")
Back to Journals » Nature and Science of Sleep » Volume 14
Sleep Quality and Associated Factors Among Adult Cancer Patients Under Treatment at Oncology Units in Amhara Region, Ethiopia
Authors Endeshaw D , Biresaw H, Asefa T , Yesuf NN, Yohannes S
Received 31 December 2021
Accepted for publication 19 May 2022
Published 1 June 2022 Volume 2022:14 Pages 1049—1062
DOI https://doi.org/10.2147/NSS.S356597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Destaw Endeshaw,1 Henok Biresaw,1 Tseganesh Asefa,2 Nurhusien Nuru Yesuf,3 Senay Yohannes3
1Department of Adult Health Nursing, School of Health Sciences, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Destaw Endeshaw, Bahir Dar, Ethiopia, Tel +251918281262, Email [email protected]
Introduction: Poor sleep quality, a common, under-diagnosed, and under-treated problem in cancer patients, has negative physical and psychological consequences, but its prevalence and associated factors are not well studied in Ethiopia. Thus, the present study aimed to assess the prevalence of sleep quality and its associated factors among adult cancer patients receiving treatment at oncology units in Amhara region, Ethiopia.
Methods and Materials: An institution-based cross-sectional study was conducted among adult patients with cancer under treatment at the oncology units in the Amhara region from April 12 to May 12/2021. A systematic random sampling technique was used to select 423 samples. Data were collected using a structured Interviewer-administered questionnaire. Sleep quality and depression were assessed by the Pittsburgh Sleep Quality Index and depression subscale of Hospital Anxiety and Depression Scale, respectively. Bivariable and multivariable logistic regression analyses were computed, considering p < 0.25 to select candidate variables for multivariable analysis and p < 0.05 to be statistically significant in the final model.
Results: A total of 410 cancer patients participated in this study. The mean of the participant’s age was 44.2 (range: 20– 77) years. More than half (52.7%) of participants received chemotherapy and the remaining were treated with a combination of treatments. Two-hundred ninety-three (71.5%) of participants had poor sleep quality and 28.5% had good sleep quality. The factors found to be significantly associated with poor sleep quality were advanced age [AOR = 1.037, 95% CI: (1.012– 1.062)]; having depressive symptoms [AOR = 2.862, 95% CI: (1.133, 7.228)]; having distant metastasis cancer [AOR = 3.758, 95% CI: (1.585, 8.909)]; and increased severity of pain [AOR = 1.331, 95% CI: (1.106, 1.601)].
Conclusion: The study found a high prevalence of poor sleep quality among cancer patients. Early screening and management of sleep problems are crucial in patients with cancer.
Keywords: cancer patients, Ethiopia, Pittsburgh Sleep Quality Index, PSQI, sleep quality
Introduction
Sleep is an essential component of human life that delivers necessary restorative, protective, and energy-conserving functions to the body. It must be of sufficient duration, timing, and regularity to be effective.1,2 However, it is affected by different medical conditions including cancer.3 Patients with cancer often experience several symptoms, which will be associated with the disease or treatment. Among these symptoms, poor sleep quality is the commonest problem in this particular population.4
Poor sleep quality may be described as the inability of initiating and maintaining sleep, frequent awakening, and feeling of unrest.5 Sleep-related complaints are extremely common in patients with cancer but often are not recognized, and they are rarely treated.6 In cancer patients, disturbed sleep is rated the second most bothersome symptom.7 According to different studies, 20% to 78% of cancer patients have poor sleep quality.8–20 This rate is higher than the rate in the general population, which ranges from 15% to 25%.21 Despite its high prevalence and clinical significance, sleep problems are rarely addressed in cancer practice and patients may fail to report it, assuming it to be a normal and temporary reaction to a cancer diagnosis or treatment.22
Although little is known about the prevalence of poor sleep quality in Africa, a Moroccan study found that 71.8% of cancer patients had poor sleep quality.19 In Ethiopia, a meta-analysis of studies conducted among general populations and university students indicated a 53% pooled prevalence of poor sleep quality.23 However, studies on sleep, particularly in cancer patients, are lacking.
Oncology services in Ethiopia are inadequate, and the country is ill-equipped to deal with the rising cancer burden. The number of oncology centers in the country is not keeping pace with the country’s growing population and rising cancer burden.24 Ethiopia has only one fully functional public radiation center, which is situated in the country’s capital and is attempting to serve the entire country.
In patients with cancer, the causes of poor sleep quality are multifactorial. It is affected by socio-demographic characteristics of patients like age,18,25 gender,25,26 marital, employment, and educational status.27–29 Furthermore, cancer treatments, cancer symptoms, and psychological and behavioral stressors associated with cancer and its treatment contribute to poor sleep.22,30,31 Sleep quality is also associated with the primary location of cancer,19 the location of cancer metastasis,14 the stage of cancer,11 the types of treatment provided to patients,17,32,33 and the duration of time passed since diagnosis.34 Moreover, poor functional performance status, poor social support, and higher body mass index are significant factors associated with poor sleep quality.14,35–37
Poor sleep quality in patients with cancer has detrimental physical and psychological consequences including lower quality of life and early mortality.38,39 Poor sleep quality causes serious cardiovascular problems, reduced immune function, poor healing, increased chances of cancer recurrence, impaired performance, impaired cognitive functioning, medication misuse and abuse, poor relationships, and increased healthcare costs.40–44
Recognition of the frequency and characteristics of cancer-related poor sleep quality can provide a base of new approaches to supportive care during the treatment trajectory of cancer. Therefore, a study on the quality of sleep and its associated factors is extremely important but scarce in Ethiopia. Thus, the present study aimed to assess the prevalence of sleep quality and its associated factors among cancer patients at oncology units in the Amhara region, Ethiopia.
We hypothesized that age, gender, marital status, unemployment, educational status, and clinical variables such as cancer stage, type of treatment, time since diagnosis, poor performance status, poor social support, and a higher body mass index would all be connected to poor sleep quality in cancer patients. A positive relationship would also exist between poor sleep quality and symptom severity in patients with cancer.
Methods and Materials
Study Design, Period, and Setting
An institution-based cross-sectional study design was employed from April 12 to May 12/2021 at hospitals that have oncology units in the Amhara region. Only three hospitals in the region have an oncology unit to provide care and treatment for cancer patients: Felege Hiwot Comprehensive Specialized Hospital (FHCSH), Dessie Comprehensive Specialized Hospital (DCSH), and University of Gondar Comprehensive Specialized Hospital (UoGCSH). The three hospitals; FHCSH, DCSH, and UoGCSH are located in Bahir Dar, Dessie, and Gondar cities, which are 565, 401, and 735 kilometers far from Addis Ababa, the capital city of Ethiopia, respectively. More than 1800 cancer patients were receiving cancer treatment at the three hospitals on an annual basis.
Inclusion and Exclusion Criteria
Patients who were over the age of 18 years, with a pathologically confirmed cancer diagnosis, and who were receiving a cancer treatment were included in this study; however, those with a critical medical condition who were unable to comprehend and respond to questions throughout the data collection period were excluded.
Sample Size Determination and Sampling Technique
The sample size was calculated using the single population proportion formula and by adding a 10% non-response rate the final sample size was calculated to be 423. A systematic random sampling technique was used to approach study participants from each hospital. The sampling interval was determined by dividing the total study population who had follow-up and were under treatment during one typical month (1090) by the total sample size (423). Based on this, the sampling interval (K) was calculated to be 1090/423 ≈ 2. The first participant was selected randomly by a lottery method from 1 or 2, and the next respondent was chosen at regular intervals (every 2).
Study Variables
The dependent variable was sleep quality and the independent variables were socio-demographic variables (age, sex, marital status, occupation, religion, residence, level of education, and social support), behavioral variables (coffee drinking, smoking status, alcohol use, and khat use), clinical factors (type of cancer, stage of cancer, presence of metastasis, site of metastasis, duration of time since diagnosis, the duration of time between diagnosis and treatment, treatment type, performance status, comorbid disease, and body mass index), and disease and treatment-related symptoms (pain, fatigue, anxiety, depression, numbness, dyspnea, nausea, vomiting, anorexia, sadness, drowsiness, psychological distress, dryness of mouth and problem in remembering).
