")
Back to Journals » OncoTargets and Therapy » Volume 8
Simultaneous hepatectomy and splenectomy versus hepatectomy alone for hepatocellular carcinoma complicated by hypersplenism: a meta-analysis
Authors Li W, Shen S, Wu S, Chen Z, Hu C, Yan R
Received 29 April 2015
Accepted for publication 14 July 2015
Published 19 August 2015 Volume 2015:8 Pages 2129—2137
DOI https://doi.org/10.2147/OTT.S87580
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Daniele Santini
Wei Li, Shi-Qiang Shen, Shan-Min Wu, Zu-Bing Chen, Chao Hu, Rui-Chen Yan
Department of General Surgery, Renmin Hospital of Wuhan University, Wuhan, People’s Republic of China
Background: This study systematically compared the efficacy and safety of simultaneous hepatectomy and splenectomy (HS) with hepatectomy (H) alone in patients with hepatocellular carcinoma (HCC) and hypersplenism.
Methods: The PubMed, Web of Science, Science Direct, EMBASE, and Cochrane Library databases were systematically searched by two independent researchers through to March 31, 2015 to identify relevant studies. All the extracted literature were managed by Bibliographic citation management software. Quality assessment of the included studies was performed using a modified Newcastle–Ottawa Scale judgment. The data were analyzed using RevMan5.2 software.
Results: Eight studies including a total of 761 patients with HCC and hypersplenism (360 in the HS group, 401 in the H group) were finally included in the analysis. Outcomes, including postoperative complications, perioperative mortality, operation time, 5-year survival rate, and need for blood transfusion did not differ significantly between the two groups. HS was associated with significantly more intraoperative bleeding (mean difference [MD] 57.15, 95% confidence interval [CI] 18.83–95.46, P=0.003), and CD4/CD8 ratio (MD 0.69, 95% CI 0.61–0.77, P<0.00001), CD4 subset, platelet count (MD 213.06, 95% CI 202.59–223.53, P<0.0001), white blood cell count (MD 4.85, 95% CI 4.58–5.13, P<0.0001), interferon-gamma levels (MD 18.52, 95% CI 13.93–23.11, P<0.00001), and interleukin-2 levels (MD 20.73, 95% CI 16.05–25.41, P<0.0001). In addition, lower CD8 subset (MD −7.85, 95% CI −9.07, −6.63, P<0.00001) and interleukin-10 levels (MD −18.56, 95% CI −22.61, −14.50, P<0.00001) were observed for HS.
Conclusion: We identified that simultaneous HS do not increase postoperative complications, operation time, or perioperative mortality in patients with HCC and hypersplenism. Simultaneous splenectomy can increase postoperative white blood cell and platelet counts significantly, improve blood coagulation, reduce the incidence of postoperative bleeding, and enhance immunity. Therefore, HS is safe, effective, and feasible for patients with HCC and hypersplenism.
Keywords: hepatocellular carcinoma, hypersplenism, simultaneous hepatectomy and splenectomy, hepatectomy, meta-analysis
Introduction
Hepatocellular carcinoma (HCC) is a common malignant tumor and the third leading cause of tumor-related death worldwide.1 Hepatectomy is regarded as an effective treatment for HCC, which is often complicated by splenomegaly and hypersplenism. Hypersplenism results in pancytopenia, and hepatectomy in patients with hypersplenic thrombocytopenia may cause a perioperative bleeding episode and sometimes liver failure.2 Therefore, many surgeons hesitate to perform hepatectomy for patients with HCC and hypersplenism. Splenectomy is perceived as a good management technique for hypersplenism, as it helps to improve thrombocytopenia and leukopenia and decrease pressure in the portal veins.3,4 In addition, some studies suggest that splenectomy may help to improve liver function,5–7 nutritional metabolism,6 and Child–Pugh scores.8 However, whether patients with HCC and hypersplenism should undergo hepatectomy and a concomitant splenectomy remains controversial. To address these issues and provide more references on the treatment of HCC complicated by hypersplenism, we conducted an integrated quantitative evaluation using meta-analysis to compare the efficacy and safety of simultaneous hepatectomy and splenectomy (HS) or hepatectomy (H) alone in patients with HCC and hypersplenism.
Materials and methods
Search strategy
A systematic search was conducted in the PubMed, Web of Science, Science Direct, EMBASE, and Cochrane Library databases until March 31, 2015, with no limits. The search strategies were based on combinations of the following keywords: hepatocellular carcinoma, hypersplenism, liver resection, splenectomy, comparative study, efficacy, liver cancer, primary liver carcinoma, and hepatectomy. In addition, we checked relevant reviews on the topic of interest. We traced the reference lists of selected articles and used Google Scholar to find potential studies. No approval was required from the Institutional Review Board regarding the approval for this study.
