")
Back to Journals » Cancer Management and Research » Volume 13
Sleep Quality and Related Factors in Patients with Breast Cancer: A Cross-Sectional Study in Taiwan
Authors Weng YP, Hong RM, Chen VCH, Tsai CJ, Yeh DC, Fang YH
Received 22 January 2021
Accepted for publication 24 May 2021
Published 14 June 2021 Volume 2021:13 Pages 4725—4733
DOI https://doi.org/10.2147/CMAR.S302966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Yi-Ping Weng,1,2 Rei-Mei Hong,2 Vincent Chin-Hung Chen,3,4 Chia-Jui Tsai,5,6 Dah-Cherng Yeh,7 Yu-Hung Fang8
1Department of Nursing, Chia-Yi Chang Gung Memorial Hospital, Chiayi branch, Puzi City, Chiayi County, Taiwan, R.O.C; 2Department of Nursing, Chia-Yi Chang Gung University of Science and Technology, Chiayi branch, Puzi City, Chiayi County, Taiwan, R.O.C; 3Department of Psychiatry, Chang Gung Medical Foundation, Chang Gung Memorial Hospital, Chiayi branch, Puzi City, Chiayi County, Taiwan, R.O.C; 4School of Medicine, Chang Gung University, Taoyuan City, Taiwan, R.O.C; 5Department of Psychiatry, Taichung Veterans General Hospital, Taichung, Taiwan, R.O.C; 6Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan, R.O.C; 7Breast Medical Center, Cheng Ching Hospital, Chung Kang Branch, Taichung City, Taiwan, R.O.C; 8Division of Thoracic Oncology, Department of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Chiayi branch, Puzi City, Chiayi County, 61363, Taiwan, R.O.C
Correspondence: Yu-Hung Fang
Division of Thoracic Oncology, Department of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Chiayi branch, No.6, W. Sec., Jiapu Rd, Puzi City, Chiayi County, 61363, Taiwan, R.O.C
Tel +886-5-362-1000 ext. 2762
Fax +886-5-362-3005
Email [email protected]
Background: Sleep disturbances are common and symptomatic burden in patients with breast cancer, but they are poorly documented and managed in routine clinical practice. This descriptive and cross-sectional study evaluated factors associated with post-treatment sleep disturbances in patients with breast cancer.
Patients and Methods: Patients with breast cancer who underwent standard treatment were enrolled and surveyed for their basic demographic data and precancerous and cancer treatment-related factors; they were also administered self-report questionnaires including the Family Adaptation, Partnership, Growth, Affection, Resolve questionnaire; Impact of Event Scale; Center for Epidemiologic Studies Depression Scale; and Maudsley Personality Inventory. Their sleep disturbances were evaluated using the Pittsburgh sleep quality index (PSQI). Independent sample t test and chi-square tests were used to compare the variables between patients with or without sleep disturbance, and multivariate logistic regression analyses were conducted to detect the independent factors.
Results: In total, 448 patients, including 145 with PSQI ≤ 5 and 303 with PSQI > 5, completed the investigation. Multiple logistic regression analysis revealed that significantly more patients with sleep disturbances demonstrated psychological distress, severe pain, depression, and impact of stress events than patients without sleep disturbances (adjusted odds ratios [95% confidence intervals]: 2.83 [1.135– 7.067], P = 0.026; 1.14 [1.023– 1.280], P = 0.018; 1.08 [1.036– 1.133], P < 0.001; and 1.03 [1.002– 1.051], P = 0.037, respectively).
Conclusion: Patients with breast cancer showed 67.6% prevalence of sleep disturbances after treatment. The patients with sleep disturbances were more likely to have previously experienced psychological disturbances, severe pain, depression within 5 years after diagnosis. After diagnosis for more than 5 years, higher distress caused by traumatic events still associated with sleep disturbances.
Keywords: sleep disturbance, breast cancer, depression, pain, post-traumatic stress disorder, symptoms cluster
Introduction
Breast cancer is the second most common cancer and the most common cancer among women in the world.1 In Taiwan, 1 in 120 women have breast cancer, and the incidence is rising.2 In total, 25% of all cancers diagnosed in women are breast cancer.3 The 5-year cancer-specific survival was only 74.0% during 1975–1979, and it increased significantly to 88.5% over 2010–2015.4 However, approximately 15% of overall cancer-related deaths remain attributable to breast cancer.1
During the course of cancer diagnosis and therapy, patients undergo medical and invasive surgical procedures and receive treatments potentially influencing emotional or psychological health including chemotherapy, radiotherapy, and hormone therapy.5 Sleep disturbances are common symptoms in individuals with breast cancer. The incidence varies across studies depending on the study design and assessment methods, but most studies have reported that 60%–90% of patients with breast cancer have sleep disturbances—much higher than that in the healthy population.6–9 Sleep disturbances are classified by the Sleep Disorders Classification Committee of the American Academy of Sleep Medicine into five major categories: insomnia, sleep apnea, hypersomnia of central origin, circadian rhythm sleep disorders, and parasomnias.10 Of these, insomnia is the most common in patients with breast cancer.11 Despite the significant and symptomatic burden, sleep disturbances are poorly documented and managed in routine clinical practice.12
Sleep disturbances worsen quality of life, increase health concerns and cancer recurrence, severe pain, and vasomotor symptoms, and reduce energy.12–14 Symptom clusters, such as depression, anxiety, and cancer-related fatigue, are closely associated with sleep disturbances in patients with breast cancer.13 Hospitalized women with breast cancer and sleep disturbances experience more complications and have longer hospital stays.15 Several studies have also reported that reduced sleep duration is associated with increased breast cancer recurrence, breast cancer-specific mortality, and all-cause mortality risks.16,17 Randomized controlled studies have reported that patients with breast cancer who underwent cognitive behavioral therapy for insomnia demonstrated decreased depression and anxiety levels, alleviated general and clinical fatigue, and improved global quality of life.18,19
In the current study, sleep disturbances prevalence and the related precancerous, psychosocial, and treatment-related factors in patients with breast cancer were assessed to identify independent predictors of sleep disturbances risks. and Methods
Participants
This study was a single-center, descriptive, cross-sectional study conducted at a teaching hospital on outpatients from its breast surgical oncology outpatient department between April 2011 and April 2012. All patients were sampled for histological examination to confirm their breast cancer diagnoses. All patients had undergone conventional cancer treatment including surgery, chemotherapy, target radiotherapy, and hormone therapy according to clinical practice guidelines developed by the multidisciplinary commitment of the hospital.
