")
Back to Journals » Clinical Interventions in Aging » Volume 14
Significance of advance care planning in nursing homes: views from patients with cognitive impairment, their next of kin, health personnel, and managers
Authors Sævareid TJL , Førde R, Thoresen L, Lillemoen L , Pedersen R
Received 29 January 2019
Accepted for publication 18 April 2019
Published 29 May 2019 Volume 2019:14 Pages 997—1005
DOI https://doi.org/10.2147/CIA.S203298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Trygve Johannes Lereim Sævareid,1 Reidun Førde,1 Lisbeth Thoresen,1,2 Lillian Lillemoen,1 Reidar Pedersen1
1Centre for Medical Ethics, University of Oslo, Oslo, Norway; 2Department of Health Sciences, University of Oslo, Oslo, Norway
Purpose: Advance care planning (ACP) performed by regular staff, which also includes patients with cognitive impairment and their next of kin, is scarcely studied. Thus, we planned an implementation study including key stakeholders (patients, next of kin, and health care personnel) using a whole-ward/system approach to ACP. We explored how they experienced ACP and its significance.
Patients and methods: This qualitative study is part of a mixed-method implementation study of ACP. In four nursing homes, we did qualitative interviews and audio-recordings of meetings. We completed 20 individual semistructured interviews with participants soon after ACP conversations. The interviews included patients with cognitive impairment, their next of kin, and health care personnel. We also conducted four focus group interviews with staff and managers in the nursing homes and audio-recorded four network meetings with the project teams implementing ACP.
Results: All participants appreciated taking part in ACP. Patients and next of kin focused more on the past and present than future treatment preferences. Still, ACP seemed to contribute to a stronger patient focus on end-of-life conversations. More generally, ACP seemed to contribute to valuable information for future decision-making, trusting relations, improved end-of-life communication, and saving time and resources.
Conclusion: Safeguarding a strong patient focus on ACP and fostering a person-centered care culture in nursing home wards seem to be achievable through implementation of ACP that includes regular staff, patients with cognitive impairment, and their next of kin.
Keywords: qualitative, person-centered care, whole-system approach, implementation, cognitive impairment
Introduction
Advance care planning (ACP) is a communicative process that supports individuals in understanding and sharing their personal values, life goals, and preferences regarding future medical treatment and care.1,2 Possible outcomes of ACP are increased completion of advance directives,3,4 occurrence of conversations,4 improving communication skills,5 concordance between treatment given and patient’s wishes,4,6 improved documentation of conversations and patient’s preferences,6,7 improved knowledge of patient’s preferences,8 cost-effectiveness,9,10 and hospitalization effects.3,11,12 Many outcome studies have been performed in nursing homes.7,9,12–14 However, there are few studies from nursing homes assessing the significance of ACP that is performed by regular staff and includes patients with cognitive impairment and their next of kin.7
National guidelines in Norway strongly recommend that severely ill patients are given opportunities to express their values and preferences through ACP.15 However, we know that ACP in nursing homes, which is the place of death for half the Norwegian population,16 is scarce.17 In addition, health care personnel report a lack of routines for ACP in nursing homes18 and are in need of more competence in discussing death and dying.19
In order to provide the health services with a knowledge-based approach to ACP, to give patients a better opportunity to express their values and preferences, and to give health care personnel competence and routines in doing ACP, we planned an ACP implementation study that introduced an educational program for nursing homes.20 We had a “whole-ward” or “whole-system” approach,21,22 which meant:
- Regular staff at the ward performed ACP since we wanted the staff involved in ACP as much as possible and considered this more sustainable than external facilitators,
- Managers should endorse the project and participate in the local project team,
- We encouraged participation also of patients with cognitive impairment,
- We encouraged the next of kin to participate together with the patient or alone when the patient could not participate,
- Using a sustainable train-the-trainer model with limited out-of-site training time and a freely available ACP-guide (see below),
- ACP is viewed as a process consisting of more than one conversation and that ACP may be supplemented by more informal conversations or “windows of opportunities” – ie, spontaneous conversations on matters of importance to the patient – for example, existential aspects or end-of-life issues typically discussed between health care personnel and patient during daily activities and initiated by the patient,23 and
- ACP should be voluntary.
