")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Short Term and Long-Term Efficacy of Calcipotriene/ Betamethasone Dipropionate Foam Combination
Authors Jalili A, Bewley A , Sticherling M, Stein Gold L
Received 16 February 2022
Accepted for publication 15 April 2022
Published 2 May 2022 Volume 2022:15 Pages 809—814
DOI https://doi.org/10.2147/CCID.S361884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Ahmad Jalili,1 Anthony Bewley,2 Michael Sticherling,3 Linda Stein Gold4
1Dermatology & Skin Care Clinic, Buochs, Switzerland; 2Barts Health NHS Trust and Queen Mary University London, London, UK; 3Department of Dermatology, Psoriasis Center, University Medical Center, Erlangen, Germany; 4Department of Dermatology, Henry Ford Health System, Detroit, MI, USA
Correspondence: Linda Stein Gold, Department of Dermatology, Henry Ford Health System, Detroit, MI, USA, Email [email protected]
Abstract: Psoriasis is a well-known chronic disease characterized by the development of erythematous, indurated, scaly, pruritic plaques on the skin with cycles of remission and symptom flare-ups. The management of patients with chronic plaque psoriasis has been more challenging since the Covid-19 pandemic as health care professionals have had to adapt to remote consultations for some patients, and patients have had to adapt to the changing health landscape. The rapid resolution of psoriasis symptoms especially those with a substantial impact on quality of life can improve patient satisfaction and adherence, making it an important factor in successful treatment. Cal/BD foam contributes to improved patient adherence and treatment outcome through its rapid action and superior efficacy versus Cal or BD monotherapy, Cal/BD ointment and gel and clobetasol cream in the short-term flare treatment of psoriasis. Moreover, the benefits of proactive long-term management of psoriasis compared to reactive management and its favourable safety profile are higher efficacy and a better health-related quality of life. Cal/BD foam should be considered an effective topical treatment for short-term flare treatment and long-term control of adult psoriatic patients.
Keywords: psoriasis, adherence, proactive management, quality of life
Introduction
The short paper below will address the content of 2 industry hubs presented at the virtual EADV 2021, focusing on the holistic management of psoriasis with topical treatments, treating flare-ups in the short term and controlling disease relapses in the long term.
Management of patients with chronic plaque psoriasis is optimal when it is patient-centric. The holistic management of psoriasis with topical combination Calcipotriol/Betamethasone (Cal/BD) treatments, treating the flare-ups in the short term and controlling disease relapses in the long-term is both patient-centric and a helpful alternative in light of changes in consultation since the Covid 19 pandemic. Cal/BD foam formulation presents two main advantages compared to other topical treatments: firstly, its rapid onset of action which can be attributed to the foam formulation leading to fast resolution of symptoms with a positive impact on quality of life (QoL) and the potential improvement of patients’ adherence and thus the outcome; secondly, the superior efficacy of proactive long-term management with Cal/BD foam versus the reactive management of psoriasis.1–3
Discussion
Psoriasis is a well-known chronic disease characterized by development of erythematous, indurated, scaly, pruritic plaques on the skin with cycles of remission and symptom flare-ups. The treatment depends on the severity of the disease; mild or moderate psoriasis, represented by 80% of patients, is managed with topical treatments.4
