")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 11
Social Return On Investment For Patient Treated By Continuous Ambulatory Peritoneal Dialysis: A Case Study In Ubon Ratchathani Province, Thailand
Authors Lophongpanit P , Tongsiri S, Thongprasert N
Received 30 May 2019
Accepted for publication 10 September 2019
Published 23 September 2019 Volume 2019:11 Pages 569—578
DOI https://doi.org/10.2147/CEOR.S217785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Pattama Lophongpanit,1 Sirinart Tongsiri,2 Nalinee Thongprasert3
1Health Science Program, Faculty of Medicine, Mahasarakham University, Talat Subdistrict, Mueang, Maha Sarakham Province 44000, Thailand; 2Faculty of Medicine, Mahasarakham University, Talat Subdistrict, Mueang, Maha Sarakham Province 44000, Thailand; 3Faculty of Business Administration and Management, Ubon Ratchathani Rajabhat University, Mueang, Ubon Ratchathani Province 34000, Thailand
Correspondence: Pattama Lophongpanit
Faculty of Medicine, Mahasarakham University, 269 Talat Subdistrict, Mueang District, Maha Sarakham Province 44000, Thailand
Tel +668 1876 5762
Email [email protected]
Purpose: In Thailand, continuous ambulatory peritoneal dialysis (CAPD) has become the first option for renal replacement therapy (RRT) under the universal health coverage scheme (UCS) for more than a decade. However, there is limited evidence to demonstrate the social value of this policy. Hence, this study aims to evaluate the social return on investment (SROI) of end-stage renal disease (ESRD) patients treated by CAPD modality under UCS in Ubon Ratchathani province, Thailand.
Patients and methods: This study follows six steps of SROI principle and framework. It is a mixed method of exploratory sequential design divided into 2 parts; the first part is qualitative research using content analytics to ascertain find out what is the cost in societal view and social value outcome. Then in the second part, take it information gathered from the first part was used to create a research tool to quantitatively collect the data from 191 informants. The data has been analyzed to calculate SROI ratio and interpret the amount of social value created per 1 Thai Baht (THB) of investment.
Results: The key social value outcomes are; CAPD patients have a good quality of life, not being a burden on society and willing to undergo kidney transplantation in the future. The costs in societal view are direct medical costs reimbursement from the national health security office (NHSO), direct non-medical costs, and indirect costs are CAPD patients’ out-of-pocket expense. The proportion of the costs from NHSO and the patient is 81:19. The SROI ratio is 1.60:1. It means that 1 THB on investment can generate the social value of 1.60 THB.
Conclusion: The investment for ESRD patient treated by CAPD modality is worth social value benefits.
Keywords: social value, social return on investment, continuous ambulatory peritoneal dialysis
Introduction
End-stage renal disease (ESRD) is becoming a global major health challenge as its etiology has been emerging with age-related renal function decline accelerated in diabetes, hypertension, and renal disorder.1–3 Renal replacement therapy (RRT) as peritoneal dialysis (PD), hemodialysis (HD) and kidney transplantation (KT) are three modality choices for ESRD treatment.4,5 In 2010, 2.168 million people received RRT worldwide, and this number will be increase to 5·439 million people by 2030, with the most growth in Asia.4
RRT had not been initially covered by the universal coverage scheme (UCS) in Thailand because of its cost. However, there was intense pressure from various stakeholders to include RRT to UCS campaign on the grounds of equity, emphasizing the disparity between the three public schemes, as well as the catastrophic expenditures incurred by patients on low incomes.6,7 In 2004–2006, The national health security office (NHSO), which responsible for UCS commissioned series of study using cost-effectiveness analysis (CEA) and cost-utility analysis (CUA) to provide scientific evidence for policymakers to make decisions on whether to provide dialysis treatments for ESRD patients under USC. The result shows that the annual cost of HD and PD per quality-adjusted life year were higher than three times of gross domestic product (GDP) per capita of Thai people. So, neither HD nor PD is cost-effective,8 but PD could be provided cheaper than HD and with better outcomes.7,9 Finally, in 2008, RRT had been included in USC campaign as a PD first policy with HD and KT were second choices treatment for those who are not eligible for PD.9 Afterward, the prevalence of RRT increased sharply from 528.4 patient per million population (pmp) during the year 2008 to 1,306.6 pmp in 2015. 88.8% of RRT under UCS received continuous ambulatory peritoneal dialysis (CAPD) modality, 25.1% received HD, and 13.9% received KT, respectively.10
CAPD has been shown to increase the life expectancy of patients from at least five years11 compared to the previous situation where median patient survival time was 46.4 months.12 Furthermore, quality of life was measured using the European Quality of Life Measure-5 Domain-5-Level (EQ-5D-5L) and visual analog scale (VAS). The results show that mean utility and VAS scores of CAPD patients were 0.83 (SD 0.23) and 69.9 (SD 19.9), respectively. There were no significant differences in quality of life between PD and HD patients in all domains.13 Meanwhile, there are a large number of plastic waste from this treatment, which may affect the environment. So, treatment with CAPD modality offers better clinical outcome for a decade, but there is limited evidence to demonstrate the impact on social value, which is social, environmental, and financial.
