")
Back to Journals » Patient Preference and Adherence » Volume 10
Sex differences in the quality of life of patients with acute coronary syndrome treated with percutaneous coronary intervention after a 3-year follow-up
Authors Jankowska-Polańska B , Uchmanowicz I , Dudek K , łoboz-Grudzień K
Received 17 February 2016
Accepted for publication 31 March 2016
Published 20 July 2016 Volume 2016:10 Pages 1279—1287
DOI https://doi.org/10.2147/PPA.S106577
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Beata Jankowska-Polańska,1 Izabella Uchmanowicz,1 Krzysztof Dudek,2 Krystyna Łoboz-Grudzień1,3
1Department of Clinical Nursing, Wrocław Medical University, 2Department of Logistics and Transport Systems, Faculty of Mechanical Engineering, Wrocław University of Technology, 3Cardiology Unit, T Marciniak Lower Silesian Specialist Hospital, Emergency Medicine Centre, Wrocław, Poland
Background: The aims of this study were to analyze the dynamics of quality of life (QoL) changes after 36 months from the percutaneous coronary intervention (PCI) depending on sex and identify baseline predictors of the follow-up QoL of patients hospitalized for acute coronary syndrome (ACS) and subjected to PCI.
Methods and results: The study included 137 patients, females (n=67) and males (n=70), with ACS who underwent PCI. The QoL was assessed using the MacNew Heart Disease Health-Related Quality of Life questionnaire. The group of females scored lower in all the domains of the MacNew Heart Disease Health-Related Quality of Life questionnaire in the initial measurement (B1), in the measurement after 6 months (B2), and in the long-term follow-up measurement (36 months – B3). Despite the fact that both groups achieved improved QoL, its values were higher in the males. The average growth rate of the QoL score in the period from the sixth month to 36th month was higher in females than in males. In the univariate and multivariate analyses, significant independent predictors with a negative influence on the long-term QoL score included female sex (Ρ=−0.190, β=−0.21), age >60 years (Ρ=−0.255, β=−0.186), and diabetes (Ρ=−0.216, β=−0.216).
Conclusion: In a 36-month follow-up of ACS patients treated with PCI, there were no statistically significant differences in QoL between sexes. In the entire cohort, there was improvement in QoL, which was higher in the case of the females studied. For the entire group, significant independent determinants of lower QoL 3 years after ACS included female sex, age >60 years, and diabetes.
Keywords: quality of life, percutaneous coronary intervention, sex differences
Background
Percutaneous coronary intervention (PCI) is currently considered to be the most effective method for treating acute coronary syndrome (ACS) in both males and females. At present, PCI is the method of choice in the treatment of ACS.1 It was shown that females undergoing percutaneous revascularization exhibit worse immediate results of the procedure; however, long-term results are similar for both sexes.2–7 The worse prognosis of females hospitalized for ACS may result from their older age at the onset of the disease, more frequent concomitant diseases, such as diabetes and hypertension, as well as anatomical and pathophysiological differences in the structure of the heart and coronary vessels (in females, coronary vessels are more angled and their diameter is smaller and there are also differences in the composition and properties of the atherosclerotic plaque).7,8
According to the European Society of Cardiology guidelines, a quality of life (QoL) score should also be included in the assessment of the effectiveness of the treatment applied, apart from symptomatic improvement, reduction in angina pectoris, and improved exercise tolerance.1
During the last few years, QoL score has become an important indicator of the total benefit achieved by a patient during different diagnostic and therapeutic procedures. Referring to treatment results from the perspective of QoL provided medicine with an opportunity to present long-term effects in the management of diseases. Patients who had suffered myocardial infarction exhibited a decrease in their QoL.9
The available research indicates that sex is a determinant affecting QoL after ACS. However, there is still an ongoing discussion in the literature, and the data concerning the role of sex are still ambiguous. In several publications, male patients undergoing coronary revascularization exhibited higher QoL in comparison to female patients.10,11 The initial QoL score is an important determinant for the long-term QoL score.12 The dynamics of changes observed in QoL reveal an improvement in both sexes, which is, however, more pronounced in males.13,14 There are publications that find no differences between the sexes in terms of the level of QoL, with improvement occurring regardless of sex.15 In our previous research, we reported that 6 months after ACS, improvement in QoL occurred in both sexes at the physical level, but only in females at the psychological level.16
Numerous studies indicate that PCI conducted in patients with ACS considerably reduces mortality,17,18 but there are only a few publications concerning both survival assessment19–21 and comparative analysis of QoL, early and long-term, several years after PCI, which would analyze this quality with reference to sex.22,23
Aim of the study
The aims of this study were to research the dynamics of changes in QoL 36 months after PCI with reference to sex and to identify the predictors (baseline) that may influence the long-term QoL in patients hospitalized for ACS undergoing PCI.
