")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
Significant lung volume reduction with endobronchial valves in a patient despite the presence of microcollaterals masked by low-flow Chartis phenotype
Authors Yin Y , Hou G, Herth FJ , Wang X, Wang Q, Kang J
Received 4 August 2016
Accepted for publication 19 October 2016
Published 24 November 2016 Volume 2016:11(1) Pages 2913—2917
DOI https://doi.org/10.2147/COPD.S118919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Yan Yin,1 Gang Hou,1 Felix J Herth,2 Xiao-bo Wang,1 Qiu-yue Wang,1 Jian Kang1
1Department of Respiratory Medicine, The First Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of Pneumology and Critical Care Medicine, Thoraxklinik, University of Heidelberg, Heidelberg, Germany
Abstract: Satisfactory functional outcomes following bronchoscopic lung volume reduction (BLVR) using endobronchial valves (EBVs) depend on the absence of collateral ventilation (CV) between the target and adjunct lobes. The Chartis system has proven to be useful for determining whether CV is present or absent, but this system can also erroneously indicate the absence of CV, which can lead to BLVR failure. Here, we describe low-flow Chartis phenotype in the target lobe resulted in difficult judgment of existence of CV. Consequently, BLVR with EBVs implanted into the right upper bronchus failed to reduce lung volume or induce atelectasis. Inserting another EBV into the right middle bronchus blocked the latent CV, which led to significant lung volume reduction in the right upper lobe (RUL) and right middle lobe (RML) and to improve the pulmonary function, 6-min walking distance, and St George respiratory questionnaire scores over a 2-week follow-up period. Low flow in the target lobe is a unique Chartis phenotype and represents the uncertainty of CV, which is a risk factor for the failure of BLVR using EBVs. Clinicians should be aware of this possibility and might be able to resolve the problem by blocking the RUL and RML between which the CV occurs.
Keywords: COPD, bronchoscopic lung volume reduction, collateral ventilation, endobronchial valves, Chartis assessment
Introduction
Bronchoscopic lung volume reduction (BLVR) using endobronchial valves (EBVs) has been utilized in the treatment of COPD with emphysema. This technique relieves the hyperinflation status and improves lung function, exercise capacity, and quality of life.1,2 The elements of successful BLVR using EBVs include successful lobe occlusion and complete fissures.1,3–6 In addition to evaluating fissure integrity with computed tomography (CT), the Chartis system (Pulmonx Inc., Redwood City, CA, USA) can help physicians to detect collateral ventilation (CV) with high positive (71%) and negative (83%) predictive values. Therefore, this system provides satisfactory evaluation of patients requiring lung volume reduction,7,8 with the exception of some situations, such as a low-flow Chartis phenotype in the target lobe. Few studies have focused on the low-flow Chartis phenotype,9–11 and this condition has been attributed to a so-called “dynamic collapse” phenomenon. Although the occurrence of “low flow” in Chartis assessment has been documented, the effects of this phenomenon on the clinical outcomes of EBV-based BLVR remain unclear. Here, we report a case of BLVR failure caused by latent CV between the right upper lobe (RUL) and right middle lobe (RML), which was masked by a low-flow Chartis phenotype in the RUL. This patient experienced significant clinical benefit after the elimination of the latent CV via the implantation of an EBV in the RML. The patient provided written informed consent to have the case report and any accompanying images published.
Case report
A 63-year-old Chinese male with COPD was admitted to our hospital in October 2013. He was presented with a 20-year history of chronic productive cough and progressive dyspnea. The patient was an ex-smoker (40 pack-years), had suffered from secondary tuberculosis before 30 years, and had been taking salmeterol/fluticasone propionate (50/500 μg) twice daily for 2 years. Pulmonary function tests administered on admission revealed severe irreversible airflow obstruction after bronchodilator inhalation (forced expiratory volume in one second [FEV1]/forced vital capacity [FVC] =46.9%; FEV1 =0.89 L, 28.9% of predicted value) and severe hyperinflation (residual volume [RV] =5.03 L, 222% of predicted value, total lung capacity [TLC] =7.92 L, 131% of predicted value). Additional tests revealed the following: 6-min walking distance (6MWD), 144 m; St George respiratory questionnaire (SGRQ) score, 64; and Modified Medical Research Council (MMRC) dyspnea score, 4. Analysis of the blood gases at pH 7.40 revealed the following: PaO2, 65.7 mmHg and PaCO2, 42.1 mmHg.
