")
Back to Journals » The Application of Clinical Genetics » Volume 12
SLC22A1 And ATM Genes Polymorphisms Are Associated With The Risk Of Type 2 Diabetes Mellitus In Western Saudi Arabia: A Case-Control Study
Authors Altall RM , Qusti SY, Filimban N, Alhozali AM, Alotaibi NA, Dallol A , Chaudhary AG, Bakhashab S
Received 7 September 2019
Accepted for publication 3 November 2019
Published 15 November 2019 Volume 2019:12 Pages 213—219
DOI https://doi.org/10.2147/TACG.S229952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Rana M Altall,1 Safaa Y Qusti,1 Najlaa Filimban,2 Amani M Alhozali,3 Najat A Alotaibi,4 Ashraf Dallol,2 Adeel G Chaudhary,2 Sherin Bakhashab1,2
1Department of Biochemistry, Faculty of Science, King Abdulaziz University, Jeddah 21589, Kingdom of Saudi Arabia; 2KACST Technology Innovation Center in Personalized Medicine, King Abdulaziz University, Jeddah 21589, Kingdom of Saudi Arabia; 3Department of Internal Medicine, Faculty of Medicine, King Abdulaziz University, Jeddah 21589, Kingdom of Saudi Arabia; 4Department of Family and Community Medicine, Faculty of Medicine, King Abdulaziz University Hospital, Jeddah 21589, Kingdom of Saudi Arabia
Correspondence: Sherin Bakhashab
King Abdulaziz University, P.O. Box 80218, Jeddah 21589, Kingdom of Saudi Arabia
Tel +966 12 6400000
Fax +966 12 6952076
Email [email protected]
Introduction: Type 2 diabetes mellitus (T2DM) is a major global health problem that is progressively affected by genetic and environmental factors. The aim of this study is to determine the influence of solute carrier family 22 member 1 (SLC22A1) rs628031 and rs461473, and ataxia telangiectasia mutated (ATM) rs11212617 polymorphisms on the risk of T2DM in Saudi Arabia by considering many parameters associated with glycemic control of T2DM, such as body mass index (BMI), fasting blood glucose, glycated hemoglobin (HbA1c), and triglyceride.
Methods: In a case-control study, genomic DNA from controls and diabetic groups was isolated and genotyped for each single-nucleotide polymorphism.
Results: There were significant correlations between T2DM and both BMI and HbA1c. Significant associations between G/G and A/G genotypes of rs628031 and rs461473 variants of SLC22A1 and high levels of HbA1c were detected. Therefore, G was predicted to be the risk allele among the assessed SLC22A1 variants. A significant correlation was observed between A/A and A/C genotypes of the rs11212617 polymorphism of ATM and elevated HbA1c. Relative risk calculation confirmed A to be the risk allele in the T2DM population.
Conclusion: Our study showed the risk of the assessed SLC22A1 and ATM variants on glycemic control parameters in diabetic patients.
Keywords: type 2 diabetes mellitus, single-nucleotide polymorphism, solute carrier family 22 member 1, ataxia telangiectasia mutated
Introduction
Type 2 diabetes mellitus (T2DM) is a major chronic disease that is affected by genetic and environmental factors.1,2 The International Diabetic Federation estimated that there were approximately 4.0 million cases of diabetes in Saudi Arabia in 2017.3 Saudi Arabia is ranked fourth in the Middle East/North Africa region in diabetes prevalence.3 Risk factors for T2DM are particularly prevalent among the Saudi Arabian population due to an increase in metabolic syndrome, physical inactivity, obesity, cigarette smoking, and poor dietary habits.4
Establishment of single-nucleotide polymorphism (SNP) databases, development and improvement of cost-effective high-throughput genotyping technology, and multicenter consortium large-scale genome-wide association studies (GWAS) are effective methods to investigate genetic susceptibility to T2DM. By searching susceptibility variants across the entire genome in an unbiased, hypothesis-free manner, GWAS have successfully identified genetic loci strongly related to T2DM, the number of which has risen from just three in 2006 to approximately 70 today.5 The first GWAS research for T2DM was performed on a European cohort in 2007. This analysis identified many novel susceptibility genes associated with T2DM.6 However, studies of European ancestry comprise only a subset of human genetic variation and are considered inadequate to fully characterize T2DM risk variants in other ethnic groups. Furthermore, the latest genome-wide genotyping arrays are less biased toward Europeans, and more recent T2DM GWAS have been performed with great success in populations from other ancestry groups, including South Asians, East Asians, Mexicans, Mexican-Americans, and African-Americans.7
