")
Back to Journals » Open Access Emergency Medicine » Volume 11
Shock index in the emergency department: utility and limitations
Authors Koch E, Lovett S, Nghiem T , Riggs RA, Rech MA
Received 25 May 2019
Accepted for publication 24 July 2019
Published 14 August 2019 Volume 2019:11 Pages 179—199
DOI https://doi.org/10.2147/OAEM.S178358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Erica Koch,1 Shannon Lovett,2 Trac Nghiem,2 Robert A Riggs,2 Megan A Rech2,3
1Stritch School of Medicine, Loyola University Chicago, Maywood, IL 60153, USA; 2Department of Emergency Medicine, Loyola University Medical Center, Maywood, IL 60153, USA; 3Department of Pharmacy, Loyola University Medical Center, Maywood, IL 60153, USA
Abstract: Shock index (SI) is defined as the heart rate (HR) divided by systolic blood pressure (SBP). It has been studied in patients either at risk of or experiencing shock from a variety of causes: trauma, hemorrhage, myocardial infarction, pulmonary embolism, sepsis, and ruptured ectopic pregnancy. While HR and SBP have traditionally been used to characterize shock in these patients, they often appear normal in the compensatory phase of shock and can be confounded by factors such as medications (eg, antihypertensives, beta-agonists). SI >1.0 has been widely found to predict increased risk of mortality and other markers of morbidity, such as need for massive transfusion protocol activation and admission to intensive care units. Recent research has aimed to study the use of SI in patients immediately on arrival to the emergency department (ED). In this review, we summarize the literature pertaining to use of SI across a variety of settings in the management of ED patients, in order to provide context for use of this measure in the triage and management of critically ill patients.
Keywords: shock index, emergency, trauma, hemorrhage, myocardial infarction, pulmonary embolism, sepsis, obstetrics, ectopic pregnancy, pediatrics
Introduction
Prediction tools and risk stratification algorithms play an important role in the evaluation and management of acutely ill and injured patients. In the compensatory phase of shock, vital signs are often initially within normal ranges. Shock index (SI), defined as the ratio of heart rate (HR) to systolic blood pressure (SBP), is one such measure that has been studied in multiple patient populations.1 First described in 1967, SI provided an approximation of hemodynamic status in addition to traditional vital signs.1 The normal range for this unitless measure is currently accepted as 0.5–0.7, though some evidence suggests that up to 0.9 is acceptable.2–5 Values approaching 1.0 are indicative of worsening hemodynamic status and shock.1 Elevation in SI has been correlated with reduced left ventricular end-diastolic pressure and circulatory volume, even when HR and SBP are within normal limits.5,6
In addition to SI, modified SI (MSI) [HR/mean arterial pressure (MAP)] and age SI (age × SI) have been proposed in continued efforts to improve the prognostic value (Table 1). MSI was developed to incorporate the MAP rather than only SBP, as DBP is also used to determine clinical severity of illness.7 Age × SI has been shown to be more indicative of mortality in geriatric patients.6 The pediatric adjusted shock index (SIPA) was developed for pediatric populations and has proven to be more reliable than the standard adult cutoffs.2,3,8 Despite these advances, there is no consensus on when, where, and if SI has a role in the emergency department (ED). The purpose of this review was to summarize and evaluate the role of SI in the ED in order to provide context for use of this measure in the triage and management of critically ill patients.
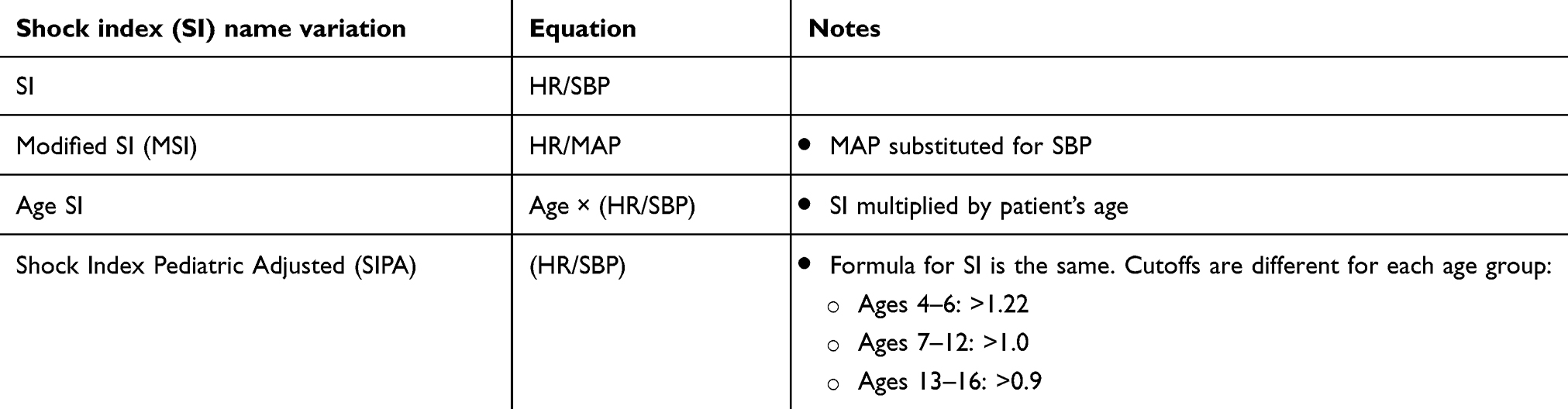 |
Table 1 Variations of shock index |
Methods
This review of therapeutics was undertaken to describe the utility of SI in emergency medicine. Articles were selected from PubMed using the following search terms: shock index in combination with trauma, hemorrhage, myocardial infarction, pulmonary embolism, sepsis, obstetrics, ectopic pregnancy, or pediatrics. Articles were reviewed for inclusion by at least two independent reviewers and selected for inclusion based on the consensus of the authors.
Triage
Traditionally, HR and SBP, among other vital signs, have been used to assess the hemodynamic status on arrival to the ED. However, these parameters can be normal, even in critically ill patients. This may lead to delayed intervention, increased need for intensive care, and morbidity and mortality.9,10 For example, patients with advanced age and chronic hypertension may not initially show signs of hemodynamic compromise, such as tachycardia and hypotension.11 Furthermore, hemorrhaging patients may have a HR and SBP within normal limits even after losing up to 450 mL of blood.12 Due to these findings, SI has been studied to identify a population at risk for decompensation and poor outcomes.
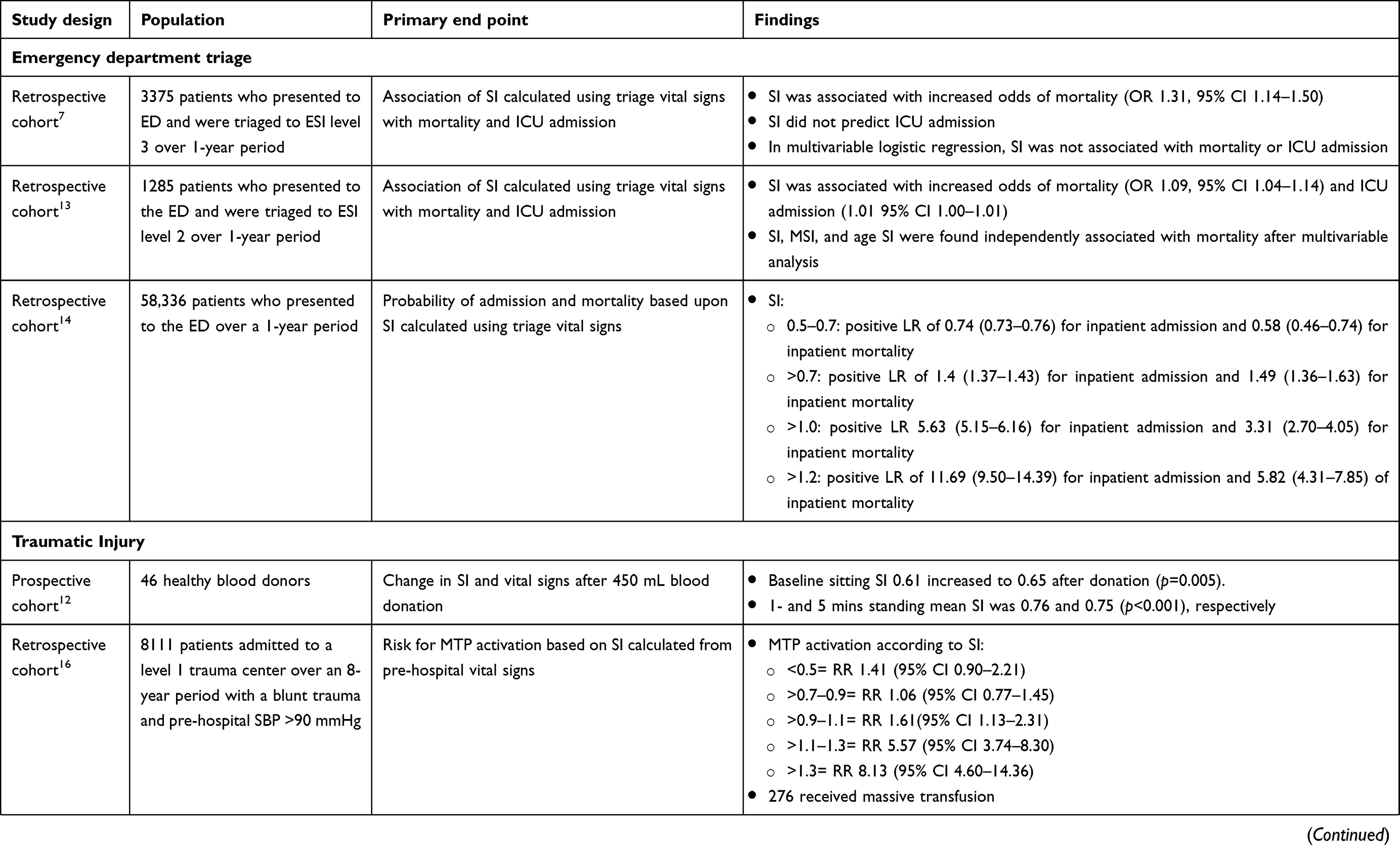
In a retrospective cohort of 1285 patients with an Emergency Severity Index (ESI) of 2 (corresponding to high risk), SI, MSI, and age SI were found to be better predictors of inpatient mortality than SBP (Table 2). However, these parameters were not predictive of intensive care unit (ICU) admission.13 A similar study included 3375 patients with ESI of 3 (stable vital signs but significant discomfort or sickness) found that all types of SI were associated with increased mortality, but only age SI predicted ICU admission.7 In an adjusted multivariable logistic regression analysis, male sex, SBP, and age SI were predictive of mortality. While this model did not account for multicollinearity, it demonstrates that age SI may be a useful tool to predict mortality. It should be noted that these two studies only included adult patients who were triaged for general medicine complaints; thus, these results may not be applicable to a surgical population.
