")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 13
Sex differences of in-hospital outcome and long-term mortality in patients with Takotsubo cardiomyopathy
Authors Weidner KJ, El-Battrawy I, Behnes M, Schramm K , Fastner C, Kuschyk J, Hoffmann U, Ansari U, Borggrefe M, Akin I
Received 6 January 2017
Accepted for publication 24 February 2017
Published 12 July 2017 Volume 2017:13 Pages 863—869
DOI https://doi.org/10.2147/TCRM.S131760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
KJ Weidner,1,* I El-Battrawy,1,2,* M Behnes,1 K Schramm,1 C Fastner,1,2 J Kuschyk,1 U Hoffmann,1,2 U Ansari,1 M Borggrefe,1,2 I Akin1,2
1First Department of Medicine, University Medical Centre Mannheim, Faculty of Medicine Mannheim, University of Heidelberg, 2DZHK (German Center for Cardiovascular Research), Partner Site, Heidelberg, Mannheim, Germany
*These authors contributed equally to this work
Background: Previous studies revealed that patients with Takotsubo cardiomyopathy (TTC) have a higher mortality rate than the general population. It is still unclear whether sex differences may influence long-term prognosis of TTC patients. The purpose of this study was to determine whether sex differences do influence the short- and long-term outcomes of TTC.
Methods and results: A total of 114 patients with TTC were admitted to the University Medical Centre Mannheim from January 2003 to September 2015 and entered into the TTC database of the University Medical Centre Mannheim, and retrospectively analyzed. Patients were diagnosed by the Mayo Clinic criteria. All-cause mortality over mean follow-up of 1,529±1,121 days was revealed. Significantly more male patients died within long-term follow-up compared to female TTC patients (log-rank test; P=0.01). Most males died of noncardiac causes. In multivariate Cox regression analysis, the male sex (P=0.02, hazard ratio [HR] 2.8, 95% CI 1.1–7.2), the ejection fraction ≤35% (P=0.01, HR 3.3, 95% CI 1.2–9.2) and glomerular filtration rate <60 mL/min (P<0.01, HR 3.1, 95% CI 1.4–7.0) figured out as independent predictors of the adverse outcome.
Conclusion: This study shows that males suffering from TTC reveal a higher long-term all-cause mortality rate than females over a 5 year follow-up period.
Keywords: Takotsubo cardiomyopathy, sex differences, outcome, mortality
Introduction
Takotsubo cardiomyopathy (TTC) is a reversible clinical condition mimicking an acute myocardial infarction (AMI).1 It consists of a transient left ventricular (LV) dysfunction being characterized by defined wall motion abnormalities in the absence of significant coronary artery stenosis.2 Even if there is no coronary artery stenosis, TTC may be associated with critical complications such as life-threatening arrhythmias, thromboembolic events, cardiac rupture and cardiogenic shock.2–6
The classification system of TTC is based on the ballooning pattern of ventricular walls, diagnosed by transthoracic echocardiography and laevocardiography.1 There are four different ballooning patterns: the apical form is the most common (81.75%), followed by the mid-ventricular form (14.6%) and the rare forms, such as the basal (2.2%) and focal (1.5%) patterns. In daily routine, TTC is a rarely diagnosed disease and its causes are still not understood completely.1,7–10 One of the most described reasons for the development of TTC may consist of emotional stress. Therefore, a link was attributed pathologically to the so-called brain–heart axis.11,12
As it is widely known, defined cardiovascular risk factors, such as patients’ age and sex, do exist influencing the occurrence and severity of many diseases.13 Specifically for the development of TTC, it was shown that most patients were postmenopausal women.14 Accordingly, most studies evaluating TTC patients focused on older female study populations. However, only a few scientific evidence is available about the differences in both sex distributions, ie, males and females, in patients with TTC.15 Murakami et al16 obtained clinical information of a multi-center database (Tokyo CCU Network). They observed 368 patients suffering from TTC during a follow-up of 3 years. They have shown that males seem to have more cardiac complications during hospitalization than females.16 Schneider et al15 reported about sex differences in the manifestation of TTC. A total of 296 female patients and 28 male patients were included. They presented a female predominance for developing a TTC but not a significant difference in the mortality between male and female patients.15–17 Brinjikji et al17 found that mortality was significantly higher in male patients with TTC during a follow-up of 1 year.16
In comparison to Murakami et al, Schneider et al and Brinjikji et al, we analyzed a database of 114 patients with a follow-up of 5 years to report about the all-cause mortality during this time in relation to sex.