There are many methods for measuring social value.14,15 At this time, no method has been widely adopted throughout the organizations as the standard for measuring social value. So, it is crucial to choose the methods that best suit their specific requirements. However, WHO European Region reviews the methodology of SROI and finds that SROI represents an opportunity to evaluate investments by considering value produced for multiple stakeholders in the triple bottom line, which are economic, social, and environmental then quantifies that value in monetary terms. They are coherent with the key features of the Health 2020 policy framework and the 2030 Agenda for Sustainable Development.16
Ubon Ratchathani province is located in the northeast region of Thailand. The sociodemographic data of CAPD patients compare with other area were similar. There are 10 CAPD service centers distribution through public hospitals to reduce patients’ travel time and a home visit from CAPD team. The average of CAPD assesses rate from 2013–2015 was 92.45% and 95.55% in 2016, respectively. CAPD project provided not only budget for treatment, but also improve quality of life and the environment, which had not assessed social value before. Hence, this study is a pilot project applying the SROI methodology to evaluate the social return on investment of ESRD patients treated with CAPD modality (CAPD patients) under UCS in NHSO region 10 Ubon Ratchathani, Thailand.
Methods
This study followed 6 stages of SROI methodology, include establishing scope of the study and identifying stakeholders, mapping outcomes as a result of stakeholder interviews into a “Theory of Change”, deciding on indicators of change for outcomes and assigning a value for them, establishing impact of the outcome in financial terms, calculating the SROI ratio, and feedback results to stakeholders.17
It is a mixed method of exploratory sequential design divided into 2 parts; the first part is qualitative research using content analytics to ascertain find out what is the cost in societal view and social value outcome. Then in the second part, take it information gathered from the first part was used to create a research tool to collect the data from the informants quantitatively.
The informants divided into 2 groups, the first group for the qualitative study were key stakeholders and the second group for the quantitative study was CAPD patients under UCS in the Fiscal year 2016 who remained alive and did not change their treatment between October 2016–July 2018.
Data has been collected from February–July 2018. The qualitative data using content analysis to develop the outcome of CAPD project and construct outcome indicator to value them. The quantitative data using descriptive statistics to analyze the cost and benefit of CAPD project.
This study received the approval from the Research Ethics Committees of Mahasarakham University (074/2560) before the commencement. All participants had been informed about the study and are given time to consider before provided written informed consent.
Results
Stage 1: Establishing Scope And Identifying Stakeholders
The meeting with CAPD project manager from NHSO and 10 peritoneal dialysis nurses (PD nurse) from 10 CAPD service centers in Ubon Ratchathani was organized to start this stage, and it allowed the authors to learn about CAPD project under USC, who are stakeholders and how to approach them. The aims of the project which were; the patients can access and receive quality services for their good quality of life, not being the burden of society and ready for KT in the future. The project supported budget for PD center services 3,000 THB (92.85 USD) per patient head per month, Erythropoietin injections depend on their hematocrit and the monthly dialysate delivery to patients’ house. Meanwhile, CAPD patients and families have invested in their treatment as house renovation cost, transportation cost for follow up, and some medical materials. Therefore, the stakeholders include CAPD patients, caregivers, CAPD service centers, and NHSO. (see Table 1) In August 2017, there were 2,328 CAPD patients under USC in Ubon Ratchathani. In view of time and budget constraints, the scope of the study was narrowed to evaluate the social return on investment of incident CAPD patients (N=224) in the Fiscal year 2016 who remained alive and did not change their treatment between October 2016–July 2018.
