")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Short-term adverse effects of the apolipoprotein E ϵ4 allele over language function and executive function in healthy older adults
Authors Li W, Qiu Q, Sun L, Li X , Xiao S
Received 8 August 2018
Accepted for publication 10 June 2019
Published 10 July 2019 Volume 2019:15 Pages 1855—1861
DOI https://doi.org/10.2147/NDT.S183064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yuping Ning
Wei Li,1,2,* Qi Qiu,1,2,* Lin Sun,1,2,* Xia Li1,2 Shifu Xiao1,2
1Department of Geriatric Psychiatry, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China; 2Alzheimer’s Disease and Related Disorders Center, Shanghai Jiao Tong University, Shanghai, China
*These authors contributed equally to this work
Background: The 4 allele of the apolipoprotein E (APOE) gene is known as a risk factor for cognitive impairment. How APOE ϵ polymorphism affects the language and executive functions of healthy aging subjects remains less clear.
Purpose: In this follow-up study, the relationship between APOE status and cognitive performance across various cognitive domains in healthy individuals (without dementia or mild cognitive impairment (MCI)) over 60 years old was investigated.
Patients and methods: Based on multiplex amplification refractory mutation system polymerase chain reaction (PCR), 228 subjects (n=228; mean age: 70.59±8.07 years old; male %=40.8%) were divided into three groups, e2 (ϵ2/ϵ2 and ϵ2/ϵ3, n=35), e3 (ϵ3/ϵ3, n=152), and e4 (ϵ2/ϵ4, ϵ3/ϵ4, and ϵ4/ϵ4, n=41).
Results: There was no statistical difference (p>0.05) in the general demographic data and neuropsychological tests among the three groups on the baseline; however, e4 group showed a greater drop rate (p<0.05) versus non-carriers on verbal fluency (e2: −0.043±0.221; e3: -0.081±0.239; e4: 0.069±0.329) and Webster picture completion (e2: 0.055±0.281; e3: 0.083±0.428; e4: 0.438±1.280) over the subsequent one year.
Conclusion: The findings suggest that possession of the APOE ϵ4 allele predicted a higher decline on tasks of language function and executive function in healthy elderly. And further research is required to determine whether strengthening the training of language function and executive function will delay the occurrence of cognitive impairment.
Keywords: APOE, language function, executive function, healthy elderly
Introduction
Apolipoprotein E (APOE) is a polymorphic protein involved in neurogenesis, repair, and plasticity, which has 3 allelic variants (ε2, ε3, and ε4)1. The ε4 allele of apolipoprotein E (APOE) is the most clearly defined genetic risk factor for sporadic Alzheimer’s disease (AD). Carriers of the ε4 allele are not only at an increased risk of AD but also are prone to early onset.2 Additionally, the probability of remaining unaffected over time will also decrease in an apoE4 gene dose-dependent manner.3 However, the prevalence of APOE ε4 among people with AD varies across geographic regions and is significantly lower in Asia than in North America and Europe.4 It has been demonstrated that APOE ε4 contributes to the biological modulation of β-amyloid (Aβ) clearance.5 Genome-wide association studies (GWASs) evaluating the cerebral amyloid burden endophenotype have also reinforced APOE ε4’s role in amyloid accumulation.6 And previous longitudinal studies find that there is only a marginal joint effect of AD genes (such as CLU, PICALM, BIN1, CR1, ABCA7, MS4A6A, MS4A4E, CD2AP, EPHA1, and CD33) on memory independent from APOE in nondemented people.5,6 What is more, patients with APOE ε4 often show some defects in the repair of nerve injury7 as well as exhibit an altered lifespan trajectory in the ability of the brain to dynamically modulate function to cognitive challenge.8
There is ample evidence that a subset of older individuals who are cognitively normal have Alzheimer’s disease (AD) pathology in their brains.9,10 And such individuals are more likely to develop cognitive decline over time, and at some point during this “preclinical” phase of disease, whose cognitive changes will become evidence.11 Mounting evidences suggest that the APOE genotype will play an important role in affecting the specific cognitive function of normal adults; for example, Reinvang et al find that in normally aging adults, the ε4 allele adversely affects their cognitive performance, particularly on tests of memory function.12 Some longitudinal studies also suggest that episodic memory declines more rapidly among cognitive normal older individuals who are ε-4 carriers than non-carriers.13 What is more, a meta-analysis shows that the e4 allele was linked to better verbal fluency scores,14 and another meta-analysis15 suggests that ApoE ɛ4 exerts broad, but specific, adverse small effects on a range of neurocognitive functions (such as episodic memory, executive functioning, and perceptual speed) in cognitively healthy adults. However, other studies16,17 do not find evidence for such association.
