")
Back to Journals » Medical Devices: Evidence and Research » Volume 11
Sleep-disordered breathing and reaction time in children
Authors Hakim M , Shafy SZ, Miller R , Jatana KR, Splaingard M , Tumin D, Tobias JD , Raman VT
Received 6 September 2018
Accepted for publication 10 October 2018
Published 12 December 2018 Volume 2018:11 Pages 413—417
DOI https://doi.org/10.2147/MDER.S186647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammed Hakim,1 Shabana Zainab Shafy,1 Rebecca Miller,1 Kris R Jatana,2 Mark Splaingard,3 Dmitry Tumin,1 Joseph D Tobias,1,4 Vidya T Raman1,4
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Pediatric Otorhinolaryngology, Nationwide Children’s Hospital, Columbus, OH, USA; 3Department of Sleep Disorders Centre, Nationwide Children’s Hospital, Columbus, OH, USA; 4Department of Anesthesiology & Pain Medicine, Ohio State University, Columbus, OH, USA
Background: The incidence of obstructive sleep apnea (OSA) and sleep-disordered breathing (SDB) in children exceeds the availability of polysomnography (PSG) to definitively diagnose OSA and identify children at higher risk of perioperative complications. As sleep deficits are associated with slower reaction times (RTs), measuring RT may be a cost-effective approach to objectively identify SDB symptoms.
Aim: The aim of this study is to compare RT on a standard 10-minute psychomotor vigilance test (PVT) based on children’s history of OSA/SDB.
Methods : Children, 6–11 years of age, were enrolled from two different clinical groups. The SDB group included children undergoing adenotonsillectomy with a clinical history of SDB, OSA, or snoring. The control group included children with no history of SDB, OSA, or snoring who were scheduled for surgery other than adenotonsillectomy. RT was measured via 10-minute PVT (Ambulatory Monitoring Inc., Ardsley, NY, USA). Median RT was calculated for each patient based on all responses to stimuli during the PVT assessment and was compared to published age-sex-specific norms. The proportion of children exceeding RT norms was compared between study groups.
Results: The study included 72 patients (36/36 male/female, median age 7 years), 46 with SDB and 26 without SDB. There was no difference in the RT between the two groups. Fifty-four percent of patients with SDB exceeded norms for median RT vs 42% of control patients (95% CI of difference: – 12, 36; P=0.326).
Conclusion: Approximately half of the patients in both groups exceeded published norms for median RT on PVT. Despite its convenience, measurement of RT did not distinguish between patients with probable SDB/OSA for preoperative risk stratification.
Keywords: psychomotor vigilance test, obstructive sleep apnea, anesthesia, polysomnography, sleep-disordered breathing
Introduction
Sleep-disordered breathing (SDB) and obstructive sleep apnea (OSA) are characterized by brief intervals of decreased air movement caused by collapse of the pharynx or restriction of the upper airway resulting in apnea or hypopnea, respectively.1 The prevalence of the two disorders from published data has ranged from 2% to 20% depending on study types, surveys, and the various definitions employed.2,3 This prevalence exceeds the availability of the routine use of polysomnography (PSG) to definitively diagnose OSA or SDB and identify patients at higher risk of perioperative complications or those who require postoperative inpatient monitoring. In adults, established preoperative screening questionnaires for OSA have been developed and validated.4 However, these guidelines do not translate to the pediatric population as the clinical presentation, PSG findings, and modes of treatment may vary from adults.5 Although PSG is considered the gold standard in establishing the diagnosis of OSA, less expensive and less time-intensive methods such as questionnaire tools have been sought to enhance preoperative screening for OSA/SDB.6,7 While the majority of research in this area has focused on subjective caregiver-reported symptoms of OSA/SDB or anthropometric measurement such as body mass index (BMI) and neck circumference (NC), objective measures of alertness may provide an additional way of rapidly identifying children with suspected OSA/SDB as these disorders may adversely affect behavioral and neurocognitive functioning.7,8
The psychomotor vigilance test (PVT) has been used extensively in sleep research to objectively measure deficits in alertness and sustained attention. Because sleep deficits are associated with slower reaction times (RTs) on PVT, measuring RT may be a cost-effective option to determine the presence of SDB in children presenting for surgery. We prospectively measured RT using the PVT in children with a history of OSA/SDB symptoms (eg, snoring). This was compared to a control group of children with no history or clinical signs of OSA/SDB and to published age-sex-specific norms for RT.9 Our primary hypothesis was that children with SDB would have longer RTs (indicating lower alertness) compared to children without SDB, and would be more likely to exceed previous published RT normative values.
