")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Smoking Cessation Beliefs Among Saudi University Students in Qassim Region, Saudi Arabia
Authors Almogbel Y
Received 8 May 2020
Accepted for publication 21 July 2020
Published 13 August 2020 Volume 2020:13 Pages 1123—1134
DOI https://doi.org/10.2147/RMHP.S261506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Marco Carotenuto
Yasser Almogbel
Department of Pharmacy Practice, College of Pharmacy, Qassim University, Buraidah, Qassim 51452, Saudi Arabia
Correspondence: Yasser Almogbel P. O. Box 6800, Department of Pharmacy Practice
College of Pharmacy, Qassim University, Buraidah, Qassim 51452, Saudi Arabia
Tel +966 16 3014601
Email [email protected]
Introduction: Despite Saudi officials initiating a variety of smoking cessation programs, smoking in the country has not decreased. Thus, the objective of this study was to identify the factors associated with Saudi students’ beliefs about available smoking cessation interventions.
Methods: A cross-sectional, pre-tested, and validated paper-based survey was administered to a cohort from a university in the Qassim region. Bivariate analyses and logistic regression were conducted to explore the factors associated with the students’ beliefs regarding behavioral and pharmacotherapy interventions for smoking cessation.
Results: Out of 1158 surveys distributed, 958 responses were received (82.7% response rate). Students aged > 23 years were more likely to believe in a behavioral intervention (marginal effect = 10.4%; 95% CI, 2.3%– 18.6%). However, the respondents who indicated that they had smoked a hookah over the past 30 days were less likely to believe in either the pharmacotherapeutic (marginal effect = -7.9%; 95% CI, − 15.6 to − 0.3%) or the behavioral (marginal effect = -8.1%; 95% CI, − 16.2% to − 0.1%) interventions. Students who believed that the hookah was the same as or less harmful than cigarettes (marginal effect = − 25.6%; 95% CI, − 34.7% to − 16.6%) and (marginal effect = − 12.3%; 95% CI, − 22.3% to − 2.3%), respectively, were less likely to believe in pharmacotherapeutic interventions. Multiple logistic regression analyses found that hookah smokers with a willingness to quit smoking were more likely to believe in the effectiveness of cessation medications (marginal effect = 42.9%; 95% CI, 28.2%– 57.6%) and behavioral interventions (marginal effect = 28.6%; 95% CI, 9.3%– 48.0%).
Conclusion: This study found that smoking a hookah and its harmfulness were negatively associated with smoking cessation medications interventions. Regarding beliefs about behavioral interventions, while age was positively associated, hookah smoking and its harmfulness had a negative association. Willingness to quit smoking was positively associated with both medication and behavioral interventions.
Keywords: behavior, college students, Kingdom of Saudi Arabia, quitting smoking, utilization of services
Introduction
In 2015, the World Health Organization (WHO) estimated that about 20% of the world’s population aged 15 years or older could be considered current smokers.1 Smoking kills more than eight million people every year,2 and exposure to secondhand smoke causes over 600,000 deaths annually.3 Additionally, a considerable number of preventable diseases and deaths are caused by tobacco.4 Life expectancy for regular smokers is at least 7 to 13 years shorter than for nonsmokers.5 Although smoking is known to have a negative impact on health, the prevalence of smoking and tobacco consumption is still high in many countries,6 and tobacco consumption using cigarettes and hookah continues to rise.7 Premature deaths due to tobacco smoking increase the economic burden on families and healthcare systems, as well as affecting a country’s overall economy.8
Since hookahs have been in use for about 400 years in a variety of regions, they have many names in different languages, including hubble-bubble, water pipes, nargeela, argeela, arghileh, shisha, okka, kalian, and gouza.9 The availability and accessibility of hookahs during familial and social gatherings actively increased its spread throughout societies.9 Smokers mistakenly perceived hookahs to be less addictive than cigarettes.10 Hookah smoke contains nicotine and other toxins such as tar and carbon monoxide (CO) connected to smoking-related diseases.11 In fact, one session smoking a hookah would expose the smoker to higher amounts of nicotine, tar, and other toxins than smoking one cigarette.12
Saudi Arabia, which is considered a high-income country, was found to have had a significant increase in smoking consumption between 1980 and 2012.13 Although the country does not produce tobacco, it is one of the top importers of tobacco products.14 Between 2010 and 2014, it imported tobacco products worth more than US$3.4 billion.15 The WHO reported that the adjusted crude prevalence in both sexes in Saudi Arabia was 15.9% (with lower and upper limits of 11% and 20.9%, respectively).1 Different studies have reported on the prevalence of hookah smoking among Saudis. This variation may have been affected by the different types of sampling based on characteristics such as age, gender, and/or level of social acceptance among different parts of the population. A study conducted in 2010 of 500 male students from three colleges in the eastern region found that 12.6% of the sample were hookah smokers.16 Another study conducted in 2011 with male Saudi university students found that about 40% of the respondents had tried water pipes at least once.17 A study conducted in 2016 on male university students in Qassim found that 32.9% were shisha smokers.18 Heavy smoking was found to be responsible for 28,000 premature deaths, and cost around US$20 billion (excluding smuggled products) between 2001 and 2010.19 This is despite the Islamic religion prohibiting any act, behavior, or practice that could affect health, including smoking;20 and the fact that at the social level, smoking is considered a shameful behavior, especially for females.20,21 Over the last 30 years, Saudi Arabia has launched several policies to decrease the consumption of tobacco, including increasing the price of tobacco in June 2017, banning smoking, and declaring smoke-free zones in government service office locations, educational institutions, and places of public gathering such as malls and parks.22–24 The government of Saudi Arabia also initiated nonprofit government tobacco cessation centers to run programs that would help smokers quit.22
Despite old and new treatments being applied, the failure to quit smoking has persisted, and the physiological withdrawal symptoms due to dependence on and craving for nicotine might be a significant reason for relapse.25 A pilot study conducted among adult smokers in the United States found that 80% had tried to quit without professional intervention, but only about 10% succeeded.26 In previously published studies, the reasons given for failing to quit included stress in daily life, inability to control withdrawal, and the belief that quitting had no value.27 It has been found that the life expectancy of tobacco smokers who quit smoking before the age of 30 was similar to those who had never smoked.28
Smoking cessation guidelines advocate strategies ranging from medical treatment to behavioral interventions,29 which can be categorized as (1) pharmacological interventions, or (2) behavioral (physiological) interventions.30 Pharmacological interventions can be further divided into nicotine replacement therapy, nicotinic receptor agonists, Varenicline, and antidepressants.31,32 Physiological interventions include educational programs for smoking cessation.33 Studies in the literature have revealed that advice and psychological support for tobacco smokers from healthcare providers would increase levels of cessation.34
Performing an action or the intention to perform an action (eg utilization of smoking cessation interventions) starts with a behavioral belief about the effect (effectiveness of smoking cessation intervention services). The health belief model (HBM) was developed to explain health-related behaviors and the uptake of healthcare services.35,36 The HBM states that prior to engaged in a behavior, it is mandatory to have a belief about the value of this behavior, such as the use of smoking cessation intervention services.36 Furthermore, in the theory of planned behavior (TPB), belief is the starting point for forming an attitude, followed by the intention to perform a behavior.36,37 The first of two studies to evaluate smoking interventions was conducted in 2010 among adult smokers from China, found that they had limited beliefs regarding behavioral and pharmacological interventions.38 The second study, performed in 2013 among Jordanian adults, reported that males were more likely to believe in the effectiveness of pharmacotherapy for smoking cessation. However, older respondents did not believe in the effectiveness of the medication and behavioral interventions for smoking cessation.39 Furthermore, respondents whose father was a smoker were less likely to believe in the behavioral interventions; and males who used other forms of tobacco were less likely to believe in the effectiveness of pharmacotherapy interventions.