Operational Definition
Sleep quality: a global Pittsburgh Sleep Quality Index (PSQI) score of greater than 5 indicates poor sleep quality and a global PSQI score of less than or equal to 5 indicates good sleep quality.45
Anxiety and depression: In our study, a patient with more than 10 points on each scale of the Hospital Anxiety and Depression Scale has anxiety and depression problems.46
Symptom severity: For all MD Anderson Symptom Inventory core symptoms, the severity scale was 0 (no symptom), 1–4 (mild symptom), and ≥5 (moderate-to-severe symptom).47
Smoking status: Never smoker was an individual who had never tried a cigarette in his/her lifetime. Former smoker was an individual who had smoked in the past but stopped smoking 30 days before the data collection period. Current smoker was an individual who smoked a cigarette one or more in the past 30 days before the survey.48
Khat chewing: Former khat chewer was an individual who had ever used khat at least once in his/her lifetime but never used it in the last 30 days. Current khat chewer was an individual who had used khat at least once in the last month before the study. Never khat chewer was an individual who never tried khat chewing in his/her lifetime at all.49
Alcohol drinking status: Former alcohol user was an individual who admitted to having ever used alcohol but stopped in the last 30 days. Current alcohol user was an individual who took alcoholic drinks within 30 days preceding the study. Never user was an individual who never used alcohol in his/her lifetime.49,50
Performance status: by using the Eastern Cooperative Oncology Group (ECOG) performance status scale, a grade of 0–1 indicates good performance status and a grade of 2–4 indicates poor performance status.35
Social support: by using the three-item Oslo social support scale (OSSS-3), a score of 3–8 represents “poor support”, 9–11 “moderate support”, and 12–14 “strong support”.51
Body mass index (BMI) was classified as underweight (BMI <18.5), normal (BMI 18.5–24.99), overweight (BMI 25.0–29.99), and obese (BMI ≥ 30.0).52
Khat is a herbal product consisting of the leaves and shoots of the shrub Catha edulis Forsk, a member (genera) of the evergreen Celastraceae (moonseed or spindle-tree) family.53
Measurements and Data Collection Technique
Data Collection Tool
A pretested, structured, interviewer-administered questionnaire and data extraction checklist were used to collect data. The following subsections make up the questionnaire.
Socio-demographic, behavioral, and clinical factors: The tools for these variables were adapted from the review of different pieces of literature.8,14,30,54
Sleep Quality
It was assessed by a widely used Pittsburgh Sleep Quality Index. The tool was designed to evaluate the subjective quality of sleep in the past month. It contains 19 self-rated questions, including seven subscale components (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction). Each component score ranges from 0 (no difficulty) to 3 (severe difficulty). The sleep component score is summed to yield a total score (referred to as global score) ranging from 0 to 21 with higher total scores indicating poor sleep quality. A global Pittsburgh Sleep Quality Index score greater than 5 yielded a diagnostic sensitivity of 89% and specificity of 86.5% (kappa = 0.75, P ≤ 0:001) in distinguishing “poor” from “good” sleepers.45 The construct validity and internal consistency are further evaluated and supported in cancer patients with a Cronbach’s α value of 0.81.55 This tool was validated in Ethiopian adults with a good psychometric validity.56 For the present study, the internal consistency measurement of the tool’s subscales found a Cronbach’s α coefficient of 0.761 which was acceptable for this study.
Anxiety and Depression
The Hospital Anxiety and Depression Scale was used to assess these variables. The 14-item measure examines depression and anxiety symptoms and is divided into two subscales, each having seven items that are assessed on a four-point scale (0–3). Each subscale’s total score runs from 0 to 21. Based on their results, the respondents can be classified as normal (0–7), borderline (8–10), or abnormal cases (11–21).57 This scale was also validated in Ethiopian cancer patients.46 In the current study, the Cronbach’s α value was 0.931 and 0.932 for anxiety and depression subscales, respectively.
The Severity of Symptoms
This was assessed by the core symptom severity subscale of the MD Anderson Symptom Inventory, a brief, valid, reliable, easily understood questionnaire. The tool measures the intensities of thirteen symptoms (pain, fatigue, numbness, dyspnea, nausea, vomiting, anorexia, sadness, drowsiness, psychological distress, dryness of mouth, sleep disturbance, and problem in remembering) on a 0 to 10 scale, with higher scores indicating more severe symptoms.58 This tool has been validated in Ethiopia, and the Amharic version was used in this study, with Cronbach’s alpha at 0.82.59
Social Support
It was measured using the three-item Oslo social support scale, which includes questions about the primary support group, others’ interest and concern, and the ease of obtaining practical help. The first item was rated on a four-point scale, while the other two were graded on a five-point scale, resulting in a total score of 14 when the three items were added together.60 Cronbach’s alpha was 0.763 in this study.
Performance status: The patients’ performance status (the patient’s level of functioning seen from their daily activity, physical ability, and self-care) was measured using the one-item Eastern cooperative oncology group (ECOG) score, which ranges from 0 (fully active) to 4 (completely disabled).61
Data Collection Technique
Data were collected by five trained nurses who have a Bachelor of Science degree through interviews, and the process was closely monitored by three trained nurses who have a Masters of Science degree. Participants were approached for the interview after finishing their examination at the oncology outpatient department. After each interview, data collectors took measurements of the participant’s weight and height. Weight was measured with a light cloth while standing, and height was measured using a straight, upright body posture. Clinical characteristics (type of cancer, stage of cancer, presence of metastasis, site of metastasis, duration of time since diagnosis, the duration of time between diagnosis and treatment, treatment type, and comorbid disease) were retrieved from medical records. To avoid the risk of COVID-19 transmission, necessary measures were taken by data collectors.
Data Management and Analysis
Data were coded and entered into Epi-data version 4.6 and then exported to SPSS version 23.0 for analysis. Data were cleaned and descriptive statistics like median, mean, frequencies, and proportions were computed for continuous as well as categorical variables accordingly and presented by using tables and texts. Model fitness was checked by the Hosmer–Lemeshow goodness of fit test. The p-value for the test was 0.830 which was greater than 0.05 indicating that the model fitted the data. The presence or absence of multi-collinearity was checked using the Variance Inflation Factor (VIF) and all its values were less than 10, which was interpreted as multi-collinearity was not problematic. Binary logistic regression analysis was computed to examine the association between the dependent and independent variables. Bivariable logistic regression analysis was performed to select candidate variables for multivariable logistic regression analysis and variables with p-values of less than 0.25 were entered into the multivariable logistic regression analysis model.62 After running multiple logistic regression analysis with the backward LR method, those with p < 0.05 were considered statistically significant.
Result
Socio-Demographic Characteristics
Out of 423 samples, data were collected from a total of 410 randomly selected patients with a response rate of 97%. Of the total respondents, nearly two-thirds (62.7%) were female. The mean age of the participants was 44.2 (range: 20–77) years. Slightly more than two-fifths (44.4%) of the participants were between the ages of 35 and 50. In terms of residency, slightly more than half of the participants (52.7%) were from rural areas. According to the unadjusted analysis, the prevalence of poor sleep was higher for participants aged 30–35 years, married, housewives, and who had poor social support (Table 1).
