")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Serum Vitamin D, Sleep Pattern and Cardiometabolic Diseases: Findings from the National Health and Nutrition Examination Survey
Authors Lo K , Huang Y, Liu L, Yu Y , Chen C , Huang J, Feng Y
Received 1 April 2020
Accepted for publication 4 May 2020
Published 14 May 2020 Volume 2020:13 Pages 1661—1668
DOI https://doi.org/10.2147/DMSO.S256133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Kenneth Lo,1,2,* Yu-qing Huang,1,* Lin Liu,1 Yu-ling Yu,1 Chao-lei Chen,1 Jia-yi Huang,1 Ying-qing Feng1
1Department of Cardiology, Guangdong Cardiovascular Institute, Hypertension Research Laboratory, Guangdong Provincial People’s Hospital, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Academy of Medical Sciences, South China University of Technology School of Medicine, Guangzhou, People’s Republic of China; 2Centre for Global Cardiometabolic Health, Department of Epidemiology, Brown University, Providence, Rhode Island, USA
*These authors contributed equally to this work
Correspondence: Kenneth Lo; Ying-qing Feng
Department of Cardiology, Guangdong Cardiovascular Institute, Hypertension Research Laboratory, Guangdong Provincial People’s Hospital, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Academy of Medical Sciences, South China University of Technology School of Medicine, Guangzhou, People’s Republic of China
Tel +86-13147550252
Email [email protected]; [email protected]
Objective: Although poor sleep health and vitamin D deficiency may be associated with diabetes and hypertension, whether this association shows a trend depending on vitamin D concentration is unclear.
Subjects and Methods: We analyzed data from 10,742 participants (4997 men) from the 2007– 2014 National Health and Nutrition Examination Survey. Abnormal sleep pattern (ie, short sleep duration, sleep complaint, and/or sleep disorder), lifestyle factors, serum vitamin D level, and the status of diabetes and hypertension were assessed. Logistic regression was performed to estimate the odds ratio (OR) and 95% confidence interval (CI).
Results: Serum vitamin D significantly interacted with short sleep duration and abnormal sleep pattern (both p = 0.003) on the association with diabetes in men. Short sleep duration (OR: 1.82, 95% CI = 1.29, 2.57) and abnormal sleep pattern (OR: 1.95, 95% CI = 1.38, 2.77) were associated with diabetes in men with serum vitamin D of > 75 nmol/L. Serum vitamin D significantly interacted with sleep complaint on the association with hypertension in men and women (both p < 0.05). The magnitude of association between sleep complaint and hypertension in men was stronger when serum vitamin D level was < 50 nmol/L (OR: 2.26, 95% CI = 1.57, 3.25) than when the level was > 75 nmol/L (OR: 1.28, 95% CI = 0.90, 1.83). Similarly, the magnitude of association between sleep complaint and hypertension in women was stronger when serum vitamin D level was < 50 nmol/L (OR: 2.09, 95% CI = 1.53, 2.86) than when the level was > 75 nmol/L (OR: 1.64, 95% CI = 0.98, 2.72). No significant interactions were observed between serum vitamin D level and other sleep variables.
Conclusion: Abnormal sleep pattern is associated with a high risk of diabetes and hypertension. The relationship between sleep complaint and hypertension may be strong in people with vitamin D deficiency, and this observation should be verified by prospective studies.
Keywords: vitamin D, sleep, diabetes, hypertension, epidemiology
Introduction
Adequate sleep duration maintains body functions and improves cardiometabolic health, such as a low risk of diabetes and hypertension.1–3 Apart from sleep duration, how sleep complaints and sleep disorders associated with diabetes and hypertension have received increasing attention in recent years.1,4 A population survey in New Zealand suggests that people with self-reported sleep complaints (eg, difficulty in falling asleep, frequent nocturnal awakenings, and/or early morning awakenings) had 92% and 58% increased chance of developing diabetes and hypertension, respectively.5 Another example is obstructive sleep apnea (OSA), a prevalent sleep disorder that may increase body weight via several pathways and by considerably elevating ghrelin levels, inducing leptin resistance, and decreasing melatonin level.6 Apart from its role in obesity etiology, OSA causes intermittent hypoxia, which can lead to increased insulin resistance, elevated sympathetic tone, and systemic inflammation, which are the precursors of an increased risk of diabetes and hypertension.7,8 These observations provide further intervention strategies for improving sleep and the effects of sleep improvement on cardiometabolic risks.
