")
Back to Journals » Infection and Drug Resistance » Volume 16
Smoking is a Factor in Discordance Between QuantiFERONTB Gold Assay and Tuberculosis Etiology: Especially in Older Patients
Authors Liu L , Wu G, Wang J , Peng L , Xu X, Cai L
Received 27 March 2023
Accepted for publication 25 May 2023
Published 1 June 2023 Volume 2023:16 Pages 3443—3451
DOI https://doi.org/10.2147/IDR.S412473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Libin Liu,1,2,* Guihua Wu,1,2 Jing Wang,1,2 Lijun Peng,1,2 Xiaoqun Xu,1,2 Long Cai1,2,*
1Centre of Laboratory Medicine, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Centre of Laboratory Medicine, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Long Cai, Centre of Laboratory Medicine, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, No. 208 East Huancheng Road, Hangzhou, 310003, People’s Republic of China, Email [email protected]
Purpose: Exploring whether smoking is an influencing factor for the inconsistency between QuantiFERONTB Gold assay (QFT-GIT) and tuberculosis etiology.
Patients and Methods: The clinical data of patients who were confirmed positive for Mycobacterium tuberculosis (MTB) after undergoing QFT-GIT testing from September 2017 to August 2021 were retrospectively analyzed. Chi-square and rank-sum tests were used to compare the differences in characteristics between smokers and non-smokers. Logistic regression was used to adjust for confounding factors affecting smoking. Propensity score matching (PSM) was used to verify the above conclusions again.
Results: Positive results of tuberculosis etiology were adopted as the standard, the incidence of inconsistent results between QFT-GIT and tuberculosis etiology was 8.90% (108/1213), of which the false negative rate was 6.27% (76/1213) and the indeterminate rate was 2.64% (32/1213). In the overall population, the smokers had a lower level of basal IFN-γ (Z=− 2.079, P=0.038). Among 382 elderly (≥ 65 years old) patients, the smokers had lower levels of antigen-stimulated IFN-γ (Z=− 2.838, P=0.005). After performing BOX-COX transformation on all non-normally distributed data, logistic stepwise regression was used to adjust confounding factors. The results showed that smoking was an influencing factor for the inconsistency between QFT-GIT and tuberculosis etiology results (OR=1.69, P=0.020). Using PSM for 1:2 matching, the results showed that smoking was still an independent risk factor for the inconsistent results of QFT-GIT and tuberculosis etiology (OR= 1.95, P=0.019). Age-stratified analysis showed that smoking was an independent risk factor in discordance between QFT-GIT and tuberculosis etiology in patients aged ≥ 65 years (OR=2.40, P=0.005), but not in patients aged < 65 years (P > 0.05).
Conclusion: Smoking can reduce the body’s IFN-γ release ability, and smoking (especially the elderly) is an influencing factor for the inconsistency between QFT-GIT and tuberculosis etiological results.
Keywords: tuberculosis etiology, PSM, inconsistency, influencing factors
Introduction
Tuberculosis is an infectious disease caused by MTB infection, which seriously endangers human life and health. According to the World Health Organization (WHO) 2022 global tuberculosis report, the number of global tuberculosis cases in 2021 will be 10.6 million.1 QuantiFERON-TB Gold In-tube (QFT-GIT) is an Interferon-Gamma Release Assay (IGRAs), this method is not affected by BCG and non-tuberculous mycobacteria (NTM). IGRAs are used as a diagnostic tool for the detection of MTB infection, it has played a major role in the early rapid screening of tuberculosis.2–4 However, in clinical practice, an average of 20% of active TB patients have false negative or indeterminate QFT-GIT results due to the interference of certain factors.4 Inconsistent results between QFT-GIT and etiological diagnosis may cause a certain degree of missed or delayed diagnosis, and promote the spread of the disease (smear-positive pulmonary tuberculosis) to close contacts.5,6 There are many factors affecting the results of QFT-GIT, the most commonly studied risk factor was advanced age, followed by low peripheral lymphocyte counts, and other factors have been proposed such as smoking.7
According to the 2019 World Health Organization (WHO) report on the global tobacco epidemic, there are about 1.337 billion tobacco users among people aged ≥15 years in the world.8 Smoking is one of the main lifestyle factors that affect human health. It is not only related to the occurrence and development of various diseases but also affects the changes of many detection indicators in the human body.9 Smoking has been reported to be an independent factor in the progression of latent tuberculosis infection to active tuberculosis and tuberculosis death.10 Exposure to tobacco smoke can reduce cellular IFN-γ production in epithelial cells after antigenic challenge and impairs IFN-γ-mediated signaling and vaccine efficacy.11,12 These findings all suggest that smoking negatively affects immune defenses, and smoking could theoretically affect the performance of immunodiagnostic tests such as (IGRAs). Martine G Aabye’s research shows, cigarette smoking was associated with false negative and indeterminate IGRA results.13 Because the sample size and predictive factors included in their study are small, the research is not enough to determine the impact of smoking on QFT-GIT results, the effect of smoking on the results of QFT-GIT needs to be confirmed by further studies.