 |
 |
 |
 |
 |
 |
 |  |
 |
 |
More recently, a retrospective cohort study included 58,336 adult ED encounters for any chief complaint over a 1-year period to determine the probability of admission and mortality based on the SI at presentation.14 SI values between 0.5 and 0.7 (normal) had the lowest likelihood of admission and inpatient mortality, whereas SI >1.2 conferred nearly 12 times more likelihood of being admitted compared to normal SI (Table 2).
As SI is calculated from data routinely collected in triage and can be incorporated automatically into the electronic medical record (EMR), it may help with resource allocation and patient flow. It can serve as another data point in addition to traditional vital signs. No prospective studies have examined the impact of triage SI on time to treatment, length of stay (LOS), and mortality.
Traumatic injury
SI has been studied most extensively in traumatic injury. Hemorrhagic shock (HS) is one of the leading causes of death during initial trauma treatment, and early recognition of shock can be challenging as normal vital signs may be present in the compensatory phase of shock.15 Over the last few decades, “late deaths”, such as that from sepsis or multi-organ failure, have decreased, while “early deaths”, such as that from HS, have remained constant.15 Much of the literature relating to SI in the ED is aimed at identifying a reliable and early tool for predicting HS, need for massive transfusion, and mortality (Table 2).
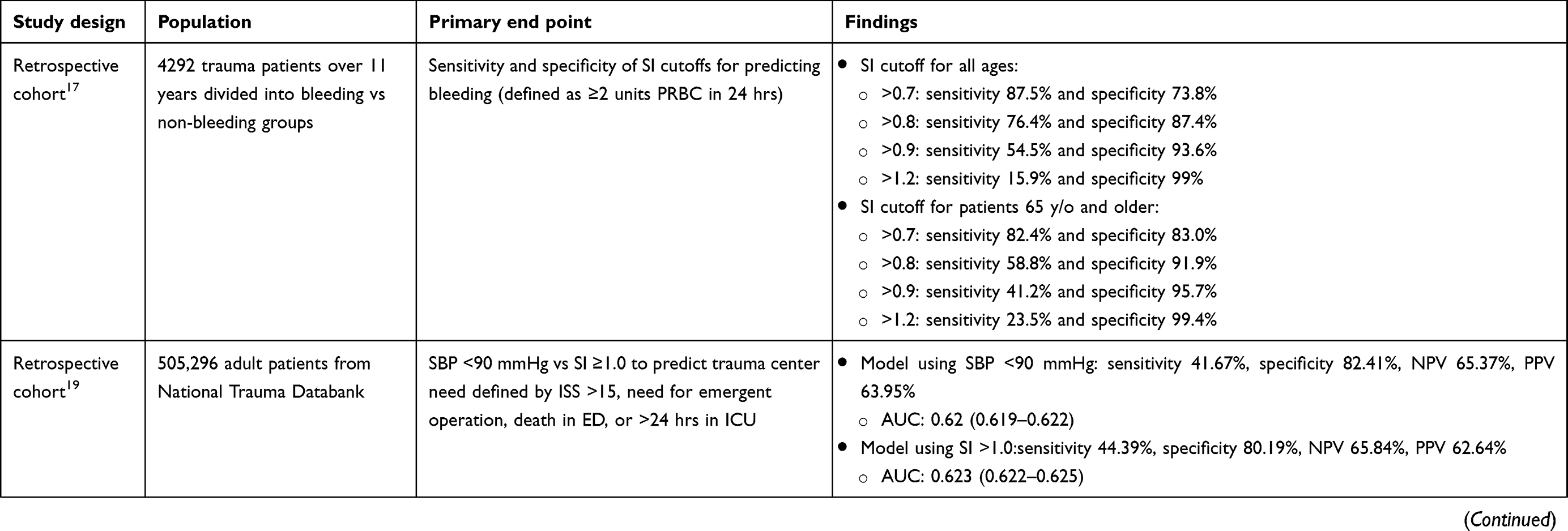
SI may be more valuable in predicting HS or bleeding requiring the activation of massive transfusion protocol (MTP) compared to traditional measures of HS such as tachycardia or hypotension.16 A prospective study in 46 healthy blood donors found that after 450 mL of blood loss, SI was persistently elevated at 1 and 5 mins, though HR and SBP were still within normal limits.12 A retrospective cohort study including 8111 patients with blunt trauma aimed to identify those at risk of requiring activation of the MTP despite relatively stable SBP (>90 mm Hg).16 In patients with SI >0.9, the risk of MTP rose substantially, despite being relatively normotensive. SI >0.9 has been the most commonly accepted value for predicting need for MTP, but more work is needed to further evaluate the best threshold, particularly in the geriatric population.17
The National Trauma Triage Protocol algorithm is comprised of four steps used to evaluate trauma patients in the field to determine treatment and transport needs.18 Step 1 involves evaluation of the following physiologic criteria that would mandate immediate transport to a trauma center: Glasgow Coma Scale <14, SBP <90 mm Hg, or respiratory rate <10 or >29 breaths per minute.18 A retrospective study of 505,296 patients substituted SI >1.0 instead of SBP <90 mm Hg to determine if SI lends additional benefit in identifying patients in need of referral to a trauma center.19 Trauma center need was defined according to the following: Injury Severity Score (ISS) ≥16 (corresponding to severe injury involving multiple systems with a chance of death >10%), need for emergent surgery, ICU LOS >24 hrs, or death in the ED.20 Substituting SI for SBP resulted in a significant reduction in under-triage rates without causing a large increase in over-triage, suggesting that SI may be more useful than SBP in determining where patients should be transferred. Future studies should evaluate longer-term outcomes like LOS beyond 24 hrs and mortality.6
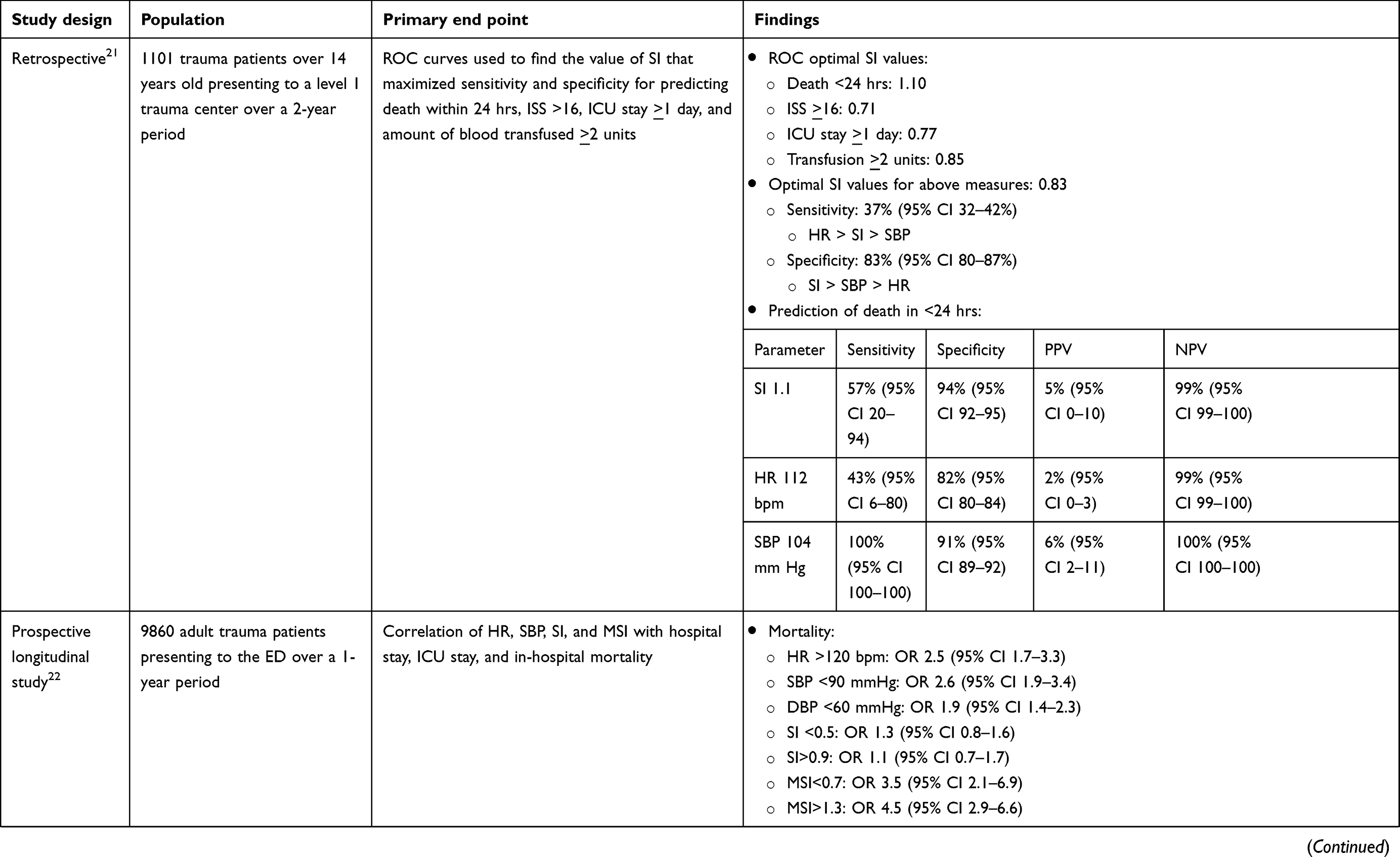
Other studies have yielded equivocal results when comparing SI to HR and BP indices.21,22 SI has been directly compared to HR and SBP in a retrospective cohort of 1101 trauma patients to predict severity measures.21 The severity measures included the following: death within 24 hrs, ISS ≥16, ICU LOS >24 hrs, and need for ≥2 units of blood. According to receiver operating curve characteristics, the optimal SI thresholds were as follows: ≥1.1 for death within 24 hrs, ≥0.71 for ISS ≥16, ≥0.77 for ICU stay ≥ 1 day, and ≥0.85 for transfusion ≥2 units. SI ≥0.83 was the best cutoff for predicting any of the severity measures.