Preventing vitamin D deficiency is an approach for improving sleep. Vitamin D is responsible for multiple physiological functions, and its deficiency can lead to adverse health outcomes, such as diabetes and hypertension.9–11 Moreover, available evidence from clinical and preclinical studies has suggested the interaction between serum vitamin D and sleep health through several possible mechanisms.12 First, vitamin D receptors are distributed in brain areas that are crucial to sleep regulation, including the hypothalamus and midbrain central gray.13,14 In addition, vitamin D regulates the conversion of tryptophan to serotonin, which is used in the production of melatonin, the hormone that controls circadian rhythms and sleep.12,15 In recent years, pooled analysis from multiple epidemiological studies has shown that people with serum vitamin D deficiency have a high risk of poor sleep quality, short sleep duration, and daytime sleepiness.16
Given the physiological relationship between vitamin D and sleep, the associations of sleep health, diabetes, and hypertension with serum vitamin D level should be explored. To provide epidemiological evidence to answer this research question, we analyzed data from the National Health and Nutrition Examination Survey (NHANES).
Subjects and Methods
Study Design
In the present study, we used data from the 2007–2014 NHANES (N = 37,520), which is a survey conducted by the Center for Disease Control and Prevention and designed for the evaluation of the health status of adults in the United States. Written informed consent was obtained from each participant. We excluded participants with incomplete exposure (sleep duration, sleep problems, and sleep disorder; N = 12,399), without serum vitamin D data (N = 2314), and with missing covariate data (N = 9475). To reduce the influence of pre-existing medical condition on sleep, we further excluded participants diagnosed with congestive heart failure, coronary heart disease, angina/angina pectoris, heart attack or stroke, and/or cancer as reported by the participants (N = 2590).17,18
Exposure and Outcome Assessment
The exposure variables were sleep duration, sleep problems, and sleep disorder.19 The questions on sleep were administered using a computer-assisted personal interviewing system as part of the household interview of the survey participants. The questions on sleep habits included those selected from the instruments of the Sleep Heart Health Study19 and have demonstrated validity and internal consistency in white and black adults.20 The participants reported their usual sleep duration at night. Short sleep was defined as <7 hours according to the recommendation of the National Sleep Foundation for adults.21 Participants with sleep complaints were self-reported in the sleep questionnaire via the question “Have you ever told a doctor or other health professional that you have trouble sleeping?” Diagnosed sleep disorders were self-reported in the sleep questionnaire via the question “Have you ever been told by a doctor or other health care professional that you have a sleep disorder?” We then created a composite variable “abnormal sleep pattern,” which is defined by any occurrence of short sleep, sleep complaint, or sleep disorder.
The outcomes were participant-reported status of diabetes or hypertension. In accordance with the classification standard of the American Diabetes Association,22 diabetes was defined as fasting blood glucose ≥126 mg/dL, hemoglobin A1C ≥6.5%, doctor-informed diagnosis (“have you ever been told by a doctor or health professional that you have diabetes or sugar diabetes?”), and/or the self-reported use of antidiabetic drugs. In accordance with the guidelines of the American Heart Association,23 hypertension was defined as systolic blood pressure ≥130 mmHg, diastolic blood pressure ≥80 mmHg, doctor-informed diagnosis (“have you ever been told by a doctor or health professional that you have hypertension, also called high blood pressure?”), and/or the self-reported use of anti-hypertensive drugs.
