")
Back to Journals » Clinical Ophthalmology » Volume 15
Sex Differences in Rate of Axial Elongation and Ocular Biometrics in Elementary School Students
Authors Terasaki H, Yamashita T, Asaoka R, Yoshihara N, Kakiuchi N, Sakamoto T
Received 12 August 2021
Accepted for publication 6 October 2021
Published 27 October 2021 Volume 2021:15 Pages 4297—4302
DOI https://doi.org/10.2147/OPTH.S333096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hiroto Terasaki,1,* Takehiro Yamashita,1,* Ryo Asaoka,2– 5 Naoya Yoshihara,1 Naoko Kakiuchi,1 Taiji Sakamoto1
1Department of Ophthalmology, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan; 2Department of Ophthalmology, Seirei Hamamatsu General Hospital, Shizuoka, Japan; 3Seirei Christopher University, Shizuoka, Japan; 4Nanovision Research Division, Research Institute of Electronics, Shizuoka University, Shizuoka, Japan; 5The Graduate School for the Creation of New Photonics Industries, Shizuoka, Japan
*These authors contributed equally to this work
Correspondence: Hiroto Terasaki
Department of Ophthalmology, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan
Tel +81 99-275-5402
Fax +81 99-265-4894
Email [email protected]
Purpose: To determine the relationship between the ocular biometrics and axial length (AL) elongation and its rate in elementary school children.
Methods: This is a prospective observational study of 102 right eyes of third-grade elementary school students who were 8 to 9 years old. All participants underwent measurements of the AL, anterior chamber depth (ACD), and lens thickness (LT) annually for 3 years. The AL elongation during the first half and second half was calculated by subtracting the AL of the 1st year from that at the 2nd year, and AL of the 3rd year minus 2nd year. The total AL elongation (TALE) was obtained by summing up the first and second half AL elongations. The growth rate change (GRC) was obtained by subtracting the first half AL elongation from second half AL elongation. Spearman correlations were used to determine the correlation between the 1st year ocular biometrics and the TALE and GRC.
Results: The mean TALE was 0.54 ± 0.26 mm in boys and 0.46 ± 0.31 mm in girls. The mean GRC was 0.00 ± 0.16 mm in boys and − 0.04 ± 0.14 mm in girls. In boys and girls, the TALE was significantly larger in the eyes with myopic ocular biometrics such as a deeper ACD, thinner LT, and longer AL during the 1st year (|r|=0.41 to 0.46, P < 0.05). The GRC was significantly accelerated in the eyes of only the girls with hyperopic ocular biometrics such as a shallower ACD, thicker LT, and shorter AL during the 1st year (|r|=0.31 to 0.41, P< 0.05).
Conclusion: In boys and girls, the TALE tends to be larger in eyes with myopic biometrics at the 1st year examination. The GRC tended to accelerate in the eyes with hyperopic ocular biometry during the 1st year only in girls.
Keywords: axial elongation rate, axial length, school myopia
Introduction
Myopia is one of the most common eye diseases, and pathological myopia is a major cause of blindness.1,2 The prevalence of myopia is increasing worldwide, and the socioeconomic impact on individuals and society is substantial.3–6 In Asian countries, it is becoming a more serious problem7–9 because the increasing incidence, and the age of the onset is becoming younger.3,4 Individuals with myopia have a significantly higher incidence of glaucomatous optic neuropathy, and those with high myopia have a higher risk of glaucoma than those with low to moderate myopia.9 Therefore, it is important to understand myopic changes such as axial length (AL) elongation during the growth phase in young children.
On average, the growth rate of the AL decreases with increasing age in children.10,11 However, the speed of AL elongation also varies among individuals, and the rate of myopia progression accelerates in some eyes.12,13 In addition, myopic changes in the eyes of young adults, such as retinal vascular shift, conus, and optic disc head tilt, tend to be more prevalent in eyes with longer axial lengths. However, there are also eyes with shorter axial lengths with greater myopic changes in the fundus and, conversely, eyes with longer axial lengths with almost no myopic changes.14 Because most myopic fundus changes occur in school-age children,15 we hypothesized that there are eyes in which the ocular structures are hyperopic in early school-age children but the ocular axial elongation is accelerated. In addition, there are eyes in which the ocular structure is myopic and the axial length elongation is decelerated. Furthermore, it has been found that there are sex differences in the ocular structures.16
Thus, we hypothesized that the ocular biometrics, such as the anterior chamber depth (ACD), lens thickness (LT), and AL, affects the growing pattern of the AL during the growth phase of an individual. Therefore, the purpose of this study was to determine the relationship between the ocular biometrics and rate of AL elongation in 8- and 9-year-old elementary school boys and girls.