Additionally, it is still unclear, whether sex differences may influence long-term prognosis of TTC patients with regard to all-cause mortality.
The purpose of this study was to investigate sex differences in prevalence and outcome of patients with TTC.
Methods
A total of 114 patients with TTC were admitted from January 2003 to September 2015 in the TTC database of our institution. Patients were diagnosed by the following Mayo Clinic criteria:18
- transient hypokinesis, akinesis or dyskinesis of the LV midsegment with or without apical involvement; the regional wall motion abnormalities extending beyond a single epicardial vascular distribution; a stressful trigger often but not always present;
- absence of obstructive coronary disease or angiographic evidence of acute plaque rupture;
- new electrocardiographic abnormalities (either ST-segment elevation and/or T-wave inversion) or modest elevation in cardiac troponin; and
- absence of pheochromocytoma or myocarditis.
The angiograms, echocardiograms and electrocardiograms (ECGs) were reviewed by two experienced independent cardiologists to evaluate the diagnosis of TTC. This retrospective study was conducted in compliance with the Declaration of Helsinki with regard to investigations in human subjects, and the study protocol was approved by the ethics committee of University Medical Centre Mannheim. A patient consent to review the medical records was not required.
In-hospital events, arrhythmias, cardiac rupture, thromboembolic events, pulmonary congestion with the use of non-invasive positive-pressure ventilation (NPPV), intubation, use of a temporary pacemaker, use of inotropic agents and in-hospital death were assessed based on chart review. All-cause mortality was revealed over a mean follow-up of 1,529±1,121 days as assessed by chart review and/or telephone review. If medical records, treating physicians or relatives were unable to provide further information concerning the circumstances of death, it was defined as death due to unknown case.
Blood sample collection
The peripheral venous or central venous blood of the probands was taken in sterile monovettes using the aspiration system.19,20 The monovettes contained EDTA, heparin and in the serum monovette a clot activating gel. All samples were analyzed immediately in the laboratory of the University Medical Centre Mannheim.
Statistics
Data are presented as mean ± standard deviation (SD) for continuous variables with a normal distribution, median (interquartile range) for continuous variables with a non-normal distribution or as frequency (%) for categorical variables. The Kolmogorov–Smirnov test was used to assess normal distribution. The Student’s t-test and the Mann–Whitney U test were used to compare continuous variables with normal and non-normal distributions, respectively. The chi-squared test or Fisher’s exact test was used to compare categorical variables. The log-rank test was used to compare the survival curves between female and male patients. Factors with P<0.10 on univariate analysis were entered into the Cox multivariate regression to define independent risk factors for the outcome. Statistical analysis was performed with IBM SPSS software in all analyses; P≤0.05 (two tailed) was considered to indicate statistical significance.
Results
Study population
Most patients were females (82%, n=93). A total of 114 patients being admitted to our hospital due to acute TTC were included in the present study. In all, 18 patients with uncertain TTC due to absence of coronary angiogram and/or follow-up echocardiogram were excluded. The baseline characteristics are shown in Table 1. The median age of all patients was 68 years (range 41–91 years). The mean duration of intermediate care unit (ICU) treatment was 4.43 days. All patients underwent coronary angiography and transthoracic echocardiography at the time of TTC development.