Studies of classic genetic screens have taught us that some candidate genes can indirectly affect the glycemic response, for example, variations in the solute carrier family 22 member 1 (SLC22A1) gene influence the rate of control of T2DM, rather than any major signaling pathway.8 The human SLC22A1 gene is located on chromosome 6q25.3 and encodes for organic cation transporter 1 (OCT1); it consists of 11 exons spanning 37 kb and has been shown to play an important role in the control of the glycemic response of T2DM.9 Population studies have shown a high level of polymorphisms for SLC22A1 in different ethnicities.10,11
Association of the polymorphism rs628031 (M408V) with the glycemic response has been assessed in many studies. It is the most common-genotyped variant with a frequency of 15% to 80% (median, 36%).12 The Japanese population has the highest frequency (80%)13 while rs628031 is present in only 40% of Caucasians.14 Another SLC22A1 variant, rs461473, has not been sufficiently studied. In the Jordanian population, the minor allele frequency was calculated in diabetic subjects (A = 10%) but no significant association between this SNP and glycemic control was detected.15
Mutations in the ataxia telangiectasia mutated (ATM) gene were proposed to have a causative role in ataxia telangiectasia, an autosomal recessive disorder with manifestations including insulin resistance and T2DM.8 A novel variant of the ATM gene (rs11212617) was shown to strongly affect glycemic control in T2DM patients.8 The discovery of the role of ATM polymorphism in the risk of T2DM modulating glycemic response might provide a clue to the treatment mechanism of this disease.16 The ATM gene contributes to DNA repair, cell cycle control and also plays a role in the adenosine monophosphate activation of protein kinase that affects glycemic control of T2DM.17 A 150 kb gene on chromosome 11q22-23, ATM contains 66 exons encoding a 13 kb transcript.9 A previous UK study showed a frequency of 44% for the C allele of the rs11212617 A>C SNP in the ATM gene, and reported that the C allele was associated with an HbA1c level of less than 7%.17 A significant association between the C allele of rs11212617 and HbA1c level in a cohort of Han Chinese diabetes mellitus patients was detected in Shanghai.18
Of great importance in the genetic studies of the pathogenesis of T2DM are the clinical parameters such as reduction of HbA1c, fasting blood glucose (FBS), and postprandial plasma glucose.19 The genotype distribution and allele frequencies of different variants related to glycemic control vary among different populations.14,20 Therefore, the aim of this study is to determine the genotype and allele frequencies of the genetic variants of SLC22A1 (rs628031 and rs461473) and ATM (rs11212617) and detect their association with T2DM risk in western Saudi Arabia.
Materials And Methods
Study Design
The inclusion criteria for this case-control study of 201 T2DM patients were: age >37 years, HbA1c <10%, and under current treatment with metformin and/or other T2DM drugs. Patients with other chronic diseases including cardiovascular disease and metabolic syndrome were excluded. The results from T2DM patients were compared with 89 non-diabetic healthy controls. Patients and controls were recruited either from King Abdulaziz University Hospital or Jeddah Care Center for Diabetes and Hypertension in Jeddah, Saudi Arabia between 2016 and 2018. The study was approved by the Biomedical Ethics Unit, Faculty of Medicine, King Abdulaziz University (approval number 371-16) and Ministry of Health (approval number A00363) and written informed consent was obtained from participants prior to sample collection. The study was conducted in accordance with the Declaration of Helsinki. All participants’ clinical parameters were recorded: age, sex, body weight, height, body mass index (BMI), HbA1c level, FBS, and lipid profile (Table 1). Most patients had a family history of diabetes.
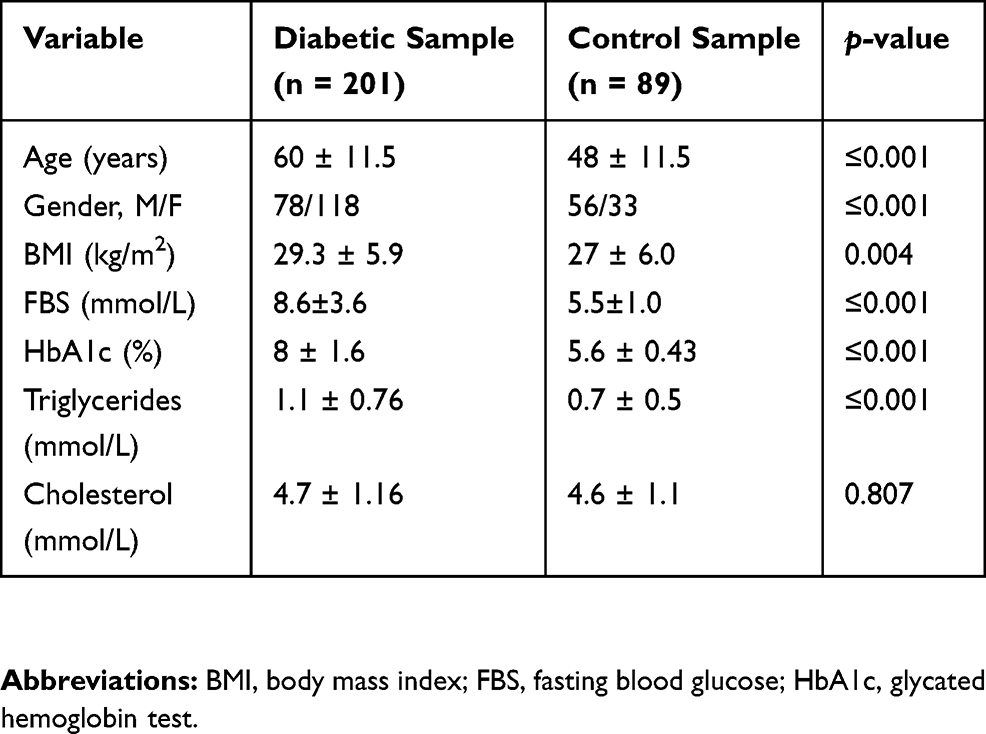 |
Table 1 Clinical Characteristics Of Diabetic And Control Subjects |
Genotyping
Genomic DNA was isolated from peripheral whole blood using the QIAamp DNA Mini Blood Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s instructions. Genotyping of the SLC22A1 variants rs628031 (assay ID: C_8709275_60), rs461473 (assay ID: C_928539_10), and ATM variant rs11212617 (assay ID: C_1314213_10) was performed using TaqMan™ SNP Genotyping Assays (Thermo Fisher Scientific, Waltham, MA, USA). Allelic polymerase chain reaction (PCR) products were analyzed using QuantStudio 12K Flex Real-Time PCR System (Thermo Fisher Scientific, Waltham, MA, USA).
