")
Back to Journals » Nature and Science of Sleep » Volume 14
Short Sleep Duration and Erectile Dysfunction: A Review of the Literature
Authors Zhang F , Xiong Y , Qin F, Yuan J
Received 5 June 2022
Accepted for publication 14 October 2022
Published 27 October 2022 Volume 2022:14 Pages 1945—1961
DOI https://doi.org/10.2147/NSS.S375571
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Fuxun Zhang1,2 *, Yang Xiong1,2 *, Feng Qin,1 Jiuhong Yuan1,2
1Andrology Laboratory, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiuhong Yuan, Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China, Email [email protected]
Abstract: The meaning of sleep has puzzled people for millennia. In modern society, short sleep duration is becoming a global problem. It has been established that short sleep duration can increase the risk of several diseases, such as cardiovascular and metabolic diseases. Currently, a growing body of research has revealed a possible link between sleep disorders and erectile dysfunction (ED). However, the mechanisms linking short sleep duration and ED are largely unknown. Thus, we provide a review of clinical trials and animal studies. In this review, we propose putative pathways connecting short sleep duration and ED, including neuroendocrine pathways and molecular mechanisms, aiming to pave the way for future research. Meanwhile, the assessment and improvement of sleep quality should be recommended in the diagnosis and treatment of ED patients.
Keywords: erectile dysfunction, molecular mechanisms, sleep disorder, short sleep duration, signaling pathway
Introduction
Sleep is vital to life. As a mystery of biology, the roles of sleep have puzzled and intrigued people for millennia.1 For adults, the recommended sleep duration is 7 to 9 hours, while short sleep duration is defined as habitual sleep time less than 6 hours.2 Sleep disorders are divided into 7 major diagnostic sections based on International Classification of Sleep Disorders-3 (ICSD-3), including insomnia, sleep-related breathing disorders, central disorders of hypersomnolence, circadian rhythm sleep-wake disorders, parasomnias, sleep-related movement disorders and other sleep disorders.3 Short sleep duration, as one of the most notable characteristics of sleep disorders and some psychiatric disorders, was received with concern in modern society.3,4 Meanwhile, it is reported that sleep disorders with short sleep duration appear to have more severe manifestation than those with normal sleep duration.5,6 Furthermore, it is estimated that the prevalence of short sleep duration has gradually increased, in which 29.1% of US adults reported short sleep duration in 2009, including the habitual short sleepers and those with medical conditions.7 Although many issues remain unresolved, the association between short sleep duration and many negative health outcomes, such as cardiovascular diseases, metabolic diseases and inflammatory disorders, has been widely investigated.8,9 Furthermore, several studies have hinted that short sleep may be associated with men’s health and sexual function.10,11
Erectile dysfunction (ED) is defined as the inability to acquire or maintain penile erection for satisfactory sexual performance.12 Although ED is not a fatal condition, it bothers a large proportion of males around the world.13,14 It is suggested that more than 80% of patients with ED have organic etiologies, including vascular, neurological and endocrine factors.12 However, ED still involves the psychological component, especially in younger males.15 Thus, it must be pointed out that previous psychological problems and the disturbance of psychosocial process, such as sleep homeostasis, may be involved in the pathophysiology of ED. Similarly, the etiology and pathophysiology of sleep disorders are thought to be associated with a variety of elements and medical conditions.16 Although ED and sleep disorders are prevalent in modern society, the mainstream in this field almost universally focuses on the relationship between sleep-related breathing disorders and ED.17,18 Therefore, current data is not enough to interpret the effects of non-apnea sleep disorders with short sleep duration on erectile function.
Actually, available evidence indicates that short sleep duration might have a negative influence on erectile function.19,20 However, ED can be either the consequence or the cause of short sleep. Due to the absence of intermediate mechanisms, it is difficult to prove a causal link between short sleep duration and ED. For example, short sleep duration and ED may influence each other via complex interactions or coexist independently in an individual patient. Even so, several pathophysiological mechanisms have been proposed to link sleep duration and medical conditions in recent years.21,22 Moreover, causal associations of short sleep duration with various diseases seem to dominate in current studies.8,23 Thus, we reviewed available data on sleep and erection (Table 1) and proposed putative mechanisms underlying causal associations of short sleep duration with ED, in order to facilitate further studies to elucidate the causal link between short sleep duration and ED.
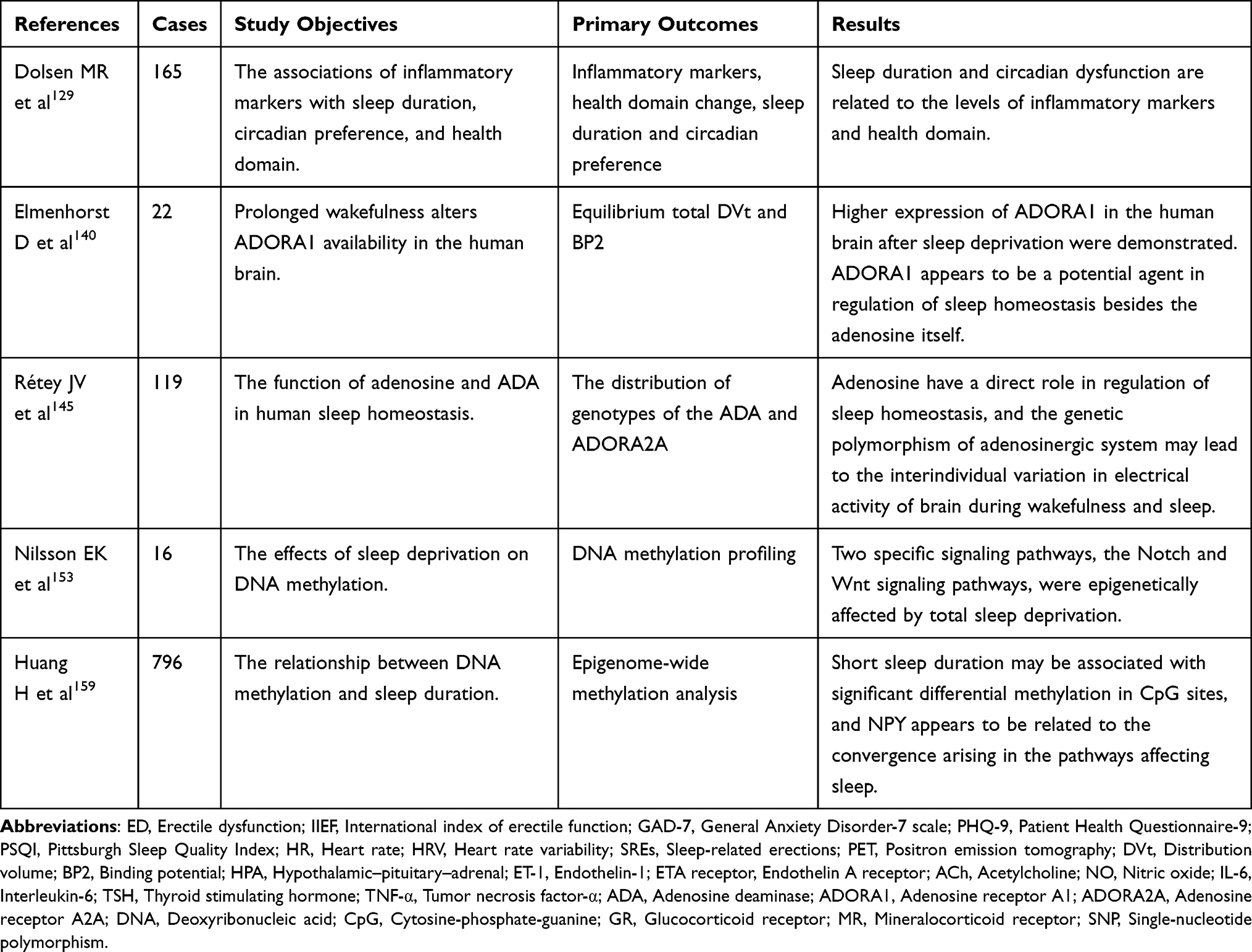 |
Table 1 Studies Linking Sleep Duration and Erectile Dysfunction in Humans |
Sleep
Normal Sleep
Sleep is a reversible natural behavior characterized by loss of consciousness, insensitivity toward stimuli, and inhibition of voluntary movements, which can be assessed by physiological, cellular, molecular and genetic levels.24 Sleep, in both animals and humans, is investigated in the laboratory by recording the activity of cortical neurons, eyes, and muscles using polysomnography (PSG).1 Meanwhile, sleep is regarded as having many neural functions, such as promoting physiological homeostasis in the brain and maintaining normal mood and cognition.25 With prolonged wakefulness, the duration and intensity of sleep are increasing, indicating that sleep might be modulated through the sleep homeostasis.26 Moreover, the circadian system is another component that regulates the timing of sleep independent of prior wakefulness.27 In mammals, the circadian clock is coordinated by the suprachiasmatic nucleus (SCN) and is responsible for synchronizing circadian rhythm on several body functions and behaviors including sleep and wake.27,28 Therefore, circadian and homeostatic components play an important role in the regulation of sleep.