Methods
After approval by the Institutional Review Board which is affiliated to Nationwide Children’s Hospital, this prospective observational study was conducted at a single institution (Nationwide Children’s Hospital, Columbus, OH, USA) in accordance with the principles of the Declaration of Helsinki. The study was registered at http://clinicaltrials.gov (NCT02053012), and written informed consent was obtained from the patients’ parent or caregiver. Children, 6–11 years of age, were enrolled into the SDB group or the control group. The SDB group included children undergoing adenotonsillectomy with a history and clinical signs of SDB, OSA, or snoring. The control group included children undergoing any procedure other than adenotonsillectomy, with no history of SDB, OSA, or snoring. Snoring was used as a primary exclusion criterion. Children were excluded from the SDB group if their caregivers did not report snoring at least three times a week. Similarly, children were excluded from the control group if their caregivers reported snoring at least three times a week. Children who were unable to understand instructions or perform the PVT test were excluded. Also, children with any psychiatric condition or on psychotropic medications were excluded from our study.
The PVT instrument (Ambulatory Monitoring Inc.) is a handheld, self-contained system used for repetitive RT measurements. Over a period of 10 minutes, patients were instructed to respond to a visual stimulus presented at a variable interval (2,000–10,000 ms) by pressing either the right or left button on the device with the thumb of the dominant hand. If the subjects pressed the button prior to the display of the visual stimulus, a “false start” message was displayed. If the button was not released after 3 seconds, a reminder message was displayed. The cognitive assessment was performed in our standard preoperative holding rooms in the presence of parents or caregivers. These rooms are private with the ability to close door to ensure privacy and quiet. Patients and their family were briefed about the PVT. Parents remained in the room during testing.
The primary outcome was the subject’s median RT (calculated over all responses to device stimuli during the test) and whether this median RT exceeded normative thresholds according to gender and age.10 Secondary outcomes included the subjects’ mean RT across all trials (ie, average of RTs across all stimuli during the test). Other data collected included demographic and anthropometric details of the patient (gender, age, height, weight, BMI, and NC) and caregiver-reported current SDB symptoms (eg, history of snoring, heavy or loud breathing, mouth breathing, daytime sleepiness, and behavioral complaints from school).
Due to a lack of preliminary data on RT in children with and without SDB, 32 children with SDB were initially enrolled out of a planned total of 50 children in this group. An interim analysis was then performed to determine the incidence of exceeding median RT norms. Based on an interim finding that 72% children with SDB exceeded normative median RT on PVT, we hypothesized that no more than 36% of children without SDB would exceed the norm. The addition of a control group with 30 subjects was deemed to attain >80% power for demonstrating this difference on a 2-sample test of proportions. Therefore, enrollment in the study continued with the aim of enrolling 50 children with SDB and 30 children without SDB. Continuous variables were expressed as a median and IQR, and categorical variables were expressed as a count and percentage. Characteristics were compared between study groups (stratified on known history of SDB/OSA) using chi-squared tests, Fisher’s exact tests, tests of independent proportions for categorical data, and rank-sum tests for continuous data. Data analysis was performed in Stata/IC 14.2 (StataCorp LP, College Station, TX, USA), and P<0.05 was considered statistically significant.