Methods
Ethics Statement
All of the procedures used conformed to the tenets of the Declaration of Helsinki, and they were approved by the Ethics Committee of Kagoshima University Hospital. A written informed assent and informed consent were obtained from all subjects and their parents. This study was registered with the University Hospital Medical Network-clinical trials registry (No. UMIN000015239).
Subjects
This was part of a longitudinal, prospective, observational study of third-grade students who were 8- to 9-years old at the first examination. The students attended the Elementary School of the Faculty of Education of Kagoshima University. This Kagoshima University-affiliated school was participating in a cooperative research study with our ophthalmological department. Although it was unintended, it is highly likely that the parents of these children at this elementary school had a higher socioeconomic status. Thus, the children may have been more myopic.
There were 144 students in the third grade. An informed consent was obtained from 122 (87.4%) students and their parents. The students were examined from November 17 to December 18, 2014 in the initial year and were examined during the same period annually for three years. Six students were excluded due to truancy or transfer. Fourteen eyes were excluded because of the difficulty in measuring the ACD and LT. In the end, the right eyes of 102 individuals were used for the analyses. Color fundus photographs were taken with the 3D OCT-1 Maestro (Topcon, Tokyo, Japan), and the AL, ACD, and the LT were measured with the OA-2000 Optical Biometer (Tomey, Nagoya, Japan).
Calculation and Classification of Rate of Axial Elongation
The AL, ACD, and LT were measured annually for 3 years without cycloplegia. The AL elongation of first period was calculated by subtracting the 1st year AL from the 2nd year AL, and the AL elongation during the second period was calculated by subtracting the 2nd year AL from the 3rd year AL. Then, the total AL elongation (TALE) was calculated by summing up the first and second periods of AL elongations. The growth rate change (GRC) was obtained by subtracting the AL elongation of second period from the AL elongation in the first period. These calculations were performed for only the right eye. A minus GRC value indicated a deceleration, and a plus GRC value indicated an acceleration of the AL elongation rate.
Statistical Analyses
All statistical analyses were performed with the SPSS statistics 21 for Windows (SPSS Inc., IBM, Somers, New York, USA). The significance of the sex differences of the ocular biometrics in the first year was determined by Mann–Whitney U-tests. The significance of the differences between AL elongation of first period and that of second period was determined by Wilcoxon signed rank tests. Spearman correlations were used to determine whether there were significant correlations between the 1st year ocular biometric values and the TALE and GRC values.
Results
The subjects included 50 boys and 52 girls. The mean ± standard deviation of the ocular biometrics are shown in Table 1. The AL elongation during the second half was significantly smaller than the first half AL elongation in girls (P = 0.022) but not in boys (P = 0.117). The mean ± standard deviation of the GRC (second half AL elongation minus first half AL elongation) was 0.00 ± 0.16 mm in boys and −0.04 ± 0.14 mm in girls. The AL elongation speed of 22 eyes (21.6%, 14 eyes of boys, 8 eyes of girls) accelerated (GRC was more than 0.05 mm), 43 eyes (42.2%, 18 eyes of boys, 25 eyes of girls) were stable (GRC was between −0.05 and 0.05 mm), and 37 eyes (36.3%) (boys 18 eyes, girls 19 eyes) decelerated (GRC was less than −0.05 mm) during this period.