By ACP being voluntary, we mean that the patient greatly influences what and how much is discussed. Furthermore, ACP should not be dominated by health care personnel’s agenda. Rather, the patient, including those with cognitive impairment, should be given excessive opportunity to contribute with their perspectives. We find this whole-ward approach to be in line with person-centered care. Person-centered care includes relationships in enhancing respect for patient autonomy. A person’s autonomy, according to person-centered care, relies more on his or her relational and social context than what is proposed in individualist- and cognitive-based approaches to autonomy.24 Furthermore, next of kin, through so-called supported decision-making,25,26 may assist in increasing the autonomy of a person with cognitive impairment. Decision-making processes in person-centered care are characterized by a dynamic dialog between the patient, their next of kin, and health care personnel.27
We evaluated the intervention through both quantitative and qualitative research, including this study, observation of the conversations, and using pair-matched cluster-randomized trial design. The intervention was the implementation of ACP. Implementation support included training (2-day seminar) and supervision of health care personnel and establishing local project teams (preferably nurse, ward manager, and physician) at the nursing home wards. Furthermore, together with the project teams, we developed an ACP guide28 and a documentation template. For more information about implementation support, the background of the study, and design, we refer to our protocol article.20
The focus of ACP has broadened from eliciting future treatment preferences to include the patient’s existential, psychosocial, and spiritual needs.1,29 One reason for this is that seriously ill patients may find enhancing relationships and improving communication more important and less intrusive than completing advance directives or living wills.30 Furthermore, family members may value general end-of-life conversations more than writing down more formal and specified directives.31 Nursing home patients are generally positive to ACP,32 but some patients may experience unpleasant feelings when confronted with end-of-life issues or detailed questions, eg, about resuscitation or not.33 On the other hand, addressing difficult issues without “going too far” can make the patients feel comfortable and respected, enabling them to be open about their wishes and thoughts.33 Consequently, the ACP in this implementation study emphasized quality of life and existential aspects as central, in addition to end-of-life care preferences.
This article has the following research questions: 1) what are the experiences of patients, next of kin, and health care personnel who participated in ACP and 2) what is the significance of ACP for patients, next of kin, health care personnel, and nursing home managers?
Material and methods
Data consisted of transcripts of semistructured individual interviews, focus group interview, as well as recordings from network meetings. Four wards from the four nursing homes in the intervention group participated in this study.
The individual interviews included patients, next of kin, and health care personnel who had participated in ACP, see Table 1. All individual interviews took place shortly after the ACP, except for one patient and one health care personnel whom we interviewed 2 days after ACP. One patient requested that her niece be present during the interview. All patients and their next of kin met the researcher for the first time on the day of these interviews. Some of the health care professionals participating in these interviews were also local project team members, and knew the researchers, while the rest of participating health care personnel did not know the researchers.
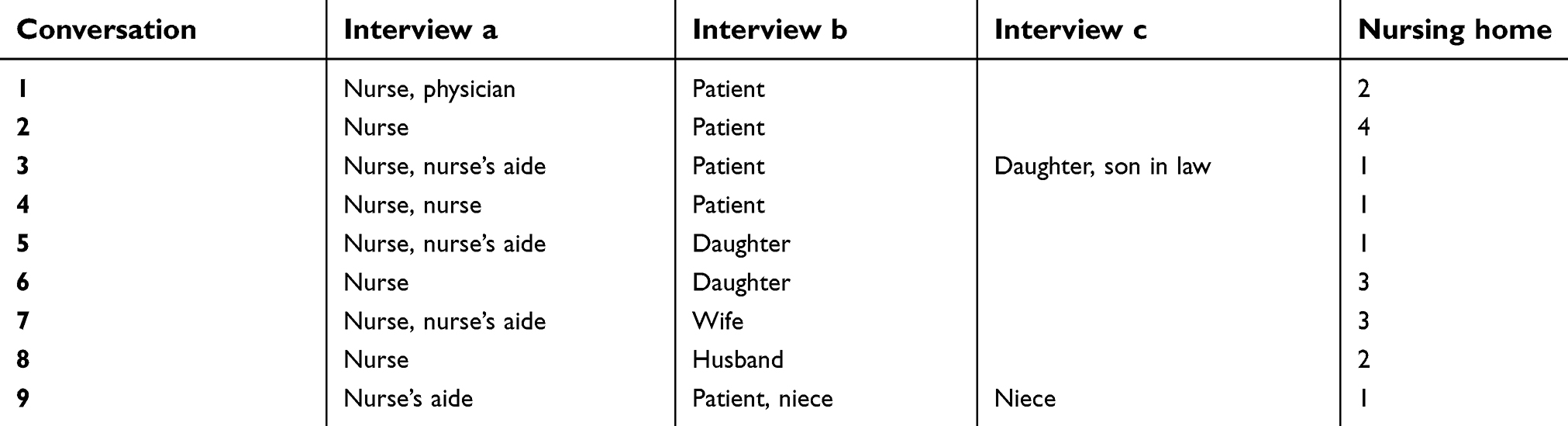 | Table 1 Semistructured interview participants |
In order to get more and broader information about the experience and significance of ACP, we also collected data from focus group interviews with health care personnel at the wards and network meetings with the project teams. Project team members had established a relationship with the researchers, while the rest of participating health care personnel did not know the researchers.
