")
Back to Journals » Nature and Science of Sleep » Volume 15
Sleep Apnea Detection by Tracheal Motion and Sound, and Oximetry via Application of Deep Neural Networks
Authors Montazeri Ghahjaverestan N , Aguiar C, Hummel R, Cao X, Yu J, Bradley TD
Received 11 November 2022
Accepted for publication 24 April 2023
Published 30 May 2023 Volume 2023:15 Pages 423—432
DOI https://doi.org/10.2147/NSS.S397196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ahmed BaHammam
Nasim Montazeri Ghahjaverestan,1,2 Cristiano Aguiar,3 Richard Hummel,3 Xiaoshu Cao,4,5 Jackson Yu,3 T Douglas Bradley2,3,5,6
1Sleep and Brain Health Laboratory, Sunnybrook Research Institute, Toronto, Ontario, Canada; 2Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada; 3Bresotec Inc, Toronto, Ontario, Canada; 4Institute of Biomedical Engineering, University of Toronto, Toronto, Ontario, Canada; 5KITE, Toronto Rehabilitation Institute, University Health Network, Toronto, Ontario, Canada; 6Department of Medicine of the University Health Network, Toronto General Hospital, Toronto, Ontario, Canada
Correspondence: T Douglas Bradley, University Health Network Toronto General Hospital, Room 9N-943, 200 Elizabeth Street, Toronto, ON, M5G 2C4, Canada, Tel +416-340-4719, Fax +416-340-4197, Email [email protected]
Purpose: Sleep apnea (SA) is highly prevalent, but under diagnosed due to inaccessibility of sleep testing. To address this issue, portable devices for home sleep testing have been developed to provide convenience with reasonable accuracy in diagnosing SA. The objective of this study was to test the validity a novel portable sleep apnea testing device, BresoDX1, in SA diagnosis, via recording of trachea-sternal motion, tracheal sound and oximetry.
Patients and Methods: Adults with a suspected sleep disorder were recruited to undergo in-laboratory polysomnography (PSG) and a simultaneous BresoDX1 recording. Data from BresoDX1 were collected and features related to breathing sounds, body motions and oximetry were extracted. A deep neural network (DNN) model was trained with 61-second epochs of the extracted features to detect apneas and hypopneas from which an apnea-hypopnea index (AHI) was calculated. The AHI estimated by BresoDX1 (AHIbreso) was compared to the AHI determined from PSG (AHIPSG) and the sensitivity and specificity of SA diagnosis were assessed at an AHIPSG ≥ 15.
Results: Two-hundred thirty-three participants (mean ± SD) 50 ± 16 years of age, with BMI of 29.8 ± 6.6 and AHI of 19.5 ± 22.7, were included. There was a strong relationship between AHIbreso and AHIPSG (r = 0.91, p < 0.001). SA detection for an AHIPSG ≥ 15 was highly sensitive (90.0%) and specific (85.9%).
Conclusion: We conclude that the DNN model we developed via recording and analyses of trachea-sternal motion and sound along with oximetry provides an accurate estimate of the AHIPSG with high sensitivity and specificity. Therefore, BresoDX1 is a simple, convenient and accurate portable SA monitoring device that could be employed for home SA testing in the future.
Keywords: sleep apnea, portable sleep testing, tracheal acoustics
Introduction
Sleep apnea (SA) is a chronic condition characterized by repetitive cessations (apnea), or reductions (hypopnea) in breathing resulting in recurrent hypoxia and arousals from sleep. Despite the high prevalence in the general population (approximately 10%),1,2 SA is underdiagnosed.3 One reason for this is that standard diagnostic overnight, polysomnography (PSG), is costly, relatively inaccessible and, because it requires an overnight stay in a sleep laboratory, is inconvenient for patients.4 To address this diagnostic deficiency, several portable sleep apnea monitoring devices have been developed for home use. Despite having reasonable accuracy in identifying subjects with SA, such devices can be less accurate and reliable in detecting apneas and hypopneas than PSG.5
Portable devices generally use nasal pressure cannulae for measuring airflow, respiratory inductance plethysmography (RIP) or piezo-electric crystals for measuring respiratory motion and finger oximetry to measure arterial oxyhemoglobin saturation (SaO2) to detect respiratory events. However, during unattended sleep monitoring at home, nasal cannulae, respiratory bands and oximeters can be displaced so that signals may either be inconsistent or lost. Another potential and convenient means of assessing respiratory motion and airflow is through recording of tracheal motion and breath sounds.6 These can be assessed by securing an accelerometer and a microphone over the trachea in the suprasternal notch to measure trachea-sternal movements and tracheal sounds, respectively. Previous studies have shown that the apnea-hypopnea index (AHI) can be estimated using only tracheal sounds,7–9 tracheal motion,9–13 or both7,14 in relatively small numbers of subjects with reasonable accuracy, but not in sufficient numbers to provide reliable diagnoses in the clinical setting.
We have recently demonstrated that the analysis of trachea-sternal motion and breath sounds can provide a very accurate estimate of respiratory motion, as assessed by RIP, and changes in airflow, as assessed by nasal pressure, during both wakefulness and sleep.15 In that study, we also showed that the accuracy of detecting changes in airflow was highest during apneas and hypopneas. The objective of the present study was to develop a method to accurately detect SA by recording trachea-sternal motion and sound, along with SaO2 and subjecting these signals to deep neural networks (DNNs) with high computing potential.16 Recent advances in artificial intelligence approaches, especially development of DNNs, have led to their extensive use in health-care applications and specifically increasing the accuracy of diagnostic sleep apnea testing.17 We employed these techniques to estimate AHI in a larger population than in previous studies using similar technology. This work has not been published elsewhere except as an abstract at the Sleep Meeting in 2022.
