")
Back to Journals » Journal of Asthma and Allergy » Volume 9
Smoking cessation strategies for patients with asthma: improving patient outcomes
Authors Perret J, Boneveski B , McDonald C, Abramson M
Received 18 January 2016
Accepted for publication 16 March 2016
Published 24 June 2016 Volume 2016:9 Pages 117—128
DOI https://doi.org/10.2147/JAA.S85615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Jennifer L Perret,1–3 Billie Bonevski,4 Christine F McDonald,2,3,5 Michael J Abramson6,7
1Allergy and Lung Health Unit, The University of Melbourne, Melbourne, VIC, 2Institute for Breathing & Sleep, Melbourne, VIC, 3Department of Respiratory and Sleep Medicine, Austin Hospital, Melbourne, VIC, 4School of Medicine & Public Health, University of Newcastle, NSW, 5Department of Medicine, The University of Melbourne, Melbourne, VIC, 6School of Public Health & Preventive Medicine, Monash University, Melbourne, VIC, 7Allergy, Immunology & Respiratory Medicine, The Alfred Hospital, Melbourne, VIC, Australia
Abstract: Smoking is common in adults with asthma, yet a paucity of literature exists on smoking cessation strategies specifically targeting this subgroup. Adverse respiratory effects from personal smoking include worse asthma control and a predisposition to lower lung function and chronic obstructive pulmonary disease. Some data suggest that individuals with asthma are more likely than their non-asthmatic peers to smoke regularly at an earlier age. While quit attempts can be more frequent in smokers with asthma, they are also of shorter duration than in non-asthmatics. Considering these asthma-specific characteristics is important in order to individualize smoking cessation strategies. In particular, asthma-specific information such as “lung age” should be provided and longer-term follow-up is advised. Promising emerging strategies include reminders by cellular phone and web-based interventions using consumer health informatics. For adolescents, training older peers to deliver asthma education is another promising strategy. For smokers who are hospitalized for asthma, inpatient nicotine replacement therapy and counseling are a priority. Overall, improving smoking cessation rates in smokers with asthma may rely on a more personalized approach, with the potential for substantial health benefits to individuals and the population at large.
Keywords: asthma, smoking cessation, asthma-COPD overlap syndrome, ACOS, lung function, patient outcomes
Introduction
Most smokers who consider quitting do so because of concerns about their physical health, which are most commonly related to the development of lung cancer and emphysema.1 “Smokers with asthma” are a distinct subgroup of smokers. They have the propensity to poorer asthma control and the development of asthma–chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS), which results in lung function deficits similar to COPD. Despite these potential consequences, some evidence suggests that such smokers are less likely to quit smoking than smokers without asthma (Table 1).2,3 Acknowledgment of these worse patient outcomes has given rise to an opportunity to improve current management practices.
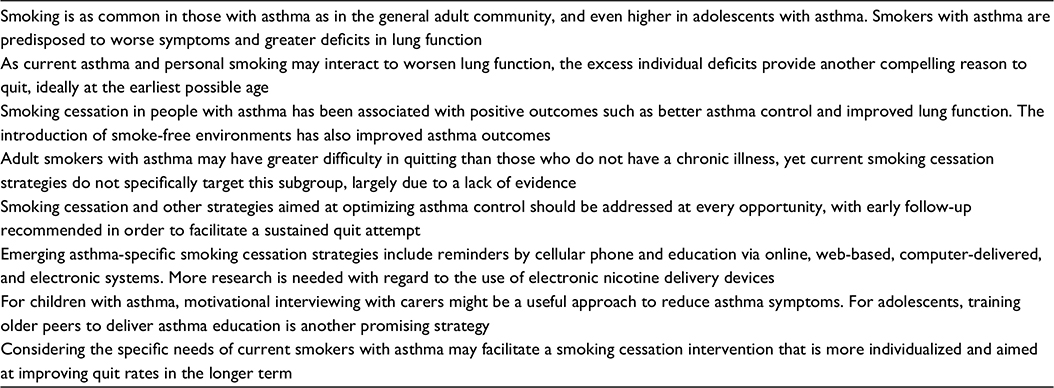 | Table 1 Key points |
We searched the full available range of articles written in English on PubMed using the search terms “asthma”, “smoking cessation”, and “patient outcomes” (search was last updated on December 2, 2015). Of the 38 articles identified, 23 were selected and 16 articles were included. Selection was based on review articles (narrative, systematic, and meta-analyses) and clinical studies addressing the lack, efficacy of, and emergent asthma-related smoking cessation strategies. References were also selected from a bibliographical search. They were excluded if primarily related to COPD and/or practice change, rather than to asthma patient outcomes (n=16).
Asthma in adult and adolescent smokers
Prevalence of smoking in people with asthma
The prevalence of smoking in people with asthma is similar to, or even higher than the general community, being ˜19% to 25% for European and Northern American countries prior to 2004.4–6 In the European Community Respiratory Health Survey, a lower prevalence of continued smoking was seen for participants who also had asthma (26.3% vs 30.1%, P=0.018), although a greater attrition of smokers with asthma between the two surveys might have been a possible explanation.7
Several studies have shown that adolescents with asthma are more likely to smoke, especially at the more severe end of the spectrum.8,9 Adolescents with or without asthma in the US Add Health Project were equally as likely to progress to heavier levels of smoking,10 whereas in a Danish study, the odds for smoking at least 15 cigarettes per day were almost 1.5-fold higher for adolescents with asthma.11
Smoking-related beliefs and knowledge in those with asthma
Even 20 years ago, substantially more Australian smokers with asthma “believed that smoking has had at least a moderately bad effect on their own health” than smokers without asthma (58% vs 38%, P<0.001).12 The perception of higher health risks from smoking can contribute to motivation to quit, but these perceptions are balanced against the perceived benefits to an individual of continued smoking and ability to resist the smoking influences from parents and close friends.13 Asthma diagnosis is associated with earlier age of regular smoking onset, higher number of quit attempts, and reasons for quitting related to self-control, suggesting that smokers with asthma may have more difficulty quitting and unique reasons for quitting.14 Anxiety sensitivity, the fear of aversive internal anxiety states, might offer some explanation as to why sustained quitting can be more difficult for smokers with asthma compared with non-asthmatics.3
Quitting and smokers with asthma
Asthma-specific reasons for quitting can include heightened health concerns and need for self-control.14 Smokers with asthma have increased odds of reporting high or very high nicotine addiction compared with smokers without asthma (adjusted odds ratio [OR], 1.57; 95% confidence interval [CI], 1.16–2.10), with their doctors more likely to advise the participants to quit smoking (adjusted OR, 2.22; 95% CI, 1.35–3.65).5 US primary care physicians more frequently provided counseling to smokers with COPD than smokers without chronic diseases (46% vs 25%, P<0.001) or to smokers with asthma (31%).15 Adults enrolled in the telephone counseling service, Quitline, were only a small fraction of all smokers attempting to quit, but those with asthma and/or COPD were found to be less likely to have quit smoking after 30 days.2 This contrasts similar abstinence rates at a smoking cessation clinic in Greece, which considered individual asthma, COPD, and overlap subgroups separately.16
Smoking abstinence is particularly important in adolescence, as nicotine exposure from cigarette experimentation during this period may be more likely to lead to sustained dependence and progression to regular smoking.17,18 Some evidence suggests that dependence and progression develop more quickly in adolescents with asthma, corresponding with greater difficulty quitting and more quit attempts.19 As an interaction between the adverse effects of current asthma and personal smoking on post-bronchodilator (BD) airflow obstruction in mid-adult life is likely,20,21 smoking abstinence at the earliest opportunity is key to maintaining optimal lung function in later life.