This study aims to evaluate the effect of smoking on IFN-γ responsiveness and investigate whether smoking is an influencing factor for the inconsistency between QFT-GIT and tuberculosis etiological results, to provide a reference for clinicians.
Materials and Methods
We retrospectively analyzed the clinical data of patients who were confirmed positive for MTB by solid and liquid culture after undergoing QFT-GIT tests hospitalized at the Hangzhou Chest Hospital Affiliated to Zhejiang University School of Medicine from September 2017 to August 2021. All positive samples from patients were identified by p-nitrobenzoic acid (PNB) drug susceptibility test or biochip assay. The basic characteristics and various clinical information of the patients were collected from the electronic medical record database: including age, gender, smoking, drinking, underlying diseases, hypoalbuminemia, chronic liver disease, chronic kidney disease, immune disease, tumor, diabetes, chronic lung disease, hypertension, cardiovascular disease, serum total protein, albumin, globulin, c-reactive protein, white blood cells, lymphocyte count, lymphocyte percentage and hemoglobin. Chronic kidney disease is defined as a disease that causes a gradual loss of kidney function. Cardiovascular disease is defined as conditions that require long-term use of cardiac medications, such as coronary artery disease, valvular disease, cardiomyopathy, and cardiac arrhythmias. Chronic liver disease is defined as a disease that results in progressive destruction and regeneration of the liver parenchyma, such as chronic viral hepatitis, alcoholic liver disease, and hepatic insufficiency.
This study is a retrospective study, because the patients could not be found when the data was collected, and personal privacy and commercial interests were not involved. An exemption from the informed consent requirement was approved by the ethics committee of Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine (Ethical Application Ref:2023YS034). This study protocol strictly complied with the requirements of the Helsinki Declaration of the World Medical Association. Members of our research project teams are committed to maintaining the confidentiality of all patient information collected in electronic medical record databases.
Patient Selection
Inclusion criteria: (1) inpatients have detailed hospitalization information and various clinical test indicators; (2) all patients have undergone QFT-GIT; (3) MTB has been confirmed positive. Exclusion criteria: (1) positive mycobacterial culture, identified as NTM by drug sensitivity test or biochip assay; (2) cases aged <15 years; (3) QFT-GIT test was performed after anti-tuberculosis treatment > 1 week; (4) lack of smoking history. Smokers were defined as current smokers. Study outcome grouping: positive results of QFT-GIT were the consistent group, and false negative and indeterminate results were the inconsistent group.
QFT-GIT
Specimen Collection and Processing
4–6 mL of peripheral venous whole blood was collected from the patient, placed in a lithium heparin anticoagulant tube, and sent to the laboratory for testing within 4 hours. After inverting and mixing 10 times, samples were taken and placed in mitogen-positive control (Mitogen) tubes, tuberculosis antigen (TBAg) tubes, and blank control (Nil) tubes, and 1 mL was added to each tube. Then immediately shake up and down 10 times to ensure that the whole inner layer of the test tube was covered with blood to dissolve the antigen on the tube wall. It was placed upright in an incubator at 37°C for 16–24 hours, and centrifuged at 2000 × g/min for 15 min.
Calculation and Judgment of QFT-GIT Results
QFT-GIT kit was used, and the experimental process was operated strictly according to the instructions. The detection value of the microplate reader was calculated by QFT analysis software (DS2QFT 4pt v6.25 version) provided by QIAGEN, Germany, and the results were interpreted see the standard (Table S1).
MTB Culture
Lowenstein–Jensen solid medium and liquid culture medium (BACTEC MGIT 960 Mycobacteria Culture System, BD Diagnostic Systems, Sparks, MD) were used for MTB culture according to the manufacturer’s instructions at 37°C for 2–6 weeks.
Biochip Assay
Biochip assay can qualitatively identify MTB and NTM by targeting the differences in the 16S rRNA (CapitalBio, Beijing, China). The method can quickly distinguish 17 kinds of mycobacteria such as MTB, Mycobacterium intracellulare, Mycobacterium avium, Mycobacterium chelonae/Mycobacterium abscessus, and Mycobacterium kansasii. All experiments were performed according to the manufacturer’s instructions. Fluorescence intensity is measured by dedicated software called Mycobacteria Identification Array Test System.14
Statistical Analysis
For measurement data with skewed distribution, the median (M) and upper and lower quartiles (Q1, Q3) are used to describe the central tendency and dispersion of the data, and the Mann–Whitney U-test or Kruskal Wallis test is used for comparison between groups. Enumeration data were described by the number of cases (n) and constituent ratio (%), and the chi-square test or Fisher’s exact probability test was used. Since the measurement data do not follow a normal distribution, the measurement data were normalized using the Box-Cox power transformation. With 902 non-smokers and 311 smokers, a power of 89.48% could be achieved to detect a difference in between-group proportions of 0.10. Influencing factors of inconsistent results were analyzed by multivariate Logistic stepwise regression analysis. Confounding variables were balanced using propensity score matching (PSM), 1:2 matching, and proximity matching. Analyzes were stratified according to age. R statistical software (version 4.3.0) was used for statistical analysis of the data, and all tests were performed with a two-sided P<0.05 indicating statistically significant differences.