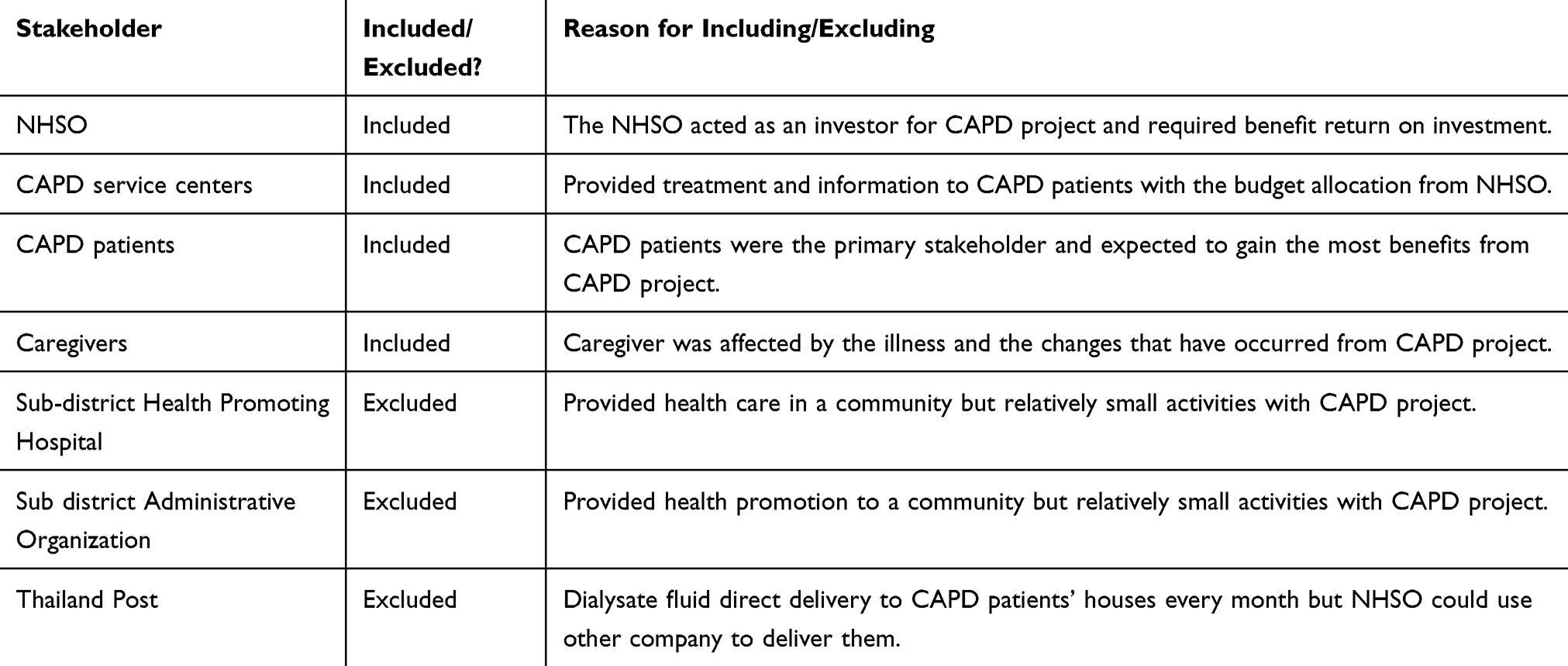 |
Table 1 Stakeholders Included And Exclude In The Stakeholder Analysis |
Stage 2: Mapping Outcomes
In this stage, the impact map was a relationship between inputs (resources used to run the activities), activities (the intervention of CAPD treatment), outputs (the tangible and intangible products from the activity), and outcomes (a result of the activity) of how CAPD project made an experience change to their life. It could ensure that the outcomes that mattered to them would get measured and valued. To construct the impact map, a representative focus group from stakeholders were brought together and interviewed with a set of open-ended questions; for example, “Can you review all of the CAPD treatment? After at least 6 months of CAPD treatment, would you describe how your life has changed, or what do you do differently now?” The data has been collected and checked for accuracy by the triangulation method. (If using the same question at different times, places, people, will the answers be the same?)18 The answer from stakeholders can be summarized into 2 themes as clinical and psychosocial output. The clinical output includes increased access to CAPD treatment rate, increasing survival rate after 12 months, decreasing complication of CAPD such as peritonitis rate, and CAPD patients or caregivers could manage home CAPD correctly. The psychosocial output was a reduction in isolation and loneliness, an increase in wellbeing from having a sense of purpose of survival, being part of the community and a reduction in stress and burden of care for caregivers. (see Table 2) Then the content analysis and theory of change17 have been applied to illustrated an impact map and experience change as a result of CAPD project as “If ESRD patients were treated with good quality and standard CAPD treatment then they would have a good quality of life, not being the burden of society and ready for KT in the future.”
