")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Social Anxiety Disorder Among Undergraduate Students of Hawassa University, College of Medicine and Health Sciences, Ethiopia
Authors Reta Y , Ayalew M, Yeneabat T , Bedaso A
Received 21 October 2019
Accepted for publication 20 February 2020
Published 26 February 2020 Volume 2020:16 Pages 571—577
DOI https://doi.org/10.2147/NDT.S235416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Yared Reta,1 Mohammed Ayalew,1 Tebikew Yeneabat,2 Asres Bedaso1
1Hawassa University, College of Medicine and Health Sciences, School of Nursing, Hawassa, SNNPR, Ethiopia; 2Debre Markos University, College of Health Sciences, Department of Midwifery, Debre Markos, Ethiopia
Correspondence: Yared Reta Email [email protected]
Introduction: Social anxiety disorder (SAD), also called social phobia, is an uncontrollable fear of social situations, which involve fear of observation or making contact with strangers. So, helping individuals with social anxiety, which is among the factors affecting mental health, can significantly influence a students’ mental health and prevent other problems.
Objective: The study aimed at assessing the magnitude of SAD and its determinants among undergraduate students of Hawassa University, College of Medicine and Health Sciences.
Methods: An institution based cross-sectional study was conducted from April 1 to May 30, 2018, in Hawassa University, College of Medicine and Health Sciences. We selected participants by a stratified random sampling method, and we collected data independently from each stratum (department) using a 17 item self-rating Social Phobia Inventory (SPIN) scale to assess SAD. We performed multiple logistic regression analysis to find factors associated with SAD.
Results: Out of 304 students, 293 completed the questionnaire, with a response rate of 96.3%. The mean age of the participants was 22.13 years with a standard deviation of ± 2.176, and 172 (58.7%) were males. The prevalence of SAD was 32.8%. Family history of mental illness (AOR=4.72, 95% CI (1.25, 17.74)), being a 3rd-year student (AOR=0.178, 95% CI (0.055, 0.57)) and being a 4th year student (AOR=0.15, 95% CI (0.049, 0.49)) were significantly associated with SAD.
Conclusion: This study showed a high prevalence of SAD among medicine and health science students of Hawassa University. Therefore, the Ethiopian Ministry of Higher Education and university officials need to draw up a plan to reduce social phobia.
Keywords: social anxiety disorder, undergraduate students, Ethiopia
Introduction
DSM-V defines Social anxiety disorder as intense fear or anxiety about one or more social situations in which the individual is exposed to scrutiny by others, for example, social interactions (eg, having a conversation, meeting new people), being observed (eg eating or drinking), and performing in front of others (eg, giving a speech).1 SAD also called Social phobia is described by an enormous, persistent, and unreasonable fear of being evaluated negatively by other persons when in social performances or social interactions such as public speaking or speaking to unfamiliar people.2,3
The circumstances where social phobia might occur include restaurants, cafeterias, dining halls, seminars, meetings, and other places where the person feels observed by others.4 The individual will experience anxiety symptoms that make it uncomfortable and shameful.5 Frequently, a variety of somatic and cognitive signs and symptoms occur because of being embarrassed or judged pessimistically by others, which is typically characterized by autonomic excitement, including symptoms like increased sweating, apnea, tremors, tachycardia, and nausea.2
Fear of speaking in public is one of the most common symptoms of social phobia; where studies found out that nearly nine out of ten people with social anxiety are frightened to speak in front of others.6 In higher educational institutions were speaking in front of others is essential academic skills and a key to participate in social activities, having a SAD will impose a significant burden on students’ academic performance and social life.7 Furthermore, severe anxiety may cause increased school dropout.8
Students with a SAD may become functionally disabled in different areas of their life, such as poorer educational achievement,9 unstable employment, absenteeism from work and decreased productivity which leads to being dependent on family, community, and country.10 Medical students with social phobia have shown low performance in clinical examinations and have reported depressive symptoms, and social phobia raises susceptibility to the frequent use of substances and results in employment difficulties in their future lives.11,12
Social phobia is one of the most prevalent anxiety disorders among adolescents and youths, and that may hinder the individual’s performance if left untreated.13,14 It is also the third most common mental disorder following depression and alcohol use disorder.6 Epidemiological studies report that the lifetime prevalence of social phobia ranges from 3 to13 percent.1 In United Kingdom (UK), a cross-sectional study revealed a 10% prevalence of social anxiety in higher education students (n=1007)15 and closer to this finding a study from India using Social Interaction Anxiety Scale (SIAS) reported 12.6% prevalence of social phobia among undergraduate medical students.16 A study with large sample size (n=4368) in Australia, 30% of first-year university students were reported to suffer from SAD,17 similarly, a study from Iraq (n=198),7 Saudi Arabia (n=283)18 and India (n=272)19 reported a prevalence of 28.3%, 29.8% and 30.5% SAD among medical students, respectively. Higher prevalence (44%) of SAD is observed in Egyptian undergraduate students (n=2919)20 and 31.2% of health science students are reported to have SAD in the University of Gondar.21