A subsequent prospective longitudinal study of 9860 adult trauma patients compared the predictive value of SI and MSI for hospital mortality. MSI <0.7 and >1.3 had higher odds of mortality compared to HR, SBP, DBP, and SI.22 A low MSI is common in head injury patients or patients with significant hyperperfusion, whereas a high MSI is more suggestive of hypoperfusion. A retrospective study including 10,480 patients similarly found a bimodal relationship with SI and mortality; however, only high SI predicted mortality in trauma patients without head injury.
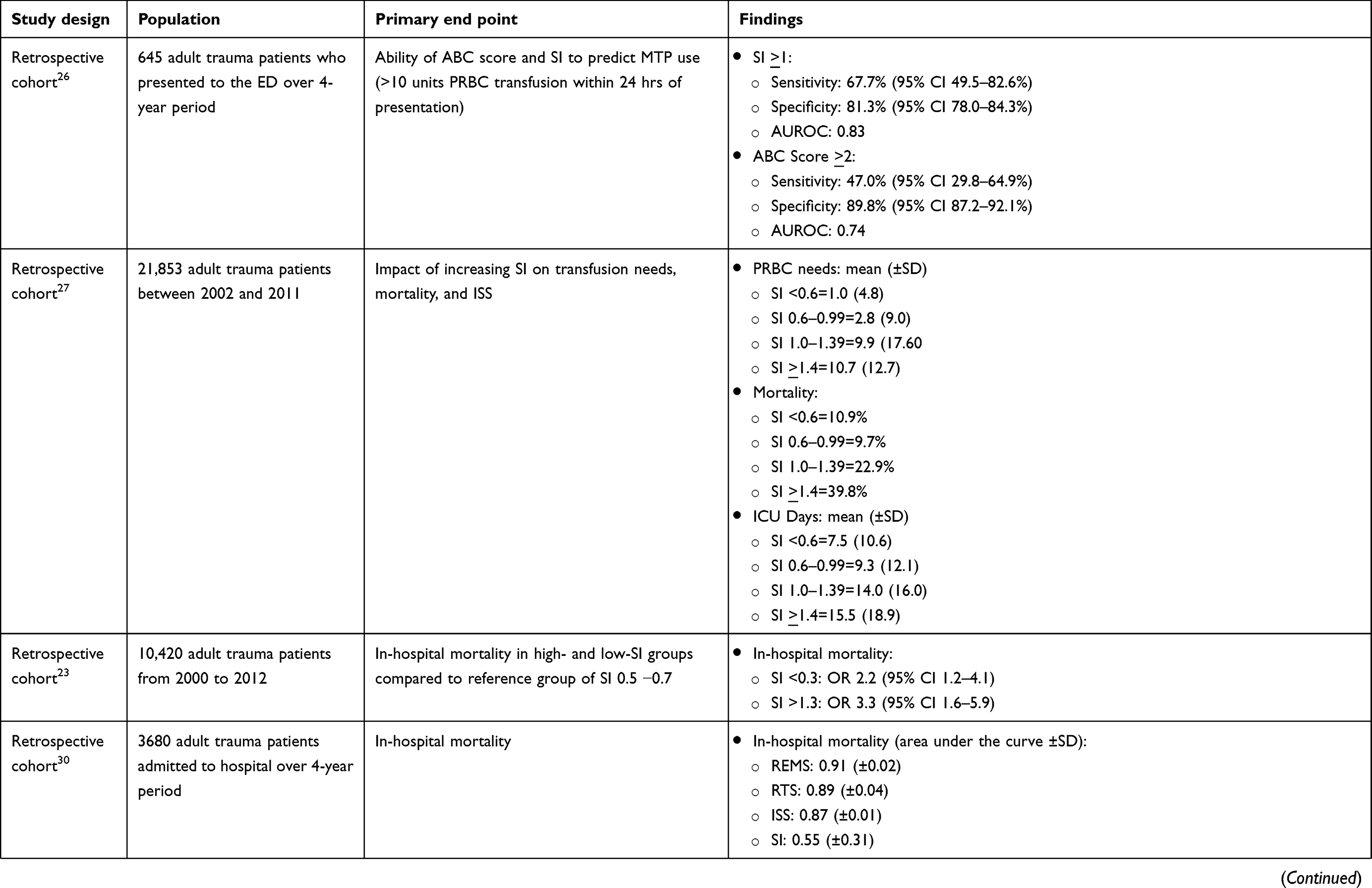
SI has been compared to other tools, including the Rapid Emergency Medicine Score (REMS). A retrospective cohort compared the discriminatory power of REMS, Revised Trauma Score (RTS), ISS, and SI. All of these scores except ISS allow for prompt calculation at the bedside, although SI is simplest and fastest. Although REMS was originally validated in nonsurgical patients, it performed similarly to RTS and superior to both ISS and SI in predicting mortality in trauma patients.23
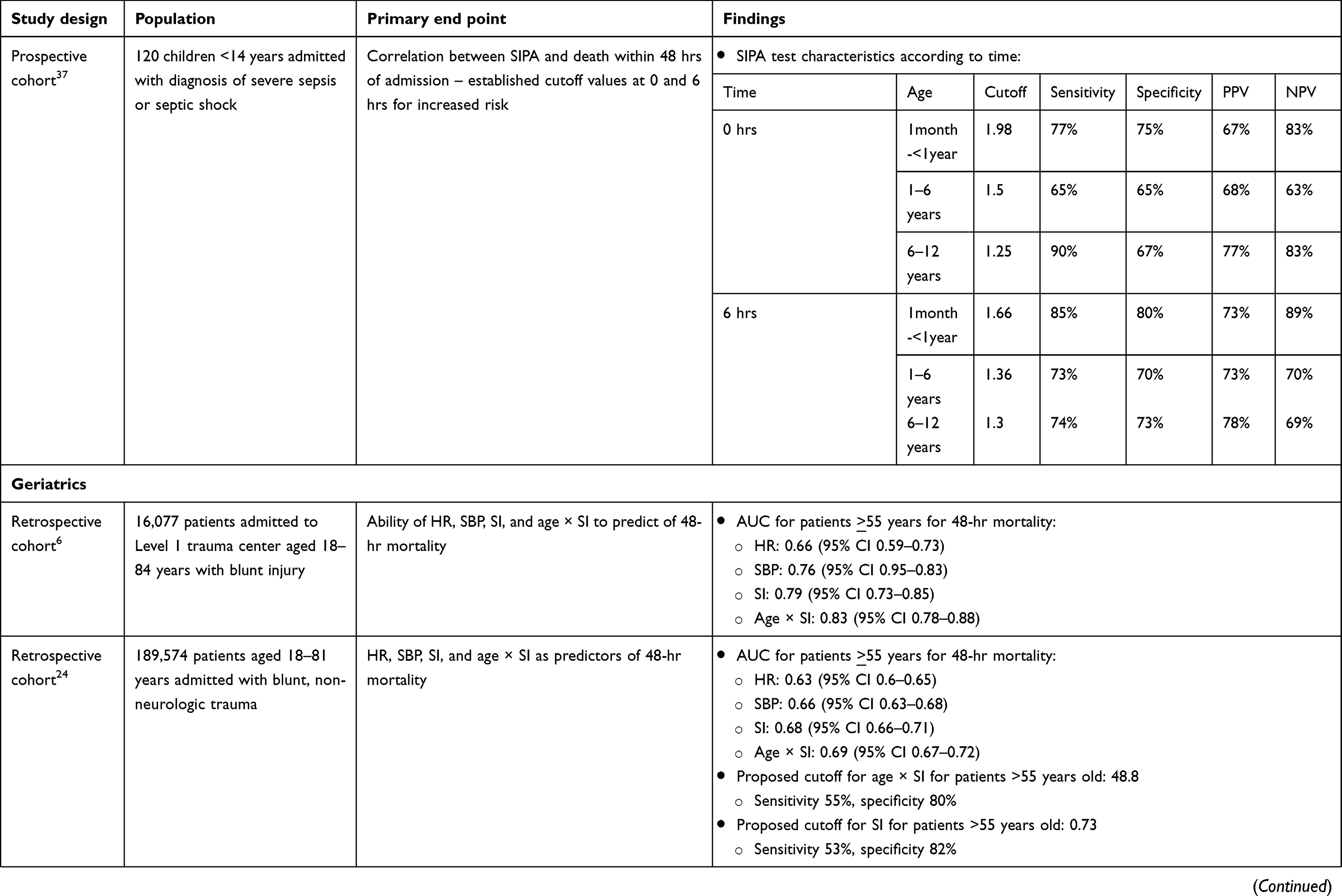
In a retrospective study of 16,077 patients, the predictive ability of HR, SBP, SI, and age × SI on 48-hr mortality in patients admitted to a level 1 trauma center with blunt injury was evaluated.6 In patients ≥55 years, SI and age SI were 0.79 (95% CI 0.73–0.85) and 0.83 (95% CI 0.78–0.88), respectively, p=0.0005. Both SI and age × SI performed better than HR and SBP alone. These findings were corroborated by similar studies.24,25
SI has also been used in comparison to the Assessment of Blood Consumption (ABC) score, which is comprised of the following: penetrating mechanism, ≤SBP of 90 mmHg, HR ≥120 bpm, and positive Focused Assessment with Sonography in Trauma exam.26 Presence of at least two criteria predicts activation of the MTP. SI was the strongest predictor followed by ABC score and had significantly greater sensitivity (p=0.04), but a significantly weaker specificity (p<0.001) compared to ABC score (Table 2). A similar study using the German Trauma Society registry found that SI was associated with increasing ISS, increased transfusion requirements, and increased mortality.27
SI has been used to predict mortality and MTP activation in trauma patients, especially values exceeding 1.0. Results comparing SI to HR and SBP in trauma patients are mixed, suggesting the need for further studies. Additional data are needed to determine if SI should be a component of the National Trauma Triage Protocol. MSI should also be further examined in trauma to determine if it is more efficacious than SI. It is unclear if any trauma centers are utilizing SI in real time and the implications thereof as all research to date in this population is retrospective. More prospective studies using SI in trauma and directly comparing SI to other predictive scores such as RTS and REMS are needed to determine if widespread utilization in trauma patients could improve outcomes.