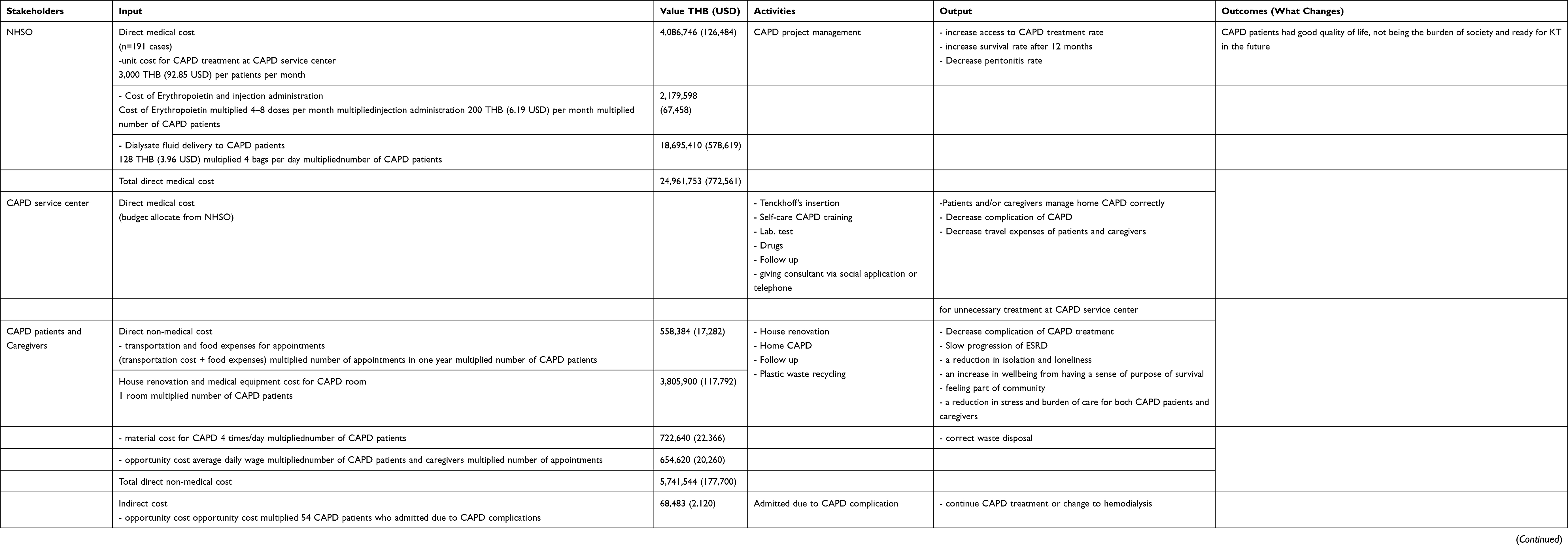 |
Table 2 Impact Map And The Investment Of CAPD Project In The Fiscal Year 2016 |
Stage 3: Evidencing Outcomes And Giving Them A Value
According to the 2nd stage, CAPD project created outcomes as “CAPD patients had a good quality of life, not being the burden of society and ready for KT in the future” have not had a market price to value them. 20 CAPD patients and caregivers were asked to describe them into an outcome indicator that was monetized by financial proxies. The outcome indicator of the good quality of life and not being the burden of society was an increase household income because after being treated by CAPD modality 2–3 months, CAPD patients felt stronger and were able to take care of themselves. Then they could be working, or their caregivers could be going back to work. The other outcome indicator of the readiness for KT in the future was saving health expenditure in the public sector because CAPD patients were hopeful that they would be donated a kidney for KT. So, everyone was trying to take care of their health. No complications caused by dialysis. Thus, it saved government expenditure for palliative treatment, as well as reduce the cost of treating complications. Although the large sample size was not required for qualitative data collection, translation of the qualitative to quantitative data implied that larger sample sizes would have increased the validity of the outcomes for each stakeholder group. Hence, the authors constructed the questionnaires to collect the outcome from the informants and monetized them (see Table 3).