Vitamin D Assessment
Total serum vitamin D (25-hydroxyvitamin D) was measured using ultra-high-performance liquid chromatography–tandem mass spectrometry. The analytes were chromatographically separated generally on a pentaflurophenyl (PFP) column (Thermo Scientific Hypersil GOLD PFP 2.1 mm × 100 mm, 1.9 µm particle size column or Phenomenex Kinetex PFP 2.1 mm × 100 mm, 1.7 µm). A detailed methodology was described elsewhere (https://wwwn.cdc.gov/nchs/nhanes/vitamind/analyticalnote.aspx). To classify participants with vitamin D deficiency, we used the cutoff values proposed by the US National Academy of Medicine (50 nmol/L) and US Endocrine Society (75 nmol/L).24
Covariates for Analysis
The covariates included age, sex, race/ethnicity (dichotomized into non-Hispanic white versus others), education level (dichotomized into college graduate or above versus others), marital status (married versus others), the use of at least 100 cigarettes in lifetime (yes versus no), time spent on physical activity in hours per week (continuous), family poverty income ratio (continuous), systolic blood pressure (average values of four measurements), dietary energy in kcal and total vitamin D intake in mcg (both assessed by 2-day food records), and the time period for data collection (November 1 through April 30 or May 1 through October 31). Waist circumference in cm was measured at the high point of the iliac crest at minimal respiration and was treated as a continuous variable in the analysis.25
Statistical Analysis
Continuous data were reported as means and standard deviations, and categorical data were presented as frequencies with percentages. Demographic characteristics by serum vitamin D status (>75, 50–74.9, and <50 nmol/L) were compared using one-way ANOVA and chi-square tests, respectively. To examine the association between sleep indicators and the likelihood of cardiometabolic diseases (diabetes and hypertension), we built logistic regression models for each disease and reported the odds