Lung function measurement in smokers in general
Although intuitively one might expect that providing smokers with evidence of smoking-related damage to their lungs might increase quit rates, a Cochrane review providing feedback of personal biomarkers including spirometry failed to find evidence that this improved quit rates in smokers.22 Measurement of lung function in conjunction with telling smokers their lung age and providing a graphical representation of lung function decline in the form of the Fletcher-Peto diagram (the age of the average person who has an forced expiratory volume in 1 second [FEV1] equal to the individual) significantly improved quit rates in a UK study in general practice.23 This applied whether the lung function was abnormal or not. However, the mechanism by which this intervention achieved its effect was unclear.
Adverse health effects
Continuous smokers have been estimated to die at least one decade earlier than nonsmokers, with approximately a 90% reduction in the risk of death if an individual quits before the age of 40 years.24 From the perspective of asthma, the main adverse outcomes include new and poorly controlled asthma, increased chronic airflow limitation, and possibly the coexistence of COPD. Relevant studies have been summarized in Table 2.
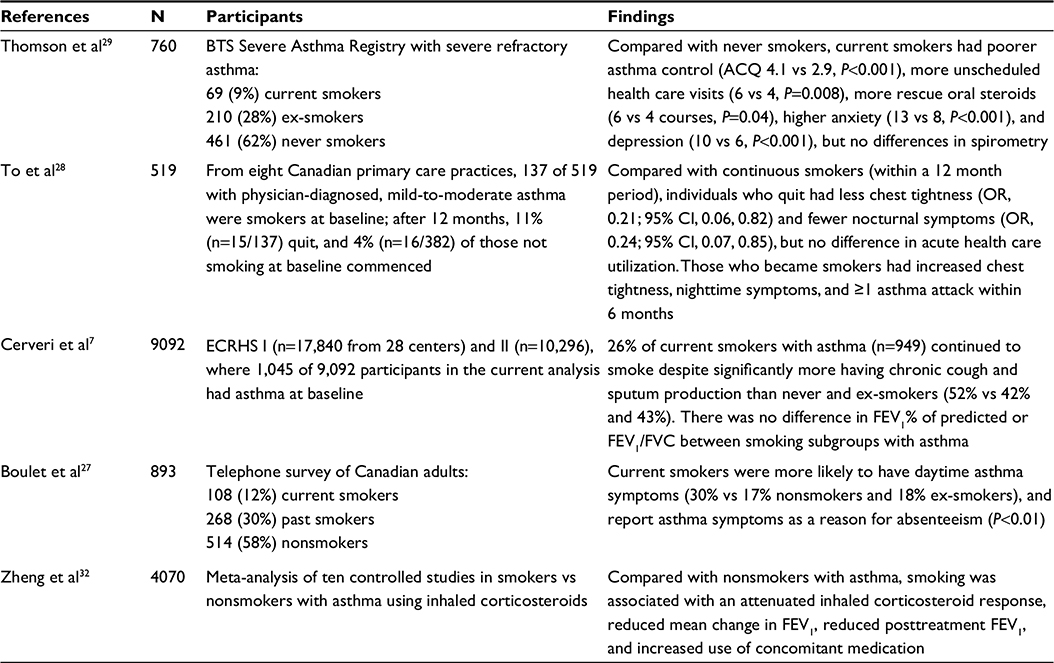 | Table 2 Key studies that examined personal smoking and adverse asthma outcomes Notes: FEV1/FVC, the ratio between FEV1 and forced vital capacity as a measure of airflow limitation/obstruction. Abbreviations: ACQ, Asthma Control Questionnaire; BTS, British Thoracic Society; ECRHS, European Community Respiratory Health Survey; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; OR, odds ratio. |
Poorly controlled adult asthma
Current active smokers who also have asthma report poorer symptom control than nonsmokers with asthma.25–27 Adverse clinical and health care outcomes have been shown in smokers with both mild-to-moderate28 and severe asthma.29
Poor asthma control in current smokers may relate to reduced efficacy of inhaled corticosteroids (ICSs),30 leading to inadequately controlled airway inflammation and increased bronchial hyperreactivity.31 In the meta-analysis of ten studies that examined ICS therapy in people with asthma, smoking was associated with reduced ICS efficacy (Table 2).32 Compared with nonsmokers, smoking at least five cigarettes per day was associated with a reduced post-ICS treatment in pre-BD FEV1 (standardized mean difference, –0.19; 95% CI, –0.33 to –0.06) and increased use of concomitant medications (standardized mean difference, 0.054; 95% CI, 0.17–0.91). This reduction in corticosteroid sensitivity can occur even in light smokers with mild asthma.30 While dose escalation of ICS might hypothetically alleviate this corticosteroid resistance,33 the addition of long-acting β-agonist (LABA) to low-to-medium dose ICS may be preferable to increasing ICS dose.34 However, more evidence is needed to assess the relative effectiveness of different treatment options that include extra-fine ICS particle formulations and leucotriene receptor antagonists.35
Many studies have shown a reduction in asthma symptoms in people who quit smoking,36 although a large Danish population-based cohort showed an increase in the odds for incident asthma over a decade, especially for “new quitters”.37
Worse asthma control has also been associated with exposure to second-hand smoke (SHS) in young adults.38 During the first 3 years following the implementation of smoke-free legislation in England, emergency admissions for asthma decreased by 4.9% (95% CI, 0.6–9.0) for those 16 years and older.39
Asthma morbidity and poorer quality of life have been linked to depression and risk-taking behaviors such as smoking.40 Asthma symptoms might also be a result of poor treatment adherence,41 and this is particularly relevant to those with difficult-to-treat asthma and major psychiatric illness.42
Asthma and lung function deficits
In addition to “reversible airflow obstruction”, the hallmark of asthma, the occurrence of “irreversible” airflow obstruction from long-standing and/or severe asthma in adult life, is well recognized.21,43 Childhood asthma as a potential predictor of reduced peak lung function in adulthood has been illustrated by the Melbourne Asthma Study in which 10-year-old participants with severe asthma were recruited in 1967 before ICSs were available.44 Compared with participants with mild asthma, the severe subgroup already had a decrement in lung function at study entry, without further deficits over the next four decades, despite ongoing symptoms.45 In terms of lung function decline, adults with asthma from the Copenhagen City Heart Study had an approximately twofold higher rate of pre-BD FEV1 decline compared with those without asthma (38 mL/year vs 22 mL/year).46
There has been recent interest in the potential for interactions between the effects of smoking and asthma on post-BD lung function. In one study of middle-aged adults, a multiplying effect was seen for current asthma and personal smoking with regard to “fixed” airflow obstruction, where the combined association was more than the sum of individual estimates.20,21 This observation may in part reflect the entity of ACOS.