Statistical Analysis
Data analysis was conducted using the IBM SPSS Statistics software, Version 24 (IBM Corp., Armonk, NY, USA). Genotypes and allelic frequencies were calculated within our cohort population to determine the significant differences between T2DM patients and control groups. A binary logistic regression unadjusted model was used to study the association between variables and the study groups. Odds ratios (ORs) were calculated to determine the risk of many variables and development of T2DM using the logistic regression test. For all correlations, p < 0.05 was considered statistically significant.
Results
Allele And Genotype Frequency
The allele frequencies and genotype distributions of SLC22A1 rs461473, rs628031, and ATM rs11212617 are listed in Table 2.
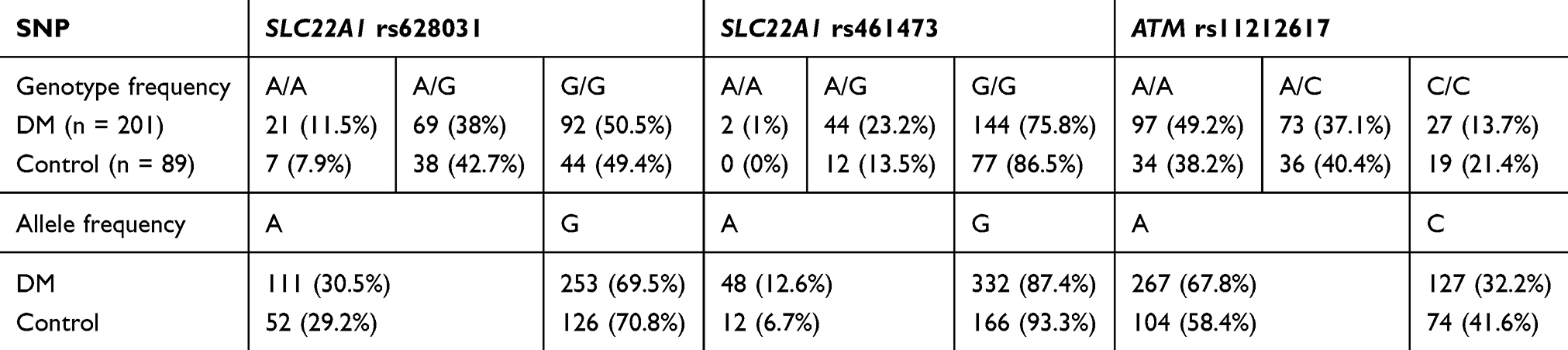 |
Table 2 Genotype And Allele Frequencies For SLC22A1 Variants Rs628031 And Rs461473, And ATM Rs11212617 |
The Association Between Multiple Factors And T2DM
The results revealed strong significant association between T2DM and BMI (OR = 1.072, p = 0.005), FBS (OR = 2.715, p < 0.001), HbA1c (OR = 52.647, p < 0.001), and triglycerides (OR = 1.013, p < 0.001) but not with the other variables using unadjusted binary logistic regression.