Recruitment of participants and data gathering
Participants were invited to take part in the study through purposive sampling. We did no repeat interviews and data saturation was not a topic during the data-gathering period. All interviews and network meetings with project teams were audio-recorded and transcribed verbatim. Transcripts were not sent to participants for comments or corrections.
Individual interviews
The project teams at the nursing home wards first invited patients and next of kin to participate in ACP. The invitation followed a template in the ACP guide.28 The project teams assessed whether patients could participate in ACP or not. They did so based on implementation support encouraging participation of patients also with cognitive impairment. Project teams then gave oral and written invitations to patients, next of kin, and health care personnel regarding being observed by the first author during the ACP and interviewed by him afterward. Interviews followed an interview guide prepared by the authors together with Elisabeth Gjerberg and lasted between 22 and 75 mins. The first author, who conducted the interviews, wrote field notes after the interviews. He is a registered nurse specialized in geriatric care, with an interest in ethics at end of life and had previous experience doing individual interviews as part of his Master of Social Science education.
Focus-group interviews
Project teams invited health care personnel who had participated in at least one ACP to a focus-group interview at their nursing home. All participants in these interviews were nurses or nurse’s aides. One interview had two participants, while the other three had four participants each. Experienced senior researchers from the Centre for Medical Ethics at the University of Oslo carried out the four interviews – LL and LT carried out three, while LL and RP did one.
Meetings with project teams
The local project teams from the four nursing homes got together at the Centre for Medical Ethics for network meetings three times during and one time after the intervention period. All nursing homes were represented in the meetings, but who participated varied. Nurses (coordinators) participated most often, some ward/nursing home managers, and one physician once.
Data analysis
We based our analysis of data on thematic analysis.34,35 Thematic analysis is a systematic approach for identifying and analyzing patterns – themes – across a dataset.35 All authors read interview transcripts in order to familiarize themselves with the data and individually selected interesting features of the data. We then met and agreed on research questions and main themes. TJLS and RF presented a text with relevant data based on the research questions and main themes to the other authors. The authors individually searched for other possible themes in the data. We further developed the main themes in drafts of the manuscript by rechecking with the data. The authors then met to agree on the themes. The themes were also slightly refined through the drafting of the manuscript.
Research ethics
Norwegian Centre for Research Data (NSD – reference number 41114), the Data Protection Official for Research, approved the study March 4, 2015. The review performed by NSD covers all main ethical issues for this kind of research, eg, related to informed consent and privacy. NSD granted permission September 22, 2015, for audio-recordings and observing conversations.
All interviewed participants received a written invitation to participate before the interview, which included information about the project and some of its goals, anonymization, and voluntary participation. Prior to the interview, they signed an informed consent form.
We also asked for consent to audio-record the meetings with the project teams.
Results
Transcription of the 20 individual interviews resulted in 318 pages of text, focus-group interviews: 123 pages, and meetings with project teams: 160 pages. All patients interviewed had some level of cognitive impairment.
Our individual interviews indicated that end-of-life decisions were not the focus in ACP for these participants. Matters of the present and the past occupied all patients and many of the next of kin. The patients, their next of kin, and the health care personnel valued the ACP. The focus on the patient in our approach was important for the patient, for the next of kin, and for the relationship between these and the health care personnel. In addition, information such as getting to know the patient as a person and their general attitudes toward life, death, or decision-making process was revealed which sometimes gave more general, but still important input to future end-of-life decisions or help next of kin to meet the death of their loved ones. Our focus-group interviews and the project team meetings confirmed these findings.
ACP – a valued experience
The patients, next of kin, as well as the health care personnel described the conversations in positive terms. “I experienced it as very good. I really did. It was good to have the opportunity to express things in words” [4b]. The same patient felt that bringing end of life into the conversation was natural … after all I live in a nursing home”.
All next of kin expressed that they appreciated the conversation, for example, one interviewee said:
this is a subject which as I see it is a little taboo, and I think it is very important, I think very many people are thinking about it, both next of kin and the patient, just elucidating it, … and talk about it, in my opinion it results in lowering your guard. [3c]
Nevertheless, it could be demanding for the next of kin “ … it is not so easy for me to talk about these things. It is easier when we sit in a group” [5b]. Some said spontaneously that such conversations should be part of the nursing home routines. They emphasized that it was important that the initiative should come from the institution, not them as a family member because “I would not have asked for such a conversation if I was not invited” [6b].
