")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Sex Differences in the Incidence and Outcomes of COPD Patients Hospitalized with Ischemic Stroke in Spain: A Population-Based Observational Study
Authors de Miguel-Díez J , López-de-Andrés A , Jiménez-García R, Hernández-Barrera V , Jiménez-Trujillo I , Ji Z , de Miguel-Yanes JM, López-Herranz M
Received 19 March 2021
Accepted for publication 4 May 2021
Published 18 June 2021 Volume 2021:16 Pages 1851—1862
DOI https://doi.org/10.2147/COPD.S311826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Javier de Miguel-Díez,1,2 Ana López-de-Andrés,3 Rodrigo Jiménez-García,3 Valentín Hernández-Barrera,4 Isabel Jiménez-Trujillo,4 Zichen Ji,1 José María de Miguel-Yanes,5 Marta López-Herranz6
1Pneumology Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain; 2Department of Medicine, Faculty of Medicine, Universidad Complutense de Madrid, Madrid, Spain; 3Department of Public Health & Maternal and Child Health, Faculty of Medicine, Universidad Complutense de Madrid, Madrid, Spain; 4Preventive Medicine and Public Health Teaching and Research Unit, Health Sciences Faculty, Universidad Rey Juan Carlos, Madrid, Spain; 5Internal Medicine Department, Hospital General Universitario Gregorio Marañón, Universidad Complutense de Madrid, Instituto de Investigación Sanitaria Gregorio Marañón (IiSGM), Madrid, Spain; 6Faculty of Nursing, Physiotherapy and Podology, Universidad Complutense de Madrid, Madrid, 28040, Spain
Correspondence: Ana López-de-Andrés
Department of Public Health & Maternal and Child Health, Faculty of Medicine, Universidad Complutense de Madrid, Madrid, 28040, Spain
Tel +91 394 1523
Fax +91 394 1524
Email [email protected]
Purpose: To compare the incidence, clinical characteristics and outcomes of patients admitted with ischemic stroke (IS) according to the presence of COPD and sex in Spain (2016– 2018).
Patients and Methods: We selected all admissions with IS (≥ 35 years) included in the Spanish National Hospital Discharge Database. We matched each patient suffering COPD with a non-COPD patient with identical age, sex, IS type and year of hospitalization.
Results: IS was coded in 92,524 men and 79,731 women (8.67% with COPD). The incidence of IS was higher in COPD men than in non-COPD men (IRR 1.04; 95% CI 1.03– 1.06), although the differences were not significant among women. COPD men had twice higher incidence of IS than COPD women (IRR 2.00; 95% CI 1.93– 2.07). After matching, COPD men had a higher in-hospital mortality (IHM) than non-COPD men (11.48% vs 9.80%; p< 0.001), and the same happened among women (14.09% vs 11.96%; p=0.002). COPD men received thrombolytic therapy less frequently than non-COPD men. For men and women, the risk of dying in the hospital increased with age, some comorbidities and mechanical ventilation use. After multivariable adjustment, COPD increased the risk of IHM in men (OR 1.16; 95% CI 1.06– 1.28) and women (OR 1.12; 95% CI 1.01– 1.27). Finally, among COPD patients, being women increased the risk of dying during the hospitalization with IS by 15% (OR 1.15; 95% CI 1.03– 1.28).
Conclusion: Incidence of IS was higher in COPD patients, although the difference was only significant for men. COPD was associated with an increased risk of IHM. Among COPD patients, women had higher IHM.
Keywords: ischemic stroke, COPD, sex differences, incidence, in-hospital mortality, Spain
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide. Consequently, it induces a substantial and increasing economic and social burden.1 Much of the disease burden is associated with the management of its comorbidities.2 Cardiovascular diseases rank among the most frequently observed in people with COPD and they could contribute to disease progression, poor clinical outcomes and mortality in this population.3 In recent years, several studies have also shown that COPD may be a risk factor for stroke, another major cause of death worldwide.4,5
The factors linking COPD and stroke are currently not fully understood. It cannot be completely explained by common risk factors such as aging and smoking and has been also attributed to chronic systemic inflammation, tissue hypoxia and oxidative stress.6–9 Anyway, currently there is a growing interest to study lung–brain interactions.
Despite epidemiological and pathophysiological considerations described, scarce information exists on subtypes of stroke in COPD patients.10 Current data suggest that COPD may increase the risk of hemorrhagic stroke.5 In addition, the incidence of other stroke subtypes may also be increased in COPD or may be due to confounding factors. In this sense, recent studies have shown that carotid arteries plaque burden is increased in COPD patients and that these plaques are more prone to rupture, due to an increased lipid content, which could lead to ischemic stroke,11 which is the most common subtype.12
Recently, it has been described that men and women are differently affected by an ischemic stroke. So, for example, women patients with this disease have a higher chance of receiving intraarterial treatment and they have a more favorable in-hospital recovery than men.13 However, to our knowledge, there are no studies that have evaluated the existence of sex differences in patients with stroke based on the presence or not of COPD.
The objectives of this investigation are to assess the differences, according to the presence of COPD and sex, in the incidence of patients admitted with a primary diagnosis of ischemic stroke and to compare their clinical characteristics and in hospital outcomes. We also tried to assess which variables are independently associated with a higher mortality after hospitalization by ischemic stroke among men and women with COPD.
Patients and Methods
Study Design and Data Source
This is an epidemiological retrospective observational study. The database used is the Spanish National Hospital Discharge Database (SNHDD). This database is managed by the Spanish Ministry of Health and collects over 95% of all hospitals (public and private) discharges in Spain. The SNHDD uses the International Classification of Disease version 10 (ICD-10) for coding. The variables and characteristic of the SNHDD can be found online.14
Study Population
We have analyzed data from all subjects aged ≥35 years hospitalized and recorded in the SNHDD from 2016 to 2018. The reason to include only those aged 35 years or over is the very low prevalence of COPD among those aged under this age in Spain.15
Our study population includes subjects discharged with a primary diagnosis of ischemic stroke identified with the ICD-10 codes shown in Supplementary Table S1.
The population was stratified according sex and to the presence or not of a COPD diagnosis code (J44.0, J44.1, and J44.9) in any diagnosis position (2–20).
Study Variables
Our main outcome variables of interest included the incidence of ischemic stroke, in hospital mortality (IHM) and length of hospital stay (LOHS). We also analyzed the use of endovascular thrombectomy and thrombolytic therapy during the hospitalization.