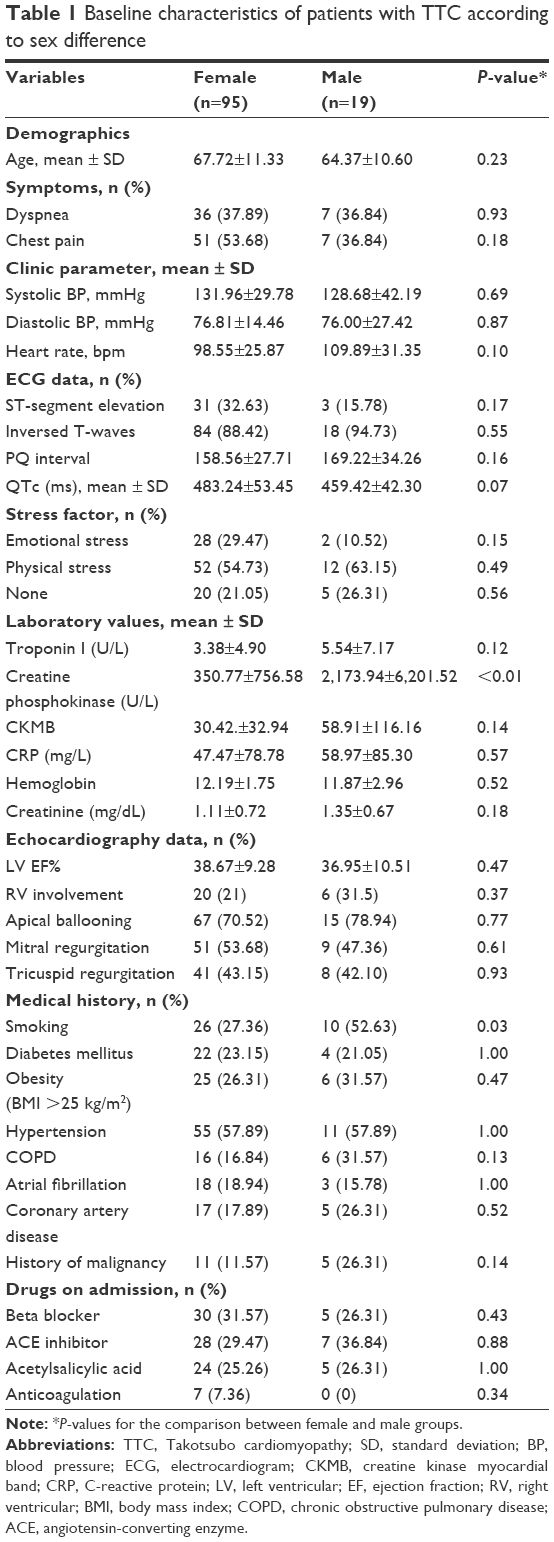 | Table 1 Baseline characteristics of patients with TTC according to sex difference |
Differences in patient characteristics related to female and male sex
Comparing the age in the female and male groups, no statistically significant difference was shown (Table 1). Vital signs such as blood pressure and heart rate were also similar in both groups. Regarding patient’s history, the ratio of female patients suffering from angina was not different from the ratio of men (54% versus 37%, P>0.05). Female patients did not complain more often about emotional stress than male patients (30% versus 11%, P=0.15). Males also did not more likely suffer from physical stress than female patients (63% versus 55%, P=0.49).
The prevalence of malignancy was higher in male patients compared to females, but this was not statistically significant.
ECG recordings revealed a higher incidence of ST segment elevations and QT prolongation in females compared to males (33% versus 16%). However, no difference in T-wave inversions was observed. Transthoracic echocardiography show an increased incidence of right ventricular (RV) involvement in male patients compared to females (32% versus 21%). The apical type of TCC was most common (70% in females and 79% in males), followed by midventricular type occurring in 27% of females and 21% of males.
Regarding baseline laboratory values, no differences were observed for troponin I, C-reactive protein (CRP) or creatinine. Compared to females, males revealed significantly higher levels of creatinine kinase (CK).
No statistically significant differences were observed with respect to medical treatment at the time of TTC development between males and females.
The in-hospital events are shown in Table 2. Although males did have a higher incidence of life-threatening arrhythmias, in-hospital death and resuscitation than females, this difference was not significant. A difference was shown in the mechanical respiratory support (P=0.06). Males had a higher incidence of NPPV and intubation than females. No difference was shown in the length of stay at ICU. Noteworthy, the incidence for thromboembolic events was higher in females than in males.