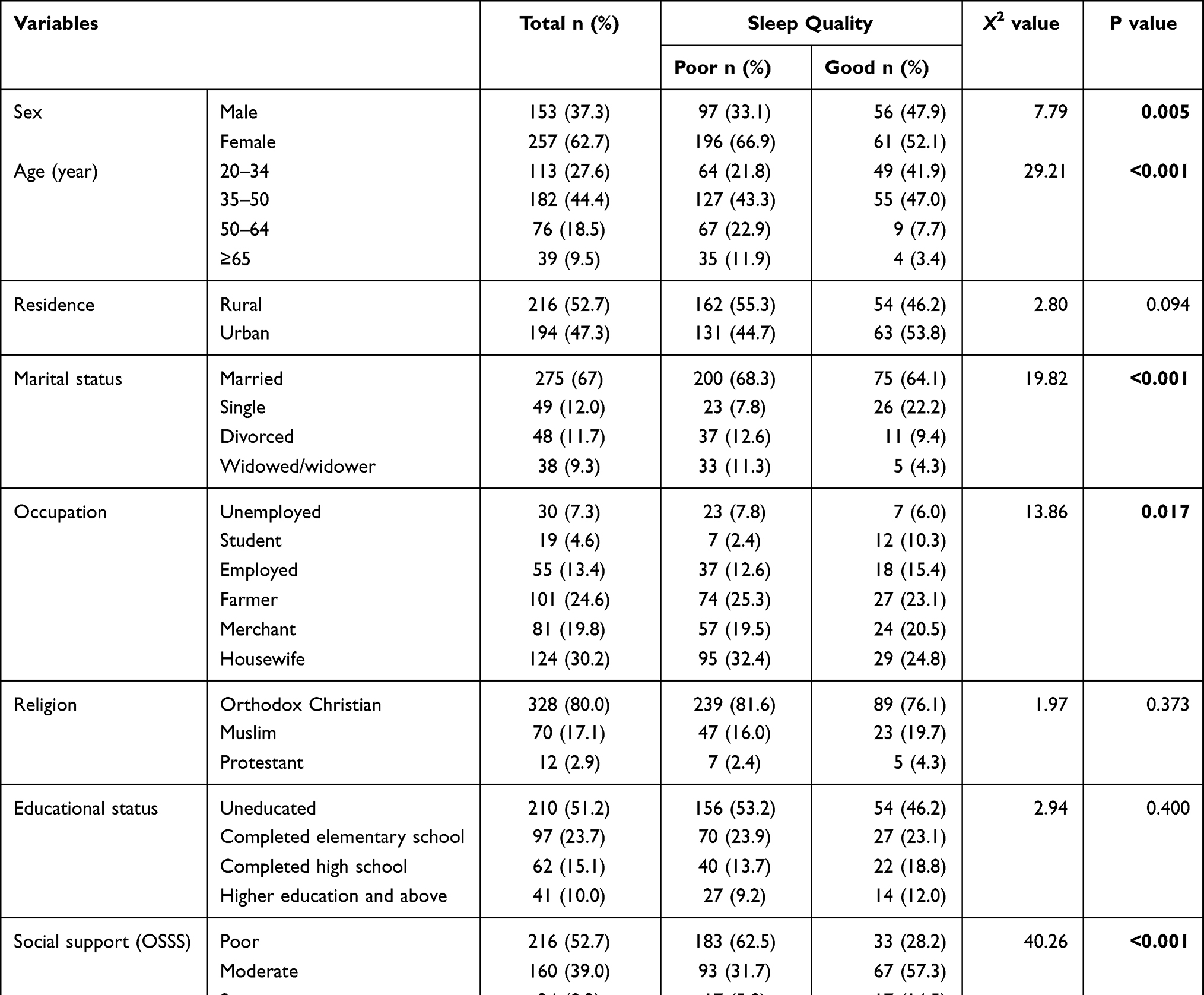 |
Table 1 Socio-Demographic Characteristics of Study Participants Attending Oncology Units in Amhara Region Hospitals, 2021 (n = 410) |
Behavioral Characteristics
Of 410 study participants, more than half (55.1%) drink coffee daily. Only 12% of the participants were current users of alcohol, whereas slightly more than half (51.5%) were former drinkers. Only a few of them (3.4%) and (2.4%) were current khat chewers and current cigarette smokers, respectively. The majority (49.8%) of the poor sleepers were daily coffee drinkers, followed by occasional (24.9) and never (25.3) coffee drinkers (Table 2).
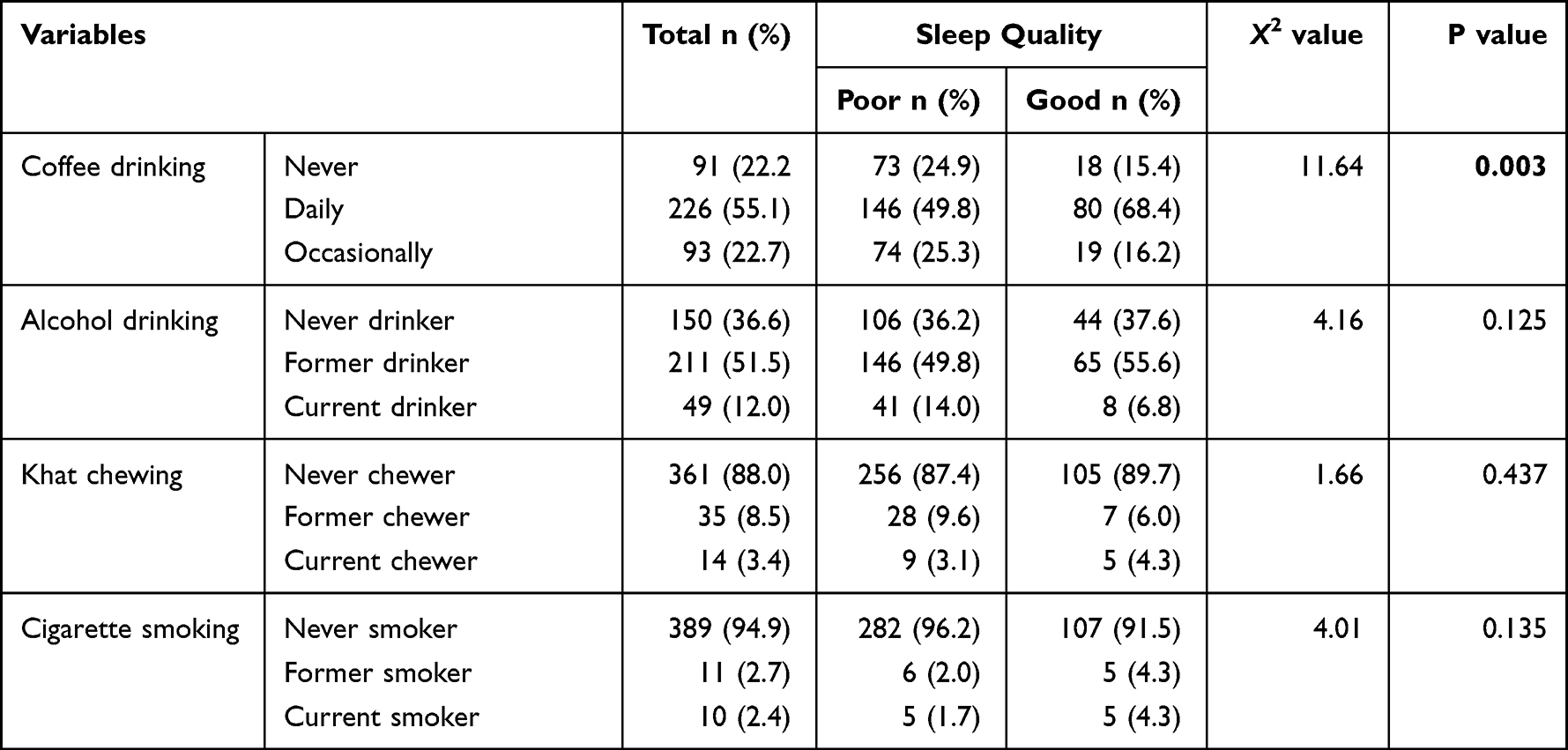 |
Table 2 Behavioral Characteristics of Study Participants Attending Oncology Units in Amhara Region Hospitals, 2021 (n = 410) |
Clinical Characteristics
Cancers of the gastrointestinal tract (32.0%), breast cancer (24.9%), and gynecological cancers (15.4%) were the most common malignancies in this study. Slightly more than half (52.7%) of participants were treated with chemotherapy alone, while 35.4% were treated with a combination of surgery and chemotherapy. Around two-fifths of patients (41%) were diagnosed with early-stage cancer (stage I and II), whereas the remaining three-fifths (59%) were diagnosed with advanced cancer (stage III and IV). In terms of psychological problems, 33.9% and 33.2% of participants, respectively, experienced anxiety and depression symptoms. In this study, those who underwent chemotherapy had more sleeping difficulty than those who received surgery and chemotherapy (60.1% vs 28.3%, p-value <0.001). Likewise, cancer patients who had anxiety symptoms experienced more sleep difficulty than their counterparts (Table 3).