Inclusion and exclusion criteria
Randomized controlled trials, clinical controlled studies, and case-control studies were identified. The inclusion criteria were: a clear diagnosis of HCC (including computed tomography, magnetic resonance imaging, serum alpha-fetoprotein levels, and pathology after surgery) and a diagnosis of hypersplenism (mild, white blood cell [WBC] count <3.5×109/L and/or platelet count <150×109/L, severe, WBC count <2.0×109/L and/or platelet count <75×109/L, and splenomegaly that was classified as greater than class I [spleen enlarged beyond left subcostal margin and palpable]);9 comparison of HS with H; and available data for each surgical regimen. The exclusion criteria were: compared two surgical procedures in an animal model; only reported one surgical procedure (hepatectomy or splenectomy); data could not be used for statistical analysis; hepatectomy and splenectomy was conducted step by step or by laparoscopic surgery; basic preoperative situation of the two groups was obviously different; and articles from the same author or institution that contained significant overlap of patient data.
Data extraction and quality assessment
Data on all variables and outcomes were extracted from eligible studies by two reviewers independently. The extracted information included: baseline information on articles (authors, research areas, publication year, and grouping methods); general information (case numbers, operative methods, Child–Pugh classification, tumor size, mean age, sex ratio); treatment outcomes (eg, perioperative mortality, postoperative complications [pleural effusion, upper gastrointestinal hemorrhage, bile leakage, pulmonary infection, abdominal cavity hemorrhage, incision infection, hyperbilirubinemia], CD4, CD8, CD4/CD8 ratio, interferon [IFN]-γ levels, interleukin [IL]-2 levels, IL-10 levels, postoperative WBC and platelet counts, and 5-year survival rate). Disagreements were resolved by discussion or consulting experts. If necessary, the primary authors were contacted to obtain missing data. A modification of the Newcastle–Ottawa Scale was used as an assessment tool for selection, comparability, and outcome assessment.
Outcome definition
Perioperative mortality was defined as death in hospital within 30 days following surgery. Complications included both hepatic and extrahepatic events.
Statistical analysis
The data were analyzed using RevMan 5.2 software. We analyzed dichotomous variables using odds ratios (ORs) or risk differences along with 95% confidence intervals (CIs), and analyzed continuous data using mean differences (MDs) along with 95% CIs. The I2 and P-value were used for evaluation of heterogeneity. A fixed-effects model was used when the heterogeneity test showed better homogeneity (P>0.1).10,11 Otherwise, a random-effects model was used. With regard to outcomes when significant heterogeneity existed across studies, sensitivity analysis was conducted by respectively omitting each study to explore the influence of each individual study on the merged data.
Assessment of publication bias
Publication bias is an important factor that affects the authenticity of the results of meta-analyses. For various reasons, the literature published in journals may differ from unpublished studies. The existence of this type of bias cannot be completely resolved by a meta-analysis itself. In this meta-analysis, a funnel plot was drawn using the funnel plot command in the RevMan software (Figure 1), which indicated no obvious publication bias in the studies included.
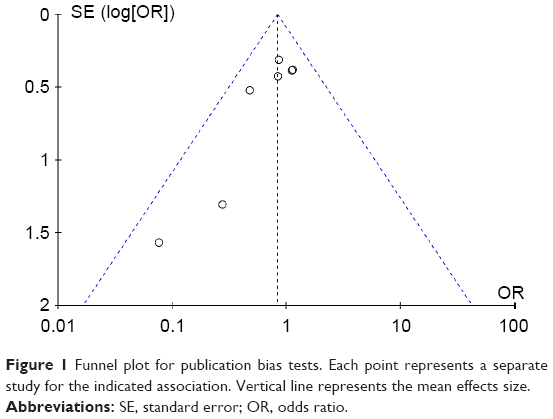 | Figure 1 Funnel plot for publication bias tests. Each point represents a separate study for the indicated association. Vertical line represents the mean effects size. |
Results
Characteristics of pooled studies
A flow diagram of the search strategy for study selection and inclusion is shown in Figure 2. A total of 325 relevant abstracts were retrieved in the initial search based on the search strategy described above. A total of 291 studies were excluded for having irrelevant titles, and/or abstracts. Twenty-one studies were excluded for being reviews or updates, or containing data that were not able to be compared, three studies were excluded because they were published by the same authors and institutions and contained significant overlap of patient data which had already been published in other studies,12–14 and another two studies were excluded because the H groups were not complicated with hypersplenism.15,16 Consequently, eight studies including a total of 761 patients comparing the outcomes of HS with H alone were included in this meta-analysis.17–24 The basic characteristics of all studies included in the meta-analysis are detailed in Table 1.