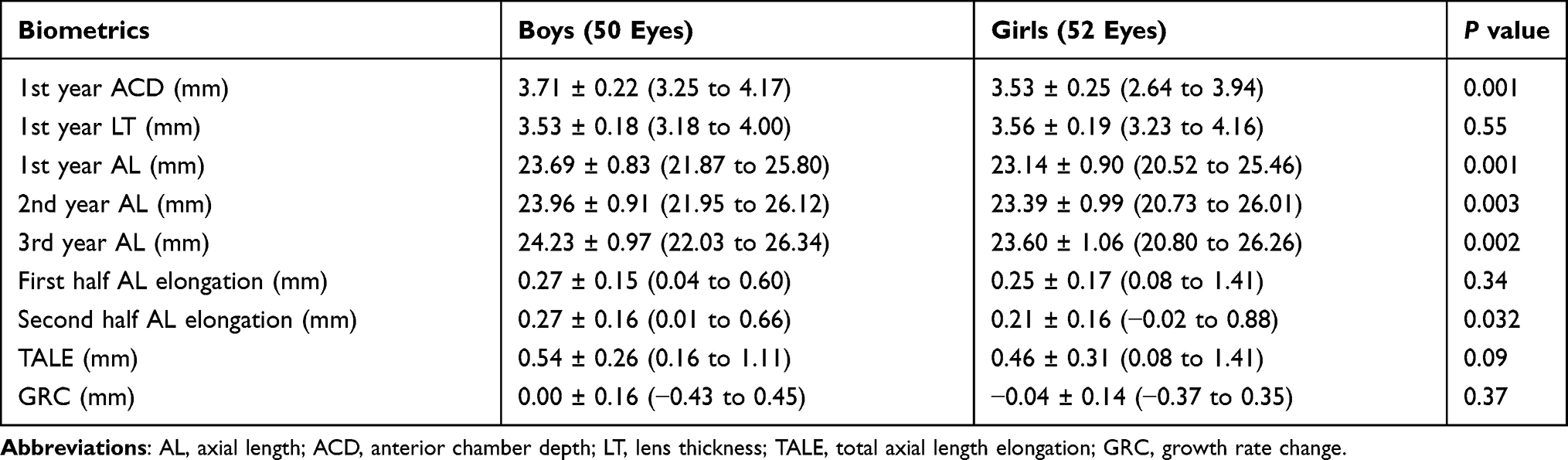 |
Table 1 Ocular Biometrics of Boys and Girls |
The ACD and AL during the 1st year and the AL during the 2nd year and the 3rd year AL and second half AL elongation of boys were significantly larger than those of girls (P < 0.05). The 1st year LT, first half AL elongation, TALE, and GRC were not significant different between boys and girls (Table 1).
In boys, the TALE was significantly larger in the eyes with myopic ocular biometrics such as a deeper ACD (r = 0.45, P = 0.001), thinner LT (r = −0.46, P = 0.001), and longer AL (r = 0.42, P = 0.002) at the initial examination. In girls, the TALE was significantly larger in the eyes with myopic ocular biometric values such as a deeper ACD (r = 0.41, P = 0.002), thinner LT (r = −0.44, P = 0.001), and longer AL (r = 0.42, P = 0.002) at the 1st year (Figure 1A–C).
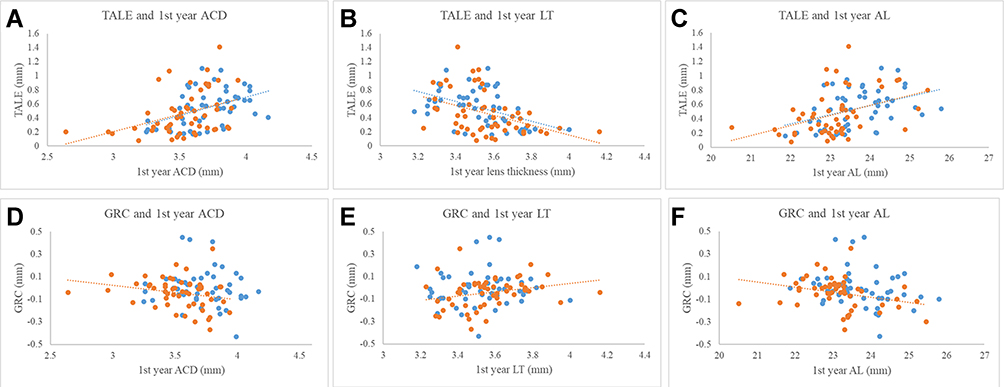 |
Figure 1 Scatter plot of the first year ocular biometrics, viz., the anterior chamber depth (ACD), lens thickness (LT), axial length (AL), and total axial length elongation (TALE) (A–C), and growth rate change (GRC) (D–F) in boys (blue dots) and girls (red dots). In boys, the TALE was significantly larger in the eyes with myopic ocular biometrics such as a deeper ACD (r = 0.45, P = 0.001, (A), thinner LT (r = −0.46, P = 0.001, (B), and longer AL (r = 0.42, P = 0.002, (C) at the initial examination. In girls, the TALE was significantly larger in the eyes with myopic ocular biometric values such as a deeper ACD (r = 0.41, P = 0.002, (A), thinner LT (r = −0.44, P = 0.001, (B), and longer AL (r = 0.42, P = 0.002, (C) at the 1st year. The GRC accelerated significantly in the eyes of girls only with hyperopic ocular biometrics such as a shallower ACD (r = −0.32, P = 0.022, (D), thicker LT (r = 0.31, P = 0.027, (E), and shorter AL (r = −0.41, P = 0.003, (F) at the 1st year measurements. Similar tendencies were observed in boys (ACD, r = −0.09, P = 0.52, D; LT, r = 0.07, P = 0.65, E; AL, r = −0.27, P = 0.055, (F), but the differences were not significant. |
The GRC accelerated significantly in the eyes of girls only with hyperopic ocular biometrics such as a shallower ACD (r = −0.32, P = 0.022), thicker LT (r = 0.31, P = 0.027), and shorter AL (r = −0.41, P = 0.003) at the 1st year measurements. Similar tendencies were observed in boys (ACD, r = −0.09, P = 0.52; LT, r = 0.07, P = 0.65; AL, r = −0.27, P = 0.055), but the differences were not significant (Figure 1D–F).