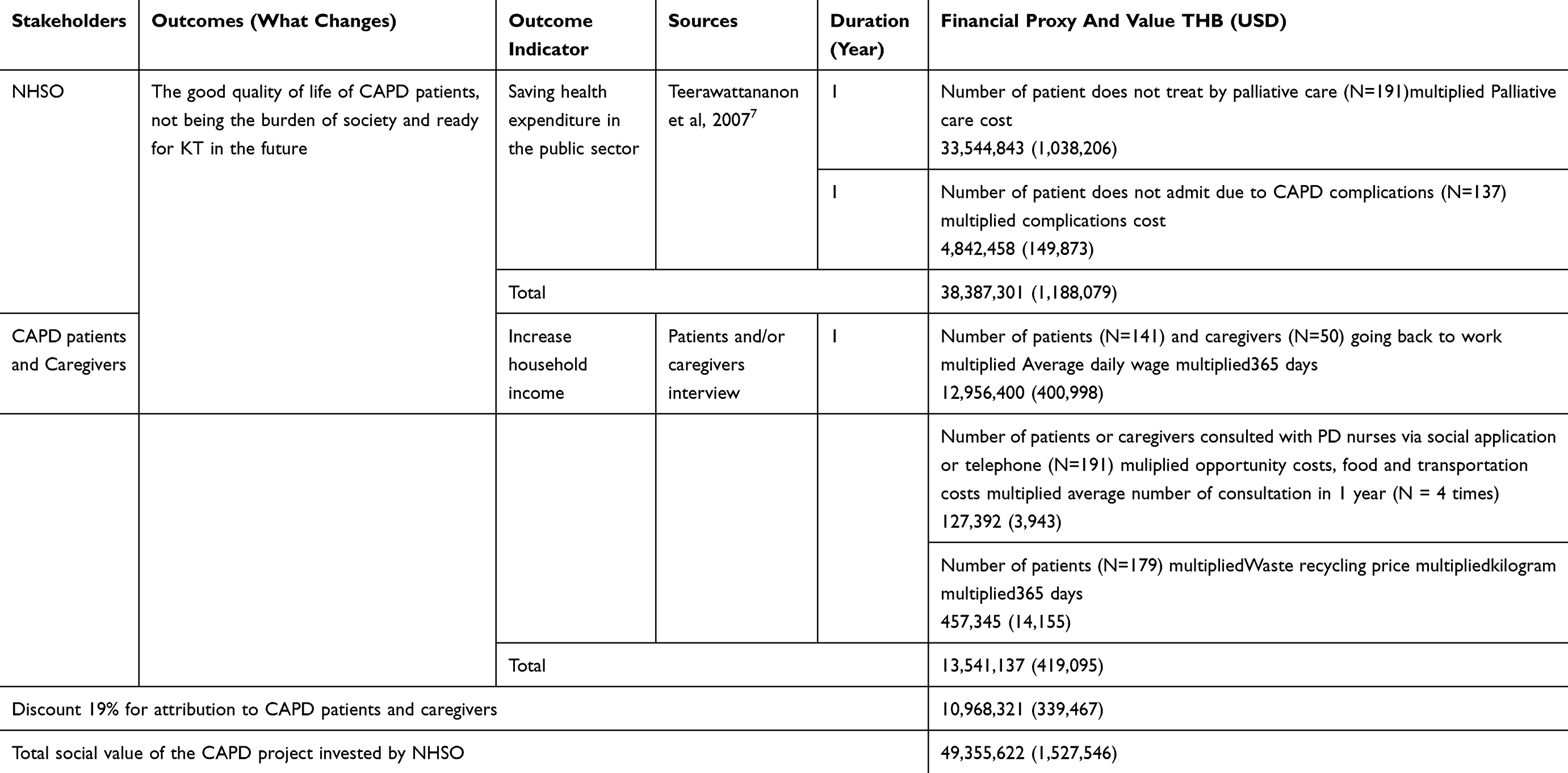 |
Table 3 Outcome, Outcome Indicator Financial Proxies And Social Value |
Stage 4: Establishing Impact
To minimize the risk of over claiming any benefits created by CAPD project, the concepts of deadweight (the amount of outcome that would have happened even if the activity had not taken place), attribution (the amount of the outcome caused by the contribution of other organizations or people), and drop-off (how long the outcomes lasted) were considered at this stage and applied to the valuation determined in the previous step. The focus group from stakeholders were brought together again to discuss and were assigned a 0% deduction for deadweight because the outcome only happened from CAPD project, 19% deduction for attribution because 81% of total costs came from NHSO and 19% from patients and their families, and 100% deduction for drop-off after year 1.