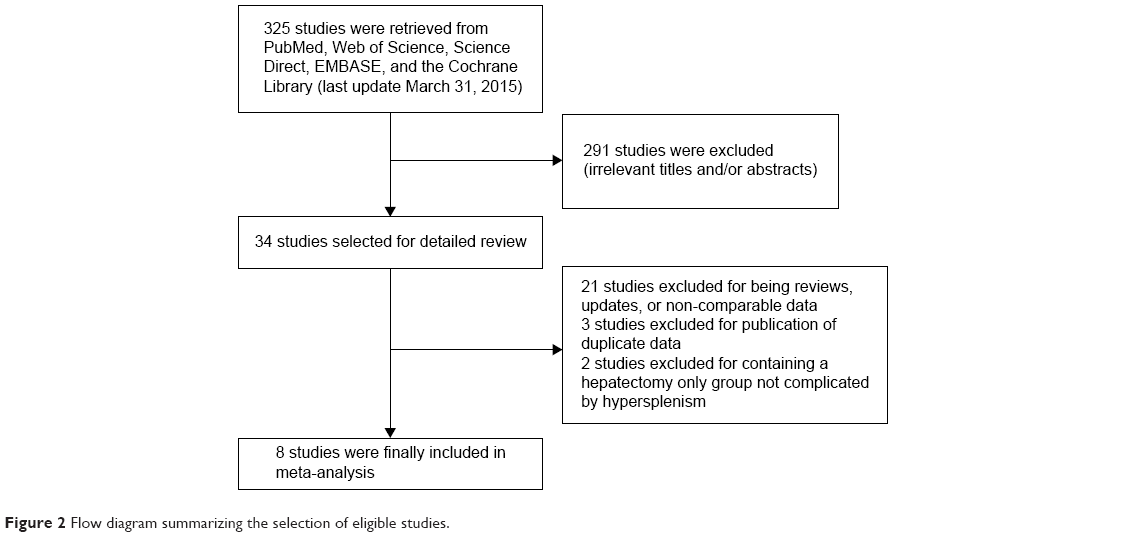 | Figure 2 Flow diagram summarizing the selection of eligible studies. |
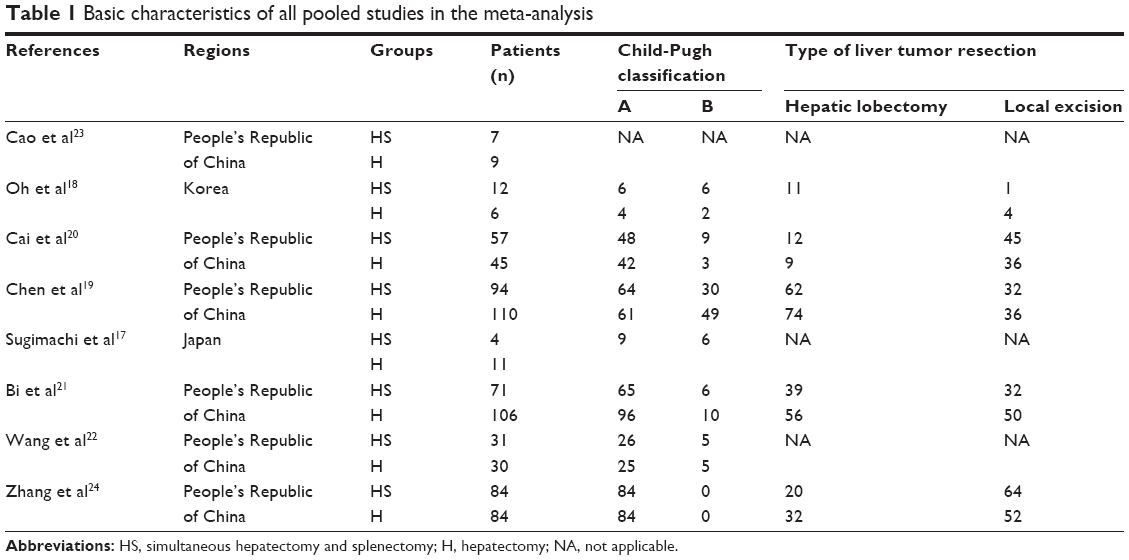 | Table 1 Basic characteristics of all pooled studies in the meta-analysis |
Quality judgments for studies
All the included studies were analyzed retrospectively. Due to the specificity and ethics, the surgeons could not randomly allocate patients into the two groups. Finally, eight retrospective case-control studies were included in the analysis. The quality of the literature was assessed using a modification of the Newcastle–Ottawa Scale.25 The results of this assessment are shown in Table 2. Of the eight included articles, three were published before 2005, and the other five were published after 2005. Studies given more than four stars were recognized as being moderate to high quality.