However, despite the large range of available products, treatment adherence remains low, leading to suboptimal disease resolution and then poor QoL by the presence of the plaques with physical symptoms such as itching (64–97% of patients with psoriasis suffer from itching), itch-related sleep loss, and psychological and social well-being consequences.1,2,5,6 The Global Burden of Disease project revealed that skin and subcutaneous disorders are the 4th most important cause of non-fatal disease burden with a deterioration of health-related QoL similar to cancer and cardiovascular disease.1,6 Recent studies have shown that for almost 75% of patients their psoriasis has a moderate to large impact on their QoL, 34% experiencing sleep disorders and more than 5% suicidal ideation.1,2,7 Effective improvement on outcomes linked to QoL and rapid onset of action is a key factor for treatment success and has the potential to improve adherence to treatment.1,6
Short Term Efficacy
Findings across pooled analysis of Phase II/III studies revealed that Cal/BD foam has a rapid onset of action, provides fast resolution of psoriasis symptoms with visible results as early as week 1, particularly those shown to have a significant impact on QoL versus Cal/BD gel or foam vehicle, and has the potential to improve adherence and thus patient outcomes in psoriasis.8,9
A pooled analysis of three Phase II/III studies assessing efficacy and health-related QoL outcomes showed a rapid reduction in itching as early as Day 3 through Week 4 associated with significant improvements in itch-related sleep loss and sleep quality for patients treated with Cal/BD foam versus foam vehicle.10
In addition, a second post-hoc, pooled analysis of three Phase II/III trials described a rapid mode of action with Cal/BD foam, and a greater proportion of Cal/BD foam-treated patients achieving absolute mPASI targets and improving QoL outcomes as early as week 1 versus foam vehicle treated patients.9
Cal/BD foam has also shown superior efficacy to its individual components, calcipotriol and betamethasone dipropionate, Cal/BD gel and ointment formulations as well as clobetasol cream.11–14
In one study, the percentage of patients achieving treatment success after 4 weeks, defined by a PGA score is higher in the Cal/BD foam group than in the Cal/BD ointment group (54.6% vs 43%).13 In a second study, 52.1% of patients receiving Cal/BD foam achieved PASI75 after 4 weeks, compared with 24.3% receiving Cal/BD gel.12
Cal/BD foam has also demonstrated superior effectiveness to clobetasol cream, along with higher levels of patient satisfaction.14 In a recent interventional investigator-initiated Phase IV study, more patients treated with Cal/BD foam achieved a total clinical score of 1 or less, indicating better clinical resolution than with clobetasol.14 Cal/BD foam induced a significantly faster response than clobetasol, with 80% of patients achieving a meaningful reduction in total clinical score, versus 43.4% at 4 weeks.14 Despite the increased penetration of calcipotriol and betamethasone, no increased AEs or negative safety outcomes has been observed.15
The rationale for the superior efficacy of Cal/BD foam can be explained by the association of the two components and the foam formulation:
In combination, calcipotriol and betamethasone dipropionate have complementary, synergistic effects that help controlling psoriasis inflammation.16
Propellants contained in the foam formulation evaporate rapidly and lead to the formation of a thin supersaturated layer on the skin increasing the penetration and the bioavailability of active ingredients Cal/BD.17,18
In addition to data showing the superiority of Cal/BD foam over its individual components and Cal/BD ointment and gel formulations, the early efficacy of Cal/BD foam was demonstrated in the treatment of psoriasis flare-ups.
In the lead-in open label Phase of the PSO-LONG 52-week study, 80% of patients (n=521) achieved treatment success, measured by PGA clear and almost clear, with at least a 2-grade improvement from baseline after 4 weeks of treatment. Of these responders, 21.1% and 78.9% had a PGA score of clear and almost clear, respectively. The mean change from baseline in mPASI score at Week 4 was 82.1%, with a mean change in body surface area of 56.6%.19