We included female patients aged >18 years, newly diagnosed as having breast cancer, capable of verbal and written communication, and aware of the research purpose and procedure. All included patients provided written informed consent to undergo the relevant procedures. Patients who could not provide written consent because of reasons such as language barrier, intellectual disabilities, or dementia were excluded from this study.
The current study protocol was approved by the Institutional Review Board of Taichung Veterans General Hospital and conformed to the Helsinki Declaration. Participants were confirmed to have completely understood the researcher identity and research process and purpose before participating in the research. During the data collection process, if participants needed health care or had questions, the researcher agreed to actively provide consultation after data processing. Withdrawal or nonparticipation did not affect the participants’ medical rights. The disclosure of any personal information was strictly prohibited, and the research questionnaire was used for analysis alone.
Data Collection and Questionnaires
Breast cancer patients regular follow up at our breast surgery or oncology outpatient clinics were invited to take part in this study. Research assistants went to the above settings to contact patients after receiving referral from in-charge doctors or case managers. After informed the study procedure and aims, those who signed an informed consent form were enrolled in the study. Research assistants under the supervision of a psychiatrist and clinical psychologists administered these questionnaires. We collected basic patient demographic and individual characteristics including age, education, marital status, career, smoking and drinking habits, diet, and exercise (defined as 3 times a week at least). In addition, their previous medical records were analyzed to assemble precancerous factors; these included menstruation and reproduction history, precancerous breast condition, family history of breast cancer, psychiatric clinic visits, and family history of psychological disorders. Cancer-related factors were also recorded; these included cancer stage and therapy, such as surgery, radiation therapy, chemotherapy, hormone therapy, and target radiotherapy.
We used four questionnaires to evaluate different psychological problems of the patient. The Family Adaptation, Partnership, Growth, Affection, Resolve (APGAR) questionnaire, including five questions, was used to screen out family dysfunctional patients in daily office practice.20,21 Impact of Event Scale (IER-S)—a 22-item self-report measure for subjective distress caused by specific stressors, including the three symptoms of post-traumatic stress disorder (PTSD), namely intrusion, avoidance, and hyperarousal22,23—is commonly used in patients with cancer.24 The Center for Epidemiologic Studies Depression Scale (CES-D) is a widely used self-report questionnaire comprising a 20-item index of depression symptoms associated with depression, such as restless sleep, poor appetite, and feeling lonely. Each item ranges from “0” (never or rarely) to “3” (often) points, and total scores of >20 represent the current depression tendency of a patient.25,26 Maudsley Personality Inventory (MPI) is a questionnaire designed to reflect a constellation of traits including extroversion, psychoticism, or neuroticism.27,28
Here, patients’ sleep quality was assessed using the Pittsburgh sleep quality index (PSQI), which contains 19 questions distributed among seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleeping medication use, and daytime dysfunction. The overall score is between 0 and 21, and PSQI > 5 indicates poor sleep quality.29 In other words, the higher the score, the worse is the sleep quality.
Statistical Analysis
According to the purpose of this study, the data were analyzed using SPSS for Windows version 26.0 (IBM SPSS Inc, Chicago, IL, USA)., including descriptive statistics, independent sample t-test, chi-square test, and logistic regression analysis. We conducted independent sample t-test for continuous variable and chi-square tests for categorical variable to compare the variables between heroin users with and without sleep disturbance. A p-value of less than 0.05 was considered to have statistical significance. We then conducted multivariate logistic regression analyses to detect the independent factors associated with sleep disturbances by including those variables significantly associated with sleep disturbance in the univariate analyses.
Results
Initially, 465 patients with breast cancer in total were screened, but 14 were excluded because they did not meet the inclusion criteria. Thus, 451 were invited to participate in the study. However, of them, one had missing data and two did not fill out the PSQI questionnaire. Finally, the data of 448 women with breast cancer were statistically analyzed further.
Comparison of Demographic and Precancerous Factors
Table 1 indicates sociodemographic and precancerous factors of breast cancer patients with and without sleep disturbances. The univariate analysis using the chi-square test revealed that compared with those with a lower PSQI (≤5), significantly more patients with higher PSQI (>5) tend to have a low education level (high school and below; 60.4% vs 46.2%, P = 0.005), full-time career (60.9% vs 47.6%, P = 0.008), previous experiences with psychological disorders (18.5% vs 4.1%, P < 0.001), more psychiatric clinic visits (12.2% vs 2.1%, P < 0.001), family history of psychological disorders (12.2% vs 2.1%, P < 0.001), and high chronic pain frequency (34.7% vs 19.3%, P < 0.001). There is one missing data in patients with PSQI > 5 on marital status, career and family history of breast cancer.