ratios (ORs) and 95% confidence intervals (CIs). To prevent collinearity, we placed sleep variables into separate regression models. The results of regression analysis were stratified by sex (men, women) and the levels of serum vitamin D (>75, 50–74.9, and <50 nmol/L). Potential interactions between sleep and serum vitamin D were determined by placing cross-product terms (the product between sleep indicators and level of serum vitamin D) into the regression models. All analyses were conducted using SPSS 23.0 (SPSS Inc., Chicago, IL, USA) with complex sampling for the prevention of sampling bias, unequal probability of selection, and oversampling. Statistical significance level was set at 0.05.
Results
A total of 10,742 participants (4997 men) in NHANES with complete data were included for analysis. Table 1 compares the characteristics of the participants by their serum vitamin D status. In general, significant differences were found across multiple variables. For example, people who had low serum vitamin D levels had short sleep durations and high waist circumferences. The exceptions were the insignificant difference in the rate of sleep disorder, rate of diabetes, level of systolic blood pressure, and dietary energy.
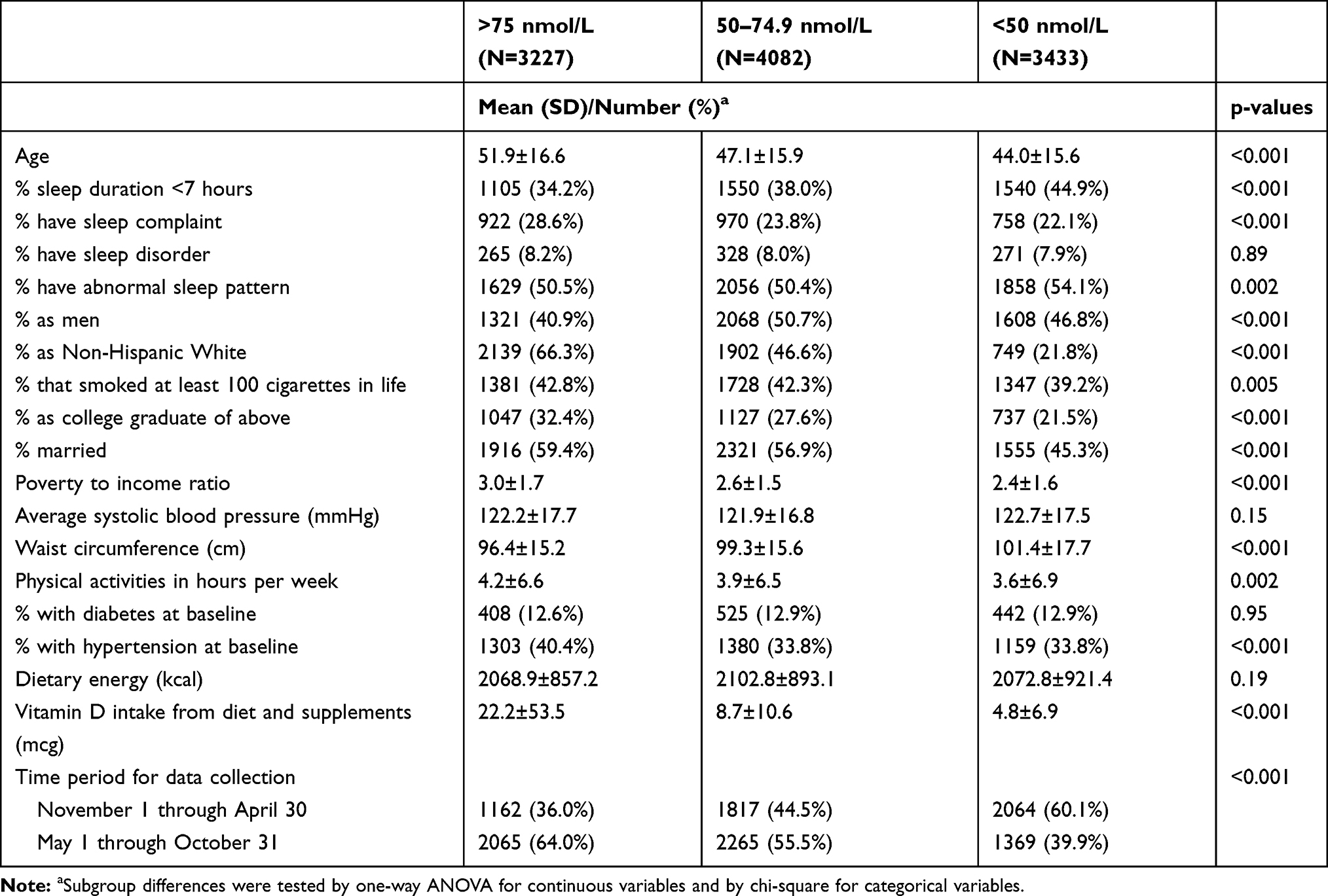 |
Table 1 Characteristics of Included Participants Stratified by Levels of Serum Vitamin D |
Table 2 demonstrates the association between sleep and cardiometabolic diseases as stratified by sex and serum vitamin D. Serum vitamin D significantly interacted with short sleep duration and abnormal sleep pattern with the association of diabetes in men. Short sleep duration was associated with diabetes (OR: 1.82, 95% CI = 1.29, 2.57) in men with serum vitamin D level of >75 nmol/L. Abnormal sleep pattern was associated with diabetes (OR: 1.95, 95% CI = 1.38, 2.77) in men with serum vitamin D level of >75 nmol/L. Serum vitamin D did not interact with sleep complaint and sleep disorder to influence the relationship with diabetes. Sleep