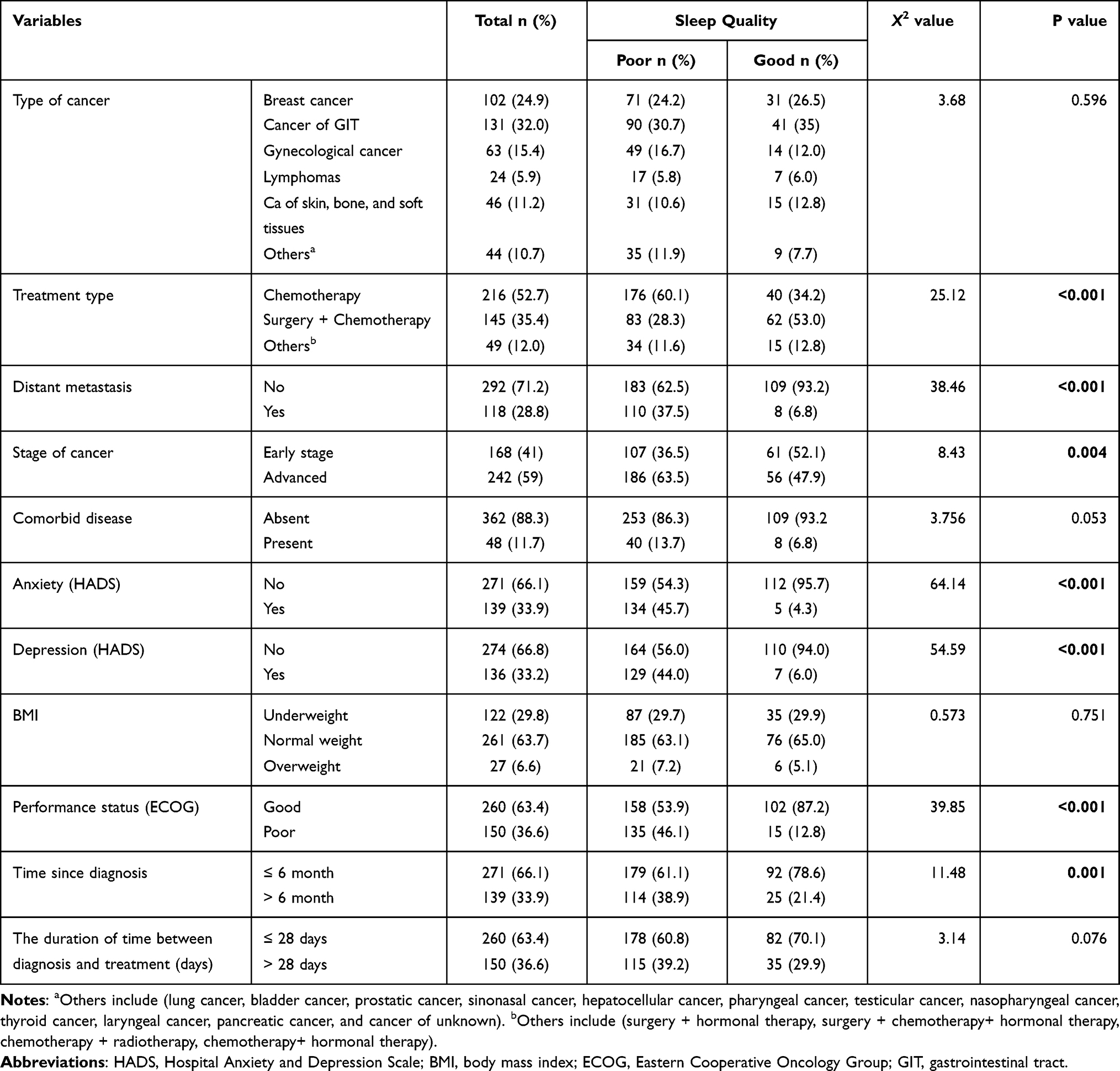 |
Table 3 Clinical Characteristics of Study Participants Attending Oncology Units in Amhara Region Hospitals, 2021 (n = 410) |
Symptom Severity of Study Participants
Almost one-third of study participants (32.4%) experienced moderate-to-severe pain based on the MD Anderson Symptom Inventory core symptom severity scale. On the other hand, one-third of participants (33.4%) reported moderate-to-severe lack of appetite, whereas one-fifth (20.2%) of them reported moderate-to-severe numbness (Table 4).
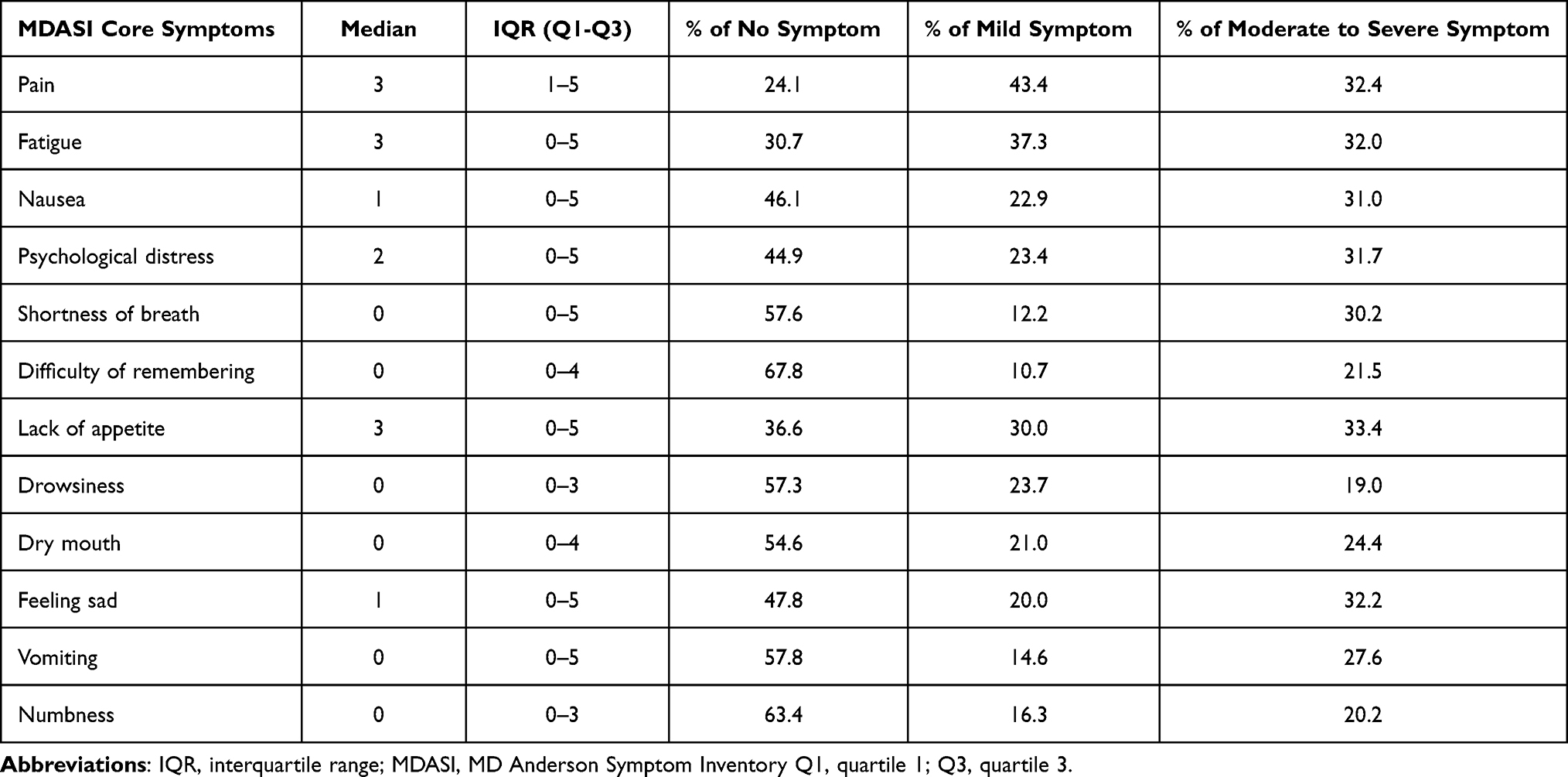 |
Table 4 Descriptive Statistics of Symptom Severity Points Among Patients with Cancer Attending Oncology Units in Amhara Region Hospitals, 2021 (n = 410) |
Sleep Quality
In this study, the majority (71.5%) (95% CI: 66.8, 75.8) of study participants had poor sleep quality and the remaining 28.5% (95% CI: 24.2, 33.2) had good sleep quality.
The median PSQI global score was 7 with an IQR of 5–10. The median sleep efficiency score was 75% with a minimum of 13% and a maximum of 95%. The minimum actual sleep duration time was 2 hours and the maximum was 12 hours (Table 5).
