")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
SLCO1B1 and ABCG2 Gene Polymorphisms in a Thai Population
Authors Rattanacheeworn P , Chamnanphon M , Thongthip S, Kittanamongkolchai W , Townamchai N , Avihingsanon Y, Udomnilobol U , Prueksaritanont T, Jianmongkol S , Chariyavilaskul P
Received 19 June 2020
Accepted for publication 21 September 2020
Published 22 October 2020 Volume 2020:13 Pages 521—530
DOI https://doi.org/10.2147/PGPM.S268457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
Punyabhorn Rattanacheeworn,1,2 Monpat Chamnanphon,1 Siriwan Thongthip,3 Wonngarm Kittanamongkolchai,3 Natavudh Townamchai,1,4 Yingyos Avihingsanon,1,4 Udomsak Udomnilobol,5 Thomayant Prueksaritanont,5 Suree Jianmongkol,5,6 Pajaree Chariyavilaskul1,2
1Clinical Pharmacokinetics and Pharmacogenomics Research Unit, Chulalongkorn University, Bangkok, Thailand; 2Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Maha Chakri Sirindhorn Clinical Research Center Under the Royal Patronage, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 4Division of Nephrology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Chulalongkorn University Drug and Health Products Innovation Promotion Center, Faculty of Pharmaceutical Sciences, Chulalongkorn University, Bangkok, Thailand; 6Department of Pharmacology and Physiology, Faculty of Pharmaceutical Sciences, Chulalongkorn University, Bangkok, Thailand
Correspondence: Pajaree Chariyavilaskul
Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Tel +66816134664
Fax +6622564481 Ext.1
Email [email protected]
Introduction: Genetic polymorphisms of drug transporters influence drug transporter activity and alter pharmacokinetic profiles of the drugs. Organic anion transporting polypeptide 1B1 (OATP1B1) and breast cancer resistance protein (BCRP) are important transporters encoded by solute carrier organic anion transporter family member 1B1 (SLCO1B1) gene and ATP-binding cassette subfamily G member 2 (ABCG2) gene, respectively. Polymorphisms in these genes are associated with increased plasma statins concentrations, statin-induced myopathy and poor response to allopurinol treatment.
Purpose: We explored allele and genotype frequencies of SLCO1B1 and ABCG2 genes including their predicted phenotypes in 53 Thai participants. Of these, 17 had chronic kidney disease and were on statins.
Materials and Methods: Genotyping analysis for SLCO1B1 c.521T>C (rs4149056), c.388A>G (rs2306283), g.-11187G>A (rs4149015), and ABCG2 c.421C>A (rs2231142) was done by using TaqMan® Real time PCR. All were tested for Hardy–Weinberg Equilibrium.
Results: Most of the participants (80%) had normal function haplotypes SLCO1B1 (*1A and *1B) while decreased (*5, *15, and *17) and unknown (*21) function haplotypes were less observed. Four phenotypes of SLCO1B1 were observed: 69.81% had normal function (*1A/*1A,*1A/*1B, and *1B/*1B), 13.21% had intermediate function (*1A/*17, *1B/*15 and *1B/*17), 9.43% had indeterminate function (*1A/*21 and *1B/*21) and 7.55% had low function (*5/*15, *15/*15, and *15/*17). ABCG2 c.421A allele frequency was 25%. The frequency of ABCG2 c.421CA and AA phenotypes were 37.7% and 5.7%, respectively. The allele and genotype frequencies observed are consistent with reports in Asians. However, there were differences in major allele distributions between Asians and Caucasians for SLCO1B1 c.388A>G; SLCO1B1 c.388G were highly found in Asians, but c.388A were more observed in Caucasians.
Conclusion: This study showed that in the Thai population, there were 4 SNPs of SLCO1B1 and ABCG2 genes. This finding may be clinically applied to minimize inter-individual variability of drugs such as statins and allopurinol. Further study with a larger sample size is needed to assess the drug profiles and responses to treatment.
Keywords: pharmacogenetics, pharmacogenomics, drug transporters, SLCO1B1, ABCG2, OATP1B1, BRCP
Introduction
Drug transporters are mostly localized at the basolateral or apical membranes of organs involved in drug biotransformation such as the liver, intestine, brain, and kidneys, and play an important role in pharmacokinetic process.1–3 Genetic polymorphisms of drug transporters affect drug transportation across membranes, and contribute to variability in drug disposition and responses.4
Solute-Linked Carrier (SLC) and ATP-binding cassette (ABC) are two major superfamilies of drug transporters. SLC, including SLCO (also known as SLC21), SLC22, and SLC47 encode membrane proteins that are mainly responsible for drug uptake. An uptake transporter, organic anion transporting polypeptides (OATPs) including OATP1B1, is encoded by solute carrier organic anion transporter family member 1B1 (SLCO1B1) gene. OATP1B1 is a sodium-independent bile acid transporter that generally transports amphipathic molecules through the basolateral membrane of the hepatocytes.5,6 On the other hand, an efflux transporter, breast cancer resistance protein (BCRP), is encoded by ATP binding cassette subfamily G member 2 (ABCG2) gene of the ABC family and is involved in drug resistance.2–4
Previous reports have shown the effects of genetic polymorphisms of OATP1B1 hepatic uptake transporter and BCRP efflux transporter on pharmacokinetic properties of statins.4,5,7–10 The Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline, therefore, recommends genetic testing for these genes prior to starting treatment with statins in order to minimize the risk of developing statins-induced myopathy.11 Moreover, BCRP transporter polymorphism, rs2231142 c.421C>A, is also associated with urate transporter dysfunction which causes the patients to have a higher risk for developing gout and hyperuricemia by overloading the renal urate and under excreting the products out of the extrarenal system.12 However, there were reports of differences in allele frequencies of SLCO1B1 and ABCG2 genes among different ethnicities. SLCO1B1 c.521T>C variant is commonly found in Caucasians whereas ABCG2 c.421C>A variant is highly observed in Asians.4,7,13–19 However, data in the Thai population in regards to genetic polymorphisms of these drug transporters are limited. It is very important to fully obtain the overall allele and genotype frequencies of both SLC and ABC families of drug transporters and factors associated with clinical data in real-life setting among Thai patients who are treated with statins.