In the Phase III, randomised PSO-FAST study, Cal/BD foam was shown to improve the health-related QoL (primarily driven by pain/discomfort and anxiety/depression) for moderate to severe psoriasis patients receiving it after 4-weeks, with most of them experiencing clinically meaningful improvements (DLQI and EQ-5D scores) and almost 50% reporting no impairment to QoL at all (DLQI = 0/1) (Figure 1). For itching, one of the main symptoms responsible for the discomfort, 84% of patients receiving Cal/BD foam achieved at least a 70% reduction in itching by Week 4. The correlation between itching and DLQI has been shown to be strong, suggesting the substantial impact of itching on QoL, and the importance of prioritising this symptom during treatment.2
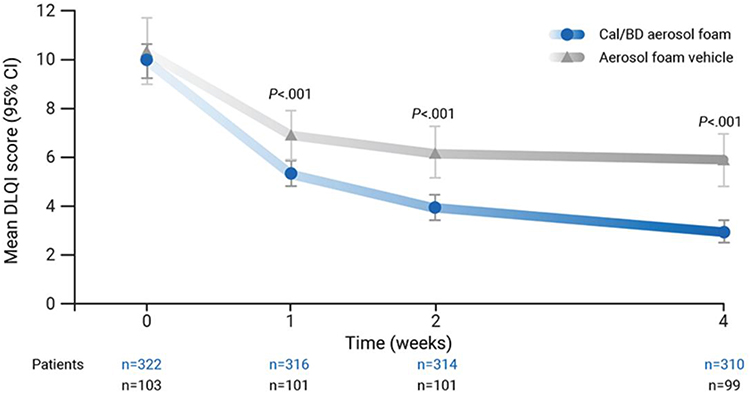 |
Figure 1 Mean dermatology life-quality index score by visit (observed cases). Phase III randomized PSO-FAST study (N=426). |
Data from 5 different real-world studies in more than 1400 patients across the US and Europe (Greece, Germany and Spain-2 studies) show similar improvements in effectiveness, QoL (PGA, change in BSA, PASI and DLQI), patient-reported outcomes, and confirmation of the safety profile of Cal/BD foam established in randomised controlled trials.20–24
In the Spanish studies, adherence to treatment with Cal/BD foam was high (100% and 73.8% of patients after 4 and 12 weeks respectively) and the percentage of patient satisfaction (completely satisfied) was 84.6%. 93% of physicians believed that using Cal/BD foam had a quite good or a very good influence on adherence.22,23
Cal/BD foam was shown to induce rapid, effective responses, resolve troublesome symptoms like itch, improve QoL and was well tolerated. Thus, patients and physicians were satisfied with treatment leading to high levels of product acceptability and adherence.20–24
Long-Term Efficacy
Leading experts in psoriasis identified an unmet need for longer-term solutions for flare control in patients treated through topical therapy.4
Despite the availability of several treatments’ options, many patients do not achieve complete and sustained disease resolution in the long term with negative impact on patients’ QoL. Long-term management of psoriasis is challenging because of the relapsing and remitting, chronic nature of the disease, delayed treatment responses and poor adherence.6,25 Currently, it relies on a reactive approach to treat disease relapses rather than a proactive approach to maintain remission.
However, relapse is common as underlying residual lesion can remain following initial skin clearance and lesions tend to recur after therapy has been discontinued.6,26–28
The randomised, Phase III PSO-LONG study provides evidence of the benefits of long-term, proactive management of Cal/BD foam (twice weekly) in treating psoriasis and the superiority to reactive management (flare treatment once daily for 4 weeks), increasing time to first relapse (+26 days), and reducing the number of relapses (risk of experiencing first relapse reduced by 46% and lower predicted number of relapses per year of exposure) and increasing days in remission (+41 days).3
The side effects of steroid-based topicals are considered a major barrier to long-term use. This aspect was approached by a sub-analysis of the Phase III PSO-LONG which assessed the safety of long-term proactive management with Cal/BD foam over 52 weeks in patients with more severe psoriasis (PGA≥3 and affected BSA 10–30%). These patients may be more susceptible to corticosteroid-induced HPA-axis suppression and a higher risk of corticosteroid-induced systemic toxicity.6,29
However, no clinically significant HPA-axis suppression in either the reactive or proactive treatment groups was found, no new safety signals were detected and the safety profile was similar for both proactive and reactive treatments.29