Results
Initial screening was performed on 1572 patients. After identification by drug susceptibility test or biochip detection, 194 cases were excluded as NTM, 1378 cases were confirmed as tuberculosis patients.14 patients <15 years old, and 151 patients missing smoking status were excluded. As a result, 1213 patients were included in the study, including 311 smokers, one of whom was HIV-positive; and 902 non-smokers, two of whom were HIV-positive. All 311 smokers had QFT-GIT results, including 270 (86.82%) positive cases, 25 (8.04%) negative cases, and 16 (5.14%) indeterminate cases. All 902 non-smokers had QFT-GIT results, including 835 (92.57%) positive cases, 51 (5.65%) negative cases, and 16 (1.77%) indeterminate cases. Taking the positive results of tuberculosis etiology as the standard, the incidences of inconsistency, false negative, and indeterminate results between QFT-GIT and tuberculosis etiology in 1213 patients were 8.90% (108/1213), 6.27% (76/1213), 2.64% (32/1213) (Figure 1).
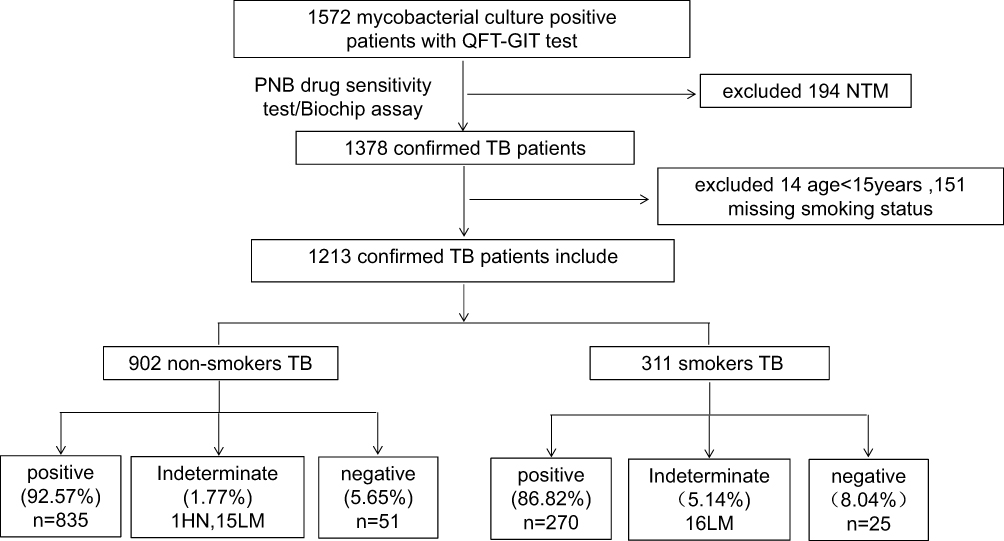 |
Figure 1 The entry rules of study population. Abbreviations: NTM, nontuberculous mycobacteria; PNB, p-nitrobenzoic acid; HN, high-nil (>8 IU/mL); LM, low mitogen (<0.5 IU/mL) response. |
Effects of Smoking on IFN-γ Levels in Different Age Groups
Among all patients, smokers had lower levels of basal IFN-γ.(Z = −2.079, P = 0.038) (Figure 2A); In the < 65 years group, baseline, antigen-stimulated, and mitogen-stimulated IFN-γ levels were not statistically different between smokers and non-smokers (all P-values > 0.05) (Figure 2B); Among patients aged ≥ 65 years, smokers had lower levels of antigen-stimulated IFN-γ (Z = −2.838, P = 0.005), but basal and mitogen-stimulated IFN-γ levels were not significantly lower in smokers (all P-values > 0.05) (Figure 2C).