All health care personnel described the ACP as pleasant with a relaxed atmosphere, despite one nurses’ aide feeling stressed about limited time. The active patient participation in the ACP, as well as learning more of the patient’s history, further contributed to experiencing the ACP participation as positive. Most participants felt well-prepared for the conversation and sufficiently informed about what to expect. However, due to cognitive impairment, some of the patients had difficulties in retrospect to explain how they were informed about the aim and content of the ACP.
The significance of ACP
For a stronger patient focus
The patients praised the way they were treated in the nursing home. The ACP gave them an opportunity to address things of importance to them, which were otherwise difficult to communicate due to personnel’s lack of time “... it means very much to have an opportunity to share the thoughts I am preoccupied with” [4b].
The next of kin stressed that it was important for them that the conversation was on the patient’s premises, that it was individualized and adapted to what the patient wanted to talk about, and that the patient was the focus of the conversation.
The patient focus in ACP was valued also by health care personnel “it puts the patient very much in focus” [2a]. Health care personnel perceived this approach to ACP strengthened their respect for the patient and the patient’s integrity “we empower the patient” [2a]. One nurse claimed she individualized her approach to patients more generally in her work, in line with another who said “For me, the most important thing was to get to know the patient in a different way … And perhaps from the daughter’s information, get a more complete picture” [6a]. A nurse’s aide said
I for my part think that the patient should feel that he is seen. That one can obtain more insight into who the patient is and what he wishes us to do in an acute event. Also, that the patient should feel that he is taken care of and that he should feel seen and heard about thoughts that he may not share with many others. It is not good to be alone with these kinds of thoughts. [9a]
For building trusting relations
One ward manager said that ACP, through sharing what is of importance to the patients, made patients feel safer. The next of kin claimed that their relationship with the health care personnel strengthened because they had shared something personal. One next of kin said her family member had been a patient in the institution for 6 months but it was not until the ACP that she felt that the personnel acknowledged her.
Next of kin received the opportunity to share what they knew about the patient’s life, values, and interests. This felt meaningful since they could contribute with key information about the patient as a person, and thus influence their stay.
I feel safe because they are interested in knowing my mother better, kind of learning about her situation, how it was before and how things are now, and at the same time to inform me… The most important part of the conversation is to know that my mother is in safe hands and this is comforting me. [6b]
ACP strengthened the next of kin’s feeling of being seen and heard and acknowledged as an important person for the patient. Some of them had talked about their relationship to the patient and through this, the health care personnel who knew the patient confirmed next of kin’s important role in the patient’s life. Familiarity with the staff who participated in ACP and that would continue to take care of the patient was important to next of kin and the patient.
In addition, ACP could increase trust and improve the cooperation between next of kin and the institution, according to health care personnel “and through this (ACP) make it easier for patient and next of kin to relate to the institution” [nurse 5a].
For discussing end-of-life care
None of the patients said that it was important for them to decide about life-prolonging treatment. However, talking about their own future death was not difficult. Several patients expressed a trust in health care personnel making end-of-life decisions according to their best interests. One patient said she felt safe in their care and trusted their decisions “one hundred percent” [4b]. “That day will come. It is a good thing that we know nothing”, another patient said [1b]. One patient admitted that she was thinking a lot about what will happen before she dies “But then I figure, I will probably get the help I need … Yes, I will be ok, I think, because many people have gone before me” [3b]. She did not recall that future medical decisions were touched upon in the conversation. Life was good, a patient said “it (end of life) comes when it comes, for sure, but when I can live the life as I do today, I am very pleased” [4b]. Another patient said explicitly that she thought it was a good thing not to know what would happen and that she put her fate in God’s hands. A few patients nevertheless gave unexpectedly clear responses to questions of life-prolonging treatment (nurse, focus group Nh1). Health care personnel did not regard any preferences for future treatment expressed by patients as final decisions since “Things happen that we cannot control or change” [8a], necessitating possible reconsiderations in the future.
Most of the interviewees stressed that such conversations should not be a onetime event, and follow-ups are necessary. ACP as a process is probably crucial because “some next of kin find it hard to say something there and then” [nurse, focus group Nh 2]. “However, when this structured conversation has taken place, I think that it is easier to keep that door open … one can refer to that conversation; bring up the themes once more” [nurse 5a].
Some next of kin confirmed the patients’ descriptions that they were not afraid of death and dying. “She is not afraid, what will happen happens” [9c]. Talking about end of life could also give the next of kin new information about the patient “at the same time I got some information about how they look at him as a patient, how he had developed” [7b].