Here, we investigated the allele and genotype frequencies of both SLCO1B1 gene (rs4149056, rs2306283, rs4149015) and ABCG2 gene (rs2231142) in a cohort of Thai patients attending an Out-Patients Clinic of the King Chulalongkorn Memorial Hospital, Bangkok, Thailand.
Materials and Methods
This cross-sectional study was a sub-study of a clinical trial entitled, “CYP3A and drug transporters activity changes in Thai elderly with or without chronic kidney disease using a microdose cocktail” (#TCTR20180312002; manuscript in preparation). The study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand, and was conducted in compliance with the Declaration of Helsinki and the Principle of Good Clinical Practice. Written informed consents were obtained from all participants prior to the start of the study.
Participants
Fifty-three Thai participants were enrolled into the study. Of these, 36 healthy adults were aged 20–70 years, did not have hypertension or dyslipidemia, had normal physical examination and laboratory results. Seventeen participants had Chronic Kidney Disease (CKD) and were treated with statins (simvastatin or atorvastatin). Comorbidity, history of statin treatment, dose per day, duration of use, and reasons for changing statin were retrospectively extracted from the participants’ medical history from 2007 to 2019.
Genotyping Analysis and Predicted Phenotypes
Venous blood sample (3 mL) was collected from each participant into an EDTA tube. Genomic DNA was extracted by PureLink® Genomic DNA kit (ThermoFisher Scientific). SLCO1B1 c.521T>C (rs4149056), c.388A>G (rs2306283), g.