")
Back to Journals » Substance Abuse and Rehabilitation » Volume 11
Sex Differences in Substance Use and Misuse: A Toxicology Investigators’ Consortium (ToxIC) Registry Analysis
Authors Beauchamp GA, Carey JL , Hurwitz MB, Tully BN, Cook MD, Cannon RD, Katz KD, Koons AL, Kincaid H, Greenberg MR
Received 17 May 2020
Accepted for publication 6 August 2020
Published 29 September 2020 Volume 2020:11 Pages 23—31
DOI https://doi.org/10.2147/SAR.S263165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christine Timko
Gillian A Beauchamp,1,2 Jennifer L Carey,3 Mikayla B Hurwitz,1 Briana N Tully,1 Matthew D Cook,1,2 Robert D Cannon,1,2 Kenneth D Katz,1,2 Andrew L Koons,1,2 Hope Kincaid,4 Marna Rayl Greenberg1 On Behalf of the Toxicology Investigators Consortium (ToxIC)
1Department of Emergency and Hospital Medicine, Lehigh Valley Health Network/University of South Florida (USF) Morsani College of Medicine, Allentown, PA 18103, USA; 2Section of Medical Toxicology, Department of Emergency and Hospital Medicine, Lehigh Valley Health Network/USF Morsani College of Medicine, Allentown, PA 18103, USA; 3Division of Medical Toxicology, Department of Emergency Medicine, University of Massachusetts Medical School, Worcester, MA 01655, USA; 4Network Office of Research and Innovation, Lehigh Valley Health Network/USF Morsani College of Medicine, Allentown, PA 18103, USA
Correspondence: Marna Rayl Greenberg 1909 Earls Court, Allentown, PA 18103, USA
Tel +1 610-967-3140
Email [email protected]
Background: Variations between male and female populations are previously reported in classes of harmfully used/misused drugs, severity of substance use disorder and risk of relapse. The aim of this study was to provide a review of bedside medical toxicologist managed, sex-specific poisonings in adults that present with harmful drug use/misuse.
Methods: ToxIC Registry cases ≥ 19 and ≤ 65 years old, with harmful drug use or misuse during the timeframe June 2010–December 2016, were studied. Demographics, primary agents of toxic exposure, administration route and complications were analyzed. Descriptive methods were used in the analysis.
Results: The database included 51,440 cases. Of these, 3426 cases were analyzed in which the primary reason for the encounter was harmful substance use/misuse. Females were found to harmfully use/misuse pharmaceutical drugs (N=806, 65.6%) more than nonpharmaceutical drugs (N=423, 34.4%). Males more frequently used nonpharmaceutical drugs (N=1189, 54.1%) than pharmaceutical drugs (1008, 45.9%). Analgesics were used by females (N= 215, 18.2%) and males (N=137, 6.6%). Sedative hypnotics were used by females (N=165, 14%) and males (N=160, 7.8%). Psychoactive agents were used by males (N=325, 15.8%) and females (N=67, 5.7%). Sympathomimetics were used by males (N=381, 18.5%) and females (N=151, 12.8%). The majority of both male and female participants, 1712 (57.9%), utilized an oral route of administration. However, 312 (16.5%) of males utilized inhalation vs 73 (6.8%) of females inhaled their substance.
Conclusion: There were sex-specific differences among patients evaluated for harmful substance use/misuse by toxicologists. Considering these differences in regards to management and preventive approaches may be indicated.