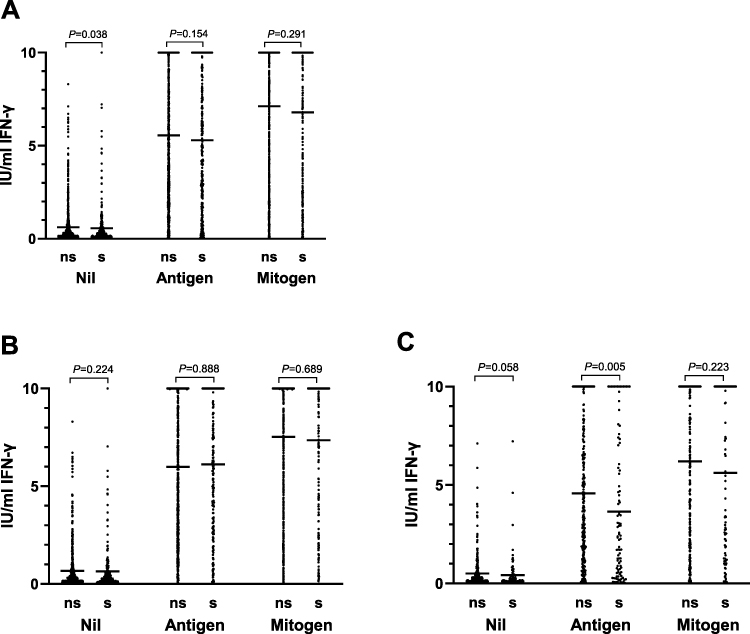 |
Figure 2 Effects of smoking on IFN-γlevels in different age groups. (A) total patients. (B) paitents’ age < 65 years. (C) patients’ age ≥ 65 years. Abbreviations: ns, non-smokers; s, smokers. Notes: Nil, levels of Interferon-γ were measured in supernatants from QuantiFERON-TB Gold In tube blood collection tubes after incubation with saline; Antigen, (M) tuberculosis-specific antigens; Mitogen, phytohaemagglutinin. |
Comparison of Background Characteristics of Smokers and Non-Smokers
A total of 1213 patients were finally included in this study, the basic characteristics, clinical characteristics, and laboratory test results of smokers and non-smokers were compared. The results showed that age, sex, alcohol consumption, diabetes, albumin, c-reactive protein, white blood cells, lymphocyte percentage, and hemoglobin were different between the two groups. The difference is statistically significant (all P-values < 0.05) (Table 1).
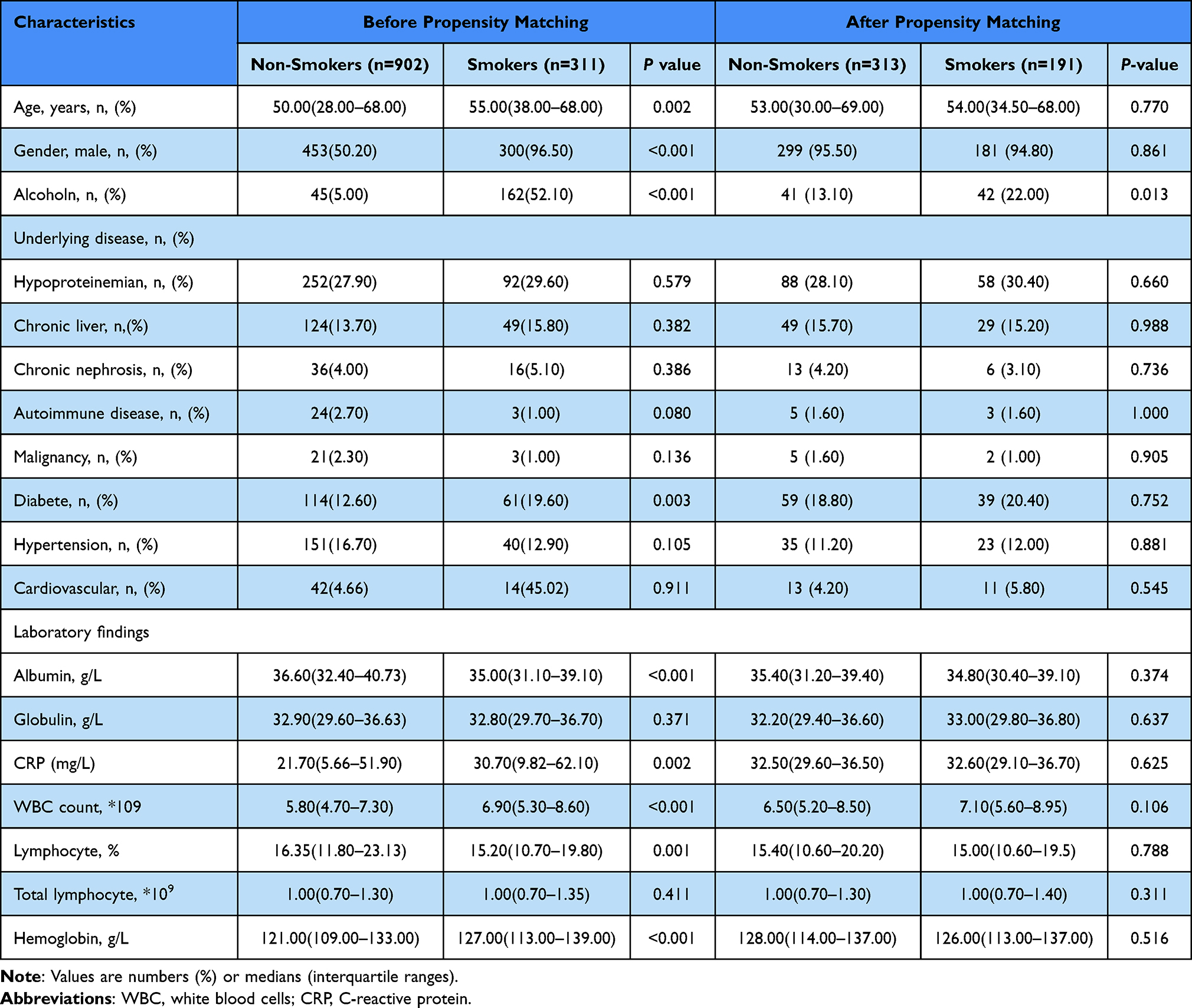 |
Table 1 Comparison of Background Characteristics of Smokers and Non-Smokers Before and After Matching |
Adjusting for Confounding Factors Affecting Smoking