The objectives of this study were to explore the beliefs of Saudi students in the Qassim region about the effectiveness of smoking cessation medications and behavioral interventions currently available, and to understand the factors that influence smokers’ beliefs about such services. The perspectives of young adults, especially smokers, are crucial for designing and tailoring effective interventions to meet the needs of smokers to succeed in quitting smoking.
Methods
Study Design and Data Sources
A cross-sectional cohort study was conducted to explore factors affecting beliefs about hookah smoking cessation interventions using a paper-based survey. Data were collected between November 2018 and April 2019 at a higher education institute in Qassim province.
Participants
The research was conducted in colleges that agreed to participate, including health sciences, humanities, and social science colleges. All colleges in the Saudi educational system admit students after they have completed their secondary school degree (18 years and above).
Each of the participating teaching faculties were asked to distribute the survey and consent forms to students and to allot 20 minutes for students to complete the survey. Participation was anonymous and voluntary. Each student was asked to drop the completed survey in a box; they were allowed to stop at any time without providing a reason.
Survey Design
This study was conducted using a pre-tested, validated, paper-based survey that was used previously in two studies.38–41 The back-translation method was used by two independent translators for translating the survey, which was developed initially in English.40,42 Two public health specialists checked the survey. Furthermore, an interview was conducted with five students and they were asked to think aloud to check the clarity and understandability of the survey. Before distributing the survey, reliability was tested with ten students using test–retest reliability and allowing two weeks between the two tests (r = 0.92).
Variables
Outcome variables
Several variables were included in this study. Two main dependent variables regarding beliefs were measured: (1) smoking cessation medications and (2) behavioral interventions. Both were measured as a dichotomous variable (believe about the effect = 1, do not believe about the effect = 0). The question that was asked was “Which of the following strategies would be effective in helping you or others quit smoking?”
Independent Variables
The covariates considered included demographics, academic performance, current hookah smokers, harmful effects of the hookah, and social acceptance. These variables were selected from a 44-question survey. In the first section, a question was asked, please specify socio-demographic information for the following (1) age, (2) gender, and (3) monthly income. Age was collected as a continuous variable that was subcategorized into two groups (18–23 and >23 years). The reason for subcategorization was to evaluate whether being an overaged student had an effect on the student’s beliefs. Gender was categorized into male or female. Details of income were collected and then divided into two categories based on regular Saudi students’ financial aid (Saudi riyals 990/month = US$264/month) to assess the effect of receiving more money than students on financial aid. Also, participants were asked to indicate their marital status with four responses choices (married, single, divorced, or widowed). The marital status covariate was recoded to married and non-married (single, divorced, or widowed) because some response choices were not chosen. Academic performance was ascertained by asking the students to report the grade they had most frequently received during their education, with two possible responses: excellent to good and poor to fail. Current hookah smokers were defined as those who had smoked a hookahs one or more times within the past 30 days, and the answer choice was yes or no. Harmfulness of smoking hookah was assessed as: “Do you think the hookah is harmful?” with the responses being that it is less harmful than cigarettes, or the same or more harmful than cigarettes. Students were asked to assess social acceptability: “What is the social acceptability of using hookah among your peers,” and the response was none, low, medium, or high. One question asked smokers about their willingness to quit smoking; the response was yes or no—another question asked how often they smoked a hookah (three days or less, or more than three days). Finally, they were asked whether or not they own a hookah.
Statistical Analysis
Descriptive statistics and chi-square analyses were performed to explore the frequencies and associations between the dependent and independent variables. All covariates with a p-value ≤0.2 in the chi-square analysis were included in the multiple logistic regression to control for covariates that are not statistically significant.43 Also, age and income were added for their importance as well as indicators of face validity.44 Both inferential statistics (bivariate and multiple logistic regression) were conducted twice for each intervention. Thereafter, a simple logistic regression was conducted for a subset of the sample (hookah smokers). All data collected were coded and entered using Microsoft Excel 2016, and statistical analyses were performed using Stata 16.
Results
Out of the 1158 surveys distributed, 958 were received, for a response rate of 82.7%. The mean age of the participants was 22.1 ± 2.5 years. About 20% of the respondents reported that they had smoked a hookah within the past 30 days. The average age of the participants when they starting hookah smoking was 16.9 ± 4.4 years.
Descriptive statistics were calculated for the smoking cessation medication cohort and the behavioral intervention cohort. Participants were grouped into two age categories (Tables 1 and 2). In both cohorts, around 78% of the respondents were in the 18–23 age group. Moreover, ≈95%, of the sample were unmarried, ≈96% had an income of more than US$264/month, ≈95% had good to excellent academic performance, and ≈80% were not hookah smokers. Furthermore, ≈70% of the respondents thought that hookah smoking was less harmful than cigarette smoking. When asked to assess the social acceptability of hookah smoking, ≈46% of the students answered “none” suggesting that hookah smoking is not socially acceptable.