Different factors may increase the probability of having SAD; for instance, females are more dominantly affected by SAD than males,1,20–22 on the other hand, clinical samples showed males are more vulnerable to SAD.3,11 Its onset may occur as early as age 5, but it is most common in the mid-teens and uncommon above 30 years of age.23 Poor social support, a field of study and academic year were the other factors that may lead to SAD.7,9,20,21
Social phobia is associated with significant impairment in educational achievement, occupational performance, social interaction, relationships, and quality of life that leads to decrease achievement, lower-income and reduce individuals’ quality of life.9,24 Medical and health science students are often confronted with various stressors and the need to become accustomed suitably to achieve academic and professional success elucidates the importance of having good mental health.9,25 Therefore, understanding the level of SAD is crucial to reveal facts which can significantly influence a students’ mental health and prevent other related problems.
To the best of the authors’ knowledge, SAD is hardly ever recognized and managed in universities of Ethiopia. So, this study measures the level of SAD and examines the relationships of various factors with SAD among medical and health science students and the findings of this study could deliver valuable information to other researchers and results could be an asset by revealing the gap of information for university officials and policymakers.
Methods
Study Design, Area and Period
An institution-based cross-sectional study was conducted from April to May 2018, at Hawassa University, College of Medicine and Health Sciences. Hawassa University is one of the 44 universities in Ethiopia which is found 273 km from the capital city Addis Ababa. The university has around seven colleges and Hawassa University, College of Medicine and Health Sciences is one of the seven colleges which was established in 1996 in Hawassa town, and the campus has ten departments in undergraduate studies (Medicine, Public Health Officer, Anesthesia, Psychiatry nursing, Nursing, Midwifery, Medical laboratory, Radiology, Optometry, and Environmental Health).
Population
All regular undergraduate students at Hawassa University, College of Medicine and Health Sciences who are available during the study period were the source population. Regular undergraduate students selected during sampling were considered as the study population.
Sample Size
The sample size was determined using a single population proportion formula considering assumptions like the proportion (p= 27.5%) from the study conducted in Woldiya preparatory school,26 sampling error 5%, Confidence interval 95%. Since the source population is less than 10,000, we used a correction formula, adding 10% nonresponse rate, the final sample size was 304.
Sampling Technique
The study population was selected by stratified random sampling methods by assuming their department of study as a stratum and the total sample size was proportionally allocated based on the total number of students in each department. Then data was taken independently from each stratum (department) by simple random sampling techniques.
Data Collection Instrument and Procedure
We collected the data using a pretested, structured self-administered questionnaire. We used a nine-item structured questionnaire to assess socio-demographic, academic and clinical characteristics of the students, and trained data collectors and supervisors facilitated the data collection. A 17 item self-rating scale called Social Phobia Inventory (SPIN) scale in which each point is ranked with a five-degree Likert scale (0=No, 1=Low, 2=Somewhat, 3=High, 4=Very Much) was used to assess social phobia.27–29 In Nigeria, SPIN was validated with sensitivity and specificity of 82.2% and 77.6% respectively.30 SPIN also reported having high reliability and validity in different countries.27,29,31 The total score ranges from 0–64, thus an individual who scores 20 or more is considered to have a SAD.27,30
We used Oslo-3 item social support scale to assess social support. Each item was scored from one to four, yielding a total score ranging from 3 to 14. A score of 3 to 8 shows “poor support”, 9 to 11 shows “moderate support”, and 12 to 14 shows “strong support”. Different studies reported that good predictive validity for the scale regarding psychological problems32–34 and the scale was found to have acceptable validity and reliability in the African context.35
Data Processing and Analysis
After checking for completeness and consistency, the collected data was entered and analyzed using SPSS version 22. We used binary logistic regression to examine the association between the dependent variable and each independent variable. Variables that showed statistical significance during binary logistic regression analysis at p-value ≤ 0.25 were entered into multiple logistic regressions to identify an independent effect of the determinants. Adjusted odds ratios (AOR) with 95% CI, were estimated to assess the strength of associations and variables with p-value <0.05 were considered as having a significant association.