The Association Of SLC22A1 Variants Rs628031 And Rs461473 And ATM Variant Rs11212617 With Clinical Parameters For T2DM Patients
The impact of BMI, FBS, HbA1c, and triglycerides on T2DM in the presence of SLC22A1 and ATM variants was determined using binary logistic regression. There was a significant association between BMI and the genotype G/G of SLC22A1 SNP rs628031 (OR = 1.13, p = 0.003). In addition, significant elevation in FBS was more likely associated with G/G and A/G genotypes of SLC22A1 rs628031 (OR = 4.060, p < 0.001; OR = 3.260, p < 0.001). We also found a significant correlation between G/G and A/G genotypes with HbA1c (OR = 156.924, p < 0.001 and OR = 65.6, p < 0.001, respectively); the patients with G/G and A/G are more likely to have a high level of HbA1c than patients with A/A in the rs628031 variant. In addition, G/G and A/G genotypes were correlated with an increase in triglycerides (OR = 1.019, p = 0.001 and OR = 1.01, p = 0.027, respectively). Hence, the G allele in rs628031 is potentially a risk allele associated with high BMI, FBS, HbA1c, and triglycerides in T2DM (summarized in Table 3).
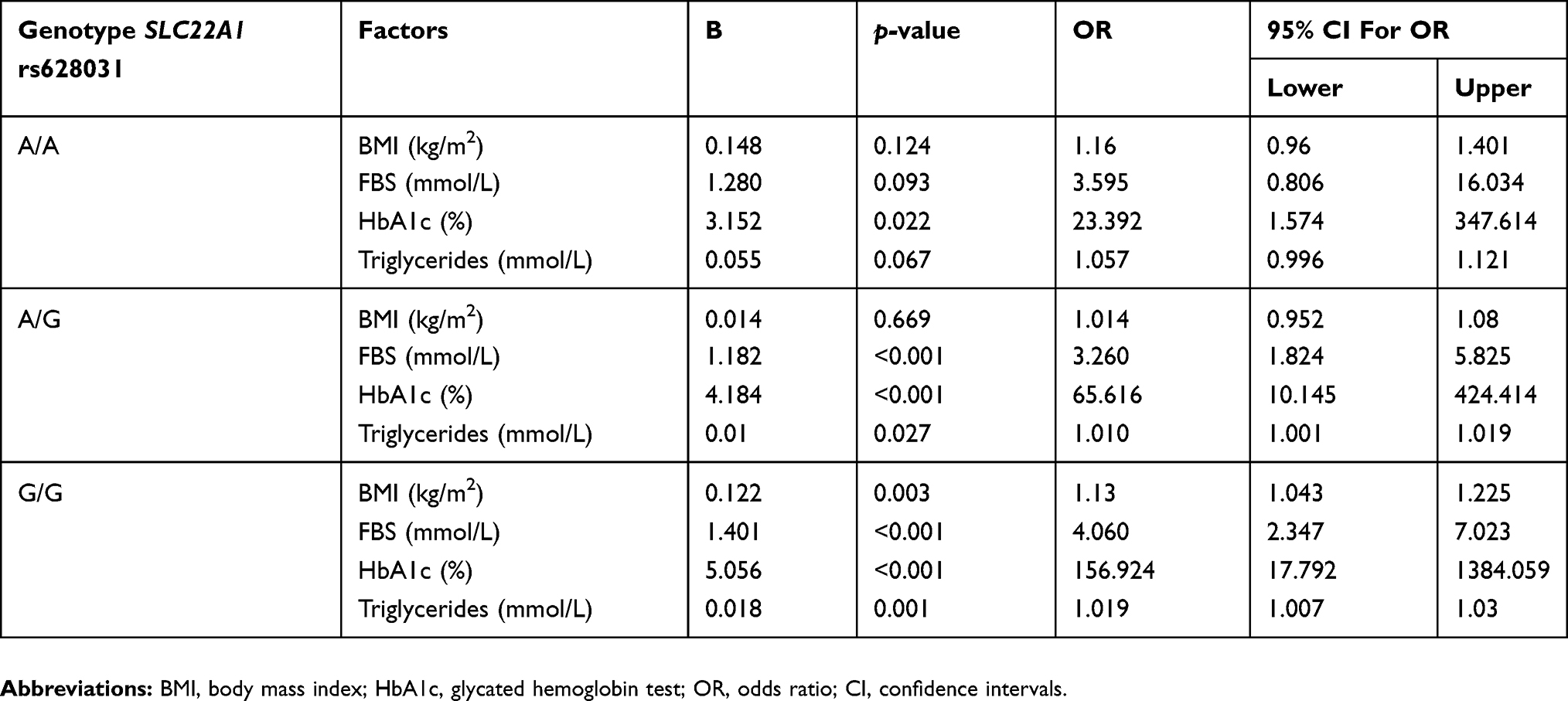 |
Table 3 The Association Of SLC22A1 Variant Rs628031 With T2DM Phenotypes Using Binary Logistic Regression For Patients In Regard To Controls |
Our results showed a significant association between BMI and the genotype G/G of SLC22A1 rs461473 (OR = 1.107, p = 0.001). In addition, patients with G/G and A/G genotypes of SLC22A1 rs461473 were more likely to have high levels of FBS (OR =2.543, p < 0.001 and OR = 14.231, p = 0.008, respectively). There was a significant correlation between G/G and A/G genotypes with HbA1c (OR = 64.124, p < 0.001 and OR = 31.055, p = 0.004, respectively). Therefore, the patients with G/G and A/G are more likely to have greater HbA1c than patients with A/A in rs461473. Furthermore, G/G and A/G genotypes correlated with an increase in triglycerides (OR = 1.013, p < 0.001 and OR = 1.028, p = 0.035, respectively). Thus, the G allele in rs461473 is potentially a risk allele associated with high BMI, FBS, HbA1c, and triglycerides in T2DM (summarized in Table 4).