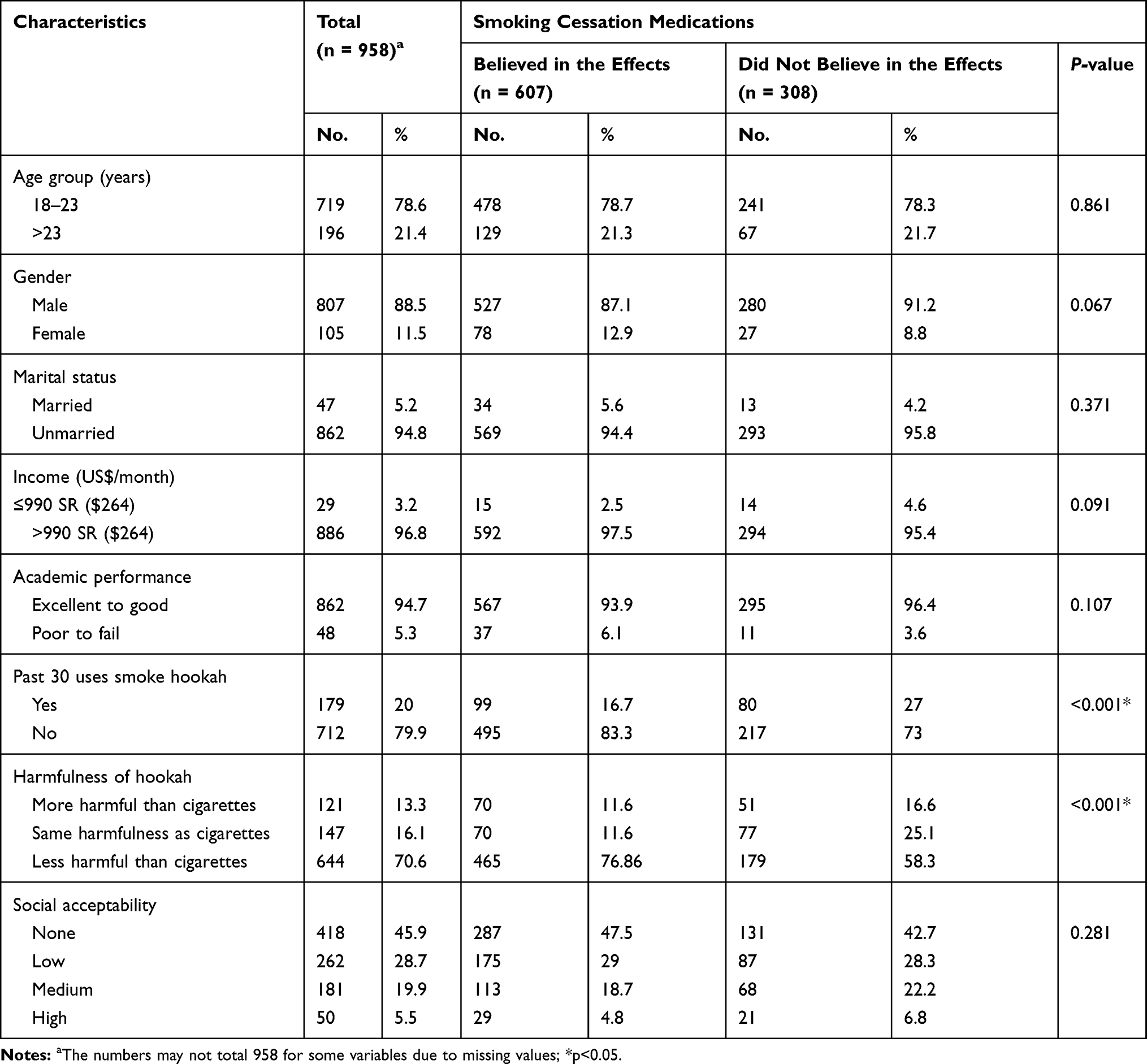 |
Table 1 Demographic Characteristics and Bivariate Analysis of Factors Associated with Beliefs Among College Students in Saudi Arabia About Using Cessation Medications in the Qassim Region |
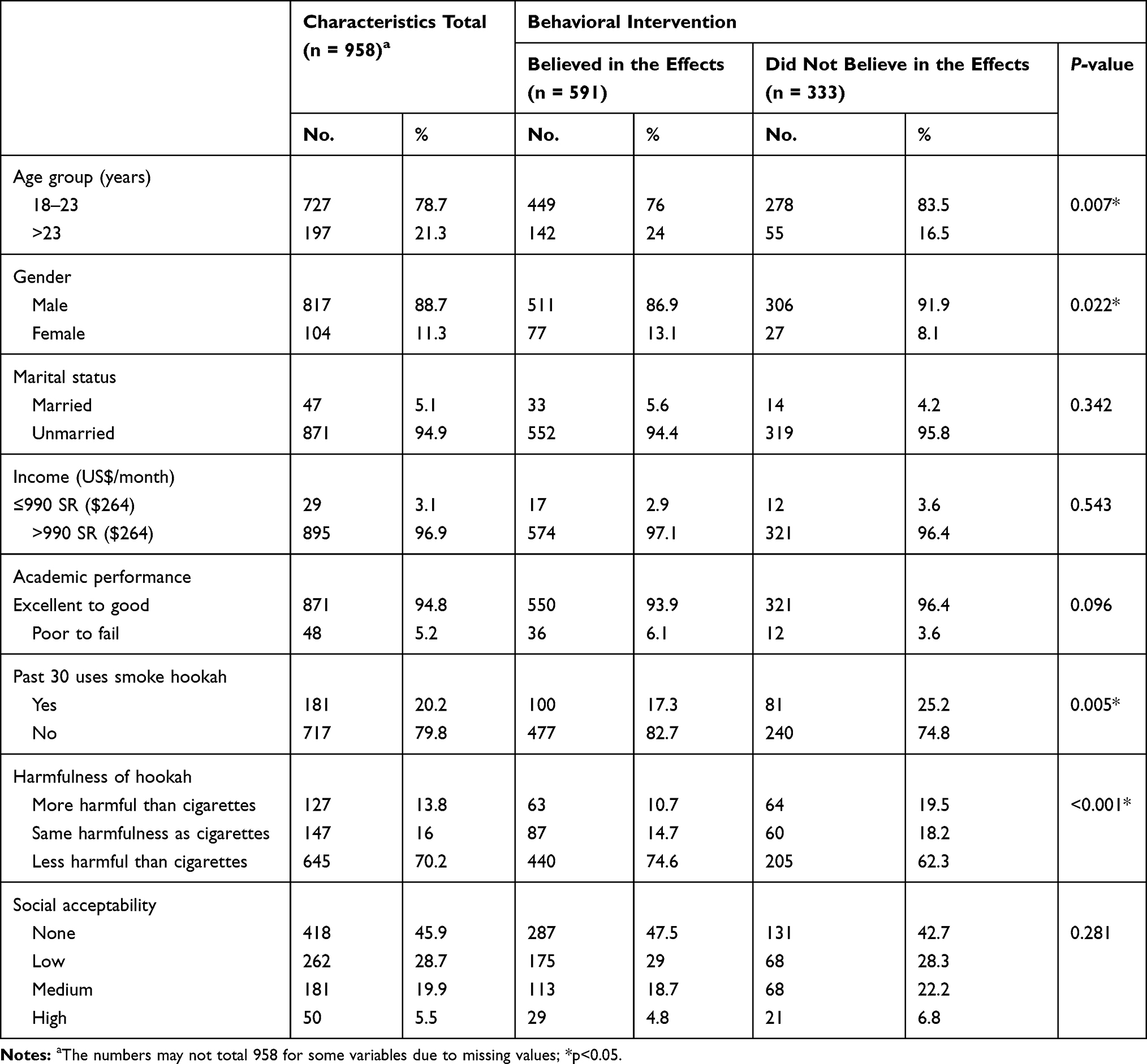 |
Table 2 Demographic Characteristics and Bivariate Analysis of Factors Associated with Beliefs Among College Students in Saudi Arabia About Using Behavioral Interventions in the Qassim Region |
The results of the bivariate analyses of the demographic covariates (eg age, gender, income) as well as the other smoking-related variables are shown in Tables 1 and 2. Table 1 shows the association between these variables and participants’ belief in the effectiveness of the medication intervention for smoking cessation. The demographic covariates did not show any significant association with their beliefs regarding the medication intervention. A significantly greater number of participants who believed in the effectiveness of the medication intervention did not smoke a hookah (p <0.001). However, the belief in the harmful effects of smoking a hookah was significant, with most of the respondents who believed in the effectiveness of the smoking cessation medication intervention indicating that they believe that hookah smoking was less harmful than cigarette smoking (p < 0.001).