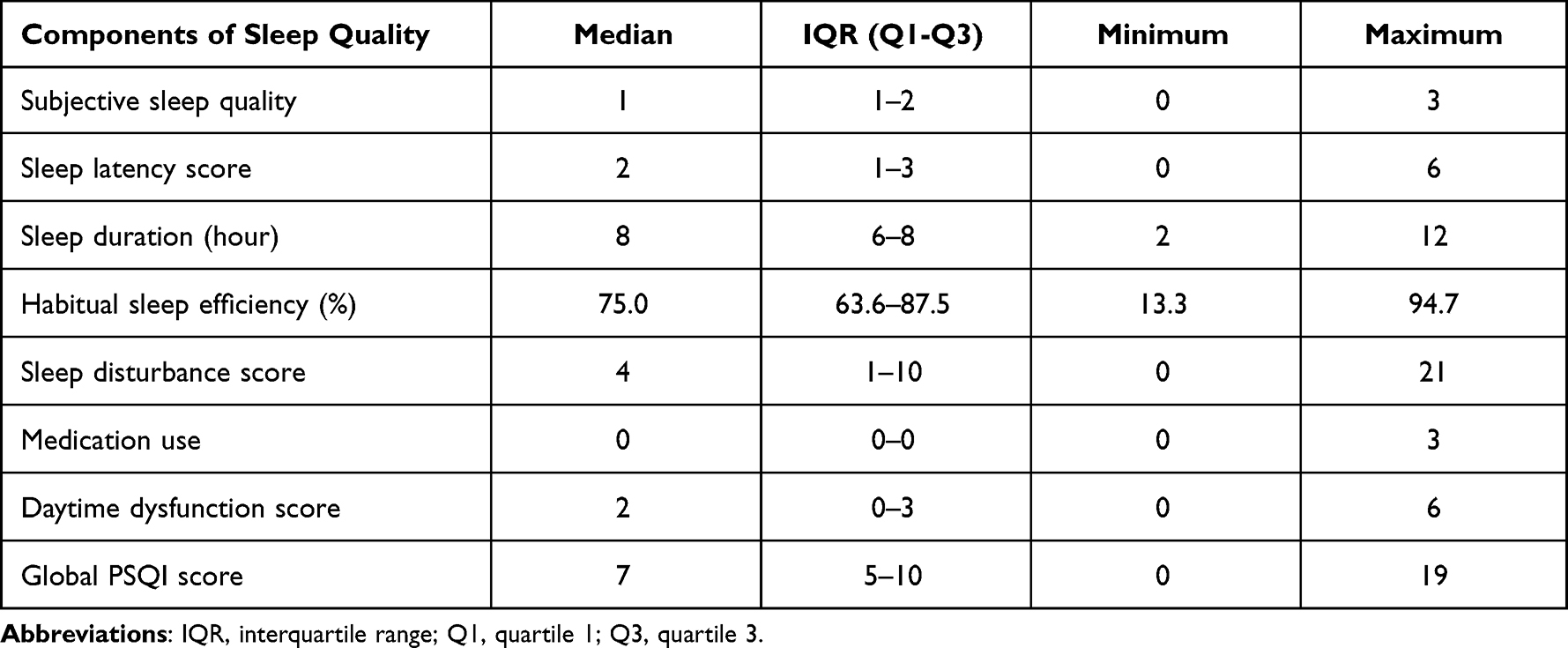 |
Table 5 Descriptive Statistics of Component and Global Sleep Quality Index Score Among Patients with Cancer Attending Oncology Units in Amhara Region Hospitals, 2021 (n = 410) |
Factors Associated with Sleep Quality
In bi-variable logistic regression analysis, thirty independent variables (age, sex, marital status, residence, occupation, coffee drinking, smoking status, alcohol use, time since diagnosis, cancer type, stage of cancer, treatment type, comorbid disease, presence of metastasis, performance status, pain, fatigue, anxiety, depression, numbness, dyspnea, nausea, vomiting, psychological distress, drowsiness, anorexia, sadness, problem in remembering, dry mouth, and social support) were found to have P-value <0.25 (Table 6 and Supplementary Table 1). Subsequently, these variables were entered into the multivariable analysis.
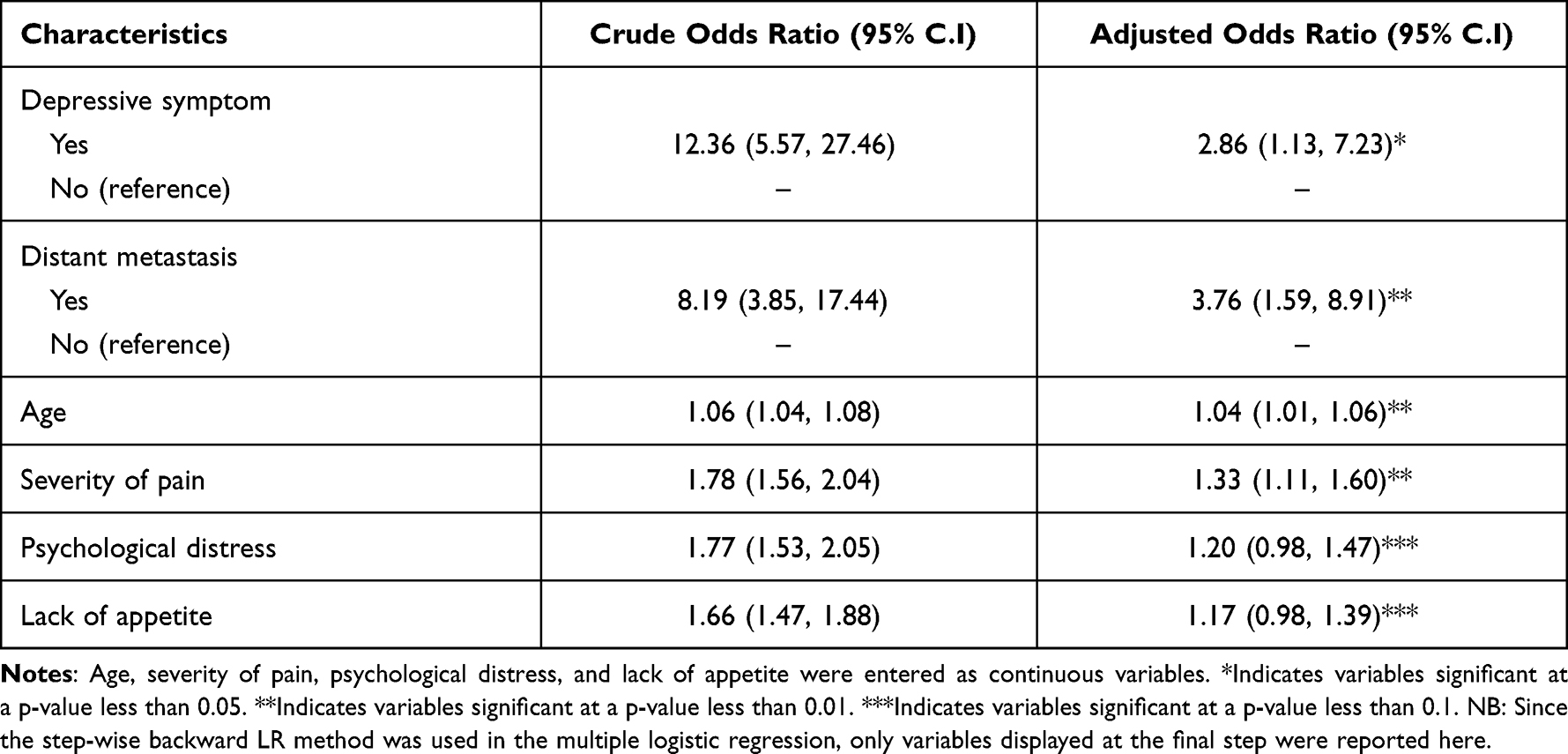 |
Table 6 Factors Associated with Poor Sleep Quality of Study Participants at Oncology Units in Amhara Region Hospitals, 2021 |
In multivariable analysis, age, depressive symptoms, presence of distant metastasis, and severity of pain showed statistically significant association with poor sleep quality among cancer patients. Accordingly, when the age of a patient increases by one year, the odds of having poor sleep quality increase by a factor of 1.037 [AOR = 1.037, 95% CI: (1.012–1.062)]. The odds of having poor sleep quality were 2.9 times among patients who had depressive symptoms as compared to those patients who do not have depressive symptoms [AOR = 2.862, 95% CI: (1.133, 7.228)]. Regarding distant metastasis, the odds of having poor sleep quality among patients who had distant metastasis cancer were 3.8 times compared with those who do not have distant metastasis [AOR = 3.758, 95% CI: (1.585, 8.909)]. On the other hand, when the severity of pain increased by one point on a 0–10 scale, the odds of having poor sleep quality increased by a factor of 1.331 [AOR = 1.331, 95% CI: (1.106, 1.601)].