Patients
The study included 140 patients (70 females and 70 males) aged between 32 years and 95 years (mean age: 63.4 years) hospitalized for ACS, who were subjected to PCI at the Department of Cardiology, T Marciniak Lower Silesian Specialist Hospital, Wrocław, between September 2009 and March 2010. The clinical diagnosis of ACS was based on the general criteria adopted by the European Society of Cardiology.24
The patients were examined by the cardiologist, who diagnosed ACS on the basis of electrocardiogram and biomarkers. The firm diagnosis of the myocardial infarct, the application of the PCI, and the written informed consent were the inclusion criteria. The exclusion criteria were the hemodynamic instability and the lack of the informed consent to participate in the study. Questionnaires were distributed by a cardiac nurse 2–4 days after PCI. All patients were informed of the purpose and nature of this study and provided their written informed consent to be included in it. All patients completed all questionnaires. Information concerning the sociodemographic and clinical data came from the hospital registry files.
The study was conducted with the consent of the Bioethical Committee of the Wrocław Medical University (consent no KB-234/2009).
The patients were divided into groups based on their sex: Group I (n=70): females with ACS without non-ST elevation myocardial infarction (NSTEMI; n=14) subjected to early invasive strategy and with ST-elevation myocardial infarction (STEMI; n=56) subjected to PCI, aged between 44 years and 95 years (mean age: 67.6 years) and Group II (n=70): males with ACS without ST elevation (NSTEMI; n=9) subjected to early invasive strategy and with ST elevation (STEMI; n=61) subjected to PCI, aged between 32 years and 95 years (mean age: 59.2 years).
The study was prospective. The assessment of quality of life was conducted during week 1 and after PCI (B1) as well as 6 months (B2) and 36 months (B3) after the procedure. Both in week 1 after the procedure and 6 months later, the surveys were filled in directly in the presence of a person conducting the research. Measurement B2, 6 months after PCI, took place at the Hospital Outpatient Clinic of Cardiology during the follow-up visits. The measurement conducted 6 months after PCI included 67 females and 70 males, as three females qualified for the initial measurement had died. The deaths, which occurred 5–6 months after the initial measurement, were due to cardiovascular reasons.
The third measurement (B3) was obtained through correspondence with the use of questionnaires sent by post. Before sending the surveys, the participants were contacted over the phone and informed about the researchers’ intention to conduct these surveys. Ultimately, 113 patients participated in measurement B3 (seven people did not send their surveys back despite previous phone contact and 17 [12.2%] people died, including nine [6.4%] females).
Methods
QoL assessment
The MacNew Heart Disease Health-Related Quality of Life (MacNew) is one of the most popular questionnaires specifically designed to establish health-related QoL of cardiac patients.25 It contains 27 questions associated with cardiac health during 2 weeks prior to questionnaire administration. Answers to individual sets of questions are given with the use of the 7-point Likert scale, from 1 (all the time) to 7 (never). Each answer in individual domains is assigned an appropriate number of points – the lower the number of points, the lower the QoL. The results are calculated for three dimensions of QoL: physical, emotional, and social functioning. It is also possible to establish the global QoL score of a given patient by adding the weights of all answers and dividing the result by the number of questions that the patient answered. The Polish version, with Oldridge’s consent, was prepared in 2002 by two independent teams from two places: Łódź, led by Zielińska from the Clinic of Cardiology at the Medical University of Łódź, and Warsaw, led by Wrześniewski.26 The reliability of the Polish version of MacNew was verified by establishing internal compliance and temporal stability. The questionnaire possesses satisfactory psychometric properties: Cronbach’s alpha from 0.87 to 0.93 and a correlation coefficient from 0.55 to 0.87.26 The MacNew questionnaire is a reliable and valid method of assessing changes in health-related QoL among population with heart disease and discriminates better between angina grades.27,28
Multivariate ANOVA analysis was used in the study to compare the general QoL results of the MacNew questionnaire and establish the influence of selected variables on QoL. The predictors included in the study were sociodemographic factors (sex, age, marital status, education, occupational activity), clinical features (form of ACS), and risk factors (tobacco smoking, obesity [body mass index {BMI} ≥30 kg/m2 was considered as obesity and BMI =25–29.9 kg/m2 as overweight; waist–hip ratio was assumed as a standardized method for monitoring central obesity; waist circumference ≥90 was considered as abdominal obesity, which is in line with the guidelines of the Polish Diabetological Society of 2014], lipid metabolism [definition of dyslipidemia – based on the criteria of Adult Treatment Panel III], assumed values [triglycerides ≥150 mg/dL, high-density lipoprotein cholesterol <40 mg/dL {1.0 mmol/L} in males and 45 mg/dL {1.3 mmol/L} in females, total cholesterol ≥190 mg/dL, low-density lipoprotein cholesterol ≥115 mg/dL], diabetes [diagnosed on the basis of medical history of regular use of hypoglycemic agents and/or laboratory test results],29 and hypertension [in two measurements of arterial pressure; hypertension was diagnosed when the value of systolic blood pressure was ≥140 mmHg and/or diastolic blood pressure was ≥90 mmHg or when patients regularly used antihypertensive drugs, which is in line with the guidelines of the Polish Society of Hypertension; Table 1]).30
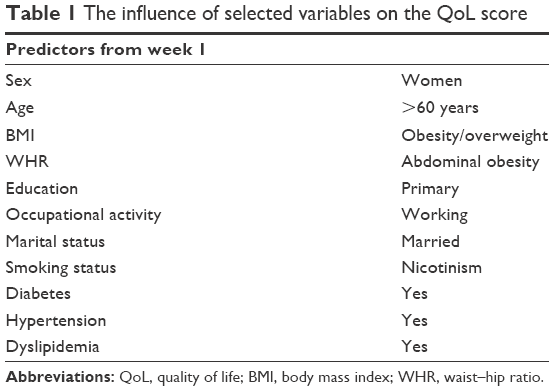 | Table 1 The influence of selected variables on the QoL score |
Results
Sociodemographic and clinical analysis revealed that females with ACS are older by 7–8 years on average than males (67.6±12.7 vs 59.2±10.7; P<0.0001) at the onset of the disease. They are also less educated (35.7% vs 11.4% received only primary education; P<0.001) and are less occupationally active (17.1% vs 38.6% working males; P<0.003). They more frequently suffer from hypertension (71.4% vs 37.1%; P<0.001), diabetes (40% vs 21.4%; P<0.028), and obesity (BMI 30.5±5.5 vs BMI 29.6±3.4; P<0.001), while males more often exhibit positive family history of cardiovascular disease (67.1% vs 45.7%; P<0.017) and smoke more cigarettes (42.9% vs 8.6% smoked cigarettes on admission for ACS; P<0.001; Table 2).