Univariate analysis showed that, compared with non-smokers, the risk of discordance between QFT-GIT and tuberculosis etiology results was increased in smokers (OR=1.89, P=0.002). After performing BOX-COX transformation on all non-normally distributed data (Table S2), the logistic stepwise regression analysis results showed that adjusting for hypoalbuminemia, chronic liver disease, and variables converted by BOX-COX (lymphocyte percentage, age, globulin), smoking was still an independent risk factor leading to inconsistency between QFT detection and tuberculosis etiology (OR=1.69, P=0.020) (Table 2). Smoking was an influencing factor of QFT-GIT indeterminate results (OR=4.17, P=0.001), but not a factor of QFT-GIT false negative (OR=1.52, P=0.099) (Table S3).
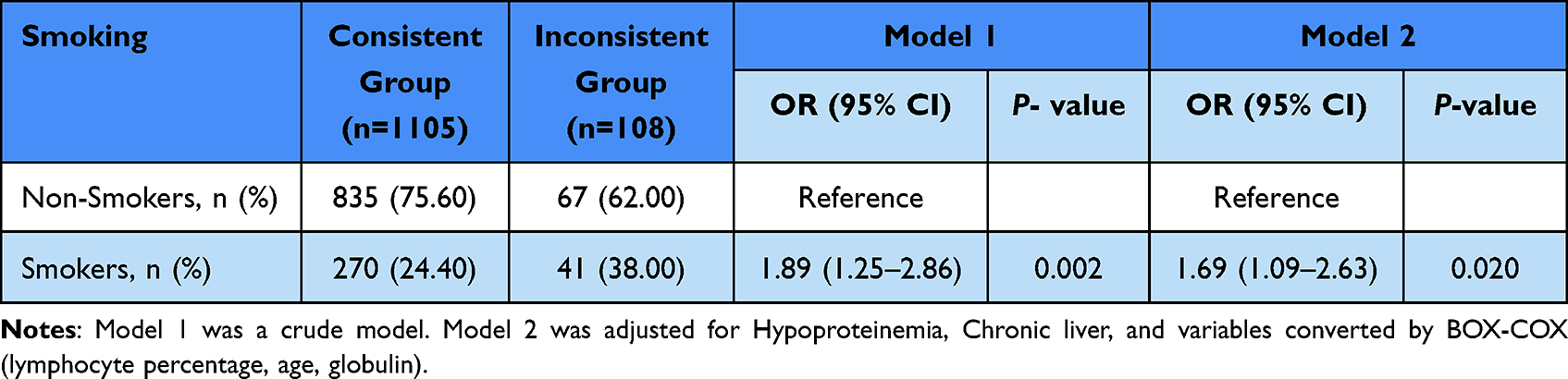 |
Table 2 Logistic Regression Analysis of the Influence of Smoking on the Inconsistency Between QFT Detection and Tuberculosis Etiology |
Propensity-Matched Analysis for Smoking Factors
A total of 1213 patients were included in the study, including 311 smokers and 902 non-smokers. We used PSM for 1:2 matching, and we matched a total of 504 patients (313 non-smokers and 191 smokers) (Table 1). Multivariate logistic regression was used to analyze the matched data, and the results showed that smoking was still an independent risk factor for the inconsistency between QFT-GIT and tuberculosis etiology (OR=1.95, P=0.019) (Table 3).