High-resolution chest CT (HRCT) indicated heterogeneous emphysema with a marked predominance in the bilateral upper lobes and middle lobe (Figure 1A and B). The right oblique fissure was complete, and a peripheral minor defect was found on the horizontal fissure in the coronary and sagittal views; however, we calculated the integrity of horizontal fissure to be 91.6% and 91%, respectively (Figure 1C and D).
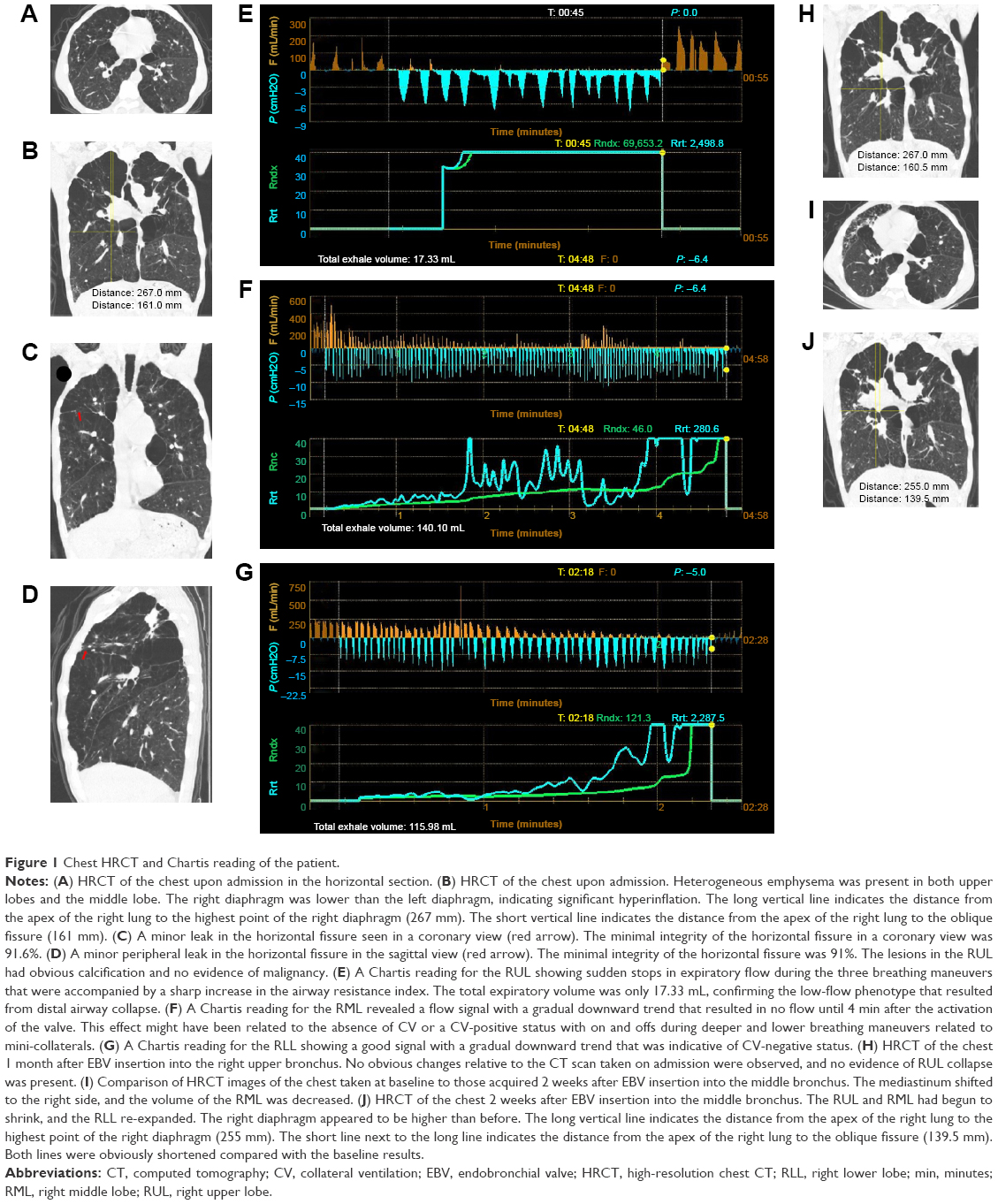 | Figure 1 Chest HRCT and Chartis reading of the patient. |
We performed a purified protein derivative test, erythrocyte sedimentation rate analysis, contrast CT, sputum smears, and cytopathology. No evidence of lung cancer or active secondary tuberculosis was present. With the patient’s informed consent for BLVR, we administered 0.5 mg atropine to minimize bronchial secretion and 50 mg pethidine to reduce the cough. We performed bronchoscopy using 20 mL lidocaine as a local anesthetic and measured the CV using the Chartis system. We blocked the right upper bronchus using a balloon catheter and measured the expiratory airflow. This assessment revealed sudden stops in expiratory flow during the three breathing maneuvers that were accompanied by sharp increases in resistance, which is a common characteristic of the low-flow phenotype (Figure 1E). It was difficult to confirm whether CV was present; therefore, we measured CV in the ipsilateral lobes. Assessment of the middle lobe revealed that CV was negative or CV was positive with on/offs in expiratory flow that occurred during deeper and lower breathing maneuvers, which were signs of mini-collaterals that were open only during deeper inspirations (Figure 1F). Assessment of the right lower lobe (RLL) revealed a good signal with a gradual downward trend without CV (Figure 1G). We implanted three EBVs (Zephyr EBV 4.0; Pulmonx) in the right upper bronchus for economic reasons.