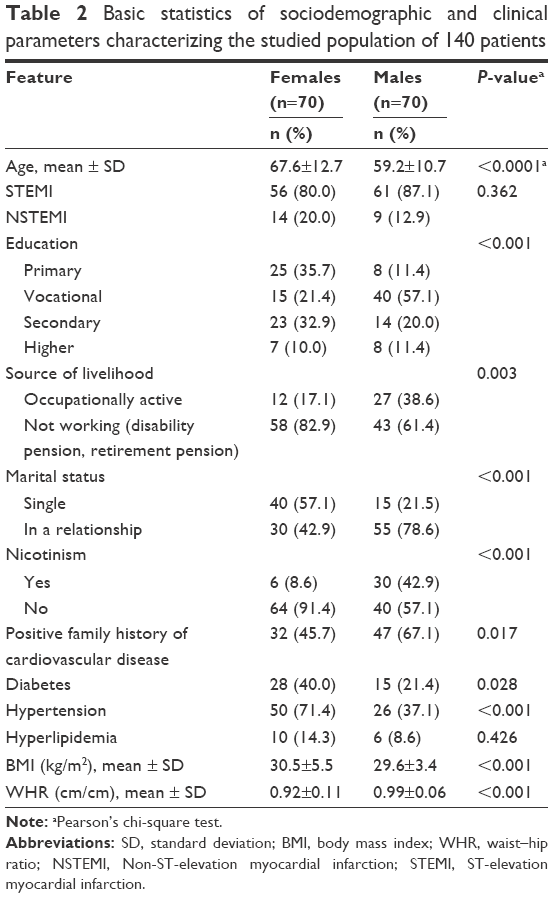 | Table 2 Basic statistics of sociodemographic and clinical parameters characterizing the studied population of 140 patients |
QoL analysis
In the group of females, in comparison to the group of males, we found lower values of QoL in all the domains of the MacNew questionnaire in the initial measurement (B1), in the measurement after 6 months (B2), and in the long-term follow-up (36 months – B3), respectively: physical functioning, 3.81 (95% CI: 3.54–4.09) vs 4.32 (95% CI: 4.0–4.62), 4.18 (95% CI: 3.86–4.49) vs 4.79 (95% CI: 4.49–5.09), and 4.48 (95% CI: 4.22–4.75) vs 4.93 (95% CI: 4.62–5.24); emotional functioning, 3.05 (95% CI: 2.70–3.40) vs 3.74 (95% CI: 3.35–4.12), 4.72 (95% CI: 4.39–5.05) vs 5.18 (95% CI: 4.93–5.43), and 4.99 (95% CI: 4.76–5.23) vs 5.31 (95% CI: 5.03–5.60); and social functioning, 3.81 (95% CI: 3.47–4.14) vs 4.44 (95% CI: 4.02–4.85), 4.90 (95% CI: 4.58–5.22) vs 5.37 (95% CI: 5.08–5.66), and 5.09 (95% CI: 4.80–5.37) vs 5.52 (95% CI: 5.21–5.84). Global QoL in all three measurements was higher in the males studied in comparison to the females: physical functioning, 3.56 (95% CI: 3.26–3.87) vs 4.17 (95% CI: 3.81–4.53), emotional functioning, 4.60 (95% CI: 4.29–4.91) vs 5.11 (95% CI: 4.84–5.39), and social functioning, 4.86 (95% CI: 4.61–5.11) vs 5.26 (95% CI: 4.96–5.55). Differences in all values were significant only in observations B1 and B2 after PCI. In measurement B3 (36 months), the differences in QoL between sexes were not statistically significant apart from physical functioning (Table 3).