Various explanations for these conflicting results may be put forward. First, cross-sectional studies are not able to determine definitely whether possession of the ε4 allele is associated with within-person cognitive changes.18 Second, genes are not the determinants of cognitive changes, and copies of ε4 only modulate effects of other features (such as age, illiteracy, and female) over cognitive decline.19 Third, many studies only focus on general cognitive ability rather than assessing a range of specific cognitive domains.19 Furthermore, vascular risk factors, such as smoking, drinking wine, hypertension, and diabetes, are associated with cognitive performance as well as APOE genotype,20 but few studies correct for these potential confounding factors. Therefore, in the present study, we attempted to address the above-mentioned limitations accompanying earlier research, by using a longitudinal design, to explore the relationship between APOE genotype and different domains of cognitive function (such as the language function and executive function) among the healthy elderly in China.
Materials and methods
Participants
All participants were recruited from urban sites in the North XinJing district of Shanghai, China. And the method of sampling has been described in our previous studies.21 The inclusion criteria were as follows: 1) 60 years and older; 2) denial of memory impairment and other cognitive impairments; 3) without major medical abnormalities, including unstable, acute, or life-threatening medical illness and central nervous system diseases; 4) was able to complete the entire inspection. Subjects with a history of severe mental problems (eg, schizophrenia, depression, anxiety, mild cognitive impairment (MCI), and dementia) or major medical abnormalities (eg, cancer and infection) that might affect cognitive function were excluded. All participants needed to complete a clinical evaluation and some neuropsychological tests. What is more, we also used a standardized questionnaire to collect their general demography data, including name, sex, profession, educational degree as well as medical history (such as hypertension, diabetes, and hyperlipidemia). Finally, 562 healthy older adults (mean age: 72.21±8.20; mean years of education: 8.94±4.72; 232 males) completed the baseline assessment, and 228 healthy subjects (mean age: 70.59±8.07; mean years of education: 9.62±4.14; 93males) completed the one-year follow-up assessment as well as the APOE allele detection. Reasons for not attending included withdrawal (n=76), inability, or refusal to participate (n=107), having moved away (n=28), exclusion due to memory problems or depression (n=37), and data missing (n=86). Table 1 lists the general demographic data of the 228 people.
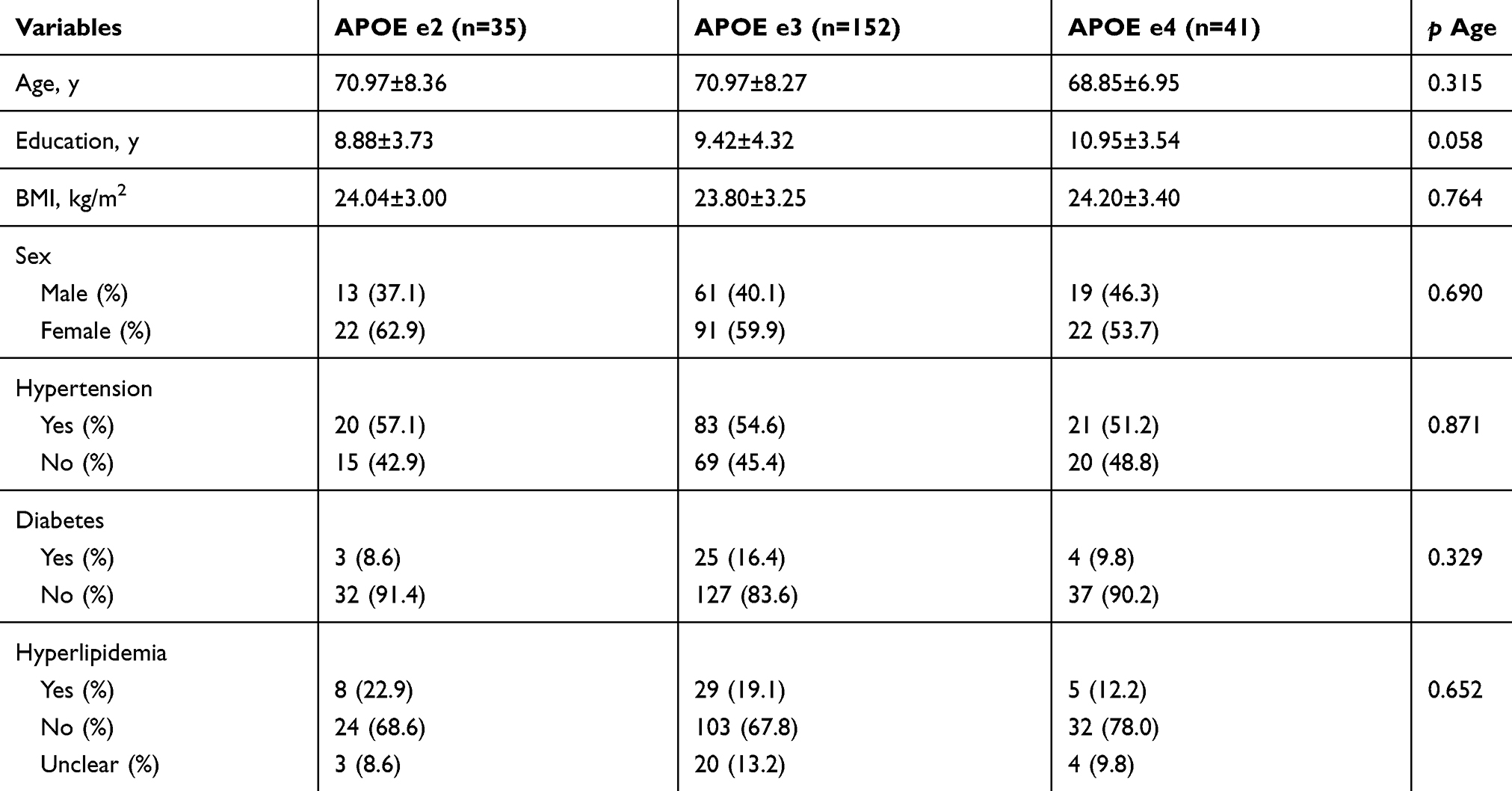 |
Table 1 Comparison of main characteristic variables among the 3 groups |
This study was conducted in accordance with the principles of Declaration of Helsinki. The Research Ethical Committee of the affiliated mental health center of Shanghai Jiaotong University School of Medicine approved this study, and written informed consent was obtained from all participants.