complaint was associated with diabetes regardless of sex and serum vitamin D level, except in men (OR: 1.02, 95% CI = 0.72, 1.44) and women (OR: 1.32, 95% CI = 0.98, 1.77) with serum vitamin D level of <50 nmol/L. The presence of a sleep disorder was associated with diabetes in men with a serum vitamin D level of 50–74.9 nmol/L (OR: 1.88, 95% CI = 1.26, 2.81).
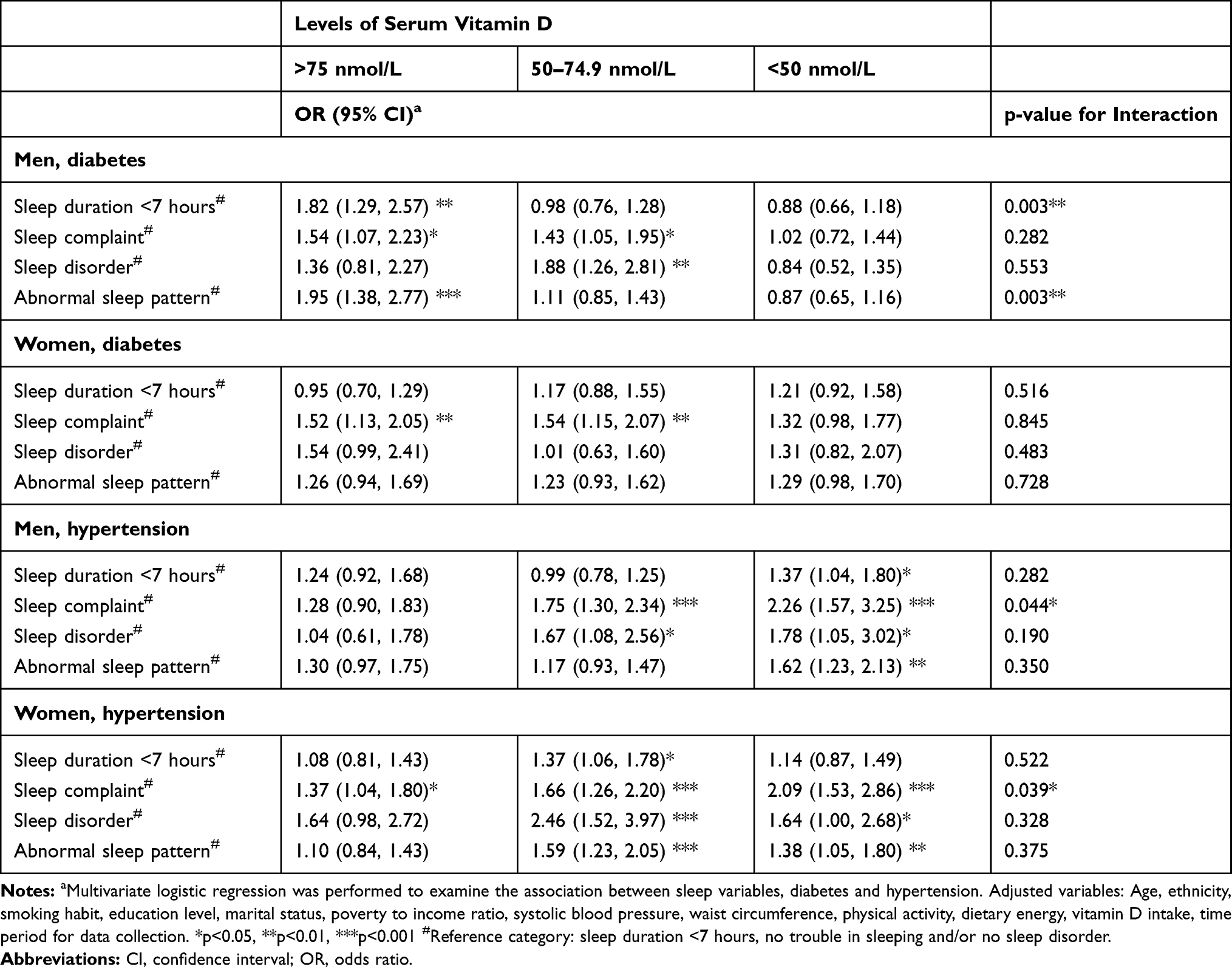 |
Table 2 Sex and Serum Vitamin D-Stratified Associations Between Sleep, Diabetes and Hypertension |
Moreover, serum vitamin D significantly interacted with sleep complaint on the association with hypertension in men (p = 0.044) and women (p = 0.039). The magnitude of the association between sleep complaint and hypertension in men was stronger when serum vitamin D level was <50 nmol/L (OR: 2.26, 95% CI = 1.57, 3.25) than when the level was >75 nmol/L (OR: 1.28, 95% CI = 0.90, 1.83). Similarly, the magnitude of the association between sleep complaint and hypertension in women was stronger when serum vitamin D level was <50 nmol/L (OR: 2.09, 95% CI = 1.53, 2.86) than when the level was >75 nmol/L (OR: 1.64, 95% CI = 0.98, 2.72). Serum vitamin D did not interact with sleep duration, sleep disorder, and abnormal sleep pattern to influence the relationship with hypertension. Short sleep duration was associated with hypertension in men with serum vitamin D level of <50 nmol/L (OR: 1.37, 95% CI = 1.04, 1.80) and women with serum vitamin D level ranging from 50 nmol/L to 74.9 nmol/L (OR: 1.37, 95% CI = 1.06, 1.78). Sleep disorder remained significantly associated with the chance of hypertension in women with serum vitamin D levels of 50–74.9 nmol/L (OR: 2.46, 95% CI = 1.53, 2.86) and <50 nmol/L (OR: 1.64, 95% CI = 1.00, 2.68). Abnormal sleep pattern was associated with hypertension in men with serum vitamin D levels of <50 nmol/L (OR: 1.62, 95% CI = 1.23, 2.13) and women with serum vitamin D levels of 50–74.9 nmol/L (OR: 1.59, 95% CI = 1.23, 2.05) and <50 nmol/L (OR: 1.38, 95% CI = 1.05, 1.80).