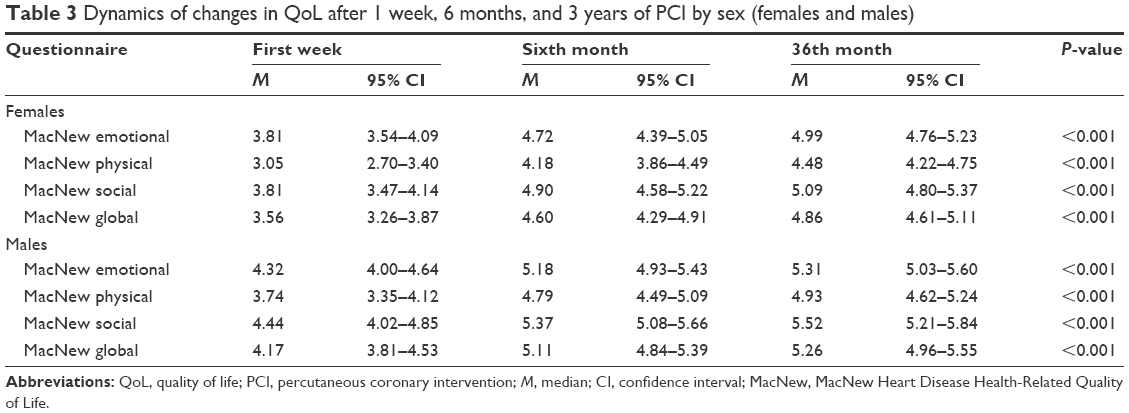 | Table 3 Dynamics of changes in QoL after 1 week, 6 months, and 3 years of PCI by sex (females and males) |
The analysis of the dynamics of changes in QoL revealed a favorable comparable trend in both females and males in all the domains of the MacNew questionnaire: in the physical domain, 3.05 vs 4.18 vs 4.48 for females and 3.74 vs 4.79 vs 4.93 for males; in the emotional domain, 3.81 vs 4.72 vs 4.99 for females and 4.32 vs 5.18 vs 5.31 for males; in the social domain, 3.81 vs 4.90 vs 5.09 for females and 4.44 vs 5.37 vs 5.52 for males; and in the global QoL domain 3.56 vs 4.60 vs 4.86 for females and 4.17 vs 5.11 vs 5.26 for males. These values were statistically significantly different and are presented in Table 3.
Classic measures of time series dynamics, ie, increments (Δ) and indices of dynamics (i), were used to establish the dynamics of changes in QoL. Table 4 includes the increments and indices of the dynamics of changes in QoL of males and females assessed with the use of the MacNew questionnaire in the physical, emotional, and social dimensions as well as globally; the average rate of change G was also assessed (geometric mean of chain indices; Table 4).
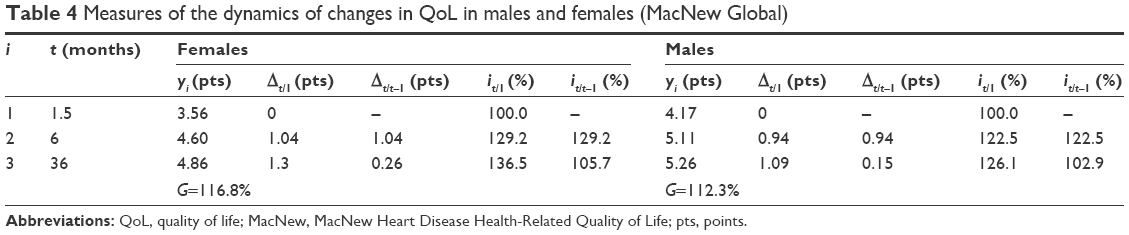 | Table 4 Measures of the dynamics of changes in QoL in males and females (MacNew Global) |
Despite the fact that both groups achieved improved QoL, its values were higher in the males studied in all three measurements. The average growth rate of the QoL score in the period from the sixth month to 36th month was higher in females than in males in all the domains studied with the use of the MacNew questionnaire. Thus, after 36 months, the differences in the QoL score between females and males decreased significantly.
Furthermore in the study, a multiple regression model was applied with the use of the stepwise method, including selected sociodemographic and clinical predictors from week 1 and assessing their influence on the QoL score achieved with the use of the MacNew questionnaire (Table 5). In the univariate analysis, the predictors with a negative influence on the QoL score for the entire group included age >60 years (ρ=−0.255; P=0.007), female sex (ρ=−0.190; P=0.045), and diabetes (ρ=−0.261; P=0.006). Occupational activity had a positive influence on the QoL score (ρ=6.11; P=0.015); Table 5).