Materials and Methods
Subjects
Men and women aged 18 years and above who were referred to the University Health Network (UHN) sleep laboratories for assessment of a possible sleep disorder were included in this study. In-hospital patients, those with self-reported neuromuscular disorders, obesity hypoventilation, chronic obstructive pulmonary disease, heart failure and subjects who were not fluent in English were excluded. The study was approved by the Research Ethics Board of the University Health Network (IRB #: 17–6258 and 19–5601). All participants provided written informed consent prior to participation. The study complied with the Declaration of Helsinki.
Measurements
Polysomnography
Participants underwent an overnight PSG, from which sleep stages, arousals, apneas, and hypopneas were scored by technicians, blinded to the results of our portable SA monitoring system (BresoDX1, Bresotec Inc., Toronto, ON, Canada) recordings, according to the American Academy of Sleep Medicine (AASM) guidelines version 2.6.18 Airflow was measured using a nasal cannula, thoracoabdominal movements by RIP, and SaO2 by a pulse oximeter. Apnea was defined as a ≥90% reduction in the airflow for ≥10 seconds. Hypopnea was defined as 30% to 89% reduction in the airflow with either ≥3% oxygen desaturation and/or terminated by a cortical arousal. All signals were recorded on a computerized system (Embla® S4500, Natus Medical Incorporated, Middleton, WI, USA).
Tracheal Signals
Simultaneous to PSG, trachea-sternal motion and tracheal sound were recorded by a 3-dimensional accelerometer and a microphone, respectively, embedded in a small module, BresoDX1, attached to the suprasternal notch with adhesive tape (Figure 1). Tracheo-sternal motion and sound were recorded at 100 and 8000 Hz, respectively, and were transmitted by Wi-Fi to the data collection unit placed on a bedside table A finger pulse oximeter (Nonin 3150 WristOx2® pulse oximeter-K102350, Plymouth, MN, USA) recorded SaO2 data and transmitted them to the data collection unit via Bluetooth (Figure 1). The BresoDX1 recordings were synchronized to the PSG recording.
 |
Figure 1 The BresoDX1 and its computing module, which simultaneously collects trachea-sternal motion and tracheal sound from the BresoDX1 and SaO2 from the pulse oximeter. |
Data Analysis
The BresoDX1 data and apneas and hypopneas scored on PSG recordings were analyzed by Python software to develop a machine learning algorithm. The model was designed to use trachea-sternal motion, tracheal sound, and oximetry data to detect apneas and hypopneas. From apneas and hypopneas detected by BresoDX1, the AHI was estimated (AHIbreso), blinded to the AHI scored from the PSG, and then compared to the PSG-based AHI (AHIPSG).
Preprocessing
Trachea-sternal motion (the three dimensions measured by the accelerometer were, x: cranio-caudal, y: transverse, z: postero-anterior) and tracheal sound were filtered using five-order zero-phase bandpass Butterworth filters with 0.2–5 Hz and 200–2000 Hz bandwidths, respectively. Then, the filtered signals were down-sampled to 10 Hz and deemed movement signals. To remove abrupt changes in the baseline of the signals due to changes in position and motion artifacts, the signals were segmentally normalized between their 2nd and 98th percentiles. (See the On-line Supplement for more details). The SaO2 signal was smoothed by a fifth-order median filter. The drops in the smoothed SaO2 (desaturations) were identified if: i) the drop occurred at least 10 seconds after the previous drop, if there was any, ii) the time between the baseline before the drop and nadir of the drop (dropdepth) was between 2 and 60 seconds, iii) the baseline after the drop occurred at least 1 second after minimum level of the drop, otherwise the drop was not considered to be due to an apnea or hypopnea. Drops longer than 50 seconds were excluded.
Feature Extraction
From the filtered trachea-sternal motion, tracheal sound and the drops in SaO2, a set of features was extracted within a ten-second window which moved second by second, deemed an extraction window. The features were as follows:
Trachea-Sternal Motion
From the 3-dimensional accelerometer: 1) the sum of the three motions (motionsum), and 2) the rotational angles defined as [θ = arctan (-x/(y2 + z2)0.5), φ = arctan (y/z)] were extracted.
Tracheal Sound
In order to detect breathing sounds in a manner similar to the human ear,19 first, Mel-frequency cepstral coefficients (MFCC; 24 features) were extracted from the filtered sound. The more audible the breathing sounds, the greater the MFCCs that are obtained. Additionally, the signal to noise ratio (SNR), as the second feature, was determined based on the improved minima controlled recursive averaging technique (IMCRA).20 In IMCRA, first the periodogram of tracheal sound was calculated. Then, the noise power was estimated for each frequency bin by controlled recursive averaging of the local minima. Finally, signal power was calculated by spectral subtraction of the estimated noise power from the spectral content of the sound. Signals were identified as breathing and snoring sounds, and were separated from non-white and time-variant background noise.
Oximetry
From the oximeter: 1) the occurrence of a drop in SaO2 of ≥3% within a duration of 10 to 50 seconds, 2) the dropdepth; and 3) the slope of the drop, ie, dropdepth over the length of the drop (dropslope) were calculated. Figure 2 illustrates how the SaO2 signal was analyzed. If there was no drop in SaO2, this was considered zero.