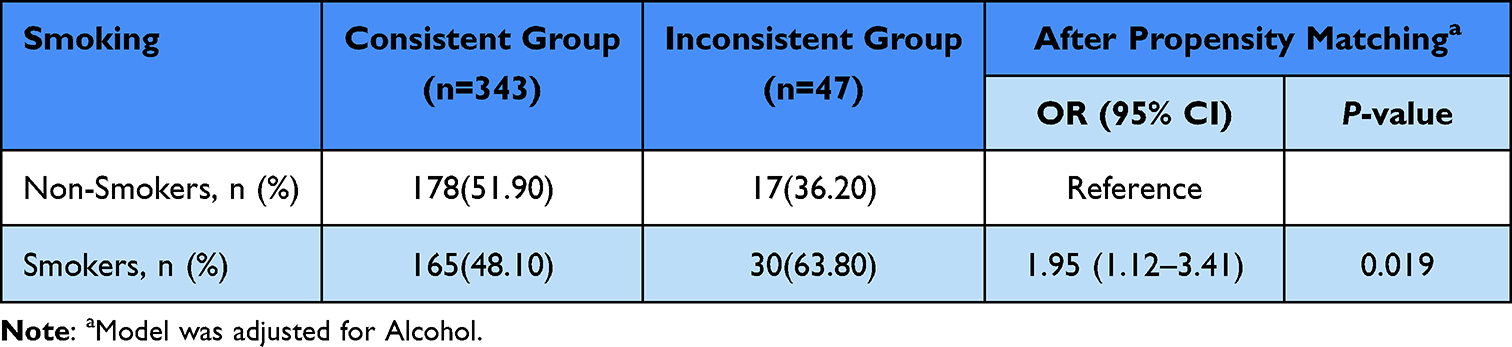 |
Table 3 Comparison of Smoking After Propensity Matching by Logistic Regression Analysis |
Age-Stratified Analysis
Among patients aged <65 years, smoking was not an independent risk factor for discordance between QFT detection and tuberculosis etiology (P>0.05) (Table S4). Among patients aged ≥65 years, univariate analysis showed that compared with non-smokers, the risk of QFT-GIT discordance with tuberculosis etiological results was increased in smokers (OR=2.40, P=0.002). After adjusting smoking confounding factors (hypoalbuminemia, chronic liver disease, cardiovascular disease, percentage of lymphocytes after box-cox transformation), the results showed that smoking was still an independent risk factor for discordance between QFT detection and tuberculosis etiology (OR= 2.40, P=0.005) (Table 4).
 |
Table 4 Logistic Regression Analysis of the Influence of Smoking on the Inconsistency Between QFT Detection and Tuberculosis Etiology in Patients Aged ≥65 Years |
Discussion
QFT-GIT plays an important role in the early diagnosis of tuberculosis. Compared with the tuberculin skin test (TST) method, this method is easier to make an early diagnosis of tuberculosis.15 However, in the diagnosis process of tuberculosis, some QFT-GIT results are inconsistent with the results of tuberculosis etiology, which seriously interferes with the diagnosis of tuberculosis by clinicians. The discordance between QFT-GIT results and tuberculosis etiology results included false negative and indeterminate results. There are many studies on the influencing factors that lead to false negative and indeterminate results, but there are not many studies on whether smoking affects the results of QFT-GIT.
This study showed that taking the positive results of tuberculosis etiology as the standard, the incidences of inconsistent, false negative and indeterminate results between QFT-GIT and tuberculosis etiology were 8.90%, 6.27% and 2.64%, which were lower than the Tanzanian group 49/172 (28.49%), 12.79% (22/172), and 15.70% (27/172) reported by Martine G Aabye.13 The reason may be related to the population included in the study. Only 0.25% (3 cases) of the patients in our study were HIV patients, while 43.6% were HIV patients in the Martine G Aabye study. Numerous studies have shown that HIV infection is associated with QFT-GIT false negatives.16–18 Taking this group of people as the research object will lead to a significant increase in the incidence of inconsistencies.