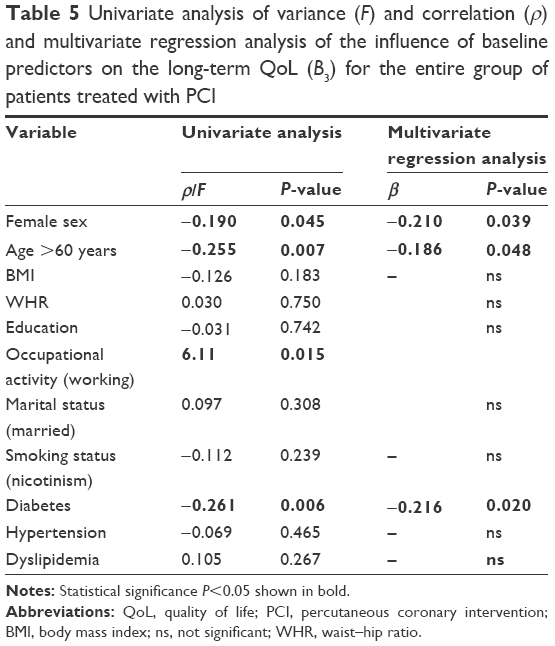 | Table 5 Univariate analysis of variance (F) and correlation (ρ) and multivariate regression analysis of the influence of baseline predictors on the long-term QoL (B3) for the entire group of patients treated with PCI |
In the univariate and multivariate analyses, significant independent predictors with a negative influence on the long-term QoL score included female sex (ρ=−0.190, β=−0.21), age >60 years (ρ=−0.255, β=−0.186), and diabetes (ρ=−0.261, β=−0.216). Negative values of the standardized correlation coefficient (ρ) point to a negative influence of female sex, age >60 years, and diabetes on the long-term QoL score. Occupational activity had a positive influence on the QoL score (ρ=6.11). Ultimately, the model took the following form: F(8; 99) =4.17; P<0.001; and R=0.502 (Table 5).
Analysis of the influence of selected variables during first week following PCI on long-term QoL (36 months) was conducted for both sexes. The results are presented in Tables 6 and 7.
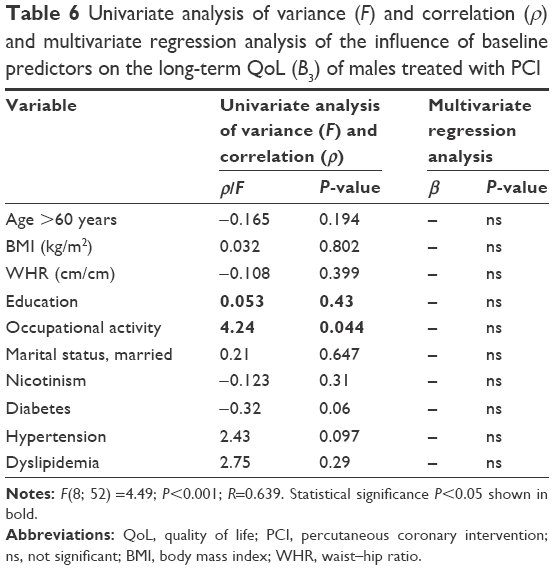 | Table 6 Univariate analysis of variance (F) and correlation (ρ) and multivariate regression analysis of the influence of baseline predictors on the long-term QoL (B3) of males treated with PCI |
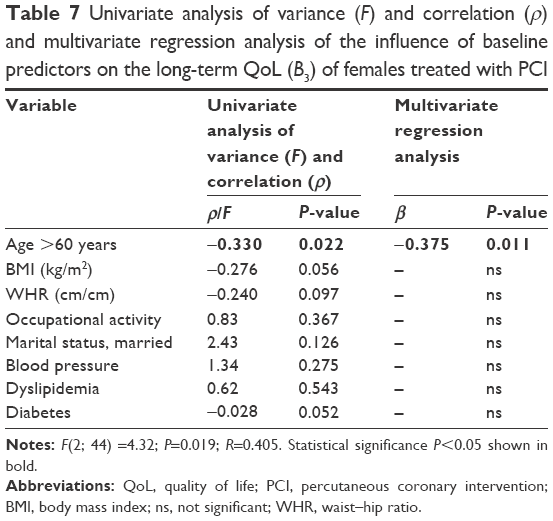 | Table 7 Univariate analysis of variance (F) and correlation (ρ) and multivariate regression analysis of the influence of baseline predictors on the long-term QoL (B3) of females treated with PCI |
In the univariate analysis, the variables related to the QoL of the males studied included occupational activity. Positive coefficient values indicate a positive influence on the QoL score (Table 6).
In the group of females studied, the predictor influencing the long-term QoL score in uni- and multivariate analyses was age >60 years. Its negative value points to a negative influence on the QoL score at 36 months after PCI (Table 7).
Discussion
In the literature, there are some papers that evaluate the early QoL11–14 of the patients after ACS treated with PCI, but there are only a few papers that evaluate distant QoL and their determinants resulting from the sex differences.9,31–33 Our study collected QoL data for a relatively long period of time compared to other studies.
In our study, females with ACS treated with PCI had lower QoL than males in measurements conducted during week 1 as well as after 6 months and 36 months. In measurements B1 and B2, the differences in QoL between the sexes were statistically significant, while in the measurement conducted after 36 months (B3), the differences in QoL were not significant. Females had lower score of QoL than males despite the improvement. The results of our study are consistent with the results in the literature concerning sex differences in the QoL of patients treated with PCI. According to some studies, females assess their QoL as worse than males.14,34,35 In our research, similar to the results obtained by Agewall et al13 after 1–12 months of ACS, the QoL of females was lower in all the domains of the MacNew questionnaire.
The results obtained by Włodarczyk revealed higher values in the physical and emotional aspects of life in the males studied in follow-ups 2 months and 3 months after ACS. However, in a follow-up after 1 year, no sex differences in QoL were found.31 In our study at baseline and 6 months after ACS, lower score of QoL in females was observed than males, but after 36 months, the differences were not significant. In a study conducted by Pettersen et al,35 2.5 years after ACS, the lower the evaluation of QoL, the older the females were, but in each case, the QoL score of females was lower than that of males.