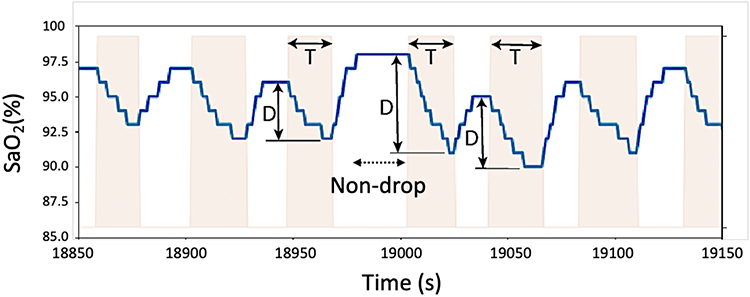 |
Figure 2 Features extracted from oximetry, including SaO2 dropdepth (D), drop duration (T) and dropslope = D/T. |
For each of the features extracted within the extraction moving window, the root of the arithmetic mean of the squared values (RMS), the 5th and 95th percentiles, inter-quartile range (IQR) derived as the difference between the 75th and 25th percentiles, and median were calculated and fed into a machine learning algorithm, which detected the respiratory events.
Event Detection
To detect respiratory events, the above-described features were extracted within a detection window of 61 seconds moving second by second and used as the input of a mathematical model. The model classified each 61-second window into event or non-event. The model includes two DNNs, one for detecting spontaneous (short-term) changes in the extracted features (DNN1) and another for detecting long-term changes (DNN2) that were presumably associated with respiratory events and their iterations (See the On-line Supplementary for further details). In our previous work,21 we developed an algorithm, based on tracheal recordings, in which body movements associated with wakefulness could be detected, and deemed in-valid recording time, while periods in which body movements were low acted as a surrogate for sleep that was deemed valid recording time. Accordingly, in this study, we used this algorithm to assess the amount of movements in each 30-second epoch of tracheal signals: periods of low body movements were considered valid recording time, while periods with high levels of body movements were considered non-valid recording time.
The periods of valid recording and the outputs of the two DNNs were then fed into a logistic regression model to generate the final output indicating the probability of a respiratory event’s occurrence. A threshold (Tevent) was applied to the final output to classify each second into event or non-event.
To train the models, tune the hyperparameters of the DNNs, and optimize the value of Tevent, a training set, which contained 74 of the subjects, was randomly selected. Using the training set, a four-round hold-out validation was implemented and the models that gave the best F1 score were chosen. Each fold consists of the data of subjects who were randomly selected within each AHI groups: 1) no sleep apnea: AHI <5, 2) mild sleep apnea: AHI of 5 to <15, 3) moderate sleep apnea: AHI of 15 to <30, and 4) severe sleep apnea: AHI ≥30. To optimize Tevent, precision-recall curves were used on the training set. Finally, the trained event detection algorithm was tested on the rest of the dataset (the test set, consisting of the remaining of the subjects [N = 159]).
AHI Estimation
Among the detected respiratory events, those detected during non-valid periods were removed. Then, the AHIbreso was estimated for each subject as the number of respiratory events divided by the total valid recording time.
Evaluation Metrics and Statistical Analysis
Statistical analyses were performed in R (i386 3.4.1) software. Demographic characteristics were extracted for the four AHI groups and the Analysis of Variance (ANOVA) was used to detect significant differences over groups. The performance of the event-detection algorithm was analyzed by calculating AHI from the detected events and diagnosing sleep apnea for different AHI cut-offs. Accordingly, precision, sensitivity and F1 scores were calculated for each AHI group to determine the accuracy of the event-detection. The diagnostic performance based on the four AHI cutoffs was presented with accuracy, sensitivity, specificity, F1 and precision. These metrics were reported for the detection algorithm trained by the three feature sets (tracheo-sternal motion, tracheal sound and oximetry) compared to the feature subgroups when one of the features was excluded. Also, Pearson correlation and a Bland-Altman plot were used to compare the estimated AHIbreso to the AHIPSG.
Results
Characteristics of the 233 participants are displayed in Table 1. They were, on average, middle-aged and overweight with a moderate degree of SA. Figure 3 illustrates a representative trace of BresoDX1 oximeter, sound and accelerometer signals compared to the simultaneous respiratory reference signals from a PSG during repetitive apneas.