 |
Table 4 The Association Of SLC22A1 Variant Rs461473 With T2DM Phenotypes Using Binary Logistic Regression For Patients In Regard To Controls |
In ATM variant rs11212617, there was a significant association between FBS and the genotypes A/A (OR = 5.369, p < 0.001) and A/C (OR = 3.059, p < 0.001). In addition, a significant positive correlation between A/A and A/C genotypes and HbA1c was detected (OR = 62.239, p < 0.001 and OR = 83.349, p < 0.001, respectively, Table 5). To confirm the risk allele, the relative risk was calculated to define A as the risk allele highly correlated to T2DM 1.137 times more than the control group.
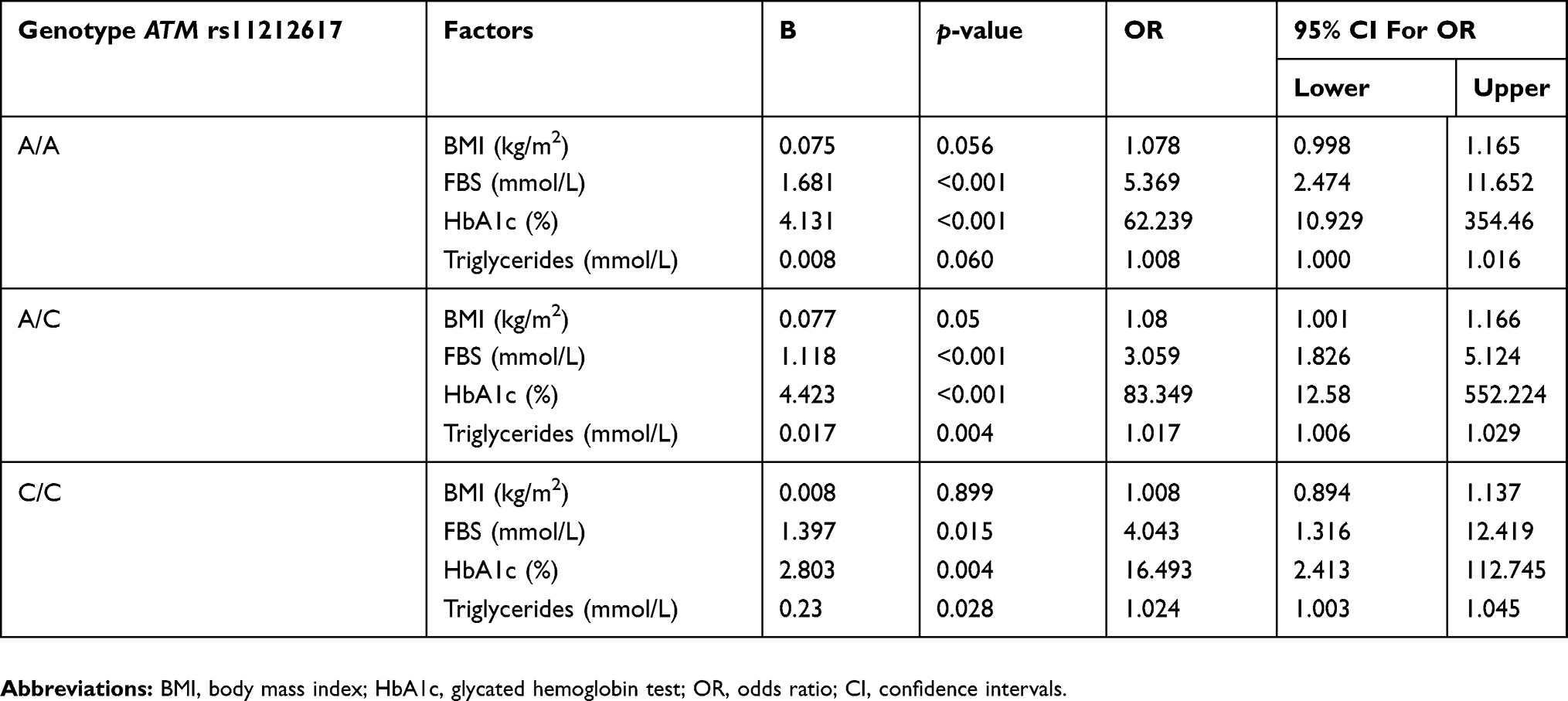 |
Table 5 The Correlation Of ATM Variant Rs11212617 With T2DM Phenotypes Using Binary Logistic Regression For Patients In Regard To Controls |
Discussion
T2DM is a complex metabolic disease with an increasing prevalence particularly over the past two decades,4 in which both genetic determinants and environmental factors play important roles.21 The glycemic control of T2DM varies widely from person to person; research has shown that more than one-third of T2DM patients do not achieve appropriate control of fasting glucose levels.16 The major cause of the uncontrolled glycemic levels of these patients is genetic variation.9,22 The candidate gene approach for conducting genetic association studies focuses on relations between genetic variation within prespecified genes of interest and phenotypes or disease states. Various susceptibility genes for T2DM have recently been identified for several populations through GWAS.4
Studies have largely used genotyping technology with moderate sample sizes to find genetic variants related to T2DM risk.21 Case-control studies are often used to find differences in the allele frequency of a candidate gene among case and control subjects.23,24 Research has shown that the SLC22A1 and ATM genes play an important role in glycemic control in T2DM patients.2,25–27 Most studies have used HbA1c as a surrogate marker for glycemic response and association of candidate genes variants with the risk of T2DM.9 In this study, we showed an association between SLC22A1 and ATM variants and the risk of T2DM in Saudi subjects, and investigated the effect of the genotypes on BMI, FBS, HbA1c, triglycerides, and other factors for T2DM patients.
