that out of 81 patients admitted to the Phlebolymphology Service of the National Institute of Angiology and Vascular Surgery (INACV) with a diagnosis of phlebostatic ulcers, 72.8% required hospitalization, in our study, the percentage of patients hospitalized during treatment was 23.09%.17
Compression therapy, through bandages, is considered the Gold Standard in the treatment of venous ulcers.18 This measure increases the healing rate of venous ulcers by reducing venous stasis,19 In our study, all patients had multilayer compression in addition to unsaturated topical treatment.
In Colombia, access to specialized groups for the management of venous ulcer has a direct impact on its evolution and resolution, extending care times, health costs and reintegration to the patient’s activities. This is exacerbated in patients under the subsidized regime.
Evidence confirms that the management of chronic wounds with a multidisciplinary wound care team significantly improves wound healing and reduces the severity of pain associated with the wound and the daily treatments required for wounds compared to people who are not managed by such a team;19 in our study 97.14% of patients received their treatment by wound clinic involving qualified personnel for their management.
Regarding the use of topical treatment and special dressings for wound care in patients with venous ulcers, the current evidence remains controversial, since the use of these special materials occupies 22% to 30% of the total cost to cure an ulcer. Currently, there is a wide range of dressings and topical creams that provide options according to the characteristics of ulcer.
In our study, multiple creams, gels and dressings were used based on the protocols that wound clinic employs, regarding the use of dressings and other technologies, they were used in 30% of patients in the contributive regime vs 24.35% of patients in the subsidized regime.
Regarding the epithelialization and healing of venous ulcers, Selvaraj stated that patients of low and middle socioeconomic stratum favored the development of venous ulcers.20 Similarly, Marques found a higher prevalence in individuals of low socioeconomic stratum, low income and low educational level,11 as did Alvarez del Rio who reported that belonging to socioeconomic stratum lower than 2 was a negative factor for the healing of venous ulcers. Findings that were also present in this research.21
Our study showed that 67.27% of patients in the contributive regime achieved epithelialization vs 26% of patients in the subsidized regime, showing additionally that size is crucial for epithelialization, with a greater epithelialization in smaller ulcers of less than 50 cm (48.21%) vs ulcers of more than 50 cm (40.7%) and in comparison, with the subsidized regime. The overall epithelialization rate was higher in patients of the contributive regime (64.94%) vs the subsidized regime (29.19%).
Similarly, patients who have a longer evolution time of their ulcer require more time in treatment to achieve its closure and this is related to the regime, since patients in the subsidized regime have a worse prognosis than patients in the contributive regime.
Regarding the use of advanced technologies, growth factors have recently gained clinical importance in wound treatment. It has been shown that the application of recombinant growth factors activates cell migration, proliferation and differentiation which allows external modulation of the healing process.22
One of these, epidermal growth factor is secreted by fibroblasts, platelets and macrophages and is localized throughout the epidermis, particularly in the basal layer.23 Several studies reported in the literature have used epidermal growth factor in the treatment of chronic wounds reporting positive results, likewise several clinical trials have evaluated the successful regenerative potential of EGF in diabetic ulcers and other retrospective studies have assessed its use in venous ulcers.24,25 Therefore, the use of EGF appears to be an interesting and promising alternative for the treatment of chronic ulcers, such as those of venous etiology.
Our study showed that of the 55 patients who epithelialized (49.52%), 35 (63.6%) achieved it with the use of FCE and of these 77.14% (27 patients) achieved it in 8 weeks or less.
Suffering from an ulcer involves long periods of incapacity for work and difficulty in ambulation. Our study showed that the percentage of incapacity in these patients was 65.71%, observing that 100% of the patients actively working in the subsidized regime required incapacity, which corresponds to 16 patients vs 20 of 38 patients actively working, which corresponds to 19.04% of the contributive regime, which leads to an increase in lost working days and a greater increase in the cost of treatment of this pathology.