Asthma–COPD overlap syndrome
It is widely acknowledged that adult smokers with asthma and atopic individuals with COPD are two populations who have largely been excluded from clinical trials in the past. These “overlap” individuals have recently been highlighted as a subgroup which may show a greater benefit from ICS therapy given their relative corticosteroid responsiveness.47 The combined Global initiative for chronic Obstructive Lung Disease (GOLD) and Global Initiative for Asthma (GINA) strategy has now formally labeled this clinical entity as ACOS.48
ACOS is estimated to account for ˜15%–25% of obstructive airway diseases. Compared with patients with COPD, patients with ACOS are generally younger with the combined risk factors of smoking and atopy, and have higher rates of exacerbations without more severe chronic airways obstruction.49,50
Smoking from a public health perspective
Antismoking campaigns and the general population
A number of public health programs followed the release of the 1964 US Surgeon General’s “report on smoking and health”, including mass media campaigns, increasing the federal cigarette tax, restrictions on tobacco advertizing,51 and most recently, the introduction of plain cigarette packaging in Australia in 2012. The Surgeon General’s 1986 and 2006 reports documented links between parental smoking, childhood respiratory illness, and reduced lung function growth.52 The 1986 report led to the first successful implementation of a smoke-free environment in a US medical facility.53
Between 2001 and 2010 in Australia, regular smoking decreased from 25% to 19% for adult males, compared with 21% to 16% for adult women.54 While Australia and other high-income countries have made major progress to control tobacco consumption, the highest levels of preventable and premature death can be still attributed to personal smoking,55 and this is still rising in low- and middle-income countries.
Parental smoking and childhood asthma
A causal link has been established between early childhood exposure to SHS and the incidence of new-onset wheeze and asthma,56 suggesting that SHS exposure may unmask clinical symptoms of asthma in those otherwise susceptible. Maternal smoking during pregnancy has been shown to be most closely related to incident asthma,57 and persistent asthma among Mexican, Puerto Rican, and black children.58 It has been documented that children with respiratory illness can be aware of the negative consequences of smoking and exposure to SHS.59
Smoking cessation strategies
As smoking is a modifiable risk factor for poorer asthma control and greater symptom severity, smoking cessation in asthmatic individuals is a clinical strategy likely to improve patient outcomes. However, only few studies have assessed evidence-based treatments for nicotine dependence in people with asthma.60 As a result, many of the following strategies relate to smokers in general, unless otherwise specified. While still relevant to the smoker who has asthma, the integration of these smoking cessation strategies into asthma care is important and has been addressed by subsequent sections.
Brief interventions for smoking cessation in those with asthma can involve opportunistic advice,61 such as when individuals present for a review of their asthma and/or lung function testing. Public education, resources, and advice could be more heavily targeted toward this more susceptible group.
Advice from a health professional
Health professionals have the potential to assist people to give up smoking through giving advice, encouragement, and support, regardless of asthma status. It is best practice to ask smokers if they are ready to quit using the “five As” approach, originally proposed by the US Clinical Practice Guideline, and is summarized in Table 3.62 Even if people appear not to be ready to quit, advice from a health professional can still be a trigger to quit, particularly in the context of adverse health problems.63 Thus, there is benefit in urging all smokers to think about quitting whenever the opportunity arises.
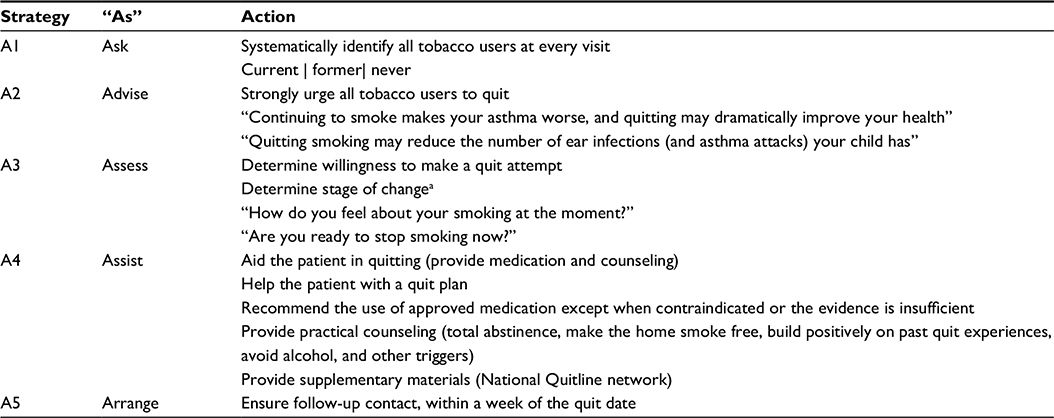 | Table 3 The “five As” strategic model for treating tobacco use and dependence, for the patient willing to quit Notes: Adapted from Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service; 2008.62 aThe Australian Clinical Guidelines now emphasize the “stages of change”, as opposed to “readiness to quit”.61 |
The current evidence does not support restricting quitting advice and encouragement only to those smokers perceived to be “ready to quit”, and thus guidelines now recommend that all smokers are advised to quit regardless of readiness.61 If a smoker is ambivalent, then motivational interviewing can be used to resolve ambiguity and facilitate commitment to quitting. The rationale of this new approach is based on other aspects of medical care where patients can usually “opt out” by declining treatment.64
Telephone Quitlines are an essential strategy for smoking cessation, as they provide a brief and minimally invasive intervention which can be particularly convenient for people with physical impairment from chronic diseases such as asthma and COPD.62 A dose–response in effectiveness is apparent, with at least three calls increasing the chances of quitting smoking when compared with individual strategies that include standard self-help materials, brief advice, or pharmacotherapy alone.65
Cognitive and behavioral strategies
Behavioral counseling and motivational interviewing
Brief or intensive counseling has been shown to increase quit rates, with or without concurrent pharmacotherapy.66 Behavioral support in person or via telephone increases the chance of success by up to 25%, especially for those having at least four contact sessions.67 Brief motivational advice from health professionals has been shown to be effective in encouraging smoking cessation in all current smokers,68 and even a brief (<3 minutes) intervention can make a significant difference (relative risk, 1.66; 95% CI, 1.42–1.94). The interaction involves asking open-ended questions, reflective listening, and summarizing. The likes and dislikes of the smoking habit and the act of quitting can be listed, and inconsistencies in the smoker’s beliefs and personal goals regarding health and fitness discussed. In the lead-up to the quit day, individuals can keep a smoking diary that may identify smoking triggers and high-risk environments, such that the risk of relapse can be lessened by avoiding such situations. The smoker can also list the benefits of quitting and the adverse consequences should smoking recommence. Thus, behavioral strategies can be individualized to help people cope with triggers and high-risk situations. Similarly, a range of cognitive and behavioral strategies such as acceptance and commitment therapy and mindfulness training could be applied to block thoughts about withdrawal symptoms and other perceived benefits of restarting smoking.