Similarly positive results were seen in a recent analysis of PSO-LONG by Kircik et al, which looked at skin atrophy and local tolerability of long-term treatment with Cal/BD foam. Regarding skin disorders, assessments done at visits where the patient was not starting or ending a relapse, or in a relapse, low levels of dryness, erosion, erythema, oedema or burning or pain were reported. At the start and end of relapses, local skin reactions and burning or pain were present at slightly higher levels than non-relapse-related visits but were absent for around 90% of patients in both treatment groups, with cases usually mild. Skin atrophy was not reported by investigators at any point, in either treatment group.30
Added to the primary efficacy results from PSO-LONG study, a recent post-hoc analysis of this study shows data supporting these primary outcomes. In this post-hoc analysis, authors projected the clinical course of patients over a 1-year period using a multistate model, which assessed four different states; remission (after the open-label lead-in phase and re-entered if they achieved clear or almost clear skin defined by a PGA <2 after 4 weeks of relapse treatment), relapse (confirmed relapse, or a PGA ≥2), end of treatment (day of premature withdrawal and the completion of the study) and treatment failure (no achievement of clear or almost clear skin after 4 weeks of relapse treatment). The estimated mean stay in the remission state was 81.3 days for proactive management versus 48.9 days for reactive management. Patients in the proactive management group had an estimated 36 more total days in remission and 34 less total days in relapse compared to reactive management and they were also expected to have fewer relapses than patients in the reactive management group – 2 versus 3.2 relapses, respectively.31
Two other post-hoc analyses from PSO-LONG investigated the quality-of-life benefits after long-term management with Cal/BD foam, focussing on the impact of treatment on patient reported outcomes such as perceived symptom severity and health-related QoL. In both analyses there were significant advantages of a proactive, twice-weekly, management approach with Cal/BD foam versus reactive flare treatment, with patients reporting better and more sustained health-related QoL outcomes. In the first analysis, patients showed sustained improvement in DLQI, PSI and EQ–5D scores with significantly greater improvement in the proactive group during both the open-label and maintenance phases (DLQI and PSI 15% lower in proactive group vs reactive group).32 In the second analysis, proactive management using Cal/BD foam prolongs time with health-related QoL improvement compared with reactive management: the risk of patients losing DLQI benefit (0/1) was reduced by 48% in the proactive group and the median time to lost response was almost 3.5 times longer for the proactive group (Figure 2).33
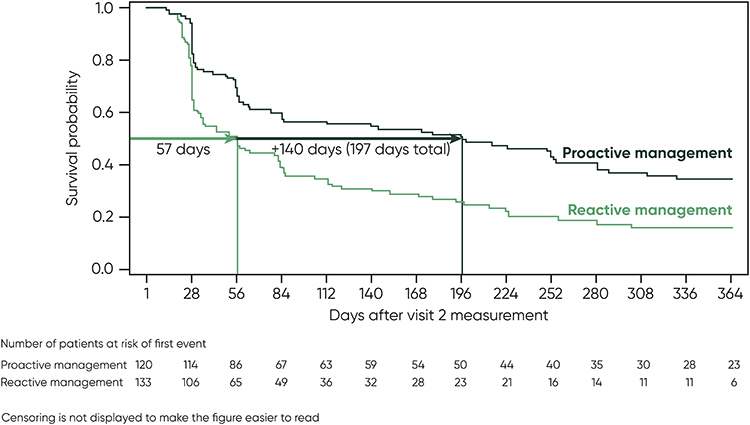 |
Figure 2 Estimated survival curve for time to first DLQI>1. PSO-LONG study. |
Conclusion
Rapid resolution of psoriasis symptoms especially those with a substantial impact on quality of life can improve patient satisfaction and adherence, making it an important factor in successful treatment. Cal/BD foam contributes to improve patient adherence and treatment outcome by its rapid onset of action and its superior efficacy versus Cal or BD monotherapy, Cal/BD ointment and gel and clobetasol cream in short term flare treatment of psoriasis. Moreover, the benefits of proactive long-term management of psoriasis are the superiority in term of efficacy and improvements in health-related quality of life compared to reactive management and its favourable safety profile.
Cal/BD foam should be considered an effective topical treatment for short term flare-up treatment and long-term control of adult psoriatic patients.