Results
The study enrolled 80 patients, of whom 50 had a history of SDB symptoms and 30 were controls. We excluded four patients from the SDB group due to snoring not being reported at the time of data collection, and we excluded four patients from the control group due to snoring being reported on the caregiving questionnaire. The remaining 72 patients (36 males, 36 females) had a median age of 7 years (IQR: 6, 9), a median BMI of 18 kg/m2 (IQR: 16, 25), and a median NC of 29 cm (IQR: 27, 33). Median RT was 440 ms (IQR: 363, 559) and mean RT was 533 ms (IQR: 389, 752). In the SDB group, the most common SDB symptoms reported at the time of study participation included loud breathing (95%), breathing through the mouth (84%), and having a dry mouth in the morning (83%), whereas not waking up feeling refreshed was reported for only 64% of patients. SDB-associated symptoms reported for children with no prior history of OSA/SDB were most commonly being hard to wake up in the morning (31%), breathing through the mouth (22%), and having a dry mouth in the morning (18%), although none of the children included in the control group for our data analysis were reported by caregivers to snore three or more times a week.
Patient characteristics and PVT performance are summarized in accordance with study groups in Table 1. The likelihood of exceeding median RT norms did not differ significantly between study groups. In the SDB group, 54% of SDB patients exceeded median RT norms compared to 42% of control patients (95% CI of difference: –12, 36; P=0.326). When evaluating continuous RT data, median RT in the SDB group was 437 ms as compared to 445 ms in the control group (95% CI of difference: –88, 39; P=0.389). Results were consistent when analyzing the mean RT, rather than the median RT during the 10-minute PVT session.
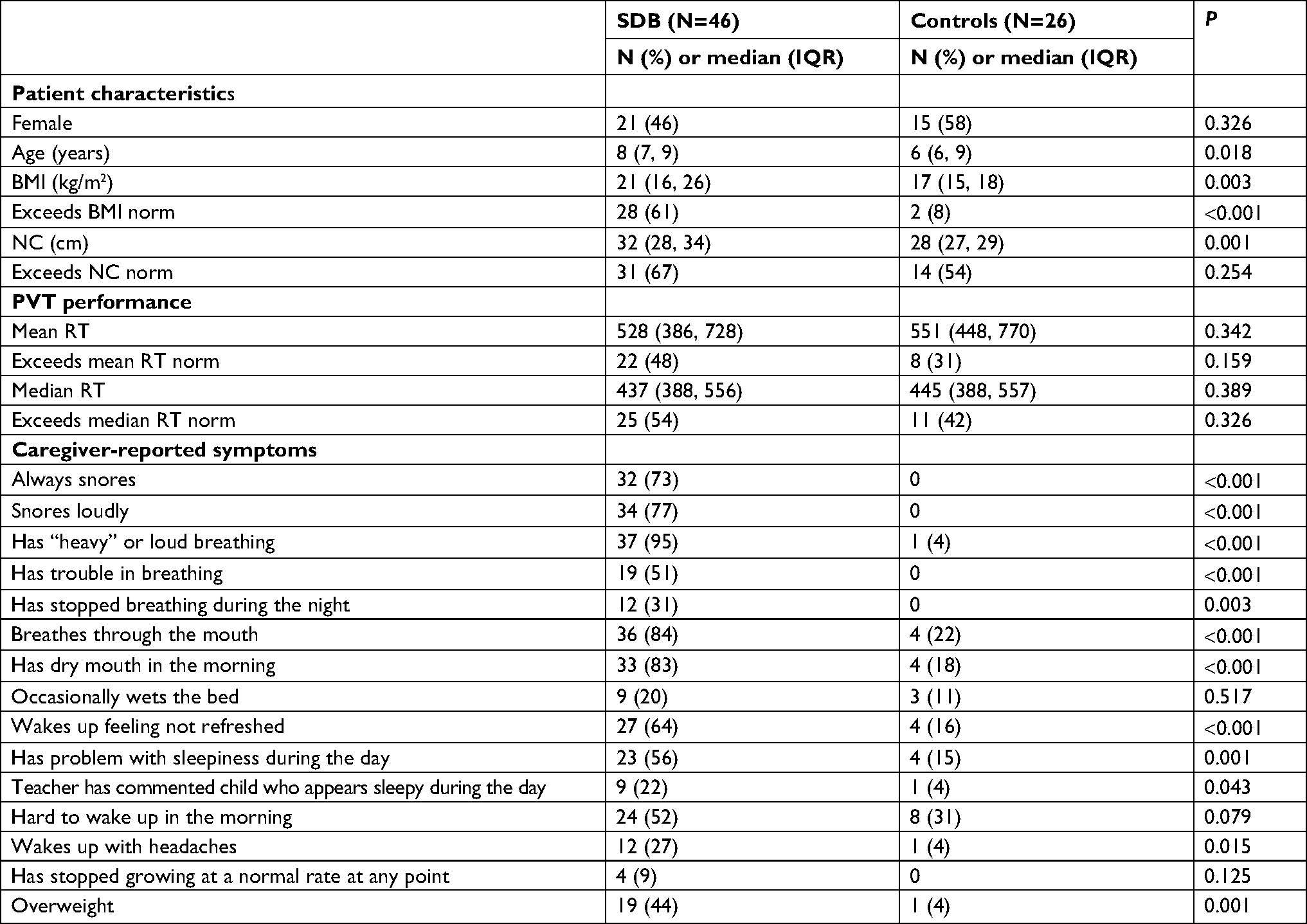 | Table 1 Patient characteristics according to history of SDB, OSA, or snoring Abbreviations: SDB, sleep-disordered breathing; OSA, obstructive sleep apnea; BMI, body mass index; NC, neck circumference; PVT, psychomotor vigilance test; RT, reaction time. |
Discussion
SDB in children can present with a broad clinical spectrum, ranging from excessive daytime sleepiness, snoring, upper airway resistance syndrome, and OSA–hypopnea syndrome.10 All of these features can negatively affect the behavioral and cognitive functioning of children, ultimately leading to neurodevelopmental delay and reduced school performance.4 However, there can be multiple contributors to a presenting symptom in a given patient. Various etiological factors can range from anatomical abnormalities (obstruction, decreased tone, and reduced patency of upper airway); allergies; adenoid and tonsillar hypertrophy; and especially, obesity.11 While symptoms of pediatric OSA/SDB are considered to be linked to lower daytime alertness, our prospective study found no evidence that the standard PVT assessment of RT can be used to distinguish children with a history of OSA/SDB from children not known to have OSA, SDB, or snoring problems.