Discussion
In the present study, short sleep duration and the presence of sleep complaint, sleeping disorder, and/or abnormal sleep pattern were associated with a high chance of diabetes and hypertension. Serum vitamin D and sleep complaint had significant interactions to influence the likelihood of hypertension. Furthermore, the magnitude of the association between sleep complaint and hypertension appeared to be stronger in participants with the lowest level of serum vitamin D levels than in the participants with the highest levels. Although the present study did not provide prospective evidence because of the cross-sectional design, this observation may provide a hypothesis that is worth verifying in future prospective studies.
The association between sleep and diabetes in this study was consistent with previous literature.1,26 Insufficient sleep, poor sleep, or sleep disorder may upregulate ghrelin (the hormone that promotes appetite), reduce energy expenditure, and increase the time for eating.27,28 These factors may induce weight gain and impaired glucose metabolism, leading to an increased risk of diabetes. Moreover, the significant association between sleep complaint and hypertension was consistent with the findings from a recent meta-analysis on the relationship between subjective sleep quality and hypertension.29 Subjective sleep quality was mainly assessed using the Pittsburgh sleep quality index, a validated tool for evaluating the several important aspects of sleep, including sleep duration, sleep problems, and sleep medications.30 People with poor sleep quality have a 48% increased probability of having hypertension.29 A meta-analysis of prospective cohorts showed that vitamin D deficiency is associated with a 24% increased risk of developing hypertension.9
Although our findings suggested that the association between sleep complaint and hypertension may show a trend depending on vitamin D concentration, the mechanism behind this relationship warrants further investigation. First, deficient serum vitamin D may be related to the level of blood pressure through the renin–angiotensin system (RAS) and endothelial vasodilator dysfunction.31,32 Animal experiments indicate that vitamin D deficiency can activate the RAS system, thereby causing hypertension, left ventricular hypertrophy, and atherosclerosis.33,34 Moreover, a pooled analysis of case–control studies showed that OSA, a type of sleep disorder, is associated with the high levels of the biomarkers of RAS system activities (eg aldosterone), especially in patients with hypertension.35 A clinical experiment showed that RAS activity as reflected by aldosterone fluctuates with circadian rhythm.36 These findings imply that poor sleep health may cause hypertension by stimulating RAS. Further studies are needed to explore the common pathways (eg, RAS system) and associated biomarkers for vitamin D and sleep health to exert their physiological effects.
For research on serum vitamin D, sleep, and cardiometabolic health, another unanswered question is whether vitamin D from diet or supplements associates with better cardiometabolic outcomes by improving sleep health. A meta-analysis of randomized controlled trials suggested that vitamin D supplementation for more than 3 months has a modest but significant reduction in systolic blood pressure.37 Another randomized controlled trial showed that 50,000 IU vitamin D supplementation significantly improves sleep quality, reduces sleep latency, and increases the sleep duration of people with sleep disorders after 8 weeks. Patients in the trial showed significant improvements in serum vitamin D level (25.00 ng/mL before the intervention to 37.69 ng/mL after intervention).38 However, the authors did not examine how vitamin D supplementation may influence cardiometabolic risks. In addition, the efficacy of intervention may vary among geographical regions and with baseline serum vitamin D level. A subgroup analysis of another meta-analysis found a significant decrease in peripheral systolic blood pressure and diastolic blood pressure in patients with vitamin D deficiency, studies performed in Asia, trials lasted for at least 8 weeks, and studies that administered >5000 IU vitamin D to each patient daily.39 In summary, vitamin D supplements have preferable changes when administered at high dosages and for long intervention periods to people with vitamin D deficiency.
The current study has several limitations that should be noted for cautious interpretation. First, the current study is cross-sectional in nature. Therefore, bias due to reverse caution may exist. For example, participants with the lowest serum vitamin D levels had the lowest prevalence of hypertension. Possibly, participants with chronic diseases were more aware of their lifestyle and therefore had a lower percentage of vitamin D deficiency than those without. Despite the limitation from reverse causation, the association between sleep and cardiometabolic disease and the health benefit of vitamin D agreed with the physiological mechanisms. Further prospective studies should simultaneously consider the effect of vitamin D and sleep health to establish a temporal relationship. Second, exposure and outcomes were self-reported and may thus have introduced misclassification bias. Future studies can improve the validity by using objective measurements (eg, polysomnography or actigraphy for sleep measurement) and medical records to verify disease outcomes. Third, not every participant had available vitamin D data, and thus the representativeness of the study population may have been affected. Fourth, personal sun exposure, a main predictor of serum vitamin D level, was not determined in this study. We took the seasonality effect of sun exposure on serum vitamin D into account by adjusting the time period for data collection.