We calculated incidence rates of admission for ischemic stroke hospitalization per 100,000 inhabitants with and without COPD for the period 2016–18. The estimated Spanish population suffering COPD was obtained using data from the 2016/17 Spanish National Health Survey (SNHS2017).16 The SNHS is a periodical survey that constitutes the main source of information on the health of the population residing in Spain. It is performed every six years and is a part of the National Health System’s (NHS) Information System. It collects data on a representative sample of the Spanish Population and yields prevalence estimations of chronic diseases. In the SNHS2017, 23,090 adults aged ≥15 years were interviewed. Using the database of the SNHS2017 we obtained the prevalence of COPD for men and women in the age groups used in our investigation (35–49 years, 50–64 years, 65–79 years and ≥80 years). These specific sex-age group prevalence of COPD were then multiplied by the population living in Spain on 1 July 2017 in each of these sex and age strata. The populations according to age and sex can be freely downloaded from the Spanish National Statistics Institute webpage.17 We then divided the number of ischemic stroke hospitalization among COPD patients in each sex and age group by estimated number of subjects suffering COPD living in Spain in that same sex-age groups to obtain the incidence of ischemic stroke hospitalization per 100,000 persons with COPD. The same method was used to calculate the sex and age group incidences among those without COPD.
Independent variables included sex, age, comorbidities and procedures conducted during the hospital admission. To quantify comorbidity, the Charlson Comorbidity Index (CCI) was calculated for each patient with the algorithms described by Sundararajan et al.18
We specifically also described and compared the prevalence between patients with and without COPD of cardiovascular risk factors (obesity, hypertension, lipid metabolism disorders), chronic diseases present at admission (renal disease, acute myocardial infarction, atrial fibrillation, congestive heart failure, dementia, anemia, peripheral vascular disease, alcohol abuse, depression) and therapeutic procedure (mechanical ventilation, endovascular thrombectomy and thrombolytic therapy). The ICD10 codes used appear in Supplementary Table S1 and reference #18.
Matching Method
We matched within the database of the SNHDD each man suffering COPD with a non-COPD man with identical age, type of ischemic stroke (using up to the second ICD 10 code digit) and year of hospitalization. The same process was done for women. Also, to assess sex differences, a pair matching was done for each COPD woman with a COPD man using the three variables described before.
Statistical Analysis
The statistical analysis was conducted separately for women and men.
Descriptive statistics for continuous variables were reported as means with standard deviation or medians with interquartile range and with absolute frequency and percentage for categorical variables.
To estimate the differences in the incidence between study groups, the statistical method used was Poisson regression. We constructed models adjusted by age and sex or only age depending on the groups being compared.
Student’s t-test or Mann–Whitney test was used to compare means and medians, respectively. Prevalence and proportions were compared with the chi-square tests.