Stage 5: Calculating The SROI
Once the total value has been calculated, and deduction has been applied. At this stage, the result of the calculated value was compared with the investment to determine the ratio. The SROI ratio was determined by dividing the value of benefits by the total investment (SROI ratio = present value/value of inputs).
There were 85.27% (N=191) of CAPD patients who meet the inclusion criteria and willing to participate in this study. 14.73% excluded by changing their treatment to HD or dead between October 2016–July 2018. The average age was 57.10 years, 56.50% (N = 108) were female, 81.20% (N = 155) were married, 44.40% (N = 84) graduated from high school. The average distance from home to CAPD center service was 42.63 kilometers, the frequency of follow-up between 3–12 times per year and there were 1–3 caregivers who also took CAPD patients to each follow-up. The data on total costs and outcomes were collected by reviewing documentation, telephone interviewing, or meeting face to face.
The total costs in societal view was 30,771,780 THB (952,380 USD). The average of total costs was 172,831 THB (5,349 USD). Direct medical costs include budget allocated from NHSO to PD center 3,000 THB per patient head per month, Erythropoietin, and dialysates direct delivery to patients’ houses was 24,961,753 THB (772,561 USD). Direct non-medical costs as opportunity costs, food and transportation costs, house renovation for CAPD room, and material costs were 5,741,544 THB (177,700 USD). Indirect costs, which is an opportunity costs for 54 CAPD patients who admitted due to exit-site infection, was 68,483 THB (2,120 USD).
The social value in monetary term for increase household income was 13,541,137 THB (419,095 USD) (average 70,896 THB or 2,194 USD/case). When given a discount for attribution of 19%, the balance was 10,968,321 THB (339,467 USD). The social value for saving health expenditure in the public sector was 38,387,301 THB (1,188,079 USD) (average 200,981 THB or 6,220 USD/case). The total of social value was 49,355,622 THB (1,527,546 USD).
The total social value of the CAPD project was calculated at 49.3 million THB, whereas the total investment in societal view was calculated at 30.7 million THB. The ratio equation, therefore, was 49.3 million THB/30.7 million THB, equating to a ratio of 1.60: 1.00; in other words, for every 1 THB (USD) invested in this CAPD project, 1.60 THB (USD) of social value is created. When the scenario by changes attribution and deadweight was compared with the discount rate between 1.75 to 3.0%, the SROI ratio changed to 1.15 to 1.49, respectively.
Stage 6: Reporting, Using, And Embedding
The results of this SROI were consulted and reviewed by the Social value Thailand that specialized in SROI analyses and also is the associate network of Social value international in the United Kingdom, in order to ensure that the study using the SROI principle and framework. The results were presented to the stakeholders and discussed the way to maximize social value.
The suggestion for NHSO included: firstly, reducing the complication of CAPD treatment by developing CAPD mobile application to increase the access for medically frail patients, the versatility of dialysates delivery, information repetition to enhance knowledge retention, and interpersonal connection for educational and emotional support. This could reduce the stress and burden of the nurses who take care of CAPD patients, their caregivers, as well as reduce the complications’ costs. Secondly, the training workshop for the family care team to increase their ability to prevent the complications, slow down the degeneration of the kidneys and reduce the unnecessary expenditure of receiving medical care of CAPD patients in their area effectively. Finally, a review of CAPD service center management, the study found that some service centers had a reduction of CAPD patients, so making budget allocation by patient headcount was not sufficient for support the activities for CAPD patients. The transfer of CAPD patients to CAPD service center nearby should be considered. The suggestions for CAPD patients and their caregivers’ focused on training them to be able to produce various types of products, (for example handbag, backpack, umbrella, and raincoat) from waste dialysate bag and catheter and distributed the products themselves or through agencies. The benefit of this activity was to increase their self-esteem, independent, and household income. It also helped reduce pollution from plastic waste, too.