For carers of children with asthma, the effectiveness of parental education and counseling programs has not been proven.69 Nonetheless, motivational interviewing or intensive counseling of parents toward quitting might be useful strategies to reduce asthma symptoms in children, particularly if the public health message conveys the children’s concerns.59
Group behavior therapy
As distinct from social support from family and friends, for smokers in general, professional group therapy can offer more benefit than self-help and other less intensive interventions.70 Pooled results from 55 studies showed group programs to be more effective than self-help (OR 2.04 [95% CI 1.6–2.6]) or no intervention (OR 2.17 [1.4–3.5]). Specifically, in the Lung Health Study, 22% of smokers who received 12 sessions of group behavior modification techniques and nicotine gum were sustained quitters with the fewest respiratory symptoms after 5 years, as compared with 5% of participants in the usual care group.71 Such intensive therapy generally depends on a trained facilitator, and it is not clear whether these group therapies are more effective or cost-effective than intensive individual counseling.70 No information about individuals with asthma was available in this review.
Pharmacotherapies
There are few studies of pharmacotherapy for smoking cessation in patients with asthma. For smokers in general, nicotine replacement therapy (NRT), sustained release bupropion, and varenicline may be considered as first-line smoking cessation medications.61 Unlike NRT, bupropion and varenicline have not been shown to be effective without counseling and support. For each individual smoker, the choice of pharmacotherapy can be personalized depending on circumstances and preferences that include drug contraindications, adverse effects, previous experience from quit attempts, cost, and convenience. There are limited clinical data for adolescents <18 years of age, and varenicline has not been evaluated as a treatment modality in this group.72
Nicotine replacement therapy
Only one randomized controlled trial has addressed the efficacy of NRT in the subgroup of people with asthma.6 Of 220 Danish smokers with asthma, participants were allocated to 1) complete cessation, 2) reduction to fewer than seven cigarettes daily, and 3) usual smoking, where loss to follow-up was greatest for those assigned to the intervention.73 Subjects received short-acting NRT to curb acute cravings (chewing gum and/or inhaler), but neither long-acting nicotine patches nor counseling. Either 2 mg or 4 mg strengths of nicotine gum were prescribed depending on Fagerstrom score. At 4 months, compared with a 5% cessation rate for control subjects, abstinence rates were 15% for both reduction and cessation groups which equaled 12% for the entire group. A further 15% reduced their tobacco consumption to fewer than seven cigarettes per day. While this intervention only modestly improved asthma symptoms, there was a decrease in bronchial reactivity and reduction in ICS dose at the follow-up. Thus, NRT was effective in smokers with asthma in the absence of counseling, and statistically significant respiratory outcomes were achieved.
Generally, provision of a combination of short- and long-acting NRT is recommended. Research has repeatedly shown that a combination of pharmacotherapy and behavioral support results in higher cessation rates than either approach alone. For example, West and Owen found 52-week follow-up abstinence rates of 7% for English smokers using single type of NRT alone, 10% for smokers using dual NRT alone, and 20% for smokers using combination NRT plus behavioral support.74
Other pharmacotherapy
The use of bupropion and varenicline combined with counseling is regarded as an appropriate smoking cessation strategy,6 although trials of such strategies targeting smokers with asthma are lacking. In brief, bupropion was originally developed as an antidepressant, and while it increases the quitting rate compared with placebo, it is not as effective as varenicline.61 Varenicline is a nicotine receptor partial agonist, which can increase the odds of smoking abstinence at least twofold when compared with pharmacologically unassisted quit attempts.75 It has been found to be more effective than bupropion, but the lack of efficacy over NRT may reflect the paucity of comparative studies. Serious adverse associations between varenicline, acute cardiovascular events, and suicidal ideation have not yet been excluded, and these possibilities should be discussed when considering which pharmacotherapy is most appropriate.61 The increased risk of seizures from bupropion (1:1,000) is also an important consideration.76
Potential asthma-specific strategies for smoking cessation
Technologies and smoking cessation
Consumer health informatics applications provide health information via hardware, software, and web-based applications to facilitate health-related decisions made by the health care consumer.77 Reviews have consistently demonstrated the effectiveness of online or web-based,78 computer-delivered,79 and electronic system80 interventions for smoking cessation, compared with printed materials, emailed messages, and no intervention controls. In another review of 146 studies that looked at interventions such as interactive multimedia, web-based computer programs, and monitoring systems,81 none had specifically targeted smokers with asthma.
For smokers in general, web-based internet programs have the potential for high cost-effectiveness as user acceptability is higher than for clinical, work-site, and/or telephone programs, and the costs per user are relatively low.82 Interventions range from providing a list of smoking cessation websites, to moderately interactive and tailored programs, to high-depth tailored stories, and highly personalized message sources. In some cases, the individualization of one-to-one counseling can be effectively replicated.83 Such innovative interventions are likely to be particularly useful for adolescents and young adults who are most familiar with the technology, and may be of more limited benefit for those who are older, have higher nicotine dependence, and/or are from a lower socioeconomic background.82 An independent meta-analysis of 22 randomized controlled trials favored the use of web- and computer-based smoking cessation programs over no intervention (overall relative risk, 1.44; 95% CI, 1.27–1.64; n=29,549),84 while the Cochrane review suggested that further studies that focused on interactivity and tailoring to subpopulations were needed.83
Text messages to cellular phones have been used successfully both to improve quit rates in the general population and to improve asthma symptoms in a small group of nonsmokers.85,86 In the systematic review,85 favorable results were reported by two randomized controlled trials, although generalizability of the findings may be limited to contemplative smokers and respondents to web-based advertisements.87,88 While evidence for and against the use of text messaging in improving asthma symptoms or quit rates in smokers with asthma is still lacking, this form of intervention has the advantages of being personalized, affordable, and location independent.87
Potential barriers to consumer health informatics applications for all smokers include usability (technical plus limited literacy, language, and technological skills), limited clinician endorsement, lack of access, and concerns about data security and privacy.81 Future studies that assess the acceptability, reach, efficacy, and cost-effectiveness of these strategies for smokers with and without asthma should clarify the role for consumer health informatics in this emerging field.
Electronic nicotine devices and smoking cessation
Electronic nicotine devices (ENDs; otherwise known as e-cigarettes) have been commercially available since 2006 with sales growing steadily, such that their use by American adolescents now exceeds that of conventional cigarettes.89 Unlike combustible tobacco cigarettes, ENDs deliver nicotine in an inhalable form without the smoke, thereby minimizing exposure to non-nicotine constituents that can cause harmful health effects. As with traditional NRT, the provision of nicotine reduces withdrawal symptoms. ENDs additionally mimic the hand-to-mouth action and inhaling and exhaling of “smoke” or vapor.
Although using ENDs has been estimated to be ˜95% safer than smoking combustible tobacco cigarettes,90 the data regarding their use in smokers with asthma are lacking. In a small, retrospective study of 18 smokers with asthma who became regular END users for more than 12 months, the mean conventional cigarette consumption decreased from 22 to 1.7 daily, with a small increase in FEV1 (3.30 L vs 3.40 L, P=0.005).91 The null finding with regard to asthma exacerbations may have been due to limited power (P=0.15). These data have been included in a Cochrane systematic review,92 where the bold suggestion was made that ENDs might be an option for individuals with asthma who are otherwise unable to quit smoking. While the change from conventional cigarettes to ENDs might offer potential harm minimization in asthma, nicotine exposure still has adverse effects especially in pregnancy and cardiovascular disease, and more research is needed to clarify its safety profile.