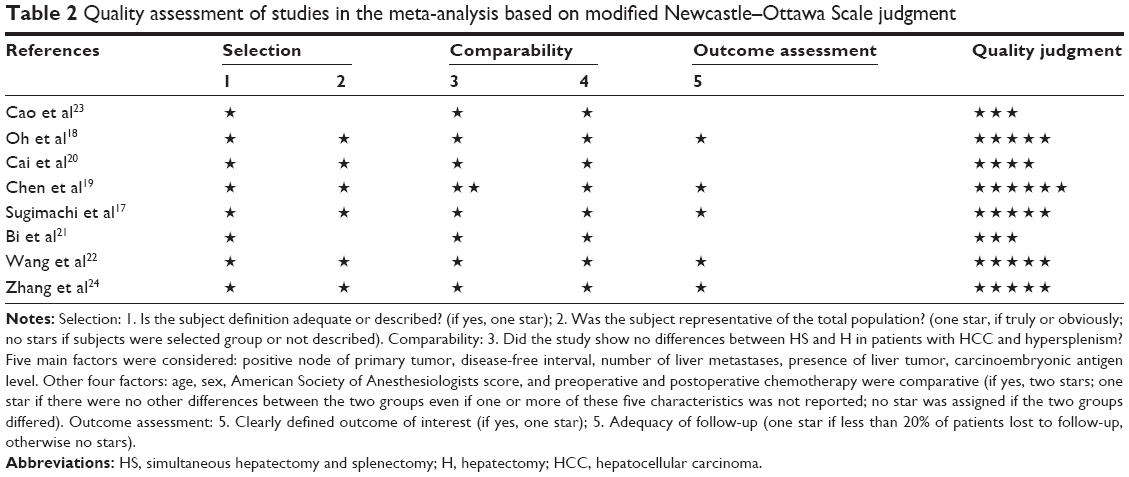 | Table 2 Quality assessment of studies in the meta-analysis based on modified Newcastle–Ottawa Scale judgment |
Immunology results
With respect to immune function and cell count-related outcomes, eight endpoints, including CD4/CD8 ratio, CD4 subset, CD8 subset, IFN-γ levels, IL-10 levels, IL-2 levels, and WBC and platelet counts, were analyzed. High IL-2 levels, IFN-γ levels, CD4 subset, and CD4/CD8 ratio, and low IL-10 levels and CD8 subset in HS were highly significant (P<0.00001–0.005). Moreover, in the quantitative analysis of WBC counts, HS was significantly superior to H (MD 4.85, 95% CI 4.58–5.13, P<0.00001) and platelet counts were higher in HS than that in H alone (MD 213.06, 95% CI 202.59–223.53, P<0.00001; Table 3).
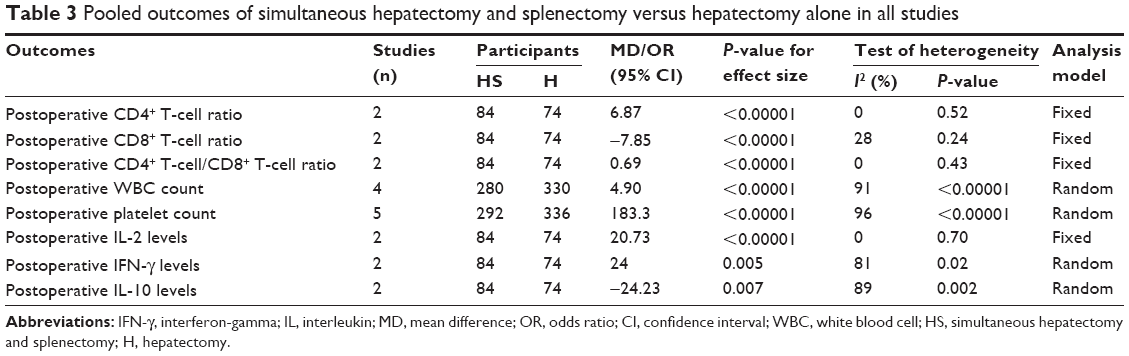 | Table 3 Pooled outcomes of simultaneous hepatectomy and splenectomy versus hepatectomy alone in all studies |
Operation-related results
With respect to operation-related outcomes, five endpoints, including postoperative complications, perioperative mortality, operation time, intraoperative blood loss, and need for blood transfusion were analyzed. Three studies reported perioperative mortality.17,18,20 Overall, perioperative mortality did not differ significantly between the two surgical approaches (OR 0.48, 95% CI 0.09–2.50, P=0.38; Figure 3A). Seven studies reported postoperative complications.17–22,24 Postoperative complications were assessed with no significant difference between the two surgical approaches for patients with HCC and hypersplenism (OR 0.84, 95% CI 0.60–1.17, P=0.29; Figure 3B). Six studies reported intraoperative blood loss.17–19,21,22,24 More intraoperative blood loss was found with simultaneous HS, which was highly significant (MD 57.15, 95% CI 18.83–95.46, P=0.003; Figure 3C). Four studies reported operation time,17–19,21 which was not significantly different between the two surgical approaches (MD 37.99, 95% CI −11.75, 87.73, P=0.13; Figure 3D). Moreover, three studies reported blood transfusion,17,19,24 which did not differ significantly between the two surgical approaches (OR 1, 95% CI 0.58–1.71, P=0.99; Figure 3E). In terms of long-term results, two studies were pooled for analysis19,20 and no significant difference in 5-year overall survival rates was observed between the two surgical approaches for patients with HCC and hypersplenism (risk difference 0.08, 95% CI −0.03, 0.19, P=0.18; Figure 3F).