Hypothalamic–Pituitary–Adrenal Axis and Autonomic Nervous System
Sleep has a regulatory effect on the hypothalamic–pituitary–adrenal (HPA) axis and the autonomic nervous system (ANS).29 Different from sleep-related breathing disorders, the exact mechanisms of non-apnea sleep disorders affecting health have not been elucidated. It is reported that short sleep duration could result in hyperarousal characterized by a high level of physiological arousal both in wakefulness and sleep.30 In particular, patients with short sleep always have increased activity of the HPA axis and imbalance of ANS.29,31 Additionally, short sleep is thought to be not only a phenotype of some sleep disorders but a causal risk factor for several diseases.32
The HPA axis linking to the circadian rhythm of sleep is primarily regulated by the circadian oscillator.21 Generally, sleep could inhibit the activity of the HPA axis, and increased HPA axis activity can result in the hyper-arousal and sleep disturbance.33 The increased plasma concentrations of adrenocorticotropic hormone (ACTH) and cortisol were found in healthy subjects after one night of sleep deprivation, indicating the nervous hyper-arousal.34 Moreover, as a shortened sleep in the experimental setting, sleep deprivation in animal models also leads to the increased secretion of inflammatory cytokines, such as tumor necrosis factor-α (TNF-α), and recovery sleep following sleep deprivation seems to inhibit these inflammatory cytokines which might be potential mediators of sleepiness.35,36 Accordingly, the interactions between the HPA axis and inflammatory cytokines might be important to sleep regulation. At the same time, overactivity of the HPA axis could be considered as a potential pathway connecting short sleep and conditions.
The relationship between sleep and ANS is bidirectional. The activity of ANS is influenced by sleep, and changes in different stages of sleep.37 In all, the neuronal populations associated with the transition of sleep stages have close ties with the nervous area controlling the cardiovascular system.38 During normal sleep, the heart rate and blood pressure increase at the rapid eye movement (REM) stage and drop at the non-REM sleep stage, demonstrating the oscillation of ANS activity.39 It is believed that patients with sleep disorders are susceptible to autonomic dysfunction, and most of them have increased sympathetic activity with higher levels of circulating catecholamine and inflammatory markers.40 Meanwhile, several sleep disorders characterized by short sleep duration might result in unbalancing of ANS activity.41 Taken together, the abnormal HPA axis and imbalanced ANS may be the main connection link short sleep and other diseases including ED, and the signaling pathway between short sleep duration and ED is complicated and extensive.
Penile Erection and ED
Penile erection is a complicated physiological process. Generally, sexual stimulation activates the erectile tissue through the non-adrenergic non-cholinergic (NANC) fibers and parasympathetic cholinergic fibers, resulting in the activation of neural nitric oxide synthase (nNOS) and endothelial nitric oxide synthase (eNOS), and subsequently release of nitric oxide (NO).12 NO activates guanylyl cyclase (GC) following entering corpus cavernosum smooth muscle cells (CCSMC), and increases the cyclic guanosine monophosphate (cGMP) level in the cytoplasm, resulting in the decreased intracellular levels of calcium, the relaxation of CCSMC and penile erection. Meanwhile, cGMP could be hydrolyzed by phosphodiesterase (PDE) in CCSMC, leading to the increase of calcium in the cytoplasm and a flaccid penis.12,42 There are 13 kinds of PDE in corpus cavernosum of human.43 Among them, the higher expression of PDE5 in corpus cavernosum has been established, and PDE5 inhibitors (PDE5Is) have been widely applied as a therapeutic revolution in the management of ED.44
On the contrary, the flaccidity of the penis is maintained by chronic contraction of CCSMC.45 The molecular mechanism of penile flaccidity is mainly regulated by noradrenaline (NA), endothelin-1 (ET-1), and angiotensin II (Ang-II) signaling, which triggers an increase in intracellular calcium and thereby results in the contraction of CCSMC via the phosphorylation of myosin light chain (MLC).42,45 However, the contraction of smooth muscle is not paralleled with the levels of intracellular calcium and the phosphorylation of MLC, suggesting the existence of signal pathway which inhibits the smooth muscle relaxation independent of NO.46 Ras homolog gene family member A (RhoA) is a small GTPase that can activate Rho-associated coiled-coil containing kinase (ROCK). ROCK deactivates the myosin light-chain phosphatase (MLCP) by phosphorylating myosin phosphatase target subunit 1 (MYPT1), or directly phosphorylates the myosin light chain 2 (MLC2), promoting the smooth muscle contraction and penile flaccidity, which is also known as the calcium-sensitized pathway.47,48
On the other hand, noradrenaline (NA) released from adrenergic nerve binds the adrenergic receptors (ADRs) in corpus cavernosum and leads to a contraction which involves the influx of calcium in CCSMC and calcium-sensitized pathway.49 It has been demonstrated that penile erection in humans was accompanied by a remarkable decrease of NA in cavernous blood.50 Meanwhile, current evidence supports the viewpoint that post-synaptic adrenergic receptor α1 (ADRα1) in smooth muscle may play a leading role in contraction.51 Existing data have demonstrated the potential effect of adenosine in penile erection, priapism, and ED.52 The role of adenosine is played through its binding to specific G protein-coupled receptors, including A1, A2A, A2B, and A3.53 Among them, adenosine receptor (ADOR) A2B appears to be required for vasodilation and erection via cAMP and cGMP induction.54 In line with previous studies, it was reported that adenosine-induced vasodilation is also mediated through ADOR A2A signaling, conversely, ADOR A1 signaling has an effect on vascular tone regulation.55 Moreover, the regulation of penile erection has close links with many other agents and signaling pathways, including endothelins-1 (ET-1), TNF-α and reactive oxygen species (ROS).56,57
In short, the regulation of normal erectile function is a sophisticated balance of molecular mechanisms and multi-factor process, in which potential risk factors might cause an imbalance and trigger ED (Figure 1). Meanwhile, spinal and central nervous regulation of the penile erection involves various molecules, such as serotonin, dopamine, oxytocin and many peptides. However, most of them are only partly known. Thus, ED is a common but multidimensional psychosomatic disorder and psychological and central nervous components or pathways should not be overlooked.
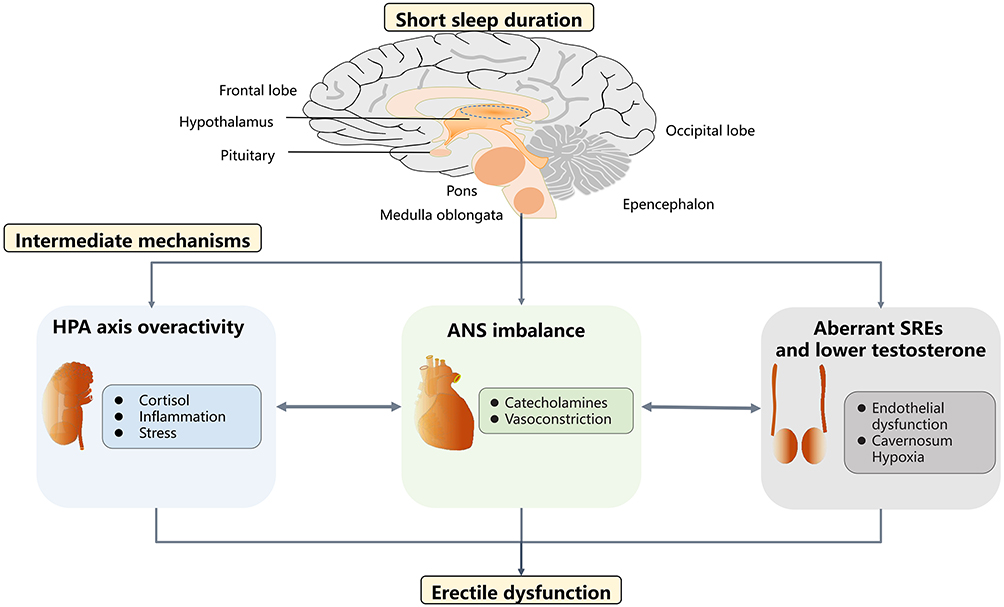 |
Figure 1 Putative mechanisms linking short sleep duration and erectile dysfunction. Short sleep duration caused by sleep disorders or lifestyle might provoke the over-activity of the HPA axis, the imbalance of ANS, aberrant SREs and low levels of testosterone. These intermediate mechanisms could lead to unwanted effects on penile erection through varied downstream molecular signaling, including but not limited to endothelial dysfunction, excessive vasoconstriction, inflammation and hypoxia. Abbreviations: HPA axis: Hypothalamic-pituitary-adrenal axis; ANS: Autonomic nervous system; SREs: Sleep-related erections; NPY: Neuropeptide Y. |
Short Sleep Duration and ED
Short sleep duration might be associated with social elements, including but not limited to shift work, intense work mission or unhealthy lifestyles in modern society.58 Meanwhile, short sleep duration has been demonstrated to be related to a large group of disorders, such as diabetes, hypertension, major depressive disorder, and other morbidities.59,60 Actually, the relationship between several sleep disorders and ED has been revealed by previous studies.61,62 However, most of these studies focus on the sleep-related breathing disorders characterized by hypoxaemia, such as obstructive sleep apnea (OSA).62,63 Actually, short sleep duration as an important phenotype of sleep disorders should be payed more attention. Thus, despite the connection between short sleep duration and ED is mainly based on some circumstantial evidence, it is necessary to explore the putative links between them.