One month later, the patient exhibited limited improvements in lung function, 6MWD, and volume reduction of the RUL on HRCT (Figure 1H). We speculated that this lack of improvement might have been associated with latent CV between the RUL and RML that caused a minor leak in the horizontal fissure. Therefore, we decided to block the right middle bronchus using another EBV (Zephyr EBV 5.5).
Two weeks later, quantitative analysis of the HRCT images (Lung CAD1.2; Neusoft, Shenyang, People’s Republic of China) revealed that the volume of the right lung had decreased from 3,838 to 2,935 mL, the RUL and RML had begun to shrink, the right diaphragm had become elevated, and the mediastinum had shifted to the right side (Figure 1I and J). The patient exhibited significant clinical improvement. The FEV1 increased to 1.52 L (+0.63 L) and the 6MWD increased to 216 m (+72 m); in addition, the RV decreased to 4.21 L (−16.3%), the TLC decreased to 7.10 L (−10.4%), the SGRQ score decreased to 41, and the MMRC dyspnea score decreased to 2.
The patient reported slight chest pain after the second EBV implantation, and HRCT revealed some pleural effusion, which was localized to the minor fissure and absorbed spontaneously.
Discussion
The absence of CV is a strong predictor of successful BLVR.1–3 The Chartis system has been proven to be useful for detecting CV and predicting the success of BLVR, but how to analyze and judge the Chartis reading should be paid more attention. It is difficult in some conditions because different breathing efforts and/or variable levels of conscious sedation may lead to the variable amplitude of the Chartis reading.3,4,8,9,12 However, some patients exhibit poor clinical responses even when the Chartis analysis has detected no CV, and the EBV has completely blocked the target bronchus. Treatment failure in these patients is ultimately determined to have resulted from latent CV that was undetected by the Chartis system. Such false negative readings result from several causes, including catheter blockage and low flow in the target lobe.8,13 Low flow is a unique Chartis phenotype and can be classified as either CV positive or CV negative. Low flow is likely a sign of dynamic collapse of the airways distal to the balloon of Chartis catheter. Other possible causes of low flow include extra-wide collateral channels between the lobes that induce a reverse flow in the catheter that cannot be displayed on the monitor. The Chartis catheter itself may also be responsible for the inherent resistance in these particular assessments. When low flow exists in Chartis reading of target lobe, ipsilateral lobes should be carefully assessed. Previous study revealed that low-flow patients with ipsilateral CV-negative lobe also showed an improvement in pulmonary function and target lobe volume reduction (TLVR) after valve insertion.11 But the relationship should be focused between the varying levels of volume reduction and the clinical outcomes. Patients in whom TLVR was obtained had greater improvements in clinical outcomes, even in the patients with incomplete fissures who had a TLVR >50%.14
In our case, the low-flow Chartis phenotype led us to fail to recognize latent CV between the RUL and RML. These findings may be attributable to the existence of mini-collaterals that open only during deeper inspirations. In addition, the minor defect in the fissure should be considered as one of the risk factors of treatment failure, even when its integrity was more than 90% on HRCT. Although the accuracy of Chartis assessment or HRCT fissure analysis for the prediction of TLVR <80%, evaluations of figure integrity using HRCT and the Chartis system are complementary.15 Moreover, our case revealed that Chartis assessment in combination with HRCT fissure analysis also has difficulties in assessing CV when the low-flow Chartis phenotype exists. Pu et al found that defects in the right horizontal fissure make the RUL a poor target for valves.16 Our case showed that patients with low-flow Chartis phenotype in the RUL that masks CV positivity can still benefit from BLVR if an EBV is used to block the middle bronchus and eliminate the CV. If CV is found between the RUL and RLL, BLVR with a thermal vapor or coil may be an effective alternative.17,18
Last but not the least, caution should be in place not only in patient selection but also in the follow-up of treatment, when the potentially malignant lesions in the target lobe. Just like the lesions located in the RUL of our case, lung cancer should be excluded carefully because lung cancer is one of the common comorbidities of COPD.