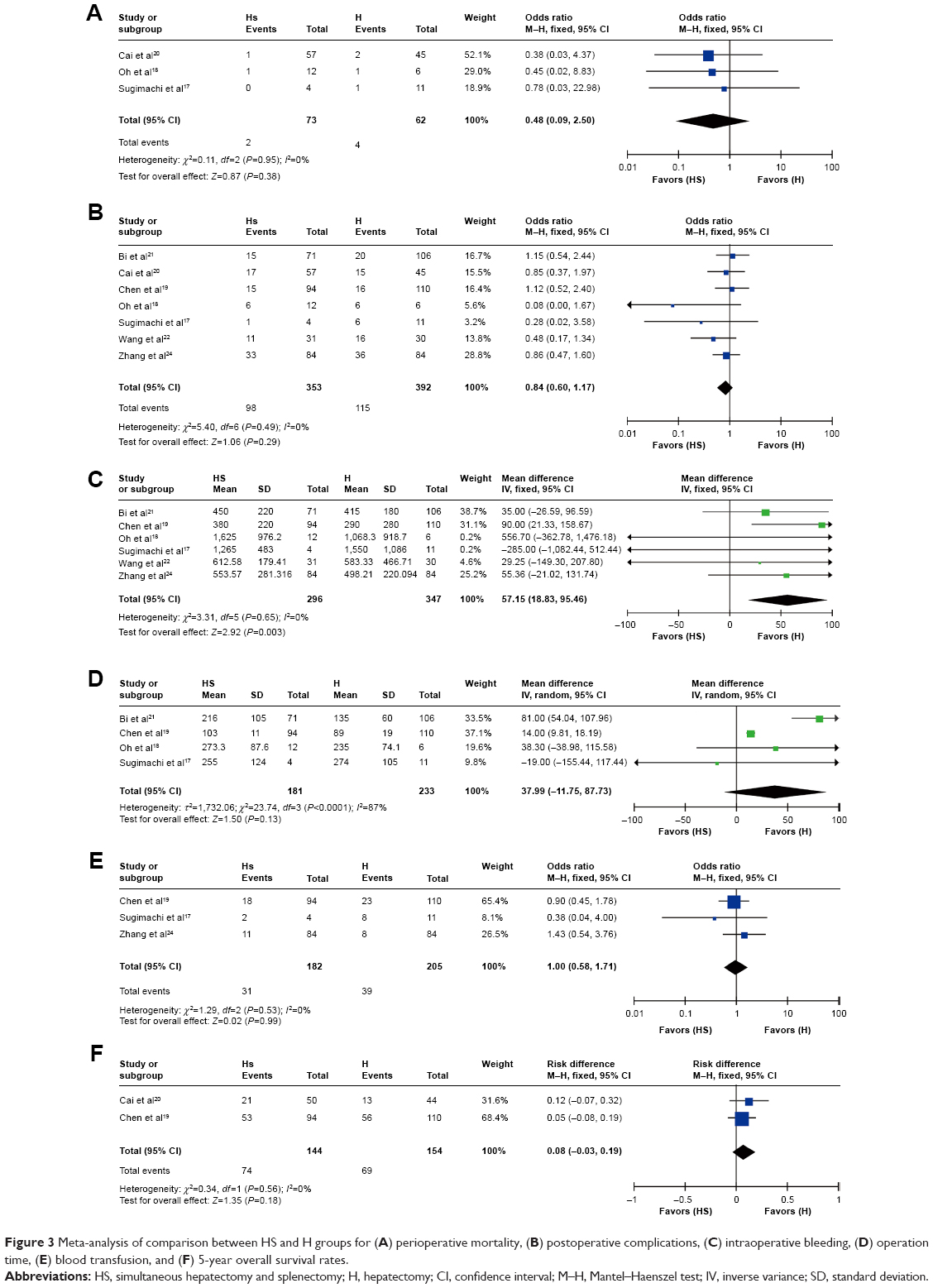 | Figure 3 Meta-analysis of comparison between HS and H groups for (A) perioperative mortality, (B) postoperative complications, (C) intraoperative bleeding, (D) operation time, (E) blood transfusion, and (F) 5-year overall survival rates. |
Heterogeneity
High heterogeneity was detected for WBC counts (I2=91%, P<0.00001), platelet counts (I2=96%, P<0.00001), IL-10 levels (I2 =89%, P=0.002), IFN-γ levels (I2=81%, P=0.02), and operation time (I2=87%, P<0.0001). Sensitivity analysis was then conducted by omitting each single study. There were no changes in outcomes compared with primary outcomes.