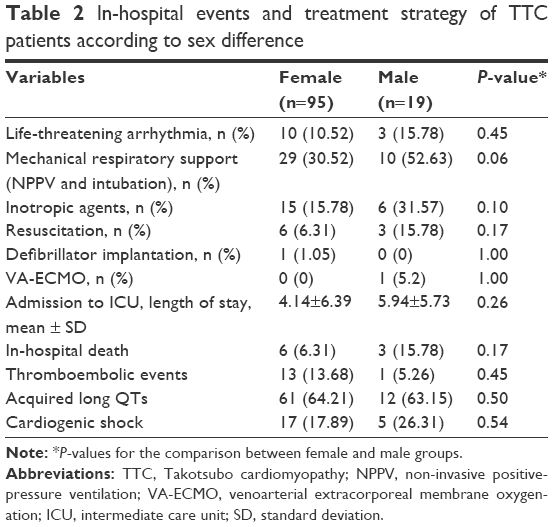 | Table 2 In-hospital events and treatment strategy of TTC patients according to sex difference |
Long-term all-cause mortality in TTC patients related to sex
As men showed higher mortality by tendency than women during 4 and 5 years (P=0.085 and P=0.093, respectively, significant by tendency), we included as further information the exact time of death in the continuous calculation and performed a Kaplan–Meier analysis. Analyzing the survival curves, within 5 years, the risk for death (all-cause mortality) of male patients revealed to be 2.6 times higher than that for female patients (hazard ratio [HR] 2.6, 95% CI 1.2–5.7, P=0.01; Figure 1). Most males died of noncardiac causes such as progressive cancer disease and sepsis. The mortality regarding cardiac death was equal in females and males. In Cox univariate analysis, male sex (P=0.01), CRP (P<0.01), glomerular filtration rate (GFR) <60 mL/min (P=0.01), ejection fraction (EF) ≤35% (P<0.01), shock (P<0.01) and the use if inotropic drugs (P<0.01) were associated with all-cause mortality. In multivariate Cox regression analysis, male sex (P=0.02, HR 2.8, 95% CI 1.1–7.2), EF ≤35% (P=0.01, HR 3.3, 95% CI 1.2–9.2) and GFR <60 mL/min (P<0.01, HR 3.1, 95% CI 1.4–7.0) figured out as independent predictors of all-cause mortality even after adjusting for all other variables being significant in univariate analysis (Table 3).
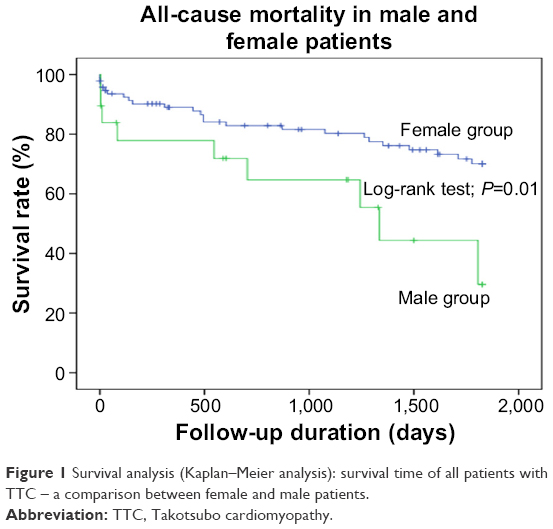 | Figure 1 Survival analysis (Kaplan–Meier analysis): survival time of all patients with TTC – a comparison between female and male patients. |
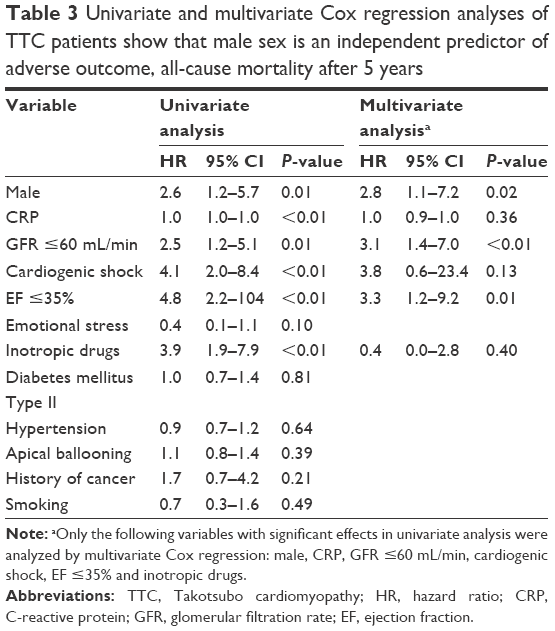 | Table 3 Univariate and multivariate Cox regression analyses of TTC patients show that male sex is an independent predictor of adverse outcome, all-cause mortality after 5 years |
Discussion
The present monocentric retrospective study investigated sex differences of baseline characteristics and 5 years all-cause mortality in patients suffering from TTC. First, this study confirmed that sex differences were found for patients’ symptoms at baseline clinical presentation. For instance, a higher rate of angina and emotional stress was found in females, whereas a higher rate of physical stress, smoking status and malignancies was found in males. Second, the present study demonstrated a higher rate of all-cause mortality after 5 years in male TTC patients compared to females, triggered by death due to cancer.