Results
Socio-Demographic, Psychosocial and Clinical Characteristics of Study Participants
A total of 304 study participants were included in this study, of which 293 students completely filled the questionnaire with a response rate of 96.3%. Of the total participants, 172 (58.7%) were males between the ages of 18 and 30 years. The mean age of the respondents was 22.13 with a SD of +2.18. Majorities 95.6% (n=280) were single, Amhara by ethnicity (48.1% (n=141)), and Ethiopian orthodox followers (63.1% (n=185)). The large proportion, 72.0% (n=211) of the students were below 4th year of study and around half of the study participants were medical students (56.7% (n=166)) (Table 1).
 |
Table 1 Frequency and Percentage Distribution of Sociodemographic, Psychosocial and Clinical Characteristics of Undergraduate Students of Hawassa University, College of Medicine and Health Sciences, Hawassa, Ethiopia, May 2018 |
According to the Oslo score substantial proportion, 24.2% (n=71) of the students reported having excellent social support, about 15% (n=44) of the students reported having poor social support. Around 8.5% (n=25) of the students reported having a previous history of mental illness, and 7.5% (n=22) had a family history of mental illness (Table 1).
Factors Associated with Social Anxiety Disorder
During multiple logistic regression, we found years of study and family history of mental illness to have a significant association with SAD. Being 3rd-year students (P=0.004, AOR=0.178, 95% CI (0.05, 0.57)) was 17.8% less likely to develop SAD compared with 5th-year students and 4th year students were 15.5% less likely to develop SAD compared with 5th-year students (P=0.001, AOR=0.155, 95% CI (0.049, 0.49)). Students who have a family history of mental illness (p<0.022, AOR=4.72, 95%, CI (1.256, 17.749)) were 4.7 times more likely to develop a SAD than who did not have a family history of mental illness (Table 2).
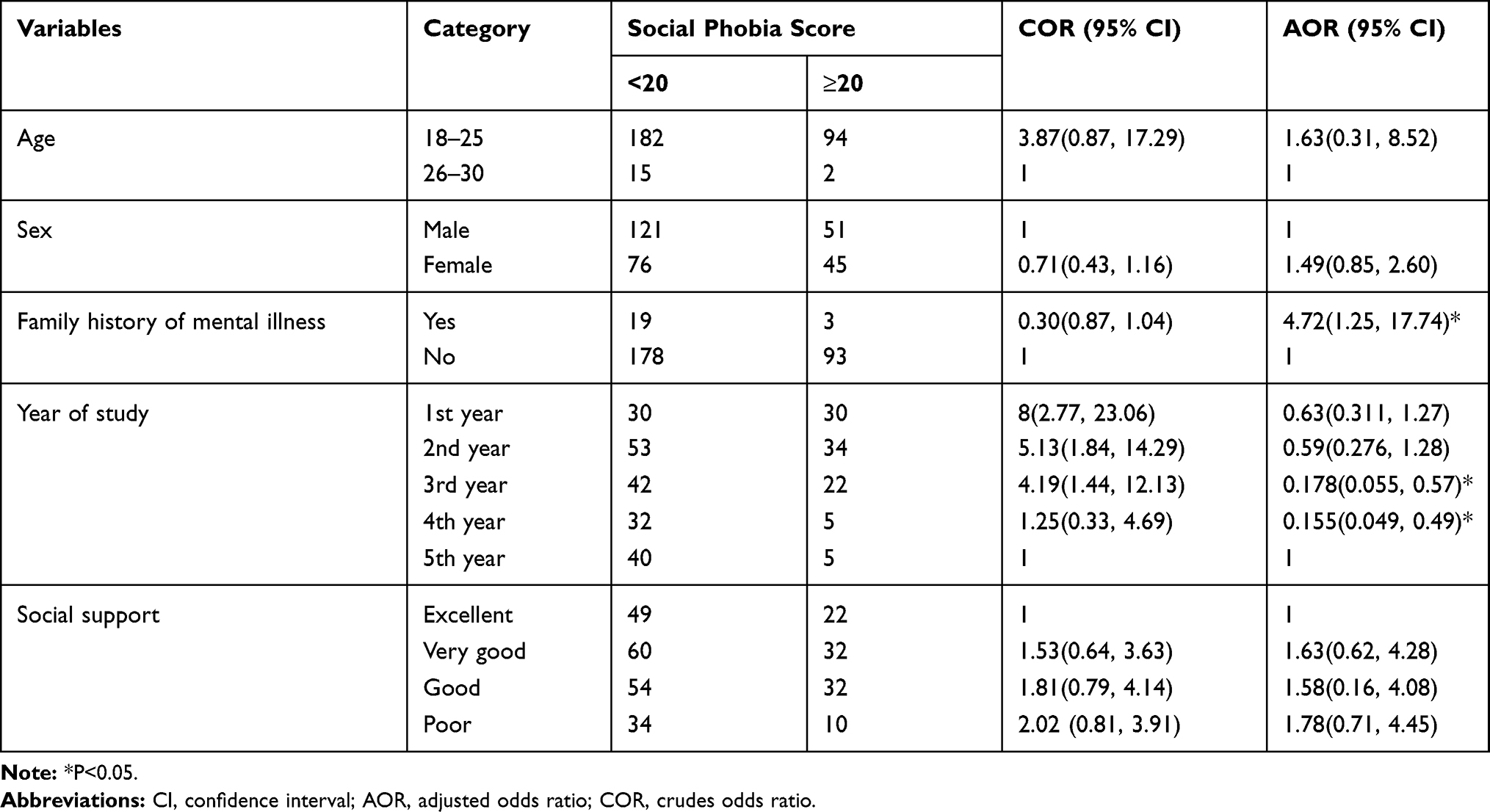 |
Table 2 Bivariate and Multivariate Logistic Regression Analysis of SAD Among Undergraduate Students of Hawassa University, College of Medicine and Health Sciences, Hawassa, Ethiopia, May 2018 |
Discussion
The overall prevalence of SAD in this study was 32.8%, and this finding is consistent with a similar study in the Ethiopian University of Gondar (31.2%),21 and it is also in line with studies from universities of Iraq (28.3%),7 Saudi Arabiya (29.8%),18 India (30.5%)19 and Australia (30.0%).17 Agreement of these studies with our result can be explained by similar study population7,17–19,21 and using similar screening tool.19,21