Most next of kin believed patients wanted the doctors to decide future medical treatment, trusted the professionals, and agreed to this. A few stated that they knew about their loved one’s will because they had talked about end of life when a relative had died.
Talking about end of life prepared next of kin for what they knew will come. Broaching the subjects of the ACP conversations more generally would make it easier to discuss them in more detail later, if needed.
Some of the next of kin thought health personnel should not insist on discussing particular topics during ACP. One spouse informed that he had had two conversations about end-of-life aspects before this ACP implementation project. However, these conversations were “rather short, about end of life treatment … it [was] obvious what the doctor’s aim was … to have something to show, in situations at end of life” [8b].
At the same time, the health care personnel emphasized that there was a risk avoiding difficult topics – which the patient wanted to talk about at least on a general level - altogether. Frequently, “we hide the upcoming death” [through comments like] “you may live until you are hundred” [nurse 3a].
ACP made it possible to tailor the end-of-life communication to the needs of the individual patient and their next of kin “one really important thing to know when one is living here, [is] whether you are afraid of it [death] or whether next of kin are afraid of it, whether they need more information, less information” [nurse 3a]. Through ACP and learning more of the others’ needs, health care personnel adapted both the care and information given both to the patient and to next of kin.
For the nursing homes
ACP had started up something important, stated health care personnel, as a preparation for later ACP with the same patient and the next of kin. Moreover, they described a more general change in the ward culture and attitudes, ie, focusing more on the patient in interactions with patient and next of kin.
Furthermore, the staff and managers stated that getting to know the patient better may save time and resources in future difficult end-of-life decisions, for example, avoiding conflicts, complaints, or overtreatment.
ACP – together with the implementation support to the whole wards – had also influenced the awareness and attitudes among health care personnel to life and death issues. Some had done similar conversation also before this ACP project; however, now they carried them out differently and related to the patient in new ways, both in ACP and more generally. For example, now health care personnel will more often enter into informal conversations about existential and end-of-life topics initiated by the patient – windows of opportunities – rather than avoiding them.
The implementation of ACP also led to a more methodical approach to end-of-life care conversations, for example, a greater recognition of the importance of documenting ACP, as well as windows of opportunities. Physicians with limited knowledge of the patients and that had not themselves participated in the ACP had positively commented on the documentation, a nurse said in a focus group interview. Another physician, who probably would not have participated in such a conversation with the patient if not for ACP, emphasized the value of involving next of kin in ACP to get to know the patient better. However, for some of the patients, these conversations about life and death decisions came too late “when the patient moves in here, they are often in a bad shape both physically and psychologically, making it difficult to talk” [nurse and nurse’s aide 7a].
Discussion
The participants in this ACP-implementation study in nursing homes experienced ACP – with a whole-ward approach (eg, performed by regular staff, including patients with cognitive impairment and their next of kin) – as positive and worthwhile. ACP performed in this way, and adapted to the individual patient, seems to lead to a better and stronger patient focus both in the ACP conversation and more generally in the nursing homes. In line with others, we found ACP did not often lead to concrete and specific guidance for future decisions concerning life-prolonging treatment,36,37 and future treatment decisions were not the main focus in the ACP.7,38 Nevertheless, health care personnel reported that they, to a greater extent, saw the value of accessible documentation of ACP, in particular of specific future treatment preferences. Deciding about future life-prolonging treatment did not seem important to the patients participating in this study. Other studies have similar results. One review indicated people with dementia may be reluctant to think about their deaths and future end-of-life preferences.39 Elderly persons with early-stage Alzheimer’s disease did not reflect on future care,40 and elderly persons with dementia were not always able or wanted to discuss future care.41 Finally, most nursing home patients in a study of experiences with ACP expressed a desire not to think about the future and instead preferred to “live for the day”.42 Future not being important to patients in this study may partly be a consequence of their cognitive impairment;40,43 however it could relate to patients trusting health care professionals in making the right decisions for them, a finding also found by others.44 A main reported result of ACP was better and more trustful relationships between the patient, the next of kin, and the staff,45 thus making it easier to make difficult decisions together at a later time and may save time and resources. Furthermore, talking about past and present, and more generally about hopes, worries, and preferences for the future, may provide relevant information for future decisions on life-prolonging treatment. These findings are in line with the ideals of person-centered care – respecting the patient autonomy in a social and relational context.
The health care personnel stressed viewing ACP as a process that opened up doors, sensitized patients and next of kin to the topic, and made it easier to talk about end-of-life issues. Patients or their next of kin did not consider talking about death and dying scary or intrusive. Both patients and their next of kin wanted health care personnel to initiate ACP43,44,46 and preferred knowing the ACP facilitator.22 At the same time, more formal ACP seems to have the potential to promote windows of opportunities and more informal end-of-life communication initiated by the patient.