Keywords: gender studies, substance use, toxicology, overdose, substance misuse
Introduction
Harmful use of substances is an ongoing worldwide problem. Prior research has found that many risk factors contribute to harmful substance use and overdose.1 There are many factors that contribute to the risk of overdose, such as intravenous administration, poly-drug use, drug impurity, and even brief abstinence preceding exposure.1 Due to the complexities that contribute to harmful substance use, the CDC continues to recommend research and development into strategies to mitigate risk for those vulnerable to overdose by identifying what substance use profiles to anticipate from an individual.1 Previous research has found a variety of sex-based differences around harmful substance use.2 In a study looking at people who filled an opioid prescription, the authors found that women received lower opioid doses than men, but were more likely to have antidepressant, benzodiazepine, or zolpidem prescriptions.3 Becker et al also found that women began self-administering illicit and licit drugs at lower doses, but experience a quicker increase in their addiction to these drugs, as well as a higher difficulty of cessation.4,5 Another study found that women reported more prescription opioid use in their lifetime than men.6 Graziani et al specifically studied oxycodone and hydrocodone and found that, although the pharmacokinetic and pharmacodynamic effects do not differ significantly between males and females, females tend to experience more gastrointestinal adverse reaction from their use than males.7
While there is not much known about how sex plays a role in post-discharge referrals, it is known that females with substance use disorders tend to experience greater financial issues, health difficulties, risk for recurrence of use,4 and mental health morbidity.3 It has been reported that women experience greater adverse symptoms after cessation of drug use, as well as worse effects on their mood and anxiety levels, which could help explain their increased risk of recurrence of use.5 The misuse of, and addiction to, opioids is a serious national crisis in the United States. Strategies to mitigate risk factors and provide data to continue the expansion of risk assessment tools are needed to help mitigate harmful use in the adult population.8
Additional research in sex factors in adults that affect harmful use of substances may allow us to find novel early sex-specific prevention programs, early intervention assessments, as well as risk assessment tools to hone our strategies.1 The influence of sex and gender on diagnosis, management, and even substance use prevention has been discussed previously in the literature.1,8 For instance, there are differences between the sexes in diagnoses related to opioid disbursement, response to opioids, opioid use disorder, pain, pain perception, and psychosocial factors.9 Treatments for opioid use disorder generally focus on a uniform perspective that does not appropriately target these differences.9
United States’ trends demonstrate increased heroin use while nonmedical prescription opioid use is decreasing.10 Although recent studies have shown that both heroin and nonmedical prescription opioid use are more prevalent in men than women, women are increasingly using heroin at a faster rate and lessening use of nonmedical prescription opioids at a slower rate than me.10 It has been found that substance use disorder progresses more rapidly in women than in men; this factor may contribute to the reason for women with harmful substance use becoming the quickest-growing population in the United States.11 Full exploration and knowledge of differences between males and females could lead to separate prevention and treatment programs, identification of medical and psychiatric comorbidities, and interventions for them, tailored by sex.11
This identification of observed sex differences among adult patients may provide us with the additional information that will have implications for prevention, management, and treatment measures. Given broad access to electronic medical records, additional information on sex differences may be beneficial with multiple different applications; for example, using flags within the EMR system when a medication is prescribed to high-risk groups could alert a provider of precaution with prescribing certain medications (in particular if prescribing to those with risk factors like depression or anxiety disorders). Substance use recovery may require treatment that expands the parameters of acute hospitalization; prior studies have shown that more women compared to men are discharged to non-detox-related facilities which may influence relapse in this population.2 Reviewing additional information on a simplistic level of patient differentiation, such as sex, helps identify and target specialized risk-mitigating strategies to these groups.1
This study’s aim was to provide a review of bedside medical toxicologist managed, sex-specific poisonings in adults that present with harmful drug use/misuse.
Materials and Methods
The study data were obtained from the Toxicology Investigator’s Consortium (ToxIC) registry. The American College of Medical Toxicology (ACMT) produced the ToxIC registry in 2010 to compile data from medical toxicologists that were recorded in outpatient and inpatient settings. Medical toxicologists at numerous institutions nationally and internationally participate voluntarily by entering de-identified information into an online data collection form for all patients evaluated in person. The data collected include multiple demographic factors including sex, age and race; setting of consultation; clinical presentation; provided interventions; poisoning type; and the reason for toxicological exposure.