Discussion
The results showed that the eyes with the longer ALs, thinner LT, and deeper ACD at the initial examination had significantly greater TALE. This trend was found in both boys and girls and is consistent with earlier studies that showed that eyes with longer ALs tended to have a greater degree of eye elongations.12 They are also consistent with the reports that the more myopic eyes had a faster progression of myopia.15,17
In 78.4% of the eyes, the GRC was stable or decelerated, ie, the growth rate change was less than 0.05 mm. Previous studies reported that the annual axial length growth rate decreased gradually with increasing age10,11 which is consistent with the results of this study.
On the other hand, it has been reported that there are some children whose myopia progressed rapidly during the school age years.12,13 In our cohort, we found that 21.6% of the eyes had accelerated GRC. When we investigated the relationship between the parameters of the eye shape and the GRC, the results showed that the eyes of girls with shorter AL, shallower ACD, and thicker LT at the initial examination had a greater GRC, ie, a significant acceleration of annual axial elongation. A similar trend was observed for boys although the changes were not significant. A recent large cohort study (136,333 children, 4–17 years old) reported that the myopia progression during the first 11–24 months was greater in the 7–9 and 10–12 age groups, and it was consistent with our results for girls.18
These factors, shorter AL, shallower ACD, and thicker LT are the common risk factors for primary angle closure glaucoma.19 In eyes with primary angle closure, the pressure in the posterior chamber is higher than that of the anterior chamber. This would cause the iris to bow anteriorly. Conversely, a deeper ACD, longer AL, and thinner LT are known risk factors for the pigment dispersion syndrome. In this disorder, the pressure in the anterior chamber is higher than that of the posterior chamber resulting in a posterior bowing of the iris.19 The iris curvature was reportedly variable in vivo due to the difference in the pressures of the anterior and posterior chambers.20 Shah et al examined the iris curvature in boys ages 10 to 12 years by anterior segment OCT and reported that the iris of some eyes was curved posteriorly (concave iris curvature) while others were curved anteriorly (convex iris curvature).21 These changes occurred around the age of 10 years that the time when the lens and other ocular tissues become firmer.4 Thus, we suggest that differences in the anterior and posterior chamber pressures may affect the acceleration and deceleration of axial elongation during this period. However, there are no data about iris curvature in this study and this suggestion is a complete speculation. Further studies are needed to investigate the relationship between iris curvature and the rate of axial elongation.
It has been reported that eyes with elongated posterior segment have an oval shape with a longer anterior-posterior segment and are more common in female individuals.22,23 In clinical practice, there are eyes with myopic features such as tilted optic disc, myopic conus, and arcade vessels close to the macula in the fundus, even though the axial length is not long. These eyes are referred to as having a paradoxical fundus.14 In the present study, eyes with shallower anterior chamber, thicker lens, and shorter axis length that were present in girls had significantly accelerated eye elongation. These findings suggest that the cause of the paradoxical fundus is the greater acceleration of elongation during this period. To confirm this, long-term follow-up studies are needed.