Several studies have reported a positive association between SLC22A1 variants and T2DM risk28 among Asian, European, and Caucasian populations.12 The common polymorphism of SLC22A1, rs628031 (A>G) causes a missense variant with variable frequencies in different ethnic populations. This polymorphism tends to lower SLC22A1 mRNA expression in enterocytes leading to decreased intestinal uptake and subsequent accumulation of drugs.29 No significant effects of this polymorphism against glycemic response have been detected in Iranians,9 Indians,30 or Japanese populations.13,31 In our study, the frequency of the G allele in rs628031 was 69.5%, similar to other populations such as Koreans (74%),32 Asians living in the USA (76.2%), and African-Americans (73.5%).33 The frequency was slightly lower in European Caucasians (59.8%),33 in Germany (57.4%),34 and in the Netherlands.14 In Han Chinese, the G/G genotype of rs628031 correlated to a significant reduction in fasting plasma glucose and higher levels of HbA1c, whereas the A/A genotype was associated with a significant reduction in HbA1c,18 and a positive predictor of treatment efficacy in the Japanese population.31 Similarly, in the present study, we showed that the G allele in the rs628031 variant is the risk allele, and patients with the G/G genotype have higher levels of HbA1c and FBS than those with A/G and A/A genotypes. Reduced-function polymorphisms of OCT1 were significantly associated with high levels of cholesterol, triglycerides, and low-density lipoprotein. An Oct1 knockout mice model showed loss of function of OCT1 through decreased thiamine uptake in the liver that leads to reduced levels of thiamine pyrophosphate activity causing disruption in the fatty acid oxidation pathway.35 This could explain our genetic finding that OCT1 variants are potentially a genetic risk factor associated with high triglyceride levels in T2DM.
An intronic variant rs461473 in SLC22A1 was also found to be associated with a decrease in HbA1c and glucose lowering after initiation of treatment.36 This finding is compatible with our results as we found a link between the G allele in the SLC22A1 rs461473 variant and raised levels of HbA1c. In contrast, other studies found no significant relationship between the variant and the glycemic control of T2DM patients in Dutch,14 Japanese,31 or Jordanian populations.15
The role of ATM gene variant rs1121617 in the etiology of diabetes was assessed by comparing the allele and genotype frequencies between T2DM patients and control groups. The frequencies follow the Hardy–Weinberg equilibrium, and the A allele is the major allele and the C allele is the minor allele. The frequency of the C allele calculated in our study (32.2%) is similar to that found in South Indian (35%) but it less than those observed in Caucasian (47%), Chinese (69%), Japanese (62%), and African (81%) populations.8 The relationship of the rs1121617 variant to glycemic response as investigated in combined meta-analysis of small cohort studies, suggested that the rs1121617 C allele might be considered the first common susceptibility locus associated with successful treatment in patients with T2DM.17,27 This is consistent with results, which showed T2DM patients carrying the A/A and A/C genotypes of ATM rs11212617 variant had significantly higher levels of HbA1c than the carriers of the C/C genotype, thus, the minor allele C is the protective allele for this variant. In contrast to our results, C carriers in the Diabetes Prevention Program showed no significant differences in treatment effects on insulin sensitivity, FBS, and HbA1c compared to A carriers.25 This could be due to the sample size, period of treatment, or race differences. Replication studies in a relatively large population in a multiethnic diabetic cohort are needed to confirm the role of rs628031 and rs461473 variants of SLC22A1 and rs11212617 polymorphism of ATM on glycemic response to treatment.