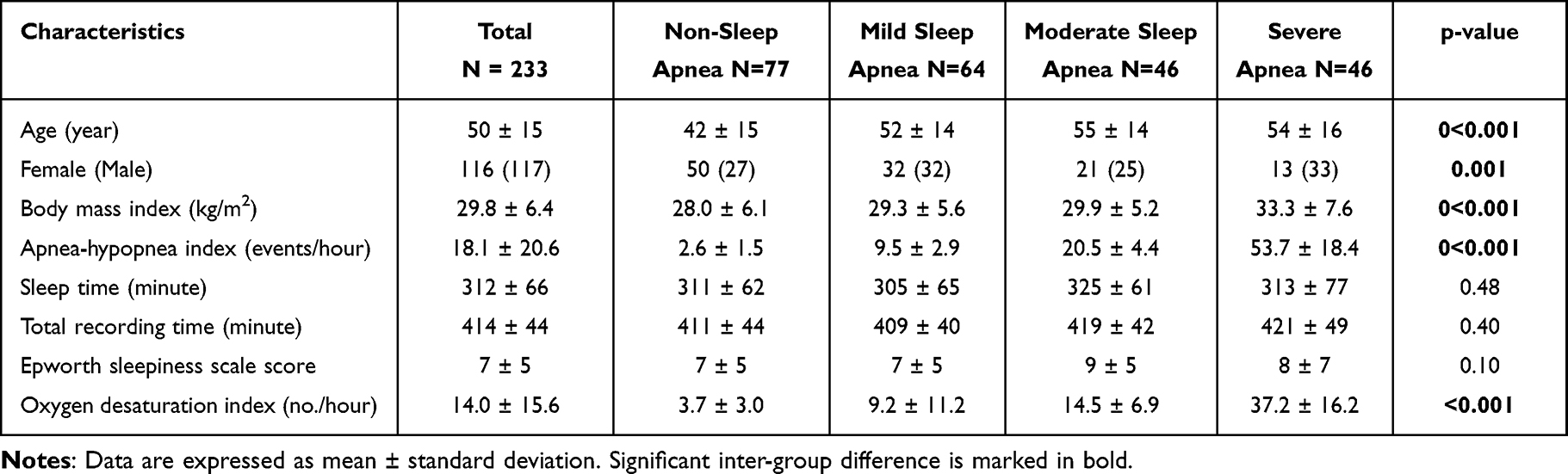 |
Table 1 Demographics |
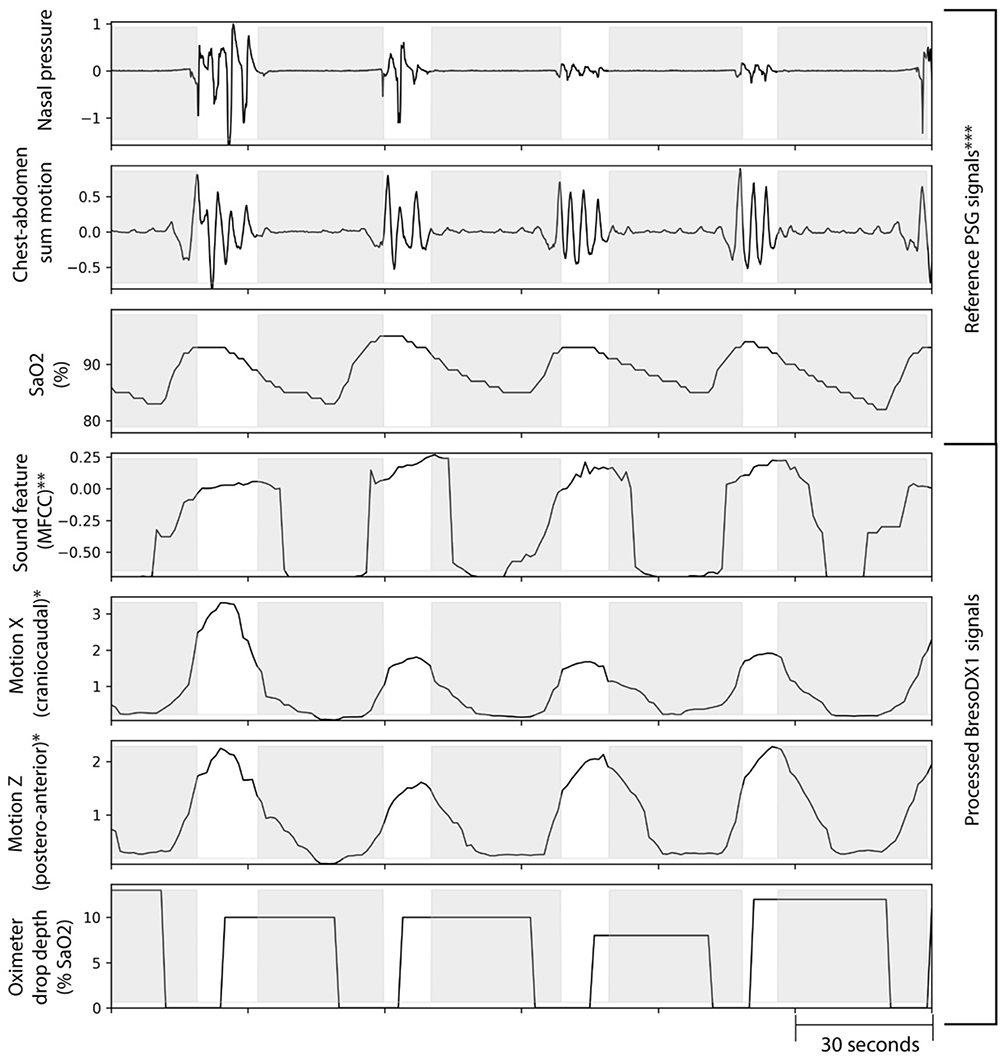 |
Figure 3 An example of extracted features from BresoDX1 recordings compared to reference nasal pressure, the sum of chest-abdominal motion and SaO2 from polysomnography (PSG) during intermittent apneas highlighted by shading. *Motion signals from BresoDX1 are normalized; **Mel-frequency cepstral coefficients (MFCC) have arbitrary units. ***Reference signals from PSG are normalized from arbitrary units. |
Figure 4 compares the events detected by BresoDX1 qualitatively with PSG-based event scores in a subject without SA (AHI = 4.0) and a subject with severe SA (AHI = 71.5).