Acknowledgments
Editorial assistance was provided by Peggy Cance, of Alhena Consult SAS (Valbonne, France). This assistance was supported by Leo Pharma.
Disclosure
Dr Jalili has been a consultant and advisor and/or received speaking fees and/or grants and/or served as an investigator in clinical trials for the following companies: AbbVie, Amgen, Boehringer Ingelheim, BMS, Celgene, Eli Lilly, GSK, LEO Pharma, Janssen, MSD, Novartis and Sanofi. Pr Bewley reports a research grant from the European Academy of Dermatology Venereology for Practical Psychodermatology; ad hoc consultancy and travel grants from Almirall, Janssen and LEO Pharma; and consultancy fees from AbbVie, Almirall, Celgene, Galderma, Janssen, LEO Pharma, Eli Lilly, Novartis, Sanofi, UCB Pharma. He is also Treasurer and a member of guidelines committees for the British Association of Dermatology, Secretary of the European Society for Dermatology and Psychiatry, Chair of the All-Party Parliamentary Group on Skin, and acts as an Advisor for the Psoriasis Association, Changing Faces, Ichthyosis Support Group and the National Eczema Society. Pr Sticherling was an advisor and/or received honoraria for speaking and/or received grants and/or participated in clinical trials for AbbVie, Almirall, Amgen, Boehringer Ingelheim, BMS, Celgene, Eli Lilly, Galderma, GSK, Janssen-Cilag, LEO Pharma, MSD, Novartis, Pfizer, Regeneron, Sanofi, Sandoz/Hexal, and UCB Pharma. Dr. Stein Gold is a consultant, investigator and/or speaker for LEO Pharma, Arcutis, Dermavant, Pfizer, AbbVie, Lilly, and Ortho Derm. The authors report no other conflicts of interest in this work.
References
1. Jalili A, Yosipovitch G. Fixed‐dose combination calcipotriol/betamethasone dipropionate foam provides a rapid onset of action, effective itch relief and improves patient quality of life. J Eur Acad Dermatol Venereol. 2021;35(Suppl 1):20–27. doi:10.1111/jdv.17085
2. Leonardi C, Bagel J, Yamauchi P, et al. The aerosol foam formulation of the fixed combination calcipotriene plus betamethasone dipropionate improves the health-related quality of life in patients with psoriasis vulgaris: results from the randomized PSO-FAST study. J Drugs Dermatol. 2016;15(8):981–987.
3. Lebwohl M, Kircik L, Lacour JP, et al. Twice-weekly topical calcipotriene/betamethasone dipropionate foam as proactive management of plaque psoriasis increases time in remission and is well tolerated over 52 weeks (PSO-LONG trial). J Am Acad Dermatol. 2021;84(5):1269–1277. doi:10.1016/j.jaad.2020.09.037
4. Segaert S, Calzavara-Pinton P, De la Cueva P, et al. Long-term topical management of psoriasis: the road ahead. J Dermatolog Treat. 2020;24:1–10.
5. Thaçi D, De la Cueva P, Pink A, et al. General practice recommendations for the topical treatment of psoriasis: a modified-Delphi approach. BJGP Open. 2020;4(5):bjgpopen20X101108. doi:10.3399/bjgpopen20X101108
6. Lebwohl M, Thaçi D, Warren RB. Addressing challenges associated with long‐term topical treatment and benefits of proactive management in patients with psoriasis. J Eur Acad Dermatol Venereol. 2021;35(Suppl 1):35–41. doi:10.1111/jdv.17053
7. Bhosle MJ, Kulkarni A, Feldman SR, Balkrishnan R. Quality of life in patients with psoriasis. Health Qual Life Outcomes. 2006;4(1):35. doi:10.1186/1477-7525-4-35
8. World Health Organization. Global report on psoriasis. World Health Organization; 2016. Available from: https://apps.who.int/iris/handle/10665/204417.