There are limitations in this study. First, we did not consider the scleral rigidity, intraocular pressure, and differences in the pressure between the anterior and posterior chambers. Further studies including corneal measurements by Scheimpflug Technology Instruments, ocular response analyzer, and anterior segment imaging are needed to confirm the hypothesis. Second, we examined the ALs and not the refractive errors. Even though the AL is longer in myopic eyes, there is no systematic correlation with myopia.24 To know the true refractive error of children, it is necessary to use a cycloplegic agent with parental consent. Unfortunately, an agreement was not always obtained, and so we focused on the AL without measuring the refractive error. Although an elongation of the AL plays a substantial role in the development of school myopia in the East Asian populations,6,25,26 a reliable measurement of the AL is necessary when monitoring the myopia progression in school children.27–30 On the other hand, the refractive error is determined by three factors: the corneal refractive power, the lens refractive power, and the ocular axial length.10,11 There are various causes for the changes of these three factors during growth. When researching the causes of the refractive errors, it is difficult to draw conclusions due to the complex interplay of these factors that affect these three factors. In this study, the refractive error was not examined because the main purpose was to investigate factors that affected the ocular axial elongation. Myopia progression is greater in the winter than in the summer months.31 In this study, due to the educational program of the elementary school, only this time of the year was allowed for the measurements. This is a limitation of this study. Another limitation is that these findings were made on Japanese children which is the most myopic population.5 Thus, the results may not be generalized to other populations.
In conclusion, the axial elongation in 8- and 9-year-old children tended to be longer in the eyes with myopic ocular biometric values at the initial examination. The growth rate of the eyes tended to accelerate in the eyes with hyperopic ocular biometrics at the 1st year examinations. These individual variations of axial elongation speed may be affected by ocular biometry during this growth period.
Abbreviations
AL, axial length; ACD, anterior chamber depth; LT, lens thickness; TALE, the total AL elongation; GRC, growth rate change.
Statement of Ethics
All of the procedures used conformed to the tenets of the Declaration of Helsinki, and they were approved by the Ethics Committee of Kagoshima University Hospital. A written informed assent and informed consent were obtained from all subjects and their parents. This study was registered with the University Hospital Medical Network-clinical trials registry (No. UMIN000015239).
Funding
The funding organizations had no role in the design or conduct of this research. This study was supported by JSPS KAKENHI grant number 21H03095, 21K09704 and Suda memorial glaucoma research grant.
Disclosure
Dr Takehiro Yamashita reports grants from Alcon and Novartis, outside the submitted work. The authors declare that they have no other conflicts of interest.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Galvis V, Tello A, Otero J, et al. Prevalence of refractive errors in Colombia: MIOPUR study. Br J Ophthalmol. 2018;102(10):1320–1323. doi:10.1136/bjophthalmol-2018-312149
3. Rahi JS, Cumberland PM, Peckham CS. Myopia over the lifecourse: prevalence and early life influences in the 1958 British birth cohort. Ophthalmology. 2011;118(5):797–804. doi:10.1016/j.ophtha.2010.09.025
4. Foster PJ, Jiang Y. Epidemiology of myopia. Eye. 2014;28(2):202–208. doi:10.1038/eye.2013.280
5. Sawada A, Tomidokoro A, Araie M, Iwase A, Yamamoto T; Tajimi Study Group. Refractive errors in an elderly Japanese population: the Tajimi study. Ophthalmology. 2008;115(2):363–370.e3. doi:10.1016/j.ophtha.2007.03.075
6. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singap. 2004;33(1):27–33.
7. Iwase A, Araie M, Tomidokoro A, et al. Prevalence and causes of low vision and blindness in a Japanese adult population: the Tajimi Study. Ophthalmology. 2006;113(8):1354–1362. doi:10.1016/j.ophtha.2006.04.022
8. Xu L, Wang Y, Li Y, et al. Causes of blindness and visual impairment in urban and rural areas in Beijing: the Beijing Eye Study. Ophthalmology. 2006;113(7):
9. Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology. 1999;106(10):2010–2015. doi:10.1016/s0161-6420(99)90416-5
10. Jones LA, Mitchell GL, Mutti DO, Hayes JR, Moeschberger ML, Zadnik K. Comparison of ocular component growth curves among refractive error groups in children. Invest Ophthalmol Vis Sci. 2005;46(7):2317–2327. doi:10.1167/iovs.04-0945
11. Wong HB, Machin D, Tan SB, Wong TY, Saw SM. Ocular component growth curves among Singaporean children with different refractive error status. Invest Ophthalmol Vis Sci. 2010;51(3):1341–1347. doi:10.1167/iovs.09-3431
12. Mutti DO, Hayes JR, Mitchell GL, et al. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007;48(6):2510–2519. doi:10.1167/iovs.06-0562
13. Yip VC, Pan CW, Lin XY, et al. The relationship between growth spurts and myopia in Singapore children. Invest Ophthalmol Vis Sci. 2012;53(13):7961–7966. doi:10.1167/iovs.12-10402
14. Yamashita T, Sakamoto T, Terasaki H, Tanaka M, Kii Y, Nakao K. Quantification of retinal nerve fiber and retinal artery trajectories using second-order polynomial equation and its association with axial length. Invest Ophthalmol Vis Sci. 2014;55(8):5176–5182. doi:10.1167/iovs.14-14105
15. Guo Y, Liu LJ, Tang P, et al. Parapapillary gamma zone and progression of myopia in school children: the Beijing Children Eye Study. Invest Ophthalmol Vis Sci. 2018;59(3):1609–1616. doi:10.1167/iovs.17-21665
16. Richter GM, Wang M, Jiang X, et al.; Chinese American Eye Study Group. Ocular determinants of refractive error and its age- and sex-related variations in the Chinese American Eye Study. JAMA Ophthalmol. 2017;135(7):724–732. doi:10.1001/jamaophthalmol.2017.1176.