What constitutes good ACP is still debated, eg, the need to clarify specific treatment preferences before it is too late. Our approach to ACP acknowledged both patient’s existential needs and the possibility to elicit future life-prolonging treatment preferences. In addition, we had a whole-ward approach.21,22 Furthermore, we emphasized ACP to have a patient focus. Focusing on the patients in ACP may seem superfluous. However, our previously published observations of ACP and other end-of-life conversations indicate that this may not be as self-evident as it seems,36,47 ie, the ACP may easily be dominated too much by the professionals. In this study, we found indications that next of kin involvement in ACP is valuable, in particular to patients with cognitive impairment, at least as long as the patient remains the focus of the ACP. A sub-study of this study concluded similarly “if the aim of ACP is to get to know important issues and values to frail elderly patients, family members may play a very important role”.48 This finding indicates our approach to ACP may support more person-centered care. Health care personnel nevertheless noted that at admission to nursing homes, some patients are unable to participate in ACP. Thus, initiation of ACP at an earlier stage may be the best timing.49
We have also observed the ACP in which the participants in the individual interviews took part. Results from the observations also indicate that health care personnel had a strong patient focus during the ACP (even when only the next of kin participated), patients focused more on past and present than future, and next of kin as valuable in supporting the patient. The main results reported above are also supported by another sub-study of this mixed-method implementation study.
Limitations
This study interviewed mainly nurses and nurse’s aides and only one physician. Experiences from physicians and other relevant health care personnel in doing ACP would have enriched our data. In general, qualitative findings cannot be generalized beyond participants and contexts we studied. However, the main findings are supported by the other sub-studies from this project using other methodological approaches. It could be argued that particularly our finding of building more trusting relationships, but also a stronger patients focus, may be a result of simply taking more time to talk to patients and their next of kin. Future studies could randomize between ACP and unstructured friendly conversations to assess the specific effects of ACP.
Conclusion
Safeguarding a strong patient focus in ACP and fostering a patient-focused culture in nursing home wards seem to be achievable through a whole-ward approach to ACP implementation. In this approach, patients with cognitive impairment and next of kin are encouraged to participate in ACP performed by regular staff. ACP implemented in this way is experienced as positive and worthwhile for all stakeholders and may contribute to person-centered care, both in ACP and more generally at the ward. In addition, it may build trusting relationships and better end-of-life communication and may save time and resources.
The patients and next of kin focused more on the past and present, and more general hopes, worries, and preferences than specific future life-prolonging treatment. However, ACP can still give valuable information for future treatment decisions and facilitate future communication and shared decision-making.
Acknowledgments
Many thanks to Elisabeth Gjerberg, researcher in the research group, who contributed to the conception of the study. We acknowledge the valuable work of Kristin Weaver (research support), Anders Tvedt (transcription), Helene Alice Vestad Nortvedt (transcription), and Kristi Barcus (copyediting) in this study.
Disclosure
Prof. Dr. Reidar Pedersen reports grants from The Norwegian Research Council, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Rietjens JAC, Sudore RL, Connolly M, et al. Definition and recommendations for advance care planning: an international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017;18(9):e543–e551. doi:10.1016/S1470-2045(17)30582-X
2. Sudore RL, Lum HD, You JJ, et al. Defining advance care planning for adults: a consensus definition from a multidisciplinary delphi panel. J Pain Symptom Manage. 2017;53(5):821–832. doi:10.1016/j.jpainsymman.2016.12.331
3. Brinkman-Stoppelenburg A, Rietjens JA, van der Heide A. The effects of advance care planning on end-of-life care: a systematic review. Palliat Med. 2014;28(8):1000–1025. doi:10.1177/0269216314526272
4. Houben CH, Spruit MA, Groenen MT, Wouters EF, Janssen DJ. Efficacy of advance care planning: a systematic review and meta-analysis. J Am Med Dir Assoc. 2014;15(7):477–489. doi:10.1016/j.jamda.2014.01.008
5. Lund S, Richardson A, May C. Barriers to advance care planning at the end of life: an explanatory systematic review of implementation studies. PLoS One. 2015;10:2. doi:10.1371/journal.pone.0116629
6. Weathers E, O’caoimh R, Cornally N, et al. Advance care planning: a systematic review of randomised controlled trials conducted with older adults. Maturitas. 2016;91:101–109. doi:10.1016/j.maturitas.2016.06.016
7. Flo E, Husebo BS, Bruusgaard P, et al. A review of the implementation and research strategies of advance care planning in nursing homes. BMC Geriatr. 2016;16:24.
8. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. Br Med J. 2010;340:c1345. doi:10.1136/bmj.c1345
9. Dixon J, Karagiannidou M, Knapp M. The effectiveness of advance care planning in improving end-of-life outcomes for people with dementia and their carers: a systematic review and critical discussion. J Pain Symptom Manage. 2018;55(1):132–150. doi:10.1016/j.jpainsymman.2017.04.009
10. Klingler C, in der Schmitten J, Marckmann G. Does facilitated advance care planning reduce the costs of care near the end of life? Systematic review and ethical considerations. Palliat Med. 2016;30(5):423–433. doi:10.1177/0269216315601346
11. Brazil K, Carter G, Cardwell C, et al. Effectiveness of advance care planning with family carers in dementia nursing homes: a paired cluster randomized controlled trial. Palliat Med. 2018;32(3):603–612. doi:10.1177/0269216317722413
12. Martin RS, Hayes B, Gregorevic K, Lim WK. The effects of advance care planning interventions on nursing home residents: a systematic review. J Am Med Dir Assoc. 2016;17(4):284–293.
13. Séchaud L, Goulet C, Morin D, Mazzocato C. Advance care planning for institutionalised older people: an integrative review of the literature. Int J Older People Nurs. 2014;9(2):159–168. doi:10.1111/opn.12033
14. Sharp T, Moran E, Kuhn I, Barclay S. Do the elderly have a voice? Advance care planning discussions with frail and older individuals: a systematic literature review and narrative synthesis. Br J Gen Pract. 2013;63(615):e657–e668. doi:10.3399/bjgp13X673667
15.
16. Dødsårsaksregisteret. D3a: dødsfall etter dødssted og bofylke − Antall dødsfall. Folkehelseinstituttet. Available from:
17. Gjerberg E, Lillemoen L, Weaver K, Pedersen R, Forde R. Advance care planning in Norwegian nursing homes. Tidsskrift for den Norske laegeforening. 2017;137(6):447–450. doi:10.4045/tidsskr.16.0284
18. Fosse A, Zuidema S, Boersma F, Malterud K, Schaufel MA, Ruths S. Nursing home physicians’ assessments of barriers and strategies for end-of-life care in Norway and The Netherlands. J Am Med Dir Assoc. 2017;18(8):713–718. doi:10.1016/j.jamda.2017.03.005
19. Gjerberg E, Førde R, Bjørndal A. Staff and family relationships in end-of-life nursing home care. Nurs Ethics. 2011;18(1):42. doi:10.1177/0969733010386160
20. Sævareid TJL, Lillemoen L, Thoresen L, Førde R, Gjerberg E, Pedersen R. Implementing advance care planning in nursing homes – study protocol of a cluster-randomized clinical trial. BMC Geriatr. 2018;18(1):180. doi:10.1186/s12877-018-0869-1
21. Gilissen J, Pivodic L, Gastmans C, et al. How to achieve the desired outcomes of advance care planning in nursing homes: a theory of change. (Report). BMC Geriatr. 2018;18:1. doi:10.1186/s12877-018-0723-5
22. Gilissen J, Pivodic L, Smets T, et al. Preconditions for successful advance care planning in nursing homes: a systematic review. Int J Nurs Stud. 2017;66:47–59. doi:10.1016/j.ijnurstu.2016.12.003
23. Seymour J, Almack K, Kennedy S. Implementing advance care planning: a qualitative study of community nurses’ views and experiences. BMC Palliat Care. 2010;9:4. doi:10.1186/1472-684X-9-4
24. O’Connor D, Purves B, Downs M. Decision-making and Dementia: toward a social model of understanding. In: O’Connor D, Purves B, editors. Decision-Making, Personhood and Dementia: Exploring the Interface. London: Jessica Kingsley Publishers; 2009:203–214.
25. Harding R, Taşcıoğlu E. Supported decision-making from theory to practice: implementing the right to enjoy legal capacity. Societies. 2018;8:25. doi:10.3390/soc8020025
26. Keeling A. Supported decision making: the rights of people with dementia. Nurs Stand. 2016;30(30):38–44. doi:10.7748/ns.30.30.38.s45
27.