Multivariable logistic regression models were constructed, using IHM as the dependent variable, to identify those variables independently associated with dying during the hospital admission after ischaemic stroke. Separate models for men, women and both sexes according to the presence of COPD were constructed following the recommendations of Hosmer et al.19
Stata version 14 (Stata, College Station, Texas, USA) was the statistical software for matching and descriptive and bivariate and multivariable analytical statistics. Two-sided P-value of <0.05 was the cut-point used for significance.
Sensitivity Analysis
To confirm the results of the pair matching method, we also analyzed the database without matching to assess the effect of sex on the IHM among all COPD patients hospitalized with ischemic stroke using multivariable logistic regression. Finally, we also analyzed all men and women hospitalized with ischemic stroke to confirm the possible influence of COPD in the IHM using the same statistical method.
Ethical Aspects
The SHDD database can be requested by any researcher from the Spanish Ministry of Health using the online questionnaire.20 According to Spanish law, the use of anonymized databases provided by official bodies does not require authorization from an Ethics Committee. This is so because the Ministry of Health only transfers the data if all ethical requirements are guaranteed.
Results
The number of hospital discharges in Spain from 2016 to 2018 for patients aged 35 years or over with a primary diagnosis of ischemic stroke was 172,255, men represent 53.71% (N=92,524) and women 46.29% (N=79,731). The overall prevalence of COPD was 8.67% (10.91% for men and 6.08% for women; p<0.001).
Incidence of Ischemic Stroke According to COPD Status
As can be seen in Table 1, the total crude incidence of ischemic stroke is higher (P<0.001) among the COPD population (1025.07 per 100,000 persons with COPD) than among those without COPD (566.78 per 100,000 persons without COPD), resulting in an age-sex-adjusted IRR of 1.02 (95% CI 1.01–1.03).
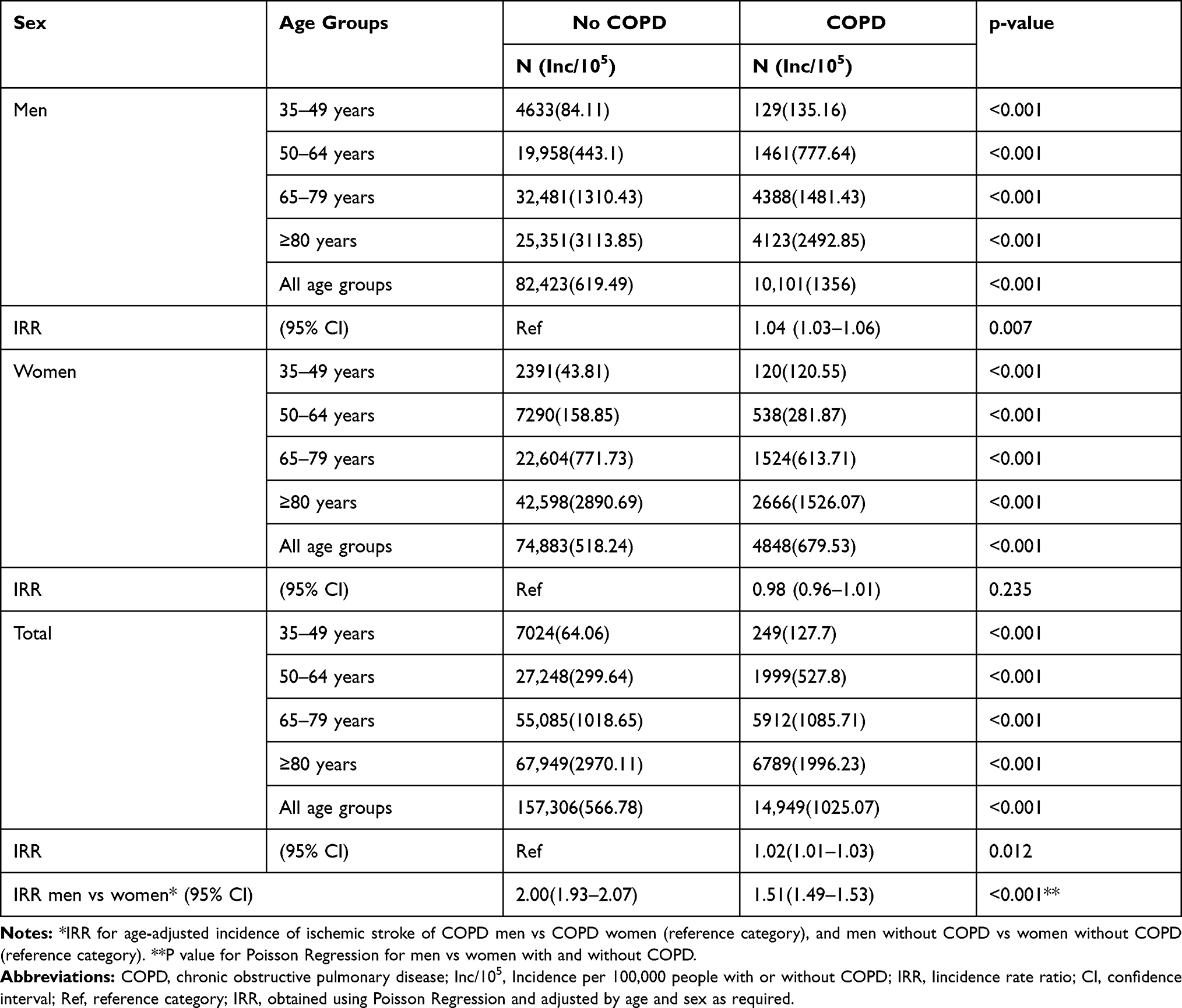 |
Table 1 Incidence of Ischemic Stroke Hospitalizations According to Presence of COPD, Sex and Age Groups |
According to sex, we found that among men with COPD the ischemic stroke incidence was significantly higher (1356 vs 619.49; Age-adjusted IRR 1.04 95% CI 1.03–1.06) than among non-COPD men. Among women, we found no differences in the age adjusted incidence of ischemic stroke (IRR 0.98; 95% CI 0.96–1.01).
Men with COPD had twice higher age-adjusted incidence of ischemic stroke than COPD women (IRR 2.00; 95% CI 1.93–2.07). Among men without COPD the age-adjusted incidence was also higher than in non-COPD women (IRR 1.51; 95% CI 1.49–1.53).
Clinical Characteristics and Hospital Outcomes for Men and Women with Ischemic Stroke According to COPD Status
The clinical characteristics, therapeutic procedures and hospital outcomes before and after pair-matching by age and ischemic stroke type for men hospitalized with ischemic stroke according to the presence of COPD are shown in Table 2.
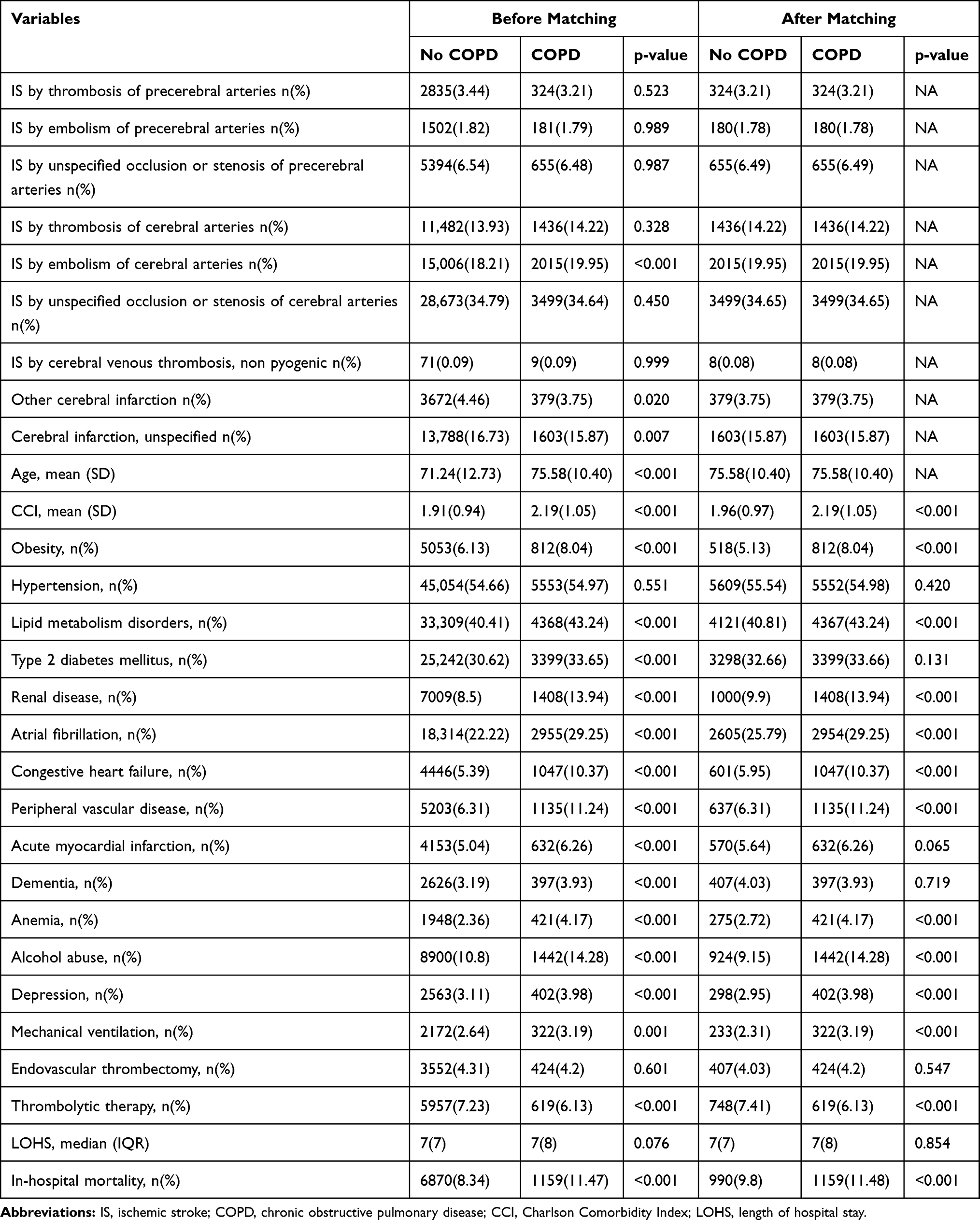 |
Table 2 Clinical Characteristics, Use of Therapeutic Procedures and Hospital Outcomes Before and After Matching by Age and Ischemic Stroke Type (ICD 10) for Men Hospitalized with Ischemic Stroke According to the Presence of COPD |
After matching, men with COPD have more mean number of comorbid conditions according to the CCI than non-COPD men (2.19 vs 1.96; p<0.001). Remarkably higher is the prevalence of obesity, lipid metabolism disorders, renal disease, atrial fibrillation, congestive heart failure, peripheral vascular disease, anemia and depression. The prevalence of alcohol abuse was also higher among COPD men (14.28% vs 9.15%; p<0.001).