Shift work, an underlying cause of short sleeper, is a prevalent working schedule in the world, which involves about 20% of the labor force worldwide.64 Common schedules in shift work comprise standard and non-standard formats, including morning, night, evening shifts, and irregular rotation occurring outside of a standard time in the workday.65 Similar to sleep disorders, shift work might result in the circadian disturbance, daytime dysfunction, acute sleep loss and short sleep.64 Although the original researches demonstrated mixed results, shift work might be a risk factor for cancer, stroke and cardio-metabolic diseases.66 It is suggested that men occupied in shift work have worse penile erection, especially those work night shifts, which may attribute to short sleep and disrupted circadian rhythm.67 Moreover, men working non-standard shifts are susceptible to short sleep duration and shift work sleep disorders, which are associated with frequent hypogonadal symptoms and poor erectile function.68 These studies add the growing evidence that sleep is important to erectile function. However, there are some inevitable confounding factors existed in shift work comparing with the short sleep duration, and the situation of the working shift seems to be not completely same with common sleep disorders.
Recently, a prospective cohort study investigated the association between sleep parameters and ED using both questionnaires and sleep monitors, demonstrating that sleep duration, including total sleep duration and deep sleep duration, is significantly different between healthy subjects and ED patients who have significantly shorter sleep time.69 Meanwhile, some previous studies seem to provide consistent evidence. A longitudinal population-based cohort study conducted a longer follow-up to participants with sleep disorders and found that those with short sleep duration had the increased risk of developing ED after accounting for age and comorbidities.19 Meanwhile, an investigation performed via Amazon’s Mechanical Turk (MTurk) showed a significant relationship between insomnia and sexual function in males after adjustment for other variables about anxious and depressive symptoms.70 It is reasonable to infer that short sleep might participate in the process of ED among insomnia patients. Similarly, a cross-sectional designed pilot study using mobile health platforms showed an underlying connection between poor sleep quality and ED.71 In addition, a subgroup analysis of older adults suggested that self-reported sleep duration might be related to sexual dysfunction.11
In recent years, although mixed results were concluded usually, more and more studies provided clues that short sleep duration might be a risk factor for ED.69,72 However, the cross-sectional nature of those studies restrict the establishment of a causal relationship, and impede the development of further research. Accordingly, new insights from experimental evidence involving potential molecular mechanisms are needed.
Putative Pathways Linking Short Sleep Duration and ED
Hypothalamic–Pituitary–Adrenal Axis
The HPA axis consists of stimulating and inhibitory loops involving the pituitary and adrenal glands, which regulate the secretion of glucocorticoids, such as the cortisol released from the adrenal cortex.73 It is pointed out that short sleep duration, recurrent sleep disturbance and chronic insomnia symptoms are associated with cortisol-secreting patterns throughout the day.74,75 In humans, short sleep duration induced by sleep deprivation or restriction results in some higher levels of cortisol with the circadian variation.76 Although mixed results were concluded in studies on sleep-deprived animal models, sleep deprivation procedures have a tendency to affect the levels of corticosterone of rodents.29,77 In short, the changes of cortisol secretion in short sleepers may reflect the dysfunction of the HPA axis, and have adverse effects on erectile function.
Actually, cortisol plays an important role in maintaining the tone of vascular smooth muscles (VSMCs) via increasing vascular responses to vasoconstrictors.78 It is proven that sustained elevation of serum cortisol facilitates the contraction of coronary VSMCs by enhancing RhoA/ROCK signaling pathway.79 Conversely, adrenalectomized animal models show decreased responsiveness to the administration of vasoactive agents, which are similar to Addisonian in humans.80 With regard to sexual function, it has been reported that the levels of serum cortisol are negatively correlated with some domains of the International Index of Erectile Function-5 (IIEF-5) score and males with high levels of serum cortisol might be vulnerable to ED.81 Although this was previously interpreted as a stress-related outcome due to the relationship between the HPA axis and stress, we hold the opinion that the disordered the HPA axis might be an important cog between sleep disorders and ED (Figure 1). Meanwhile, short sleep, stress and disordered HPA axis may coexist inevitably and have the complex interplay in sleep-related conditions.
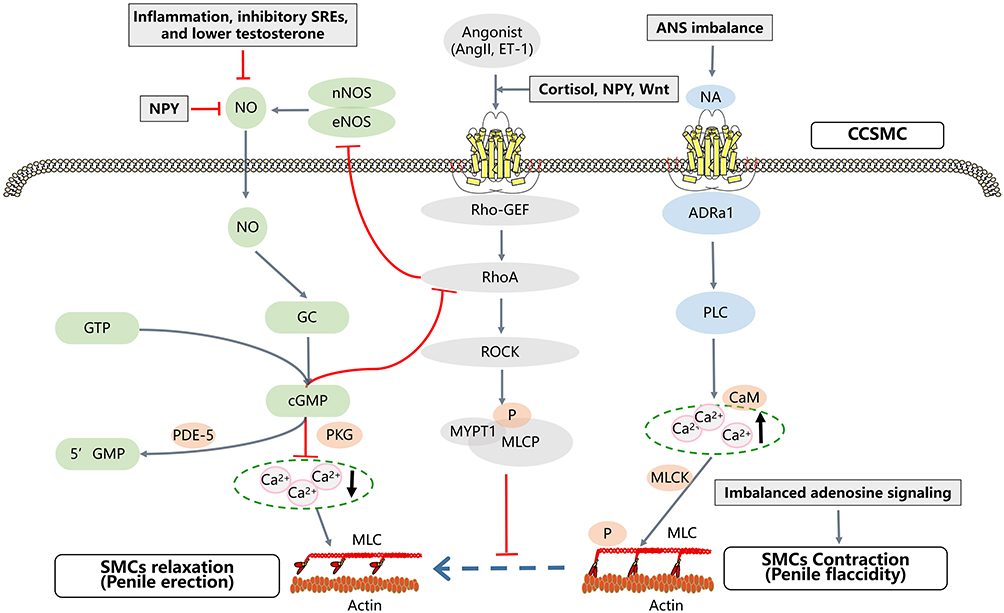 |
Figure 2 Principal molecular mechanisms of penile erection, and possible targets by which short sleep duration impairing the erectile function.The molecular mechanisms of penile erection involve a balance of signaling between relaxation and contraction of CCSMC. Generally, the NOS-NO-cGMP signaling pathway is considered as the most important mechanism of penile erection, involving the PKG activation and decreased intracellular levels of calcium. On the contrary, penile flaccidity is mainly regulated by the NA, ET-1, and AngII signaling, involving increasing levels of intracellular calcium . Meanwhile, RhoA/ROCK signaling known as the calcium-sensitized pathway, and NA-ADRa1 signaling are crucial to regulate the chronic contraction of CCSMC. In all, ROCK deactivates the MLCP by phosphorylating MYPT1, or directly phosphorylates the MLC2, promoting the contraction of CCSMC. Additionally, the adenosine signaling pathway also has a role in the regulation of erectile function. In short, the short sleep duration might break the balance between the signaling pathways associated with penile erection and flaccidity, resulting in ED. Abbreviations: ED: Erectile dysfunction; HPA axis: Hypothalamic-pituitary-adrenal axis; ANS: Autonomic nervous system; SREs: Sleep-related erections; NPY: Neuropeptide Y; CCSMC: Corpus cavernosum smooth muscle cell; SMCs: smooth muscle cells; nNOS, Neural nitric oxide synthase; eNOS; Endothelial nitric oxide synthase; NO, Nitric oxide; NANC fibers: non-adrenergic non-cholinergic fibers; GC: Guanylyl cyclase; PKG: Protein kinase G; cGMP: Cyclic guanosine monophosphate; PDE: phosphodiesterase; NA: Noradrenaline; ET-1: Endothelin-1; Ang II: Angiotensin II; ADRa1: adrenergic receptor α- 1; RhoA: Ras homolog gene family member A; Rho-GEF: Rho guanosine exchange factor; ROCK: Rho-associated coiled-coil containing kinase; MLC: Myosin light chain; MLCP: Myosin light-chain phosphatase; MYPT1: Myosin phosphatase target subunit 1; MLC2: myosin light-chain 2; MLCK: Myosin light-chain kinase; CaM: Calmodulin; |
Autonomic Nervous System
The ANS imbalance as a potential risk factor for various diseases has been widely investigated.21 Short sleep duration is found to be involved changes in the ANS characterized by lower levels of parasympathetic tone and global sympathetic overactivity.82 Meanwhile, most data reveal that short sleepers are susceptible to have increased sympathetic activity, which could be carried into the daytime, as well as altered autonomic function following short sleep duration might result in serious repercussions for well-being and health condition.83,84 On the other hand, short sleep duration always co-occurs with the increased levels of circulating blood catecholamines, which might mediate some adverse effects of sleep disorders on erectile function.85,86 It is established that noradrenaline could regulate the influx of Ca2+ into smooth muscle cells and inhibits the penile erection via α-adrenergic receptors.87 Therefore, the autonomic imbalance towards sympathetic activity might take part in the association of short sleep with ED. However, the parasympathetic nervous system also plays an important role in regulation of erectile function, which seems to be under-researched in the context of autonomic dysregulation with excessive parasympathetic activity.