Smoking cessation and relapse
In general, many smokers make multiple attempts before successfully quitting. In addition to individual vulnerability to tobacco withdrawal symptoms, factors contributing to relapse include social situations when drinking alcohol, being around other smokers, as well as stress related to work, relationships, and finances.1 A different drug or combination of smoking cessation medications may be trialed for smokers who have been unsuccessful in their quit attempt or, a combination of NRT can be repeated for a subsequent attempt.93
Depending on the pharmacotherapy used, 5%–25% of smokers who attempt to quit abstain at 6 months, but around half of those who are abstinent at 1 year, relapse within the next 7 years.94 Thus, follow-up by a health professional is essential, preferably in the first week and month after quitting and thereafter for at least 5 years.61
Smoking cessation as a component of the Asthma management plan
People with asthma who smoke should be encouraged strongly to quit, as a successful attempt might effectively optimize the anti-inflammatory action of their prescribed ICSs.33 Including this intervention within asthma self-management empowers people with asthma to act in their own best interests, while the health practitioner can act primarily as an educator and a facilitator.95 Asthma-specific considerations for smoking cessation have been suggested in Table 4.
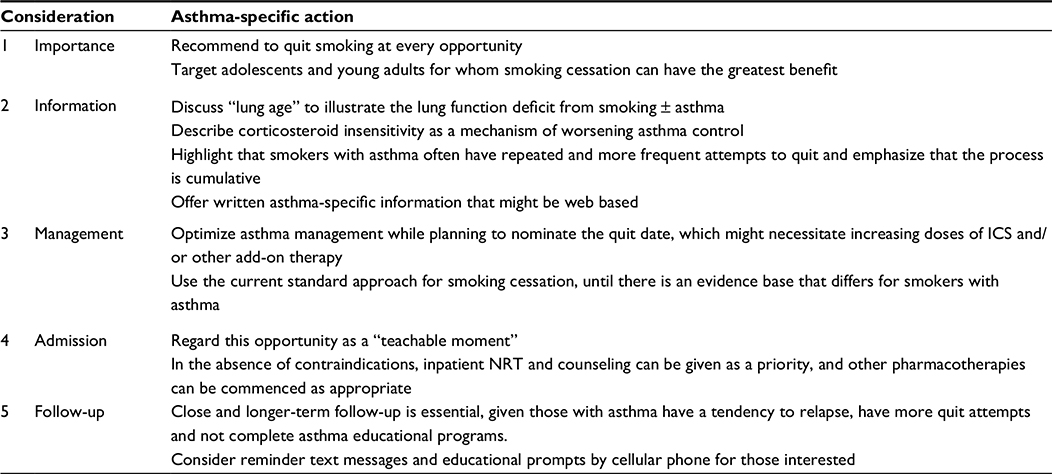 | Table 4 Asthma-specific considerations when quitting Abbreviations: ICS, inhaled corticosteroid; NRT, nicotine replacement therapy. |
Opportunities for smoking cessation
During the inpatient admission
Hospitalization of a current smoker with an acute exacerbation or “attack” of asthma may be an ideal time to provide smoking cessation advice, being a so-called teachable moment. Not only is the patient prohibited from smoking as virtually all hospitals are now smoke-free environments, the admission will most likely highlight the individual’s vulnerability to asthma exacerbation from smoking.62 This hospital-enforced abstinence, as well as the obvious link between the admission and the underlying smoking behavior, provides a pressing opportunity to prescribe NRT to lessen the withdrawal symptoms, to be followed by motivational interviewing and prescription of other pharmacotherapy as appropriate. It is possible that a more positive experience of nicotine withdrawal during the admission might facilitate the maintenance of abstinence and/or success in a future quit attempt.62 It is imperative that these individuals have short- as well as longer-term supportive contact from health professionals in order to minimize the likelihood of relapse.96
During the outpatient consultation
For individuals who smoke and present to ambulatory care with asthma symptoms, it is important to view this as an opportunity to optimize asthma medication and provide smoking cessation advice. This is relevant to all, but particularly for those with severe asthma,29 and women who are pregnant.97
For young adolescents presenting for review of their asthma, establishing their smoking status in addition to their degree of asthma control is crucial. This can be often difficult unless this is discussed without the presence of their parent and/or guardian. Smoking cessation advice in addition to optimizing medication dosage, delivery, and adherence can then be provided.
Potential for improved patient outcomes
Smoking cessation and improved asthma control
In a community-based Canadian cohort of 519 people with asthma, smoking abstinence at 12 months was achieved by 11% and was associated with a significant reduction in chest tightness (OR, 0.21; 95% CI, 0.06, 0.82) and nighttime symptoms (OR, 0.24; 95% CI, 0.07, 0.085; Table 2).28 Symptoms including chest tightness, nocturnal symptoms, asthma attacks, and clinic attendances for asthma increased for current smokers during the follow-up period.
Smoking cessation and improved lung function
While many studies support the observation that abstaining from smoking improves asthma symptoms,36 few studies have measured the impact of quitting on spirometry. Improvements occurred after 6 weeks in a small study (n=20) in which the mean increase in pre-BD FEV1 from baseline was 407 mL only in quitters (95% CI, 21, 793).98
The Lung Health Study randomized smokers with mild-to-moderate airflow obstruction to an intensive, long-term smoking cessation program or usual care more than 5 years.99 Pre-BD lung function improved during the first year for sustained quitters (FEV1 +47 mL), and mean (±SD) rate of FEV1 decline for sustained quitters was 31±48 mL/year, compared with the rate for continuing smokers (62±55 mL/year). As asthma was not an exclusion criterion, the study may have included some individuals with the ACOS.
Personalized professional support
The GINA recommends for current and former smokers with asthma to be assessed for the coexistence of chronic airflow limitation, where the definition of this ACOS is still evolving.43 Through the measurement of post-BD spirometry, the individual’s lung age can be determined and airflow obstruction that meets the lung function criterion for COPD can be identified. In the absence of diagnostic uncertainty or atypical symptoms and signs, initial therapy would include low-to-moderate dose ICS for symptom control, and the avoidance of LABA monotherapy for safety reasons.43
For such smokers with asthma, ideally a tailored individualized approach should be taken to manage their both asthma and smoking habit. For smokers with poorly controlled asthma, optimizing asthma therapy, while simultaneously planning a suitable quit date, would seem appropriate. Within the GINA framework, higher-dose ICS may be needed to control symptoms, and smoke exposure that is either from personal use or environmental sources should be strongly discouraged. Other pharmaceutical options that have been studied include adding a LABA to ICS,34 and further research is needed with regard to fine-particle ICS, and/or add-on antileukotriene therapy.35 For smokers of at least 15 cigarettes per day who fulfill clinical criteria for ACOS,48 the addition of bupropion to NRT and counseling may be considered based on the evidence for mild-to-moderate COPD.100 Careful multidisciplinary management using mental health services is also appropriate for smokers with asthma and coexistent mental health issues.