Obstetrics
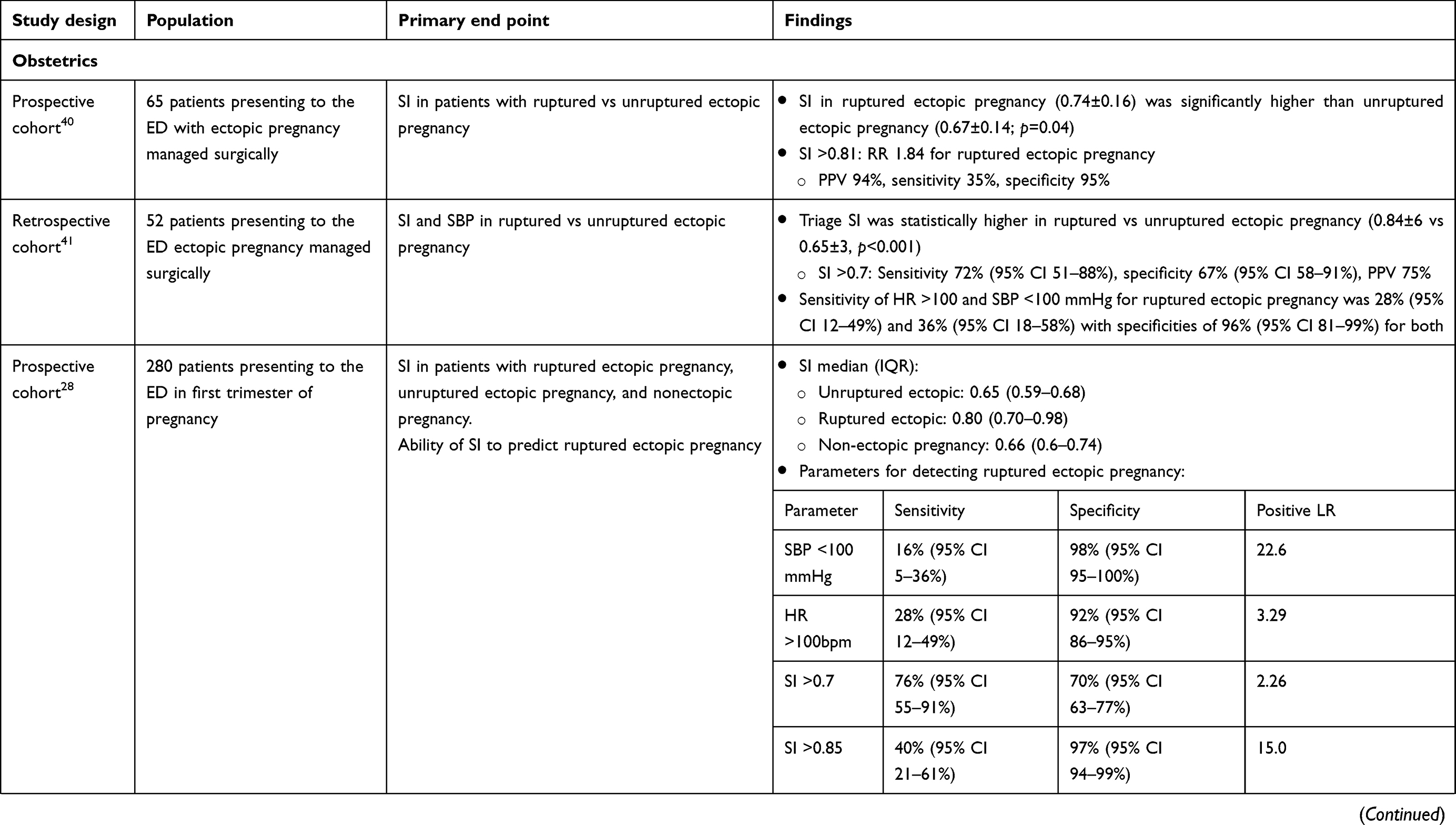
In an obstetric population, SI has been used in ectopic pregnancy as a diagnostic tool and predictor of rupture (Table 2). In a prospective cohort study of 65 ED patients who presented in need of surgical management for ectopic pregnancy, a significant difference in SI was observed between ruptured and unruptured pregnancies (0.74±0.16 vs 0.67±0.14, respectively; p=0.04); however, this absolute difference of 0.07 has questionable clinical relevance.27 Nevertheless, this study found that SI ≥0.81 corresponded with increased risk for ruptured ectopic pregnancy (Table 2). A retrospective case–control study of 52 patients found that patients with ruptured ectopic pregnancy had a significant elevation in triage HR and SI, but not SBP.28 Finally, a subsequent prospective cohort of 280 patients presenting to the ED in the first trimester of pregnancy determined the optimal cutoff for SI in the prediction of ruptured ectopic pregnancy (Table 2).28 An SI cutoff value of 0.7 had 76% sensitivity and 70% specificity in detecting ruptured ectopic pregnancy. Increasing this value to SI ≥0.85 lowered the sensitivity to 40% while increasing the specificity to 97%. Based on these results, marked elevation in SI (>0.85) may be useful for identifying patients at increased risk of ruptured ectopic pregnancy. Since SI appears more sensitive in this setting than HR or SBP, it may be useful as a screening tool. Considering its lack of specificity, transvaginal ultrasound remains the standard of care. Further prospective studies could examine the utility of SI in predicting which patients require immediate intervention through urgent obstetrics consultation and bedside ultrasound in preparation for emergent surgical intervention.
Sepsis
Systemic Inflammatory Response (SIRS) criteria have traditionally been used to screen for sepsis in patients presenting to the ED.29 SIRS criteria were used to define sepsis until the 2016 Third International Consensus Definitions Task Force changed the definition to a life-threatening organ dysfunction due to a dysregulated host response to infection, as quantified by the use of Sequential Organ Failure Assessment (SOFA) and qSOFA (“quick” SOFA; ≥2 of the following: respiratory rate ≥22/minute, SBP ≤100 mm Hg or altered mentation) were recommended to identify sepsis in the hospital and ED settings, respectively.30,31 While SI has been investigated as an additional measure to identify patients meeting SIRS criteria in need of immediate intervention, it has not been compared or added to SOFA or qSOFA.