Limitations
A limitation of the study was the under-recording found in the clinical histories, these did not have in many occasions all the necessary data in the evaluations and consultations that these patients had regarding their ulcer, reason for which the sample was reduced. The data that was rarely recorded corresponded to the size of the ulcer in linear terms.
In addition, it is also important to mention that in the hospital in which the patients of the subsidized regime were registered, the digital medical record was implemented until 2017. The previous years have some folios of the manual clinical history uploaded in PDF files in the system; however, not all patients have all the documentation of their care, and this is a characteristic of the manual medical history, as the handwriting in some parts does not allow for interpretation, which is why many patients could not be included in this study.
Conclusions
Venous ulcer disease is a public health problem that causes an increase in the cost of care and an impact on the patient’s quality of life when there are delays or suboptimal treatments. This deficit is observed to a greater extent in the subsidized regime.
The prognostic factors that favor wound epithelialization are related to ulcers smaller than 25 cm, lesion evolution time under 36 months, having been managed with dressings and other advanced technologies, and belonging to the contributory regime.
The factors that delay healing are associated with wound size greater than 25 cm, time of evolution greater than 36 months, use of therapy with gels or creams and belonging to the subsidized regime in which the socioeconomic stratum is 1 and 2.
According to the records of the study, it can be seen that access to technologies such as growth factor is lower in the subsidized regime, since only 40% of the group of 50 patients were able to access and benefit from this treatment.
The highest percentage of hospitalizations was obtained in the subsidized regime, and all patients who were working required incapacity for work.
Ethical Considerations
Regarding ethical considerations, the study was submitted for review and approval by the Research Ethics Committee - CEDIFF, this being a retrospective study, the procedure of making a series of communications to the research subjects was approved where they were requested their consent to participate in the study only with their clinical data for statistical purposes, no information on the identification of the subjects would be used and their confidentiality and privacy would be maintained, the researchers to carry out this study are welcomed and declare that the study was carried out in accordance with the Declaration of Helsinki and the respective permits were requested for each of the institutions where the study was carried out.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Calderón CA, Botero JC, Bolaños JO, Martínez RR. The Colombian healthcare system: 20 years of achievements and problems. Cien Saude Colet. 2011;16(6). ISSN 1413-8123. doi:10.1590/S1413-81232011000600020
2. Evangelista DG, Magalhães ERM, Moretão DIC, Stival MM, Lima LR. Impact of chronic wounds on the quality of life of users of the family health strategy. Rev Enferm Centro O Min. 2012;2(2):254–263.
3. Moffatt CJ, Dorman MC. Recurrence of leg ulcers within a community service. J Wound Care. 1995;4(2):57–61. doi:10.12968/jowc.1995.4.2.57
4. Ramírez LS, Leonard DP, López AÁ, Díaz LC, Villalonga LE. Bacterial germs frequently isolated in phlebostatic ulcers of admitted patients. Cuban J Angiol Vasc Surg. 2021;22(1):e181.
5. Eklof B, Rutherford RB, Bergan JJ, et al. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004;40:1248–1252. doi:10.1016/j.jvs.2004.09.027
6. García Vargas WG, Pastrana Parra MF, Vargas CruZ LD; Universidad de Ciencias Aplicadas y Ambientales. Calidad de vida en personas que presentan úlceras venosas en miembros inferiores. Una revisión integradora. Available from: https://repository.udca.edu.co/bitstream/11158/931/1/Calidad%20de%20vida%20en%20%C3%BAlceras%20venosas.pdf.
7. O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG, Martyn-St James M, Richardson R. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev. 2014;1:
8. Sánchez-Nicolat NE, Guardado-Bermúdez F, Arriaga-Caballero JE, Torres-Martínez JA. Review in venous ulcers: epidemiology, current pathophysiology, diagnosis and treatment. Angiol Mex Mag. 2019;47(1):26–38.