Discussion
This study was a pilot project demonstrated the processes of constructing the SROI impact map and identified the issues at each stage, establishing the resources used, the activities, the outputs and the outcome under participated from stakeholders. Furthermore, this study has added to previous findings by creating the theory of change that explained how the CAPD project’s activities led to the outcomes. The clinical and psychosocial output from CAPD project’s activities as 1) an increased access to CAPD treatment rate, 2) increasing survival rate after 12 months, 3) decreasing complication of CAPD such as peritonitis rate, 4) CAPD patients or caregivers could manage home CAPD correctly, 5) a slowing progression of ESRD by reducing the occurrence of complications that cause patients to change treatment and extend survival rate for more than 10 years, 6) reduction in isolation and loneliness, 7) an increase in wellbeing from having a sense of purpose of survival, 8) being part of community and a reduction in stress and burden of care for caregivers. So, the findings output added evidence to the project outcome as CAPD patients had a good quality of life, not being the burden of society and ready for KT in the future. Thus, CAPD project provided personal and social value to CAPD patients, their caregivers, and NHSO supporting the groups, with a social value 1.60 THB (USD) for every 1 THB (USD) invested.
Although the SROI methodology can be used to monitor and indicate the way to maximize the social value, the authors found that the greatest difficulty was to find the indicators and the financial proxies to value the outcomes19–21 due to the lack of information as SROI was still a relatively new method in Thailand. It was important that in the future, funder such as NHSO should develop a database which contained information on project activities, outputs, and outcome indicators to evaluate the changes that have occurred by the project. Notably, the data on outcome indicators and the value of outcome indicators at the national level should also be systematically collected.
This study has considered commonality with CAPD project for other location. However, CAPD patients may have significant demographic, socio-economic, and giving establishing impact differences from the other.18 It varied with some attributes of the population participating, condition, and age: younger individuals may benefit more than older. For this reason, although this study suggested that SROI methodology may be useful in evaluating the social value of CAPD project, the ratio obtained was not transferrable to other populations and conditions. Further SROI evaluations of CAPD project could be built on the experience from this case study and lead by the academic researchers to tailor and validate the methodology for this purpose.
Strengths And Limitation
The strength of the SROI process was that by assigning financial values to social impacts, SROI created a common language to evaluate interventions. The SROI methodology offered the ability to measure broader and more patient-centered impacts from healthcare interventions. However, even with this methodology, some benefits were difficult to monetize and therefore may be relatively undervalued. There were two limitations of this pilot study; first, there was a relatively small proportion of informants participated in the evaluation. It was possible that these responders may have represented those with more favorable responses and attitudes to the project. This, in turn, would have overestimated the modeled number of people experiencing positive outcomes. The other limitation was that the authors use only unit cost which NHSO allocate to PD centers for direct medical costs, and it was not the total costs for ESRD treatment. If the SROI methodology was adopted to evaluate other CAPD project, consideration could be given to incorporating the evaluation more closely into the project, to enable the collection of data from the majority of informants.
Conclusion
This study aimed to evaluate the social return on investment for ESRD patients treated by CAPD modality under UCS in Ubon Ratchathani province, Thailand. The findings from this study demonstrated PD first policy under UCS as a worthwhile investment, not only for ESRD patients and their caregivers but also for the NHSO who funded the policy. It demonstrated that this policy could generate a positive social return on investment as CAPD patients had a good quality of life, not being the burden of society and willing to go under kidney transplantation in the future. It also guides how each stakeholder could increase social value higher. This study was hoped to make for policymaker and NHSO those looking for a better outcome for ESRD patients. Furthermore, the authors hoped to have shown how to apply SROI methodology with traditional health economic evaluation to provide social benefit where a monetary value of the intervention was not yet known.
Acknowledgments
This study was supported by The National Research Council of Thailand Fund. The authors gratefully acknowledged the stakeholders who participated in this study, Ms Junchay Pramukkul, project manager, National Health Security Office 10 Ubon Ratchathani and Ms Nisa Thongbor, PD Nurse for useful information and Social Value Thailand for validation results.
Author Contributions
PL gathered data and ran the analysis, based on feedback from the other authors. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
PL is a Ph.D. student of Faculty of Medicine, Mahasarakham University and instructor from Faculty of Public Health, Ubon Ratchathani Rajabhat University who received research funding from The National Research Council of Thailand. ST is an advisor and instructor from the Faculty of Medicine, Mahasarakham University. Finally, NT is co-advisor and an instructor from the Faculty of Business Administration and Management, Ubon Ratchathani Rajabhat University. The authors report no other conflicts of interest in this work.