Discussion
In recent years, the 5-year survival rate has been reported to reach 50%–70% in strictly selected patients undergoing liver resection, percutaneous radiofrequency ablation, or liver transplantation for the treatment of early HCC.26 Under current medical conditions, hepatectomy is still the primary treatment for HCC. Splenectomy has been suggested for the treatment of secondary hypersplenism and thrombocytopenia.27 Sugawara et al28 recommended splenectomy as an aid to extend the patient selection criteria for hepatectomy to patients with HCC and hypersplenism. Hypersplenism can lead to decreased WBC and platelet counts, which can lower the body’s resistance to infection and cause coagulopathy, which is traditionally considered as a contraindication to HS for patients with HCC and hypersplenism. However, some patients have good hepatic reserve, and improvements in preoperative preparation, surgical techniques, and postoperative care can raise the ability to tolerate HS. Two-stage hepatectomy and splenectomy may lead to complications and inevitably prolongs the overall treatment time. Hepatectomy conducted after splenectomy when WBC and platelet counts return to normal may reduce the surgical risk, but may increase the risks of tumor recurrence and metastasis. Hepatectomy before splenectomy may result in uncontrolled intraoperative and postoperative oozing of blood from surgical wounds and lead to further severe liver damage, uncontrolled hemorrhagic shock, and multiple organ failure due to factors such as coagulation disorder and thrombocytopenia. Simultaneous splenectomy can increase postoperative WBC and platelet counts significantly, improve blood coagulation, and reduce the incidence of postoperative bleeding. Therefore, some researchers17–24 have considered HS to be beneficial for patients with HCC and hypersplenism. However, their studies have been retrospective in nature and have included limited numbers of cases. There has been no convincing evidence for the efficacy and safety of simultaneous HS for patients with HCC and hypersplenism. The aim of this meta-analysis was to evaluate the efficacy and safety of HS versus H alone in patients with HCC and hypersplenism by comparing the short-term and long-term results between the two groups.
In addition to complications related to technical errors and perioperative evaluation, portal vein thrombosis and uncontrolled infection are known to be life-threatening complications after simultaneous HS.29–31 The results of our meta-analysis indicate that there is no significant difference in terms of perioperative mortality between simultaneous HS and H alone for patients with HCC and hypersplenism, and HS does not increase the risk of postoperative complications. Overwhelming infection is a well-known and much feared complication after splenectomy. The incidence is low, with a higher death rate in children. The interval between splenectomy and first infection ranges from 15 to 49.7 months. Theoretically, liver cirrhosis is an immunocompromised condition, but overwhelming sepsis has rarely been reported after splenectomy for hypersplenism in cirrhotic patients in other studies.32,33 No overwhelming post splenectomy infection was reported over a long follow-up period in patients who underwent simultaneous HS in any of the included studies. Portal vein thrombosis refers to the complete or partial obstruction of blood flow in the portal vein due to the presence of a thrombus in the vasal lumen, and is a severe complication after splenectomy. In our study, only one patient was identified to have portal vein thrombus, which resolved on conservative treatment. Hepatectomy also raises the portal vein pressure, which increases the risk of upper gastrointestinal hemorrhage. Splenectomy reduces the portal vein inflow by 20%–30%, consequently decreasing portal vein pressure34 and reducing the risk of upper gastrointestinal hemorrhage. In our meta-analysis, the incidence of upper gastrointestinal hemorrhage after simultaneous HS was 2.63 % (five of 190 cases), whereas the incidence of upper gastrointestinal hemorrhage after H alone was 5% (ten of 200 cases).
Acknowledging that the spleen normally plays a key role in preventing infection, the changes in immune function caused by splenectomy is another concern. The spleen in a patient with HCC and hypersplenism often shows negative immune function. In addition, research has shown that the spleen in a tumor-burdened host attracts a large number of inhibitory macrophages; these cells change the structure and function of the TCR-CD3 complex, thus inhibiting the immune function of T lymphocytes.35 The cellular response plays a central role in anti-tumor immunity. CD4 T lymphocytes mainly produce cytokines to regulate anti-tumor immunity, and CD8 T lymphocyte cells produce immunosuppressive cytokines. So, to a certain extent, determination of T lymphocyte subsets could reflect the body’s immune function. Th1 cells produce IL-2 and IFN-γ and promote a cellular immune response, so play an important role in anti-tumor immunity, whereas Th2 cells mainly produce IL-4 and IL-10 and inhibit secretion of Th1 cells. Splenectomy may reduce destruction and storage of platelets and WBCs in the spleen, and at the same time reduce platelet-related antibody levels in serum and increase platelet production by increasing the release of thrombopoietin. The results of our meta-analysis showed that after simultaneous HS, postoperative WBC and platelet counts return to normal, and T lymphocyte subsets such as CD4 and CD4/CD8 and levels of Th1 lymphocyte cytokines such as IL-2 and IFN-γ increased, but T lymphocyte subsets such as CD8 and Th2 lymphocyte cytokines such as IL-10 decreased. These variations indicate, to some extent, that simultaneous HS reduced the risk of perioperative bleeding, avoided immunosuppression of the spleen, and enhanced anti-tumor immunity. Moreover, it created favorable conditions for subsequent transcatheter arterial chemoembolization and adjuvant chemotherapy, hopefully improving the prognosis for patients.36
The results of our meta-analysis indicate more intraoperative blood loss with simultaneous HS than with H alone. However, operation time and need for blood transfusion did not differ significantly between the two surgical approaches. Patients with HCC and hypersplenism often have severe cirrhosis, and simultaneous HS increased the surgical trauma. Therefore, reasonable perioperative management, and careful operation are helpful to decrease perioperative bleeding and are the key to successful surgery and an uneventful postoperative recovery.