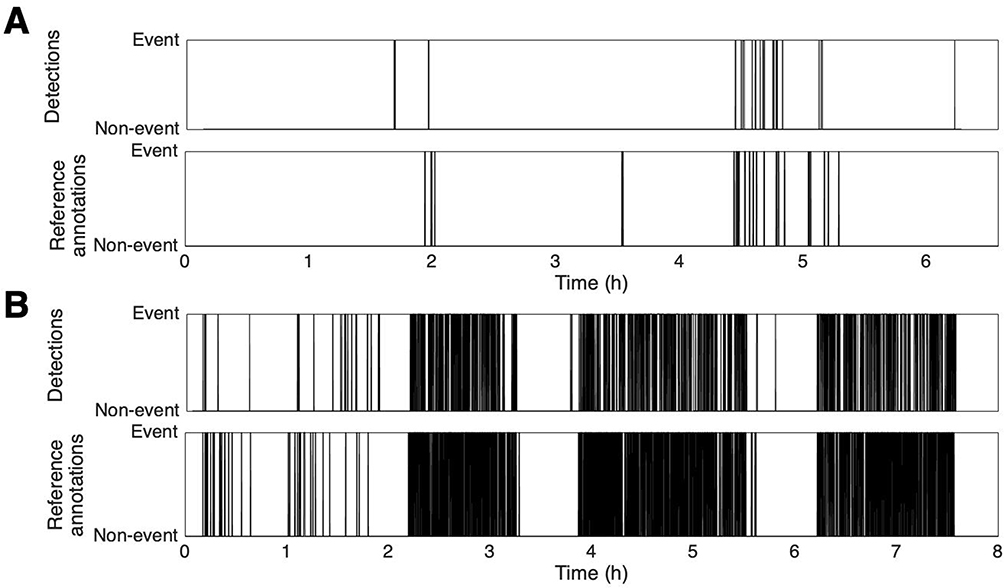 |
Figure 4 The comparison of detected events by the BresoDx1 with the reference annotated events extracted from polysomnography (PSG) in two subjects: (A) with an AHIPSG of 4, and (B) with an AHIPSG of 71.5. The corresponding AHIbreso were 3.9, and 72.5, respectively. |
There was a strong correlation between AHIbreso and AHIPSG (r = 0.91, p < 0.001, Figure 5). According to the Bland-Altman plot, the average error between AHIbreso and AHIPSG was −3 event/hour with 95% confidence interval [−12 – 15]. Table 2 presents the performance of BresoDX1 in diagnosing SA. Based on an AHI cutoff of ≥15, BresoDX1 diagnosed SA with 90.0% sensitivity, 85.9% specificity and 87.4% accuracy. Furthermore, the accuracy of BresoDX1 in diagnosing mild SA (AHI cutoff of ≥5) and severe SA (AHI cutoff of ≥30) was 84.3% and 92.5%, respectively (Table 2). Moreover, Table 2 shows ablation test reflecting the effect of each feature group in improving the accuracy of diagnosis. Overall, the results confirm that the highest accuracy occurs when the three feature groups were used in training the event-detection model.
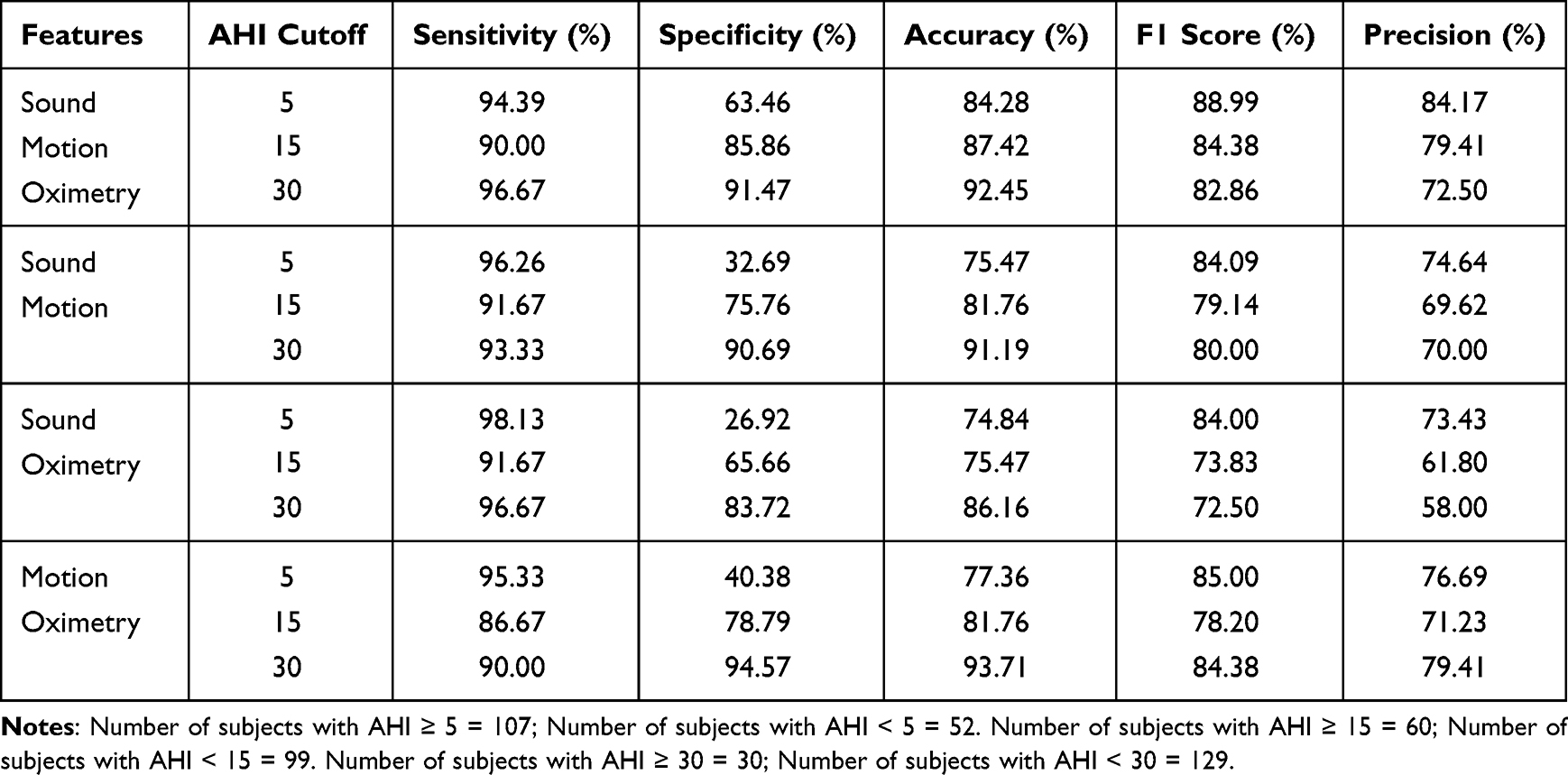 |
Table 2 Diagnosis of Sleep Apnea Based on Different AHI Cutoffs for 159 Individuals in the Test Set Using Sound, Motion and Oximetry Compared to Their Ablation Tests |
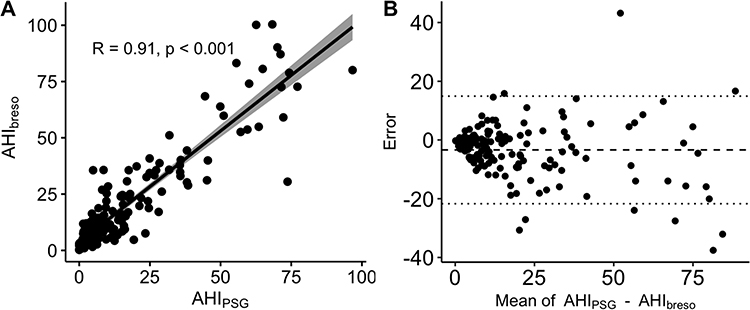 |
Figure 5 The agreement between estimated AHIbreso and the reference AHIPSG analyzed by (A): Pearson correlation, (B): Bland-Altman plot. |
Discussion
In this study, we developed a deep learning model for analyzing tracheo-sternal motions, tracheal sounds and oximetry from BresoDX1 recordings to estimate AHI and determine the severity of SA. Using this model, we were able to obtain strong agreement between the BresoDX1-based and PSG-based AHIs (r = 0.91, p < 0.001) and diagnose SA with an AHI cutoff of ≥15 with 90.0% sensitivity and 85.9% specificity and 84.4% F1 score.
In our previous study,15 using the BresoDX1 module, we demonstrated that trachea-sternal motion provided an excellent estimate of chest wall motion assessed by RIP, and a reasonably good estimate of changes in airflow assessed by nasal pressure during simultaneous PSG. However, a combination of trachea-sternal motion and tracheal sound improved the estimate of changes in PSG-measured airflow such that mean squared error was less than 5% during normal breathing and less than 2.5% during apneas and hypopneas. The closer proximity of the tracheal microphone to the airway allows more accurate detection of intraluminal airflow with higher SNR than a microphone on the chest wall even at low airflow rates.22