It is demonstrated that ED patients exhibit different heart rate variation (HRV) parameters compared with controls, suggesting that not only sympathetic but also general imbalance of the ANS might be an underlying cause of ED.88 Meanwhile, patients with some diseases that directly lead to collective autonomic dysfunction and neuropathy, such as primary autonomic failure and diabetes, are prone to ED.89 Sometimes autonomic imbalance is implicated in higher levels of both the parasympathetic and sympathetic system, which is inconsistent with the fact that sexual stimulation results in the penile tumescence through release of NO from parasympathetic cholinergic fibers.40 However, it should be noted that parasympathetic activity is different from the single effect of cholinergic transmitters, and other neurotransmitters may be co-released from nervous terminals.90 Actually, co-released transmitters from imbalanced global autonomic function might produce mixed effects on the regulation of erectile function, which might become a risk factor for ED. Given the regulation of ANS is under the control of the central nervous system, we hypothesized that putative pathways linking sleep disorders and ED might involve in the autonomic dysregulation with sympathetic or parasympathetic over-activity (Figure 1). Generally speaking, the evaluation of autonomic function, such as HRV analysis, can provide valuable information for the diagnosis of patients with both sleep disorders and ED.
Dopamine as the main catecholamine in the central nervous system is considered to be involved in sexual function.91 It is suggested that dopamine might participate in the somatic and autonomic regulation of penile erection, which has been illustrated through animal experiments.92 The involvement of dopamine in erectile function has been proven by previous studies in which penile erection could be induced using dopamine receptor agonists.93 Moreover, impaired dopaminergic neurons and dopamine D2 receptor signaling at the nucleus accumbens might result in the inhibition of erectile function and sexual arousal.94 In the periphery, however, the role of dopamine receptors in the regulation of erectile function is less certain, which still requires further research.
Sleep-Related Erection and Testosterone
Sleep-related erections (SREs) are undesirable penile erections that appear cyclically during REM sleep in normal healthy men from infancy to old age.95 SREs testing as a part of polysomnographic technique in sleep medicine has been used in the evaluation and classification of ED for a long time.96 Despite the well-researched mechanisms of REM sleep, the exact mechanism of SREs remains unclear. On the other hand, impaired SREs might be an indicator of some medical conditions at the early stage.95,97 In this regard, the impaired SREs have been observed in patients with diabetes, renal disease, hypertension, hypogonadism and some sleep disorders.98 Meanwhile, it is reported that SREs are diminished in those with major depressive disorders characterized by REM sleep alterations.98 Significantly, an abnormal extension of SREs, so-called sleep-related painful erection (SRPE), characterized by penile pain during REM sleep could cause sleep fragmentation or sleep deprivation, which is a rare and poorly recognized condition.99 However, the sleep-related painful erection seems to be a reason rather than a consequence of poor sleep. Together with these findings, we hypothesize that the short sleep duration might reduce the frequency of REM sleep and SREs. Furthermore, decreased SREs may lead to the insufficiency of arterial inflow, and the accumulation of metabolite in erectile tissue, which induces the hypoxemic and acidotic damage of cavernosum, and subsequently impairs the erectile function.
It has been established that androgens, especially testosterone, could influence erectile function via both central and peripheral effects, especially in the maintenance of libido.100 Reduced levels of testosterone in males always lead to a decline in sexual interest and erectile function, while administration of testosterone recovers libido and sexual activity in hypogonadal males.101 Meanwhile, testosterone as an important factor associated with SREs has been investigated in male sexual function.102 It is demonstrated that reduced levels of androgen via administration of luteinizing-hormone releasing-hormone agonists in young adult males do not eliminate but adversely affect the SREs, and the cessation of testosterone replacement in hypogonadal males triggers the similar descending of SREs measurements.102,103 Moreover, sleep restriction and sleep fragmentation are associated with lower levels of testosterone, which might be explained by the fact that the major secretion of daily testosterone in males appears in sleep.86,104 Thus, it is reasonable to assume that short sleep can directly reduce SREs, not just because of disturbed REM sleep, but also because of decreased testosterone levels. Taken together, we speculate that reduced testosterone and impaired SREs might be also involved in the connection between short sleep and ED (Figure 1).
Possible Molecular Mechanisms Between Short Sleep Duration and ED
Endothelial Dysfunction
Current evidence suggests that short sleep duration might be implicated with the risk of cardiovascular diseases, and sufficient sleep duration has the role of protection for cardiovascular health.105 Previous studies based on animal models have manifested the consistent results that sleep deprivation is involved in deteriorated cardiovascular function.106,107 Meanwhile, several factors are associated with the maintenance of vascular homeostasis, including NO, ET-1 and angiotensin signaling, which are also important for erectile function. It is demonstrated that sleep deprivation could induce endothelial dysfunction, increased blood pressure and oxidative stress in experimental models.108 Meanwhile, it is reported that sleep deprivation led to impaired erectile dysfunction in rats through down-regulation of NO/cGMP signaling, which was abolished by supplementation of glutamine.109
In humans, short sleep duration damages the endothelial function through diminishing NO bioavailability and inhibiting the NO-cGMP pathway, which is measured by a reduction in forearm blood flow.110,111 Similarly, the total sleep deprivation seems to drive an attenuation in endothelial-dependent vasodilation, and this endothelial dysfunction is dependent on altered NO signaling and independent of sympathetic signaling.112 However, ED patients with some psychiatric disorders characterized by short sleep duration, such as major depression disorders or post-trauma stress disorders, always show poor response to PDE5I therapy.113,114 This inconsistency suggests that other signaling pathways may concurrently participate in the pathophysiology of ED in short sleepers.
It is reported that adults with short sleep duration may have higher levels of ET-1 that is associated with increased vascular tone and cardiovascular risk.115 On the contrary, non-pharmacological interventions, such as regular aerobic exercise, can reduce the levels of ET-1 and improve endothelial vasodilation in subjects with habitual insufficient sleep.116 Meanwhile, the circadian of angiotensin (Ang)-converting enzyme (ACE) has been demonstrated in subjects with normal blood pressure and uncomplicated hypertension and could be modified through sleep deprivation.117,118 The circulatory Ang II and tissue angiotensin type-1 (AT1) receptor expression have revealed circadian rhythmicity, indicating the intimate links between sleep and renin-angiotensin-aldosterone system (RAAS).119 Interestingly, Ang II and ET-1 also are agonists in corpus cavernosum, activating the RhoA/ROCK signaling pathway that inhibits the penile erection. Furthermore, several inflammatory markers including intercellular adhesion molecule 1 (sICAM-1), interleukin-6 (IL-6), C-reactive protein (CRP) and TNF-α may mediate the association between sleep duration and endothelial function.120,121
As discussed above, endothelial dysfunction may be the probable pathway linking short sleep duration and ED (Figure 1 and 2); however, many factors are involved in endothelial homeostasis related to erectile function, highlighting a complex relationship between sleep duration and endothelial-dependent erection. Consequently, this may support the above-mentioned unsatisfactory treatment of PDE5I in patients with short sleep duration.
Inflammation
Inflammation is considered as an important mechanism connecting the sleep and the development of various conditions.122,123 Actually, there is a lot of evidence that poor sleep contributes to the increases of inflammatory markers.124,125 Among them, shorter sleep duration was reportedly associated with higher levels of CRP.124 Meanwhile, the sleep deprivation of a night might result in significantly increased monocyte production of IL-6 and TNF-α in the morning compared with normal sleep, which may be mediated by the nuclear factor kappa B (NF-κB) inflammatory signaling and hormone response pathways.126 Moreover, an increased level of interferon γ (IFN-γ) has been observed in real-life models after a night of sleep deprivation with unchanged levels of TNF-α, interleukin-2 (IL-2) and interleukin-10 (IL-10).127
Although inconsistent data on inflammatory markers after sleep deprivation are reported in previous studies, several markers, such as IL-6 and CRP, appear to have more consistent results.124,128 On the other hand, longitudinal analyses have indicated that effective intervention, such as recovery sleep, might decrease the levels of baseline inflammatory markers and health risk.129 In the clinical setting, the IL-6 and CRP have been shown to be associated with vascular risk and coronary heart disease.130,131 Meanwhile, IL-6 seems to mediate the vascular contraction through inhibiting the endothelium-dependent NO-cGMP pathway in animal models.132
In agreement with cardiovascular diseases, increased circulating levels of inflammatory cytokines are found to be associated with the presence and severity of ED.133 Similar findings have been reported in studies on the molecular mechanisms between chronic pelvic pain syndrome (CPPS) and ED. Rat models of CPPS via experimental autoimmune prostatitis seem to have higher levels of serum inflammatory compounds, including IL-6, CRP and TNF-α, and have reduced eNOS expression in corpus cavernosum and impaired erectile function.134 Furthermore, increased levels of IL-6 are found at 24 hours after the prostatectomy in clinical data, and the inhibition of IL-6 could attenuate ED in animal models of cavernous nerve dissection.135 Accordingly, the systemic inflammatory state might be a plausible explanation for the relationship between short sleep and ED (Figure 1 and 2). Given the crosstalk between inflammation and endothelial dysfunction, it might be necessary in order to incorporate the inflammatory markers into the diagnostic work-up of patients with ED who suffered sleep problems, in order to pursue essential benefits from treatment.