Table 2 shows the bivariate analysis results based on participants’ beliefs in the effectiveness of behavioral interventions. There was a significantly greater number of students in the 18–23 age group (p = 0.007) viewing the behavioral intervention favorably. While gender did not have a significant association with beliefs regarding medication cessation, more males believed in the effectiveness of the behavioral interventions (p = 0.022). There was a significantly greater number of hookah nonsmokers who believed in the effectiveness of behavioral interventions (p = 0.005). Moreover, students who believe in the effects of a behavioral intervention also tended to think of hookah smoking as less harmful than cigarettes (p < 0.001).
Two multiple logistic regression analyses were conducted: one for smoking cessation medication (Table 3) and one for behavioral intervention (Table 4). In Table 3, the total sample size excluding missing values was 878 students. Smoking a hookah within the past 30 days was associated with less likelihood of believing in the effectiveness of smoking cessation medication interventions (marginal effect = -7.9%; 95% CI, −15.6 to −0.3%). In addition, respondents who thought that hookahs are the same as or less harmful than cigarettes were less likely to believe in the effects of medication interventions compared to the reference group respondents (more harmful than cigarettes), (marginal effect = -25.6%; 95% CI, −34.7% to −16.6%) and (marginal effect = -12.3%; 95% CI, −22.3% to −2.3%), respectively. The Hosmer−Lemeshow goodness of fit test was conducted to identify the model fit and it indicated a good fit for the model (p = 0.370).
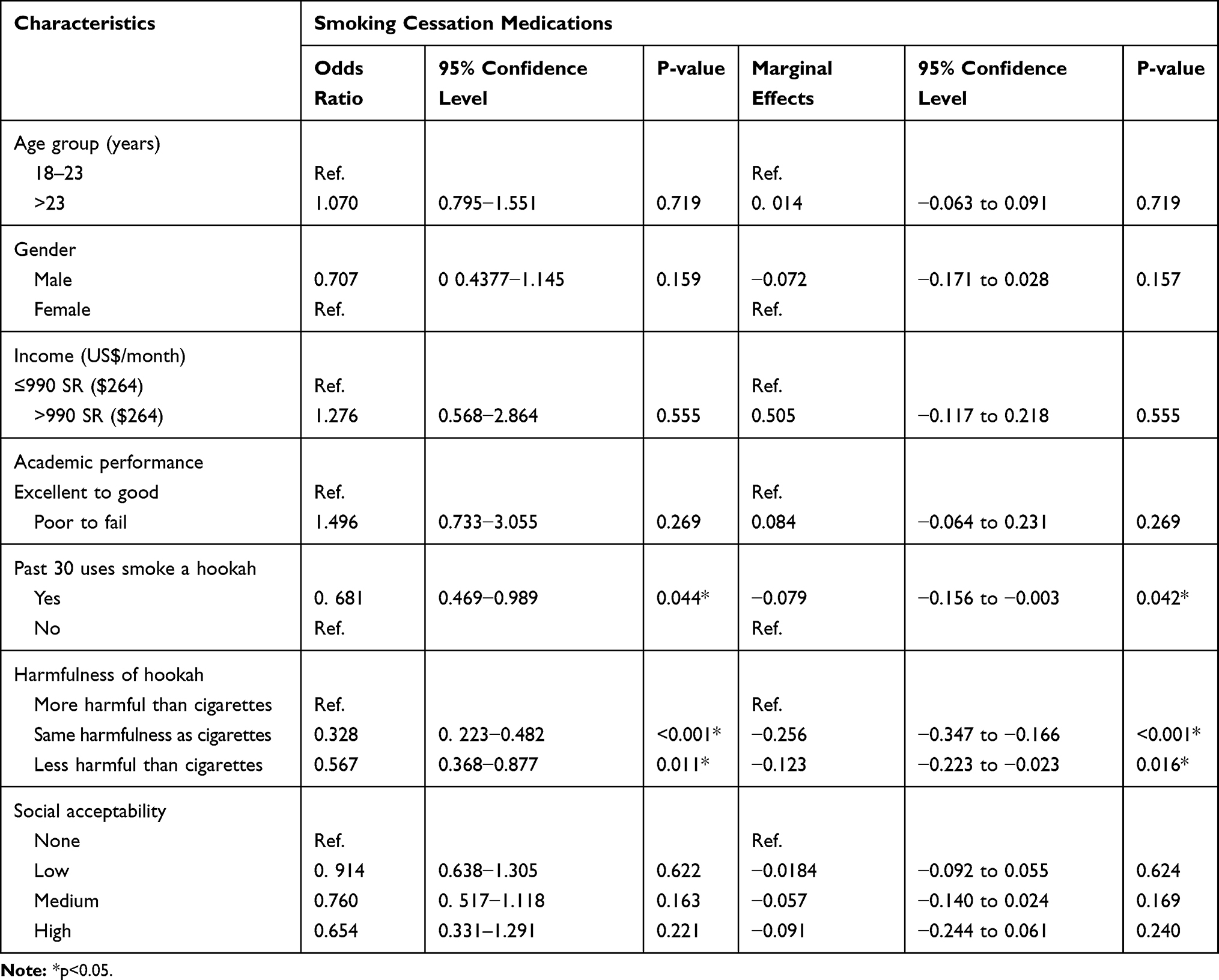 |
Table 3 Multiple Logistic Regression Results of Factors Associated with Beliefs Among College Students in Saudi Arabia About Using Cessation Medications in the Qassim Region (n=878) |
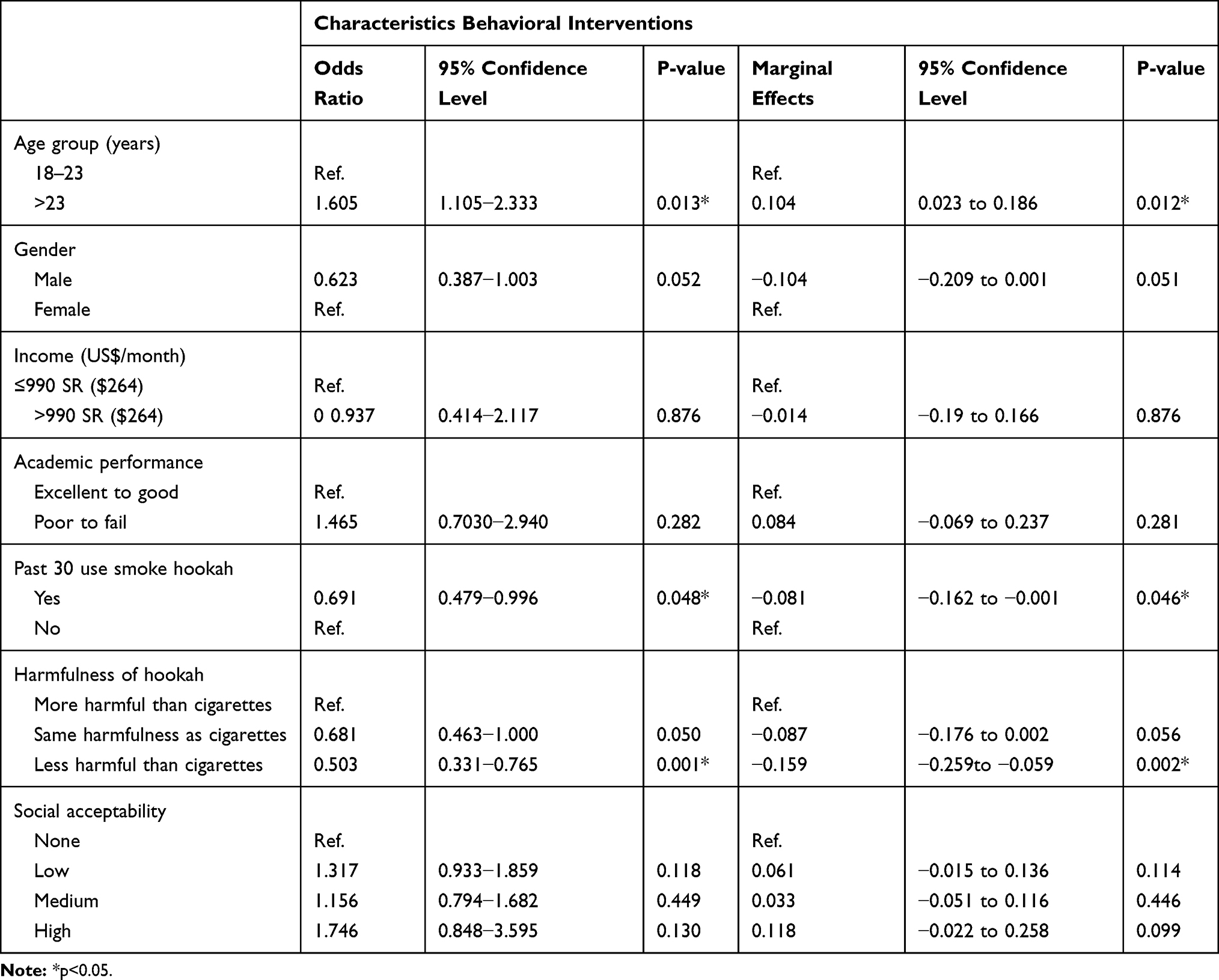 |
Table 4 Multiple Logistic Regression Results of Factors Associated with Beliefs Among College Students in Saudi Arabia About Using Behavioral Interventions in the Qassim Region (N=885) |