After matching, COPD men have more frequently received mechanical ventilation (3.19% vs 2.31%; p<0.001); however, they received less thrombolytic therapy than non-COPD men (6.13% vs 7.41%; p<0.001). IHM was significantly higher in COPD men than in men without COPD (11.48% vs 9.8%; p<0.001).
When we compare women with and without COPD who suffered ischemic stroke before and after matching, we obtain the results shown in Table 3. Like described for men, women with COPD have significantly higher mean CCI (2.09 vs 1.90; p<0.001). Also, alcohol abuse and the prevalence of most clinical conditions were higher among matched COPD women. However, hypertension and dementia were significantly more frequent among non-COPD women (58.99% and 6.79% vs 55.92% and 5.78%, respectively; p<0.001).
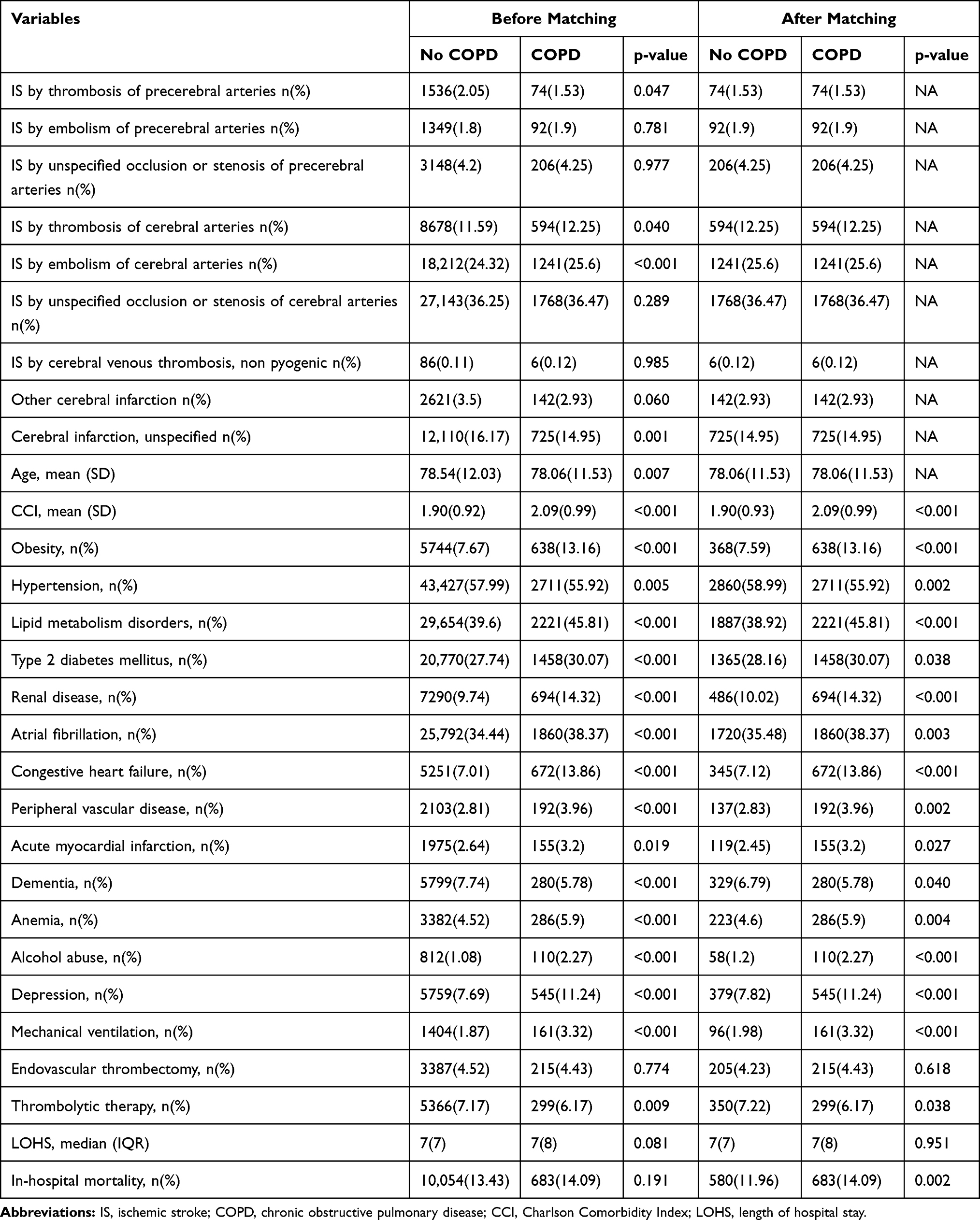 |
Table 3 Clinical Characteristics, Use of Therapeutic Procedures and Hospital Outcomes Before and After Matching by Age and Ischemic Stroke Type (ICD 10) for Women Hospitalized with Ischemic Stroke According to the Presence of COPD |
Regarding procedures and hospital outcomes, we found that after matching, women with COPD have more frequently a code for mechanical ventilation (3.32% vs 1.98%; p<0.001). The IHM was significantly different higher among COPD women after matching (14.09% vs 11.96%; p=0.002).
Clinical Characteristics and Hospital Outcomes for COPD Patients with Ischemic Stroke According to Sex
As can be seen in Table 4, after matching, COPD men who suffered ischemic stroke had a higher mean CCI than COPD women (2.22 vs 2.09; p<0.001). Specifically, men had higher prevalence of type 2 diabetes mellitus (32.68% vs 30.52; p=0.025), renal disease (15.91% vs 14.03; p=0.011), peripheral vascular disease (10.34% vs 4.06%; p<0.001) and acute myocardial infarction (6.37% vs 3.09%; p<0.001); however, they had lower prevalence of obesity, hypertension, lipid metabolism disorders, atrial fibrillation, congestive heart failure, anemia and depression. Also, men had a higher prevalence of alcohol abuse than women (12.45% vs 2.31%; p<0.001).