Conclusion
In summary, we found that rs628031 and rs461473 of the SLC22A1 gene and rs11212617 of ATM polymorphisms may interact to affect the risk of T2DM by altering the glycemic parameters and other factors in Saudi populations. Our data indicate that T2DM patients with G/G genotype of both rs628031 and rs461473 SLC22A1 variants and A/A genotype of rs11212617 polymorphism of the ATM gene may influence the glycemic response of T2DM patients. In addition, SLC22A1 variants rs628031 and rs461473 could be risk factors for obesity and cardiovascular disease in T2DM as these variants were associated with BMI and triglycerides.
Acknowledgment
The authors would like to show great appreciation to all members of Jeddah Care Center for Diabetes and Hypertension, Jeddah, Saudi Arabia for their kind assistance in collecting the blood samples from the subjects.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Sherifali D, Nerenberg K, Pullenayegum E, Cheng JE, Gerstein HC. The effect of oral antidiabetic agents on A1C levels: a systematic review and meta-analysis. Diabetes Care. 2010;33(8):1859–1864. doi:10.2337/dc09-1727
2. Zhou K, Donnelly LA, Kimber CH, et al. Reduced-function SLC22A1 polymorphisms encoding organic cation transporter 1 and glycemic response to metformin: a GoDARTS study. Diabetes. 2009;58(6):1434–1439. doi:10.2337/db08-0896
3. Diabetes in MENA. IDF diabetes atlas 8th edn 2017. Available from: https://idf.org/our-network/regions-members/middle-east-and-north-africa/diabetes-in-mena.html.
4. Bazzi MD, Nasr FA, Alanazi MS, et al. Association between FTO, MC4R, SLC30A8, and KCNQ1 gene variants and type 2 diabetes in Saudi population. Genet Mol Res. 2014;13(4):10194–10203. doi:10.4238/2014.
5. Kato N. Insights into the genetic basis of type 2 diabetes. J Diabetes Investig. 2013;4(3):233–244. doi:10.1111/jdi.2013.4.
6. Xiao S, Zeng X, Fan Y, et al. Gene polymorphism association with type 2 diabetes and related gene-gene and gene-environment interactions in a Uyghur population. Med Sci Monit. 2016;22:474–487. doi:10.12659/msm.895347
7. Mahajan A, Go MJ, Zhang W, et al. Genome-wide trans-ancestry meta-analysis provides insight into the genetic architecture of type 2 diabetes susceptibility. Nat Genet. 2014;46(3):234–244. doi:10.1038/ng.2897
8. Vilvanathan S, Gurusamy U, Mukta V, Das AK, Chandrasekaran A. Allele and genotype frequency of a genetic variant in ataxia telangiectasia mutated gene affecting glycemic response to metformin in South Indian population. Indian J Endocrinol Metab. 2014;18(6):850–854. doi:10.4103/2230-8210.119944
9. Shokri F, Ghaedi H, Ghafouri Fard S, et al. Impact of ATM and SLC22A1 polymorphisms on therapeutic response to metformin in Iranian diabetic patients. Int J Mol Cell Med. 2016;5(1):1–7.
10. Jacobs C, Pearce B, Du Plessis M, Hoosain N, Benjeddou M. Genetic polymorphisms and haplotypes of the organic cation transporter 1 gene (SLC22A1) in the Xhosa population of South Africa. Genet Mol Biol. 2014;37(2):350–359. doi:10.1590/S1415-47572014005000002
11. Ebid AHIM, Ehab M, Ismail A, Soror S, Mahmoud MA. The influence of SLC22A1 rs622342 and ABCC8 rs757110 genetic variants on the efficacy of metformin and glimepiride combination therapy in Egyptian patients with type 2 diabetes. J Drug Assess. 2019;8(1):115–121. doi:10.1080/21556660.2019.1619571
12. Mato-Mofo E, Guewo Fokeng M, Essop MF, Owira P. Genetic polymorphisms of organic cation transporter 1 (OCT1) and responses to metformin therapy in individuals with type 2 diabetes: a systematic review. Medicine. 2018;97:e11349.
13. Chen L, Takizawa M, Chen E, et al. Genetic polymorphisms in organic cation transporter 1 (OCT1) in Chinese and Japanese populations exhibit altered function. J Pharmacol Exp Ther. 2010;335(1):42–50. doi:10.1124/jpet.110.170159
14. Becker ML, Visser LE, van Schaik RH, Hofman A, Uitterlinden AG, Stricker BH. Genetic variation in the organic cation transporter 1 is associated with metformin response in patients with diabetes mellitus. Pharmacogenomics J. 2009;9(4):242–247. doi:10.1038/tpj.2009.15
15. Al-Eitan LN, Almomani BA, Nassar AM, Elsaqa BZ, Saadeh NA. Metformin pharmacogenetics: effects of SLC22A1, SLC22A2, and SLC22A3 polymorphisms on glycemic control and HbA1c levels. J Pers Med. 2019;9:1. doi:10.3390/jpm9010017
16. Birnbaum MJ, Shaw RJ. Genomics: drugs, diabetes and cancer. Nature. 2011;470(7334):338–339. doi:10.1038/470338a
17. GoDarts, Group UDPS, Wellcome Trust Case Control Consortium, Zhou K, et al. Common variants near ATM are associated with glycemic response to metformin in type 2 diabetes. Nat Genet. 2011;43(2):117–120.