Table 4 shows the results of the multiple logistic regression on the factors associated with beliefs in the behavioral intervention. This analysis included 885 participants. Students aged >23 years were 10.4% more likely to believe in the effectiveness of a behavioral intervention (marginal effect = 10.4%; 95% CI, 2.3%–18.6%). Smoking a hookah within the past 30 days was associated with less likelihood of believing in behavioral interventions (marginal effect = -8.1%; 95% CI, −16.2% to −0.1%). Furthermore, students who thought that hookahs were less harmful than cigarettes were less likely to believe in the positive effects of behavioral interventions (marginal effect = −15.9%; 95% CI, −25.9% to −5.9%). Regarding model fit, the Hosmer−Lemeshow goodness of fit test showed the model fit the data well (p = 0.274).
A third multiple logistic regression was conducted for the 70 participants who indicated that they were hookah smokers to explore factors associated with their beliefs regarding medication interventions (Table 5). Those with a willingness to quit smoking a hookah were more likely to believe in smoking cessation medications (marginal effect = 42.9%; 95% CI, 28.2%–57.6%). The Hosmer–Lemeshow goodness of fit test for this model showed the model fit the data well (p = 0.1210).
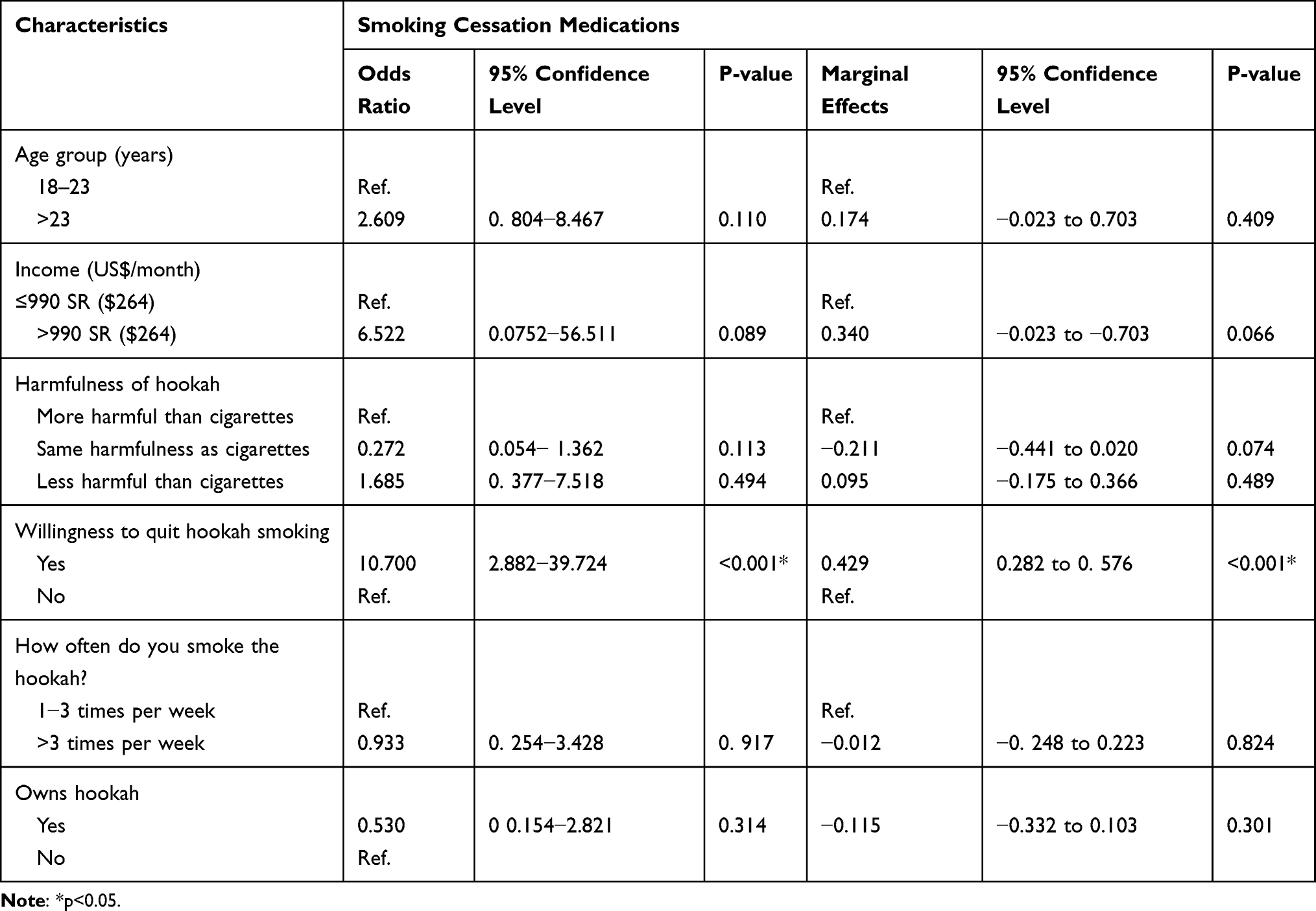 |
Table 5 Multiple Logistic Regression Results of Factors Associated with Beliefs Among Smoking College Students in Saudi Arabia Regarding the Use of Cessation Medications in the Qassim Region (n=70) |
Table 6 shows the last multiple logistic regression performed for factors associated with beliefs among smokers about behavioral interventions. When the same independent variable was tested on the sample sub-population (hookah smokers) to evaluate its association with the behavioral intervention, a significant positive association was found. Students who were more willing to quit smoking a hookah were more likely to believe in a behavioral intervention (marginal effect = 28.6%; 95% CI, 9.3%–48.0%). The Hosmer–Lemeshow goodness of fit test reflected that this model fit the data well (p = 0.1142).