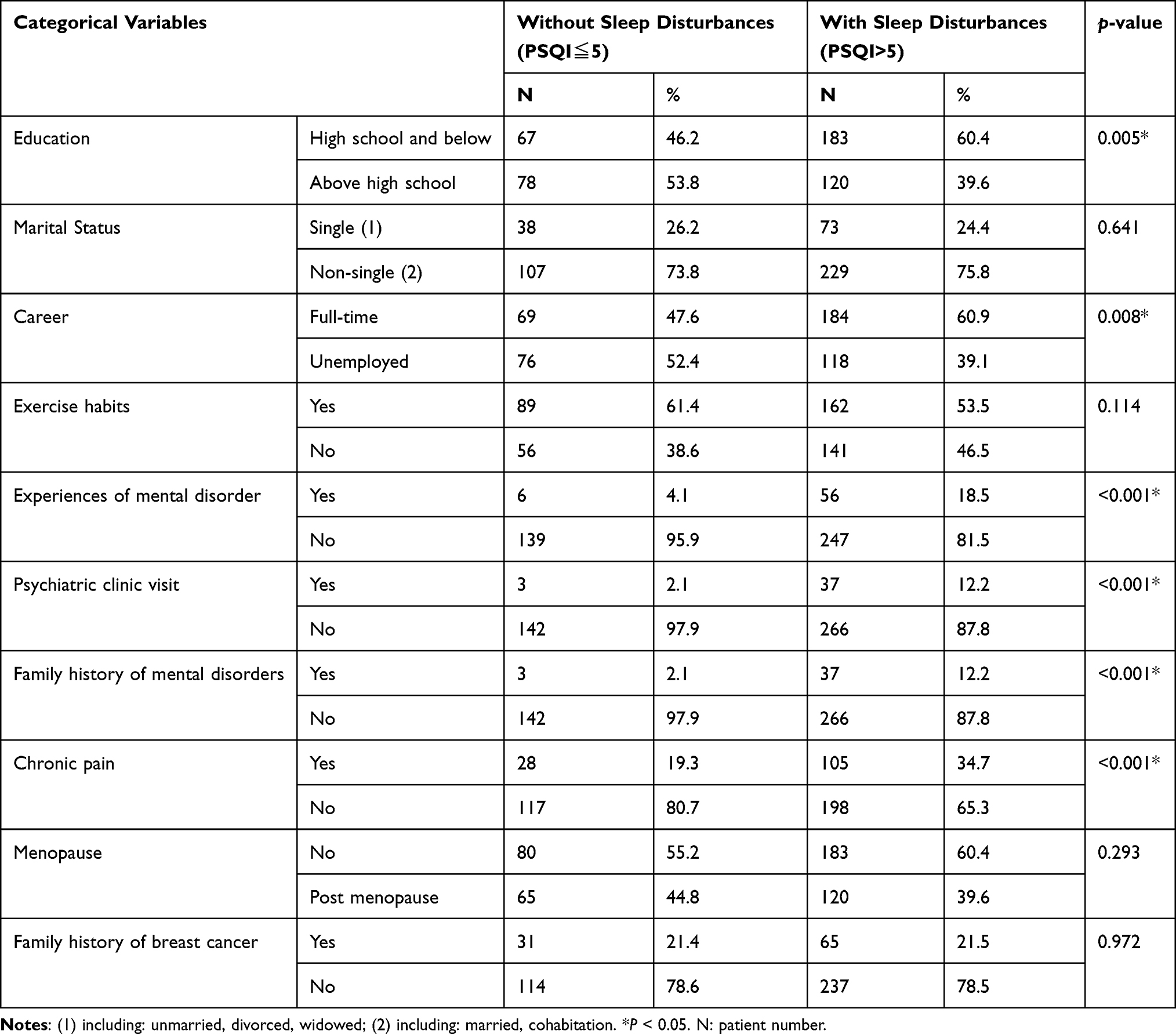 |
Table 1 Chi-Square Test Results for the Sociodemographic and Precancerous Factors of Breast Cancer Patients with and without Sleep Disturbances |
Table 2 presents sociodemographic and psychosocial factors of breast cancer patients with or without sleep disturbance. We used an independent t-test for analysis. No significant differences were observed between patients with PSQI > 5 and ≤ 5 in terms of age, body mass index (BMI), time of breast cancer diagnosis, and age at menopause. Compared with patients with PSQI ≤ 5, patients with PSQI > 5 had more severe pain (1.01 ± 2.05 vs 1.84 ± 2.32) and higher CES-D scores (12.77 ± 5.31 vs 17.62 ± 7.53), IES-R scores (12.18 ± 10.63 vs 21.55 ± 14.48), and MPI scores (12.18 ± 10.63 vs 21.55 ± 14.48; all P < 0.001).
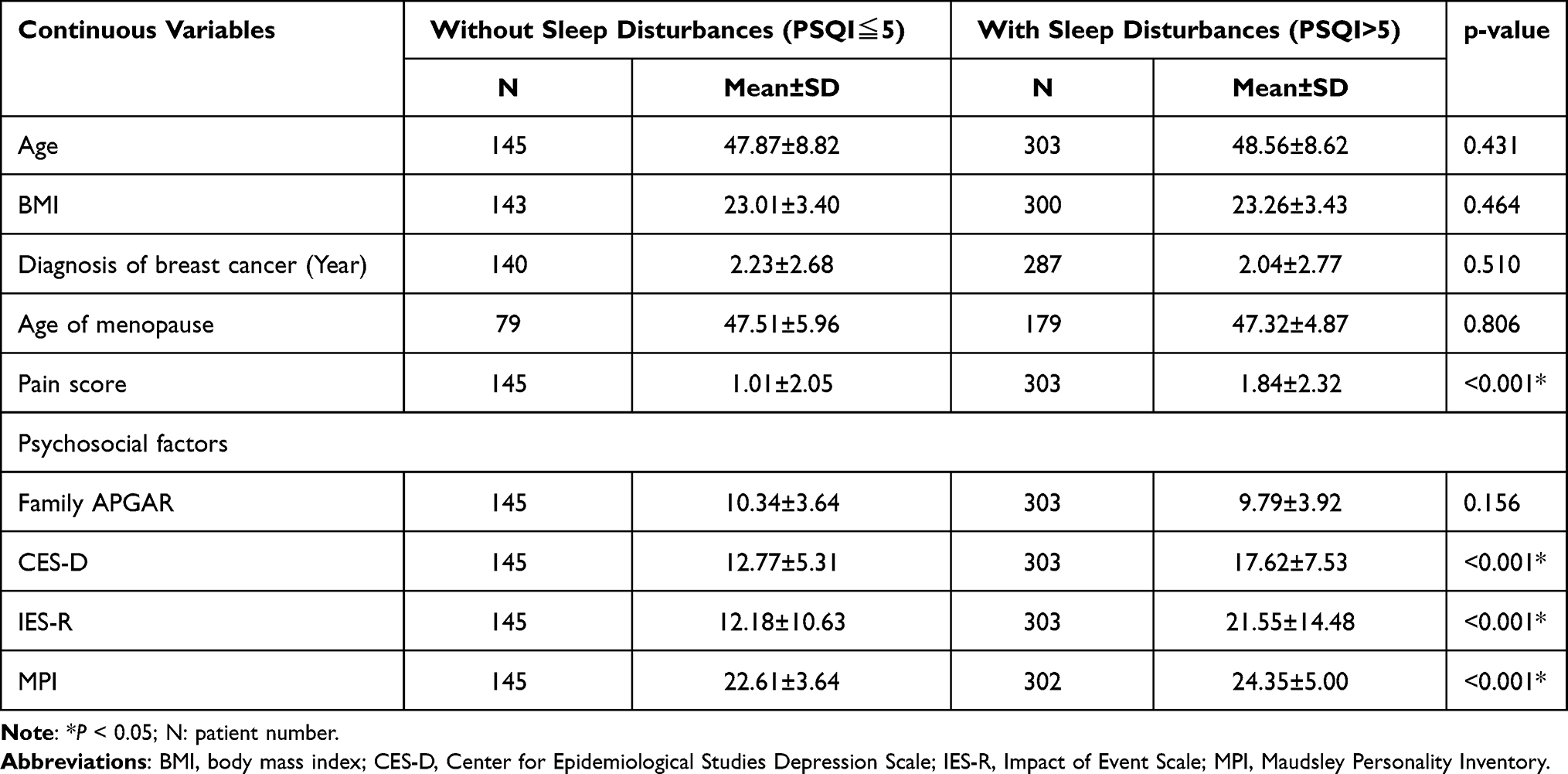 |
Table 2 Independent t-test Results for the Sociodemographic and Precancerous Factors of Breast Cancer Patients with and without Sleep Disturbances |
Comparison of Cancer Treatment and Stage at Diagnosis