28. Thoresen L, Lillemoen L, Sævareid TJL, Gjerberg E, Førde R, Pedersen R Guide. Advance Care Planning (ACP) – planning for future health care and end-of-life care together. Available from:
29. Martin DK, Emanuel LL, Singer PA. Planning for the end of life. Lancet. 2000;356(9242):1672–1676. doi:10.1016/S0140-6736(00)03168-8
30. Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. Cmaj. 2006;174(5):627–633. doi:10.1503/cmaj.050626
31. Saini G, Sampson EL, Davis S, et al. An ethnographic study of strategies to support discussions with family members on end-of-life care for people with advanced dementia in nursing homes. BMC Palliat Care. 2016;15:55. doi:10.1186/s12904-016-0127-2
32. Mignani V, Ingravallo F, Mariani E, Chattat R. Perspectives of older people living in long-term care facilities and of their family members toward advance care planning discussions: a systematic review and thematic synthesis. Clin Interv Aging. 2017;12:475–484. doi:10.2147/CIA.S128937
33. Zwakman M, Jabbarian LJ, van Delden J, et al. Advance care planning: a systematic review about experiences of patients with a life-threatening or life-limiting illness. Palliat Med. 2018;32(8):1305–1321. doi:10.1177/0269216318784474
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
35. Braun V, Clarke V. Successful Qualitative Research: A Practical Guide for Beginners. Los Angeles (CA): Sage; 2013.
36. Thoresen L, Ahlzén R, Solbrække KN. Advance Care Planning in Norwegian nursing homes—who is it for? J Aging Stud. 2016;38:16–26. doi:10.1016/j.jaging.2016.04.003
37. De Vleminck A, Pardon K, Beernaert K, Houttekier D, Vander Stichele R, Deliens L. How do general practitioners conceptualise advance care planning in their practice?: a qualitative study. PLoS One. 2016. doi:10.1371/journal.pone.0153747
38. Ampe S, Sevenants A, Smets T, Declercq A, Van Audenhove C. Advance care planning for nursing home residents with dementia: influence of ‘we DECide’ on policy and practice. Patient Educ Couns. 2017;100(1):139–146. doi:10.1016/j.pec.2016.08.010
39. Birchley G, Jones K, Huxtable R, Dixon J, Kitzinger J, Clare L. Dying well with reduced agency: a scoping review and thematic synthesis of the decision-making process in dementia, traumatic brain injury and frailty. BMC Med Ethics. 2016;17(1):46. doi:10.1186/s12910-016-0130-4
40. De Boer ME, Dröes R-M, Jonker C, Eefsting JA, Hertogh CMPM. Thoughts on the future: the perspectives of elderly people with early-stage alzheimer’s disease and the implications for advance care planning. AJOB Prim Res. 2012;3(1):14–22. doi:10.1080/21507716.2011.636784
41. Goodman C, Amador S, Elmore N, Machen I, Mathie E. Preferences and priorities for ongoing and end-of-life care: a qualitative study of older people with dementia resident in care homes. Int J Nurs Stud. 2013;50(12):1639–1647. doi:10.1016/j.ijnurstu.2013.06.008
42. Ingravallo F, Mignani V, Mariani E, Ottoboni G, Melon MC, Chattat R. Discussing advance care planning: insights from older people living in nursing homes and from family members. Int psychogeriatrics/IPA. 2018;30(4):569–579. doi:10.1017/S1041610217001983
43. Piers R, Albers G, Gilissen J, et al. Advance care planning in dementia: recommendations for healthcare professionals. BMC Palliat Care. 2018;17:1. doi:10.1186/s12904-018-0373-6
44. Musa I, Seymour J, Narayanasamy MJ, Wada T, Conroy S. A survey of older peoples’ attitudes towards advance care planning. Age Ageing. 2015;44(3):371. doi:10.1093/ageing/afu189
45. Fosse A, Ruths S, Malterud K. Doctors learning experiences in end-of-life care - a focus group study from nursing homes. BMC Med Educ. 2017;17:1. doi:10.1186/s12909-017-0865-8
46. van Der Steen JT, Galway K, Carter G, Brazil K. Initiating advance care planning on end-of-life issues in dementia: ambiguity among UK and Dutch physicians. Arch Gerontol Geriatr. 2016;65:225–230. doi:10.1016/j.archger.2016.04.005
47. Fine E, Reid MC, Shengelia R, Adelman RD. Directly observed patient-physician discussions in palliative and end-of-life care: a systematic review of the literature. J Palliat Med. 2010;13(5):595–603. doi:10.1089/jpm.2009.0388
48. Thoresen L, Lillemoen L. “I just think that we should be informed” a qualitative study of family involvement in advance care planning in nursing homes. BMC Med Ethics. 2016;17(1):72. doi:10.1186/s12910-016-0130-4
49. Froggatt K, Vaughan S, Bernard C, Wild D. Advance care planning in care homes for older people: an English perspective. Palliat Med. 2009;23(4):332–338. doi:10.1177/0269216309103802
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.