For adolescents, asthma education delivered to 8–10-year-old Jordanian students by older peer leaders was also successful in teaching about asthma self-management and motivating students to avoid smoking.101 Using the Arabic version of the self-efficacy subscale of the Self-Administered Nicotine Dependence Scale,102 self-efficacy to resist smoking was significantly higher in the intervention group (mean score 11.5 vs 6.9), and the mean difference was statistically significant (mean difference 4.6; 95% CI, 2.9–6.4; P=0.03). This peer-led intervention was in part designed to assess the effectiveness of the Adolescent Asthma Action (Triple A) program on the capacity to resist smoking, which was originally developed in Australia to be implemented in a supportive school environment.103 The National Asthma Council offers a website for adolescents with a link to this program: http://www.asthmahandbook.org.au/populations/adolescents/self-management. The following website: http://www.asthmahandbook.org.au/management/adults, may be appropriate for relatively well educated adults.
Future integration of smoking cessation strategies into asthma care
Quitting smoking can improve asthma symptoms and reduced lung function, but the relatively low rates of successful quitting places these smokers with asthma at greater risk of adverse health effects including poorly controlled asthma and the potential for the ACOS. For smokers with asthma, the integration of pharmacotherapy for smoking cessation with counseling is still best practice. Where appropriate, asthma medication can be intensified while planning a cessation date. A discussion around lung age and the provision of asthma-specific reading material can personalize management for individuals. For smokers, regardless of asthma status, communication and web-based technologies based on consumer health informatics show some promise to aid smoking cessation over the course of the quitting process. Specifically for smokers with asthma, further studies that address the issue of acceptability, reach, efficacy, and cost-effectiveness will provide valuable information to tailor more optimal strategies for this more susceptible subgroup. The GINA strategy has provided updated guidelines for the management of asthma and the ACOS.43
As a health priority, the substantial benefits of smoking cessation should be emphasized to current smokers with asthma, through positive educational messages delivered by health practitioners and supported by Quitlines. Targeting adolescents and young adults before they become established smokers is vital because the earlier smokers quit, the easier cessation is to achieve and the health benefits are greatest. Considering the specific needs of current smokers with asthma may facilitate a smoking cessation intervention that is more individualized and aimed at improving quit rates in the longer term. Public education, resources, and advice could be more strongly focused toward this more susceptible group.
Disclosure
Christine F McDonald is on Advisory Boards for Novartis, Astra Zeneca and GlaxoSmithKline, has received speaker fees from Astra Zeneca and GlaxoSmithKline, and conference assistance from Boehringer Ingelheim. Michael J Abramson has received a consultancy from AstraZeneca, conference support from Boehringer-Ingelheim and Sanofi, and together with Billie Bonevski, received investigator initiated grants from Pfizer and Boehringer-Ingelheim. Billie Bonevski is supported by career development fellowships from the National Health & Medical Research Council (NHMRC 1063206) and Gladys M Brawn. Jennifer L Perret is supported by a post-doctoral fellowship from the Center for Air quality and health Research evaluation (CAR) which is funded by the NHMRC, and reports no competing financial interests.
References
Cancer Institute NSW. New South Wales Smoking and Health Survey 2009. Sydney: Cancer Institute NSW; 2009. | ||
Bush T, Zbikowski SM, Mahoney L, Deprey M, Mowery P, Cerutti B. State quitlines and cessation patterns among adults with selected chronic diseases in 15 states, 2005-2008. Prev Chronic Dis. 2012;9:120105. | ||
McLeish AC, Johnson AL, Avallone KM, Zvolensky MJ. Evaluating the role of anxiety sensitivity in barriers to cessation and reasons for quitting among smokers with asthma. Psychol Health Med. 2015:1–12. | ||
Thomson NC, Chaudhuri R, Livingston E. Asthma and cigarette smoking. Eur Respir J. 2004;24(5):822–833. | ||
Vozoris NT, Stanbrook MB. Smoking prevalence, behaviours, and cessation among individuals with COPD or asthma. Respir Med. 2011;105(3):477–484. | ||
Jimenez-Ruiz CA, Andreas S, Lewis KE, et al. Statement on smoking cessation in COPD and other pulmonary diseases and in smokers with comorbidities who find it difficult to quit. Eur Respir J. 2015;46(1):61–79. | ||
Cerveri I, Cazzoletti L, Corsico AG, et al. The impact of cigarette smoking on asthma: a population-based international cohort study. Int Arch Allergy Immunol. 2012;158(2):175–183. | ||
Zbikowski SM, Klesges RC, Robinson LA, Alfano CM. Risk factors for smoking among adolescents with asthma. J Adolesc Health. 2002;30(4):279–287. | ||
Van de Ven MO, Engels RC, Kerstjens HA, Van den Eijnden RJ. Bidirectionality in the relationship between asthma and smoking in adolescents: a population-based cohort study. J Adolesc Health. 2007;41(5):444–454. | ||
Tercyak KP. Brief report: social risk factors predict cigarette smoking progression among adolescents with asthma. J Pediatr Psychol. 2006;31(3):246–251. | ||
Precht DH, Keiding L, Madsen M. Smoking patterns among adolescents with asthma attending upper secondary schools: a community-based study. Pediatrics. 2003;111(5 pt 1):e562–e568. | ||
Wakefield M, Ruffin R, Campbell D, Roberts L, Wilson D. Smoking-related beliefs and behaviour among adults with asthma in a representative population sample. Aust N Z J Med. 1995;25(1):12–17. | ||
van Zundert RM, Engels RC, Kleinjan M, van den Eijnden RJ. An integration of parents’ and best friends’ smoking, smoking-specific cognitions, and nicotine dependence in relation to readiness to quit smoking: a comparison between adolescents with and without asthma. J Pediatr Psychol. 2008;33(8):821–832. | ||
Avallone KM, McLeish AC, Zvolensky MJ, Kraemer KM, Luberto CM, Jeffries ER. Asthma and its relation to smoking behavior and cessation motives among adult daily smokers. J Health Psychol. 2013;18(6):788–799. | ||
Nelson KE, Hersh AL, Nkoy FL, Maselli JH, Srivastava R, Cabana MD. Primary care physician smoking screening and counseling for patients with chronic disease. Prev Med. 2015;71:77–82. | ||
Gratziou C, Florou A, Ischaki E, et al. Smoking cessation effectiveness in smokers with COPD and asthma under real life conditions. Respir Med. 2014;108(4):577–583. | ||
Leone FT, Ferkol TW. Such are the impositions of Quackery: E-cigarettes. Ann Am Thorac Soc. 2015;12(6):787–788. | ||