Discussion
This study aimed to assess the prevalence and associated factors of sleep quality among patients with cancer at oncology units in Amhara region hospitals by using a cross-sectional study. Based on this objective, the prevalence of poor sleep quality in this study was 71.5% (95% CI: 66.8, 75.8). This finding was consistent with previous studies conducted in Taiwan (72%) and Morocco (71.8%).16,19 On the other hand, it was lower than a multicenter study conducted in five countries in Europe (78%).8 This discrepancy could be explained by the difference in study populations. In the current study, patients with all stages of cancer were included, whereas, in the European study, patients with advanced cancer were included. Since pieces of evidence showed that patients with advanced cancer had a higher risk of poor sleep quality than those with localized disease, including those with all stages of cancer in the current study may lower the prevalence of poor sleep quality compared to the European study.30
In contrast, the prevalence of poor sleep quality in the current study was higher than the study done in Italy (58.8%), and Denmark (57.9%).13,18 This inconsistency might be due to differences in characteristics of study participants in terms of the inclusion and exclusion criteria they used. In the present study, patients with all grades of ECOG performance status ranging from 0 to 4 were included but in the Italian study, only patients with performance status grades less than two were included. This performance status difference between the Italian and current study participants makes the prevalence of poor sleep quality high in the present study because pieces of evidence indicated that patients with higher scores of ECOG performance status are more likely to become poor sleepers.14,35 In Denmark, patients who had distant metastasis cancer were excluded from the study, which lowers the prevalence of poor sleep quality in that study. Similarly, the prevalence of poor sleep quality in the current study was also higher than the studies conducted in India (57.6%), Turkey (40.4%), Iran (51.4%), and America (64%).11,14,17,20 This discrepancy might be due to the variation in the country’s level of healthcare provision. In low-income countries including Ethiopia, the access to quality cancer treatment and palliative care is often poor which may affect patients’ sleep quality negatively.24,63 This implies that strengthening the healthcare system in general and expanding quality oncology services, in particular, may reduce the prevalence of poor sleep quality.
In the present study, the odds of having poor sleep quality were increased when the age of the patient increases. Even though contradicting results are available from studies conducted in Morocco and the Netherlands,19,26 the current study result was in line with the studies conducted in Denmark and Iran where older age is associated with poor sleep quality in patients with cancer.18,25 The possible justification for this association might be due to the reduction of melatonin levels during aging. The possible mechanism for age-related melatonin changes is age-related degenerative alterations of the suprachiasmatic nucleus in the hypothalamus, which regulates the melatonin levels. Consequently, when melatonin levels become low there may be impairment of homeostatic sleep regulation and circadian rhythm, which ultimately results in poor sleep quality.64 Since age is a non-modifiable risk factor, the finding of this study points out the requirement of higher emphasis for elderly cancer patients.
On the other hand, the odds of poor sleep quality in the current study were higher among patients who had depressive symptoms than those who do not have it. This finding was in line with the studies conducted in Turkey and Brazil.15,65 The reason for this association might be because depressed individuals have a disruption in both homeostatic and circadian drives to sleep which might be related to deficiencies in key neurotransmitters, such as serotonin (5-HT), noradrenaline, or acetylcholine.66 This disruption finally leads to a symptom of daytime sleepiness, which consequently decreases the number of hours slept per night and had frequent waking up in the night. On the other hand, sleep problems have also a significant role in the development of depression. This suggests the presence of a bidirectional association between sleep problems and depression.66,67 This implies that targeted management of one may improve the other. Therefore, treating depression might improve sleep quality, and addressing sleep problems may relieve psychological morbidity.
As revealed by the result of this study, the odds of having poor sleep quality were significantly higher among patients who had distant metastasis cancer than those with no distant metastasis. This might be justified by the fact that patients with metastatic cancer have a high symptom burden due to multi-organ involvement of the disease. As a result, patients may expose to maladaptive behaviors like spending prolonged time in bed at day time, napping, and reduced daily activity. All these practices lead to dysregulation of sleep-wake cycles and make it difficult for individuals to fall and stay asleep during regular sleep hours at night.30 It is also true that those with distant metastases are also more likely to receive more intensive treatment (eg, additional rounds of radiation), which might also cause sleep disturbances.33
Increased pain intensity as measured with a 0 to 10 numeric pain scale was also significantly associated with poor sleep in the current study. This finding was supported by studies conducted in America, Iran, and different European countries.8,17,68 Pain is a common symptom in patients with cancer that negatively affects falling and staying asleep. The possible mechanism might be due to the neurotransmitter dopamine dysregulation in the brain. When there are alterations or disturbances in the signaling of dopamine induced by pain, it could lead to prolonged periods of sleep loss and greater disruption of sleep continuity. However, the presence of poor sleep quality has also the potential to increase pain and its sensitivity. This states the reciprocal association between them which creates a self-perpetuating cycle of sleep disruption and pain intensification.69 This indicates the complexity of the problem and the need for more effective symptom management for patients with cancer.
Although not seen in our study, anxiety has a clinical and statistical relationship with sleep quality.30 Anxiety causes mental hyperarousal, which can keep the patient from falling asleep. It also prevents someone from staying asleep long enough to feel fully rested.70 Besides, anxiety disturbs sleep by causing vivid dreams via influencing rapid eye movement (REM) sleep.71
Cancer treatment type has also a significant relationship with poor sleep quality. Chemotherapy and radiotherapy have been linked to significantly lower sleep quality because they increase the production of pro-inflammatory cytokines, which act on the central nervous system, altering rest-activity cycles and influencing sleep negatively.17,32,33 Although this clinical importance is known, our research found no statistically significant relationship between them. Furthermore, as shown in the previous literature, cancer and cancer treatment symptoms like fatigue, dyspnea, numbness, drowsiness, nausea, and vomiting significantly affect sleep quality.17,68,72,73 However, these variables had no statistically significant relationship with sleep quality in our study. These could be due to differences in sample characteristics between studies, such as different types of cancer and different cancer treatment regimens, which strengthen the link between sleep disturbance and other variables. This suggests that more research may be required to reconcile these inconsistencies.
Limitation of the Study
There are some limitations to this research. A temporal relationship between the outcome variable and independent variables could not be established because of the cross-sectional nature of the study design. Another limitation is that the self-reported questionnaire measures of sleep quality are prone to recall bias, which may misestimate the prevalence. Aside from the aforementioned limitations, using the step-wise backward LR method of analysis may be regarded as a limitation because it needs model selection by parameter inference, which can lead to parameter biases, over-fitting, and incorrect significance tests.
Conclusion and Recommendation
The present study found a high prevalence of poor sleep quality. Advanced age, presence of depressive symptoms, presence of distant metastasis, and increased severity of pain were factors that significantly affect sleep quality in cancer patients.
Health professionals shall integrate the assessment of sleep problems into routine care and provide appropriate management through a multi-disciplinary approach for patients with cancer. Furthermore, they need to provide special consideration to those whose age is advanced, have metastatic cancer, and experiencing severe pain. During treatment trajectory, cancer patients must be carefully screened for depression and given appropriate medication. Policymakers and program planners should think about developing a practical method for screening and managing sleep quality problems in cancer patients and integrating it into the current cancer treatment and palliative care program. Additionally, they need to consider expanding quality oncology service centers with the appropriate resources. Future researchers also consider conducting a study at the country level since our study is not generalizable to a country as a whole.
Abbreviations
ECOG, Eastern Cooperative Oncology Group; PSQI, Pittsburgh Sleep Quality Index.
Ethics Approval and Consent to Participate
The research was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from the University of Gondar College of Medicine and Health Sciences School of Nursing Ethical Committee (Ref No. S/N/164/7/2013). A formal letter was written to all three hospitals, and written informed consent was obtained from each participant. Confidentiality was maintained by omitting the participant’s name and personal identification, and the collected information was not revealed to anyone except the principal investigators and kept locked with a key. Privacy was maintained by arranging a quiet place during the interview.