The study protocol was reviewed by the lead author’s institutional review board (IRB) and due to the nature of the database, being deidentified and a part of national registry, it was determined that it did not require IRB review. The following were obtained from the ToxIC registry: data regarding the reason for drug abuse/misuse, not including self-harm intent; single vs multiple exposures; type of exposure (acute, chronic or acute-on-chronic); agent of exposure; route of administration; clinical complications, including vital sign abnormalities, cardiovascular effects, neurological effects, life support and death; and treatment, including pharmacologic support, CPR, ECMO and intubation/ventilation. The analyses in this study included all cases in the ToxIC registry for patients age ≥19 and ≤65 with substance misuse or abuse between January 2010 and December 2016. Cases with missing data for age, or primary reason for encounter, or whose reason for intentional encounter was not misuse/abuse were excluded from analysis. Descriptive statistics were used to assess study variables by sex. For purposes of this paper, the ToxIC registry term “drug abuse” was reported consistent with newer nomenclature as “harmful substance use.”12
Results
The registry had 51,440 cases between 01/2010-12/2016. The sex distribution in the registry was similar with 25,871 (50.3%) females and 25,569 (49.7%) males. Of the 51,440, a total of 34,255 were between the ages of 19–65, among which, 3426 were included for misuse/harmful use of a pharmaceutical or nonpharmaceutical substance (Figure 1, Flow Diagram). Table 1 depicts the demographics for the study sample according to sex. There were 2179 (64%) male subjects and 1229 (36%) female subjects, 24 (2%) of whom were pregnant. In regards to race, 1626 (55%) were reported as Caucasian and 653 (22.1%) had an unknown/uncertain race.
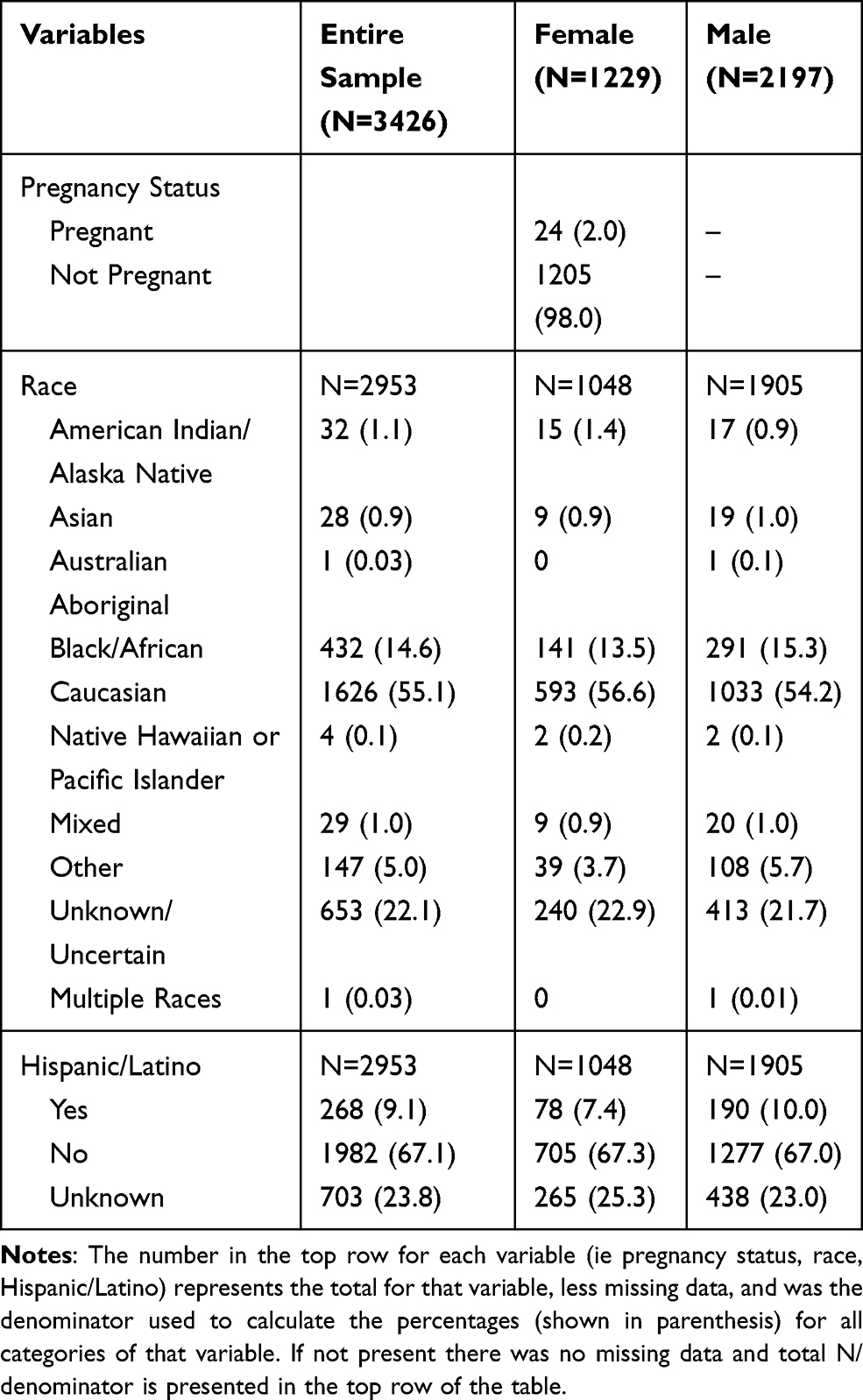 |
Table 1 Demographics |
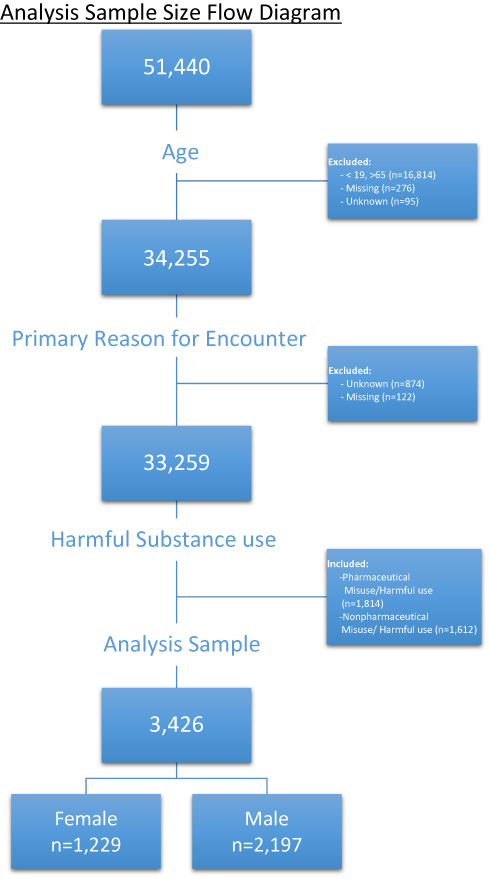 |
Figure 1 Flow diagram. |
Table 2 represents the harmful substance use/misuse information including reason for use, number of uses, agent of exposure and route of administration. Females were found to harmfully use/misuse pharmaceutical drugs more than nonpharmaceutical drugs: 806 (65.6%) of females used pharmaceutical drugs and 423 (34.4%) used nonpharmaceutical drugs. Of the females with reported pharmaceutical drug use, 312 (39.4%) were taking a prescribed medication more than intended and 167 (21.1%) were taking the medication to elicit a pleasurable sensation. Males were found to use nonpharmaceutical drugs more frequently than pharmaceutical drugs: 1008 (45.9%) of males used pharmaceutical drugs and 1189 (54.1%) used nonpharmaceutical drugs.
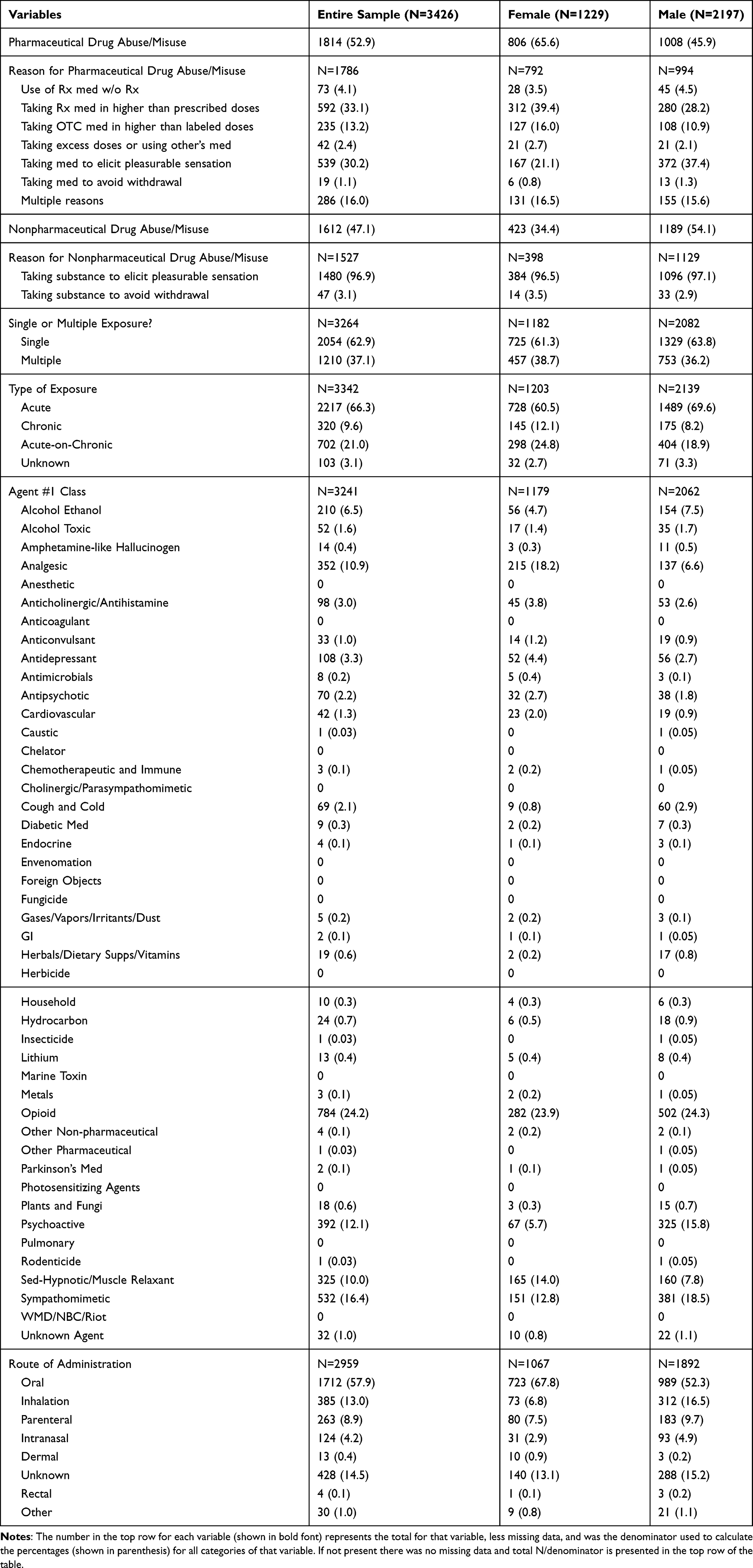 |
Table 2 Harmful Drug Use/Misuse Information |