Numerous studies have shown that long-term exposure to tobacco smoke can damage the immune defense function of the host and reduce the level of IFN-γ secreted by T lymphocytes.4,5,19 This study showed that among all the studied patients, the smokers had lower baseline levels, but the smokers did not have lower IFN-γ levels after antigen stimulation or mitogen stimulation. It is considered that there are two main reasons. On the one hand, the young age group (<65 years old) accounted for 68.51% (831/1213) of the total population in this study. Since the exposure time of the young age group to tobacco is relatively short, the white blood cells in the young age group will increase their reactivity after being stimulated by tobacco smoke. Even if the function of T lymphocytes is damaged, the body can compensate to varying degrees.20 On the other hand, since the mitogen response often exceeds the upper limit of the QFT assay, the test cannot quantify the IFN-γ response exceeding the upper limit, so the difference in the level of the FN-γ response after mitogen stimulation is not easily visualized. Subsequently, this study explored the effect of smoking on IFN-γ response levels in different age groups. The study showed that after antigen stimulation, the IFN-γ response level of the older (≥65 years old) smoking group was lower, but the younger smoking group (<65 years old)) is not lowered. The reason may be that, on the one hand, with the increase of age, compared with the younger age group, the cellular immune response of the older age group to the Mycobacterium tuberculosis-specific antigen weakens, the level of IFN-γ production in the cells stimulated by the antigen decreases. On the other hand, the older age group has a relatively longer exposure time, and the amount of exposure can also influence on the results, Unfortunately, we cannot collect this information accurately. Our conclusions are consistent with previous studies.18,21
The above studies have shown that the level of IFN-γ produced by smokers in the study population is lower than that of non-smokers. We speculate that smoking may affect the results of QFT-GIT which uses IFN-γ as the detection target. To verify the above speculation, we first conducted a univariate regression analysis on smoking factors, and the results showed that compared with non-smokers, the risk of inconsistency between QFT-GIT and tuberculosis etiology in the smoking population increased, and the difference was statistically significant (OR= 1.89, P=0.002). Subsequently, we adjusted hypoalbuminemia, chronic liver disease, and variables converted by BOX-COX (lymphocyte percentage, age, globulin) using stepwise logistic regression. The results showed that smoking was still an influencing factor for the inconsistency between QFT-GIT and tuberculosis etiology results (OR=1.69, P=0.020). There are two forms of discordance between QFT-GIT and tuberculosis etiology, including false negatives and indeterminate. In this study, multiple regression was used to analyze the two situations. The study found that smoking mainly promoted the occurrence of QFT-GIT indeterminate results, and smoking was not an influencing factor for QFT-GIT false negatives. This is different from reports such as Martine G Aabye,13 whose research shows that smoking is closely related to false negative and indeterminate. Further studies are needed to explore whether the effect of smoking on QFT-GIT is mainly focused on false negatives or indeterminate.
This study is a retrospective observational study. Due to various reasons, there are many data deviations and confounding variables in the study. If the data are not adjusted, it is easy to get wrong conclusions. To further verify the above research conclusions, we then carried out a propensity score matching analysis on smoking factors. Propensity score matching can reduce the interference of confounding variables on research, so that a more reasonable comparison between the experimental group and the control group can be made.22 Due to the large difference in case data between the two groups (311 cases for smokers and 902 cases for non-smokers), in order to obtain better matching while minimizing data loss, we chose 1:2 matching. The results showed that, except for the drinking variable, other variables were well matched, then we adjusted the drinking variable. The study showed that smoking was still a risk factor for the occurrence of inconsistency between QFT-GIT and tuberculosis etiology.
It is worth noting that a meta-analysis in 2020 showed that advanced age is a common risk factor affecting the results of QFT-GIT.12 Our previous research found that there are differences in IFN-γ release levels among smoking groups of different age groups. We speculated that the effect of smoking on QFT-GIT may be closely related to age, and then we did an age-stratified study. The results of the study confirmed our conjecture that smokers of advanced age (≥65 years old) were more likely to have inconsistencies between QFT-GIT and tuberculosis etiology results.
There are still some limitations in this study. First, different studies have different conclusions due to different inclusion factors and population characteristics. Since the diseases included in this study are not classified in a refined manner, especially the definition of chronic diseases is vague, which makes it difficult to accurately analyze the influencing factors. Second, the population included in this study was current smokers, the study could not conduct an accurate analysis of tobacco exposure time and daily smoking frequency, and these factors may also have an important impact on the results. Third, the population included in this study lacks HIV cases, immune diseases, and treatment information, so it is impossible to know whether these factors affect the production of IFN-γ. Finally, the level of IFN-γ induced by antigen and the mitogen frequently overshot the upper limit of the QFT assay making quantification of responses in the high range impossible, missing information can obscure differences and may affect conclusions.
Conclusion
Overall, smoking can reduce the body’s IFN-γ release ability, especially in the elderly group. Smoking is an influencing factor leading to the inconsistency between QFT-GIT and tuberculosis etiology results, which is mainly reflected in the increased incidence of indeterminate results. For smoking patients, it is recommended to improve clinical examinations such as imaging, smear, mycobacterial culture, and various tuberculosis molecular tests. For patients with little or no sputum, bronchoalveolar lavage fluid examination can be performed, to improve the diagnosis of tuberculosis.
Acknowledgments
We would like to express our gratitude to the patients and their families.
Funding
This study was supported by the Hangzhou Medical and Health Science and Technology Project (A20210187, A20220174), Hangzhou Biomedicine and Health Industry Support Science and Technology Project (2021WJCY321), Major project of Hangzhou Medical and Health Science and Technology Plan (Z20220032), Health Commission of Zhejiang Province (2023KY969).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2021. World Health Organization; 2022.
2. Mazurek GH, Jereb J, Vernon A, et al. Updated guidelines for using interferon gamma release assays to detect MTB infection - United States, 2010. MMWR Recomm Rep. 2010;59(RR–5):1–25.