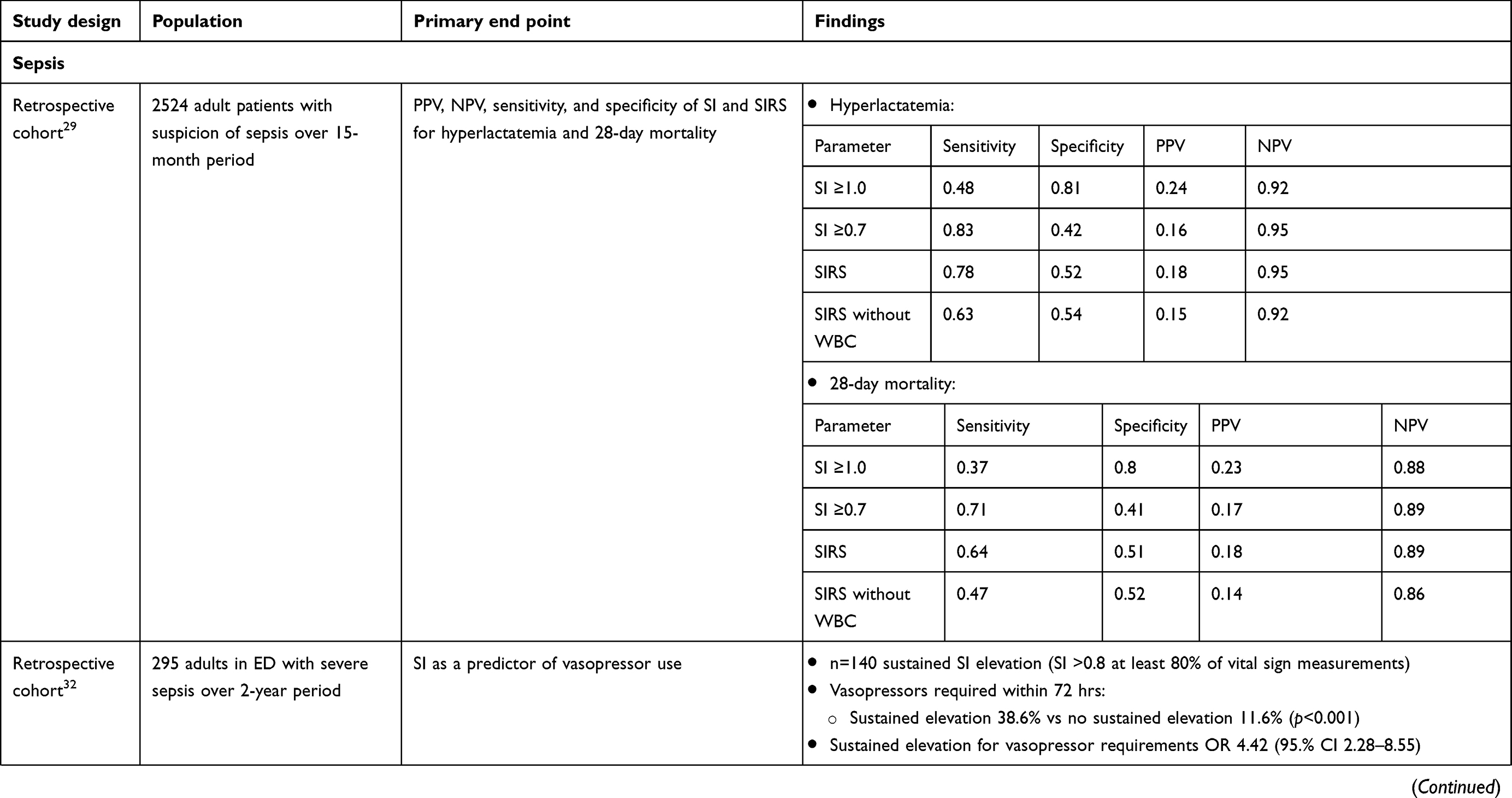
A retrospective cohort of 2524 adult patients compared SI with ≥2 SIRS criteria and modified SIRS (SIRS excluding white blood count) to predict serum lactate ≥4 mmol/L (Table 2).29 When the SI was >0.7, subjects had a 3 times higher likelihood of hyperlactatemia when compared to those with SI <0.7. Perhaps, the most useful finding from this study was that the negative predictive value (NPV) was 95% in patients with normal SI. Positive predictive value (PPV) was poor for predicting both hyperlactatemia and 28-day mortality for SI, SIRS, and modified SIRS. While it is unclear at this time how SI compares to SOFA or qSOFA as a predictor for the development of septic shock or outcomes like morbidity and mortality, it may prove useful at centers using SIRS-based assessments.
In 295 patients with severe sepsis, 38.6% of patients with sustained elevation in SI >0.8 for at least 80% of ED vital sign measurements required vasopressors within 72 hrs of admission, compared to only 11.6% of patients without a sustained elevation in SI.32 Instead of using a single SI value (ie triage of vital signs), this study assessed trends over time. SI used at a single time point at the initiation of sepsis care did not predict vasopressor use or mortality. Similar to other vital signs, trending SI over time using the EMS may identify patients at of septic shock.
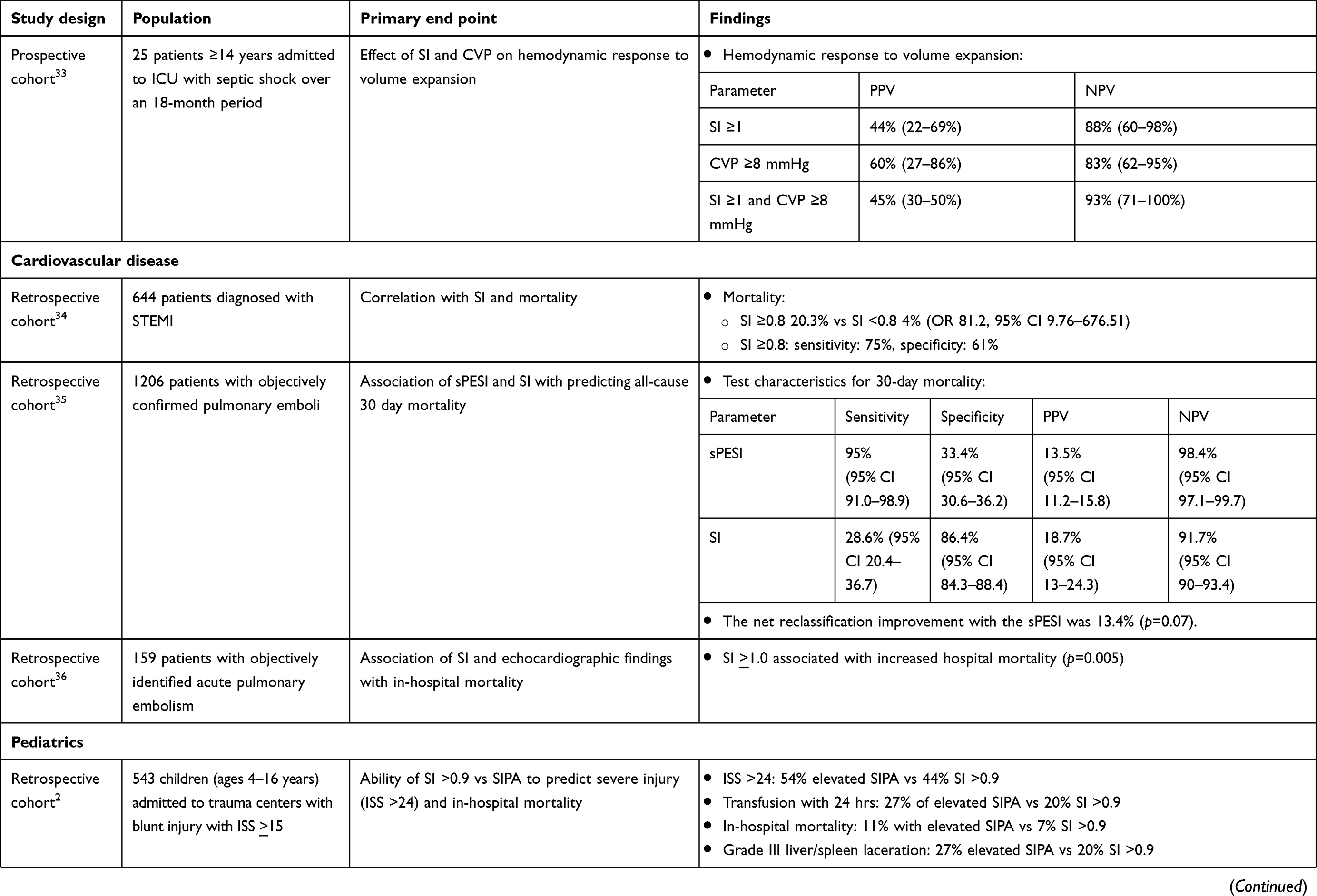
SI has also been evaluated in the context of predicting hemodynamic response to volume expansion. A prospective observational study of 25 patients with 34 volume expansions (10 mL/kg over <20 mins) with septic shock examined central venous pressure (CVP), SI, and volume responsiveness.33 The primary outcome was an increase of cardiac index (CI) measured by echocardiography of ≥15% after expansion. Patients with a CVP ≥8 mm Hg and SI ≤1 were unlikely to respond to volume expansion (13 nonresponders and 1 responder), with a NPV of 93% (95% CI 71–100%). Patients with an SI >1 were more likely to be fluid-responsive. This indicates that the combination of a high CVP and relatively low SI is better than either alone when assessing if a patient will respond to further fluid boluses, which may aid in avoiding fluid overload in critically ill patients.