Regarding the agent of exposure, opioids were the most commonly identified drugs among the entire sample: 784 (24.2%) of the cases reported opioids as the agent of exposure. Of the total of female and male participants, 282 (23.9%) females and 502 (24.3%) males were reported with opioids as agent of exposure. Sex differences were observed for other agents of exposure. Analgesics were used by females (N= 215, 18.2%) and males (N=137, 6.6%). Sedative hypnotics were used by females (N=165, 14%) and males (N=160, 7.8%). Psychoactive agents were used by males (N=325, 15.8%) and females (N=67, 5.7%). Sympathomimetics were used by males (N=381, 18.5%) and females (N=151, 12.8%).
The majority of both male and female participants, 1712 (57.9%), utilized an oral route of administration. However, 312 (16.5%) of males utilized inhalation, vs 73 (6.8%) of females inhaled their substance.
Table 3 shows the complications experienced by the participants, including systemic involvement (cardiovascular and nervous system), life support, pharmacologic support, CPR, ECMO and intubation/ventilation. Major vital sign abnormalities were reported, with 64.3% of females and 60.3% of males reported with none. Of the nervous system complications reported on, 39.9% of females and 38.5% of males experienced coma. Pharmacological support data were provided and benzodiazepines were used as a treatment method for 49.0% of males in comparison to 35.2% of females.