Adenosine
The neurotransmitter adenosine links neuronal activity, sleep, energy metabolism and penile erection.52,136 Adenosine signaling may be a common pathway for several sleep factors, and adenosine A1 receptor and adenosine A2A receptor are reportedly implicated in the regulation of sleep homeostasis through excitation of sleep active neurons.137 In this regard, central and systemic delivery of adenosine could provoke sleepiness, while caffeine serving as antagonists to both adenosine A1 and A2A receptors could counteract the sleepiness caused by adenosine signaling.137,138 Moreover, adenosine concentration significantly increases in the basal forebrain, which might be a central area associated with the facilitation of recovery sleep following prolonged wakefulness or sleep deprivation.136,139 Additionally, the up-regulation of adenosine A1 receptor in cortical and subcortical regions after sleep deprivation has been shown in vivo evidence, suggesting that short sleep could result in alteration of gene transcription associated with the homeostatic sleep regulation and even other cellular functions.140
Similar to NO, adenosine characterized by potent vasodilation and short half-life has been demonstrated to relax the cavernosal smooth muscles and subsequently promote the penile erection.141 Different cellular functions of adenosine receptors have been described. In all, adenosine receptors A1 and A3 coupling to adenylyl cyclase at the inhibitory G protein subunit (Gαi) serve to decrease the intracellular cAMP, and adenosine receptors A2A and A2B coupling to adenylyl cyclase at the G protein stimulatory subunit (Gαs) could increase the levels of intracellular cAMP.142 Previous studies have identified the distinct roles of adenosine receptors in cavernosal smooth muscles utilizing four adenosine receptors-deficient mice administrated by different dosages of adenosine.54 Among them, adenosine receptor A2B is required for adenosine signaling to induce penile erection, as well as adenosine receptor A1 is enriched on neurons and its downstream signaling appears to reduce the NE release and facilitate penile erection.143
Several stressful factors, such as hypoxia, could increase extracellular adenosine, which is paralleled to the effects of sleep deprivation on the central nervous system.144 Despite increased extracellular adenosine seems to be inconsistent with ED, it needs to be highlighted that the expression of adenosine receptors and adenosine deaminase (ADA) might play a major part in regulation of erectile function. Moreover, it is reported that the genetic variant of ADA might be correlated to reduced metabolism of adenosine during deep sleep.145 Thus, we hypothesized that short sleep may break the balance between adenosine metabolism and adenosine receptor signaling, leading to impaired erectile function (Figure 2). From another perspective, short sleep duration may result in cavernosal hypoxemia through decreasing arterial oxygen during sleep via disturbing the sleep-related erections, which might induce the accumulation of adenosine and lower the affinity of adenosine receptor A2B to adenosine. Eventually, downstream signaling related to penile erection is suppressed.
Wnt Proteins
In recent years, Wnt signaling pathway has become a fundamental growth control pathway, ranging from neoplasm to animal evolution. There are 19 Wnt genes in mammals, and mutated Wnt pathway components are thought to be implicated in various diseases.146 The Wnt signaling pathway is commonly classified into β-catenin dependent and β-catenin independent pathways, which have various downstream signaling pathways.147 Among them, RhoA/ROCK signaling plays a key role in β-catenin independent pathway and mediates pathophysiological mechanisms of several Wnt-related diseases, such as hypertension.148 In diabetic ED models, aberrant expression of Wnts in the corpus cavernosum has been identified, suggesting that Wnt signaling might contribute to the development of ED.149 Meanwhile, the inhibition of Wnt signaling via Dickkopf3 (DKK3) could improve the erectile function in diabetic models through restoring the cavernous vascular integrity and endothelial function.150 Hence, the Wnt pathway may represent a potential target in the management of ED.
It is reported that the disturbance of circadian rhythms could enhance the signaling of WNT/β-catenin pathway in autism spectrum disorder (ASD) characterized by sleep disorders.151 Meanwhile, Wnt signaling pathway has been shown to be associated with clock gene brain and muscle Arnt-like 1 (Bmal1) in regulation of adipocyte development.152 In gene set enrichment analysis, Wnt signaling pathways have been detected to be enriched in the distinctly methylated genes altered by total acute sleep deprivation in human subjects.153 In short, WNT/β-catenin pathway might be involved the connection between short sleep duration and ED, and the downstream unwanted effects on erectile function may be mediated by the RhoA/ROCK pathway (Figure 2).
Neuropeptide Y
Neuropeptide Y (NPY) consisting of 36 amino acids is co-released with noradrenaline (NA) from sympathetic nerve on electrical stimulation.154 Except for human and pig bone marrow, many organs have been found to express NPY, including heart, liver, adrenal gland and urogenital tracts.155,156 Among them, the adrenal medulla characterized by abundant sympathetic innervation is thought to be the major source of circulating NPY, which might be an important factor related to sleep regulation and homeostatic balance.156,157 It is reported that chronic sleep deprivation serving as a stressor significantly increases NPY expression in the hypothalamus, which might mediate the connection between sleep disorders and various diseases.158 Meanwhile, it is presumed that short sleep duration in humans might be associated with significant differential methylation in cytosine-phosphate-guanine (CpG) sites, and NPY appears to be related to the convergence arising in the pathways affecting sleep.159 Moreover, NPY has been shown to ameliorate the hyperdynamic circulation in cirrhotic animal models through splanchnic vasoconstriction by activating RhoA/ROCK signaling and inhibiting NO signaling.160
Actually, NPY localized with sympathetic perivascular nerve is also distributed in erectile tissues around helicine arteries with a high density.161 NPY has been found to have bidirectional effects on penile resistance arteries via different NPY receptors (Y-receptors), of which Y1/Y2-postsynaptic receptors are involved in the enhancement of noradrenaline vasoconstriction and Y2-presynaptic receptors associated with the inhibition of noradrenaline release.162 Meanwhile, Y1 receptor as a G protein-coupled receptor could strengthen the responses of small arteries to other vasoconstrictors through inhibiting the cAMP signaling and depolarizing the smooth muscles in arteries.163 Additionally, a recent study indicates that the production of NPY is under the control of the autonomic nervous in osteocyte.164 Thus, we believe that NPY signaling may intermediate the crosstalk between short sleep duration and ED, involving autonomic dysfunction and the RhoA/ROCK signaling pathway (Figure 1 and 2).
Summary
Sleep problems have prompted much public concern around the world. Short sleep duration as a central feature of sleep disorders is significantly associated with many diseases and health risks. Although the assumption that short sleep duration may impair erectile function has long existed, the underlying mechanisms are inconclusive and require further elucidation. Current data from clinical studies and animal models appear to support the crosstalk between sleep duration and penile erection. However, the causal link between short sleep and ED is not validated. This review summarized possible mechanisms linking short sleep duration and ED and provided clues for future investigations in this field. In short, we hypothesize that short sleep duration may be an independent risk factor of ED for certain subgroups. Meanwhile, neuroendocrine systems, various molecular mechanisms and signaling pathways may participate in the process of ED in patients with short sleep duration, and the improvement sleep quality and habits may be conducive to the treatment of ED. However, the negative influence of sleep disorders on erectile function is complicated, and the role of short sleep duration is just a part of it, which is a key limitation of this review.
In the future, a clear understanding of the molecular mechanisms linking short sleep duration and impaired erectile function will be required based on clinical and experimental studies. Among them, detailed knowledge of central transmitters involves both sleep duration and penile erection will be important. At the same time, it should be noted that current pharmacotherapy for ED may be ineffective in dealing with the underlying motivators that suppress erectile function in males. More importantly, short sleep duration as a risk factor appears to be potentially modifiable and curative compared to vascular and nervous lesion. Thus, we hold the opinion that the assessment of sleep quality should be incorporated into the diagnostic work-up of ED, and the treatment options for ED patients with short sleep duration should comprise not only the PDE5Is but also the measures for improvement of sleep quality.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Funding
This work was supported by the Natural Science Foundation of China (No. 81871147 and No. 82071639) and the Sichuan Science and Technology Program (No. 2022YFS0028 and No. 2022YFS0134).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown RE, Basheer R, McKenna JT., et al. Control of sleep and wakefulness. Physiol Rev. 2012;92(3):1087–1187.
2. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: final report. Sleep Health. 2015;1(4):233–243.
3. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394.
4. Tobaldini E, Fiorelli EM, Solbiati M, et al. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol. 2019;16(4):213–224.
5. Vgontzas AN, Fernandez-Mendoza J, Liao D, et al. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17(4):241–254.
6. Ren R, Covassin N, Yang L, et al. Objective but not subjective short sleep duration is associated with hypertension in obstructive sleep apnea. Hypertension. 2018;72(3):610–617.
7. St-Onge MP, Grandner MA, Brown D, et al. Sleep duration and quality: impact on lifestyle behaviors and cardiometabolic health: a scientific statement from the American Heart Association. Circulation. 2016;134(18):e367–e386.
8. Ai S, Zhang J, Zhao G, et al. Causal associations of short and long sleep durations with 12 cardiovascular diseases: linear and nonlinear Mendelian randomization analyses in UK Biobank. Eur Heart J. 2021;42(34):3349–3357.
9. Grandner MA, Patel NP, Gehrman PR, et al. Problems associated with short sleep: bridging the gap between laboratory and epidemiological studies. Sleep Med Rev. 2010;14(4):239–247.
10. de Zambotti M, Goldstone A, Colrain IM, et al. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24.
11. Smith L, Grabovac I, Veronese N, et al. Sleep quality, duration, and associated sexual function at older age: findings from the English longitudinal study of ageing. J Sex Med. 2019;16(3):427–433.
12. Yafi FA, Jenkins L, Albersen M, et al. Erectile dysfunction. Nat Rev Dis Primers. 2016;2:16003.
13. Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61.
14. Capogrosso P, Colicchia M, Ventimiglia E, et al. One patient out of four with newly diagnosed erectile dysfunction is a young man--worrisome picture from the everyday clinical practice. J Sex Med. 2013;10(7):1833–1841.