-11187G>A (rs4149015), and ABCG2 c.421C>A (rs2231142) were detected by TaqMan® Real time Polymerase Chain Reaction (PCR) using TaqMan Drug Metabolism Genotyping Assays (Applied Biosystem, ThermoFisher Scientific). PCR was performed with the quantitative real-time PCR (q-PCR) system (StepOnePlus™ Real-Time PCR System, ThermoFisher Scientific). Predicted functions of the haplotypes were assigned according to PharmGKB.20 Predicted phenotypes and * allele nomenclature of OATP1B1 were assigned according to the Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline.11
Statistical Analysis
Allele and genotype frequencies were directly calculated and reported using descriptive statistics. Heterogenous and homozygous genotypes were defined as genotypes consisted of one and two copies of variant alleles, respectively. The Hardy-Weinberg equilibrium test was determined by Haploview version 4.2. P-value of <0.05 was considered statistically significant.
Results
The overall characteristics of 53 participants are summarized in Table 1. There were 28 females and 25 males in this cohort. The minor allele frequencies of SLCO1B1 and ABCG2 genes in this study and other ethnicities are summarized in Table 2.
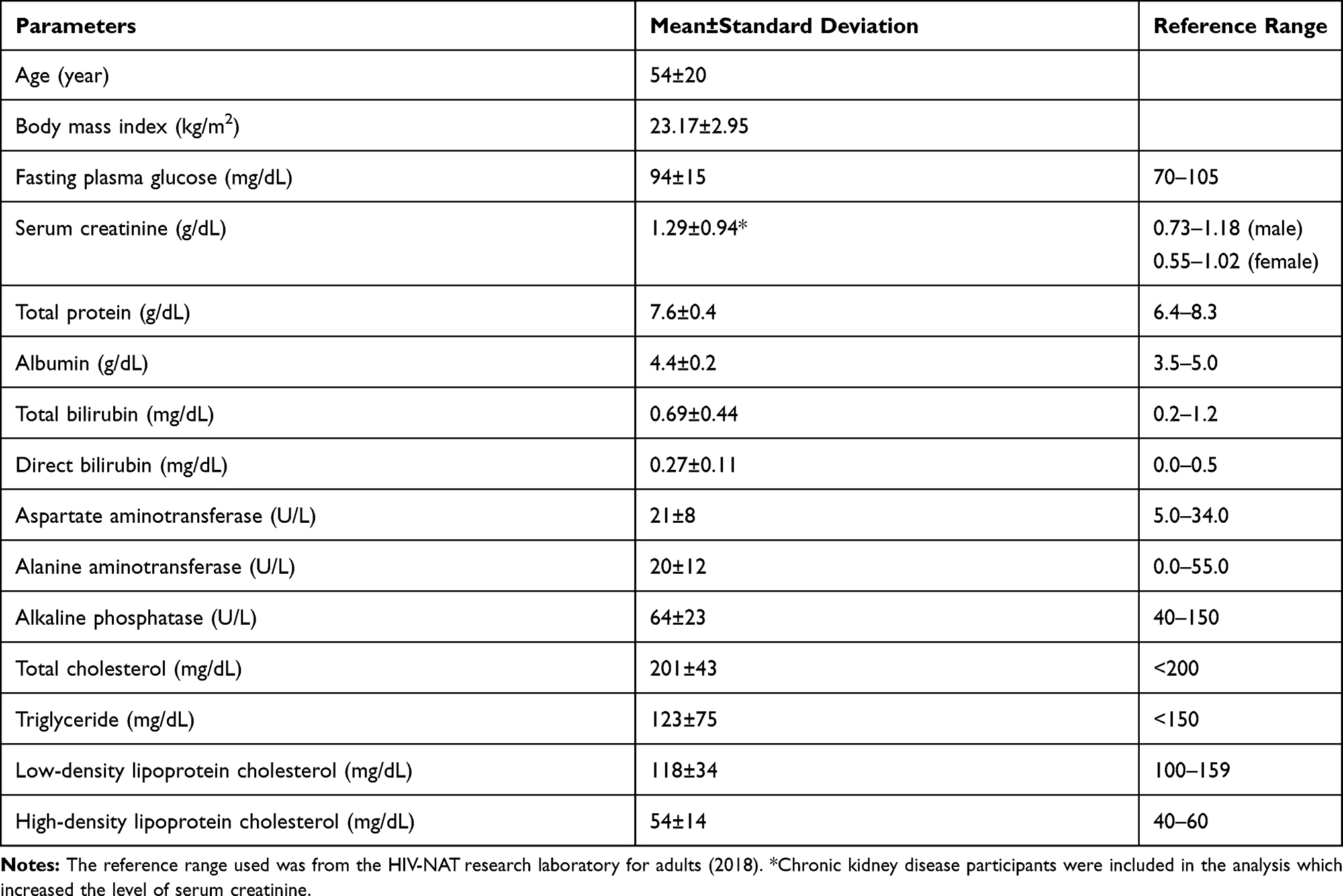 |
Table 1 Characteristics of the Participants (n = 53) |
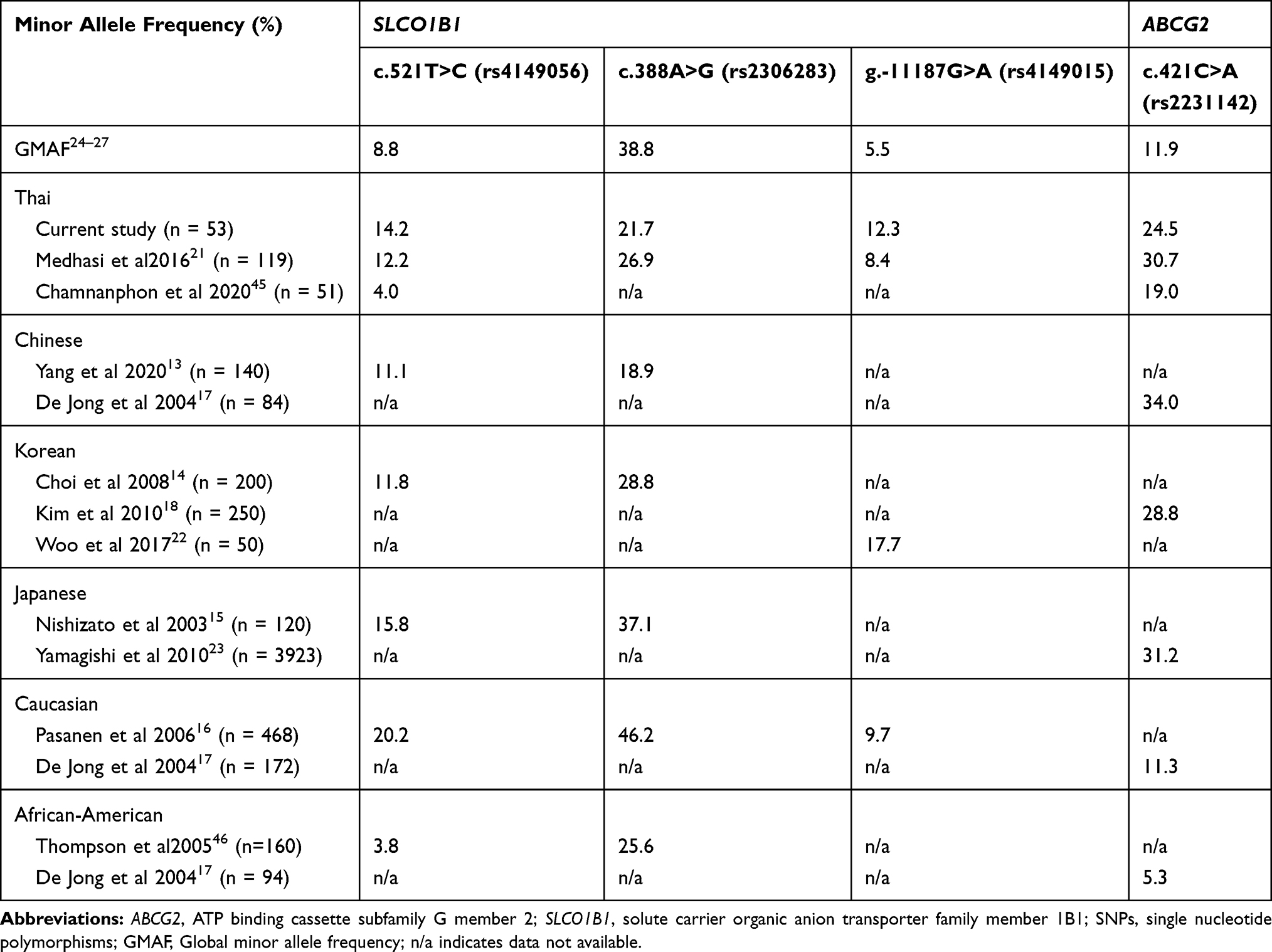 |
Table 2 Minor Allele Frequencies of SLCO1B1 and ABCG2 Genes |
The predicted normal function haplotypes of SLCO1B1 (*1A and *1B) were mostly found in the participants while predicted decreased (*5, *15, and *17) and unknown (*21) function haplotypes were also observed in approximately 20% of the participants (Figure 1A).