Table 3 compares different cancer treatments and stages among our patients. More patients with PSQI > 5 underwent radiotherapy (48.3% vs 59.7%, P = 0.022) than those with PSQI ≤ 5.
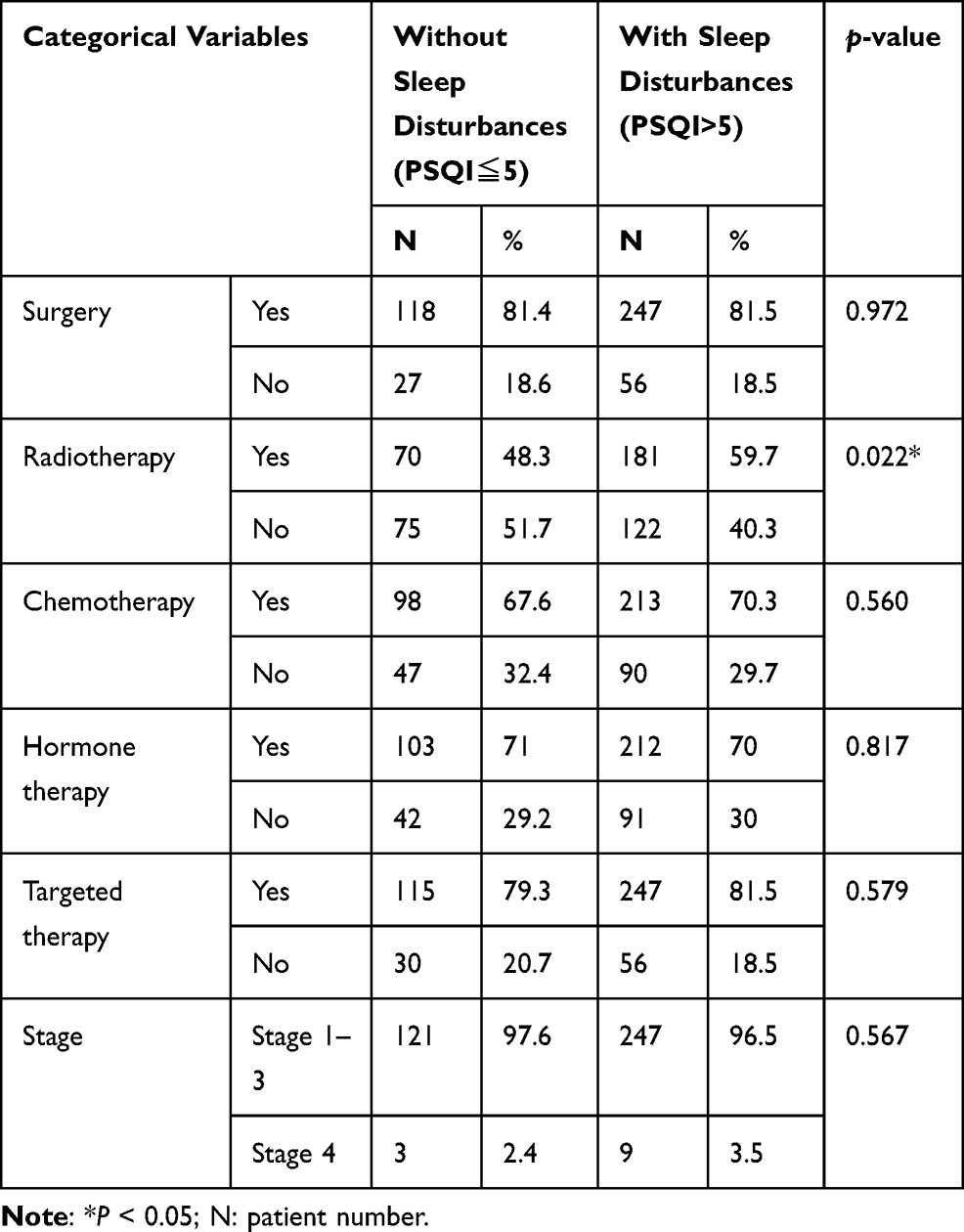 |
Table 3 Chi-Square Test for Treatment Differences Between Breast Cancer Patients with and without Sleep Disturbances |
Multiple Logistic Regression Analysis
We selected variables demonstrating significant between-group differences in the univariate analysis and used them in multiple logistic regression analyses to study the predictors of sleep disturbance in patients with breast cancer. After correcting demographic variables, Table 4 shows that compared with those with PSQI ≤ 5, more patients with PSQI > 5 demonstrated previous experiences of psychological distress, severe pain, high depression scores, and impact of stress events (adjusted odds ratios [95% confidence intervals]: 2.97 [1.185–7.431], P = 0.020; 1.15 [1.024–1.285], P = 0.018; 1.08 [1.035–1.133], P < 0.001; and 1.03 [1.003–1.054], P = 0.027, respectively). Patients received radiotherapy are associated with higher PSQI scores (adjusted odds ratios [95% confidence intervals]: 1.87 [1.194–2.941], P = 0.006).