While SI has been compared to SIRS for outcomes in sepsis, it is unclear how SI would compare to SOFA and qSOFA, which have improved test characteristics compared to SIRS. Furthermore, pairing the higher sensitivity of SIRS criteria with the improved specificity of SI >1 may yield a more accurate way to identify septic patients needing immediate intervention. It appears that SI >1 may be used to help guide fluid resuscitation and vasopressor use, though more studies are needed to determine populations that benefit most and specific cut points in SI that yield the best test characteristics.
Cardiovascular disease
SI has been used across a variety of cardiovascular disorders (Table 2). In a retrospective study including 644 consecutive acute ST elevation myocardial infarction (MI) patients, SI was evaluated as a marker for patients at risk for cardiogenic shock (N=96).34 SI ≥0.8 on admission to a percutaneous coronary intervention center was predictive of in-hospital mortality. Of those with SI ≥0.8, 20.3% died compared to 4% with SI <0.8. Though these findings are impressive, replication is needed to explore SI’s predictive ability in acute coronary syndromes.
A retrospective study of 1206 patients diagnosed with known or suspected PE compared the Simplified Pulmonary Embolism Severity Index (sPESI) and SI to predict 30-day mortality.35 The sPESI variables include age ≥80, history of cancer, chronic cardiopulmonary disease, HR >110 bpm, SBP <100 mmHg, and arterial oxygen saturation <90%.35 Presence of one or more variables deemed the patient high risk. The cutoff for high risk SI was 1. There were significantly more patients categorized as low risk via SI (85%) relative to low-risk sPESI (31%). More low-risk SI patients died compared to low-risk sPESI subjects (8.3% vs 1.6%). sPESI had better test characteristics compared to SI and thus SI cannot be reliably used to predict high-risk PE and mortality.
A similar retrospective study of 159 patients diagnosed with PE via spiral CT or high probability V/Q scanning found that an elevated SI ≥1, independent of echocardiogram findings for evidence of right ventricular dysfunction (ie RV hypokinesis/RV dilation/pulmonary hypertension), was associated with increased in-hospital mortality (p<0.05).36 Furthermore, the mortality rate for patients with moderate-to-severe RV hypokinesis was higher regardless of SI (p<0.05).
Though these studies are retrospective and limited in size, they suggest there may be a role for SI in the evaluation of patients presenting to the ED with cardiopulmonary disease. Prospective studies using a lower cutoff (perhaps 0.8) are needed to determine if a different SI threshold yields better test characteristics. More prospective studies overall are needed in the ED setting in patients with cardiopulmonary disease as initial retrospective data are promising that SI can be useful in predicting mortality.
Pediatrics
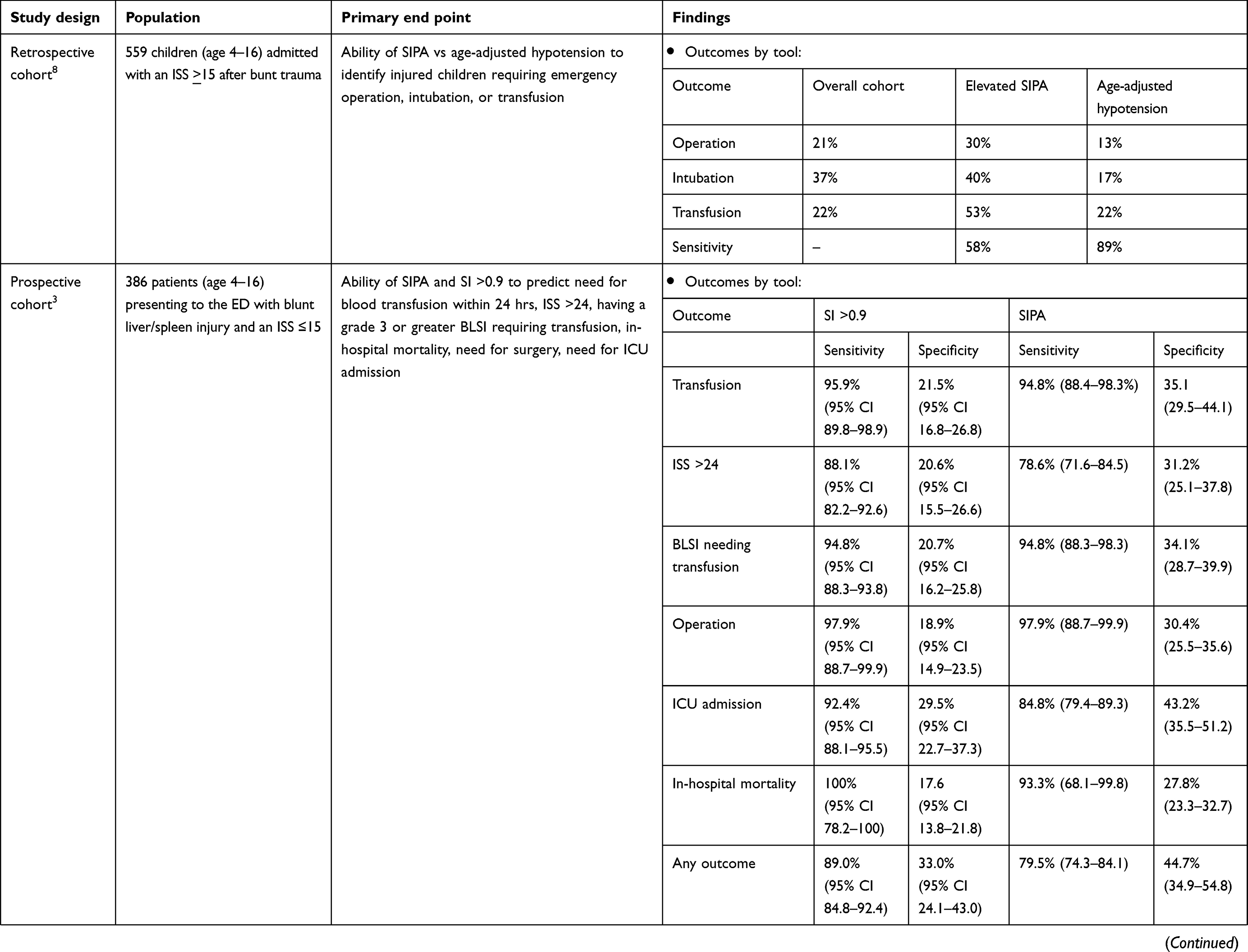
Pediatric physiology and reserves differ from adults. In addition, normal pediatric vital signs vary by age, which can greatly influence SI values. Age-adjusted SI has been proposed by multiple studies to identify and predict outcomes in ill children.2 Pediatric age-adjusted SI (SIPA) was defined by maximum normal HR and minimum normal SBP by age in a retrospective study of 543 children (Table 2).2–5,8,37 SIPA more accurately identified children who were severely injured and at risk for in-hospital mortality when compared to SI. Unfortunately, there were no further analyses comparing the sensitivity and specificity of SIPA vs SI >0.9. However, a higher percentage of patients with elevated SIPA were found to have ISS >24, in-hospital mortality, and blood transfusion in the first 24 hrs. These findings suggest that SIPA may be more specific than vital signs or SI alone at predicting these outcomes. In a subsequent study of 559 children ages 5–16, SIPA better predicted the need for operation, endotracheal intubation, and blood transfusion when compared to age-adjusted hypotension at presentation (SBP <90 mmHg in ages 4–6 and SBP <100 mmHg in ages 7–16).8
SIPA has since been validated in a prospective pediatric study of 386 patients in blunt liver and spleen injury (BLSI).3 Outcomes were blood transfusion in first 24 hrs, ISS >24, grade ≥3 BLSI requiring transfusion, need for operation, ICU admission, and in-hospital mortality. Sensitivity decreased slightly across all outcomes for SIPA compared to SI >0.9. However, specificity improved for all parameters for SIPA compared to SI. This could lead to less over-triage in the initial phase of resuscitation.