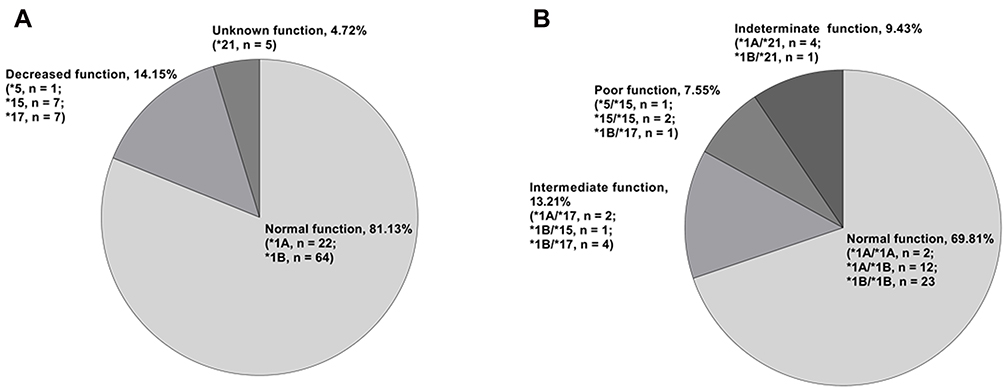 |
Figure 1 Haplotype, genotype, and predicted phenotype frequencies of SLOC1B1 gene. (A) Haplotype and predicted functions (total n = 106). (B) Genotype and predicted phenotypes (total n = 53). |
Four predicted phenotypes were observed (Figure 1B). More than half of the participants had normal function phenotypes of SLCO1B1 (*1A/*1A, *1A/*1B, and *1B/*1B). Interestingly, 9.43% of the participants had indeterminate function phenotypes of SLCO1B1 (*1A/*21 and *1B/*21) while only 7.55% of the participants had low function phenotypes (*5/*15, *15/*15, and *15/*17).
Statins treatment for CKD participants are shown in Table 3. Most of the participants received either simvastatin (current dose range 10–40 mg/day) or atorvastatin (current dose range 20–40 mg/day). Fourteen participants had SLCO1B1 predicted phenotype normal function. One participant (participant number 04) had SLCO1B1 intermediate function and another one participant (participant number 09) had SLCO1B1 poor function. Two participants (participant number 08 and participant number 13) were in the indeterminate function group. There was no serious adverse event related to statins-induced myopathy. There were some statin dose reduction/increase or change of statin used but these were due to other factors and were not related to any adverse events.
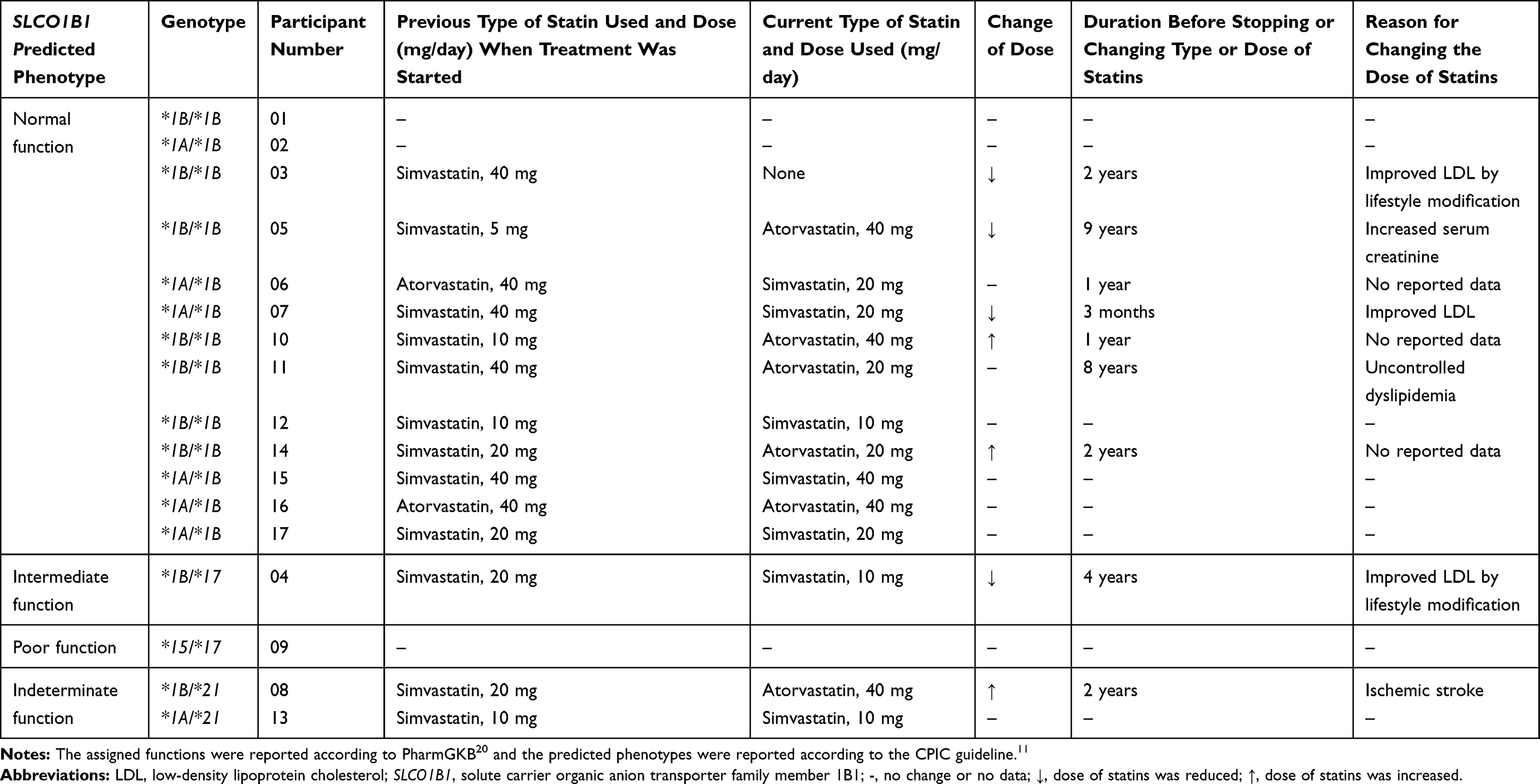 |
Table 3 Genotype and Predicted Phenotype of SLCO1B1 with Current Types of Statins Used, Doses and Reasons for Changing Type or Dose of the Statins in 17 CKD Participants |
As SLCO1B1 c.521T>C and ABCG2 c.421C>A were associated with the pharmacokinetic process of rosuvastatin, plasma rosuvastatin concentration in 17 CKD participants were estimated (Table 4). Nine out of 17 participants were likely to have increased plasma rosuvastatin concentrations if the standard dose of rosuvastatin were administered. Participant number 09 had SLCO1B1 c.521T>C and ABCG2 c.421C>A genes and the genotypes were CC and CA, respectively. This participant is likely to be most affected by these genetic alterations in terms of increased plasma rosuvastatin concentrations.