Acknowledgments
We would like to thank study participants, data collectors, and supervisors for their valuable contribution to the success of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have drafted or written, or substantially revised or critically reviewed the article; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eugene AR, Masiak J. The neuroprotective aspects of sleep. Medtube Sci. 2015;3(1):35–40.
2. Brinkman JERV, Sharma S. Physiology, sleep. Treasure Island (FL): StatPearls Publishing; [updated April 29, 2020; cited February 3, 2021]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482512/.
3. Parish JM. Sleep-related problems in common medical conditions. Chest. 2009;135(2):563–572. doi:10.1378/chest.08-0934
4. Kirkova J, Aktas A, Walsh D, Davis MP. Cancer symptom clusters: clinical and research methodology. J Palliat Med. 2011;14(10):1149–1166. doi:10.1089/jpm.2010.0507
5. National Sleep Foundation. What is sleep quality?; 2020. Available from: https://www.thensf.org/what-is-sleep-quality/.
6. Dahiya S, Ahluwalia MS, Walia HK. Sleep disturbances in cancer patients: underrecognized and undertreated. Cleve Clin J Med. 2013;80(11):722–732. doi:10.3949/ccjm.80a.12170
7. Cleeland CS, Zhao F, Chang VT, et al. The symptom burden of cancer: evidence for a core set of cancer-related and treatment-related symptoms from the Eastern Cooperative Oncology Group Symptom Outcomes and Practice Patterns study. Cancer. 2013;119(24):4333–4340. doi:10.1002/cncr.28376
8. Jakobsen G, Engstrøm M, Fayers P, et al. Sleep quality with WHO step III opioid use for cancer pain. BMJ Support Palliat Care. 2019;9(3):307–315. doi:10.1136/bmjspcare-2017-001399
9. Palesh OG, Roscoe JA, Mustian KM, et al. Prevalence, demographics, and psychological associations of sleep disruption in patients with cancer: university of Rochester cancer center–community clinical oncology program. J Clin Oncol. 2010;28(2):292. doi:10.1200/JCO.2009.22.5011
10. Strollo SE, Fallon EA, Gapstur SM, Smith TG. Cancer-related problems, sleep quality, and sleep disturbance among long-term cancer survivors at 9-years post diagnosis. Sleep Med. 2020;65:177–185. doi:10.1016/j.sleep.2019.10.008
11. Pai A, Sivanandh B, Udupa K. Quality of sleep in patients with cancer: a Cross-Sectional Observational Study. Indian J Palliat Care. 2020;26(1):9–12. doi:10.4103/IJPC.IJPC_164_19
12. Romito F, Cormio C, De Padova S, et al. Patients attitudes towards sleep disturbances during chemotherapy. Eur J Cancer Care. 2014;23(3):385–393. doi:10.1111/ecc.12106
13. Saini A, Berruti A, Ferini-Strambi L, et al. Restless legs syndrome as a cause of sleep disturbances in cancer patients receiving chemotherapy. J Pain Symptom Manage. 2013;46(1):56–64. doi:10.1016/j.jpainsymman.2012.06.018
14. Akman T, Yavuzsen T, Sevgen Z, Ellidokuz H, Yilmaz AU. Evaluation of sleep disorders in cancer patients based on Pittsburgh sleep quality index. Eur J Cancer Care. 2015;24(4):553–559. doi:10.1111/ecc.12296
15. Şanlier NT, Şahin MA, Demirkazik A, Özkan A, Şenler FÇ. Sleep quality of cancer patients receiving systemic treatment: a Cross-Sectional Study. J Oncol Sci. 2020;6(1):15–22. doi:10.37047/jos.2019-71898
16. Sun JL, Wu SC, Chang LI, Chiou JF, Chou PL, Lin CC. The relationship between light exposure and sleep, fatigue, and depression in cancer outpatients: test of the mediating effect. Cancer Nurs. 2014;37(5):382–390. doi:10.1097/NCC.0000000000000106
17. Jalali R, Rezaei M, Khaledi Paveh B, Aznab M, AmiriFard N, Mohammadi E. Sleep disorder and its correlates in patients undergoing chemotherapy. Iran J Nurs Res. 2016;29(99):76–85. doi:10.29252/ijn.29.99.100.76
18. Colagiuri B, Christensen S, Jensen AB, Price MA, Butow PN, Zachariae R. Prevalence and predictors of sleep difficulty in a national cohort of women with primary breast cancer three to four months postsurgery. J Pain Symptom Manage. 2011;42(5):710–720. doi:10.1016/j.jpainsymman.2011.02.012
19. Echchikhi Y, El-Abbassi S, Touil A, et al. Sleep disorders and sleep quality in Moroccan adult patients with cancer during treatment. J Cancer Sci Ther. 2017;9(09):637–643. doi:10.4172/1948-5956.1000486
20. Narayanan S, Reddy A, Lopez G, et al. Sleep disturbance in cancer patients referred to an ambulatory integrative oncology consultation. Support Care Cancer. 2022;30(3):2417–2425. doi:10.1007/s00520-021-06668-x
21. Grandner MA, Martin JL, Patel NP, et al. Age and sleep disturbances among American men and women: data from the US behavioral risk factor surveillance system. Sleep. 2012;35(3):395–406. doi:10.5665/sleep.1704
22. Howell D, Oliver T, Keller-Olaman S, et al. Sleep disturbance in adults with cancer: a systematic review of evidence for best practices in assessment and management for clinical practice. Ann Oncol. 2014;25(4):791–800. doi:10.1093/annonc/mdt506
23. Manzar MD, Bekele BB, Noohu MM, et al. Prevalence of poor sleep quality in the Ethiopian population: a systematic review and meta-analysis. Sleep Breathing. 2020;24(2):709–716. doi:10.1007/s11325-019-01871-x
24. Gelibo T, Getachew T, Bekele A, et al. Availability and readiness of services for cancer care at health facilities in Ethiopia: implication for action. Ethiop J Health Dev. 2017;31(1):391–396.
25. Bagheri-Nesami M, Goudarzian AH, Jan Babaei G, Badiee M, Mousavi M, Sadegh Sharifi M. Sleep quality and associated risk factors in leukemia patients undergoing chemotherapy in Iran. Asian Pac J Cancer Prev. 2016;17(S3):107–111. doi:10.7314/APJCP.2016.17.S3.107
26. Santoso AMM, Jansen F, Lissenberg-Witte BI, et al. Poor sleep quality among newly diagnosed head and neck cancer patients: prevalence and associated factors. Support Care Cancer. 2021;29(2):1035–1045. doi:10.1007/s00520-020-05577-9
27. Eghtedar S, Nahamin M, Hassanzadeh R, Aparnak F-S, Asghari E. Other side of breast cancer: sleep quality. J Sleep Res. 2016;1(4):169–175.
28. Tel H. Sleep quality and quality of life among the elderly people. Neurol Psychiatry Bra. 2013;19(1):48–52. doi:10.1016/j.npbr.2012.10.002
29. Park JH, Lee SJ, Gwak JI, Shim JY, Lee JK. Sleep quality of breast cancer patients receiving chemotherapy in the outpatients setting. Korean J Fam Med. 2010;31(10):778–785. doi:10.4082/kjfm.2010.31.10.778
30. Palesh O, Peppone L, Innominato PF, et al. Prevalence, putative mechanisms, and current management of sleep problems during chemotherapy for cancer. Nat Sci Sleep. 2012;4:151–162. doi:10.2147/NSS.S18895
31. Leysen L, Lahousse A, Nijs J, et al. Prevalence and risk factors of sleep disturbances in breast cancersurvivors: systematic review and meta-analyses. Support Care Cancer. 2019;27(12):4401–4433. doi:10.1007/s00520-019-04936-5
32. Hansen M, Madsen M, Wildschiødtz G, Rosenberg J, Gögenur I. Sleep disturbances and changes in urinary 6‐sulphatoxymelatonin levels in patients with breast cancer undergoing lumpectomy. Acta Anaesthesiol Scand. 2013;57(9):1146–1153. doi:10.1111/aas.12157
33. Tian J, Chen GL, Zhang HR. Sleep status of cervical cancer patients and predictors of poor sleep quality during adjuvant therapy. Support Care Cancer. 2015;23(5):1401–1408. doi:10.1007/s00520-014-2493-8
34. Noroozi M. Quality of sleep and related factors in breast cancer patients receiving chemotherapy in Qom 2011. Iran J Breast Dis. 2012;4:51–60.