In our study, dynamics of QoL change between the assessment at baseline and the evaluation after 6 months and 36 months of PCI revealed a positive tendency for improvement in both sexes. In a study conducted by Dueñas et al,14 6 months after infarction, males exhibited a favorable trend for improvement, especially in most domains constituting the overall assessment of physical health in the 36-Item Short Form Health Survey questionnaire, while females exhibited improvement only in the Physical Component Summary and social functioning domains. The cited authors considered mental health as the most important determinant of lower QoL in both sexes.14 Similar to our studies, Włodarczyk did not find any differences in the levels of QoL between the sexes in a long-term 1 year follow-up after PCI.31 Similar conclusions were presented in a study by Brink et al,32 where both sexes achieved QoL improvement in a year after infarction, but females scored their QoL higher in the psychological health domain, while males did so in the physical health domain.
The available publications document that QoL becomes reduced together with the presence and intensity of modifiable risk factors for cardiovascular events, such as hypertension, active nicotinism, lipid metabolism disorders, diabetes, obesity, and sedentary lifestyle.12,36 Therefore, the assessment of the influence of selected sociodemographic and clinical variables on the QoL score is an important element of a study. In the research conducted by Kwaśniewska and Drygas,37 the presence of even a single risk factor for atherosclerosis caused a significant deterioration in the subjective assessment of the QoL parameters; the more the factors present at the same time, the lower the QoL score.
In our own research, females treated for ACS were on average 7–8 years older and less educated than males; they also more frequently suffered from diabetes, hypertension, and obesity. Males, on the other hand, exhibited lipid metabolism disorders and smoked tobacco more frequently than females.
In the univariate analysis in the authors’ own research, the negative predictors influencing long-term QoL included female sex, age >60 years, and diabetes. The predictor with a positive influence on the QoL score was occupational activity, especially in the group of males. In a study by Hawkes et al,38 lower QoL in the physical domain was mainly exhibited by the unemployed and elderly people, while lower QoL in the psychological domain was mainly exhibited by the younger people.
In our analysis, age >60 years was associated with a negative QoL score and constituted an independent determinant of lower QoL in the multivariate analysis of the entire group and a separate analysis conducted in females. The negative impact of the age on the evaluation of the QoL might be explained by the mobility restrictions and difficulties in the familial, social, and professional life.
In a research by Beck et al,39 younger age was a predictor of a higher QoL score, especially in terms of physical functioning (PCS), between 6 months and 12 months after infarction. However, in a study by Brown et al,33 patients <55 years of age scored their QoL much lower than older individuals in a 4-year follow-up after ACS. The authors explain this fact by limitations in the participation in occupational and social activities.39 In studies conducted by other authors, age was a determinant of lower QoL, but only in females,35 or it influenced the reduction in QoL only in the Mental Component summary domain of the 36-Item Short Form Health Survey.40
Sex constitutes another determinant of QoL after 3 years of follow-up. In our analysis, female sex was an independent predictor negatively affecting QoL in the “global” domain of the MacNew questionnaire. The lower QoL of females is explained by their lower education and higher limitations of physical and social activities. It is worth mentioning that despite the improvement in QoL in both sexes in the 3-year follow-up, females achieved higher dynamics of favorable changes. The studies confirm the impact of sex on QoL: some of them on all the QoL domains15 and some of them only on the physical domain.40
Diabetes is an important predictor affecting the QoL score. The authors’ own research shows its negative influence both in the uni- and multivariate analyses conducted for the entire group. The published research emphasizes the negative relationship of diabetes with lower QoL. Research conducted by Gijsberts et al41 documents the negative influence of diabetes on QoL of males after PCI. However, in research by Dias et al,12 a lower QoL score after 16 months of ACS in the physical domain was associated with diabetes, female sex, hypertension, dyslipidemia, and low level of education. In a study by Uchmanowicz et al42 conducted 6 months after ACS, patients with diabetes had lower QoL scores than nondiabetic patients.
The observation of QoL seems to be of importance for clinical practice, and the authors’ own results are among the few that show the dynamics of QoL changes in the long-term follow-up after ACS, especially with regard to sex differences. The presented model of recovery after ACS shows that special attention needs to be paid to the females studied who score their QoL lower than the males despite the achieved improvement. What is also surprising is the result indicating lower dynamics of QoL improvement among males after 3 years of infarction.
Practical implications
Regardless of sex, all patients after infarction should receive support and motivation to continue treatment and pharmacotherapy, as well as should implement and maintain healthy changes in their lifestyles.
Medical personnel should focus particularly on patients who exhibit determinants associated with a decrease in QoL, as is the case with elderly females and patients with diabetes.
Limitation of study
The limitations of this study include the small size of the study group, which decreased during the 3 years following ACS. The fact that the measurements were performed after 6 months and 36 months did not allow for an in-depth observation in the time between the second and third assessments.
The other study limitation was not taking into account some additional factors, which might influence the QoL: prior coronary artery disease, size/location of myocardial infarction, left ventricular ejection fraction, presence of congestive heart failure, and discharge to home vs nursing home.