3. Diel R, Goletti D, Ferrara G, et al. Interferon-γ release assays for the diagnosis of latent MTB infection: a systematic review and meta-analysis. Eur Respir J. 2011;37(1):88–99. doi:10.1183/09031936.00115110
4. Sester M, Sotgiu G, Lange C, et al. Interferon-γ release assays for the diagnosis of active tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2011;37(1):100–111. doi:10.1183/09031936.00114810
5. Getnet F, Demissie M, Assefa N, et al. Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and meta-analysis. BMC Pulm Med. 2017;17(1):202. doi:10.1186/s12890-017-0551-y
6. Cheng S, Chen W, Yang Y, et al. Effect of diagnostic and treatment delay on the risk of tuberculosis transmission in Shenzhen, China: an observational cohort study, 1993–2010. PLoS One. 2013;8(6):e67516. doi:10.1371/journal.pone.0067516
7. Yamasue M, Komiya K, Usagawa Y, et al. Factors associated with false negative interferon-γ release assay results in patients with tuberculosis: a systematic review with meta-analysis. Sci Rep. 2020;10(1):1607. doi:10.1038/s41598-020-58459-9
8. World Health Organization report on the global tobacco epidemic 2019: offer help to quit tobacco use[EB/OL]; 2019. Available from: https://www.who.int/publications/i/item/9789241516204.
9. Yanbaeva DG, Dentener MA, Creutzberg EC, et al. Systemic effects of smoking. Chest. 2007;131(5):1557–1566. doi:10.1378/chest.06-2179
10. Slama K, Chiang C, Enarson DA, et al. Tobacco and tuberculosis: a qualitative systematic review and meta-analysis. Int J Tuberc Lung Dis. 2007;11(10):1049–1061.
11. Feng Y, Kong Y, Barnes PF, et al. Exposure to cigarette smoke inhibits the pulmonary T-cell response to influenza virus and Mycobacterium tuberculosis. Infect Immun. 2011;79(1):229–237. doi:10.1128/IAI.00709-10
12. Modestou MA, Manzel J, El-Mahdy S, et al. Inhibition of IFN-gamma-dependent antiviral airway epithelial defense by cigarette smoke. Respir Res. 2010;11(1):64. doi:10.1186/1465-9921-11-64
13. Aabye MG, Hermansen S, Ruhwald M, et al. Negative effect of smoking on the performance of the QuantiFERON TB gold in tube test. BMC Infect Dis. 2012;12:379. doi:10.1186/1471-2334-12-379
14. Zhu L, Jiang G, Wang S, et al. Biochip system for rapid and accurate identification of mycobacterial species from isolates and sputum. J Clin Microbiol. 2010;48:3654–3660. doi:10.1128/JCM.00158-10
15. Gao L, Lu W, Bai L, et al. Latent tuberculosis infection in rural China: baseline results of a population-based, multicentre, prospective cohort study. Lancet Infect Dis. 2015;15(3):310–319. doi:10.1016/S1473-3099(14)71085-0
16. Nguyen DT, Teeter LD, Graves J, et al. Characteristics associated with negative interferon-γ release assay results in culture-confirmed tuberculosis patients, Texas, USA, 2013–2015. Emerg Infect Dis. 2018;24:534–540.
17. Choi JC, Jarlsberg LG, Grinsdale JA, et al. Reduced sensitivity of the QuantiFERON(®) test in diabetic patients with smear-negative tuberculosis.Int. J Tuberc Lung Dis. 2015;19:582–588. doi:10.5588/ijtld.14.0553
18. Hang L, Lien T, Kobayashi N, et al. Analysis of factors lowering sensitivity of interferon-γ release assay for tuberculosis. PLoS One. 2011;6(8):e23806. doi:10.1371/journal.pone.0023806
19. Doyle I, Ratcliffe M, Walding A, et al. Differential gene expression analysis in human monocyte-derived macrophages: impact of cigarette smoke on host defence. Mol Immunol. 2010;47(5):1058–1065. doi:10.1016/j.molimm.2009.11.008
20. Holt PG, Keast D. Environmentally induced changes in immunological function: acute and chronic effects of inhalation of tobacco smoke and other atmospheric contaminants in man and experimental animals. Bacteriol Rev. 1977;41(1):205–216. doi:10.1128/br.41.1.205-216.1977
21. Kobashi Y, Mouri K, Yagi S, et al. Clinical utility of the QuantiFERON TB-2G test for elderly patients with active tuberculosis. Chest. 2008;133:1196–1202. doi:10.1378/chest.07-1995
22. Liang J, Hu Z, Zhan C, et al. Using propensity score matching to balance the baseline characteristics. J Thorac Oncol. 2021;16:e45–e46. doi:10.1016/j.jtho.2020.11.030
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.