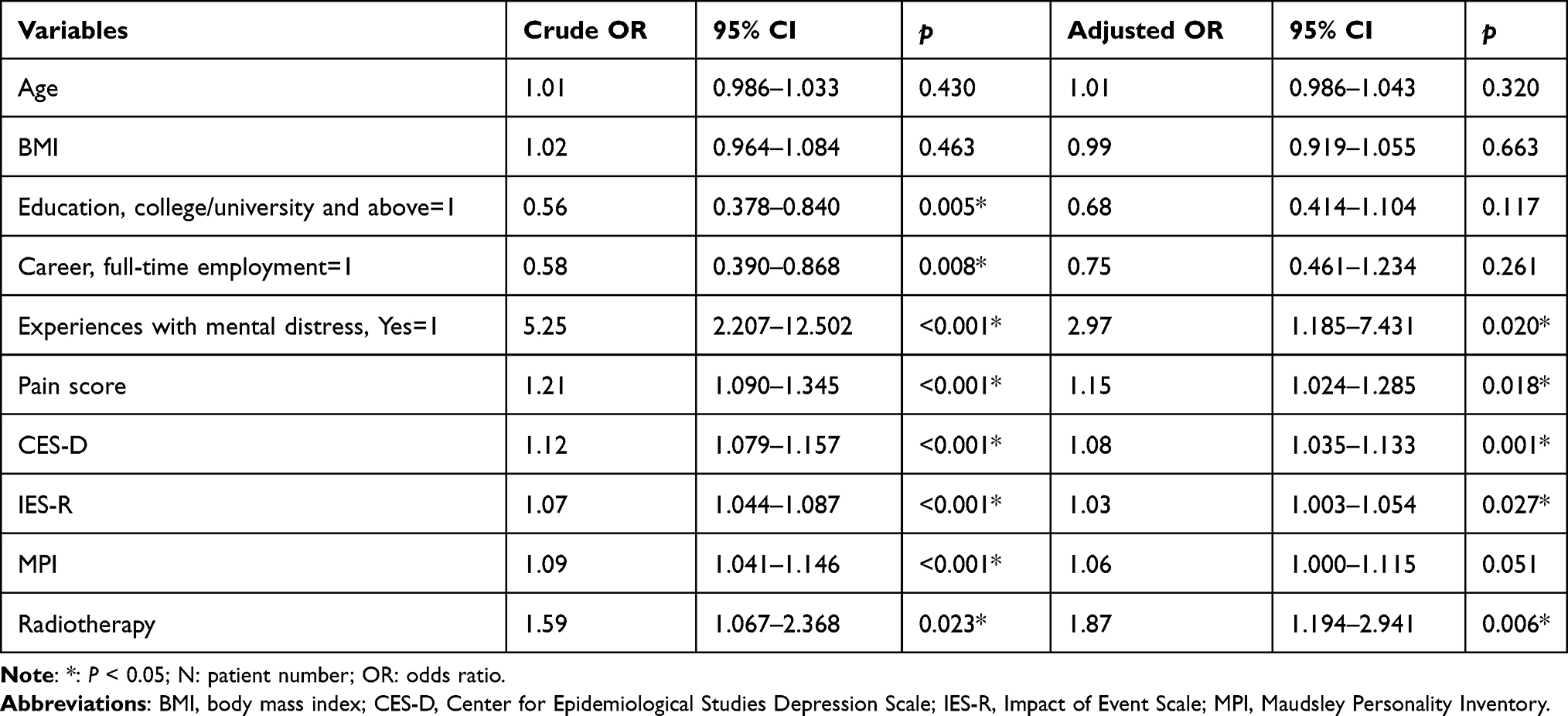 |
Table 4 Multiple Logistic Regression Analysis for Sleep Disorder Predictors in Patients with Breast Cancer |
The impact of age, BMI, education, and career on sleep disturbances remained nonsignificant in this multiple logistic regression analysis. In Table 5, for patients diagnosed with breast cancer within 5 years, independent factors that associated with sleep disturbance including previous experiences of psychological distress, severe pain, high depression scores and received radiotherapy (adjusted odds ratios [95% confidence intervals]: 3.028 [1.105–8.297], P = 0.031; 1.159 [1.022–1.314], P = 0.022; 1.092 [1.039–1.147], P < 0.001; and 1.978 [1.209–3.236], P = 0.007, respectively). After 5 years, only high IES-R scale is independently associated with sleep disturbance. (adjusted odds ratios [95% confidence intervals]: 1.130 [1.021–1.252], P = 0.018)
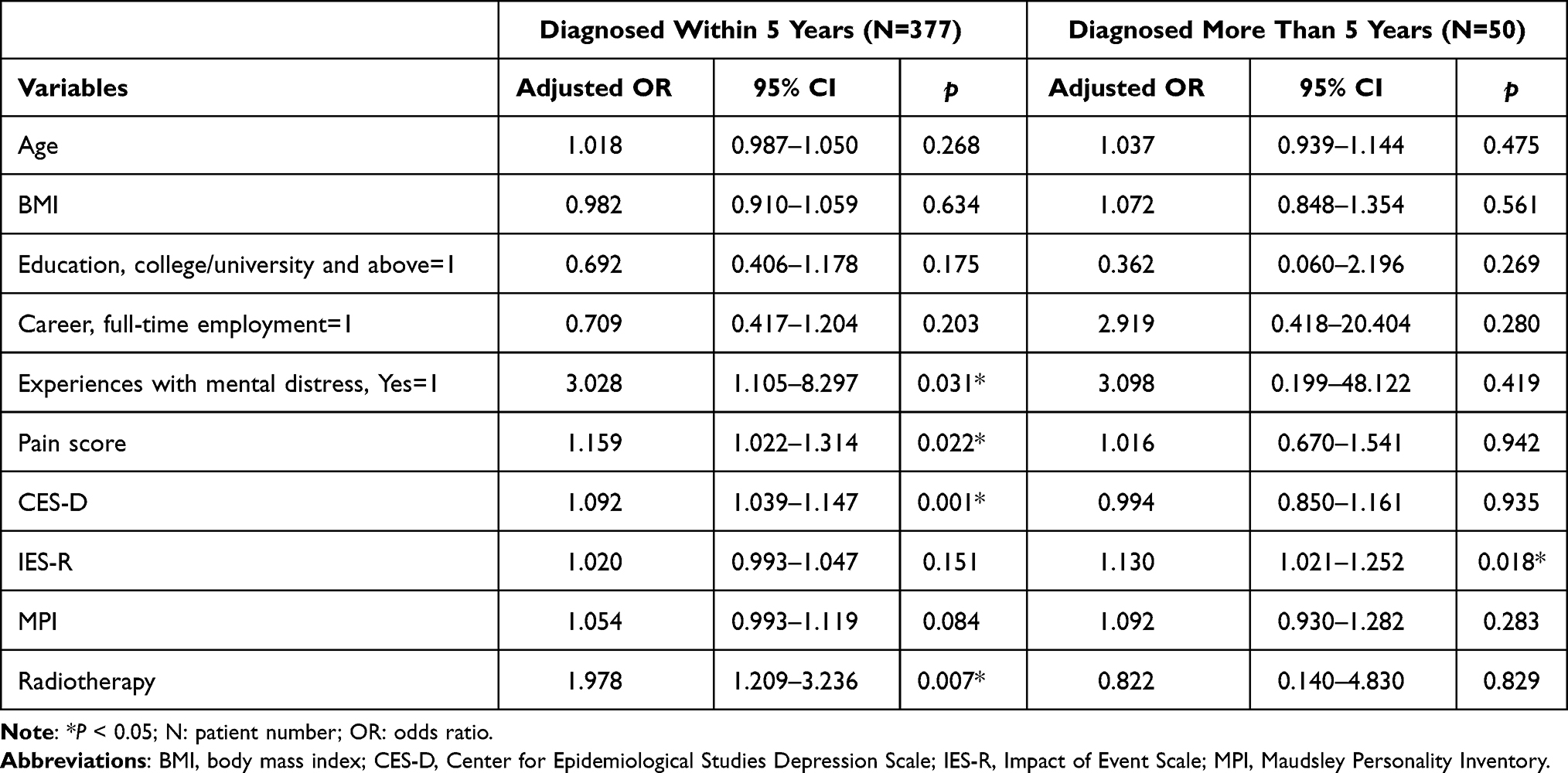 |
Table 5 Multiple Logistic Regression Analysis for Sleep Disturbance in Patients with Breast Cancer Within 5 Years or More Than 5 Years |
Discussion
The present study indicated that patients with breast cancer with more severe post-treatment sleep disturbances were more likely to have previously experienced psychological disorders as well as high pain, CES-D, and IES-R scores. The prevalence of post-treatment sleep disturbances (indicated by a PSQI of >5) in patients with breast cancer was 67.6%, similar to that reported previously—ranging from 60% to 90%.6–9 The differences in precancerous or treatment-related factors between patients with and without sleep disturbances, however, remained nonsignificant in the multivariate analysis.
Pain and depression scores were significantly associated with sleep disturbances, indicating the presence of cluster symptoms after treatment in patients with breast cancer. In an analysis of 200 patients with breast cancer, a low post-treatment PSQI was associated with low quality of life, increased pain, and increased health and recurrence concerns; however, depression was not significantly associated with sleep quality.14 A possible reason for this is that the study enrolled patients after 1–10 years of treatment. Nevertheless, in a cohort study, depression incidence did not differ between the breast cancer and control groups 4 years postoperatively.30 Clinically, during the treatment process of breast cancer, patients may experience several associated side effects, which may contribute to impaired sleep qualities. The cumulative effect of toxic agents may cause nausea, vomiting, anorexia, diarrhea, and fatigue. Radiotherapy may cause skin reactions. Surgical interventions may cause wound pain and changes in body image. Clinicians should thus be familiar with the coexisting symptoms in patients with breast cancer and identify the aggravating or relieving factors to coordinate treatment recommendations by using strategies likely to be beneficial for alleviating a range of symptoms.31