The prevalence of SAD in this study was higher than the study conducted in the UK (10%)15 and Delhi, India (12.6%).16 This difference might be because of socio-cultural differences between the UK and Ethiopia. For instance, in Ethiopia, shyness is a measure of politeness and has been emphasized as a dominant cultural norm.36 The other reason for this difference might be the tool used in the current study, which is a nondiagnostic self-administered tool, and this might overestimate the prevalence of SAD among students.27,37
In this study, a family history of mental illness has a significant association with social phobia. The odds of having SAD is 4.72 times more likely among students with a family history of mental illness than those students with no family history of mental illness. Genetic studies have produced substantial evidence that at least some genetic component contributes to the development of SAD, and heredity has been recognized as a predisposing factor.1,2
The year of study also has a significant association with social phobia. In this study, 3rd-year and 4th-year students are significantly predicted social phobia in which a 3rd-year student is 17.8% less likely to develop SAD compared with a 5th-year student and 4th-year students are 15.5% less likely to develop SAD as compared to 5th-year students. This result contradicts the results report by Gondar University, Iraq and Egypt,7,20,21 in which most studies support the prevalence of SAD reduces as the academic year increases. The potential explanation for this disparity could be that besides attending classes, 5th-year students are loaded with internship examinations, community training programs, and research projects which can exacerbate SAD, and we also recommend further robust studies which can come up with strong evidence for explaining this gap.
Conclusion
The overall prevalence of SAD in Hawassa University College of Medicine and Health Sciences was high (32.8%). Factors like the year of study and family history of mental illness played a significant role in the development of SAD. The Ethiopian Ministry of Higher Education and university officials, therefore, need to draw up a plan to reduce social phobia. We suggest that campus psychologists pay particular attention to improving the psychological well-being of students and that teachers may provide enhanced pedagogical support to students with SAD.