Conclusion
In conclusion, low flow in the target lobe can lead to incorrect evaluations of CV in patients who are scheduled for EBV-based BLVR, especially when the CV of ipsilateral lobes is difficult to judge. Such incorrect evaluations can lead to unsatisfactory clinical outcomes of BLVR. Our experience suggests that at least some low-flow patients with micro-CV between the RUL and RML can benefit from implantation of EBVs into the upper and middle bronchi.
Acknowledgments
This research was supported by project grant 2014225006 from Department of Science and Technology of Liaoning Province, People’s Republic of China and project grant LNCCC-D03-2015 from Youth Fund of Health and Family Planning Commission of Liaoning Province, People’s Republic of China.
Author contributions
GH performed patient selection, bronchoscopic lung volume reduction, and wrote the manuscript. YY and X-bW helped to follow-up the patient and to collect data and write the manuscript. Q-yW helped with patient selection and writing the manuscript. FJH and JK contributed to the analyses and interpreting the data, writing the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. | ||
Liu H, Xu M, Xie Y, Gao J, Ni S. Efficacy and safety of endobronchial valves for advanced emphysema: a meta analysis. J Thorac Dis. 2015;7(3):320–328. | ||
Herth FJ, Noppen M, Valipour A, et al. Efficacy predictors of lung volume reduction with Zephyr valves in a European cohort. Eur Respir J. 2012;39(6):1334–1342. | ||
Klooster K, ten Hacken NH, Hartman JE, Kerstjens HA, van Rikxoort EM, Slebos DJ. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. | ||
Iftikhar IH, McGuire FR, Musani AI. Predictors of efficacy for endobronchial valves in bronchoscopic lung volume reduction: a meta-analysis. Chron Respir Dis. 2014;11(4):237–245. | ||
Tian Q, An Y, Xiao BB, Chen LA. Treatment of giant emphysamous bulla with endobronchial valves in patients with chronic obstructive pulmonary disease: a case series. J Thorac Dis. 2014;6(12):1674–1680. | ||
Mantri S, Macaraeg C, Shetty S, et al. Technical advances: measurement of collateral flow in the lung with a dedicated endobronchial catheter system. J Bronchology Interv Pulmonol. 2009;16(2):141–144. | ||
Herth FJ, Eberhardt R, Gompelmann D, et al. Radiological and clinical outcomes of using Chartis to plan endobronchial valve treatment. Eur Respir J. 2013;41(2):302–308. | ||
Gesierich W, Samitas K, Behr J. Determining collateral ventilation during bronchoscopy: unanswered questions. Thorax. 2014;69(3):289–290. | ||
Shah PL, Herth FJ. Dynamic expiratory airway collapse and evaluation of collateral ventilation with Chartis. Thorax. 2014;69(3):290–291. | ||
Herzog D, Thomsen C, Poellinger A, et al. Outcomes of endobronchial valve treatment based on the precise criteria of an endobronchial catheter for detection of collateral ventilation under spontaneous breathing. Respiration. 2016;91(1):69–78. | ||
Tian Q, An Y, Xiao BB, Chen LA. Endobronchial valve to treat large bulla at right middle lobe in chronic obstructive pulmonary disease patients. J Thorac Dis. 2015;7(9):E374–E377. | ||
Gompelmann D, Eberhardt R, Ernst A, et al. The localized inflammatory response to bronchoscopic thermal vapor ablation. Respiration. 2013;86(4):324–331. | ||
Valipour A, Herth FJ, Burghuber OC, et al. Target lobe volume reduction and COPD outcome measures after endobronchial valve therapy. Eur Respir J. 2014;43(2):387–396. | ||
Gompelmann D, Eberhardt R, Slebos DJ, et al. Diagnostic performance comparison of the Chartis System and high-resolution computerized tomography fissure analysis for planning endoscopic lung volume reduction. Respirology. 2014;19(4):524–530. | ||
Pu J, Wang Z, Gu S, et al. Pulmonary fissure integrity and collateral ventilation in COPD patients. PLoS One. 2014;9(5):e96631. | ||
Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med. 2016;4(3):185–193. | ||
Kontogianni K, Gerovasili V, Gompelmann D, et al. Effectiveness of endobronchial coil treatment for lung volume reduction in patients with severe heterogeneous emphysema and bilateral incomplete fissures: a 6-month follow-up. Respiration. 2014;88(1):52–60. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.