Clinical assessment and cognitive assessment
In order to exclude depression, dementia, and other mental diseases, all participants underwent a screening process that included a review of their medical history, physical and neurological examinations (by an experienced psychiatrist), laboratory tests, and MRI scans. The Mini-Mental State Examination (MMSE) and the Neuropsychological Test Battery (include Wechsler Memory Scale (WMS), Verbal Associates immediate and 30-mins delayed test, Digit span, Picture completion, Rey Auditory Verbal Learning and 30-mins Delayed test, etc.) were used as tools to assess their general cognitive ability and specific cognitive domains, respectively.
MMSE is a short test that assesses cognitive functions like memory, recall, alertness, speech, language reception as well as orientation to time and space.22 It is widely used in clinical practice and has been proved to be effective in distinguishing between dementia and normal people.23 However, the main limitation of MMSE is its poor sensitivity in detecting a mild degree of cognitive impairment, namely the ceiling effect, which is becoming a particularly important issue with the recent increased focus of researchers on cognitive function.24
Neuropsychological Test Battery (NTB) comprises digit span, auditory verbal learning test (AVLT) (immediate and delayed recall), associative learning, visual identification test, verbal fluency test, picture completion test, and block design, and all the tests are time-limited:25
- Digit span (scores range from 0 to 17) is measured for forward and backward recall of digit sequences. They are presented beginning with a length of two digits and two trails are presented at each increasing list length. Test will cease when the subjects fail to accurately report either trail at one sequence length or when the maximal list length is reached (9 digit forward, 8 back ward). This test is used to assess attention and working memory.26
- Auditory verbal learning test (AVLT) (scores range from 0 to 75):27 It is a serial word list learning task presenting 15 words over 5 trials. A distractor list is presented for a single trial, followed by spontaneous recall of the initial 15 words. Following a 30 mins delay, free recall of the original word list is obtained followed by recognition. This test is used to assess learning ability, delayed free recall, and recognition memory.
- Webster picture completion (scores range from 0 to 22):28 this test contains 21 incomplete pictures, and each picture lacks the most important part. The subjects need to point out the missing part of each picture. This test is used to evaluate the executive function.
- Webster block design (scores range from 0 to 48):29 this test requires construction of abstract designs from colored blocks. The total raw score is recorded to assess visuospatial and executive function.
- Associative learning and visual identification test (scores range from 0 to 25): This test consists of four tests: functional connection, semantic connection, recognition, visual matching, and reasoning. It can measure the function of visual attention and processing speed.
- Verbal fluency (scores range from above 0):30 the subjects are asked to give words beginning with three different letters, and the total number of correct response is recorded. We use this test to measure language ability related to executive function.
So NTB is able to quantitatively evaluate 5 cognitive domains, including attention, working memory, language, visuospatial function, visual memory and executive function.31 And it has been considered as the most valid instrument for monitoring cognitive decline in aMCI and dementia associated with AD.32
Through a combined application of the above two scales, we were able to assess the cognitive function of those subjects in a more comprehensive way. And the cognitive assessments were performed by psychologists at baseline and 12 months, respectively.
Genotyping of APOE
Genomic DNA was extracted from peripheral blood (Morning fasting whole blood) by using a Blood Genomic DNA Extraction Kit (Qiagen NV, Venlo, the Netherlands). APOE genotype was determined by multiplex amplification refractory mutation system polymerase chain reaction (PCR). And this method (Single nucleotide polymorphisms (SNPs) at nucleotides 112 and 158 of the gene were amplified by PCR using Taq DNA polymerase and a thermal profile were optimized for the locus. By identifying the alleles present at the 112 and 158 polymorphisms, APOE genotype was defined) had been described by Donohoe et al.33 According to the methods previously described,34 these 228 subjects were divided into three groups, e2 (ε2/ε2 and ε2/ε3, n=35), e3 (ε3/ε3, n=152), and e4 (ε2/ε4, ε3/ε4, and ε4/ε4, n=41).35 And Table 2 lists the information about the gene distribution in detail.