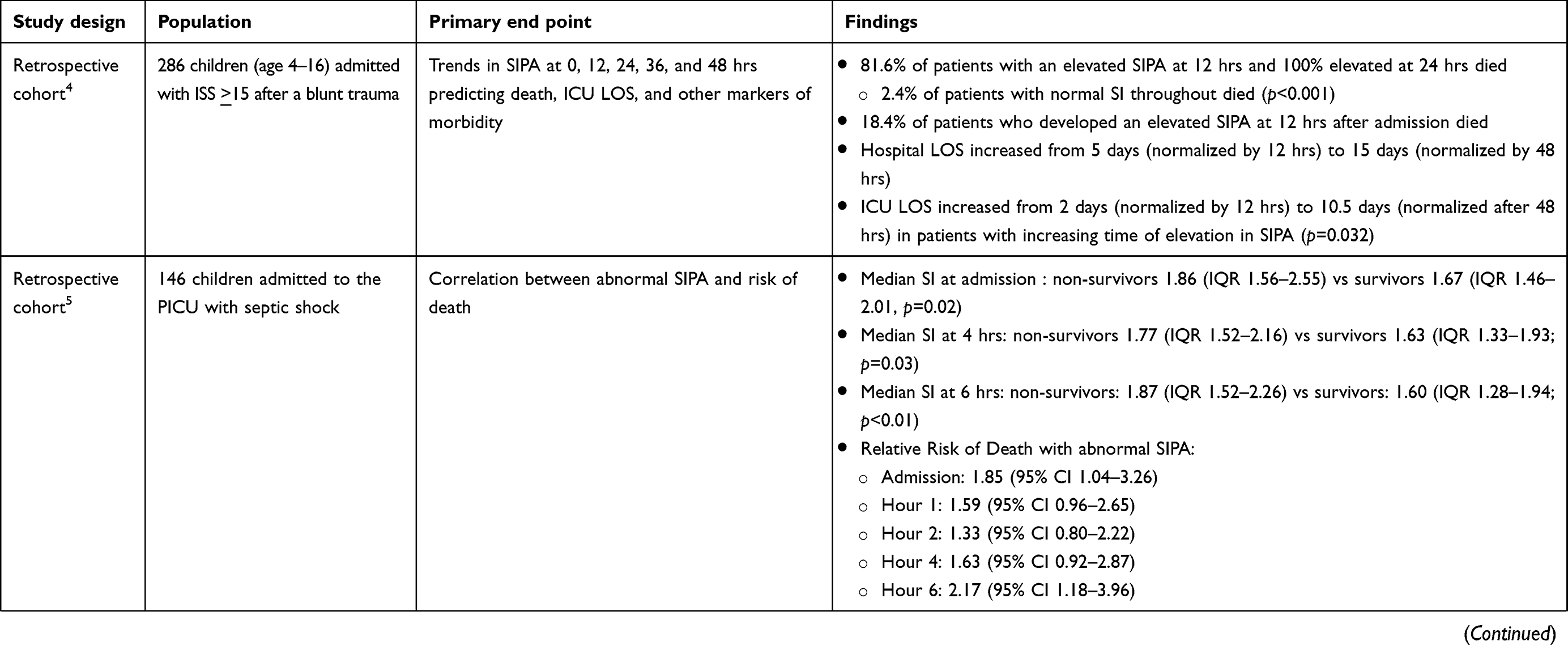
A retrospective study of 286 pediatric patients investigated the utility of trending SIPA after admission.4 Patients with a normal baseline SIPA that subsequently increased during the first 24 hrs of admission had an increased risk of mortality compared to those whose SIPA remained normal. Overall, 81.6% and 100% of patients with an abnormal SIPA after 12 and 24 hrs died. Similarly, time to normalize an elevated admission SIPA appeared to directly correlate with hospital LOS, ICU LOS, and other markers of morbidity. When time to normalize SIPA increased from 12 to 48 hrs, ICU LOS increased from 2 to 10 days, and hospital LOS increased from 5 to 15 days.
Finally, SIPA has also been used as a noninvasive marker of mortality risk in pediatric sepsis. A retrospective study of 146 children admitted to the pediatric ICU with septic shock showed that relative risk of mortality was higher in patients with persistently elevated SIPA if still elevated 6 h after admission.5 A prospective study of 120 children <14 years old concluded that SIPA cutoff values may identify children at high risk of early mortality in severe sepsis/septic shock.37 SIPA cutoff suggested upon arrival were 1.98 for 1 month to <1 year, 1.5 for 1–6 years, and 1.25 for 6–12 years. After 6 hrs, cutoffs were determined to be 1.66, 1.36, and 1.30, respectively.
These studies suggest that SIPA can be used in pediatric populations to assess patients at arrival, trend progress, and predict prognosis. However, prospective studies comparing SIPA to other resuscitative measures (eg, SBP, MAP, and lactate) are lacking. Additionally, there are no prospective studies incorporating SIPA with a treatment plan to determine if additional measures based on elevated SIPA can decrease mortality. To date, SIPA is not routinely accepted as standard practice in this population.
Geriatrics
As the population ages, more patients are diagnosed with chronic medical conditions, such as hypertension and diabetes. Although a normal SI is commonly considered 0.5–0.7, most studies did not take these confounding factors altering vital signs into account. In general, geriatric patients tend to have a slower HR response to physiologic stressors.11,38 Hypertension alters baseline SBP, and medications, such as beta-blockers and calcium channel blockers, may blunt the tachycardia in response to hypovolemia.11 Heart failure may limit the physiologic response to shock. In a retrospective cohort study of 111,019 patients, beta or calcium channel blocker usage, hypertension, diabetes, and age >65 were recorded to determine if these factors weakened the association between SI and prediction of mortality (Table 2).11 Patients >65 with an SI ≥1 had increased odds of 30-day mortality. Beta-blocker or calcium channel blocker use modified the odds of death. However, diabetes was not found to influence mortality. This study found that old age, hypertension, and beta-blocker or calcium channel blocker usage weaken the association between SI and mortality. However, SI >1 increased risk of 30-day mortality in all ED patients.
No study to date has examined SI in septic geriatric patients. One retrospective study including 409 patients ≥65 years with influenza found that SI ≥1 has a high specificity, NPV, and odds of 30-day mortality.39 Although promising as a marker for those at risk for increased mortality, more research needs to be done to gain a better understanding of the utility of the SI, and perhaps age × SI, in geriatric patients with infections.
For geriatric patients, SI and age × SI may have better discrimination for mortality and other outcomes compared to HR and SBP alone. However, prospective studies are needed to determine if basing interventions on these measures has a widespread impact. Both measures can be automatically calculated in the EMR and included with the vital signs in the triage analysis of the patient. This may present a challenge as medical history and medications may not be immediately available upon patient arrival to the ED as it appears that antihypertensive use may blunt the association between SI and mortality.
Limitations
While SI has proven useful in some settings, validation with prospective studies is limited. There is considerable heterogeneity across studies and disease states in terms of a specific threshold above which would be considered abnormal. Furthermore, utility of SI in the elderly, febrile patients, or those with chronic conditions that may alter baseline hemodynamics (eg, hypertension) may not have consistent changes in HR in response to hemodynamic stress. In addition, medications such as beta-blockers, beta-agonists, or other antihypertensives clearly affect vital signs and have been shown to alter the association of SI and mortality. Finally, there are many areas and populations that have yet to be studied, including burn injury and cardiogenic shock.
Conclusion
SI has been the subject of many studies in conditions including trauma, sepsis, ectopic pregnancy, MI, and pulmonary embolism (Table 3). As SI is based on factors immediately available on patient arrival, it can be automatically calculated in the EMR in triage in real time. Elevated SI (>0.7) has been shown to correlate with increased likelihood of inpatient admission, mortality, and other outcomes like MTP activation in trauma. Overall, SI carries poor sensitivity in predicting mortality. It should never be used to diagnose or rule out critical illness in isolation. Rather, it could be used in conjunction with vital signs and other markers in the clinical decision-making of patients at risk for outcomes like hospital or ICU admission, shock, and mortality.
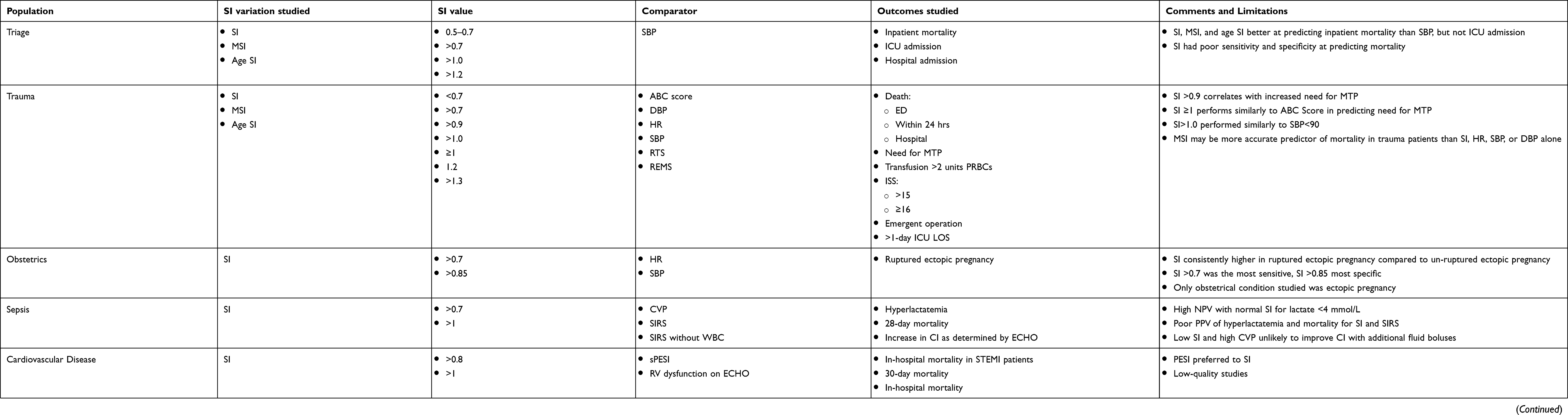 |
Table 3 Shock index summary |
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allgower M, Burri C. Shock index. Dtsch Med Wochenschr. 1967;92(43):1947–1950. doi:10.1055/s-0028-1106070
2. Acker SN, Ross JT, Partrick DA, Tong S, Bensard DD. Pediatric specific shock index accurately identifies severely injured children. J Pediatr Surg. 2015;50(2):331–334. doi:10.1016/j.jpedsurg.2014.08.009
3. Linnaus ME, Notrica DM, Langlais CS, et al. Prospective validation of the shock index pediatric-adjusted (SIPA) in blunt liver and spleen trauma: an ATOMAC+ study. J Pediatr Surg. 2017;52(2):340–344. doi:10.1016/j.jpedsurg.2016.09.060
4. Vandewalle RJ, Peceny JK, Dolejs SC, Raymond JL, Rouse TM. Trends in pediatric adjusted shock index predict morbidity and mortality in children with severe blunt injuries. J Pediatr Surg. 2018;53(2):362–366. doi:10.1016/j.jpedsurg.2017.10.045
5. Rousseaux J, Grandbastien B, Dorkenoo A, Lampin M, Leteurtre S, Leclerc F. Prognostic value of shock index in children with septic shock. Pediatr Emerg Care. 2013;29(10):1055–1059. doi:10.1097/PEC.0b013e3182a5c99c
6. Zarzaur BL, Croce MA, Fischer PE, Magnotti LJ, Fabian TC. New vitals after injury: shock index for the young and age × shock index for the old. J Surg Res. 2008;147(2):229–236. doi:10.1016/j.jss.2008.03.025
7. Torabi M, Moeinaddini S, Mirafzal A, Rastegari A, Sadeghkhani N. Shock index, modified shock index, and age shock index for prediction of mortality in emergency severity index level 3. Am J Emerg Med. 2016;34(11):2079–2083. doi:10.1016/j.ajem.2016.07.017
8. Acker SN, Bredbeck B, Partrick DA, Kulungowski AM, Barnett CC, Bensard DD. Shock index, pediatric age-adjusted (SIPA) is more accurate than age-adjusted hypotension for trauma team activation. Surgery. 2017;161(3):803–807. doi:10.1016/j.surg.2016.08.050
9. Shoemaker W. Relation of oxygen transport patterns to the pathophysiology and therapy of shock states. Intensive Care Med. 1987;13(4):230–243.