15. Papagiannopoulos D, Khare N, Nehra A. Evaluation of young men with organic erectile dysfunction. Asian J Androl. 2015;17(1):11–16.
16. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716.
17. Melehan KL, Hoyos CM, Hamilton GS, et al. Randomized trial of CPAP and vardenafil on erectile and arterial function in men with obstructive sleep apnea and erectile dysfunction. J Clin Endocrinol Metab. 2018;103(4):1601–1611.
18. Li Z, Fang Z, Xing N, et al. The effect of CPAP and PDE5i on erectile function in men with obstructive sleep apnea and erectile dysfunction: a systematic review and meta-analysis. Sleep Med Rev. 2019;48:101217.
19. Chen KF, Liang SJ, Lin CL, et al. Sleep disorders increase risk of subsequent erectile dysfunction in individuals without sleep apnea: a nationwide population-base cohort study. Sleep Med. 2016;17:64–68.
20. Deng N, Kohn TP, Lipshultz LI, et al. The relationship between shift work and men’s health. Sex Med Rev. 2018;6(3):446–456.
21. Irwin MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. 2019;19(11):702–715.
22. Matenchuk BA, Mandhane PJ, Kozyrskyj AL. Sleep, circadian rhythm, and gut microbiota. Sleep Med Rev. 2020;53:101340.
23. Fatima Y, Doi SAR, Al Mamun A. Sleep problems in adolescence and overweight/obesity in young adults: is there a causal link? Sleep Health. 2018;4(2):154–159.
24. Krueger JM, Frank MG, Wisor JP, et al. Sleep function: toward elucidating an enigma. Sleep Med Rev. 2016;28:46–54.
25. Irwin MR. Why sleep is important for health: a psychoneuroimmunology perspective. Annu Rev Psychol. 2015;66:143–172.
26. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev. 2019;99(3):1325–1380.
27. Scammell TE, Arrigoni E, Lipton JO. Neural circuitry of wakefulness and sleep. Neuron. 2017;93(4):747–765.
28. Marcheva B, Ramsey KM, Peek CB, et al. Circadian clocks and metabolism. Handb Exp Pharmacol. 2013;217:127–155.
29. Nollet M, Wisden W, Franks NP. Sleep deprivation and stress: a reciprocal relationship. Interface Focus. 2020;10(3):20190092.
30. Riemann D, Spiegelhalder K, Feige B, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev. 2010;14(1):19–31.
31. Tobaldini E, Costantino G, Solbiati M, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci Biobehav Rev. 2017;74(Pt B):321–329.
32. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1:15026.
33. Liyanarachchi K, Ross R, Debono M. Human studies on hypothalamo-pituitary-adrenal (HPA) axis. Best Pract Res Clin Endocrinol Metab. 2017;31(5):459–473.
34. Schüssler P, Uhr M, Ising M, et al. Nocturnal ghrelin, ACTH, GH and cortisol secretion after sleep deprivation in humans. Psychoneuroendocrinology. 2006;31(8):915–923.
35. Szentirmai É, Kapás L. Sleep and body temperature in TNFα knockout mice: the effects of sleep deprivation, β3-AR stimulation and exogenous TNFα. Brain Behav Immun. 2019;81:260–271.
36. Mishra I, Pullum KB, Thayer DC, et al. Chemical sympathectomy reduces peripheral inflammatory responses to acute and chronic sleep fragmentation. Am J Physiol Regul Integr Comp Physiol. 2020;318(4):R781–R789.
37. Calandra-Buonaura G, Provini F, Guaraldi P, et al. Cardiovascular autonomic dysfunctions and sleep disorders. Sleep Med Rev. 2016;26:43–56.
38. Palma JA, Benarroch EE. Neural control of the heart: recent concepts and clinical correlations. Neurology. 2014;83(3):261–271.
39. Thosar SS, Butler MP, Shea SA. Role of the circadian system in cardiovascular disease. J Clin Invest. 2018;28(6):2157–2167.
40. Farina B, Dittoni S, Colicchio S, et al. Heart rate and heart rate variability modification in chronic insomnia patients. Behav Sleep Med. 2014;12(4):290–306.
41. Hsieh CG, Martin JL. Short sleep, insomnia, and cardiovascular disease. Curr Sleep Med Rep. 2019;5(4):234–242.
42. Giuliano F, Rampin O. Neural control of erection. Physiol Behav. 2004;83(2):189–201.
43. Küthe A, Wiedenroth A, Mägert HJ, et al. Expression of different phosphodiesterase genes in human cavernous smooth muscle. J Urol. 2001;165(1):280–283.
44. Yuan J, Zhang R, Yang Z, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. Eur Urol. 2013;63(5):902–912.
45. Sopko NA, Hannan JL, Bivalacqua TJ. Understanding and targeting the Rho kinase pathway in erectile dysfunction. Nat Rev Urol. 2014;11(11):622–628.
46. Kimura K, Ito M, Amano M, et al. Regulation of myosin phosphatase by Rho and Rho-associated kinase (Rho-kinase). Science. 1996;273(5272):245–248.
47. Chitaley K, Wingard CJ, Clinton Webb R, et al. Antagonism of Rho-kinase stimulates rat penile erection via a nitric oxide-independent pathway. Nat Med. 2001;7(1):119–122.
48. Musicki B, Burnett AL. eNOS function and dysfunction in the penis. Exp Biol Med. 2006;231(2):548.
49. Andersson KE. Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction. Pharmacol Rev. 2011;63(4):811–859.
50. Becker AJ, Uckert S, Stief CG, et al. Plasma levels of cavernous and systemic norepinephrine and epinephrine in men during different phases of penile erection. J Urol. 2000;164(2):573–577.
51. Villalba N, Stankevicius E, Garcia-Sacristán A, et al. Contribution of both Ca2+ entry and Ca2+ sensitization to the alpha1-adrenergic vasoconstriction of rat penile small arteries. Am J Physiol Heart Circ Physiol. 2007;292(2):H1157–1169.
52. Yuan J, Desouza R, Westney OL, et al. Insights of priapism mechanism and rationale treatment for recurrent priapism. Asian J Androl. 2008;10(1):88–101.
53. Borea PA, Gessi S, Merighi S, et al. Pharmacology of adenosine receptors: the state of the art. Physiol Rev. 2019;98(3):1591–1625.
54. Mi T, Abbasi S, Zhang H, et al. Excess adenosine in murine penile erectile tissues contributes to priapism via A2B adenosine receptor signaling. J Clin Invest. 2008;118(4):1491–1501.
55. Labazi H, Tilley SL, Ledent C, et al. Role of adenosine receptor(s) in the control of vascular tone in the mouse pudendal artery. J Pharmacol Exp Ther. 2016;365(3):673–680.
56. Ritchie R, Endothelins SM. erectile dysfunction. Pharmacol Res. 2011;63(6):496–501.
57. Matos G, Hirotsu C, Alvarenga TA, et al. The association between TNF-α and erectile dysfunction complaints. Andrology. 2013;1(6):872–878.
58. Short MA, Booth SA, Omar O, et al. The relationship between sleep duration and mood in adolescents: a systematic review and meta-analysis. Sleep Med Rev. 2020;52:101311.
59. Itani O, Jike M, Watanabe N, et al. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246–256.
60. Dashti HS, Scheer FA, Jacques PF, et al. Short sleep duration and dietary intake: epidemiologic evidence, mechanisms, and health implications. Adv Nutr. 2015;6(6):648–659.
61. Liu PY. A clinical perspective of sleep and andrological health: assessment, treatment considerations, and future research. J Clin Endocrinol Metab. 2019;104(10):4398–4417.
62. Kellesarian SV, Malignaggi VR, Feng C, et al. Association between obstructive sleep apnea and erectile dysfunction: a systematic review and meta-analysis. Int J Impot Res. 2018;30(3):129–140.
63. Kalejaiye O, Raheem AA, Moubasher A, et al. Sleep disorders in patients with erectile dysfunction. BJU Int. 2017;120(6):855–860.
64. Wright KP Jr, Bogan RK, Wyatt JK. Shift work and the assessment and management of shift work disorder (SWD). Sleep Med Rev. 2017;17(1):41–54.
65. Wickwire EM, Geiger-Brown J, Scharf SM, et al. Shift work and shift work sleep disorder: clinical and organizational perspectives. Chest. 2016;151(5):1156–1172.
66. Kecklund G, Axelsson J. Health consequences of shift work and insufficient sleep. BMJ. 2016;355:i5210.
67. Rodriguez KM, Kohn TP, Kohn JR, et al. Shift work sleep disorder and night shift work significantly impair erectile function. J Sex Med. 2020;17(9):1687–1693.
68. Astuszak AW, Moon YM, Scovell J, et al. Poor sleep quality predicts hypogonadal symptoms and sexual dysfunction in male nonstandard shift workers. Urology. 2017;102:121–125.
69. Wu X, Zhang Y, Zhang W, et al. The association between erectile dysfunction and sleep parameters: data from a prospective, controlled Cohort. J Sex Med. 2022;S1743-6095(22):1509.
70. Seehuus M, Pigeon W. The sleep and sex survey: relationships between sexual function and sleep. J Psychosom Res. 2018;112:59–65.