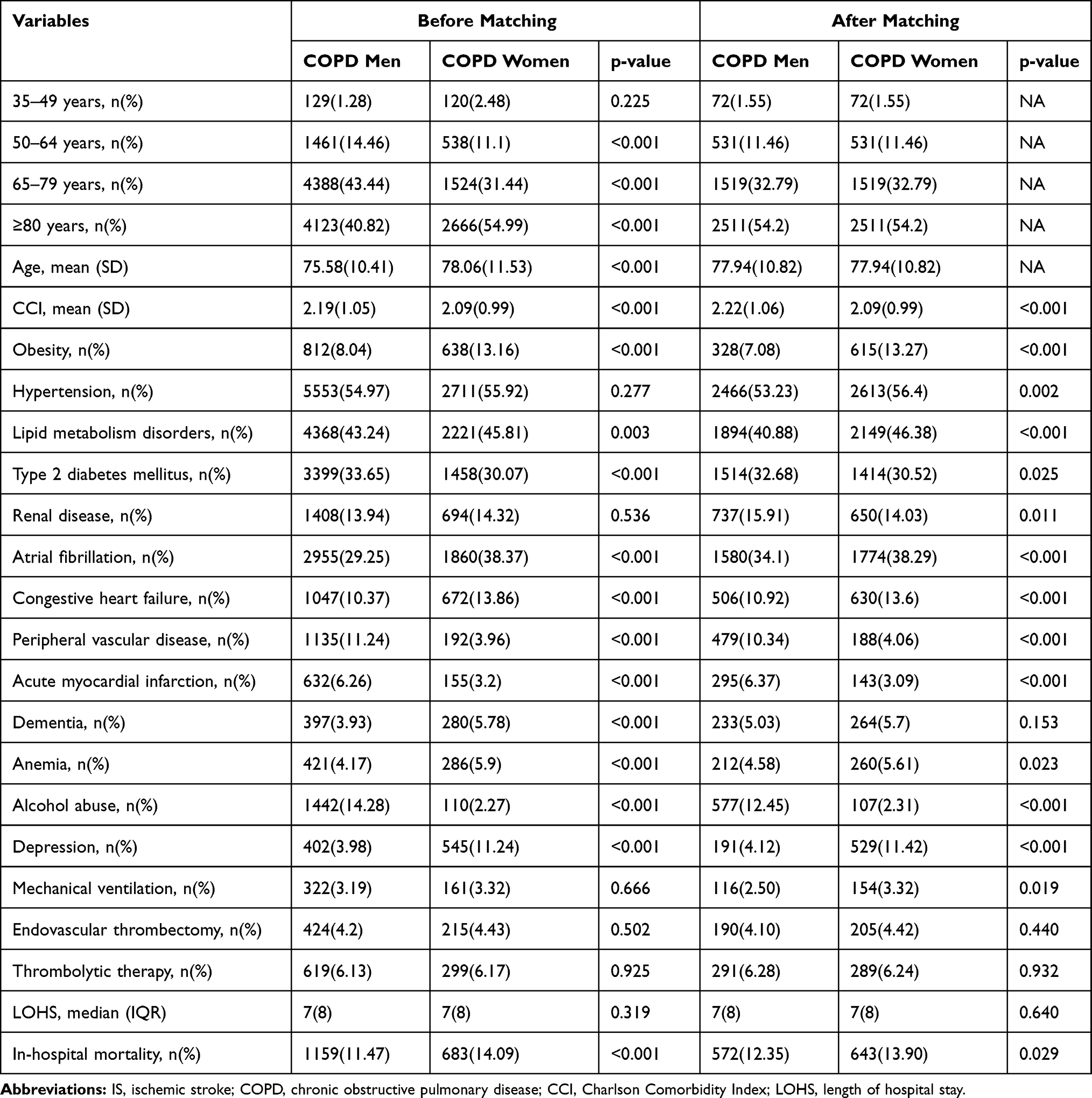 |
Table 4 Clinical Characteristics, Use of Therapeutic Procedures and Hospital Outcomes Before and After Matching by Age (ICD 10) Among Men and Women Suffering COPD Hospitalized with Ischemic Stroke |
Use of mechanical ventilation was higher in COPD women than men (3.32% vs 2.5%; p=0.019). Endovascular thrombectomy and thrombolytic therapy showed no significant difference between men and women. IHM rate was 13.9% for COPD women and 12.35% for matched COPD men (p=0.029).
Multivariable Analysis of Variables Associated with IHM Among Men and Women with COPD
The results of the multivariable logistic regression analysis among COPD patients with ischemic stroke are shown in Table 5.
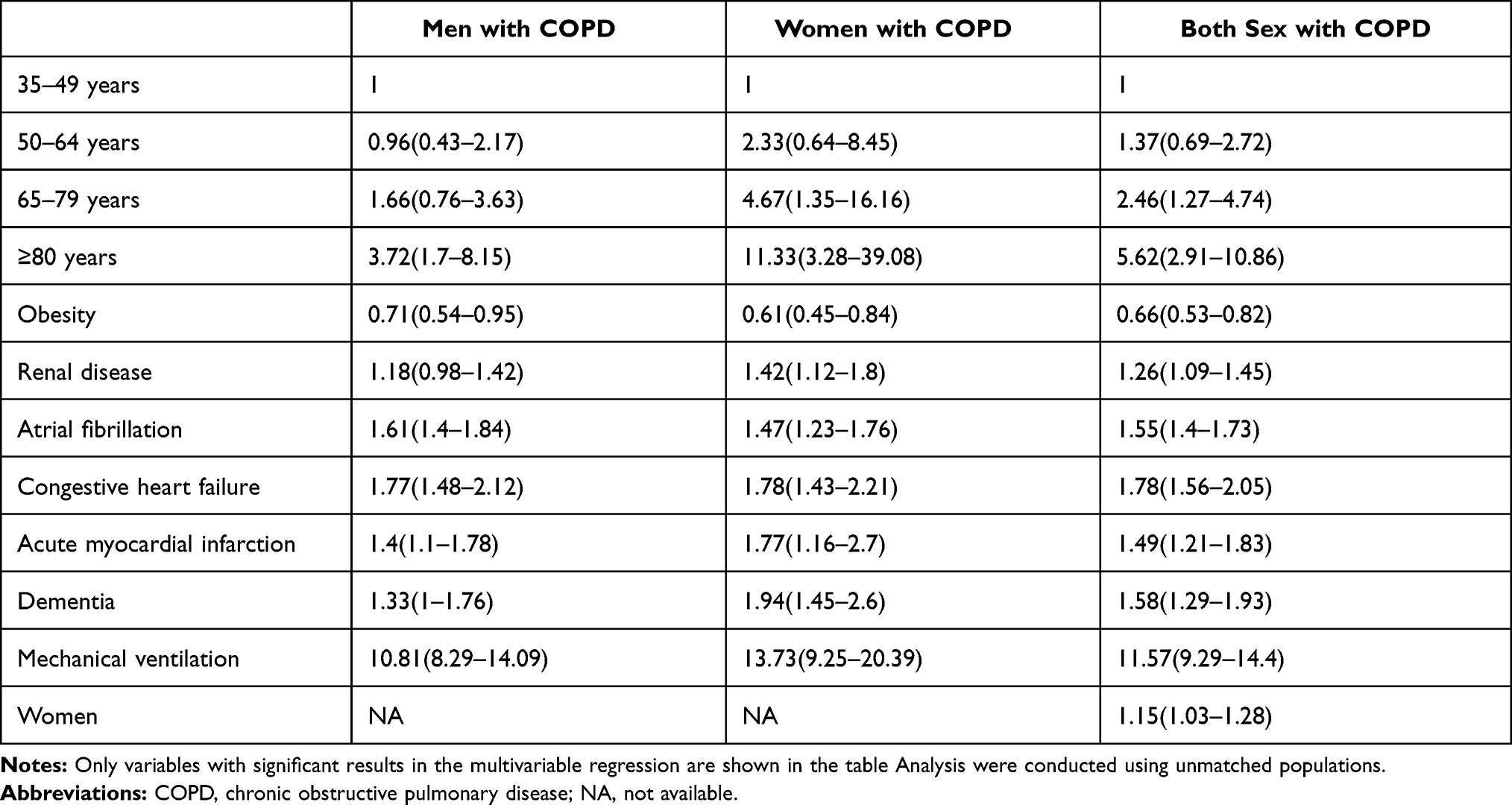 |
Table 5 Multivariable Logistic Regression Analysis of Factors Associated with in Hospital Mortality Among Men and Women Suffering COPD Hospitalized with Ischemic Stroke |
For men and women, the risk of dying in the hospital increased with age, atrial fibrillation, congestive heart failure, acute myocardial infarction, dementia and the need of mechanical ventilation during the hospitalization. In women, renal disease is also a risk factor of dying in the hospital (OR 1.42; 95% CI 1.12–1.8). Obesity reduced the IHM in both sexes.
Sensitivity Analysis
The sensitivity analysis confirmed the result obtained in the pair matched analysis as we found that, after logistic multivariable regression using the unmatched population (Table 5), women with COPD had a significantly higher risk of dying during the hospitalization than men with COPD (OR 1.15; 95% CI 1.03–1.28).
Finally, using the entire database including all men and women with ischemic stroke and after multivariable adjustment (Supplementary Table S2), COPD increasing the risk of dying during the hospitalization in both men (OR 1.16; 95% CI 1.06–1.28) and women (OR 1.12; 95% CI: 1.01–1.27), therefore ratifying the results of the matched analysis.
Discussion
In this large population-based study, we found that COPD patients had an increased incidence of ischemic stroke and a higher IHM than non-COPD population. By sex, we observed the incidence of ischemic stroke was higher in COPD men than in non-COPD men; COPD men had twice higher incidence of ischemic stroke than COPD women; being women increased the risk of dying during the hospitalization with ischemic stroke.