 |
Table 4 SLOC1B1 c.521T>C Genotype, ABCG2 c.421C>A Genotype and Estimated Rosuvastatin Plasma Concentrations in 17 CKD Participants |
Discussion
We detected 4 SNPs of SLCO1B1 and ABCG2 genes in the Thai population including SLCO1B1 c.521T>C, SLCO1B1 c.388A>G, SLCO1B1 g.-11187G>A and ABCG2 c.421C>A. We found that the genotype frequencies of SLCO1B1 and ABCG2 genes in this cohort were mostly of the wild type except for SLCO1B1 c.388A>G which was a homozygous variant and was highly observed. Minor allele frequencies of SLCO1B1 and ABCG2 genes in this study was comparable to another Thai population study21 and other Asian populations including Chinese,13,17 Korean,14,18,22 and Japanese15,23 and had slightly higher global minor allele frequency (GMAF)24–27 (Table 2).
Populations from different regions have distinct genetic variation that can cause variability in the pharmacokinetic of the drug substrates.16,24 Comparisons of the allele and genotype frequencies of these 4 SNPs among our Thai population and Chinese,13,17 Korean,14,18,22 Japanese15,19 and Caucasian16,17 are shown in Figures 2 and 3. The allele and genotype frequencies observed in this study were in line with previous reports conducted in Asians (major alleles: c.521T, g.-11187G and wild type genotypes: c.521TT and g.-11187GG, respectively). However, there were differences in major allele distributions between Asians and Caucasians for SLCO1B1 c.388A>G. SLCO1B1 c.388G were highly found in Asians but c.388A were more observed in Caucasians (Figure 2B). For ABCG2 c.421C>A, there were also similar major allele (c.421C) and genotype (c.421CC) among Asians and Caucasians except for Chinese who had slightly different genotype frequencies as shown in Figures 2D and 3D.
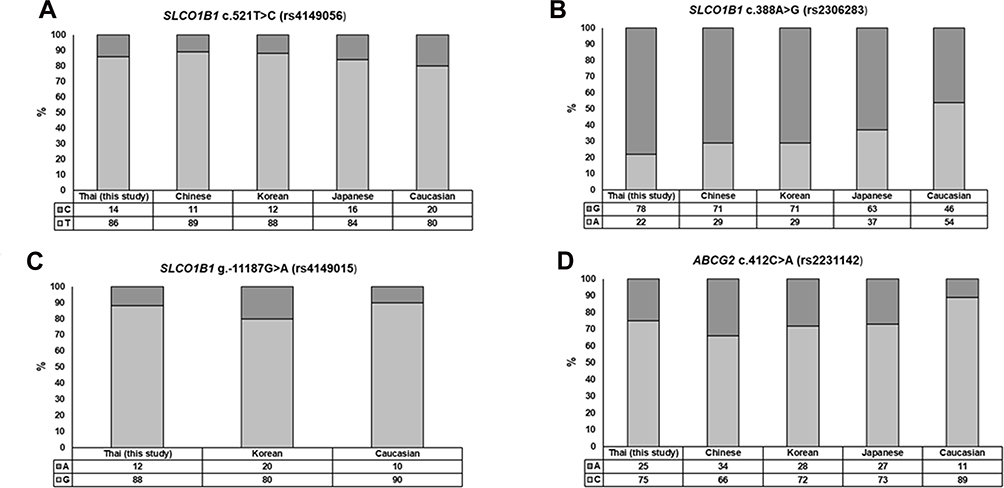 |
Figure 2 Allele frequencies of SNPs in SLCO1B1 and ABCG2 genes in Thai participants compared to other populations. |
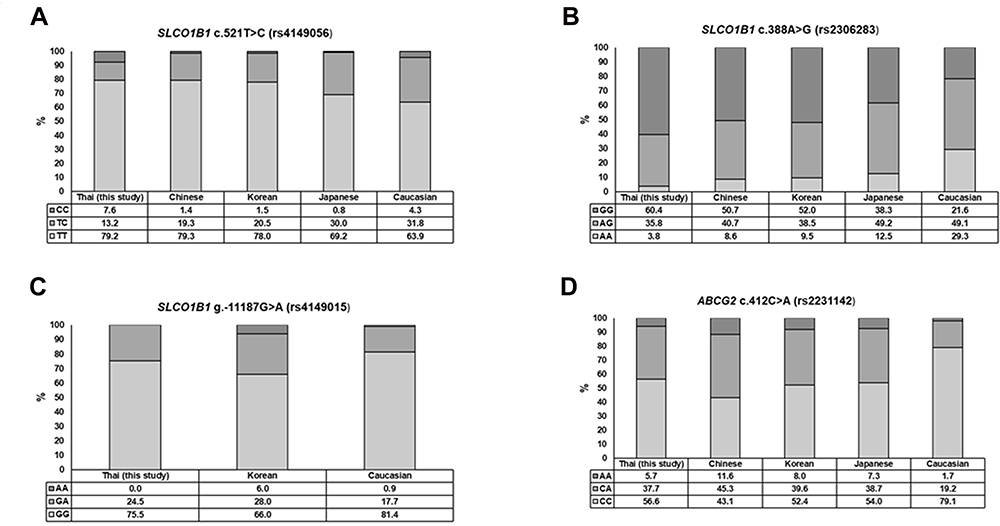 |
Figure 3 Genotype frequencies of SNPs in SLCO1B1 and ABCG2 genes in Thai participants compared to other populations. |
All SNPs measured in this study have been reported to be associated with a decreased OATP1B1 hepatic uptake transporter and BCRP efflux transporter functions. These genetic polymorphisms can result in higher drug exposure and toxicity of statins.8,14,15,29–31
Interestingly, our cohort and other Asian populations frequently had SLCO1B1 c.388GG which corresponded to SLCO1B1*15 and *17. The SLCO1B1*5 (carrying c.521T>C), *15 (carrying c.388A>G and c.521T>C) and *17 (carrying c.388A>G, c.521T>C and g.-11187G>A) were associated with a decreased OATP1B1 activity resulting in a lower clearance of simvastatin acid.11,29,30,32 In our study, we detected SLCO1B1*15 and *17 (haplotype frequency 6.6% for both, Figure 3).