Limitations of the Study
As we used a cross-sectional study design, the analysis does not allow the correlation to be inferred. Although widely used and validated as a screening tool for social phobia in other countries, including Africa, the SPI scale is no validated in Ethiopia and SPI is a nondiagnostic self-rating screening tool, it might overestimate the prevalence of SAD.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crudes odds ratio; DSM-V, diagnostic and statistical manual version four; IRB, institutional review board; SAD, social anxiety disorder; SPIN, social phobia inventory.
Data Sharing Statement
All generated data are included in this article.
Ethics Approval and Consent to Participate
We obtained ethical clearance from the Institutional Review Board (IRB) of Hawassa University, College of Medicine and Health Sciences. Participants were fully informed about the purposes of the study before the data collection, and written consent was obtained from the study participants. Study participants were also informed that; if they did not want to answer any question, they had the right to do so. All participants were randomly selected, and we carefully handled filled out questionnaires. Anonymity was maintained to ensure the confidentiality of respondents.
Acknowledgment
We would like to thank study participants for their commitment to contribute their ideas during the data collection period.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this research work.
Disclosure
The authors declare no competing interests.
References
1. Sadock BJ, Sadock VA, Ruiz P. Synopsis of Psychiatry: Behavioral Sciences, Clinical Psychiatry. Wolters Kluwer; 2015.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub; 2013.
3. Carvalho AF, McIntyre RS. Mental Disorders in Primary Care: A Guide to Their Evaluation and Management. Oxford University Press; 2017.
4. Harrison P, Fazel M. Shorter Oxford Textbook of Psychiatry. Oxford university press; 2017.
5. Bögels SM, Alden L, Beidel DC, et al. Social anxiety disorder: questions and answers for the DSM‐V. Depress Anxiety. 2010;27(2):168–189. doi:10.1002/da.v27:2
6. de Menezes GB, Coutinho ESF, Fontenelle LF, Vigne P, Figueira I, Versiani M. Second-generation antidepressants in social anxiety disorder: meta-analysis of controlled clinical trials. Psychopharmacology. 2011;215(1):1–11. doi:10.1007/s00213-010-2113-3
7. Ahmad RJ. Prevalence of social anxiety in students of college of education – University of Garmian. Int J Arts Technol. 2017;8(3):79–83.
8. Amies PL, Gilder MG, Shaw PM. Social phobia: A comparative clinical study. Br J Psychiatry. 1983;142:174–179. doi:10.1192/bjp.142.2.174
9. Liu X, Ping S, Gao W. Changes in undergraduate students’ psychological well-being as they experience university life. Int J Environ Res Public Health. 2019;16(16):2864. doi:10.3390/ijerph16162864
10. Bruce TJ, Saeed SA. Social anxiety disorder: a common, underrecognized mental disorder. Am Fam Physician. 1999;60(8):2311.
11. Alqarni AA, Zalaa MA, El-Hadad AA, et al. Prevalence of social phobia among Saudi Medical Students. Med J Cairo Univ. 2017;85(2):657–661.
12. Levpuscek MP, Berce J. Social anxiety, social acceptance and academic self-perceptions in high-school students. Drus Istraz. 2012;21(2):405.
13. Abdallah ES, Elzeiny HH, Abdel-hady RF, El-sheikh MS. Association between social phobia and parenting styles among secondary school students. Am J Nurs Sci. 2016;5(3):96–105. doi:10.11648/j.ajns.20160503.14
14. Mustafa R, Hamdan-Mansour A, Hijazeen J, et al. Social phobia among university students in Jordan. Life Sci J. 2014;11:93–98.
15. Russell G, Shaw S. A study to investigate the prevalence of social anxiety in a sample of higher education students in the United Kingdom. J Ment Health. 2009;18(3):198–206. doi:10.1080/09638230802522494
16. Preeti PD. Prevalence of social anxiety disorder and its determinants among undergraduate medical students of East Delhi. Int J Community Med Public Health. 2019;6(3):1335. doi:10.18203/2394-6040.ijcmph20190636
17. Wilson IG. Screening for social anxiety disorder in first year university students: a pilot study. Aust Fam Physician. 2005;34(11):983–984.