In the current study, we found a prevalence of COPD among ischemic stroke patients of 8.67%, slightly lower than the 12.16% reported by Lekoubou et al using the National Inpatient Sample, a national representative dataset of US hospital admissions.21 However, in a nationwide population-based cohort of Swedish residents, a lower prevalence was provided, of only 3.27%.22 The different design of the studies, especially the latter, which was population-based, could justify the results obtained.
We also found that the incidence of ischemic stroke was slightly but significantly higher in COPD patients than in those without COPD. The increase of ischemic stroke risk in people with COPD found in this study is consistent with previous findings.10 Although the reasons for the associations remain unclear, it has been suggested that systemic inflammation and high levels of cholesterol could be of importance for ischemic stroke development.23,24
Additionally, our analysis showed, for the first time, that the higher incidence of ischemic stroke in COPD patients was only significant for men. The smaller sample size of women with COPD in our study might justify these results.
To our knowledge, the incidence of ischemic stroke in COPD according to sex has not been previously reported. Our analysis also reported that men with COPD had twice higher adjusted incidence of ischemic stroke than COPD women. Among men without COPD, the adjusted incidence was also higher than in non-COPD women but with a lower IRR (1.51; 95% CI 1.49–1.53) suggesting that the negative effect of being a women is stronger among those who also suffer COPD.
We showed that COPD men received thrombolytic therapy less frequently than non-COPD men. Although the factors related to this fact have not been adequately clarified, a potential explanation is that physicians could consider COPD patients as high risk for complications due they are deemed to be older and with higher frailty.21 However, no differences were found in our study in the use of such therapy in COPD women compared to non-COPD women. On the other hand, the use of mechanical ventilation was higher in men and women with COPD than in those without this disease.