Previous studies have shown that sex differences might influence the development of TTC. Most TTC patients are older and females, whereas the incidence of TTC in males has been described to be even rare.15 Our study showed in accordance to further studies a lower incidence of male sex (16%) in TTC and younger age of these patients compared with female patients. These findings have been reported by Templin et al2 in 1,750 TTC patients. The predominance of females suffering from TTC is in clear contrast to patients with an AMI – representing the most important differential diagnosis of TTC – of which presumably males are more commonly diseased.14–16,18
This study confirms a higher rate of emotional stress in females compared to male TTC patients, whereas the sex groups were of similar age (mean: male, 64 years; female, 68 years). As it is widely known, emotional stress playing a major causative role for the development of TTC was therefore called “the broken heart syndrome”. Accordingly, a link was attributed pathologically to the so-called brain–heart axis.11,12,21 The so-called biopsychosocial disease model was described first in 1977 by Engel.22 This model expresses that the human body can manage diseases autoregulatively. This system is controlled by a circuit of several neurotransmitters, catecholamines and hormones implementing different axes to end organs such as the heart or the gastrointestinal tract. Within this model, disease development represents a dynamic process, in which the clinical manifestation follows a loss of function or overload of this controlling circuit.1,23 Beside the concept of the brain–heart axis, physical stress increases the synthesis of potentially cardiotoxic catecholamines such as epinephrine and metanephrine.23 In this context, recently published data of Templin et al presented a higher rate of physical triggers compared to emotional triggers in patients suffering from TTC.2
The etiology of TTC is understood poorly, whereas the role of impaired estrogen release is considered as a main pathomechanism,15,16 since most TTC patients are postmenopausal women.1,2 Estrogen reveals several cardioprotective effects, such as antioxidant effects, inhibition of the renin–angiotensin system and modulation of atrial natriuretic peptide.16 In human beings, the secretion of estrogen is lower in postmenopausal compared to premenopausal women and estrogen levels in postmenopausal women appear to be lower than in men at the same age.24 Therefore, the present study complements the evidence of former studies, widening the characterization of TTC patients in males and females.
As it was shown recently, emotional stress may also encourage the development of depressive disorders.25,26 Depressive symptoms were not documented in the present study cohort; however, the implication of standardized questionnaires, such as the Hospital Anxiety and Depression Scale, may become helpful to picture the intangible effects of depression and anxiety in patients with TTC.25,26 Interestingly, a prolongation of the QT interval on ECG recordings was shown to be associated with depressive symptoms in patients after suffering from an acute coronary syndrome.27 Accordingly, the present study shows that the incidence of QT-interval prolongation is very high. In addition, the data set of Templin et al2 represents a significant prolongation in the QT interval in male and female patients suffering from TTC. Schneider et al15 was able to identify a significant difference in ST-segment elevation, being less frequently in male TTC patients.18 However, no further ECG differences were found in the present study.
This study demonstrates that the 5-year all-cause mortality rate following TTC is higher in men compared to women. In patients suffering from an AMI, large-scale studies found conflicting results about sex-adjusted differences of long-term mortality.25,28 Some studies favor a higher mortality rate in women, whereas others demonstrate increasing mortality rates in males.29–31 The large International Takotsubo Registry also reported about higher long-term mortality rate in male patients compared with female patients. During long-term follow-up, cardiovascular and cerebrovascular events were more observed among male patients. In our study, the mortality rate of male patients (n=9, 47.3%) was higher than that of female patients (n=24, 25.2%), but nevertheless cardiac cause of death and cardiovascular events were similar in male and female patients. Most males died of noncardiac causes such as progressive cancer disease and sepsis.