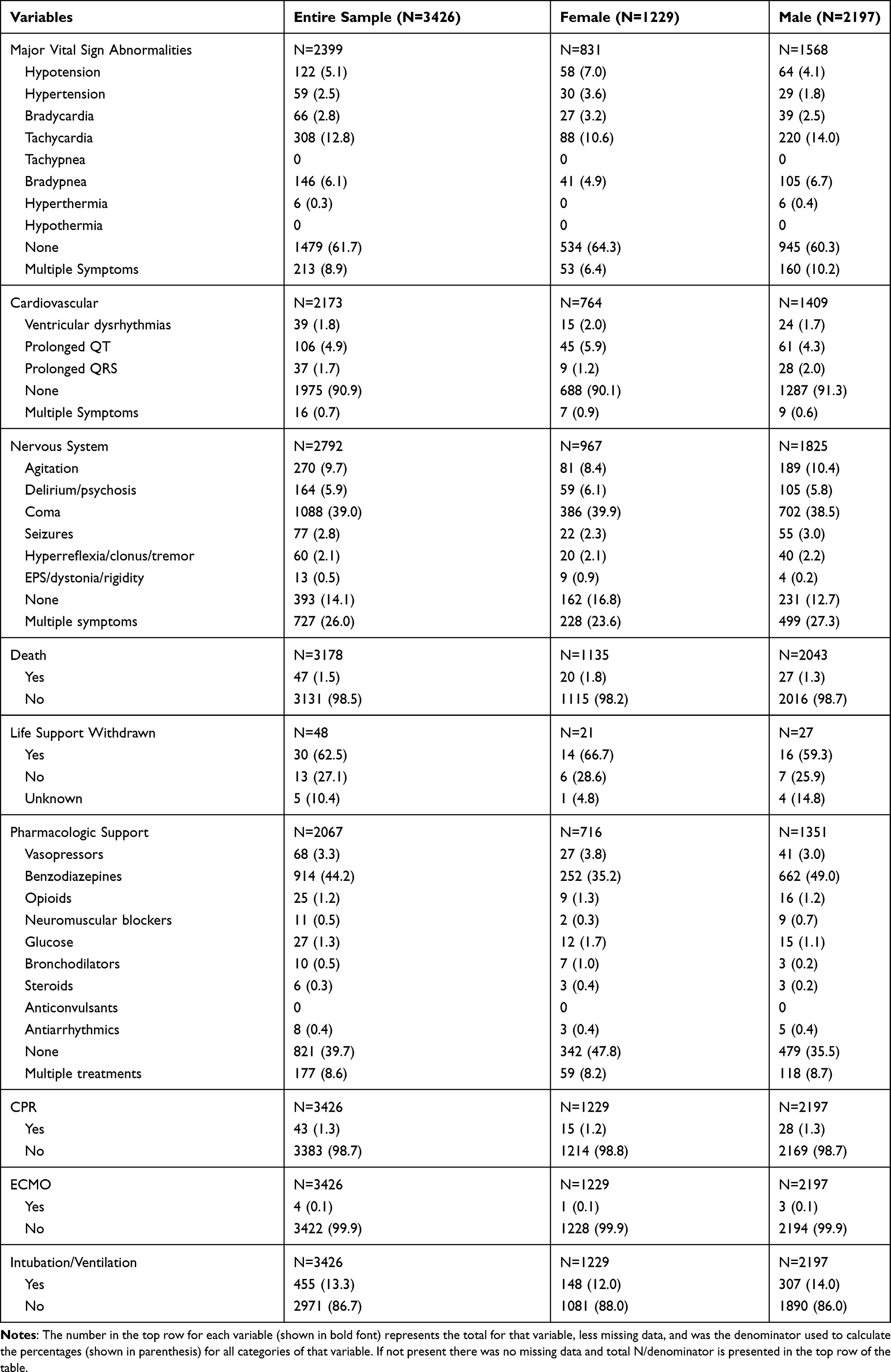 |
Table 3 Complications |
Discussion
Research on differences between sexes with respect to harmful substance use has been expanding in recent years. The 2016 National Survey on Drug Use and Health found differences in the percentages of illicit drug use by females and males in both 2015 and 2016, with males having a higher percentage of illicit drug use.13 Currently, the opioid epidemic is on the forefront of public health concerns. Our study found opioids to be the most common agent involved in harmful substance use among both males and females, but there did not appear to be a difference between the sexes in regard to the percentage who used opioids compared to other agents of exposure. This finding is inconsistent with a previous study that found in the United States, opioid use disorder was reported at significantly higher rates among women.14 However, this same study also discussed results similar to our own. They discussed that women were more likely than men to use prescription drugs and were also more likely to have concurrent use of sedative-hypnotics.14 Additionally, we found that a higher percentage of women used sedative-hypnotics and analgesics, when compared to the percentage of men that used these two agents. Men were found to have a higher rate of harmful use of psychoactive and sympathomimetic drugs.