The association between COPD status and mortality in ischemic stroke patients has not been extensively studied.21 Our study confirmed that IHM was significantly higher in COPD men and women than in those without COPD. Similar results have been described by other authors.25 Several factors may explain the increased mortality risk among patients with COPD. They include comorbid conditions that can be associated with increased mortality,26 increased risk of dysphagia, that may predispose to the development of aspiration pneumonia in these patients,27 gas exchange disturbances (hypoxemia and hypercapnia) and inflammation and oxidative stress during exacerbations.2,28
When we compared matched men and women with COPD, the IHM rate was higher for COPD women compared with COPD men. However, to our knowledge, no clinical study has been conducted so far with the aim of assessing sex-differences in stroke outcomes among COPD patients. However, epidemiological studies in the general population have shown that both ischemic stroke risk and outcome following stroke are sexually dimorphic.29–35
Women have been reported to have an overall lower ischemic stroke incidence rate than men in studies conducted in Spain and elsewhere, even if the incidences depend on age.29,31,35 On the other hand, several, but not all, investigations have found higher mortality among women.13,29–35
From a pathophysiological point of view, the reasons underlying such sex differences are complicated and probably occur as a consequence (or combination) of biological factors, like genetic predisposition, sex hormones and neuro-humoral pathways, as well as psychosocial, behavioural, and environmental factors.31–34
There is evidence for sex differences in ischemic sensitivity and cellular death pathways.31–34 Experimental studies point that women are more susceptible to neuronal cell death induced by activation of cytochrome-c and caspases, enzymes that play key roles in programmed cell death and inflammation.31 Another theory for biological differences includes chromosomal influences. In a study of aged mice with depleted or depleting oestrogen, those with two X chromosome had larger infarcts, higher neurologic deficits and greater immune-cell infiltration and activation compared to those with an X chromosome and a Y chromosome.31
Sex hormone studies have reported that lower oestrogen levels in postmenopausal women reduce the anti-inflammatory and neuroprotective effects of the hormone. Explanations for the protective effect of oestrogen include dilation of blood vessels and improvement of blood flow, as well as induction of anti-inflammatory factors.31–34 It is well established that oestrogens inhibit the development of atherosclerotic plaques due to their effects on smooth muscle, adhesion molecules and differentiation of monocytes. Consequently, higher circulating levels of oestrogens may protect females from the development of thrombotic strokes in younger ages explaining their lower incidence.31 Sex differences in coagulation and fibrinolysis, rate of progression of atherosclerosis and endothelial function in have also been associated with different outcomes after stroke.32
Previous investigations have suggested that differences in the baseline concomitant chronic conditions and cardiovascular risk factors prevalence and control can act as confounders in the sex-differences for mortality after stroke.32–34,36 Among these baseline conditions, atrial fibrillation has a special relevance.37,38 In a meta-analysis involving over four million patients, atrial fibrillation was associated with a higher risk for stroke, as well as all-cause mortality cardiac events and cardiovascular mortality, in women than men.37 Atrial fibrillation is associated to 45% of all cardioembolic-subtype strokes.30 Cardioembolic strokes have been linked to more severe strokes, higher mortality, and poorer functional outcomes.30,33,37,38
In our investigation atrial fibrillation prevalence was significantly higher among COPD women than COPD men before (38.37% vs 29.25%; p<0.001) and after PSM (38.29% vs 34.1%; p<0.001). The increased prevalence of atrial fibrillation, and consequently cardioembolic strokes in COPD women, may contribute to sex differences in mortality after ischemic stroke in our investigation.30,33,37,38 In Spain, Purroy et al after analysing registry data of 13,932 consecutive ischemic stroke patients from 19 Spanish hospitals confirmed that women suffered more cardioembolic strokes (43.3%) than men (30.2%) and had a higher IHM.35
It has been reported that nonconventional stroke symptoms are more prevalent in women than men.33,34 Furthermore, these non-traditional symptoms of stroke may lead to a delay in recognition and treatment of stroke resulting in higher mortality.33,34
Finally, worse outcomes among women may result from worse access to adequate therapies or diagnostic procedures when compared with men.34 Further investigations in this topic are necessary.
Our analysis showed that mortality risk factors in COPD men and women with ischemic stroke were similar to those that has been reported in other analyses.39,40 However, this is the first publication of in-hospital stroke mortality in COPD patients according to sex and could form the basis for future research including development of risk scores and identifying modifiable risk factors.
On the other hand, our study results support the obesity paradox among men and women suffering COPD hospitalized with ischemic stroke. These findings are consistent with other studies, which have shown that patients with higher BMI have lower mortality after stroke.41–43 Although the underlying reasons for this protective effect are poorly understood, one possible explanation could be hypoxic preconditioning.42
The current study has some limitations. First, this was a retrospective analysis of an administrative database; hence, a relatively small percentage of missing data or miscoded diagnoses is possible. Second, data on stroke severity, airflow obstruction degree, biomarkers, or medication, were not available for our analysis. Third, in this inpatient sample, we were unable to capture stroke deaths outside the hospital. Despite the limitations mentioned, the major strength of our study was the size of the database that included a large nationally representative sample of hospitalized patients, therefore increasing the generalizability of our findings.
Conclusion
In conclusion, this study revealed that incidence of ischemic stroke was higher in COPD patients than in those without COPD, although the difference was only significant for men. On the other hand, COPD men had twice higher incidence for ischemic stroke than COPD women. Finally, COPD was associated with an increased risk of IHM in both men and women with ischemic stroke and women with COPD had higher IHM than men with this condition. Our findings suggest that additional efforts are warranted in the protection of patients with COPD to reduce their medical burden and mortality. Prospective studies are required to further clarify this relationship between COPD, sex and ischemic stroke.
Acknowledgments
We thank the Spanish Ministry of Health for providing us with the database.
Funding
This research was funded by the Sociedad Española de Neumología y Cirugía Torácica (SEPAR), grant number 733 of the 2018 edition.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Available from: https://goldcopd.org.
2. Austin V, Crack PJ, Bozinovski S, et al. COPD and stroke: are systemic inflammation and oxidative stress the missing links? Clin Sci (Lond). 2016;130:1039–1050. doi:10.1042/CS20160043
3. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:155–161. doi:10.1164/rccm.201201-0034OC
4. Sin DD, Anthonisen NR, Soriano JB, et al. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28:1245–1257. doi:10.1183/09031936.00133805
5. Corlateanu A, Covantev S, Mathioudakis AG, et al. Chronic obstructive pulmonary disease and stroke. COPD. 2018;15:405–413. doi:10.1080/15412555.2018.1464551
6. Feary JR, Rodrigues LC, Smith CJ, et al. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65:956–962. doi:10.1136/thx.2009.128082
7. Maclay JD, MacNee W. Cardiovascular disease in COPD: mechanisms. Chest. 2013;143:798–807. doi:10.1378/chest.12-0938
8. Barnes PJ. Chronic obstructive pulmonary disease: effects beyond the lungs. PLoS Med. 2010;7:e1000220. doi:10.1371/journal.pmed.1000220
9. Geltser BI, Kurpatov IG, Kotelnikov VN, et al. Chronic obstructive pulmonary disease and cerebrovascular diseases: functional and clinical aspect of comorbidity. Ter Arkh. 2018;90:81–88. doi:10.26442/terarkh201890381-88
10. Söderholm M, Inghammar M, Hedblad B, et al. Incidence of stroke and stroke subtypes in chronic obstructive pulmonary disease. Eur J Epidemiol. 2016;31:159–168. doi:10.1007/s10654-015-0113-7
11. Lahousse L, Tiemeier H, Ikram MA, et al. Chronic obstructive pulmonary disease and cerebrovascular disease: a comprehensive review. Respir Med. 2015;109:1371–1380. doi:10.1016/j.rmed.2015.07.014
12. Feigin VL, Lawes CM, Bennett DA, et al. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. doi:10.1016/S1474-4422(09)70025-0
13. Bonkhoff AK, Karch A, Weber R, et al. Female stroke: sex differences in acute treatment and early outcomes of acute ischemic stroke. Stroke. 2021;52:406–415. doi:10.1161/STROKEAHA.120.032850
14. Ministerio de Sanidad, Servicios Sociales e Igualdad. Real Decreto 69/2015, de 6 de febrero, por el que se regula el Registro de Actividad de Atención Sanitaria Especializada. (Spanish National Hospital Discharge Database). BOE. 2015;35:10789–10809.