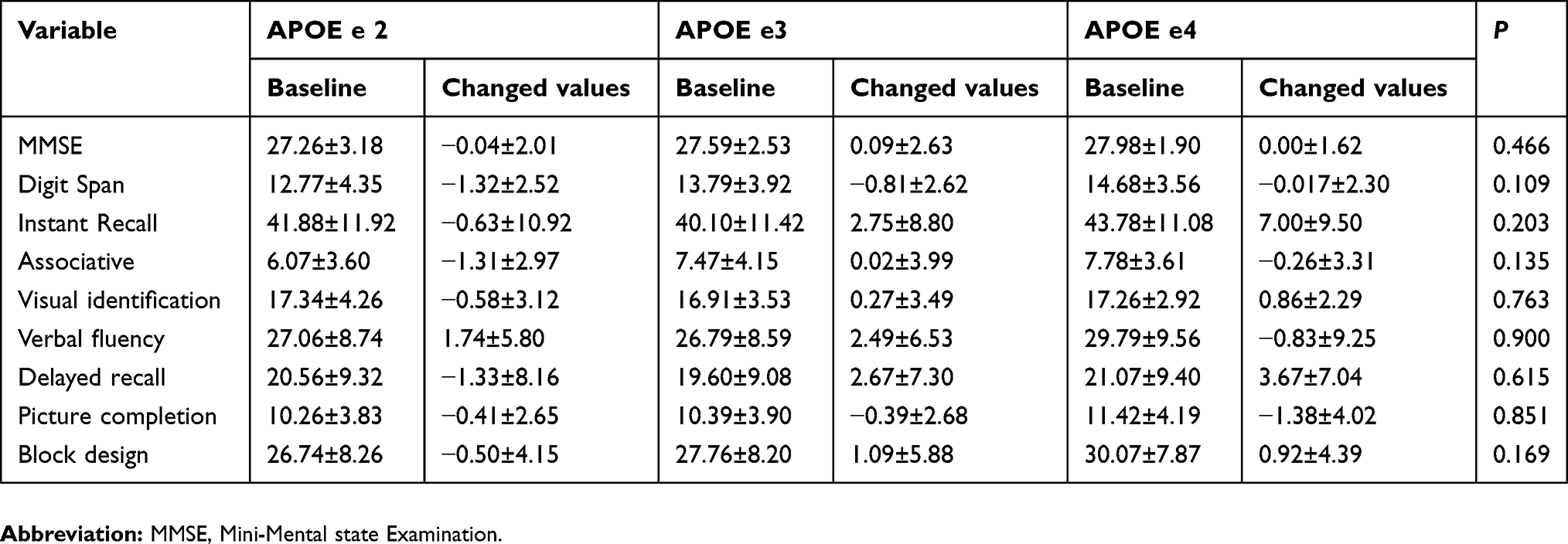 |
Table 2 Trend of outcome measurements among the 3 groups |
Statistical analysis
Continuous variables were expressed as mean and SD, and categorical variables were expressed as frequencies (%). One-way analysis of variance (ANOVA) was used to compare the differences among the e2 group, e3 group, and e4 group (for both baseline and follow-up study). Then, regression analysis was used to screen for possible cognitive factors. Two-tailed tests were used at a significance level of P<0.05 for all analyses. The data were analyzed using SPSS 22.0 (IBM Corporation, Armonk, NY, USA)
Results
Table 1 shows the baseline characteristics of the participants according to APOE ε4 carrier status. Allele frequencies in the sample were e2=15.4%, e3=66.7%, and e4=17.9%. And we found no statistical differences in the variable that might be related to cognitive function as shown above. In addition, there was no difference in baseline scores among the three groups on MMSE, digit span, and other cognitive tests (Table 2) (we had controlled certain variables that might be related to cognitive function, such as age, gender and education, and the statistical method was the One-way analysis of variance (ANOVA) analysis). However, one year later, APOE ε4 carriers showed a greater deduction rate [(baseline score-follow-up score)/baseline score] in verbal fluency and Webster picture completion test than APOE ε4 non-carriers (Table 3), but there was no statistical difference (p>0.05) in the deduction rate of verbal fluency and Webster picture completion test (Table 4). By using regression analysis, we found that the reduction rate of verbal fluency was not related to age, education, gender, BMI, hypertension, diabetes, hyperlipidemia, and APOE genotype (p>0.05). However, the reduction rate of webster picture completion was associated with APOE genotype (T=2.151, p=0.033), while it had nothing to do with age, education, gender, BMI, hypertension, diabetes, and hyperlipidemia (p>0.05).