Consistent with previous research, the results reported here demonstrate prominent disparities between the sexes with regards to pharmacological toxicities. For instance, a previous study found that females are more likely to start using drugs in order to self-medicate and reduce symptoms of mental disorders or illnesses.15 This is paralleled with our findings that females more often misused pharmaceutical drugs by taking a prescribed medication at a higher dose than medically indicated as opposed to an attempt to elicit a pleasurable response. The clear differences noted in the results of our study can be expanded upon and employed clinically to further progress how we app n b roach harmful use.
By broadening the awareness within the medical community of the differences between sexes in regard to harmful substance use, more effort can be put toward customizing treatment options for patients. For example, exercise intervention for substance use disorder has gained popularity in recent years and some research has explored differences between sexes in response to this treatment.16 Studies have found that long-term consistent aerobic exercise can help reduce smoking risks in young males and helps to increase recovery from methamphetamine dependency for men.17 However, these results were not found to be true for female participants.18 Additionally, a body-mind exercise called Qigong has been utilized as a meditation therapy to diminish symptoms of withdrawal related to substance use. It was found that females may be more responsive to meditative therapy than males since females tend to suffer from more severe withdrawal symptoms.19 The differences between how males and females respond to exercise and meditation treatment for substance use disorder are simple examples of why treatment is not “one size fits all.” The data obtained in this study can be utilized to direct future sex-specific harmful use screening techniques and treatments, as well as guide future research on the subject. Treatment for physical medical conditions is often tailored to the individual and it should be no different for harmful substance use. Further research should focus on how different treatments benefit males vs females in order to optimize outcomes and reduce withdrawal symptoms and recurrence of use.
The data forms used in the ToxIC database are completed on an elective basis at participating sites in the registry and are based on many factors. Examples for consideration could include availability or time-constraints for facilities, as well as severity and urgency of the cases, all of which may reflect a better or, more likely, a worse prognosis for cases excluded from the registry in comparison to included cases.
Therefore, cases in the ToxIC registry are not necessarily inclusive of all the toxicological consults that are completed. Therefore, comparative and perhaps more meaningful statistical analyses were not considered for our data. Readers must keep this in mind when considering the results. Incomplete, contradictory, or missing data form information resulted in the exclusion of many cases. Analyses were performed based only on the main agent considered responsible for the toxicological encounter. Thus, we could not evaluate the effects of drug interactions or multiple drugs contributing to the whole toxicological picture. Finally, the study of substance use varies over time and this dataset can only illustrate outcomes within our parameters from 2011 to 2016. The impact of these limitations on our study findings is not known.
Conclusion
We reported on characteristics of patient evaluated for harmful substance use/misuse by toxicologists. There were sex-specific differences among patients in their reason for use, number of uses, agent of exposure and route of administration. Considering these differences in regards to management and preventive approaches may be indicated.
Data Sharing Statement
The data used for this study are not listed on a public database but is available for review upon request of the communicating author.
Ethical Statement
The authors and Lehigh Valley Health Network have followed all COPE ethical guidelines and confirm that the data accessed complied with data protection and privacy regulations.
Acknowledgments
The authors would like to acknowledge the scholarly assistance of Lexis Laubach, BS and Lauren Crowley, BA.
Funding
This work was supported by the Dorothy Rider Pool Trust for Health Research and Education community foundation grant number 2017 1573-015.
Disclosure
Hope Kincaid reports grants from Dorothy Rider Pool Trust for Health Research and Education Community Foundation Grant, during the conduct of the study. The authors report no other potential conflicts of interest for this work.