In the present study, we added oximetry to tracheal signals to conform to the AASM criteria18 for a hypopnea that includes a 3% or greater fall in SaO2.18 In order to integrate SaO2 measurements with trachea-sternal motion and tracheal breath sounds to detect apneas and hypopneas, we extracted several features from these signals, including dips in SaO2 over time and fed them into a mathematical model. In a previous study in which tracheal signals and SaO2 were used to detect respiratory events during sleep, the SaO2 signal was only utilized to identify regions where potential events might occur.23 Furthermore, in that study, SaO2 was recorded from a PSG oximeter, whereas in our system, SaO2 was recorded from an oximeter integrated into the BresoDX1 device.
To detect apneas and hypopneas, and diagnose SA according to AASM criteria, commercially available portable sleep monitoring devices must assess respiratory airflow or motion plus SaO2. This requires four or five points of attachment of these instruments to patients in different areas of the body and, therefore, is somewhat complicated and inconvenient. Airflow is generally assessed by nasal pressure cannulae or thermistors, while chest wall motion is generally assessed by stretchy bands that include either RIP or piezo-electric crystals.24–26 However, thermistors are quantitatively insensitive to changes in airflow, while nasal pressure is insensitive to changes in airflow during mouth breathing and can be displaced during sleep. RIP and piezo-electric crystal recordings require wearing stretchy chest and abdominal bands that are inconvenient and can be displaced during sleep, resulting in distortion or loss of signals. In addition, piezo-electric crystals’ responses to chest wall movements are non-linear, making piezo belts insensitive to hypopneas. Therefore, they are only recommended by AASM for monitoring respiratory effort and not for respiratory event scoring.18 In contrast, BresoDX1 only requires two points of attachment: the suprasternal notch and the finger, and is therefore simpler and more convenient to apply than most other home SA monitoring devices. In addition, because the trachea-sternal module is fixed in-place by adhesive tape, it is resistant to displacement during sleep, resulting a very little signal loss. Furthermore, the integration of tracheo-sternal motion and breath sounds provides a highly accurate estimation of changes in airflow17 that, in combination with oximetry, provides a highly accurate estimate of AHI and detection of SA at various AHI cut-offs compared to PSG. The advantages of BresoDX1 compared to other portable devices are its convenience and the robustness of its composite trachea-sternal motion and tracheal sound recordings to estimate changes in airflow.15 These signals along with SaO2 provide sufficient channels to detect respiratory events during sleep and estimate AHI.