Conclusion
All patients exhibited a positive trend for QoL improvement, which was higher in the case of the females studied than males. The three evaluations of QoL pointed to significant improvement in QoL. However, after 36-month follow-up, the results of patients after ACS treated with PCI did not show statistically significant differences in QoL between sexes. For the entire study group, significant independent determinants of lower QoL after 3 years of ACS included female sex, age >60 years, and diabetes. Among females, older age (>60 years) was a significant independent determinant of lower long-term QoL. Among the males studied, occupational activity was a significant determinant with a positive influence on the QoL score.
Disclosure
The authors report no conflicts of interest in this work.
References
Windecker S, Kolh P, Alfonso F, et al. Wytyczne ESC/EACTS dotyczące rewaskularyzacji mięśnia sercowego w 2014 roku. [2014 ESC/EACTS guidelines on myocardial revascularization]. Kardiol Pol. 2014;72(12):1253–1379. Polish. | ||
Glaser R, Herrmann HC, Murphy SA, et al. Benefit of an early invasive management strategy in women with acute coronary syndromes. JAMA. 2002;288(24):3124–3129. Polish. | ||
Lagerqvist B, Säfström K, Ståhle E, Wallentin L, Swahn E; FRISC II Study Group Investigators. Is early invasive treatment of unstable coronary artery disease equally effective for both women and men? FRISC II Study Group Investigators. J Am Coll Cardiol. 2001;38(1):41–48. | ||
Wiviott SD, Cannon CP, Morrow DA, et al. Differential expression of cardiac biomarkers by gender in patients with unstable angina/non-ST-elevation myocardial infarction: a TACTICS-TIMI 18 (treat angina with aggrastat and determine cost of therapy with an invasive or conservative strategy-thrombolysis in myocardial infarction 18) substudy. Circulation. 2004;109(5):580–586. | ||
Anand SS, Xie CC, Mehta S, et al; CURE Investigators. Differences in the management and prognosis of women and men who suffer from acute coronary syndromes. J Am Coll Cardiol. 2005;46(10):1845–1851. | ||
Elsaesser A, Hamm CW. Acute coronary syndrome: the risk of being female. Circulation. 2004;109(5):565–567. | ||
Clayton TC, Pocock SJ, Henderson RA, et al. Do men benefit more than women from an interventional strategy in patients with unstable angina or non-ST-elevation myocardial infarction? The impact of gender in the RITA 3 trial. Eur Heart J. 2004;25(18):1641–1650. | ||
Tamis-Holland JE, Palazzo A, Stebbins AL, et al; GUSTO II-B Angioplasty Substudy Investigators. Benefits of direct angioplasty for women and men with acute myocardial infarction: results of the global use of strategies to open occluded arteries in acute coronary syndromes angioplasty (GUSTO II-B) angioplasty substudy. Am Heart J. 2004;147(1):133–139. | ||
Arendarczyk M, Łoboz-Grudzień K. Jakość życia chorych w dwa lata po zawale mięśnia serca. Ocena wpływu czynników. [Quality of life two years after myocardial infarction. 2. Examination of affecting factors] Pol Merkur Lekarski. 2000;8(44):94–97. Polish. | ||
Redberg RF. Gender differences in acute coronary syndrome: invasive versus conservative approach. Cardiol Rev. 2006;14(6):299–302. | ||
Dessotte CA, Dantas RA, Schmidt A, Rossi LA. Health-related quality of life in patients admitted after a first episode of acute coronary syndrome. Rev Lat Am Enfermagem. 2011;19(5):1106–1113. | ||
Dias CC, Mateus P, Santos L, et al. Acute coronary syndrome and predictors of quality of life. Rev Port Cardiol. 2005;24(6):819–831. | ||
Agewall S, Berglund M, Henareh L. Reduced quality of life after myocardial infarction in women compared with men. Clin Cardiol. 2004;27(5):271–274. | ||
Dueñas M, Ramirez C, Arana R, Failde I. Gender differences and determinants of health related quality of life in coronary patients: a follow-up study. BMC Cardiovasc Disord. 2011;11:24. | ||
Kristofferzon M, Löfmark R, Carlsson M. Coping, social support and quality of life over time after myocardial infarction. J Adv Nurs. 2005;52(2):113–124. | ||
Jankowska-Polańska B, Uchmanowicz I, Dudek K, Sokalski L, Łoboz-Grudzień K. Gender differences in health-related quality of life after percutaneous coronary intervention in patients with acute coronary syndrome. Folia Cardiol. 2014;9(3):213–226. | ||
Champney KP, Frederick PD, Bueno H, et al; NRMI Investigators. The joint contribution of sex, age and type of myocardial infarction on hospital mortality following acute myocardial infarction. Heart. 2009;95(11):895–899. | ||
Gan SC, Beaver SK, Houck PM, MacLehose RF, Lawson HW, Chan L. Treatment of acute myocardial infarction and 30-day mortality among women and men. N Engl J Med. 2000;343(1):8–15. | ||
Norris CM, Saunders LD, Ghali WA, et al; APPROACH Investigators. Health-related quality of life outcomes of patients with coronary artery disease treated with cardiac surgery, percutaneous coronary intervention or medical management. Can J Cardiol. 2004;20(12):1259–1266. | ||