PSG remains the current gold standard test used to diagnose sleep disorders, whereas the PVT is much shorter and less resource-intensive test that can be used to assess the alertness and response time of patients. The simple PVT can characterize attention and cognition issues in sleep-deprived children. It measures the speed of response of subjects to a visual stimulus using reaction-timed tasks. Because performance on PVT reflects an individual’s arousal and attentiveness, the change in RTs between sessions can vary based on sleep deprivation and other factors that affect wakefulness. In adults, it has been demonstrated that the performance of PVT is independent of aptitude, which makes it an ideal technique for repetitive testing and comparisons in both within-person and between-persons scenarios.12 The use of PVT to assess sleepiness in adults was recommended in a study by Batool-Anwar et al, while another study described that SDB specifically during non-rapid eye movement sleep was associated with performance on PVT.13
Performance on PVT is meant to reflect the alertness of the individual being tested and can be used as a measure of sleep deprivation.12 However, the arousal state of the individual may introduce error into PVT measurements.14,15 This source of error could be especially relevant in children presenting for surgery, who are likely experiencing distraction and sleep deprivation due to disruption of their daily routine with early morning awakening, sleeping in an unfamiliar environment the night prior to surgery, travel to an unfamiliar location, and fasting before surgery. In the current study, we found that approximately half of the patients in both groups, regardless of known SDB/OSA history, exceeded published norms for RT on PVT. Therefore, our preliminary data suggest that measurement of RT is insufficiently sensitive for preoperative risk stratification, when the presence and severity of OSA or SDB are uncertain. One of the limitations of our study is the relatively smaller numbers in the study cohort. Future studies may need to include larger numbers of children to further validate our preliminary findings. It is worthwhile to continue to investigate non-invasive and less expensive modalities to risk stratify children with undiagnosed OSA/SDB presenting for general anesthesia and surgical procedures.