Even if TTC is defined as a benign disease, it is associated with several complications such as peripheral or central thromboembolism.4,6 Elevated CRP levels, elevated D-dimers and severely impaired LV function seem to be a risk factor of developing thromboemboli. In our TTC cohort, the incidence of thromboembolic events is high and females are more affected than males. Templin et al2 also showed a high risk for thromboembolic events such as stroke in patients suffering from TTC. In comparison to our results, they could not show a significant sex difference.
Within a large-scale registry of TTC patients, Murakami et al16 found that male sex represents a general independent risk factor for the development of adverse cardiac events, including cardiovascular death. However, a clear follow-up in this observational analysis was not defined clearly. In addition, Brinjikji et al17 analyzed a large national database of TTC patients and found that mortality was significant higher in male patients with TTC during a follow-up of 1 year.15,16 The studies did not report about a 5-year outcome in male patients with TTC.
It might be speculated whether the female predominance of TTC is overestimated due to the fact that male patients were shown to die at earlier stages of TTC development even before definite diagnostic assessment.18 Schneider et al showed that males were more often admitted to hospital after successful or fatal cardiopulmonary resuscitation (CPR) than females, implying an impaired prognosis in males even after successful CPR.15 This might indicate a higher electrical vulnerability within the early phase of the TTC development.32 Accordingly, the rates of sudden cardiac deaths and CPR are more frequent in males than in females suffering from AMI.18 On the other hand, male patients revealed a higher rate of physical stress, smoking status and malignancies in the present study cohort. However, these risk factors were not shown to influence long-term all-cause mortality in male patients in the present study.
Conclusion
This study shows that males suffering from TTC reveal a higher risk for all-cause mortality than females over a 5 year follow-up period. A vital component of the diagnostic and disease management chain is the physicians’ experience treating patients with TTC, the involvement of an interdisciplinary team and the streamlined treatment of such complications on a patient-individualized basis. Currently, the underlying pathomechanism for sex differences in TTC is not clarified yet. Whether emotional stress, depressive symptoms and estrogen decrease may explain the differences in long-term prognosis need to be investigated in upcoming prospective randomized studies.
Acknowledgments
We thank Siegfried Lang for his statistical assistance. We acknowledge the financial support of the Deutsche Forschungsgemeinschaft and Ruprecht-Karls-Universität Heidelberg within the funding program Open Access Publishing. All data generated or analyzed during this study are included in this published article.
Disclosure
The authors report no conflicts of interest in this work.
References
Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. [Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases]. J Cardiol. 1991;21(2):203–214. Japanese. | ||
Templin C, Ghadri JR, Diekmann J, et al. Clinical features and outcomes of Takotsubo (Stress) cardiomyopathy. N Engl J Med. 2015;373(10):929–938. | ||
Becher T, El-Battrawy I, Baumann S, et al. Characteristics and long-term outcome of right ventricular involvement in Takotsubo cardiomyopathy. Int J Cardiol. 2016;220:371–375. | ||
El-Battrawy I, Borggrefe M, Akin I. Takotsubo syndrome and embolic events. Heart Fail Clin. 2016;12(4):543–550. | ||
Haghi D, Papavassiliu T, Fluchter S, et al. Variant form of the acute apical ballooning syndrome (takotsubo cardiomyopathy): observations on a novel entity. Heart. 2006;92(3):392–394. | ||
El-Battrawy I, Behnes M, Hillenbrand D, et al. Prevalence, clinical characteristics, and predictors of patients with thromboembolic events in Takotsubo cardiomyopathy. Clin Med Insights Cardiol. 2016;10:117–122. | ||
Botto F, Trivi M, Padilla LT. Transient left midventricular ballooning without apical involvement. Int J Cardiol. 2008;127(3):e158–e159. | ||