Cumulative survival rates, disease-free survival rates, and tumor recurrence rates are important outcomes to evaluate the therapeutic effect of antitumor treatment.37 It is reported that chemotherapy helps to prevent recurrence of HCC after liver resection.38,39 HCC patients often have splenomegaly and hypersplenism, which will limit their ability to tolerate postoperative chemotherapy. An increase in WBC and platelet counts after splenectomy will be favorable for postoperative chemotherapy. Unfortunately, the 5-year survival rates for the two treatment groups were not significantly different in our study; however, we could only find two relevant studies for inclusion in our meta-analysis, so more studies are needed in this area. The two studies19,24 we identified had reported that 5-year relapse-free survival was better in patients who underwent simultaneous HS than in those who underwent H alone; however, we could not compare the relapse-free survival rate between the HS and H groups because only one study provided the data needed to do so.
There are several limitations to this meta-analysis. First, the patient numbers included were small. Second, we did not include studies published in other languages (eg, German, French, Spanish), which may have resulted in a degree of selection bias. Third, a funnel plot analysis is valid only if more than ten trials are included, and we could only include eight studies.
In conclusion, we identified that simultaneous HS does not increase postoperative complications, operation time, or operative mortality in patients with HCC and hypersplenism. Simultaneous HS can increase postoperative WBC and platelet counts significantly, improve blood coagulation, reduce the incidence of postoperative bleeding, and enhance immunity. Therefore, HS is safe, effective, and feasible for patients with HCC and hypersplenism. We suggest simultaneous HS for patients with these two conditions.
Disclosure
The authors report that they have no financial and personal relationships with other people or organizations that could inappropriately influence their work, and no professional or other personal interest of any nature or kind in any product, service, and/or company that could be construed as influencing the position presented in this paper.
References
Li C, Wen TF, Liao ZX, et al. Recurrence of hepatocellular carcinoma after liver transplantation: recurrence characteristics and risk factors. Hepatogastroenterology. 2010;57:567–570. | ||
Schuppan D, Afdhal NH. Liver cirrhosis. Lancet. 2008;371:838–851. | ||
Alzen G, Basedow J, Luedemann M, Berthold LD, Zimmer KP. [Partial splenic embolization as an alternative to splenectomy in hypersplenism – single center experience in 16 years]. Klin Padiatr. 2010;222:368–373. | ||
Amin MA, el-Gendy MM, Dawoud IE, Shoma A, Negm AM, Amer TA. Partial splenic embolization versus splenectomy for the management of hypersplenism in cirrhotic patients. World J Surg. 2009;33:1702–1710. | ||
Ikegami T, Shimada M, Imura S. Recent role of splenectomy in chronic hepatic disorders. Hepatol Res. 2008;38:1159–1171. | ||
Imura S, Shimada M, Utsunomiya T, et al. Impact of splenectomy in patients with liver cirrhosis: results from 18 patients in a single center experience. Hepatol Res. 2010;40:894–900. | ||
Tomikawa M, Hashizume M, Akahoshi T, et al. Effects of splenectomy on liver volume and prognosis of cirrhosis in patients with esophageal varices. J Gastroenterol Hepatol. 2002;17:77–80. | ||
Shimada M, Hashizume M, Shirabe K, et al. A new surgical strategy for cirrhotic patients with hepatocellular carcinoma and hypersplenism: performing a hepatectomy after a laparoscopic splenectomy. Surg Endosc. 2000;14:127–130. | ||
Liangpunsakul S, Ulmer BJ, Chalasani N. Predictors and implications of severe hypersplenism in patients with cirrhosis. Am J Med Sci. 2003;326:111–116. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. | ||
Chen XP, Wu ZD, Qiu FZ. [Role of united hepatectomy and splenectomy in the surgical treatment of hepatocellular carcinoma complicated with hepatic cirrhosis and hypersplenism]. Zhonghua Wai Ke Za Zhi. 2005;43:442–446. Chinese. | ||
Cao Z, Cheng X, Wu Z. [Changes of immune function in liver cirrhosis patients after splenectomy combined with resection of hepatocellular carcinoma]. Zhonghua Wai Ke Za Zhi. 2002;40:97–99. Chinese. | ||