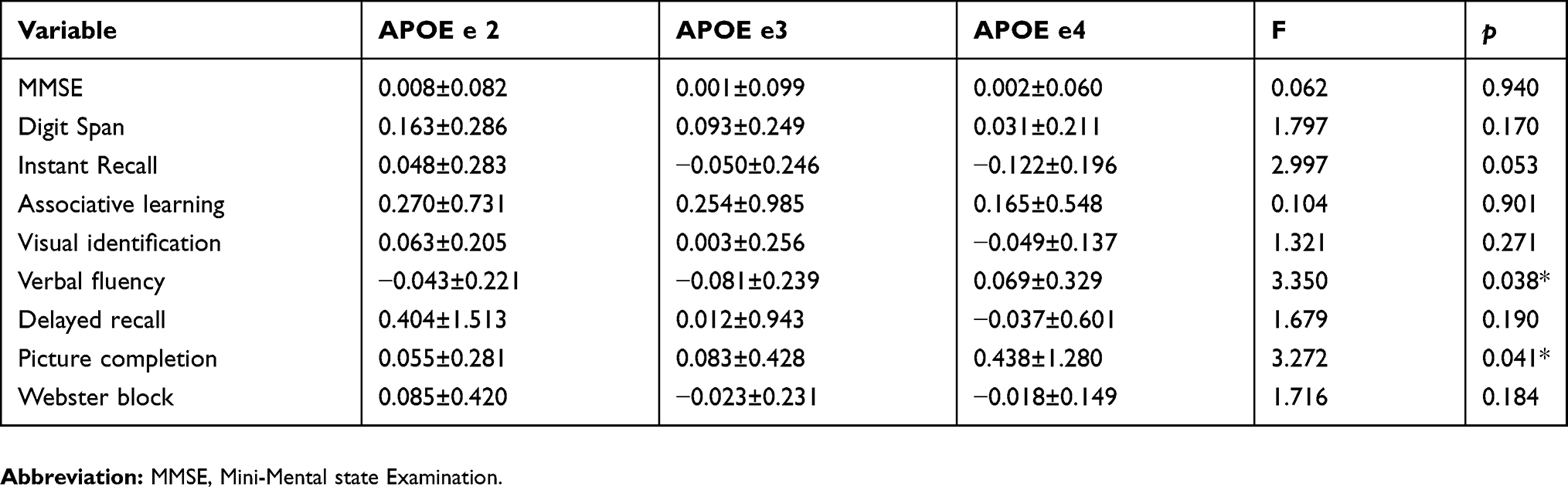 |
Table 3 Comparison of cognitive decline rate among the 3 groups |
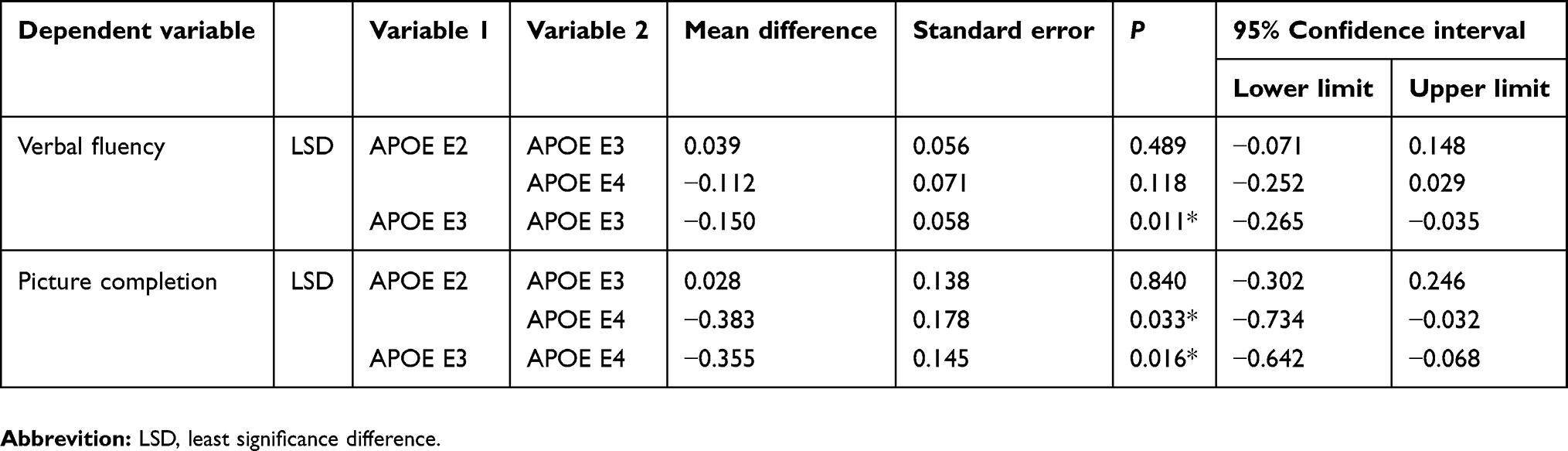 |
Table 4 Multiple comparison of cognitive decline rates among the 3 groups |
Discussion
In this study, we explored the effects of APOE polymorphisms on cognitive performance in healthy aging adults. Different from other cross-section studies,15,36 we conducted a longitudinal study to explore the effects of APOE genotype on holistic and specific cognitive function (by using MMSE and NTB). Meanwhile, we also controlled variables that might affect cognitive results, such as age, sex, education, physical disease (such as hypertension and diabetes) as well as baseline scores of cognitive function. We finally found that APOE ε4 carriers had a greater cognitive decline rate in language function and executive function; however, there was no statistical difference in other areas of cognition, such as attention, working memory, visuospatial and visual memory. Therefore, we speculate that we might predict the risk of future development of MCI and dementia by evaluating these subjects’ language function and executive function.