References
1. Khatiwoda P, Proeschold-Bell RJ, Meade CS, Park LP, Proescholdbell S. Facilitators and Barriers to Naloxone Kit Use Among Opioid-Dependent Patients Enrolled in Medication Assisted Therapy Clinics in North Carolina. N C Med J. 2018;79(3):149–155. doi:10.18043/ncm.79.3.149
2. Manuel JI, Lee J. Gender differences in discharge dispositions of emergency department visits involving drug misuse and abuse-2004–2011. Subst Abuse Treat Prev Policy. 2017. doi:10.1186/s13011-017-0114-5
3. Liang Y, Goros MW, Turner BJ. Drug overdose: differing risk models for women and men among opioid users with non-cancer pain. Pain Med. 2016;17(12):2268–2279. doi:10.1093/pm/pnw071
4. Becker JB, Hu M. Sex differences in drug abuse. Front Neuroendocrinol. 2008;29(1):36–47. doi:10.1016/j.yfrne.2007.07.003.
5. Becker JB, McClellan ML, Reed BG. Sex Differences, Gender and Addiction. J Neurosci Res. 2017;95(1–2):136–147. doi:10.1002/jnr.23963.
6. Serdarevic M, Striley CW, Cottler LB. Gender differences in prescription opioid use. Curr Opin Psychiatry. 2017;30(4):238–246. doi:10.1097/YCO.0000000000000337.
7. Graziani M, Nistico R. Gender difference in prescription opioid abuse: a focus on oxycodone and hydrocodone. Pharmacol Res. 2016;108:31–38. doi:10.1016/j.phrs.2016.04.012.
8. Greenberg MR, Safdar B, Choo EK, McGregor AJ, Becker LB, Cone DC. Future directions in sex- and gender-specific emergency medicine. Acad Emer Med. 2014;21(12):1339–1342. doi:10.1111/acem.12520
9. Banta-Green CJ, Coffin PO, Schoeppe JA, Merrill JO, Whiteside LK, Ebersol AK. Heroin and pharmaceutical opioid overdose events: emergency medical response characteristics. Drug Alcohol Depend. 2017;178:1–6. doi:10.1016/j.drugalcdep.2017.04.021
10. Marsh JC, Park K, Lin YA, Bersamira C. Gender differences in trends for heroin use and nonmedical prescription opioid use, 2007–2014. J Subst Abuse Treat. 2018;87:79–85. doi:10.1016/j.jsat.2018.01.001
11. Ait-Daoud N, Blevins D, Khanna S, Sharma S, Holstege CP. Women and Addiction. Psychiatric Clin North Am. 2017;40(2):285–297. doi:10.1016/j.psc.2017.01.005
12. Substance Use Disorders: A Guide to the Use of Language. (2004). The National Alliance of Advocates for Buprenorphine Treatment. https://www.naabt.org/documents/Languageofaddictionmedicine.pdf.
13. 2016 National Survey on Drug Use and Health: Detailed Tables. (2017). Center for Behavioral Health Statistics and Quality. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf.
14. Koons AL, Rayl Greenberg M, Cannon RD, Beauchamp GA. Women and the Experience of Pain and Opioid Use Disorder: A Literature-based Commentary. Clin Ther. 2018;40(2):190–196. doi:10.1016/j.clinthera.2017.12.016
15. Becker JB, Perry AN, Westenbroek C. Sex differences in the neural mechanisms mediating addiction: A new synthesis and hypothesis. Biol Sex Differences. 2012;3(1):14. doi:10.1186/2042-6410-3-14
16. Zhou Y, Zhao M, Zhou C, Li R. Sex differences in drug addiction and response to exercise intervention: from human to animal studies. Front Neuroendocrinol. 2016;40:24–41. doi:10.1016/j.yfrne.2015.07.001
17. Horn K, Dino G, Branstetter SA, et al. Effects of physical activity on teen smoking cessation. Pediatrics. 2011;128(4):e801–e811. doi:10.1542/peds.2010-2599
18. Dolezal BA, Chudzynski J, Storer TW, et al. Eight weeks of exercise training improves fitness measures in methamphetamine-dependent individuals in residential treatment. J Addict Med. 2013;7(2):122–128. doi:10.1097/ADM.0b013e318282475e
19. Chen KW, Comerford A, Shinnick P, Ziedonis DM. Introducing Qigong Meditation into Residential Addiction Treatment: A Pilot Study Where Gender Makes a Difference. J Alter Complement Med. 2010;16(8):875–882. doi:10.1089/acm.2009.0443
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.