Cao ZX, Chen XP, Wu ZD. Effects of splenectomy in patients with cirrhosis undergoing hepatic resection for hepatocellular carcinoma. World J Gastroenterol. 2003;9:2460–2463. | ||
Wu CC, Cheng SB, Ho WM, et al. Appraisal of concomitant splenectomy in liver resection for hepatocellular carcinoma in cirrhotic patients with hypersplenic thrombocytopenia. Surgery. 2004;136:660–668. | ||
Kim SH, Kim do Y, Lim JH, et al. Role of splenectomy in patients with hepatocellular carcinoma and hypersplenism. ANZ J Surg. 2013;83:865–870. | ||
Sugimachi K, Ikeda Y, Tomikawa M, et al. Appraisal of hepatic resection in the treatment of hepatocellular carcinoma with severe thrombocytopenia. World J Surg. 2008;32:1077–1081. | ||
Oh JW, Ahn SM, Kim KS, Choi JS, Lee WJ, Kim BR. The role of splenectomy in patients with hepatocellular carcinoma and secondary hypersplenism. Yonsei Med J. 2003;44:1053–1058. | ||
Chen XP, Wu ZD, Huang ZY, Qiu FZ. Use of hepatectomy and splenectomy to treat hepatocellular carcinoma with cirrhotic hypersplenism. Br J Surg. 2005;92:334–339. | ||
Cai JQ, Hu JQ, Bi XY, et al. [Long-term effect of united hepatectomy and splenectomy on treatment of hepatocellular carcinoma complicated with cirrhosis and hypersplenism]. Zhonghua Yi Xue Za Zhi. 2004;84:6–8. Chinese. | ||
Bi XY, Zhao JJ, Yan T, et al. [Peri-operative treatment for hepatocellular carcinoma patients complied with cirrhosis and hypersplenism]. Zhonghua Wai Ke Za Zhi. 2010;48:1539–1541. Chinese. | ||
Wang C, Li C, Wen TF, et al. Safety of synchronous hepatectomy and splenectomy for patients with hepatocellular carcinoma and hypersplenism. Hepatogastroenterology. 2012;59:526–528. | ||
Cao ZX, Chen XP, Wu ZD. Changes of immune function in patients with liver cirrhosis after splenectomy combined with resection of hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int. 2003;4:562–565. | ||
Zhang XY, Li C, Wen TF, et al. Synchronous splenectomy and hepatectomy for patients with hepatocellular carcinoma and hypersplenism: a case control study. World J Gastroenterol. 2015;21:2358–2366. | ||
Athanasiou T, Al-Ruzzeh S, Kumar P, et al. Off-pump myocardial revascularization is associated with less incidence of stroke in elderly patients. Ann Thorac Surg. 2004;77:745–753. | ||
Bruix J, Hessheimer AJ, Forner A, Boix L, Vilana R, Llovet JM. New aspects of diagnosis and therapy of hepatocellular carcinoma. Oncogene. 2006;25:3848–3356. | ||
Coon WW. Splenectomy for thrombocytopenia due to secondary hypersplenism. Arch Surg. 1988;123:369–371. | ||
Sugawara Y, Yamatomo J, Shimada K, et al. Splenectomy in patients with hepatocellular carcinoma and hypersplenism. J Am Coll Surg. 2000;190:446–450. | ||
Winslow ER, Brunt LM, Drebin JA, Soper NJ, Klingensmith M. Portal vein thrombosis after splenectomy. Am J Surg. 2002;184:631–636. | ||
van’t Riet M, Burger JW, van Muiswinkel JM, Kazemier G, Schipperus MR, Bonjer HJ. Diagnosis and treatment of portal vein thrombosis following splenectomy. Br J Surg. 2000;87:1229–1233. | ||
Atweh N, Kavic SM, Dudrick SJ. Portal vein thrombosis after splenectomy. J Am Coll Surg. 2001;192:551–552. | ||
Bisharat N, Omeri OH, Lavi I, Raz R. Risk of infection and death among post-splenectomy patients. J Infect. 2001;43:182–186. | ||
Spelman D. Prevention of overwhelming sepsis in asplenic patients: could do better. Lancet. 2001;357:2072. | ||
Lacerda CM, Freire W, Vieira de Melo PS, Lacerda HR, Carvalho G. Splenectomy and ligation of the left gastric vein in schistosomiasis mansoni: the effect on esophageal variceal pressure measured by a non-invasive technique. Keio J Med. 2002;51:89–92. | ||
Aoe T, Okamoto Y, Saito T. Activated macrophages induce structural abnormalities of the T cell receptor-CD3 complex. J Exp Med. 1995;181:1881–1886. | ||
Hirooka M, Ishida K, Kisaka Y, et al. Efficacy of splenectomy for hypersplenic patients with advanced hepatocellular carcinoma. Hepatol Res. 2008;38:1172–1177. | ||
Llovet JM, Di Bisceglie AM, Bruix J, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100:698–711. | ||
Huang YH, Wu JC, Lui WY, et al. Prospective case-controlled trial of adjuvant chemotherapy after resection of hepatocellular carcinoma. World J Surg. 2000;24:551–555. | ||
Ishikawa T, Higuchi K, Kubota T, et al. Prevention of intrahepatic distant recurrence by transcatheter arterial infusion chemotherapy with platinum agents of stage I/II hepatocellular carcinoma. Cancer. 2011;117:4018–4025. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.