Previous cross-sectional studies suggested that APOE ε4 status might differentially affect various cognitive functions, such as episodic memory and executive functioning.37 A recent longitudinal study indicated that APOE ε4 allele carrier status was associated with an increased rate of cognitive decline on the domains of verbal memory and abstract reasoning in older healthy individuals.18 And another study suggested that subjects with APOE ε4 might be a deterioration in learning or acquisition performance with age.38 However, other longitudinal studies found that APOE ε4 was only associated with memory decline in subjects with cognitive impairment, but not in normally functioning subjects.39 So the results of these studies were not very consistent.
There are several mechanisms to explain why APOE ε4 can affect specific cognitive functions (executive function and language function). First, APOE ε4 impairs neuronal insulin signaling by trapping insulin receptor in the endosomes,40 which will exert a negative impairment on executive function.41 Second, internal capsule, external capsule, and superior longitudinal fasciculus were more closely related with executive function,42 and the ε4 allele will produce deleterious effects on white matter.43 Third, observational studies in older humans indicate that elevation in cortisol is associated with smaller hippocampal volume and is a risk factor for greater decline in global cognition, executive functioning as well as verbal memory, and APOE ε4 can modify the relation between cortisol and cognitive function such that the slopes of the adverse relations are steeper in the presence of the ε4 allele.44 Fourth, APOE ε4 might contribute to the psychological symptoms, such anxiety, during AD progression.45 And elevated anxiety symptoms will result in more rapid decline in several cognitive domains (global cognition, language, and executive function).46
Although previous longitudinal studies have explored the relationship between APOE and cognitive function, few studies have addressed specific cognitive areas. In our study, we not only explore the relationship between APOE and specific cognitive fields, but also take the normal adult elderly as the research object, which is one of the main innovations of this study. However, there are also containing some limitations: our study is a single center study, and the rate of missing or lost to follow-up is high. Moreover, it is only a one-year follow-up study that cannot observe the long-term effects of APOE on cognitive function.
Conclusion
In conclusion, APOE ε4 is associated with poor performance on tasks of language function and executive function in healthy elderly. Further research is required to determine whether strengthening the training of language function and executive function will delay the occurrence of cognitive impairment.
Acknowledgments
This work was supported by grants from the China Ministry of Science and Technology (2009BAI77B03) and National Natural Science Foundation of China (number 81671402).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mahley RW, Apolipoprotein E. cholesterol transport protein with expanding role in cell biology. Science. 1998;240(4852):622–630. doi:10.1126/science.3283935
2. Nao J, Sun H, Wang Q, et al. Adverse effects of the apolipoprotein E epsilon4 allele on episodic memory, task switching and gray matter volume in healthy young adults. Front Hum Neurosci. 2017;11(19):346–355. doi:10.3389/fnhum.2017.00346
3. Li J, Kanekiyo T, Shinohara M, et al. Differential regulation of amyloid-beta endocytic trafficking and lysosomal degradation by apolipoprotein E isoforms. J Biol Chem. 2012;287(53):44593–44601. doi:10.1074/jbc.M112.420224
4. Ramanan VK, Risacher SL, Nho K, et al. APOE and BCHE as modulators of cerebral amyloid deposition: a florbetapir PET genome-wide association study. Mol Psychiatry. 2014;19(3):351–357. doi:10.1038/mp.2013.19
5. Verhaaren BF, Vernooij MW, Koudstaal PJ, et al. Alzheimer’s disease genes and cognition in the nondemented general population. Biol Psychiatry. 2013;73(5):429–434. doi:10.1016/j.biopsych.2012.04.009
6. Carrasquillo MM, Crook JE, Pedraza O, et al. Late-onset Alzheimer’s risk variants in memory decline, incident mild cognitive impairment, and Alzheimer’s disease. Neurobiol Aging. 2015;36(1):60–67. doi:10.1016/j.neurobiolaging.2014.07.042
7. Arendt T, Schindler C, Bruckner MK, et al. Plastic neuronal remodeling is impaired in patients with Alzheimer’s disease carrying apolipoprotein epsilon 4 allele. J Neurosci. 1997;17(2):516–529.