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, to meet the criteria of PTSD, the diagnosis of a life-threatening illness must be “sudden and catastrophic”.32 Breast cancer could be a life-threatening illness to be a major traumatic event. Courses of breast cancer diagnosis and treatment were stressful events that compatible with PTSD criterion A1 to be an index trauma in the development of PTSD. In a meta-analysis, approximately 9.6% of patients with breast cancer who developed PTSD symptoms were young, were non-Caucasian, and had recently completed treatment.33 In another study with 18 patients of breast cancer, the average IES-R score was 19.56 with a standard deviation from the average of 16.85. A cutoff point of 26.6 was used to indicate a powerful effect of traumatic stress on the ability to function. Moreover, IES-R scores are significantly correlated with the HADS-Anxiety, but not HADS-Depression, scores.34 According to our data, higher IES-R scores were strongly associated with poor sleep quality, and the average IES-R score was 21.55 ± 14.48. Chronic stress such as chronic pain has been shown to have diverse and lasting impacts on physical and mental health, and causes PTSD and major depression. PTSD is usually accompanied by other mental health disorders after trauma exposure. Among patients with PTSD, 30% to 50% of them had also major depression disorder. Because of the high prevalence of PTSD and major depression, patients with breast cancer experience both disorders.35 When Patients experienced stress events, sympathetic nervous system is activated and stimulates the inflammatory pathways. For example, our previous study revealed relationships between cytokine levels and depression severity among patients with breast cancers. Specific differential relationships between IL-5 levels and depression severity were found between patients with breast cancer who were receiving and not receiving chemotherapy.36 Furthermore, within a cohort of women who had breast cancer, those who experienced childhood trauma had increased expression of genes associated with inflammation.37 Patients with family history of breast cancer have more anxiety, depression and cancer-specific distress. These psychological distresses had positive correlation with negative coping style and may associate with higher risk of sleep disturbance.38
In multiple logistic regression analysis, patients with sleep disturbance are associated with higher rates of experiences with mental distress. They may search for psychiatric help because higher risk of symptoms including depression, intrusion, avoidance, and hyperarousal. In Taiwan, only psychiatrists can prescribe some specific hypnotic drugs so patients with sleep disturbance need to visit psychiatric clinics.