9. Cacua Sanchez MT, Giraldo LF, Díaz JA. Efficacy of human recombinant epidermal growth factors vs conventional therapy for the treatment of chronic venous ulcers: a retrospective case series. Wounds. 2021;33(2):41–49. PMID: 33591927.
10. Beebe-Dimmer J, Pfeifer J, Engle J, Schottenfeld J. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol. 2005;15(3):175–184. doi:10.1016/j.annepidem.2004.05.015
11. de Souza E, Yoshida W, de Melo V, Aragão J, de Oliveira L. Ulcer due to chronic venous disease: a sociodemographic study in northeastern Brazil. Ann Vasc Surg. 2013;27:571–576. doi:10.1016/j.avsg.2012.07.021
12. Vasconcelos G, Fernández I, da Silva Medeiros RK, et al. Characterization of people with venous ulcers in Brazil and Portugal: comparative study. Glob Nurs. 2013;12(32):62–74.
13. Consensus on Vascular Ulcers and Diabetic Foot of the Spanish Association of Vascular Nursing and Wounds (AEEVH)], 3rd ed. [in Spanish] Spanish Association of Vascular Nursing and Wounds, 2017.
14. Xie T, Ye J, Rerkasem K, Mani R. Venous ulcer remains a clinical challenge: an update. Trauma Burns. 2018;6:18. doi:10.1186/s41038-018-0119-y
15. Guest JF, Fuller GW, Vowden P. Venous leg ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J. 2018;15(1):29–37. PMID: 29243398. doi:10.1111/iwj.12814
16. Nemeth KA, Harrison MB, Graham ID, Burke S. Pain in pure and mixed aetiology venous leg ulcers: a three-phase point prevalence study. J Wound Care. 2003;12:336–340. doi:10.12968/jowc.2003.12.9.26532
17. Vázquez OR, Díaz LC, Mantilla ME, Villalonga LE. Characterization of patients hospitalized for phlebostatic ulcers. Cuban J Angiol Vasc Surg. 2019;20(3):e27.
18. Moffatt CJ, Franks PJ, Doherty DC, Martin R, Blewett R, Ross F. Prevalence of leg ulceration in a London population. QJM. 2004;97(7):431–437. doi:10.1093/qjmed/hch075
19. Marola S, Ferrarese A, Solej M, Enrico S, Nano M, Martino V. Management of venous ulcers: state of the art. Int J Surg. 2016;33(Supplement 1):S132–S134. doi:10.1016/j.ijsu.2016.06.015
20. Selvaraj D, Kota A, Premkumar P, Stephen E, Agarwal S. Socio-demography and clinical profile of venous ulcers. Wound Med. 2017;19:1–4. doi:10.1016/j.wndm.2017.06.004
21. Alvarez-Del-Rio RF. Factors associated to the cicatrization success of lower-limb ulcer of venous etiology. Invest Educ Enferm. 2018;36(3):e08–e08. ISSN 0120-5307. doi:10.17533/udea.iee.v36n3e08
22. Yamakawa S, Hayashida K. Advances in surgical applications of growth factors for wound healing. Burn Trauma. 2019;7:10. doi:10.1186/s41038-019-0148-1
23. Nanney LB, Magid M, Stoscheck CM, King LE
24. Gomez-Villa R, Aguilar-Rebolledo F, Lozano-Platonoff A, et al. Efficacy of intralesional recombinant human epidermal growth factor in diabetic foot ulcers in Mexican patients: a randomized double-blinded controlled trial. Wound Repair Regen. 2014;22(4):497–503. doi:10.1111/wrr.12187
25. Dumantepe M, Fazliogullari O, Seren M, Uyar I, Basar F. Efficacy of intralesional recombinant human epidermal growth factor in chronic diabetic foot ulcers. Growth Factors. 2015;33(2):128–132. doi:10.3109/08977194.2015.1031898
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.