The CPIC guideline stated that genotype of SLCO1B1 may imply SLCO1B1 phenotype which may implicate that the dose of simvastatin should be adjusted.11 In this study, we found SLCO1B1*1A/*17, *1B/*15, *1B/*17 and *5/*15, *15/*15, *15/*17 genotypes which had intermediate and low function phenotypes, respectively, in approximately 20% of the cohort. These phenotypes are associated with myopathy risk. The guideline, therefore, recommends using low dose of simvastatin when initiating statin treatment or the use of alternative statins, for example, pravastatin or rosuvastatin.11 Unfortunately, the medical history of statins in 17 CKD participants with SLCO1B1 genotypes and predicted phenotypes were not available so we could not assess the risk of developing myopathy. There was only one participant who had SLCO1B1 intermediate function and this participant had an improved low-density lipoprotein cholesterol level after lifestyle modification. Another participant had SLCO1B1 poor function and no medical history of statin use.
Previous studies have reported that ABCG2 c.421A allele was associated with high plasma rosuvastatin concentration.10,33 The Annotation of Swissmedic Label for rosuvastatin and ABCG2, SLCO1B134 also recommended that a lower dose of rosuvastatin (Crestor®) should be administered in patients who have a higher risk of rosuvastatin exposure, especially among Asians or patients with variant SLCO1B1 c.521T>C and/or ABCG2 c.421C>A. Tests for genetic polymorphisms should be acquired before starting treatment with statin. For example, participant number 09 had SLCO1B1 low function phenotype of OATP1B1, and ABCG2 c.421CA genotype. Hence, if this participant started to use rosuvastatin, the physician should consider reducing the dose of the drug.
The influence of genetic polymorphism on pharmacokinetic of other statins have also been reported. The higher plasma concentrations of pravastatin in patients with SLCO1B1 c.521C allele is associated with decreased total and non-renal clearance of pravastatin.15 Area under the plasma concentration-time curve (AUC) of pitavastatin, rosuvastatin and atorvastatin were increased with different magnitude of SLCO1B1 c.521CC genotype.8,14,31 ABCG2 c.421AA genotype was associated with an increased AUC of rosuvastatin, atorvastatin, fluvastatin and simvastatin lactone as BCRP efflux activity at the small intestine was reduced, resulting in an increased bioavailability of the drugs.10,35,36
Furthermore, BCRP is an important transporter for regulating uric acid transport in the kidneys and gastrointestinal tract.37 ABCG2 c.421C>A polymorphism reduced 53% of urate transport rate compared to wild type and was found in approximately 10% of the patients with gout in Caucasians.38 Previous studies have also reported that ABCG2 c.421C>A polymorphism was associated with significant increase in familial early-onset hyperuricemia and gout in pediatric-onset patients.39,40 Moreover, it has been reported that ABCG2 c.421C>A polymorphism reduces the activity of allopurinol, the first-line therapy for lowering serum uric acid.41,42
Of note, in our study, 7 CKD participants were on allopurinol. Of these, 3 participants had ABCG2 c.421CA and 1 participant had ABCG2c.421AA (data not shown). Unfortunately, since the data was retrieved retrospectively, we cannot find evidence of allopurinol treatment outcome for these participants. Hyperuricemia/gout is a common comorbidity of CKD. Almost 42% of patients using allopurinol failed to achieve allopurinol treatment goal.43 The key reasons for allopurinol treatment failure could either be due to the reduced renal function which causes the titration of the allopurinol dose or poor adherence.41,42 Additionally, the influence of ABCG2 c.421C>A polymorphism on allopurinol response should also be taken into account as a possible factor for allopurinol treatment failure in CKD patients.
There are some limitations in this study. The sample size was relatively small. We found no deviation from Hardy-Weinberg principle in all detected SNPs except for SLCO1B1 c.521T>C which may be due to the sample size and linkage disequilibrium.30,44 There are unknown function haplotypes (approximately 5%) and indeterminate function of predicted phenotypes (approximately 10%) of SLCO1B1 observed in our cohort which might be of interest to be further explored. However, these limitations do not make our conclusion inaccurate. This study’s genetic data are important and beneficial to the patients by providing the physicians the fundamental information on how to manage patients who have these polymorphisms and the need to be on statins.
Conclusion
In summary, this study provided the evidence that Thai patients have 4 SNPs in SLCO1B1 and ABCG2 genes. Even though we were not able to find an association of these genetic polymorphisms and the use of statins and allopurinol due to the study’s sample size, however, the results indicated that we should be more vigilant in administering drugs to the Thai population because of inter-individual variability of the drug transporter functions. A larger prospective study using genotype-guided therapy and assessing the pharmacokinetic profiles of the drugs are warranted.
Data Sharing Statement
The data are available on reasonable request to the correspondence author.