Center for Health Promotion and Education [webpage on the Internet]. The Health Consequences of Smoking, Nicotine Addiction: A Report of the Surgeon General. 1988. Available from: http://profiles.nlm.nih.gov/NN/B/B/Z/D. Accessed August 1, 2015. | ||
Van De Ven MO, van Zundert RM, Engels RC. Effects of asthma on nicotine dependence development and smoking cessation attempts in adolescence. J Asthma. 2013;50(3):250–259. | ||
Perret JL, Dharmage SC, Matheson MC, et al. The interplay between the effects of lifetime asthma, smoking, and atopy on fixed airflow obstruction in middle age. Am J Respir Crit Care Med. 2013;187(1):42–48. | ||
Perret JL, Walters EH, Abramson MJ, McDonald CF, Dharmage SC. The independent and combined effects of lifetime smoke exposures and asthma as they relate to COPD. Expert Rev Respir Med. 2014;8(4):503–514. | ||
Bize R, Burnand B, Mueller Y, Rege-Walther M, Camain JY, Cornuz J. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2012;12:CD004705. | ||
Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336(7644):598–600. | ||
Jha P, Ramasundarahettige C, Landsman V, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–350. | ||
Thomson NC, Chaudhuri R. Asthma in smokers: challenges and opportunities. Curr Opin Pulm Med. 2009;15(1):39–45. | ||
Chaudhuri R, McSharry C, McCoard A, et al. Role of symptoms and lung function in determining asthma control in smokers with asthma. Allergy. 2008;63(1):132–135. | ||
Boulet LP, FitzGerald JM, McIvor RA, Zimmerman S, Chapman KR. Influence of current or former smoking on asthma management and control. Can Respir J. 2008;15(5):275–279. | ||
To T, Daly C, Feldman R, McLimont S. Results from a community-based program evaluating the effect of changing smoking status on asthma symptom control. BMC Public Health. 2012;12:293. | ||
Thomson NC, Chaudhuri R, Heaney LG, et al. Clinical outcomes and inflammatory biomarkers in current smokers and exsmokers with severe asthma. J Allergy Clin Immunol. 2013;131(4):1008–1016. | ||
Lazarus SC, Chinchilli VM, Rollings NJ, et al. Smoking affects response to inhaled corticosteroids or leukotriene receptor antagonists in asthma. Am J Respir Crit Care Med. 2007;175(8):783–790. | ||
Chinn S, Jarvis D, Luczynska CM, et al. An increase in bronchial responsiveness is associated with continuing or restarting smoking. Am J Respir Crit Care Med. 2005;172(8):956–961. | ||
Zheng X, Guan W, Zheng J, et al. Smoking influences response to inhaled corticosteroids in patients with asthma: a meta-analysis. Curr Med Res Opin. 2012;28(11):1791–1798. | ||
Adcock IM, Barnes PJ. Molecular mechanisms of corticosteroid resistance. Chest. 2008;134(2):394–401. | ||
Clearie KL, McKinlay L, Williamson PA, Lipworth BJ. Fluticasone/Salmeterol combination confers benefits in people with asthma who smoke. Chest. 2012;141(2):330–338. | ||
Price D, Bjermer L, Popov TA, Chisholm A. Integrating evidence for managing asthma in patients who smoke. Allergy Asthma Immunol Res. 2014;6(2):114–120. | ||
McLeish AC, Zvolensky MJ. Asthma and cigarette smoking: a review of the empirical literature. J Asthma. 2010;47(4):345–361. | ||
Godtfredsen NS, Lange P, Prescott E, Osler M, Vestbo J. Changes in smoking habits and risk of asthma: a longitudinal population based study. Eur Respir J. 2001;18(3):549–554. | ||
Comhair SA, Gaston BM, Ricci KS, et al. Detrimental effects of environmental tobacco smoke in relation to asthma severity. PLoS One. 2011;6(5):e18574. | ||
Sims M, Maxwell R, Gilmore A. Short-term impact of the smokefree legislation in England on emergency hospital admissions for asthma among adults: a population-based study. Thorax. 2013;68(7):619–624. | ||
Bender BG. Risk taking, depression, adherence, and symptom control in adolescents and young adults with asthma. Am J Respir Crit Care Med. 2006;173(9):953–957. | ||
Armour CL, Lemay K, Saini B, et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J Asthma. 2011;48(9):914–922. | ||
Robinson DS, Campbell DA, Durham SR, et al. Systematic assessment of difficult-to-treat asthma. Eur Respir J. 2003;22(3):478–483. | ||
Reddel HK, Bateman ED, Becker A, et al. A summary of the new GINA strategy: a roadmap to asthma control. Eur Respir J. 2015;46(3):622–639. | ||
Phelan PD, Robertson CF, Olinsky A. The Melbourne Asthma Study: 1964-1999. J Allergy Clin Immunol. 2002;109(2):189–194. | ||
Tai A, Tran H, Roberts M, et al. Outcomes of childhood asthma to the age of 50 years. J Allergy Clin Immunol. 2014;133(6):1572e–1578e. | ||
Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339(17):1194–1200. | ||
Miravitlles M, Calle M, Soler-Cataluna JJ. Clinical phenotypes of COPD: identification, definition and implications for guidelines. Arch Bronconeumol. 2012;48(3):86–98. | ||
Global Strategy for Asthma Management and Prevention [homepage on the Internet]. Diagnosis of Diseases of Chronic Airflow Limitation: Asthma, COPD and Asthma-COPD Overlap Syndrome (ACOS). 2014. Available from: http//www.ginasthma.org. Accessed October 15, 2014. | ||
Louie S, Zeki AA, Schivo M, et al. The asthma-chronic obstructive pulmonary disease overlap syndrome: pharmacotherapeutic considerations. Expert Rev Clin Pharmacol. 2013;6(2):197–219. | ||
Hardin M, Silverman EK, Barr RG, et al. The clinical features of the overlap between COPD and asthma. Respir Res. 2011;12:127. | ||
U.S. Department of Health and Human Services. The Health Consequences of Smoking – 50 Years of Progress. Atlanta, GA: U.S. Department of Health and Human Services; 2014. | ||
Samet JM. The surgeon generals’ reports and respiratory diseases. From 1964 to 2014. Ann Am Thorac Soc. 2014;11(2):141–148. | ||
Hurt RD, Berge KG, Offord KP, et al. The making of a smoke-free medical center. JAMA. 1989;261(1):95–97. | ||
Scollo MM, Winstanley MH [homepage on the Internet]. Tobacco in Australia: Facts and issues. Melbourne: Cancer Council Victoria; 2015. Available from www.TobaccoInAustralia.org.au. Accessed November 30, 2015. | ||
Australian Institute of Health and Welfare [webpage on the Internet]. Asthma, Chronic Obstructive Pulmonary Disease and Other Respiratory Diseases in Australia. Cat. no. ACM 20. Canberra: AIHW; 2010. Available from: http://www.aihw.gov.au/publications/index.cfm/title/10518. Accessed May 23, 2012. | ||
Burke H, Leonardi-Bee J, Hashim A, et al. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics. 2012;129(4):735–744. | ||
Gilliland FD, Berhane K, Li YF, Rappaport EB, Peters JM. Effects of early onset asthma and in utero exposure to maternal smoking on childhood lung function. Am J Respir Crit Care Med. 2003;167(6):917–924. | ||
Akuete K, Oh SS, Thyne S, et al. Ethnic variability in persistent asthma after in utero tobacco exposure. Pediatrics. 2011;128(3):e623–e630. | ||
Glover M, Kira A, Faletau J. Smoke, smoking and cessation: the views of children with respiratory illness. J Asthma. 2013;50(7):722–728. | ||