35. Velinova S, Kazlauskaite R, Aguirre R, et al. The relationship between performance status and sleep quality in cancer patients. J Clin Oncol. 2013;31(15_suppl):e20544–e. doi:10.1200/jco.2013.31.15_suppl.e20544
36. Habibi F, Hashemi M, Hemati S, Gholamrezaei A. Sleep quality and its associated factors in Iranian patients with breast cancer. Int J Body Mind Cult. 2016;3:121–131.
37. Kent de Grey RG, Uchino BN, Trettevik R, Cronan S, Hogan JN. Social support and sleep: a meta-analysis. J Health Psychol. 2018;37(8):787–798. doi:10.1037/hea0000628
38. Liu L, Fiorentino L, Rissling M, et al. Decreased health-related quality of life in women with breast cancer is associated with poor sleep. Behav Sleep Med. 2013;11(3):189–206. doi:10.1080/15402002.2012.660589
39. Palesh O, Aldridge-Gerry A, Zeitzer JM, et al. Actigraphy-measured sleep disruption as a predictor of survival among women with advanced breast cancer. Sleep. 2014;37(5):837–842. doi:10.5665/sleep.3642
40. Gamaldo CE, Shaikh AK, McArthur JC. The sleep-immunity relationship. Neurol Clin. 2012;30(4):1313–1343. doi:10.1016/j.ncl.2012.08.007
41. Zimmerman ME, Aloia MS. Sleep-disordered breathing and cognition in older adults. Curr Neurol Neurosci Rep. 2012;12(5):537–546. doi:10.1007/s11910-012-0298-z
42. Ford ES, Cunningham TJ, Giles WH, Croft JB. Trends in insomnia and excessive daytime sleepiness among U.S. adults from 2002 to 2012. Sleep Med. 2015;16(3):372–378. doi:10.1016/j.sleep.2014.12.008
43. Gamaldo AA, Beydoun MA, Beydoun HA, et al. Sleep disturbances among older adults in the United States, 2002–2012: nationwide inpatient rates, predictors, and outcomes. Front Aging Neurosci. 2016;8:266. doi:10.3389/fnagi.2016.00266
44. Otte JL, Carpenter JS, Manchanda S, et al. Systematic review of sleep disorders in cancer patients: can the prevalence of sleep disorders be ascertained? Cancer Med. 2015;4(2):183–200. doi:10.1002/cam4.356
45. Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
46. Wondie Y, Mehnert A, Hinz A, Frey R. The Hospital Anxiety and Depression Scale (HADS) applied to Ethiopian cancer patients. PLoS One. 2020;15(12):e0243357. doi:10.1371/journal.pone.0243357
47. Mendoza TR, Zhao F, Cleeland CS, Wagner LI, Patrick-Miller LJ, Fisch MJ. The validity and utility of the M. D. Anderson Symptom Inventory in patients with breast cancer: evidence from the symptom outcomes and practice patterns data from the eastern cooperative oncology group. Clin Breast Cancer. 2013;13(5):325–334.
48. Eticha T, Kidane F. The prevalence of and factors associated with current smoking among College of Health Sciences students, Mekelle University in Northern Ethiopia. PLoS One. 2014;9(10):e111033. doi:10.1371/journal.pone.0111033
49. Yeshaw Y, Zerihun MF. Khat chewing prevalence and correlates among university staff in Ethiopia: a cross-sectional study. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4706-1
50. Getachew T, Defar A, Teklie H, et al. Magnitude and predictors of excessive alcohol use in Ethiopia: findings from the 2015 national non-communicable diseases STEPS survey. Ethiop J Health Dev. 2017;31(1):312–319.
51. Götze H, Ernst J, Brähler E, Romer G, von Klitzing K. Predictors of quality of life of cancer patients, their children, and partners. Psycho‐Oncology. 2015;24(7):787–795. doi:10.1002/pon.3725
52. Weir CB, Jan A. BMI Classification Percentile and Cut off Points. StatPearls [Internet]; 2019.
53. Corkery JM, Schifano F, Oyefeso A, et al. Overview of literature and information on “khat-related” mortality: a call for recognition of the issue and further research. Ann Ist Super Sanita. 2011;47:445–464. doi:10.4415/ANN_11_04_17
54. The WHO. WHO STEPwise Approach to Noncommunicable Disease Risk Factor Surveillance (STEPS). Geneva: World Health Organization; 2015.
55. Beck SL, Schwartz AL, Towsley G, Dudley W, Barsevick A. Psychometric evaluation of the Pittsburgh sleep quality index in cancer patients. J Pain Symptom Manage. 2004;27(2):140–148. doi:10.1016/j.jpainsymman.2003.12.002
56. Salahuddin M, Maru TT, Kumalo A, Pandi-Perumal SR, Bahammam AS, Manzar MD. Validation of the Pittsburgh sleep quality index in community dwelling Ethiopian adults. Health Qual Life Outcomes. 2017;15(1):58. doi:10.1186/s12955-017-0637-5
57. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
58. Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the MD Anderson Symptom Inventory. Cancer. 2000;89(7):1634–1646. doi:10.1002/1097-0142(20001001)89:7<1634::AID-CNCR29>3.0.CO;2-V
59. Anshabo AT, Migbaru S, Mulu A, et al. Validation of the amharic version of the MD Anderson Symptom Inventory and assessment of symptoms in Ethiopian cancer patients. J Pain Symptom Manage. 2016;51(5):947–953. doi:10.1016/j.jpainsymman.2015.12.333
60. Meltzer H, Nosikov A, Gudex C. Developing common instruments for health surveys. EUROHIS. 2003:35–60.
61. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–656. doi:10.1097/00000421-198212000-00014
62. Hosmer DW Jr, Lemeshow S, Sturdivant RX. Applied Logistic Regression. John Wiley & Sons; 2013.
63. Hanna TP, Kangolle AC, Hanna TP, Kangolle ACT. Cancer control in developing countries: using health data and health services research to measure and improve access, quality and efficiency. BMC Int Health Hum Rights. 2010;10(1):24. doi:10.1186/1472-698X-10-24
64. Wu YH, Swaab DF. The human pineal gland and melatonin in aging and Alzheimer’s disease. J Pineal Res. 2005;38(3):145–152.
65. Mansano-Schlosser TC, Ceolim MF. Factors associated with poor sleep quality in women with cancer. Rev Lat Am Enfermagem. 2017;25:e2858. doi:10.1590/1518-8345.1478.2858
66. Nutt D, Wilson S, Paterson L. Sleep disorders as core symptoms of depression. Dialogues Clin Neurosci. 2008;10(3):329–336. doi:10.31887/DCNS.2008.10.3/dnutt
67. Palesh OG, Collie K, Batiuchok D, et al. A longitudinal study of depression, pain, and stress as predictors of sleep disturbance among women with metastatic breast cancer. Biol Psychol. 2007;75(1):37–44. doi:10.1016/j.biopsycho.2006.11.002
68. Yennurajalingam S, Balachandran D, Cardozo SLP, et al. Patient-reported sleep disturbance in advanced cancer: frequency, predictors and screening performance of the Edmonton Symptom Assessment System sleep item. BMJ Support Palliat Care. 2017;7(3):274–280.
69. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–1552. doi:10.1016/j.jpain.2013.08.007
70. Kalmbach DA, Cuamatzi-Castelan AS, Tonnu CV, et al. Hyperarousal and sleep reactivity in insomnia: current insights. Nat Sci Sleep. 2018;10:193–201. doi:10.2147/NSS.S138823
71. Eric Suni AD; Sleep Foundation; A One Care Media Company. Anxiety and sleep; 2022 [updated March 11, 2022; cited March 23, 2022]. Available from: https://www.sleepfoundation.org/mental-health/anxiety-and-sleep.
72. Monas L, Csorba S, Kovalyo M, et al. The relationship of sleep disturbance and symptom severity, symptom interference, and hospitalization among Israeli inpatients with cancer. Oncol Nurs Forum. 2012;39(4):E361–E372. doi:10.1188/12.ONF.E361-E372
73. Akyuz RG, Ugur O, Elcigil A. Sleep quality in lung cancer patients. Asian Pac J Cancer Prev. 2013;14(5):2909–2913. doi:10.7314/APJCP.2013.14.5.2909
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.