17. Zadnik K, Sinnott LT, Cotter SA, et al. Prediction of juvenile-onset myopia. JAMA Ophthalmol. 2015;133(6):683–689. doi:10.1001/jamaophthalmol.2015.0471
18. Tricard D, Marillet S, Ingrand P, Bullimore MA, Bourne RRA, Leveziel N. Progression of myopia in children and teenagers: a nationwide longitudinal study. Br J Ophthalmol. 2021;
19. Shaarawy TM, Sherwood MB, Hitchings RA, Crowston JG. Glaucoma: Medical Diagnosis and Therapy. Philadelphia, PA: Saunders Ltd; 2009:331–333.
20. Zhang K, Qian X, Mei X, Liu Z. An inverse method to determine the mechanical properties of the iris in vivo. Biomed Eng Online. 2014;13:66. doi:10.1186/1475-925X-13-66
21. Shah A, Low S, Garway-Heath DF, Foster PJ, Barton K. Iris concavity, corneal biomechanics, and their correlations with ocular biometry in a cohort of 10- to 12-year-old UK school boys: baseline data. Invest Ophthalmol Vis Sci. 2014;55(5):3303–3310. doi:10.1167/iovs.13-13756
22. Atchison DA, Jones CE, Schmid KL, et al. Eye shape in emmetropia and myopia. Invest Ophthalmol Vis Sci. 2004;45(10):3380–3386. doi:10.1167/iovs.04-0292
23. Pope JM, Verkicharla PK, Sepehrband F, Suheimat M, Schmid KL, Atchison DA. Three-dimensional MRI study of the relationship between eye dimensions, retinal shape and myopia. Biomed Opt Express. 2017;8:2386–2395. doi:10.1364/BOE.8.002386
24. Wong TY, Foster PJ, Ng TP, Tielsch JM, Johnson GJ, Seah SK. Variations in ocular biometry in an adult Chinese population in Singapore: the Tanjong Pagar Survey. Invest Ophthalmol Vis Sci. 2001;42(1):73–80.
25. Zhang J, Hur YM, Huang W, Ding X, Feng K, He M. Shared genetic determinants of axial length and height in children: the Guangzhou twin eye study. Arch Ophthalmol. 2011;129(1):63–68. doi:10.1001/archophthalmol.2010.323
26. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1–38. doi:10.1016/j.preteyeres.2004.06.004
27. Tideman JW, Snabel MC, Tedja MS, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016;134(12):1355–1363. doi:10.1001/jamaophthalmol.2016.4009
28. Galvis V, Tello A, Rey JJ, Serrano Gomez S, Prada AM. Estimation of ocular axial length with optometric parameters is not accurate. Cont Lens Anterior Eye. 2021;101448. doi:10.1016/j.clae.2021.101448
29. Fan Q, Wang H, Jiang Z. Axial length and its relationship to refractive error in Chinese university students. Cont Lens Anterior Eye. 2021;101470. doi:10.1016/j.clae.2021.101470
30. Rose LVT, Schulz AM, Graham SL. Use baseline axial length measurements in myopic patients to predict the control of myopia with and without atropine 0.01. PLoS One. 2021;16(7):e0254061. doi:10.1371/journal.pone.0254061
31. Fujiwara M, Hasebe S, Nakanishi R, Tanigawa K, Ohtsuki H. Seasonal variation in myopia progression and axial elongation: an evaluation of Japanese children participating in a myopia control trial. Jpn J Ophthalmol. 2012;56(4):401–406. doi:10.1007/s10384-012-0148-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.