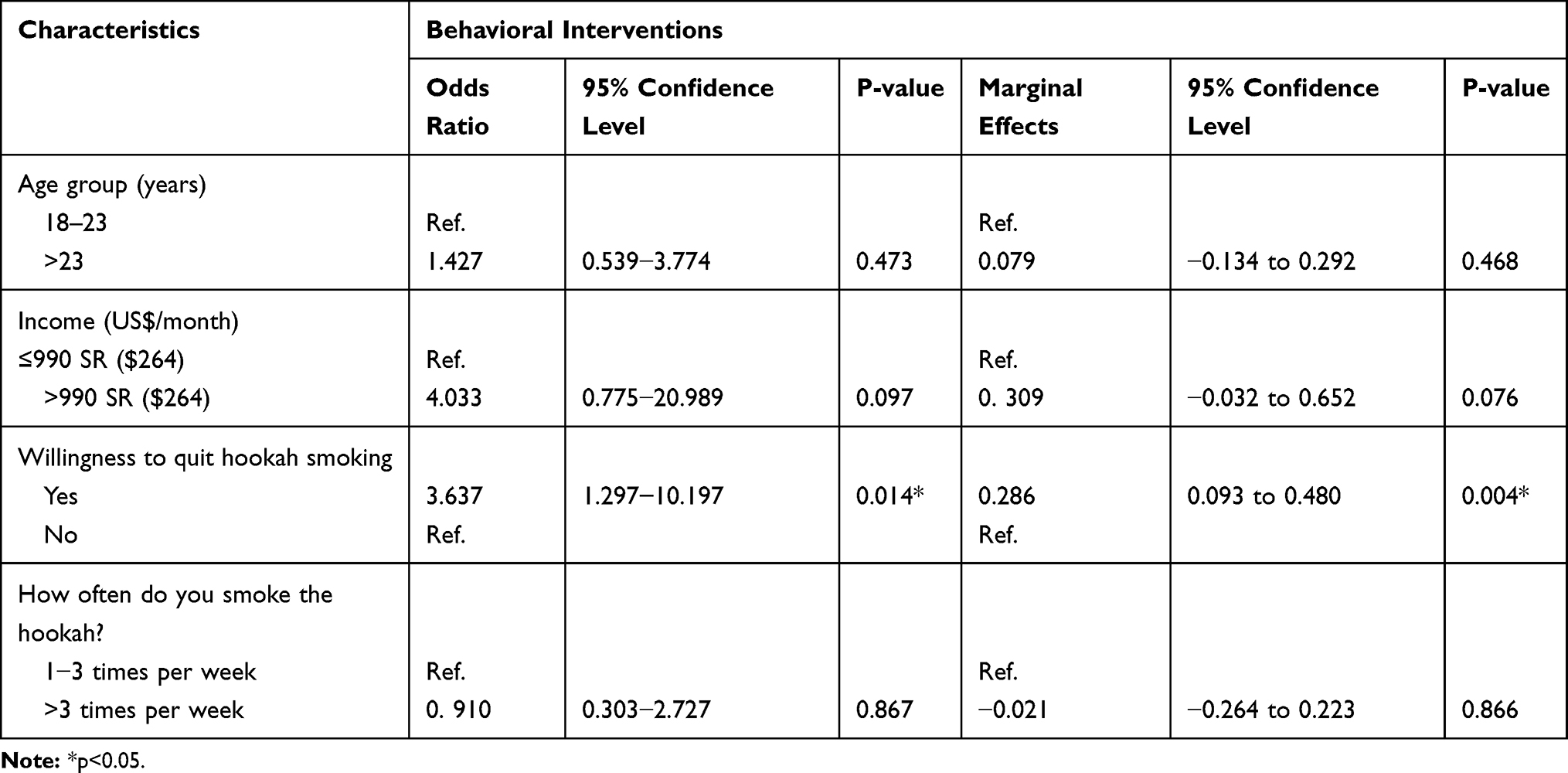 |
Table 6 Multiple Logistic Regression Results of Factors Associated with Beliefs Among College Smokers Students in Saudi Arabia Using Behavioral Interventions in the Qassim Region (n=78) |
Discussion
This study explored the beliefs about using either cessation medications or behavioral interventions to quit smoking a hookah. The multiple logistic regression models included both hookah smokers and nonsmokers. Negative associations were found between smoking a hookah, opinion of its harmfulness and both interventions. Conversely, a positive association was found between the respondent’s age and their belief in behavioral interventions. Another multiple logistic regression found statistically significant positive associations between respondents’ willingness to quit smoking and their belief in the effectiveness of both cessation medications and behavioral interventions.
This sample prevalence did not match other reported studies, particularly the two that were conducted with Saudi college students in the Qassim region.17,18 This lack of concordance could be related to a convenience sampling technique that was used for data collection. However, the current sample included twice the number of respondents as the prior two studies, both males and females, and was representative of more colleges. Thus, this study is more representative and generalizable for Saudi university students in the Qassim province compared to the previous studies.
In this study, there was a significant association between increasing age and beliefs in the effectiveness of behavioral interventions. Middle-aged individuals were more willing to attend an educational health session and a nonmandatory annual health checkup than younger participants.45 Thus, middle-aged adults would be less likely to engage in risky behaviors than younger adults. In addition to smoking and drinking alcohol, risky activities include sunbathing without sunscreen, driving without wearing a seat belt, and engaging in unprotected sex.46 This highlights that as age increases, respondents’ awareness and concern about their health increases. However, no association was found between age and belief in the effectiveness of smoking cessation medications. In two studies, conducted in Jordan and China, researchers found that smokers age was negatively associated with beliefs about both medication and behavioral interventions. Those studies only selected smokers older than the participants in the current study which may explain the reasoning behind this belief.38,39 A study conducted in 2007 on Native Americans regarding beliefs about smoking cessation found that most respondents had a negative attitude toward smoking cessation pharmacotherapy. This included fear of side effects, suspicion about the effects of such medications, and displeasure with using medications in general.47 In the current study, the average age difference was very slight (mean = 22 ± 2.2) because this study was conducted among college students (studying for their bachelor’s degrees). This might have resulted in a more narrow view of the association between age-related beliefs about medication and how it varies with age.