Conclusion
We found that approximately half of children presenting for surgery exceeded published norms for RT on a standard PVT, regardless of OSA/SDB or snoring. RT deficits were common in both groups. It may be that normal preoperative stressors such as traveling to the hospital, preoperative preparation including early morning awakening, and fear of the unknown contributed to RT deficits rendering it a less sensitive test to detect OSA/SDB. It remains to be seen whether RT measurement at home, or at another clinical encounter (eg, at the time of scheduling the surgery) could be more useful for identifying children with suspected OSA/SDB. In the preoperative setting, other noninvasive tools apart from PVT should be considered for risk stratification of children with suspected OSA/SDB.
Disclosure
Dr Raman is a member of the Society of Anesthesia and Sleep Medicine. Dr Jatana is an expert consultant for Intertek Product Intelligence. The authors report no other conflicts of interest in this work.
References
Goodwin JL, Enright PL, Kaemingk KL, et al. Feasibility of using unattended polysomnography in children for research – report of the Tucson Children’s Assessment of Sleep Apnea study (TuCASA). Sleep. 2001;24(8):937–944. | ||
Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217–1239. | ||
Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242–252. | ||
Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812–821. | ||
Rosen CL, D’Andrea L, Haddad GG. Adult criteria for obstructive sleep apnea do not identify children with serious obstruction. Am Rev Respir Dis. 1992;146(5 Pt 1):1231–1234. | ||
Meltzer LJ, Hiruma LS, Avis K, Montgomery-Downs H, Valentin J. Comparison of a commercial accelerometer with polysomnography and actigraphy in children and adolescents. Sleep. 2015;38(8):1323–1330. | ||
Raman VT, Splaingard M, Tumin D, Rice J, Jatana KR, Tobias JD. Utility of screening questionnaire, obesity, neck circumference, and sleep polysomnography to predict sleep-disordered breathing in children and adolescents. Paediatr Anaesth. 2016;26(6):655–664. | ||
Owens JA. Neurocognitive and behavioral impact of sleep disordered breathing in children. Pediatr Pulmonol. 2009;44(5):417–422. | ||
Venker CC, Goodwin JL, Roe DJ, Kaemingk KL, Mulvaney S, Quan SF. Normative psychomotor vigilance task performance in children ages 6 to 11 – the Tucson Children’s Assessment of Sleep Apnea (TuCASA). Sleep Breath. 2007;11(4):217–224. | ||
Basner M, Dinges DF. Maximizing sensitivity of the psychomotor vigilance test (PVT) to sleep loss. Sleep. 2011;34(5):581–591. | ||
Rosen CL, Storfer-Isser A, Taylor HG, Kirchner HL, Emancipator JL, Redline S. Increased behavioral morbidity in school-aged children with sleep-disordered breathing. Pediatrics. 2004;114(6):1640–1648. | ||
Dorrian J, Rogers NL, Dinges DF. Psychomotor vigilance performance: a neurocognitive assay sensitive to sleep loss. In: Kushida C, editor. Sleep Deprivation: Clinical Issues, Pharmacology, and Sleep Loss Effects. New York: Marcel Dekker, Inc; 2005:39–70. | ||
Batool-Anwar S, Kales SN, Patel SR, Varvarigou V, DeYoung PN, Malhotra A. Obstructive sleep apnea and psychomotor vigilance task performance. Nat Sci Sleep. 2014;6:65–71. | ||
Graw P, Kräuchi K, Knoblauch V, Wirz-Justice A, Cajochen C. Circadian and wake-dependent modulation of fastest and slowest reaction times during the psychomotor vigilance task. Physiol Behav. 2004;80(5):695–701. | ||
Wyatt JK, Ritz-De Cecco A, Czeisler CA, Dijk DJ. Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day. Am J Physiol. 1999;277(4 Pt 2): R1152–R1163. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.