To estimate AHI from the BresoDX1 recordings, the detection algorithm was developed using two DNNs. As DNN1 was trained to detect spontaneous changes in feature time-series, DNN2 took into account the long-term changes and thus was designed to take into account circulation delay between changes in SaO2 detected at the finger and tracheal signals. Furthermore, we extracted 124 features over time. This many features can be affected temporally by various dynamics such as respiratory event occurrence, changes in sleep stages and body posture and increases in background noise. Although DNN2 compensated for dynamic changes, and thus, accurately estimated AHI and AHI cut-offs, there is significant potential, for example via enhancing its structure, to enhance the accuracy of AHI quantification and SA detection as well as to detect sleep and wakefulness states and snoring sounds.
Our study has some limitations. First, we did not measure sleep time directly, and used valid recording time as the denominator for the AHI. Therefore, we may have over or under estimated true sleep time. Nevertheless, this approach is similar to almost all home SA detection devices, and we demonstrated BresoDX1’s accuracy in estimating AHIPSG and in detecting SA at different AHI cut-offs, indicating its validity. Second, BresoDX1 was tested during attended PSG in a sleep laboratory, not in unattended setting in subjects’ homes. Accordingly, further testing in the latter environment will be necessary to assess BresoDX1’s ability to detect SA in a more clinically relevant setting.
In conclusion, BresoDX1 is a portable SA testing device that employs trachea-sternal motion and sound, along with oximetry, to provide accurate estimates of the AHI as well as to detect SA at various AHI cut-offs. It accomplishes this through the use of deep learning to develop novel algorithms to detect respiratory events. The strengths of the device are that it is simple and convenient, since it only requires two points of contact for its sensors. Also, the tracheal module is less subject to displacement and signal loss during sleep than other devices because it is fixed to the skin by adhesive tape. In addition, since this was the first iteration of the DNNs for signal analysis, the algorithms employed should be considered prototypes. Consequently, we believe there is room to improve the accuracy of AHI quantification and SA detection as well as to estimate sleep time via further enhancements to the DNNs. Finally, as the only expendable item is the adhesive strip, it could easily be used for multiple night monitoring where necessary. It is well-known that there is considerable night-to-night variation in the AHI,27 and for this reason, there is increasing acceptance of multiple night testing to increase the accuracy of SA diagnosis.28–30
Abbreviations
SA, Sleep apnea; PSG, polysomnography; DNN, deep neural network; RIP, respiratory inductance plethysmography; UHN, University Health Network; AASM, the American Academy of Sleep Medicine; MFCC, Mel-frequency cepstral coefficients; SNR, signal to noise ratio; IMCRA, the improved minima controlled recursive averaging technique.
Acknowledgments
This study was funded by Bresotec Inc.
Disclosure
Dr. Nasim Montazeri Ghahjaveretsan reports personal fees from Bresotec Inc., during the conduct of the study. Dr. Cristiano Aguiar reports a patent Provisional patent pending to Bresotec Inc. Mr Jackson Yu reports a patent PCT/CA2022/051031 pending to YU, (Jackson) Jinxin; HUMMEL, Richard George; DE AGUIAR, Cristiano Santos; FAN, Wei; PACKER, Devin, a patent US63/216,385 pending to YU, (Jackson) Jinxin; HUMMEL, Richard George; DE AGUIAR, Cristiano Santos; FAN, Wei; PACKER, Devin, a patent US63/236,852 pending to YU, (Jackson) Jinxin; HUMMEL, Richard George; DE AGUIAR, Cristiano Santos; FAN, Wei; PACKER, Devin. Mr. Richard Hummel reports personal fees from Bresotec Inc., during the conduct of the study. In addition, Mr. Richard Hummel has a patent P63124US00 pending to Bresotec Inc;. Ms. Xiaoshu Cao reports personal fees from Bresotec inc., during the conduct of the study. Dr. T. Douglas Bradley reports personal fees from Bresotec inc., during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep‐disordered breathing and its implications. Respirology. 2020;25(7):690–702. doi:10.1111/resp.13838
2. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population—a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311. doi:10.3978/j.issn.2072-1439.2015.06.11
3. Silverberg DS, Oksenberg A, Iaina A. Sleep related breathing disorders are common contributing factors to the production of essential hypertension but are neglected, underdiagnosed, and undertreated. Am J Hypertens. 1997;10(12):1319–1325. doi:10.1016/S0895-7061(97)00322-1
4. Boulos MI, Jairam T, Kendzerska T, Im J, Mekhael A, Murray BJ. Normal polysomnography parameters in healthy adults: a systematic review and meta-analysis. Lancet Respir Med. 2019;7(6):533–543. doi:10.1016/S2213-2600(19)30057-8
5. Malhotra A, Ayappa I, Ayas N, et al. Metrics of sleep apnea severity: beyond the apnea-hypopnea index. Sleep. 2021;44(7):zsab030. doi:10.1093/sleep/zsab030
6. Penzel T, Sabil A. Physics and applications for tracheal sound recordings in sleep disorders. In: Breath Sounds. Springer; 2018:83–104.