8. Foster CM, Kennedy KM. Differential aging trajectories of modulation of activation to cognitive challenge in APOE epsilon4 groups: reduced modulation predicts poorer cognitive performance. J Neurosci.2017;37(29):6894–6901. doi:10.1523/JNEUROSCI.3900-16.2017
9. Hulette CM, Welsh-Bohmer KA, Murray MG, Saunders AM, Mash DC, McIntyre LM. Neuropathological and neuropsychological changes in “normal” aging: evidence for preclinical Alzheimer disease in cognitively normal individuals. J Neuropathol Exp Neurol. 1998;57(12):1168–1174. doi:10.1097/00005072-199812000-00009
10. Bennett DA, Schneider JA, Arvanitakis Z, et al. Neuropathology of older persons without cognitive impairment from two community-based studies. Neurology. 2006;66(12):1837–1844. doi:10.1212/01.wnl.0000219668.47116.e6
11. Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280–292. doi:10.1016/j.jalz.2011.03.003
12. Reinvang I, Winjevoll IL, Rootwelt H, Espeseth T. Working memory deficits in healthy APOE epsilon 4 carriers. Neuropsychologia. 2010;48(2):566–573. doi:10.1016/j.neuropsychologia.2009.10.018
13. Albert M, Soldan A, Gottesman R, et al. Cognitive changes preceding clinical symptom onset of mild cognitive impairment and relationship to ApoE genotype. Curr Alzheimer Res. 2014;11(8):773–784.
14. Marioni RE, Campbell A. Differential effects of the APOE e4 allele on different domains of cognitive ability across the life-course. Eur J Hum Genet. 2016;24(6):919–923.
15. Wisdom NM, Callahan JL, Hawkins KA. The effects of apolipoprotein E on non-impaired cognitive functioning: a meta-analysis. Neurobiol Aging. 2011;32(1):63–74. doi:10.1016/j.neurobiolaging.2009.02.003
16. Luciano M, Gow AJ, Taylor MD, et al. Apolipoprotein E is not related to memory abilities at 70 years of age. Behav Genet. 2009;39(1):6–14. doi:10.1007/s10519-008-9236-x
17. Bunce D, Fratiglioni L, Small BJ, Winblad B, Backman L. APOE and cognitive decline in preclinical Alzheimer disease and non-demented aging. Neurology. 2004;63(5):816–821. doi:10.1212/01.wnl.0000137041.86153.42
18. Schiepers OJ, Harris SE, Gow AJ, et al. APOE E4 status predicts age-related cognitive decline in the ninth decade: longitudinal follow-up of the Lothian Birth Cohort 1921. Mol Psychiatry. 2012;17(3):315–324. doi:10.1038/mp.2010.137
19. de Oliveira FF, Chen ES, Smith MC, Bertolucci PH. Associations of blood pressure with functional and cognitive changes in patients with Alzheimer’s disease. Dement Geriatr Cogn Disord. 2016;41(5–6):314–323. doi:10.1159/000447585
20. Fillenbaum GG, Landerman LR, Blazer DG, Saunders AM, Harris TB, Launer LJ. The relationship of APOE genotype to cognitive functioning in older African-American and Caucasian community residents. J Am Geriatr Soc. 2001;49(9):1148–1155.
21. Xiao S, Li J, Tang M, et al. Methodology of China’s national study on the evaluation, early recognition, and treatment of psychological problems in the elderly: the China Longitudinal Aging Study (CLAS). Shanghai Arch Psychiatry. 2013;25(2):91–98. doi:10.3969/j.issn.1002-0829.2013.02.005
22. Pohl R, Lewis R, Niccolini R, Rubenstein R. Teaching the mental status examination: comparison of three methods. J Med Educ. 1982;57(8):626–629.
23. Schmidt H, Elster J, Eckert I, et al. Cognitive functions after spinal tap in patients with normal pressure hydrocephalus. J Neurol. 2014;261(12):2344–2350. doi:10.1007/s00415-014-7489-2
24. Trzepacz PT, Hochstetler H, Wang S, Walker B, Saykin AJ. Relationship between the montreal cognitive assessment and mini-mental state examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015;10(19):107–114. doi:10.1186/s12877-015-0103-3
25. Morris JC, Heyman A, Mohs RC, et al. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology. 1989;39(9):1159–1165. doi:10.1212/wnl.39.9.1159
26. Woods DL, Kishiyamaa MM, Lund EW, et al. Improving digit span assessment of short-term verbal memory. J Clin Exp Neuropsychol. 2011;33(1):101–111. doi:10.1080/13803395.2010.493149
27. Loring DW, Goldstein FC, Chen C, et al. False-positive error rates for reliable digit span and auditory verbal learning test performance validity measures in amnestic mild cognitive impairment and early Alzheimer disease. Arch Clin Neuropsychol. 2016;31(4):313–331. doi:10.1093/arclin/acw014
28. Bhattacharya B, Marwaha RK, Malhotra S, Pershad D. Intellectual functions in childhood malignant disorders. Indian Pediatr. 1995;32(8):869–875.