Lukkarinen H, Hentinen M. Treatments of coronary artery disease improve quality of life in the long term. Nurs Res. 2006;55(1):26–33. | ||
Westin L, Nilstun T, Carlsson R, Erhardt L. Patients with ischemic heart disease: quality of life predicts long-term mortality. Scand Cardiovasc J. 2005;39(1–2):50–54. | ||
Fagring AJ, Gaston-Johansson F, Kjellgren KI, Welin C. Unexplained chest pain in relation to psychosocial factors and health-related quality of life in men and women. Eur J Cardiovasc Nurs. 2007;6(4):329–336. | ||
Hartman EM, Dulfer K, Utens EM, van den Berge JC, Daemen J, van Domburg RT. Gender differences in quality of life after PCI attenuate after a 10 year follow-up. Int J Cardiol. 2014;176(3):1179–1180. | ||
Van de Werf F, Bax J, Betriu A, et al; ESC Committee for Practice Guidelines (CPG). Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the task force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology. Eur Heart J. 2008;29(23):2909–2945. | ||
Dixon T, Lim LL, Oldridge NB. The MacNew heart disease health-related quality of life instrument: reference data for users. Qual Life Res. 2002;11(2):173–183. | ||
Wrześniewski K. Jak badać jakość życia pacjentów kardiologicznych? [How to assess quality of life of cardiological patients?]. Kardiol Pol. 2009;67(7):790–794. Polish. | ||
Cupples ME, Dempster M. Improving quality of life for patients with angina pectoris: a team approach to disease management. Dis Manage Health Outcomes. 2001;9(9):473–481. | ||
Höfer S, Benzer W, Schüssler G, von Steinbüchel N, Oldridge NB. Health-related quality of life in patients with coronary artery disease treated for angina: validity and reliability of German translations of two specific questionnaires. Qual Life Res. 2003;12(2):199–212. | ||
Bała MM, Płaczkiewicz-Jankowska E, Leśniak W, et al; Under The Patronage Of Diabetes Poland For The Aretaeus-2 Study Group. Management and treatment goals in polish patients with type 2 diabetes of more than ten years’ duration – results of ARETAEUS2-Grupa Study. Endokrynol Pol. 2014;65(3):158–168. | ||
Tykarski A, Narkiewicz K, Gaciong Z, et al. 2015 guidelines for the management of hypertension. Recommendations of the Polish Society of Hypertension – short version. Kardiol Pol. 2015;73(8):676–700. | ||
Włodarczyk D. Płeć a jakość życia i radzenie sobie w okresie roku po zawale serca: czy rzeczywiście mężczyźni górą? [Gender and quality of life and coping over one year after myocardial infarction: do men really have the upper hand?]. Kardiol Pol. Epub 2015 Oct 27. Polish. | ||
Brink E, Grankvist G, Karlson BW, Hallberg LR. Health-related quality of life in women and men one year after acute myocardial infarction. Qual Life Res. 2005;14(3):749–757. | ||
Brown N, Melville M, Gray D, et al. Quality of life four years after acute myocardial infarction: short form 36 scores compared with a normal population. Heart. 1999;81(4):352–358. | ||
Wrześniewski K, Włodarczyk D. Sense of coherence as a personality predictor of quality of life in men and women after myocardial infarction. Kardiol Pol. 2012;70(2):157–163. | ||
Pettersen KI, Reikvam A, Rollag A, Stavem K. Understanding sex differences in health-related quality of life following myocardial infarction. Int J Cardiol. 2008;130(3):449–456. | ||
Souza EN, Quadros AS, Maestri R, Albarrán C, Sarmento-Leite R. Predictors of quality of life change after an acute coronary event. Arq Bras Cardiol. 2008;91(4):229–235. | ||
Kwaśniewska M, Drygas W. Jakość życia u osób obciążonych czynnikami ryzyka choroby niedokrwiennej serca. [Quality of life in patients with risk factors of coronary heart disease] Przegl Lek. 2005;62(9):863–870. Polish. | ||
Hawkes AL, Patrao TA, Ware R, Atherton JJ, Taylor CB, Oldenburg BF. Predictors of physical and mental health-related quality of life outcomes among myocardial infarction patients. BMC Cardiovasc Disord. 2013;13:69. | ||
Beck CA, Joseph L, Bélisle P, Pilote L; QOLAMI Investigators (Quality of life in acute myocardial infarction). Predictors of quality of life 6 months and 1 year after acute myocardial infarction. Am Heart J. 2001;142(2):271–279. | ||
McBurney CR, Eagle KA, Kline-Rogers EM, et al. Health-related quality of life in patients 7 months after a myocardial infarction: factors affecting the short form-12. Pharmacotherapy. 2002;22(12):1616–1622. | ||
Gijsberts CM, Agostoni P, Hoefer IE, et al. Gender differences in health-related quality of life in patients undergoing coronary angiography. Open Heart. 2015;2(1):e000231. | ||
Uchmanowicz I, Loboz-Grudzien K, Jankowska-Polanska B, Sokalski L. Influence of diabetes on health-related quality of life results in patients with acute coronary syndrome treated with coronary angioplasty. Acta Diabetol. 2013;50(2):217–225. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.