In addition, hookah smokers were less likely to believe in the effectiveness of both interventions. It could be assumed that they continue to smoke due to the effects of addiction, lack of willpower, and force of habit.48 It is known that quitting smoking can be difficult because of the addictive effect of nicotine.49 A pilot study conducted with 26 smokers in the United States found that most smokers who had tried to quit smoking without professional help had failed.26 It is likely that hookah smokers who are addicted to nicotine will not be willing to quit.39 A subgroup analysis was performed with only the hookah smokers and found that only those smokers who were willing to quit had positive beliefs about the effects of the two interventions. Perceived causes are crucial because they influence the desire to seek treatment.50 In contrast, in a Canadian study of youths showed that even those who were interested in quitting may have had negative beliefs about cessation programs.51
Furthermore, a negative association was found between participants who thought that hookahs are less harmful than cigarettes and a belief in the effectiveness of behavioral interventions. Some studies have found that hookah smokers thought the waterpipe was less harmful than cigarettes because of the filtering by bubbling in the water.52 It has been found that hookahs contain significant levels of tar, nicotine, and heavy metals.53,54 Participants who did not believe in the effects of behavioral interventions also thought that the hookah was less harmful than cigarettes, which implies that respondents who were aware of their risk were less likely to believe in smoking cessation interventions.
This study had some limitations. First, because a convenience sampling method was used, the possible influence of non-respondents on our study could not be detected. Second, because generalizability is restricted to a similar population, a cross-sectional analysis may raise questions about the causality, but not the associations among variables. Third, even though the identity of the student respondents was protected, they may not have revealed their smoking status for social or religious reasons.20,21 Thus, the percentage of hookah smokers may be vulnerable to errors. Fourth, this study included 44 questions and was collected using a paper-based method. Thus, missing values may have affected the collected survey responses, especially at the end of the survey.
This study shed light on the importance of population beliefs, especially smokers, regarding smoking cessation interventions. Saudi Arabia is one of the top ten importers and consumers of tobacco worldwide,14 and deaths caused by smoking negatively affect the country’s economy.8 Despite the negative effects on health, the prevalence of smoking is still high and continues to increase.6,7 Saudi Arabia has lost 28,000 of its citizens through premature death and incurred costs of around US$20 billion between 2001 and 2010 owing to the smoking of tobacco.19 If the smoking cessation services are not used, the cost of providing free smoking cessation services will be added to costs with no value. Hence, belief is of crucial importance to facilitate usage based on the HBM and TPB.
Conclusion
This study identified factors associated with belief in the effectiveness of cessation medications or behavioral interventions for quitting hookah smoking. A significant predictor of beliefs in the effectiveness of smoking cessation medications is being a hookah smoker and belief in the harmfulness of hookahs. For behavioral interventions, increasing age was positively associated with behavioral interventions. In contrast, factors negatively associated with beliefs in behavioral interventions are being a current hookah smoker and belief in the harmfulness of hookahs. Willingness to quit smoking positively influenced belief in both cessation medications and behavioral interventions. Conducting behavioral studies is crucially important to increase the use of free health services, consequently improving health and decreasing the economic burden on individuals, society, and the government.
Abbreviations
HBM, health belief model; TPB, theory of planned behavior.
Ethical Approval
The study was approved by the Subcommittee of Health Research Ethics at the Deanship of Scientific Research at Qassim University (number: 13518). Furthermore, this study was performed according to the Declaration of Helsinki.
Acknowledgment
The researcher would like to thank the Deanship of Scientific Research, Qassim University for funding publication of this project.
Disclosure
The author reports no funding and no conflicts of interest in this work.
References
1. World Health Organization. WHO global report on trends in prevalence of tobacco smoking 2000–2025. Geneva: World Health Organization; 2018. Available from: https://www.who.int/tobacco/publications/surveillance/trends-tobacco-smoking-second-edition/en/.
2. World Health Organization. Tobacco Key Facts. Geneva: World Health Organization; 2019. Available from https://www.who.int/news-room/fact-sheets/detail/tobacco.
3. Öberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A. Worldwide burden of disease from exposure to secondhand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377(9760):139–146. doi:10.1016/S0140-6736(10)61388-8
4. Drope J, Schluger NW. The Tobacco Atlas.
5. Brønnum-Hansen H, Juel K. Abstention from smoking extends life and compresses morbidity: a population based study of health expectancy among smokers and never smokers in Denmark. Tob Control. 2001;10(3):273–278. doi:10.1136/tc.10.3.273
6. Abughosh S, Wu IH, Hawari F, et al. Cigarette smoking among Jordanian adults. J Ethn Subst Abuse. 2012;11(2):101–112. doi:10.1080/15332640.2012.674888
7. Noonan D, Kulbok PA. New tobacco trends: waterpipe (hookah) smoking and implications for healthcare providers. J Am Acad Nurse Pract. 2009;21(5):258–260. doi:10.1111/j.1745-7599.2009.00402.x
8. Thun M, Peto R, Boreham J, Lopez AD. Stages of the cigarette epidemic on entering its second century. Tob Control. 2012;21(2):96–101. doi:10.1136/tobaccocontrol-2011-050294
9. Aljarrah K, Ababneh ZQ, Al-Delaimy WK. Perceptions of hookah smoking harmfulness: predictors and characteristics among current hookah users. Tob Induc Dis. 2009;5(1):16. doi:10.1186/1617-9625-5-16
10. Akl EA, Gunukula SK, Aleem S, et al. The prevalence of waterpipe tobacco smoking among the general and specific populations: a systematic review. BMC Public Health. 2011;11(1):244. doi:10.1186/1471-2458-11-244
11. Ramôa CP, Shihadeh A, Salman R, Eissenberg T. Group waterpipe tobacco smoking increases smoke toxicant concentration. Nicotine Tobacco Res. 2016;18(5):770–776. doi:10.1093/ntr/ntv271
12. Primack BA, Carroll MV, Weiss PM, et al. Systematic review and meta-analysis of inhaled toxicants from waterpipe and cigarette smoking. Public Health Rep. 2016;131(1):76–85. doi:10.1177/003335491613100114
13. Ng M, Freeman MK, Fleming TD, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. JAMA. 2014;311(2):183–192. doi:10.1001/jama.2013.284692