Ennezat PV, Pesenti-Rossi D, Aubert JM, et al. Transient left ventricular basal dysfunction without coronary stenosis in acute cerebral disorders: a novel heart syndrome (inverted Takotsubo). Echocardiography. 2005;22(7):599–602. | ||
Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008;155(3):408–417. | ||
Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001;38(1):11–18. | ||
Samuels MA. The brain-heart connection. Circulation. 2007;116(1):77–84. | ||
Suzuki K, Osada N, Akasi YJ, et al. An atypical case of “Takotsubo cardiomyopathy” during alcohol withdrawal: abnormality in the transient left ventricular wall motion and a remarkable elevation in the ST segment. Intern Med. 2004;43(4):300–305. | ||
Regitz-Zagrosek V. Sex and gender differences in health. Science & Society Series on Sex and Science. EMBO Rep. 2012;13(7):596–603. | ||
Kurisu S, Kihara Y. Tako-tsubo cardiomyopathy: clinical presentation and underlying mechanism. J Cardiol. 2012;60(6):429–437. | ||
Schneider B, Athanasiadis A, Stollberger C, et al. Gender differences in the manifestation of tako-tsubo cardiomyopathy. Int J Cardiol. 2013;166(3):584–588. | ||
Murakami T, Yoshikawa T, Maekawa Y, et al. Gender differences in patients with Takotsubo cardiomyopathy: Multi-Center Registry from Tokyo CCU Network. PLoS One. 2015;10(8):e0136655. | ||
Brinjikji W, El-Sayed AM, Salka S. In-hospital mortality among patients with takotsubo cardiomyopathy: a study of the National Inpatient Sample 2008 to 2009. Am Heart J. 2012;164(2):215–221. | ||
Madhavan M, Prasad A. Proposed Mayo Clinic criteria for the diagnosis of Tako-Tsubo cardiomyopathy and long-term prognosis. Herz. 2010;35(4):240–243. | ||
Liu O, Li JR, Gong M, Xu M, Du J, Zhang HJ. Genetic analysis of six SNPs in candidate genes associated with high cross-race risk of development of thoracic aortic aneurysms and dissections in Chinese Han population. Acta Pharmacol Sin. 2010;31(10):1376–1380. | ||
Wang XL, Liu O, Qin YW, Zhang HJ, Lv Y. Association of the polymorphisms of MMP-9 and TIMP-3 genes with thoracic aortic dissection in Chinese Han population. Acta Pharmacol Sin. 2014;35(3):351–355. | ||
Suzuki R, Kudo T, Kurazumi H, et al. Transapical extirpation of a left ventricular thrombus in Takotsubo cardiomyopathy. J Cardiothorac Surg. 2013;8:135. | ||
Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. | ||
Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;352(6):539–548. | ||
Vermeulen A, Kaufman JM, Goemaere S, van Pottelberg I. Estradiol in elderly men. Aging Male. 2002;5(2):98–102. | ||
Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: large-scale observations from the CRUSADE (Can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J Am Coll Cardiol. 2005;45(6):832–837. | ||
Chiba S, Numakawa T, Ninomiya M, Richards MC, Wakabayashi C, Kunugi H. Chronic restraint stress causes anxiety- and depression-like behaviors, downregulates glucocorticoid receptor expression, and attenuates glutamate release induced by brain-derived neurotrophic factor in the prefrontal cortex. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(1):112–119. | ||
Wang TJ, Larson MG, Levy D, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107(23):2920–2925. | ||
Anand SS, Xie CC, Mehta S, et al. Differences in the management and prognosis of women and men who suffer from acute coronary syndromes. J Am Coll Cardiol. 2005;46(10):1845–1851. | ||
Martin CA, Thompson PL, Armstrong BK, Hobbs MS, de Klerk N. Long-term prognosis after recovery from myocardial infarction: a nine year follow-up of the Perth Coronary Register. Circulation. 1983;68(5):961–969. | ||
Moriel M, Behar S, Tzivoni D, Hod H, Boyko V, Gottlieb S. Management and outcomes of elderly women and men with acute coronary syndromes in 2000 and 2002. Arch Intern Med. 2005;165(13):1521–1526. | ||
Vaccarino V, Parsons L, Every NR, Barron HV, Krumholz HM. Sex-based differences in early mortality after myocardial infarction. National Registry of Myocardial Infarction 2 Participants. N Engl J Med. 1999;341(4):217–225. | ||
Bowker TJ, Wood DA, Davies MJ. Sudden unexpected cardiac death: methods and results of a national pilot survey. Int J Cardiol. 1995;52(3):241–250. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.