The present study has several limitations. First, we used cross-sectional design, mainly because we did not have access to longitudinal data. Second, numerous factors not included in this study can also result in sleep disturbances, eg pain control medicines and children or household responsibilities. Moreover, several symptoms such as pain and depression symptoms may gradually subside after treatment. Therefore, based on our cross-sectional analysis, we cannot conclude that only psychological distress, severe pain, high depression scores, and impact of stress events can cause sleep disturbances. Third, patients with extreme symptom burden typically do not agree to provide written informed consent and encounter difficulties in completing questionnaires. The lack of data from patients experiencing severe symptom burden may have caused selection bias. Finally, this study uses questionnaires reported by patients themselves. We had no definitely diagnosis of previous psychological diagnosis or medications, and not recorded causes of pain or pain medications.
Conclusion
Patients with breast cancer demonstrated a high prevalence (67.6%) of post-treatment sleep disturbances. Moreover, the patients with sleep disturbances were more likely to have previously experienced psychological disorders, severe pain, high depression, and radiotherapy within 5 years after diagnosis. After 5 years of diagnosis, high distress caused by traumatic events still associated with sleep disturbances.
Clinical Practice Points
- In patients with breast cancer, the prevalence of post-treatment sleep disturbances (defined as PSQI > 5) is high (67.6%).
- The patients with sleep disturbances were more likely to have previously experienced psychological disturbances, severe pain, depression and received radiotherapy within 5 years after diagnosis. After diagnosis for more than 5 years, higher distress caused by traumatic events still associated with sleep disturbances.
Abbreviations
APGAR, Family Adaptation, Partnership, Growth, Affection, Resolve; IER-S, Impact of Event Scale; CES-D, Center for Epidemiologic Studies Depression Scale; MPI, Maudsley Personality Inventory; PSQI, Pittsburgh sleep quality index; OR, odds ratio.
Acknowledgments
This study was supported by grants from Chang Gung Memorial Hospital, Chiayi, Taiwan (grant number: CMRPG6F0321, CORPG6G0101, CORPG6G0141). The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Momenimovahed Z, Salehiniya H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer. 2019;11:151–164. doi:10.2147/BCTT.S176070
2. Liu FC, Lin HT, Kuo CF, See LC, Chiou MJ, Yu HP. Epidemiology and survival outcome of breast cancer in a nationwide study. Oncotarget. 2017;8(10):16939–16950. doi:10.18632/oncotarget.15207
3. Sun YS, Zhao Z, Yang ZN, et al. Risk factors and preventions of breast cancer. Int J Biol Sci. 2017;13(11):1387–1397. doi:10.7150/ijbs.21635
4. Guo F, Kuo YF, Shih YCT, Giordano SH, Berenson AB. Trends in breast cancer mortality by stage at diagnosis among young women in the United States. Cancer. 2018;124(17):3500–3509. doi:10.1002/cncr.31638
5. Carreira H, Williams R, Muller M, Harewood R, Stanway S, Bhaskaran K. Associations between breast cancer survivorship and adverse mental health outcomes: a systematic Review. J Natl Cancer Inst. 2018;110(12):1311–1327. doi:10.1093/jnci/djy177
6. Otte JL, Davis L, Carpenter JS, et al. Sleep disorders in breast cancer survivors. Support Care Cancer. 2016;24(10):4197–4205. doi:10.1007/s00520-016-3247-6
7. Williams SA, Schreier AM. The role of education in managing fatigue, anxiety, and sleep disorders in women undergoing chemotherapy for breast cancer. Appl Nurs Res. 2005;18(3):138–147. doi:10.1016/j.apnr.2004.08.005
8. Jacob L, Scholten PC, Kostev K, Kalder M. Association between sleep disorders and the presence of breast cancer metastases in gynecological practices in Germany: a case-control study of 11,412 women. Breast Cancer Res Treat. 2018;171(2):443–448. doi:10.1007/s10549-018-4831-x
9. Tag Eldin ES, Younis SG, Aziz L, Eldin AT, Erfan ST. Evaluation of sleep pattern disorders in breast cancer patients receiving adjuvant treatment (chemotherapy and/or radiotherapy) using polysomnography. J BUON. 2019;24(2):529–534.