71. Le HH, Salas RME, Gamaldo A, et al. The utility and feasibility of assessing sleep disruption in a men’s health clinic using a mobile health platform device: a pilot study. Int J Clin Pract. 2018;72(1):68.
72. Xiong Y, Zhang FX, Zhang YC, et al. Genetically predicted insomnia causally increases the risk of erectile dysfunction. Asian J Androl. 2022;2022:5.
73. Keller J, Gomez R, Williams G, et al. HPA axis in major depression: cortisol, clinical symptomatology and genetic variation predict cognition. Mol Psychiatry. 2017;22(4):527–536.
74. Abell JG, Shipley MJ, Ferrie JE, et al. Recurrent short sleep, chronic insomnia symptoms and salivary cortisol: a 10-year follow-up in the Whitehall II study. Psychoneuroendocrinology. 2016;68:91–99.
75. Kumari M, Badrick E, Ferrie J, et al. Self-reported sleep duration and sleep disturbance are independently associated with cortisol secretion in the Whitehall II study. J Clin Endocrinol Metab. 2009;94(12):4801–4809.
76. von Treuer K, Norman TR, Armstrong SM. Overnight human plasma melatonin, cortisol, prolactin, TSH, under conditions of normal sleep, sleep deprivation, and sleep recovery. J Pineal Res. 1996;20(1):7–14.
77. Sgoifo A, Buwalda B, Roos M, et al. Effects of sleep deprivation on cardiac autonomic and pituitary-adrenocortical stress reactivity in rats. Psychoneuroendocrinology. 2006;31(2):197–208.
78. Yang S, Zhang L. Glucocorticoids and vascular reactivity. Curr Vasc Pharmacol. 2004;2(1):1–12.
79. Hizume T, Morikawa K, Takaki A, et al. Sustained elevation of serum cortisol level causes sensitization of coronary vasoconstricting responses in pigs in vivo: a possible link between stress and coronary vasospasm. Circ Res. 2006;1:548.
80. Darlington DN, Kaship K, Keil LC, et al. Vascular responsiveness in adrenalectomized rats with corticosterone replacement. Am J Physiol. 1089;256(5 Pt 2):H1274–81.
81. Kobori Y, Koh E, Sugimoto K, et al. The relationship of serum and salivary cortisol levels to male sexual dysfunction as measured by the International Index of Erectile Function. Int J Impot Res. 2009;21(4):207–212.
82. Castro-Diehl C, Diez Roux AV, Redline S, et al. Sleep duration and quality in relation to autonomic nervous system measures: the multi-ethnic study of atherosclerosis (Mesa). Sleep. 2016;39(11):1927–1940.
83. Meerlo P, Sgoifo A, Suchecki D. Restricted and disrupted sleep: effects on autonomic function, neuroendocrine stress systems and stress responsivity. Sleep Med Rev. 2008;12(3):197–210.
84. Jarrin DC, Ivers H, Lamy M, et al. Cardiovascular autonomic dysfunction in insomnia patients with objective short sleep duration. J Sleep Res. 2018;27(3):e12663.
85. Andersen ML, Martins PJ, D’Almeida V, et al. Endocrinological and catecholaminergic alterations during sleep deprivation and recovery in male rats. J Sleep Res. 2005;14(1):83–90.
86. Arnal PJ, Drogou C, Sauvet F, et al. Effect of sleep extension on the subsequent testosterone, cortisol and prolactin responses to total sleep deprivation and recovery. J Neuroendocrinol. 2016;28(2):98.
87. Cripps SM, Mattiske DM, Pask AJ. Erectile dysfunction in men on the rise: is there a link with endocrine disrupting chemicals? Sex Dev. 2021;15(1–3):187–212.
88. Lee JY, Joo KJ, Kim JT, et al. Heart rate variability in men with erectile dysfunction. Int Neurourol J. 2011;15(2):87–91.
89. Mendoza-Velásquez JJ, Flores-Vázquez JF, Barrón-Velázquez E, et al. Autonomic dysfunction in α-synucleinopathies. Front Neurol. 2019;10:363.
90. Andersson KE. The importance of the cholinergic system in neurourology. Eur Urol. 1998;34(Suppl 1):6–9.
91. Sachs BD. Contextual approaches to the physiology and classification of erectile function, erectile dysfunction, and sexual arousal. Neurosci Biobehav Rev. 2000;24(5):541–560.
92. Melis MR, Argiolas A. Central control of penile erection: a re-visitation of the role of oxytocin and its interaction with dopamine and glutamic acid in male rats. Neurosci Biobehav Rev. 2011;35(3):939–955.
93. Simonsen U, Comerma-Steffensen S, Andersson KE. Modulation of dopaminergic pathways to treat erectile dysfunction. Basic Clin Pharmacol Toxicol. 2016;119(Suppl 3):63–74.
94. Chen G, Yu D, Wu Y, et al. Dopamine D2 receptors in the nucleus accumbens modulate erectile function in a rat model of nonorganic erectile dysfunction. Andrology. 2022;10(4):808–817.
95. Hirshkowitz M, Schmidt MH. Sleep-related erections: clinical perspectives and neural mechanisms. Sleep Med Rev. 2005;9(4):311–329.
96. Zou Z, Lin H, Zhang Y, et al. The role of nocturnal penile tumescence and rigidity (NPTR) monitoring in the diagnosis of psychogenic erectile dysfunction: a review. Sex Med Rev. 2019;7(3):442–454.
97. Schmidt MH, Schmidt HS. Sleep-related erections: neural mechanisms and clinical significance. Curr Neurol Neurosci Rep. 2004;4(2):170–178.
98. Hirshkowitz M, Moore C. Sleep-related erectile activity. Neurol Clin. 1996;14(4):721–737.
99. Vreugdenhil S, Weidenaar AC, de Jong IJ, et al. Sleep-related painful erections: a meta-analysis on the pathophysiology and risks and benefits of medical treatments. J Sex Med. 2018;15(1):5–19.
100. Buvat J, Maggi M, Gooren L, et al. Endocrine aspects of male sexual dysfunctions. J Sex Med. 2010;7(4 Pt 2):1627–1656.
101. Traish AM, Goldstein I, Kim NN. Testosterone and erectile function: from basic research to a new clinical paradigm for managing men with androgen insufficiency and erectile dysfunction. Eur Urol. 2007;52(1):54–70.
102. Hirshkowitz M, Moore CA, O’Connor S, et al. Androgen and sleep-related erections. J Psychosom Res. 1997;42(6):541–546.
103. Cunningham GR, Hirshkowitz M, Korenman SG, et al. Testosterone replacement therapy and sleep-related erections in hypogonadal men. J Clin Endocrinol Metab. 1990;70(3):792–797.
104. Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2010;305(21):2173–2174.
105. Huang T, Mariani S, Redline S. Sleep irregularity and risk of cardiovascular events: the multi-ethnic study of atherosclerosis. J Am Coll Cardiol. 2020;75(9):991–999.
106. Cherubini JM, Cheng JL, Williams JS, et al. Sleep deprivation and endothelial function: reconciling seminal evidence with recent perspectives. Am J Physiol Heart Circ Physiol. 2021;320(1):H29–H35.
107. Plante GE. Sleep and vascular disorders. Metabolism. 2014;55(10 Suppl 2):S45–49.
108. Kröller-Schön S, Daiber A, Steven S, et al. Crucial role for Nox2 and sleep deprivation in aircraft noise-induced vascular and cerebral oxidative stress, inflammation, and gene regulation. Eur Heart J. 2018;39(38):3528–3539.
109. Hamed MA, Akhigbe TM, Akhigbe RE, et al. Glutamine restores testicular glutathione-dependent antioxidant defense and upregulates NO/cGMP signaling in sleep deprivation-induced reproductive dysfunction in rats. Biomed Pharmacother. 2022;148:112765.
110. Bain AR, Weil BR, Diehl KJ, et al. Insufficient sleep is associated with impaired nitric oxide-mediated endothelium-dependent vasodilation. Atherosclerosis. 2017;265:41–46.
111. Calvin AD, Covassin N, Kremers WK, et al. Experimental sleep restriction causes endothelial dysfunction in healthy humans. J Am Heart Assoc. 2014;3(6):e001143.
112. Sauvet F, Florence G, Van Beers P, et al. Total sleep deprivation alters endothelial function in rats: a nonsympathetic mechanism. Sleep. 2014;37(3):465–473.
113. Safarinejad MR, Kolahi AA, Ghaedi G. Safety and efficacy of sildenafil citrate in treating erectile dysfunction in patients with combat-related post-traumatic stress disorder: a double-blind, randomized and placebo-controlled study. BJU Int. 2009;104(3):376–383.
114. Nurnberg HG, Seidman SN, Gelenberg AJ, et al. Depression, antidepressant therapies, and erectile dysfunction: clinical trials of sildenafil citrate (Viagra) in treated and untreated patients with depression. Urology. 2002;60(2 Suppl 2):58–66.
115. Weil BR, Mestek ML, Westby CM, et al. Short sleep duration is associated with enhanced endothelin-1 vasoconstrictor tone. Can J Physiol Pharmacol. 2010;88(8):777–781.
116. Stockelman KA, Bain AR, Dow CA, et al. Regular aerobic exercise counteracts endothelial vasomotor dysfunction associated with insufficient sleep. Am J Physiol Heart Circ Physiol. 2021;320(3):H1080–H1088.
117. Smolensky MH, Hermida RC, Portaluppi F. Circadian mechanisms of 24-hour blood pressure regulation and patterning. Sleep Med Rev. 2017;33:4–16.