14. Mackay J, Eriksen M. The Tobacco Atlas. Geneva: World Health Organization; 2002.
15. Taha SM KSA imports tobacco products worth SR13 billion in 4 years. Arab News. August 12, 2014:16.
16. Taha AZ, Sabra AA, Al-Mustafa ZZ, Al-Awami HR, Al-Khalaf MA, Al-Momen MM. Water pipe (shisha) smoking among male students of medical colleges in the eastern region of Saudi Arabia. Ann Saudi Med. 2010;30(3):222–226. doi:10.4103/0256-4947.62838
17. Alzohairy MA. Water pipe & cigarette smoking among Qassim University male students: prevalence and beliefs. Int J Health Sci (Qassim). 2012;6(1):45–57. doi:10.12816/0005972
18. Muzammil A, Asmari DS, Al Rethaiaa AS, et al. Prevalence and perception of shisha smoking among university students: a cross-sectional study. J Int Soc Prev Community Dent. 2019;9(3):275–281. doi:10.4103/jispcd.JISPCD_407_18
19. AlBedah AM, Khalil MK. The economic costs of tobacco consumption in the Kingdom of Saudi Arabia. Tob Control. 2014;23(5):434–436. doi:10.1136/tobaccocontrol-2012-050665
20. Almutairi KM. Smoking among Saudi students: a review of risk factors and early intentions of smoking. J Community Health. 2014;39(5):901–907. doi:10.1007/s10900-014-9909-8
21. Jarallah JS, Al-Rubeaan KA, Al-Nuaim ARA, Al-Ruhaily AA, Kalantan KA. Prevalence and determinants of smoking in three regions of Saudi Arabia. Tob Control. 1999;8(1):53–56. doi:10.1136/tc.8.1.53
22. Alrabah M, Gamaleddin I, Allohidan F. International approaches to tobacco-use cessation programs and policy for adolescents and young adults in Saudi Arabia. Curr Addict Rep. 2018;5(1):65–71. doi:10.1007/s40429-018-0188-9
23. Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: findings from a national survey. BMC Public Health. 2015;15(1):611. doi:10.1186/s12889-015-1902-3
24. Alotaibi SA, Alsuliman MA, Durgampudi PK. Smoking tobacco prevalence among college students in the Kingdom of Saudi Arabia: systematic review and meta-analysis. Tob Induc Dis. 2019;17:35. doi:10.18332/tid/105843
25. Schuck K, Otten R, Engels RC, Kleinjan M. The relative role of nicotine dependence and smoking-related cognitions in adolescents’ process of smoking cessation. Psychol Health. 2011;26(10):1310–1326. doi:10.1080/08870446.2010.520715
26. Lenert L, Muñoz RF, Stoddard J, et al. Design and pilot evaluation of an internet smoking cessation program. J Am Med Inform Assoc. 2003;10(1):16–20. doi:10.1197/jamia.M1128
27. Hawari F, Obeidat N, Beano H, Dawahrah S, Al-Rimawi D, Ghonimat I. Smoking abstinence rates and reasons for failure to quit smoking in cancer patients in Jordan. Respiration. 2012;83(3):233–238. doi:10.1159/000328759
28. Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328(7455):1519. doi:10.1136/bmj.38142.554479.AE
29. Roberts NJ, Kerr SM, Smith SM. Behavioral interventions associated with smoking cessation in the treatment of tobacco use. Health Serv Insights. 2013;6:79–85. doi:10.4137/HSI.S11092
30. Arndt S, Turvey C, Flaum M. Addictive disorders. Psychiatric Serv. 2002;53:1176–1178. doi:10.1176/appi.ps.53.9.1176
31. Liu JA. A revolutionary approach for the cessation of smoking. Sci China Life Sci. 2010;53(5):631–632. doi:10.1007/s11427-010-0107-3
32. Jiménez-Ruiz C, Berlin I, Hering T. Varenicline: a novel pharmacotherapy for smoking cessation. Drugs. 2009;69(10):1319–1338. doi:10.2165/00003495-200969100-00003
33. Murthy P, Subodh BN. Current developments in behavioral interventions for tobacco cessation. Curr Opin Psychiatry. 2010;23(2):151–156. doi:10.1097/YCO.0b013e328336653f
34. Lancaster T, Silagy C, Fowler G. Training health professionals in smoking cessation. Cochrane Database Syst Rev. 2000;(3):CD000214.
35. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
36. Glanz K, Rimer BK, Viswanath K, eds. Health Behavior and Health Education: Theory, Research, and Practice.
37. Ajzen I. The theory of planned behavior. Organ Behav Human Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
38. Yu Y, Yang M, Sansgiry S, Essien E, Abughosh S. Beliefs in effectiveness of various smoking cessation interventions among Chinese adult smokers. Epidemiol. 2011;1(106):1161–2165. doi:10.4172/2161-1165.1000106
39. Abughosh S, Hawari F, Essien EJ, Peters RJ, Wu I-H. Beliefs in various smoking cessation interventions among Jordanian adult smokers. J Behav Health. 2013;2(3):213–222. doi:10.5455/jbh.20130403104936
40. Abughosh S, Wu IH, Rajan S, Peters RJ, Essien EJ. Waterpipe smoking among students in one US university: predictors of an intention to quit. J Am Coll Health. 2012;60(7):528–535. doi:10.1080/07448481.2012.718018
41. Abughosh S, Yang M, Wu IH, Hawari F, Peters RJ, Essien EJ. Waterpipe smoking among Jordanian adults: predictors and correlates. J Behav Health. 2012;1(1):7–15. doi:10.5455/jbh.20120313034424
42. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. doi:10.1177/135910457000100301
43. Maldonado G, Greenland S. Simulation study of confounder-selection strategies. Am J Epidemiol. 1993;138(11):923–936. doi:10.1093/oxfordjournals.aje.a116813
44. Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE. Regression Methods in Biostatistics: Linear, Logistic, Survival, and Repeated Measures Models. Springer Science & Business Media; 2011:140–141.
45. Deeks A, Lombard C, Michelmore J, Teede H. The effects of gender and age on health related behaviors. BMC Public Health. 2009;9(1):213. doi:10.1186/1471-2458-9-213
46. Rolison JJ, Hanoch Y, Wood S, Liu PJ. Risk-taking differences across the adult life span: a question of age and domain. J Gerontol B Psychol Sci Soc Sci. 2014;69(6):870–880. doi:10.1093/geronb/gbt081
47. Burgess D, Fu SS, Joseph AM, Hatsukami DK, Solomon J, van Ryn M. Beliefs and experiences regarding smoking cessation among American Indians. Nicotine Tob Res. 2007;9(Suppl_1):S19–S28. doi:10.1080/14622200601083426
48. Hughes JR. Smokers’ beliefs about the inability to stop smoking. Addict Behav. 2009;34(12):1005–1009. doi:10.1016/j.addbeh.2009.06.013
49. Abdullah A, Husten C. Promotion of smoking cessation in developing countries: a framework for urgent public health interventions. Thorax. 2004;59(7):623–630. doi:10.1136/thx.2003.018820
50. Peele S. Diseasing of America: Addiction Treatment Out of Control. Lexington, MA: Lexington Books; 1989.
51. Leatherdale ST, McDonald PW. Youth smokers’ beliefs about different cessation approaches: are we providing cessation interventions they never intend to use? Cancer Causes Control. 2007;18(7):783–791. doi:10.1007/s10552-007-9022-8
52. Kiter G, Uçan ES, Ceylan E, Kilinç O. Water-pipe smoking and pulmonary functions. Respir Med. 2000;94(9):891–894. doi:10.1053/rmed.2000.0859
53. Shihadeh A. Investigation of mainstream smoke aerosol of the argileh water pipe. Food Chem Toxicol. 2003;41(1):143–152. doi:10.1016/S0278-6915(02)00220-X
54. Shihadeh A, Saleh R. Polycyclic aromatic hydrocarbons, carbon monoxide, “tar,” and nicotine in the mainstream smoke aerosol of the narghile water pipe. Food Chem Toxicol. 2005;43(5):655–666. doi:10.1016/j.fct.2004.12.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.