29. Gao Y, Xiao Y, Miao R, et al. The characteristic of cognitive function in Type 2 diabetes mellitus. Diabetes Res Clin Pract. 2015;109(2):299–305. doi:10.1016/j.diabres.2015.05.019
30. de Paula JJ, Paiva GCC, Costa DS. Use of a modified version of the switching verbal fluency test for the assessment of cognitive flexibility. Dement Neuropsychol. 2015;9(3):258–264. doi:10.1590/1980-57642015dn93000008
31. Ahn HJ, Chin J, Park A, et al. Seoul Neuropsychological Screening Battery-dementia version (SNSB-D): a useful tool for assessing and monitoring cognitive impairments in dementia patients. J Korean Med Sci. 2010;25(7):1071–1076. doi:10.3346/jkms.2010.25.7.1071
32. Kim J, Na HK, Byun J, et al. Tracking cognitive decline in amnestic mild cognitive impairment and early-stage alzheimer dementia: mini-mental state examination versus neuropsychological battery. Dement Geriatr Cogn Disord. 2017;44(1–2):105–117. doi:10.1159/000478520
33. Donohoe GG, Salomaki A, Lehtimaki T, Pulkki K, Kairisto V. Rapid identification of apolipoprotein E genotypes by multiplex amplification refractory mutation system PCR and capillary gel electrophoresis. Clin Chem. 1999;45(1):143–146.
34. Anderson GD, Temkin NR, Dikmen SS, et al. Haptoglobin phenotype and apolipoprotein E polymorphism: relationship to posttraumatic seizures and neuropsychological functioning after traumatic brain injury. Epilepsy Behav. 2009;16(3):501–506. doi:10.1016/j.yebeh.2009.08.025
35. Rodriguez FS, Schroeter ML, Arelin K, et al. APOE e4-genotype and lifestyle interaction on cognitive performance: results of the LIFE-adult-study. Health Psychol. 2018;37(2):194–205. doi:10.1037/hea0000515
36. Lancaster C, Forster S, Tabet N, Rusted J. Putting attention in the spotlight: the influence of APOE genotype on visual search in mid adulthood. Behav Brain Res. 2017;15(334):97–104. doi:10.1016/j.bbr.2017.07.015
37. Small BJ, Rosnick CB, Fratiglioni L, Backman L. Apolipoprotein E and cognitive performance: a meta-analysis. Psychol Aging. 2004;19(4):592–600. doi:10.1037/0882-7974.19.4.592
38. Rawle MJ, Davis D, Bendayan R, Wong A, Kuh D, Richards M. Apolipoprotein-E (Apoe) ε4 and cognitive decline over the adult life course. Transl Psychiatry. 2018;8(1):10–18. doi:10.1038/s41398-017-0056-8
39. Dik MG, Jonker C, Bouter LM, Geerlings MI, van Kamp GJ, Deeg DJ. APOE-epsilon4 is associated with memory decline in cognitively impaired elderly. Neurology. 2000;54(7):1492–1497. doi:10.1212/wnl.54.7.1492
40. Zhao N, Liu CC, Van Ingelgom AJ, et al. Apolipoprotein E4 impairs neuronal insulin signaling by trapping insulin receptor inthe endosomes. Neuron. 2017;96(1):115–129. doi:10.1016/j.neuron.2017.09.003
41. Zhao Q, RO R, Ding D, et al. Diabetes is associated with worse executive function in both eastern and western populations: Shanghai aging study and Mayo clinic study of aging. J Alzheimers Dis. 2015;47(1):167–176. doi:10.3233/JAD-150073
42. Urger SE, De Bellis MD, Hooper SR, Woolley DP, Chen SD. Provenzale, J. The superior longitudinal fasciculus in typically developing children and adolescents: diffusion tensor imaging and neuropsychological correlates. J Child Neurol 2015;30(1):9–20. doi:10.1177/0883073813520503.
43. Zhang S, Chen Y, Liu Z, et al. Association of white matter integrity and cognitive functions in Chinese non-demented elderly with the APOE ɛ4 allele. J Alzheimers Dis. 2015;48(3):781–791. doi:10.3233/JAD-150357
44. Lee BK, Glass TA, Wand GS, et al. Apolipoprotein E genotype, cortisol, and cognitive function in community-dwelling older adults. Am J Psychiatry. 2008;165(11):1456–1464. doi:10.1176/appi.ajp.2008.07091532
45. Panza F, Frisardi V, Seripa D, et al. Apolipoprotein E genotypes and neuropsychiatric symptoms and syndromes in late-onset Alzheimer’s disease. Ageing Res Rev. 2012;11(1):87–103. doi:10.1016/j.arr.2011.06.005
46. Pietrzak RH, Lim YY, Neumeister A, et al. Amyloid-β, anxiety,and cognitive decline in preclinical Alzheimer disease: amulticenter, prospective cohort study. JAMAPsychiatry. 2015;72(3):284–291.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.