7. Yadollahi A, Giannouli E, Moussavi Z. Sleep apnea monitoring and diagnosis based on pulse oximetery and tracheal sound signals. Med Biol Eng Comput. 2010;48(11):1087–1097. doi:10.1007/s11517-010-0674-2
8. Nakano H, Hayashi M, Ohshima E, Nishikata N, Shinohara T. Validation of a new system of tracheal sound analysis for the diagnosis of sleep apnea-hypopnea syndrome. Sleep. 2004;27(5):951–957. doi:10.1093/sleep/27.5.951
9. Glos M, Sabil A, Jelavic KS, et al. Tracheal sound analysis for detection of sleep disordered breathing. Somnologie. 2019;23(2):80–85. doi:10.1007/s11818-019-0200-1
10. Bricout A, Fontecave-Jallon J, Pepin J, Gumery P. Accelerometry-derived respiratory index estimating apnea-hypopnea index for sleep apnea screening. Comput Methods Programs Biomed. 2021;207:106209. doi:10.1016/j.cmpb.2021.106209
11. Hafezi M, Montazeri Ghahjaverestan N, Saha S, et al. Sleep apnea severity estimation from tracheal movements using a deep learning model. IEEE Access. 2020;8:22641–22649. doi:10.1109/ACCESS.2020.2969227
12. Morillo DS, Ojeda JLR, Foix LFC, Jiménez AL. An accelerometer-based device for sleep apnea screening. IEEE Trans Inf Technol Biomed. 2009;14(2):491–499. doi:10.1109/TITB.2009.2027231
13. Dehkordi PK, Marzencki M, Tavakolian K, Kaminska M, Kaminska B. Validation of Respiratory Signal Derived from Suprasternal Notch Acceleration for Sleep Apnea Detection. IEEE; 2011:3824–3827.
14. Saha S, Kabir M, Montazeri N, et al. Apnea-Hypopnea Index (AHI) Estimation Using Breathing Sounds, Accelerometer and Pulse Oximeter. Eur Respiratory Soc; 2019.
15. Montazeri Ghahjaverestan N, Fan W, Aguiar C, Yu J, Bradley TD. Respiratory motion and airflow estimation during sleep using tracheal movement and sound. Nat Sci Sleep. 2022;14:1213. doi:10.2147/NSS.S360970
16. Hepsiba D, Anand LV, Princy RJP. Deep Learning for Sleep Disorders: A Review. IEEE; 2021:1–5.
17. Mostafa SS, Mendonça F, Ravelo-García G, Morgado-Dias F. A systematic review of detecting sleep apnea using deep learning. Sensors. 2019;19(22):4934. doi:10.3390/s19224934
18. Berry RB, Quan SF, Abreu AR, et al. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Am Academy Sleep Med. 2020;2020:1.
19. Molau S, Pitz M, Schluter R, Ney H. Computing mel-frequency cepstral coefficients on the power spectrum. IEEE. 2001;1:73–76.
20. Cohen I. Noise spectrum estimation in adverse environments: improved minima controlled recursive averaging. IEEE Trans Speech Audio Process. 2003;11(5):466–475. doi:10.1109/TSA.2003.811544
21. Montazeri Ghahjaverestan N, Akbarian S, Hafezi M, et al. Sleep/wakefulness detection using tracheal sounds and movements. Nat Sci Sleep. 2020;12:1009. doi:10.2147/NSS.S276107
22. Penzel T, Sabil A. The use of tracheal sounds for the diagnosis of sleep apnoea. Breathe. 2017;13(2):e37–e45. doi:10.1183/20734735.008817
23. Saha S, Kabir M, Montazeri Ghahjaverestan N, et al. Portable diagnosis of sleep apnea with the validation of individual event detection. Sleep Med. 2020;69:51–57. doi:10.1016/j.sleep.2019.12.021
24. Twigg GL, Mallia-Milanes B, Miras AD, Tighe H, Wilson G. 20 Validation of WatchPAT 300 for Pre-Operative of OSA Screening in Patients Undergoing Bariatric Surgery. Archives of Disease in childhood; 2021.
25. Lee JY, Kim D, Blake S, et al. 403 comparative study of wireless sensors versus type III home sleep apnea test for home-based diagnosis of obstructive sleep apnea. Sleep. 2021;44(Supplement_2):A160. doi:10.1093/sleep/zsab072.402
26. Berry RB, Purdy S, Kantner G, et al. 0463 validation of a home sleep apnea testing device for the diagnosis of sleep disordered breathing based on AASM 2012 guidelines. Sleep. 2019;42:A186. doi:10.1093/sleep/zsz067.462
27. Levendowski DJ, Zack N, Rao S, et al. Assessment of the test–retest reliability of laboratory polysomnography. Sleep Breath. 2009;13(2):163–167. doi:10.1007/s11325-008-0214-6
28. Ha Y. Should you offer multinight home sleep testing?; 2021.
29. Lechat B, Naik G, Reynolds A, et al. Multinight prevalence, variability, and diagnostic misclassification of obstructive sleep apnea. Am J Respir Crit Care Med. 2022;205(5):563–569. doi:10.1164/rccm.202107-1761OC
30. Dzierzewski JM, Dautovich ND, Rybarczyk B, Taylor SA. Night-to-night fluctuations in sleep apnea severity: diagnostic and treatment implications. J Clin Sleep Med. 2020;16(4):539–544. doi:10.5664/jcsm.8272
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.