118. Visniauskas B, Oliveira V, Carmona AK, et al. Angiotensin I-converting enzyme (ACE) activity and expression in rat central nervous system after sleep deprivation. Biol Chem. 2011;392(6):547–553.
119. Li H, Sun NL, Wang J, et al. Circadian expression of clock genes and angiotensin II type 1 receptors in suprachiasmatic nuclei of sinoaortic-denervated rats. Acta Pharmacol Sin. 2007;28(4):484–492.
120. Dzierzewski JM, Song Y, Fung CH, et al. Self-reported sleep duration mitigates the association between inflammation and cognitive functioning in hospitalized older men. Front Psychol. 2015;6(1004). doi:10.3389/fpsyg.2015.01004
121. Hahn J, Günter M, Schuhmacher J, et al. Sleep enhances numbers and function of monocytes and improves bacterial infection outcome in mice. Brain Behav Immun. 2020;87:329–338.
122. Irwin MR, Vitiello MV. Implications of sleep disturbance and inflammation for Alzheimer’s disease dementia. Lancet Neurol. 2019;18(3):296–306.
123. Schloss MJ, Swirski FK, Nahrendorf M. Modifiable cardiovascular risk, hematopoiesis, and innate immunity. Circ Res. 2020;126(9):1242–1259.
124. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52.
125. Wright KP, Drake AL, Frey DJ, et al. Influence of sleep deprivation and circadian misalignment on cortisol, inflammatory markers, and cytokine balance. Brain Behav Immun. 2015;47:24–34.
126. Irwin MR, Wang M, Campomayor CO, et al. Sleep deprivation and activation of morning levels of cellular and genomic markers of inflammation. Arch Intern Med. 2006;166(16):1756–1762.
127. Tobaldini E, Cogliati C, Fiorelli EM, et al. One night on-call: sleep deprivation affects cardiac autonomic control and inflammation in physicians. Eur J Intern Med. 2013;24(7):664–670.
128. Vgontzas AN, Papanicolaou DA, Bixler EO, et al. Circadian interleukin-6 secretion and quantity and depth of sleep. J Clin Endocrinol Metab. 1999;84(8):2603–2607.
129. Dolsen MR, Harvey AG. IL-6, sTNF-R2, and CRP in the context of sleep, circadian preference, and health in adolescents with eveningness chronotype: cross-sectional and longitudinal treatment effects. Psychoneuroendocrinology. 2021;129:105241.
130. Ridker PM, Rane M. Interleukin-6 signaling and anti-interleukin-6 therapeutics in cardiovascular disease. Circ Res. 2021;128(11):1728–1746.
131. Kaptoge S, Di Angelantonio E; Emerging Risk Factors Collaboration. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–140.
132. Orshal JM, Khalil RA. Reduced endothelial NO-cGMP-mediated vascular relaxation and hypertension in IL-6-infused pregnant rats. Hypertension. 2004;43(2):434–444.
133. Vlachopoulos C, Rokkas K, Ioakeimidis N, et al. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: common links. Eur Urol. 2007;52(6):1590–1600.
134. Hu Y, Niu X, Wang G, et al. Chronic prostatitis/chronic pelvic pain syndrome impairs erectile function through increased endothelial dysfunction, oxidative stress, apoptosis, and corporal fibrosis in a rat model. Andrology. 2016;4(6):1209–1216.
135. Yamashita S, Kato R, Kobayashi K, et al. Inhibition of interleukin-6 attenuates erectile dysfunction in a rat model of nerve-sparing radical prostatectomy. J Sex Med. 2011;8(7):1957–1964.
136. Peng W, Wu Z, Song K, et al. Regulation of sleep homeostasis mediator adenosine by basal forebrain glutamatergic neurons. Science. 2020;369(6058):eabb0556.
137. Porkka-Heiskanen T, Kalinchuk AV. Adenosine, energy metabolism and sleep homeostasis. Sleep Med Rev. 2010;15(2):123–135.
138. Clark I, Landolt HP. Coffee, caffeine, and sleep: a systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev. 2017;1:70–78.
139. Basheer R, Strecker RE, Thakkar MM, et al. Adenosine and sleep-wake regulation. Prog Neurobiol. 2002;73(6):379–396.
140. Elmenhorst D, Meyer PT, Winz OH, et al. Sleep deprivation increases A1 adenosine receptor binding in the human brain: a positron emission tomography study. J Neurosci. 2007;27(9):2410–2415.
141. Wen J, Xia Y. Adenosine signaling: good or bad in erectile function? Arterioscler Thromb Vasc Biol. 2012;32(4):845–850.
142. Godinho RO, Duarte T, Pacini ES. New perspectives in signaling mediated by receptors coupled to stimulatory G protein: the emerging significance of cAMP efflux and extracellular cAMP-adenosine pathway. Front Pharmacol. 2015;6:58.
143. Ning C, Qi L, Wen J, et al. Excessive penile norepinephrine level underlies impaired erectile function in adenosine A1 receptor deficient mice. J Sex Med. 2012;9(10):2552.
144. Eltzschig HK, Carmeliet P. Hypoxia and inflammation. N Engl J Med. 2011;364(7):656–665.
145. Rétey JV, Adam M, Honegger E, et al. A functional genetic variation of adenosine deaminase affects the duration and intensity of deep sleep in humans. Proc Natl Acad Sci U S A. 2005;102(43):15676–15681.
146. Nusse R, Clevers H. Wnt/β-Catenin Signaling, Disease, and Emerging Therapeutic Modalities. Cell. 2017;169(6):985–999.
147. Niehrs C. The complex world of WNT receptor signalling. Nat Rev Mol Cell Biol. 2012;13(12):767–779.
148. Kawarazaki W, Mizuno R, Nishimoto M, et al. Salt causes aging-associated hypertension via vascular Wnt5a under Klotho deficiency. J Clin Invest. 2020;130(8):4152–4166.
149. Shin SH, Kim WJ, Choi MJ, et al. Aberrant expression of Wnt family contributes to the pathogenesis of diabetes-induced erectile dysfunction. Andrology. 2014;2(1):107–116.
150. Song KM, Kim WJ, Choi MJ, et al. Intracavernous delivery of Dickkopf3 gene or peptide rescues erectile function through enhanced cavernous angiogenesis in the diabetic mouse. Andrology. 2020;8(5):1387–1397.
151. Vallée A, Lecarpentier Y, Guillevin R, et al. The influence of circadian rhythms and aerobic glycolysis in autism spectrum disorder. Transl Psychiatry. 2020;10(1):400.
152. Guo B, Chatterjee S, Li L, et al. The clock gene, brain and muscle Arnt-like 1, regulates adipogenesis via Wnt signaling pathway. FASEB J. 2012;26(8):3453–3463.
153. Nilsson EK, Boström AE, Mwinyi J, et al. Epigenomics of total acute sleep deprivation in relation to genome-wide DNA methylation profiles and RNA expression. OMICS. 2016;20(6):334–342.
154. Lundberg JM, Rudehill A, Sollevi A, et al. Co-release of neuropeptide Y and noradrenaline from pig spleen in vivo: importance of subcellular storage, nerve impulse frequency and pattern, feedback regulation and resupply by axonal transport. Neuroscience. 1989;28(2):475–486.
155. Batterham RL, Cowley MA, Small CJ, et al. Gut hormone PYY(3-36) physiologically inhibits food intake. Nature. 2002;8(418):650–654.
156. Dyzma M, Boudjeltia KZ, Faraut B, et al. Neuropeptide Y and sleep. Sleep Med Rev. 2010;14(3):161–165.
157. Cavadas C, Silva AP, Mosimann F, et al. NPY regulates catecholamine secretion from human adrenal chromaffin cells. J Clin Endocrinol Metab. 2001;86(12):5956–5963.
158. Koban M, Le WW, Hoffman GE. Changes in hypothalamic corticotropin-releasing hormone, neuropeptide Y, and proopiomelanocortin gene expression during chronic rapid eye movement sleep deprivation of rats. Endocrinology. 2006;14(1):421–431.
159. Huang H, Zhu Y, Eliot MN, et al. Combining human epigenetics and sleep studies in Caenorhabditis elegans: a cross-species approach for finding conserved genes regulating sleep. Sleep. 2017;40(6):zsx063.
160. Moleda L, Trebicka J, Dietrich P, et al. Amelioration of portal hypertension and the hyperdynamic circulatory syndrome in cirrhotic rats by neuropeptide Y via pronounced splanchnic vasoaction. Gut. 2011;60(8):1122–1132.
161. Kirkeby HJ, Jørgensen JC, Ottesen B. Neuropeptide Y (NPY) in human penile corpus cavernosum tissue and circumflex veins--occurrence and in vitro effects. J Urol. 1991;145(3):605–609.
162. Prieto D. Physiological regulation of penile arteries and veins. Int J Impot Res. 2008;20(1):17–29.
163. Prieto D, Buus CL, Mulvany MJ, et al. Neuropeptide Y regulates intracellular calcium through different signalling pathways linked to a Y(1)-receptor in rat mesenteric small arteries. Br J Pharmacol. 2000;129(8):1689–1699.
164. Zhang Y, Chen CY, Liu YW, et al. Neuronal induction of bone-fat imbalance through osteocyte neuropeptide Y. Adv Sci. 2021;8(24):e2100808.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.