15. Soriano JB, Alfageme I, Miravitlles M, et al. Prevalence and determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2021;57:61–69. doi:10.1016/j.arbres.2020.07.024
16. Ministry of Health. Spanish national health survey 2017 [Encuesta Nacional de Salud de España 2017]; 2017. Available from: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2017.htm.
17. Spanish National Statistics Institute. Population estimates according to sex and age; 2021. Available from: https://www.ine.es/jaxiT3/Tabla.htm?t=31304.
18. Sundararajan V, Henderson T, Perry C, et al. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57:1288–1294. doi:10.1016/j.jclinepi.2004.03.012
19. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression.
20. Ministerio de Sanidad, Consumo y Bienestar Social. Solicitud de extracción de datos – extraction request (Spanish National Hospital Discharge Database); 2021. Available from: https://www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SolicitudCMBDdocs/2018_Formulario_Peticion_Datos_RAE_CMBD.pdf.
21. Lekoubou A, Ovbiagele B. Prevalence and influence of chronic obstructive pulmonary disease on stroke outcomes in hospitalized stroke patients. eNeurologicalSci. 2017;6:21–24. doi:10.1016/j.ensci.2016.11.007
22. Yin L, Lensmar C, Ingelsson E, Bäck M. Differential association of chronic obstructive pulmonary disease with myocardial infarction and ischemic stroke in a nation-wide cohort. Int J Cardiol. 2014;173:601–603. doi:10.1016/j.ijcard.2014.03.140
23. Johnston AK, Mannino DM, Hagan GW, et al. Relationship between lung function impairment and incidence or recurrence of cardiovascular events in a middle-aged cohort. Thorax. 2008;63:599–605. doi:10.1136/thx.2007.088112
24. Hozawa A, Billings JL, Shahar E, et al. Lung function and ischemic stroke incidence: the atherosclerosis risk in communities study. Chest. 2006;130:1642–1649. doi:10.1378/chest.130.6.1642
25. Yen YS, Harnod D, Lin CL, et al. Long-term mortality and medical burden of patients with chronic obstructive pulmonary disease with and without subsequent stroke episodes. Int J Environ Res Public Health. 2020;17:2550. doi:10.3390/ijerph17072550
26. Terzano C, Conti V, Di Stefano F, et al. Comorbidity, hospitalization, and mortality in COPD: results from a longitudinal study. Lung. 2010;188:321–329. doi:10.1007/s00408-009-9222-y
27. Martino R, Foley N, Bhogal S, et al. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke. 2005;36:2756–2763. doi:10.1161/01.STR.0000190056.76543.eb
28. Portegies ML, Lahousse L, Joos GF, et al. Chronic obstructive pulmonary disease and the risk of stroke. The Rotterdam study. Am J Respir Crit Care Med. 2016;193:251–258. doi:10.1164/rccm.201505-0962OC
29. Appelros P, Stegmayr B, Terént A. Sex differences in stroke epidemiology: a systematic review. Stroke. 2009;40:1082–1090. doi:10.1161/STROKEAHA.108.540781
30. Bushnell C, McCullough LD, Awad IA, et al. Guidelines for the prevention of stroke in women: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:1545–1588. doi:10.1161/01.str.0000442009.06663.48
31. Bushnell CD, Chaturvedi S, Gage KR, et al. Sex differences in stroke: challenges and opportunities. J Cereb Blood Flow Metab. 2018;38:2179–2191. doi:10.1177/0271678X18793324
32. Roy-O’Reilly M, McCullough LD. Age and sex are critical factors in ischemic stroke pathology. Endocrinology. 2018;159:3120–3131. doi:10.1210/en.2018-00465
33. Gibson CL, Attwood L. The impact of gender on stroke pathology and treatment. Neurosci Biobehav Rev. 2016;67:119–124. doi:10.1016/j.neubiorev.2015.08.020
34. Carcel C, Woodward M, Wang X, Bushnell C, Sandset EC. Sex matters in stroke: a review of recent evidence on the differences between women and men. Front Neuroendocrinol. 2020;59:100870. doi:10.1016/j.yfrne.2020.100870
35. Purroy F, Vena A, Forné C, et al. Age- and sex-specific risk profiles and in-hospital mortality in 13,932 Spanish stroke patients. Cerebrovasc Dis. 2019;47:151–164. doi:10.1159/000500205
36. Renoux C, Coulombe J, Li L, et al. Confounding by pre-morbid functional status in studies of apparent sex differences in severity and outcome of stroke. Stroke. 2017;48:2731–2738. doi:10.1161/STROKEAHA.117.018187
37. Emdin CA, Wong CX, Hsiao AJ, et al. Atrial fibrillation as risk factor for cardiovascular disease and death in women compared with men: systematic review and meta-analysis of cohort studies. BMJ. 2016;532:h7013. doi:10.1136/bmj.h7013
38. Lang C, Seyfang L, Ferrari J, et al. Do women with atrial fibrillation experience more severe strokes? Results from the Austrian stroke unit registry. Stroke. 2017;48:778–780. doi:10.1161/STROKEAHA.116.015900
39. Viderman D, Issanov A, Temirov T, et al. Outcome predictors of stroke mortality in the neurocritical care unit. Front Neurol. 2020;11:579733. doi:10.3389/fneur.2020.579733
40. Popat C, Ruthirago D, Shehabeldin M, et al. Outcomes in patients with acute stroke requiring mechanical ventilation: predictors of mortality and successful extubation. Am J Med Sci. 2018;356:3–9. doi:10.1016/j.amjms.2018.03.013
41. Olsen TS, Dehlendorff C, Petersen HG, et al. Body mass index and poststroke mortality. Neuroepidemiology. 2008;30:93–100. doi:10.1159/000118945
42. Chaudhary D, Khan A, Gupta M, et al. Obesity and mortality after the first ischemic stroke: is obesity paradox real? PLoS One. 2021;16:e0246877. doi:10.1371/journal.pone.0246877
43. Huang ZX, Gu HQ, Yang X, et al. Risk factors for in-hospital mortality among acute ischemic stroke patients in China: a nationwide prospective study. Neurol Res. 2020;1–9. doi:10.1080/01616412.2020.1866356.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.