18. Jarallah H, Al-Omari F, Altowairiqi I, Al Saadi K. Magnitude of social anxiety disorder, and impact on quality of life among medical students. J Psychol Clin Psychiatry. 2017;7:5.
19. Dsouza MJ, Arun Daniel J, Muhammed Muntazeem G. Social anxiety disorder among medical students in a tertiary care hospital in Davangere, Karnataka. Int J Community Med Public Health. 2019;6(4):1434. doi:10.18203/2394-6040.ijcmph20191048
20. Rabie MA, Shorab E, ElGabry D, et al. Screening of social phobia symptoms in a sample of Egyptian university students. Arch Clin Psychiatry. 2019;46(2):27–32. doi:10.1590/0101-60830000000188
21. Desalegn GT, Getinet W, Tadie G. The prevalence and correlates of social phobia among undergraduate health science students in Gondar, Gondar Ethiopia. BMC Res Notes. 2019;12(1):438. doi:10.1186/s13104-019-4482-y
22. Gao W, Ping S, Liu X. Gender differences in depression, anxiety, and stress among college students: a longitudinal study from China. J Affect Disord. 2020;263:292–300. doi:10.1016/j.jad.2019.11.121
23. Pine D, Rothbaum BO, Ressler K. Anxiety Disorders: Translational Perspectives on Diagnosis and Treatment. Primer on; 2015.
24. Gallagher M, Prinstein MJ, Simon V, Spirito A. Social anxiety symptoms and suicidal ideation in a clinical sample of early adolescents: examining loneliness and social support as longitudinal mediators. J Abnorm Child Psychol. 2014;42(6):871–883. doi:10.1007/s10802-013-9844-7
25. Zare N, Daneshpajooh F, Amini M, Razeghi M, Fallahzadeh MH. The relationship between self-esteem, general health and academic achievement in students of Shiraz University of Medical Sciences. Iran J Med Educ. 2007;7(1):59–67.
26. Mekuria K, Mulat H, Derajew H, et al. High magnitude of social anxiety disorder in school adolescents. Psychiatry J. 2017;2017.
27. Connor KM, JR D, Churchill LE, Sherwood A, Foa E, Weisler RH. Psychometric properties of the social phobia inventory(SPIN). New self-rating scale. Br J Psychiatry. 2000;176:379–386. doi:10.1192/bjp.176.4.379
28. Taherifar Z, Fata L, Gharaie B. The pattern of social phobia prediction in students based on cognitive behavioral factors. Iran J Psychiatry Clin Psychol. 2010;16(2):34–45.
29. Caballo VE, Salazar IC, Irurtia MJ, Arias B, Hofmann SG. Measuring social anxiety in 11 countries. Eur J Psychol Assess. 2010;26:95–107. doi:10.1027/1015-5759/a000014
30. Chukwujekwu D, Olose E. Validation of the social phobia inventory (Spin) in Nigeria. J Psychiatry and Psychiat Disord. 2018;2:49–54. doi:10.26502/jppd.2572-519X0040
31. Ranjbaran R, Reyshahri AP, Pourseifi MS, Javidi N. The pattern to predict social phobia based on social self-efficacy, shyness and coping style in the secondary school students. Int J Med Res Health Sci. 2016;5(9):275–281.
32. Dalgard OS, Dowrick C, Lehtinen V, et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–451. doi:10.1007/s00127-006-0051-5
33. Dalgard O. Community health profile as tool for psychiatric prevention. Promot Ment Health. 1996;5:681–695.
34. Meltzer H. Development of a common instrument for mental health. In: Nosikov A, Gudex C, editors. EUROHIS: Developing Common Instruments for Health Surveys. Vol. 57. 2003:35.
35. Abiola T, Udofia O, Zakari M. Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malaysian J Psychiatry. 2013;22(2):32–41.
36. Messing SD, Prince JS. Health practices in Ethiopian pre-urban communities. J Health Hum Behav. 1966;7:272–276. doi:10.2307/2948774
37. Antony MM, Roth D, Swinson RP, Huta V, Devins GM. Illness intrusiveness in individuals with panic disorder, obsessive-compulsive disorder, or social phobia. J Nerv Ment Dis. 1998;186(5):311–315. doi:10.1097/00005053-199805000-00008
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.