10. Thorpy MJ. Classification of sleep disorders. Neurotherapeutics. 2012;9(4):687–701. doi:10.1007/s13311-012-0145-6
11. Fiorentino L, Ancoli-Israel S. Insomnia and its treatment in women with breast cancer. Sleep Med Rev. 2006;10(6):419–429. doi:10.1016/j.smrv.2006.03.005
12. Fakih R, Rahal M, Hilal L, et al. Prevalence and severity of sleep disturbances among patients with early breast cancer. Indian J Palliat Care. 2018;24(1):35–38. doi:10.4103/IJPC.IJPC_137_17
13. Fiorentino L, Rissling M, Liu L, Ancoli-Israel S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: severity of the problem and treatment options. Drug Discov Today Dis Models. 2011;8(4):167–173. doi:10.1016/j.ddmod.2011.05.001
14. Lowery-Allison AE, Passik SD, Cribbet MR, et al. Sleep problems in breast cancer survivors 1–10 years posttreatment. Palliat Support Care. 2018;16(3):325–334. doi:10.1017/S1478951517000311
15. Vin-Raviv N, Akinyemiju TF, Galea S, Bovbjerg DH. Sleep disorder diagnoses and clinical outcomes among hospitalized breast cancer patients: a nationwide inpatient sample study. Support Care Cancer. 2018;26(6):1833–1840. doi:10.1007/s00520-017-4012-1
16. Marinac CR, Nelson SH, Flatt SW, Natarajan L, Pierce JP, Patterson RE. Sleep duration and breast cancer prognosis: perspectives from the women’s healthy eating and living study. Breast Cancer Res Treat. 2017;162(3):581–589. doi:10.1007/s10549-017-4140-9
17. Mansano-Schlosser TC, Ceolim MF. Association between poor clinical prognosis and sleep duration among breast cancer patients. Rev Lat Am Enfermagem. 2017;25:e2899. doi:10.1590/1518-8345.1826.2899
18. Savard J, Simard S, Ivers H, Morin CM. Randomized study on the efficacy of cognitive-behavioral therapy for insomnia secondary to breast cancer, part I: sleep and psychological effects. J Clin Oncol. 2005;23(25):6083–6096. doi:10.1200/JCO.2005.09.548
19. Quesnel C, Savard J, Simard S, Ivers H, Morin CM. Efficacy of cognitive-behavioral therapy for insomnia in women treated for nonmetastatic breast cancer. J Consult Clin Psychol. 2003;71(1):189–200. doi:10.1037/0022-006X.71.1.189
20. Chau TT, Hsiao TM, Huang CT, Liu HW. [A preliminary study of family Apgar index in the Chinese]. Kaohsiung J Med Sci. 1991;7(1):27–31. [Indonesian]
21. Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. 1982;15(2):303–311.
22. Christianson S, Marren J. The impact of event scale - revised (IES-R). Medsurg Nurs. 2012;21(5):321–322.
23. Wu KK, Chan KS. The development of the Chinese version of impact of event scale–Revised (CIES-R). Soc Psychiatry Psychiatr Epidemiol. 2003;38(2):94–98. doi:10.1007/s00127-003-0611-x
24. Miles A, McClements PL, Steele RJ, Redeker C, Sevdalis N, Wardle J. Perceived diagnostic delay and cancer-related distress: a cross-sectional study of patients with colorectal cancer. Psycho-Oncology. 2017;26(1):29–36. doi:10.1002/pon.4093
25. Cheng CP, Yen CF, Ko CH, Yen JY. Factor structure of the center for epidemiologic studies depression scale in Taiwanese adolescents. Compr Psychiatry. 2012;53(3):299–307. doi:10.1016/j.comppsych.2011.04.056
26. Chin WY, Choi EP, Chan KT, Wong CK. The psychometric properties of the center for epidemiologic studies depression scale in chinese primary care patients: factor structure, construct validity, reliability, sensitivity and responsiveness. PLoS One. 2015;10(8):e0135131. doi:10.1371/journal.pone.0135131
27. Bartholomew AA, Marley E. The temporal reliability of the Maudsley personality inventory. J Ment Sci. 1959;105(438):238–240. doi:10.1192/bjp.105.438.238
28. Huang CL, Yang YK, Chu CL, et al. The association between the Lie scale of the Maudsley personality inventory and striatal dopamine D2/D3 receptor availability of healthy Chinese community subjects. Eur Psychiatr. 2006;21(1):62–65. doi:10.1016/j.eurpsy.2005.05.004
29. Buysse DJ, Reynolds CF
30. Kim MS, Kim SY, Kim JH, Park B, Choi HG. Depression in breast cancer patients who have undergone mastectomy: a national cohort study. PLoS One. 2017;12(4):e0175395. doi:10.1371/journal.pone.0175395
31. Kwekkeboom KL. Cancer symptom cluster management. Semin Oncol Nurs. 2016;32(4):373–382. doi:10.1016/j.soncn.2016.08.004
32. Vahia VN. Diagnostic and statistical manual of mental disorders 5: a quick glance. Indian J Psychiatry. 2013;55(3):220–223. doi:10.4103/0019-5545.117131
33. Wu X, Wang J, Cofie R, Kaminga AC, Liu A. Prevalence of posttraumatic stress disorder among breast cancer patients: a meta-analysis. Iran J Public Health. 2016;45(12):1533–1544.
34. Meisel JL, Domchek SM, Vonderheide RH, et al. Quality of life in long-term survivors of metastatic breast cancer. Clin Breast Cancer. 2012;12(2):119–126. doi:10.1016/j.clbc.2012.01.010
35. Bell TM, Vetor AN, Zarzaur BL. Prevalence and treatment of depression and posttraumatic stress disorder among trauma patients with non-neurological injuries. J Trauma Acute Care Surg. 2018;85(5):999–1006. doi:10.1097/TA.0000000000001992
36. Tzang BS, Chen VC, Hsieh CC, et al. Differential associations of proinflammatory and anti-inflammatory cytokines with depression severity from noncancer status to breast cancer course and subsequent chemotherapy. BMC Cancer. 2020;20(1):686. doi:10.1186/s12885-020-07181-w
37. Han TJ, Felger JC, Lee A, Mister D, Miller AH, Torres MA. Association of childhood trauma with fatigue, depression, stress, and inflammation in breast cancer patients undergoing radiotherapy. Psychooncology. 2016;25(2):187–193. doi:10.1002/pon.3831
38. Liu Y, Cao C. The relationship between family history of cancer, coping style and psychological distress. Pak J Med Sci. 2014;30(3):507–510. doi:10.12669/pjms.303.4634
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.