10. Shippy C, Appel P, Shoemaker W. Reliability of clinical monitoring to assess blood volume in critically ill patients. Crit Care Med. 1984;12(2):107–112. doi:10.1097/00003246-198402000-00005
11. Kristensen AKB, Holler JG, Hallas J, Lassen A, Shapiro NI. Is shock index a valid predictor of mortality in emergency department patients with hypertension, diabetes, high age, or receipt of β- or calcium channel blockers? Ann Emerg Med. 2016;67(1):106–113.e6. doi:10.1016/j.annemergmed.2015.05.020
12. Birkhahn RH, Gaeta TJ, Terry D, Bove JJ, Tloczkowski J. Shock index in diagnosing early acute hypovolemia. Am J Emerg Med. 2005;23(3):323–326.
13. Torabi M, Mirafzal A, Rastegari A, Sadeghkhani N. Association of triage time shock index, modified shock index, and age shock index with mortality in emergency severity index level 2 patients. Am J Emerg Med. 2016;34(1):63–68. doi:10.1016/j.ajem.2015.09.014
14. Balhara K, Hsieh Y, Hamade B, Circh R, Kelen G, Bayram J. Clinical metrics in emergency medicine: the shock index and the probability of hospital admission and inpatient mortality. Emerg Med J. 2017;34(2):89–94. doi:10.1136/emermed-2015-205532
15. Sobrino J, Shafi S. Timing and causes of death after injuries. Proc (Bayl Univ Med Cent). 2013;26(2):120–123. doi:10.1080/08998280.2013.11928934
16. Vandromme M, Griffin R, Kerby J, McGwin G, Rue L, Weinberg J. Identifying risk for massive transfusion in the relatively normotensive patient: utility of the prehospital shock index. J Trauma. 2011;70(2):384–388. doi:10.1097/TA.0b013e3182095a0a
17. DeMuro JP, Simmons S, Jax J, Gianelli SM. Application of the shock index to the prediction of need for hemostasis intervention. Am J Emerg Med. 2013;31(8):1260–1263. doi:10.1016/j.ajem.2013.05.027
18. Sasser S, Hunt R, Faul M, et al. Guidelines for field triage of injured patients: recommendations of the national expert panel on field triage, 2011. MMWR Recomm Rep. 2012;61(Rr–1):1–20.
19. Haider A, Azim A, Rhee P, et al. Substituting systolic blood pressure with shock index in the national trauma triage protocol. J Trauma Acute Care Surg. 2016;81(6):1136–1141. doi:10.1097/TA.0000000000001205
20. Palmer C. Major trauma and the injury severity score - where should we set the bar? Annu Proc Assoc Adv Automot Med. 2007;51:13–29.
21. King RW, Plewa MC, Buderer NMF, Knotts FB. Shock index as a marker for significant injury in trauma patients. Acad Emerg Med. 1996;3(11):1041–1045.
22. Singh A, Ali S, Agarwal A, Srivastava R. Correlation of shock index and modified shock index with the outcome of adult trauma patients: a prospective study of 9860 patients. North Am J Med Sci. 2014;6(9):450–452. doi:10.4103/1947-2714.141632
23. Odom S, Howell M, Gupta A, Silva G, Cook C, Talmor D. Extremes of shock index predicts death in trauma patients. J Emerg Trauma Shock. 2016;9(3):103–106. doi:10.4103/0974-2700.185272
24. Zarzaur BL, Croce MA, Magnotti LJ, Fabian TC. Identifying life-threatening shock in the older injured patient: an analysis of the national trauma data bank. J Trauma Acute Care Surg. 2010;68:5. doi:10.1097/TA.0b013e3181d87488
25. Kim S, Hong K, Shin S, et al. Validation of the shock index, modified shock index, and age shock index for predicting mortality of geriatric trauma patients in emergency departments. J Korean Med Sci. 2016;31(12):2026–2032. doi:10.3346/jkms.2016.31.12.2026
26. Schroll R, Swift D, Tatum D, et al. Accuracy of shock index versus ABC score to predict need for massive transfusion in trauma patients. Injury. 2018;49(1):15–19. doi:10.1016/j.injury.2017.09.015
27. Mutschler M, Nienaber U, Münzberg M, et al. The shock index revisited - a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU. Crit Care. 2013;17:4. doi:10.1186/cc12851
28. Birkhahn R, Gaeta T, Bei R, Bove J. Shock index in the first trimester of pregnancy and its relationship to ruptured ectopic pregnancy. Acad Emerg Med. 2002;9(2):115–119.
29. Berger T, Green J, Horeczko T, et al. Shock index and early recognition of sepsis in the emergency department: pilot study. West J Emerg Med. 2013;14(2):168–174. doi:10.5811/westjem.2012.8.11546
30. Imhoff BF, Thompson NJ, Hastings MA, Nazir N, Moncure M, Cannon CM. Rapid emergency medicine score (REMS) in the trauma population: a retrospective study. BMJ Open. 2014;4(5):e004738. doi:10.1136/bmjopen-2013-004738
31. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3)assessment of clinical criteria for SepsisAssessment of clinical criteria for sepsis. JAMA. 2016;315(8):762–774. doi:10.1001/jama.2016.0288
32. Wira C, Francis M, Bhat S, Ehrman R, Conner D, Siegel M. The shock index as a predictor of vasopressor use in emergency department patients with severe sepsis. West J Emerg Med. 2014;15(1):60–66. doi:10.5811/westjem.2013.7.18472
33. Lanspa MJ, Brown SM, Hirshberg EL, Jones JP, Grissom CK. Central venous pressure and shock index predict lack of hemodynamic response to volume expansion in septic shock: a prospective, observational study. J Crit Care. 2012;27(6):609–615. doi:10.1016/j.jcrc.2012.07.021
34. Bilkova D, Motovska Z, Widimsky P, Dvorak J, Lisa L, Budesinsky T. Shock index: a simple clinical parameter for quick mortality risk assessment in acute myocardial infarction. Can J Cardiol. 2011;27(6):739–742. doi:10.1016/j.cjca.2011.07.008
35. Sam A, Sánchez D, Gómez V, et al. The shock index and the simplified PESI for identification of low-risk patients with acute pulmonary embolism. Eur Respir J. 2011;37(4):762–766. doi:10.1183/09031936.00070110
36. Toosi MS, Merlino JD, Leeper KV. Prognostic value of the shock index along with transthoracic echocardiography in risk stratification of patients with acute pulmonary embolism. Am J Cardiol. 2008;101(5):700–705. doi:10.1016/j.amjcard.2007.10.038
37. Gupta S, Areesha A. Shock index-A useful noninvasive marker associated with age-specific early mortality in children with severe sepsis and septic shock: age-specific shock index cut-offs. J Intensive Care Med. 2018;088506661880277. (1525-1489 (Electronic); - 0885-0666 (Linking)):March 3, 2019. doi:10.1177/0885066618802779
38. McNab A, Burns B, Bhullar I, Chesire D, Kerwin A. An analysis of shock index as a correlate for outcomes in trauma by age group. Surgery. 2013;154(2):384–387. doi:10.1016/j.surg.2013.05.007
39. Chung J, Hsu C, Chen J, et al. Shock index predicted mortality in geriatric patients with influenza in the emergency department. Am J Emerg Med. 2019;37(3):391–394. doi:10.1016/j.ajem.2018.05.059
40. Jaramillo S, Barnhart KF, Takacs P. Use of the shock index to predict ruptured ectopic pregnancies. Int J Gynaecol Obstet. 2011;112(1):68. doi:10.1016/j.ijgo.2010.08.005
41. Birkhahn R, Gaeta T, Van Deusen S, Tloczkowski J. The ability of traditional vital signs and shock index to identify ruptured ectopic pregnancy. Am J Obstet Gynecol. 2003;189(5):1293–1296. doi:10.1067/s0002-9378(03)00663-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.