9. Pink AE, Jalili A, Berg P, et al. Rapid onset of action of calcipotriol/betamethasone dipropionate cutaneous foam in psoriasis, even in patients with more severe disease. J Eur Acad Dermatol Venereol. 2019;33(6):1116–1123. doi:10.1111/jdv.15398
10. Jalili A, Lebwohl M, Stein Gold L, et al. Itch relief in patients with psoriasis: effectiveness of calcipotriol plus betamethasone dipropionate foam. J Eur Acad Dermatol Venereol. 2019;33(4):709–717. doi:10.1111/jdv.15393
11. Lebwohl M, Tyring S, Bukhalo M, et al. Fixed combination aerosol foam calcipotriene 0.005% (cal) plus Betamethasone Dipropionate 0.064% (BD) is more efficacious than cal or BD aerosol foam alone for psoriasis vulgaris: a randomized, double-blind, multicenter, three-arm, phase 2 study. J Clin Aesthet Dermatol. 2016;9(2):34–41.
12. Paul C, Stein Gold L, Cambazard F, et al. Calcipotriol plus betamethasone dipropionate aerosol foam provides superior efficacy vs. gel in patients with psoriasis vulgaris: randomized, controlled PSO-ABLE study. J Eur Acad Dermatol Venereol. 2017;31(1):119–126. doi:10.1111/jdv.13859
13. Koo J, Tyring S, Werschler WP, et al. Superior efficacy of calcipotriene and betamethasone dipropionate aerosol foam versus ointment in patients with psoriasis vulgaris–A randomized Phase II study. J Dermatolog Treat. 2016;27(2):120–127. doi:10.3109/09546634.2015.1083935
14. Yélamos O, Alejo B, Ertekin SS, et al. Non-invasive clinical and microscopic evaluation of the response to treatment with clobetasol cream vs. calcipotriol/betamethasone dipropionate foam in mild to moderate plaque psoriasis: an investigator-initiated, Phase IV, unicentric, open, randomized clinical trial. J Eur Acad Dermatol Venereol. 2021;35(1):143–149. doi:10.1111/jdv.16559
15. Leonardi C, Bagel J, Yamauchi P, et al. Efficacy and safety of calcipotriene plus betamethasone dipropionate aerosol foam in patients with psoriasis vulgaris–a randomized phase III study (PSO-FAST). J Drugs Dermatol. 2015;14(12):1468–1477.
16. Segaert S, Shear NH, Chiricozzi A, et al. Optimizing Anti-Inflammatory and Immunomodulatory effects of corticosteroid and vitamin D analogue fixed-dose combination therapy. Dermatol Ther. 2017;7(3):265–279. doi:10.1007/s13555-017-0196-z
17. Lind M, Nielsen KT, Schefe LH, et al. Supersaturation of calcipotriene and betamethasone dipropionate in a novel aerosol foam formulation for topical treatment of psoriasis provides enhanced bioavailability of the active ingredients. Dermatol Ther. 2016;6(3):413–425. doi:10.1007/s13555-016-0125-6
18. Tada Y, Iversen L, Koo J. Early efficacy and safety data with fixed-dose combination calcipotriol/betamethasone dipropionate foam attributed to mechanism of absorption and steroid potency. J Eur Acad Dermatol Venereol. 2021;35(Suppl1):5–9. doi:10.1111/jdv.17027
19. Warren RB, Gold M, Gooderham M, et al. Four-week daily calcipotriene/betamethasone dipropionate foam is highly efficacious in patients with psoriasis (PSO-LONG lead-in phase). J Drugs Dermatol. 2021;20(4):436–441. doi:10.36849/JDD.5728
20. Rigopoulos D, Lazaridou E, Papadavid E, et al. A real-world, observational study on the effectiveness with calcipotriol/betamethasone aerosol foam in patients with plaque psoriasis in Greece: the CELSUS study. J Eur Acad Dermatol Venereol. 2021;35(7):e454–e457.