18. Zhou Y, Ye W, Wang Y, et al. Genetic variants of OCT1 influence glycemic response to metformin in Han Chinese patients with type-2 diabetes mellitus in Shanghai. Int J Clin Exp Pathol. 2015;8(8):9533–9542.
19. Becker ML, Pearson ER, Tkac I. Pharmacogenetics of oral antidiabetic drugs. Int J Endocrinol. 2013;2013:686315. doi:10.1155/2013/686315
20. Zhou Y, Guo Y, Ye W, et al. RS11212617 is associated with metformin treatment response in type 2 diabetes in Shanghai local Chinese population. Int J Clin Pract. 2014;68(12):1462–1466. doi:10.1111/ijcp.2014.68.issue-12
21. Siddiqui K, Musambil M, Usmani AM. Established type 2 diabetes-susceptibility genetic variants in Saudi ethnicity: a mini-systematic review. JBC Genetics. 2018;1(2):57–65. doi:10.24911/JBCGenetics
22. Sissung TM, Troutman SM, Campbell TJ, et al. Transporter pharmacogenetics: transporter polymorphisms affect normal physiology, diseases, and pharmacotherapy. Discov Med. 2012;13(68):19–34.
23. Kwon JM, Goate AM. The candidate gene approach. Alcohol Res Health. 2000;24(3):164–168.
24. Zhu M, Zhao S. Candidate gene identification approach: progress and challenges. Int J Biol Sci. 2007;3(7):420–427. doi:10.7150/ijbs.3.420
25. Florez JC, Jablonski KA, Taylor A, et al. The C allele of ATM rs11212617 does not associate with metformin response in the diabetes prevention program. Diabetes Care. 2012;35(9):1864–1867. doi:10.2337/dc11-2301
26. Mahrooz A, Parsanasab H, Hashemi-Soteh MB, et al. The role of clinical response to metformin in patients newly diagnosed with type 2 diabetes: a monotherapy study. Clin Exp Med. 2015;15(2):159–165. doi:10.1007/s10238-014-0283-8
27. van Leeuwen N, Nijpels G, Becker ML, et al. A gene variant near ATM is significantly associated with metformin treatment response in type 2 diabetes: a replication and meta-analysis of five cohorts. Diabetologia. 2012;55(7):1971–1977. doi:10.1007/s00125-012-2537-x
28. Dawed AY, Zhou K, Pearson ER. Pharmacogenetics in type 2 diabetes: influence on response to oral hypoglycemic agents. Pharmgenomics Pers Med. 2016;9:17–29. doi:10.2147/PGPM.S84854
29. Semiz S, Dujic T, Causevic A. Pharmacogenetics and personalized treatment of type 2 diabetes. Biochem Med (Zagreb). 2013;23(2):154–171. doi:10.11613/issn.1846-7482
30. Sur D. A tale of genetic variation in the human SLC22A1 gene encoding OCT1 among type 2 diabetes mellitus population groups of West Bengal, India. Posters-Accepted Abstracts of the 3rd International Conference on Genomics & Pharmacogenomics. San Antonio, TX, 2015. J Mol Genet Med.
31. Shikata E, Yamamoto R, Takane H, et al. Human organic cation transporter (OCT1 and OCT2) gene polymorphisms and therapeutic effects of metformin. J Hum Genet. 2007;52(2):117–122. doi:10.1007/s10038-006-0087-0
32. Kang HJ, Song IS, Shin HJ, et al. Identification and functional characterization of genetic variants of human organic cation transporters in a Korean population. Drug Metab Dispos. 2007;35(4):667–675. doi:10.1124/dmd.106.013581
33. Shu Y, Leabman MK, Feng B, et al. Evolutionary conservation predicts function of variants of the human organic cation transporter, OCT1. Proc Natl Acad Sci USA. 2003;100(10):5902–5907. doi:10.1073/pnas.0730858100
34. Tzvetkov MV, Vormfelde SV, Balen D, et al. The effects of genetic polymorphisms in the organic cation transporters OCT1, OCT2, and OCT3 on the renal clearance of metformin. Clin Pharmacol Ther. 2009;86(3):299–306. doi:10.1038/clpt.2009.92
35. Liang X, Yee SW, Chien HC, et al. Organic cation transporter 1 (OCT1) modulates multiple cardiometabolic traits through effects on hepatic thiamine content. PLoS Biol. 2018;16(4):e2002907. doi:10.1371/journal.pbio.2002907
36. Christensen MM, Brasch-Andersen C, Green H, et al. The pharmacogenetics of metformin and its impact on plasma metformin steady-state levels and glycosylated hemoglobin A1c. Pharmacogenet Genomics. 2011;21(12):837–850. doi:10.1097/FPC.0b013e32834c0010
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.