References
1. Thawornchaisit P, De Looze F, Reid CM, et al. Health-risk factors and the prevalence of chronic kidney disease: cross-sectional findings from a national cohort of 87,143 Thai Open University students. Glob J Health Sci. 2015;7(5):59–72. doi:10.5539/gjhs.v7n5p59
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Vejakama P, Ingsathit A, Attia J, Thakkinstian A. Epidemiological study of chronic kidney disease progression: a large-scale population-based cohort study. Medicine (Baltimore). 2015;94(4):e475. doi:10.1097/MD.0000000000000475
4. Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet (London, England). 2015;385(9981):1975–1982. doi:10.1016/S0140-6736(14)61601-9
5. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease - a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
6. Prakongsai P, Palmer N, Uay-Trakul P, Tangcharoensathien V, Mills A. The implications of benefit package design: the impact on poor Thai households of excluding renal replacement therapy. J Int Dev. 2009;21(2):291–308. doi:10.1002/jid.1553
7. Tantivess S, Werayingyong P, Chuengsaman P, Teerawattananon Y. Universal coverage of renal dialysis in Thailand: promise, progress, and prospects. BMJ. 2013;346:f462. doi:10.1136/bmj.f462
8. Cheawchanwattana A, Limwattananon C, Limwattananon S, Tangcharoensathien V, Sirivong T, Pongskul C. Cost utility analysis of hemodialysis and continuous ambulatory peritoneal dialysis in patients with end stage renal disease in Thailand. J Nephrol Soc Thail. 2003;9(2):158–169.
9. Teerawattananon Y, Mugford M, Tangcharoensathien V. Economic evaluation of palliative management versus peritoneal dialysis and hemodialysis for end-stage renal disease: evidence for coverage decisions in Thailand. Value Health. 2007;10(1):61–72. doi:10.1111/j.1524-4733.2006.00145.x
10. The Nephrology Society of Thailand. Thailand renal replacement therapy year 2015. Bangkok: The Nephrology Society of Thailand; 2016. Available from: http://www.nephrothai.org/images/Final_TRT_report_2015_ฉบบแก้ไข.pdf. Accessed August 25, 2019.
11. Changsirikulchai S, Sriprach S, Thokanit NS, Janma J, Chuengsaman P, Sirivongs D. Survival analysis and associated factors in thai patients on peritoneal dialysis under the PD-first policy. Perit Dial Int. 2018;38(3):172–178. doi:10.3747/pdi.2017.00127
12. Pongskul C, Sirivongs D, Keobounma T, Chanlertrith D, Promajuk P, Limwatananon C. Survival and Technical Failure in a Large Cohort of Thai CAPD Patients. Vol. 89; 2006. http://www.medassocthai.org/journal.
13. Rattanachotphanit T, Waleekhachonloet O, Chanasopon S, Ausornsagiam W, Kanjanasilp J, Suwattanasilp A. Quality of life and utilities of end stage renal disease patients undergoing dialysis. Isan J Pharm Sci. 2018;14(4):88–98.
14. Maddocks J Measuring and reporting on social value. 2015. Available from: http://www.charitysorp.org/media/642564/cipfa-draft-discussion-paper-social-value-july-2015.pdf.
15. Eurodiaconia. Measuring social value. 2016. Available from: http://www.cmsimpact.org/wp-content/uploads/2016/01/Eurodiaconia-Measuring-Social-Value.pdf.
16. Hamelmann C, Turatto F, Then V, Dyakova M. Social Return on Investment: Accounting for Value in the Context of Implementing Health 2020 and the 2030 Agenda for Sustainable Development. Copenhagen; 2017. Available from: http://www.euro.who.int/__data/assets/pdf_file/0009/347976/20170828-h0930-SROI-report-final-web.pdf?ua=1.
17. The SROI Network Accounting for Value. A guide to social return on investment. 2012. Available from: http://www.socialvalueuk.org/app/uploads/2016/03/TheGuidetoSocialReturnonInvestment2015.pdf.
18. Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–547. doi:10.1188/14.ONF.545-547
19. Muyambi K, Gurd B, Martinez L, et al. Issues in using social return on investment as an evaluation tool. Eval J Australas. 2017;17(3):32–39. doi:10.1177/1035719X1701700305
20. Chandoevwit W, Thampanishvong K, Rojjananukulpong R. Social return on investment: health promotion programs. TDRI Q Rev. 2014;29(2):4–12.
21. Watson KJ, Whitley T. Applying Social Return on Investment (SROI) to the built environment. Build Res Inf. 2017;45(8):875–891. doi:10.1080/09613218.2016.1223486
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.