21. Wu JJ, Veverka KA, Lu M, Armstrong AW. Real-world experience of calcipotriene and betamethasone dipropionate foam 0.005%/0.064% in the treatment of adults with psoriasis in the United States. J Dermatolog Treat. 2019;30(5):454–460. doi:10.1080/09546634.2018.1535689
22. Navarro-Triviño FJ, Lozano-Lozano M, Ruiz-Villaverde R. Calcipotriol/betamethasone dipropionate aerosol foam for plaque psoriasis: a prospective, observational, non-interventional, single-center study of patient adherence and satisfaction in daily use. Dermatol Pract Concept. 2021;11(3):e2021056. doi:10.5826/dpc.1103a56
23. Velasco M, González-Fernández D, Rodriguez-Martín M, Sánchez-Regaña M, Pérez-Barrio S. Patient and physician satisfaction with calcipotriol and betamethasone dipropionate aerosol foam in the treatment of plaque psoriasis on the body. Actas Dermosifiliogr. 2019;110(9):752–758. doi:10.1016/j.ad.2019.03.013
24. Gerdes S, Krakor M, Anger T, Hutt HJ, Körber A. Prospective, observational, non-interventional, multicentre study on the efficacy and tolerability of a new calcipotriol/betamethasone aerosol foam (enstilar®) in patients with plaque psoriasis under daily practice conditions. Dermatology. 2017;233(6):425–434. doi:10.1159/000486700
25. Strober BE, van der Walt JM, Armstrong AW, et al. Clinical goals and barriers to effective psoriasis care. Dermatol Ther. 2019;9(1):5–18. doi:10.1007/s13555-018-0279-5
26. Suárez-Fariñas M, Fuentes-Duculan J, Lowes MA, Krueger JG. Resolved psoriasis lesions retain expression of a subset of disease-related genes. J Invest Dermatol. 2011;131(2):391–400. doi:10.1038/jid.2010.280
27. Benezeder T, Wolf P. Resolution of plaque-type psoriasis: what is left behind (and reinitiates the disease). Semin Immunopathol. 2019;41(6):633–644. doi:10.1007/s00281-019-00766-z
28. Clark RA. Gone but not forgotten: lesional memory in psoriatic skin. J Invest Dermatol. 2011;131(2):283–285. doi:10.1038/jid.2010.374
29. Papp K, Adamski Z, Guenther L, et al. Efficacy and safety of proactive treatment with twice-weekly topical Cal/BD foam in patients with plaque psoriasis undergoing HPA-axis testing: a PSO-LONG subgroup analysis [published online ahead of print, 2021 Aug 9]. J Dermatolog Treat;2021. 1–8. doi:10.1080/09546634.2021.1959501
30. Kircik L, Holst Mørch M, Petersen B, Liljedahl M, Wollenberg A. Long-term treatment of plaque psoriasis with Cal/BD foam was locally well tolerated and not associated with skin atrophy. American Academy of Dermatology; 2021. Available from https://eposters.aad.org/abstracts/26260.
31. Gold LS, Jalili A, Danic DL, Nyholm N, Thoning H, Calzavara‐Pinton P. 26607 proactive management using Cal/BD foam in patients with plaque psoriasis prolongs time with a health-related QoL improvement, compared with reactive management. J Am Acad Dermatol. 2021;85(3):AB109. doi:10.1016/j.jaad.2021.06.455
32. Warren RB, Papp K, Holst Mørch M Long-term proactive treatment of plaque psoriasis vulgaris with Cal/BD foam was associated with prolonged time in remission and reduced number of relapses. American Academy of Dermatology; 2021. Available from: https://eposters.aad.org/abstracts/26838.
33. Jalili A, Calzavara-Pinton P, Kircik L, et al. Quality of life and patient-perceived symptoms in patients with psoriasis undergoing proactive or reactive management with the fixed-dose combination Cal/BD foam: a post-hoc analysis of PSO-LONG. J Eur Acad Dermatol Venereol. 2022;36(1):60–67. doi:10.1111/jdv.17673
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.