Gritz ER, Vidrine DJ, Fingeret MC. Smoking cessation a critical component of medical management in chronic disease populations. Am J Prev Med. 2007;33(6 suppl):S414–S422. | ||
Zwar N, Richmond R, Borland R, et al. Supporting Smoking Cessation: A Guide for Health Professionals. Melbourne: The Royal Australian College of General Practitioners; 2011. | ||
Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service; 2008. | ||
Murray RL, Lewis SA, Coleman T, Britton J, McNeill A. Unplanned attempts to quit smoking: missed opportunities for health promotion? Addiction. 2009;104(11):1901–1909. | ||
Richter KP, Ellerbeck EF. It’s time to change the default for tobacco treatment. Addiction. 2015;110(3):381–386. | ||
Stead LF, Hartmann-Boyce J, Perera R, Lancaster T. Telephone counselling for smoking cessation. Cochrane Database Syst Rev. 2013;8:CD002850. | ||
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev. 2005;(2):CD001292. | ||
Stead LF, Lancaster T. Behavioural interventions as adjuncts to pharmacotherapy for smoking cessation. Cochrane Database Syst Rev. 2012;12:CD009670. | ||
Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J, Lancaster T. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2013;5:CD000165. | ||
Baxi R, Sharma M, Roseby R, et al. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst Rev. 2014;3:CD001746. | ||
Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev. 2005;(2):CD001007. | ||
Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999;106(4):410–416. | ||
Karpinski JP, Timpe EM, Lubsch L. Smoking cessation treatment for adolescents. J Pediatr Pharmacol Ther. 2010;15(4):249–263. | ||
Tonnesen P, Pisinger C, Hvidberg S, et al. Effects of smoking cessation and reduction in asthmatics. Nicotine Tob Res. 2005;7(1):139–148. | ||
West R, Owen L [homepage on the Internet]. Estimates of 52-Week Continuous Abstinence Rates Following Selected Smoking Cessation Interventions in England Version 2. 2012. Available from: www.smokinginengland.info. Accessed November 30, 2015. | ||
Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev. 2011;(2):CD006103. | ||
Hughes JR, Stead LF, Hartmann-Boyce J, Cahill K, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2014;1:CD000031. | ||
Flaherty D, Hoffman-Goetz L, Arocha JF. What is consumer health informatics? A systematic review of published definitions. Inform Health Soc Care. 2015;40(2):91–112. | ||
Shahab L, McEwen A. Online support for smoking cessation: a systematic review of the literature. Addiction. 2009;104(11):1792–1804. | ||
Wolfenden L, Wiggers J, Campbell E, Knight J, Kerridge R, Spigelman A. Providing comprehensive smoking cessation care to surgical patients: the case for computers. Drug Alcohol Rev. 2009;28(1):60–65. | ||
Boyle R, Solberg L, Fiore M. Use of electronic health records to support smoking cessation. Cochrane Database Syst Rev. 2011;(12):CD008743. | ||
Gibbons MC, Wilson RF, Samal L, et al. Impact of consumer health informatics applications. Evid Rep Technol Assess. 2009;(188):1–546. | ||
An LC, Betzner A, Schillo B, et al. The comparative effectiveness of clinic, work-site, phone, and web-based tobacco treatment programs. Nicotine Tob Res. 2010;12(10):989–996. | ||
Civljak M, Stead LF, Hartmann-Boyce J, Sheikh A, Car J. Internet-based interventions for smoking cessation. Cochrane Database Syst Rev. 2013;7:CD007078. | ||
Myung SK, McDonnell DD, Kazinets G, Seo HG, Moskowitz JM. Effects of web- and computer-based smoking cessation programs: meta-analysis of randomized controlled trials. Arch Intern Med. 2009;169(10):929–937. | ||
Krishna S, Boren SA, Balas EA. Healthcare via cell phones: a systematic review. Telemed J E Health. 2009;15(3):231–240. | ||
Ostojic V, Cvoriscec B, Ostojic SB, Reznikoff D, Stipic-Markovic A, Tudjman Z. Improving asthma control through telemedicine: a study of short-message service. Telemed J E Health. 2005;11(1):28–35. | ||
Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control. 2005;14(4):255–261. | ||
Brendryen H, Kraft P. Happy ending: a randomized controlled trial of a digital multi-media smoking cessation intervention. Addiction. 2008;103(3):478–484. | ||
Arrazola RA, Singh T, Corey CG, et al. Tobacco use among middle and high school students – United States, 2011-2014. MMWR Morb Mortal Wkly Rep. 2015;64(14):381–385. | ||
McNeill A, Brose LS, Caldar R, Hitchman SC, Hajek P, McRobbie H. E-Cigarettes: An Evidence Update. A Report Commissioned by Public Health England. 2015. | ||
Polosa R, Morjaria J, Caponnetto P, et al. Effect of smoking abstinence and reduction in asthmatic smokers switching to electronic cigarettes: evidence for harm reversal. Int J Environ Res Public Health. 2014;11(5):4965–4977. | ||
McRobbie H, Bullen C, Hartmann-Boyce J, Hajek P. Electronic cigarettes for smoking cessation and reduction. Cochrane Database Syst Rev. 2014;12:CD010216. | ||
Stead LF, Perera R, Bullen C, Mant D, Lancaster T. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;(1):CD000146. | ||
Centers for Disease Control and Prevention (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease. A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US); 2010. | ||
Make B. Collaborative self-management strategies for patients with respiratory disease. Respir Care. 1994;39(5):566–579. discussion 79–83. | ||
Thomas D, Abramson M, Bonevski B, et al. Integrating smoking cessation into routine care in hospitals – a randomised controlled trial. Addiction. 2016;111(4):714–723. | ||
Grzeskowiak LE, Dekker G, Rivers K, et al. A randomized controlled trial to assess the clinical and cost effectiveness of a nurse-led Antenatal Asthma Management Service in South Australia (AAMS study). BMC Pregnancy Childbirth. 2014;14:9. | ||
Chaudhuri R, Livingston E, McMahon AD, et al. Effects of smoking cessation on lung function and airway inflammation in smokers with asthma. Am J Respir Crit Care Med. 2006;174(2):127–133. | ||
Scanlon PD, Connett JE, Waller LA, et al. Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. The Lung Health Study. Am J Respir Crit Care Med. 2000;161(2 pt 1):381–390. | ||
Tashkin D, Kanner R, Bailey W, et al. Smoking cessation in patients with chronic obstructive pulmonary disease: a double-blind, placebo-controlled, randomised trial. Lancet. 2001;357(9268):1571–1575. | ||
Al-sheyab N, Gallagher R, Crisp J, Shah S. Peer-led education for adolescents with asthma in Jordan: a cluster-randomized controlled trial. Pediatrics. 2012;129(1):e106–e112. | ||
Davis LJ Jr, Hurt RD, Offord KP, Lauger GG, Morse RM, Bruce BK. Self-administered Nicotine-Dependence Scale (SANDS): item selection, reliability estimation, and initial validation. J Clin Psychol. 1994;50(6):918–930. | ||
Shah S, Peat JK, Mazurski EJ, et al. Effect of peer led programme for asthma education in adolescents: cluster randomised controlled trial. BMJ. 2001;322(7286):583–585. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.