Funding
This work was supported by the Health Systems Research Institute (HSRI) grant no. 60094. Rattanacheeworn, P. was supported by the 100th Anniversary Chulalongkorn University Fund for Doctoral Scholarship. We thank the staff of the HIV Netherlands Australia Thailand Research Collaboration (HIV-NAT) laboratory for their technical assistance.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. Mizuno N, Sugiyama Y. Drug transporters: their role and importance in the selection and development of new drugs. Drug Metab Pharmacokinet. 2002;17(2):93–108. doi:10.2133/dmpk.17.93
2. Shugarts S, Benet LZ. The role of transporters in the pharmacokinetics of orally administered drugs. Pharm Res. 2009;26(9):2039–2054.
3. Keogh J, Hagenbuch B, Rynn C, Stieger B, Nicholls G. Chapter 1 membrane transporters: fundamentals, function and their role in ADME. In: Nicholls G, Youdim K, editors. Drug Transporters: Volume 1: Role and Importance in ADME and Drug Development. 1st ed. London: The Royal Society of Chemistry; 2016:1–56.
4. Franke RM, Gardner ER, Sparreboom A. Pharmacogenetics of Drug Transporters. Curr Pharm Des. 2010;16(2):220–230. doi:10.2174/138161210790112683
5. Kalliokoski A, Niemi M. Impact of OATP transporters on pharmacokinetics. Br J Pharmacol. 2009;158(3):693–705. doi:10.1111/j.1476-5381.2009.00430.x
6. Stieger B, Hagenbuch B. Chapter five - organic anion-transporting polypeptides. In: Bevensee MO, editor. Current Topics in Membranes. Vol. 73. Academic Press; 2014:205–232.
7. Birmingham BK, Bujac SR, Elsby R, et al. Impact of ABCG2 and SLCO1B1 polymorphisms on pharmacokinetics of rosuvastatin, atorvastatin and simvastatin acid in caucasian and asian subjects: a class effect? Eur J Clin Pharmacol. 2015;71(3):341–355. doi:10.1007/s00228-014-1801-z
8. Pasanen MK, Fredrikson H, Neuvonen PJ, Niemi M. Different effects of SLCO1B1 polymorphism on the pharmacokinetics of atorvastatin and rosuvastatin. Clin Pharmacol Ther. 2007;82(6):726–733. doi:10.1038/sj.clpt.6100220
9. Romaine SP, Bailey KM, Hall AS, Balmforth AJ. The influence of SLCO1B1 (OATP1B1) gene polymorphisms on response to statin therapy. Pharmacogenomics J. 2010;10(1):1–11. doi:10.1038/tpj.2009.54
10. Keskitalo JE, Zolk O, Fromm MF, Kurkinen KJ, Neuvonen PJ, Niemi M. ABCG2 polymorphism markedly affects the pharmacokinetics of atorvastatin and rosuvastatin. Clin Pharmacol Ther. 2009;86(2):197–203. doi:10.1038/clpt.2009.79
11. Ramsey LB, Johnson SG, Caudle KE, et al. The clinical pharmacogenetics implementation consortium guideline for SLCO1B1 and simvastatin-induced myopathy: 2014 update. Clin Pharmacol Ther. 2014;96(4):423–428. doi:10.1038/clpt.2014.125
12. Cleophas MC, Joosten LA, Stamp LK, Dalbeth N, Woodward OM, Merriman TR. ABCG2 polymorphisms in gout: insights into disease susceptibility and treatment approaches. Pharmgenomics Pers Med. 2017;10:129–142.
13. Yang GP, Yuan H, Tang B, et al. Lack of effect of genetic polymorphisms of SLCO1B1 on the lipid-lowering response to pitavastatin in Chinese patients. Acta Pharmacol Sin. 2010;31(3):382–386. doi:10.1038/aps.2009.203
14. Choi JH, Lee MG, Cho JY, Lee JE, Kim KH, Park K. Influence of OATP1B1 genotype on the pharmacokinetics of rosuvastatin in Koreans. Clin Pharmacol Ther. 2008;83(2):251–257. doi:10.1038/sj.clpt.6100267
15. Nishizato Y, Ieiri I, Suzuki H, et al. Polymorphisms of OATP-C (SLC21A6) and OAT3 (SLC22A8) genes: consequences for pravastatin pharmacokinetics. Clin Pharmacol Ther. 2003;73(6):554–565. doi:10.1016/S0009-9236(03)00060-2
16. Pasanen MK, Backman JT, Neuvonen PJ, Niemi M. Frequencies of single nucleotide polymorphisms and haplotypes of organic anion transporting polypeptide 1B1 SLCO1B1 gene in a Finnish population. Eur J Clin Pharmacol. 2006;62(6):409–415. doi:10.1007/s00228-006-0123-1
17. De Jong FA, Marsh S, Mathijssen RH, et al. ABCG2 pharmacogenetics: ethnic differences in allele frequency and assessment of influence on irinotecan disposition. Clin Cancer Res. 2004;10(17):5889–5894. doi:10.1158/1078-0432.CCR-04-0144
18. Kim KA, Joo HJ, Park JY. ABCG2 polymorphisms, 34G>A and 421C>A in a Korean population: analysis and a comprehensive comparison with other populations. J Clin Pharm Ther. 2010;35(6):705–712. doi:10.1111/j.1365-2710.2009.01127.x
19. Imai Y, Nakane M, Kage K, et al. C421A polymorphism in the human breast cancer resistance protein gene is associated with low expression of Q141K protein and low-level drug resistance. Mol Cancer Ther. 2002;1(8):611–616.
20. PharmGKB. SLCO1B1 allele functionality table. Available from: https://www.pharmgkb.org/page/slco1b1RefMaterials.
21. Medhasi S, Pasomsub E, Vanwong N, et al. Clinically relevant genetic variants of drug-metabolizing enzyme and transporter genes detected in Thai children and adolescents with autism spectrum disorder. Neuropsychiatr Dis Treat. 2016;12:843–851.
22. Woo HI, Kim SR, Huh W, Ko JW, Lee SY. Association of genetic variations with pharmacokinetics and lipid-lowering response to atorvastatin in healthy Korean subjects. Drug Des Devel Ther. 2017;11:1135–1146. doi:10.2147/DDDT.S131487
23. Yamagishi K, Tanigawa T, Kitamura A, et al. The rs2231142 variant of the ABCG2 gene is associated with uric acid levels and gout among Japanese people. Rheumatology. 2010;49(8):1461–1465. doi:10.1093/rheumatology/keq096
24. National center for biotechnology information. ClinVar; [VCV000037346.4]. Available from: https://www.ncbi.nlm.nih.gov/clinvar/variation/VCV000037346.4.
25. National center for biotechnology information. ClinVar; [VCV000259983.4]. Available from: https://www.ncbi.nlm.nih.gov/clinvar/variation/VCV000259983.4.
26. National center for biotechnology information. ClinVar; [VCV000225995.1]. Available from: https://www.ncbi.nlm.nih.gov/clinvar/variation/VCV000225995.
27. National center for biotechnology information. ClinVar; [VCV000030389.2]. Available from: https://www.ncbi.nlm.nih.gov/clinvar/variation/VCV000030389.2.
28. Lee HH, Ho RH. Interindividual and interethnic variability in drug disposition: polymorphisms in organic anion transporting polypeptide 1B1 (OATP1B1; SLCO1B1). Br J Clin Pharmacol. 2017;83(6):1176–1184. doi:10.1111/bcp.13207
29. Pasanen MK, Neuvonen M, Neuvonen PJ, Niemi M. SLCO1B1 polymorphism markedly affects the pharmacokinetics of simvastatin acid. Pharmacogenet Genomics. 2006;16(12):873–879. doi:10.1097/01.fpc.0000230416.82349.90
30. Link E, Parish S, Armitage J, et al. SLCO1B1 variants and statin-induced myopathy–a genomewide study. N Engl J Med. 2008;359(8):789–799.
31. Deng JW, Song IS, Shin HJ, et al. The effect of SLCO1B1*15 on the disposition of pravastatin and pitavastatin is substrate dependent: the contribution of transporting activity changes by SLCO1B1*15. Pharmacogenet Genomics. 2008;18(5):424–433. doi:10.1097/FPC.0b013e3282fb02a3
32. Duman I. Role of Pharmacogenetics on Response to Statins: A Genotypebased Approach to Statin Therapy Outcome. J Cardiol Therapy. 2014;1(6):111–120.
33. Lee HK, Hu M, Lui S, Ho CS, Wong CK, Tomlinson B. Effects of polymorphisms in ABCG2, SLCO1B1, SLC10A1 and CYP2C9/19 on plasma concentrations of rosuvastatin and lipid response in Chinese patients. Pharmacogenomics. 2013;14(11):1283–1294. doi:10.2217/pgs.13.115
34. Annotation of Swissmedic Label for rosuvastatin and ABCG2, SLCO1B1. Available from: https://www.pharmgkb.org/labelAnnotation/PA166184499.
35. Robey RW, To KK, Polgar O, et al. ABCG2: a perspective. Adv Drug Deliv Rev. 2009;61(1):3–13. doi:10.1016/j.addr.2008.11.003
36. Keskitalo JE, Pasanen MK, Neuvonen PJ, Niemi M. Different effects of the ABCG2 c.421C>A SNP on the pharmacokinetics of fluvastatin, pravastatin and simvastatin. Pharmacogenomics. 2009;10(10):1617–1624. doi:10.2217/pgs.09.85
37. Ichida K, Matsuo H, Takada T, et al. Decreased extra-renal urate excretion is a common cause of hyperuricemia. Nat Commun. 2012;3:764. doi:10.1038/ncomms1756
38. Woodward OM, Köttgen A, Coresh J, Boerwinkle E, Guggino WB, Köttgen M. Identification of a urate transporter, ABCG2, with a common functional polymorphism causing gout. Proc Natl Acad Sci U S A. 2009;106(25):10338–10342. doi:10.1073/pnas.0901249106
39. Toyoda Y, Pavelcová K, Klein M, Suzuki H, Takada T, Stiburkova B. Familial early-onset hyperuricemia and gout associated with a newly identified dysfunctional variant in urate transporter ABCG2. Arthritis Res Ther. 2019;21(1):219. doi:10.1186/s13075-019-2007-7
40. Stiburkova B, Pavelcova K, Pavlikova M, Ješina P, Pavelka K. The impact of dysfunctional variants of ABCG2 on hyperuricemia and gout in pediatric-onset patients. Arthritis Res Ther. 2019;21(1):77. doi:10.1186/s13075-019-1860-8
41. Roberts RL, Wallace MC, Phipps-Green AJ, et al. ABCG2 loss-of-function polymorphism predicts poor response to allopurinol in patients with gout. Pharmacogenomics J. 2017;17(2):201–203. doi:10.1038/tpj.2015.101
42. Wallace MC, Roberts RL, Nanavati P, et al. Association between ABCG2 rs2231142 and poor response to allopurinol: replication and meta-analysis. Rheumatology (Oxford). 2018;57(4):656–660. doi:10.1093/rheumatology/kex467
43. Becker MA, Schumacher HR, Espinoza LR, et al. The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: the CONFIRMS trial. Arthritis Res Ther. 2010;12(2):R63. doi:10.1186/ar2978
44. Li B, Leal SM. Deviations from Hardy-Weinberg equilibrium in parental and unaffected sibling genotype data. Hum Hered. 2009;67(2):104–115. doi:10.1159/000179558
45. Chamnanphon M, Gaedigk A, Puangpetch A, et al. Pharmacogene variation in thai plasmodium vivax relapse patients treated with a combination of primaquine and chloroquine. Pharmgenomics Pers Med. 2020;13:1–12.
46. Thompson JF, Man M, Johnson KJ, et al. An association study of 43 SNPs in 16 candidate genes with atorvastatin response. Pharmacogenomics J. 2005;5(6):352–358. doi:10.1038/sj.tpj.6500328
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.