Conclusions
In the participants of NHANES, abnormal sleep pattern is associated with a high risk for diabetes and hypertension. Although the relationship between sleep complaint and hypertension may be stronger in people with vitamin D deficiency, this observation should be verified by prospective cohorts. Further studies are needed to explore the common pathways and associated biomarkers for vitamin D and sleep health to exert their physiological effects.
Data Sharing Statement
The data access from the NHANES is freely available.
Ethics and Consent Statement
The study was conducted following the Declaration of Helsinki. Ethical approval was obtained from National Center for Health Statistics Ethics Review Board (Protocol #98-12, #2005–06, #2011–17). Informed written consent was obtained from all subjects enrolled in the study.
Acknowledgment
We thank all NHANES participants for their contribution to the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Anothaisintawee T, Reutrakul S, Van Cauter E, Thakkinstian A. Sleep disturbances compared to traditional risk factors for diabetes development: systematic review and meta-analysis. Sleep Med Rev. 2016;30:11–24. doi:10.1016/j.smrv.2015.10.002
2. Li H, Ren Y, Wu Y, Zhao X. Correlation between sleep duration and hypertension: a dose-response meta-analysis. J Hum Hypertens. 2019;33(3):218–228. doi:10.1038/s41371-018-0135-1
3. Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246–256. doi:10.1016/j.sleep.2016.08.006
4. Hou H, Zhao Y, Yu W, et al. Association of obstructive sleep apnea with hypertension: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010405. doi:10.7189/jogh.08.010405
5. Paine SJ, Harris R, Cormack D, Stanley J. Self-reported sleep complaints are associated with adverse health outcomes: cross-sectional analysis of the 2002/03 New Zealand Health Survey. Ethn Health. 2019;24(1):44–56. doi:10.1080/13557858.2017.1315368
6. Muscogiuri G, Barrea L, Annunziata G, et al. Obesity and sleep disturbance: the chicken or the egg? Crit Rev Food Sci Nutr. 2019;59(13):2158–2165. doi:10.1080/10408398.2018.1506979
7. Cai A, Wang L, Zhou Y. Hypertension and obstructive sleep apnea. Hypertens Res. 2016;39(6):391–395. doi:10.1038/hr.2016.11
8. Pugliese G, Barrea L, Laudisio D, et al. Sleep apnea, obesity, and disturbed glucose homeostasis: epidemiologic evidence, biologic insights, and therapeutic strategies. Curr Obes Rep. 2020;9(1):30–38. doi:10.1007/s13679-020-00369-y
9. Qi D, Nie XL, Wu S, Cai J. Vitamin D and hypertension: prospective study and meta-analysis. PLoS One. 2017;12(3):e0174298. doi:10.1371/journal.pone.0174298
10. Lucato P, Solmi M, Maggi S, et al. Low vitamin D levels increase the risk of type 2 diabetes in older adults: a systematic review and meta-analysis. Maturitas. 2017;100:8–15. doi:10.1016/j.maturitas.2017.02.016
11. Li X, Liu Y, Zheng Y, Wang P, Zhang Y. The effect of vitamin D supplementation on glycemic control in type 2 diabetes patients: a systematic review and meta-analysis. Nutrients. 2018;10:375.
12. Muscogiuri G, Barrea L, Scannapieco M, et al. The lullaby of the sun: the role of vitamin D in sleep disturbance. Sleep Med. 2019;54:262–265. doi:10.1016/j.sleep.2018.10.033
13. Stumpf WE, Bidmon HJ, Li L, et al. Nuclear receptor sites for vitamin D-soltriol in midbrain and hindbrain of Siberian hamster (Phodopus sungorus) assessed by autoradiography. Histochemistry. 1992;98(3):155–164. doi:10.1007/BF00315874
14. Stumpf WE. Drug localization and targeting with receptor microscopic autoradiography. J Pharmacol Toxicol. 2005;51(1):25–40. doi:10.1016/j.vascn.2004.09.001
15. Golan D, Staun-Ram E, Glass-Marmor L, et al. The influence of vitamin D supplementation on melatonin status in patients with multiple sclerosis. Brain Behav Immun. 2013;32:180–185. doi:10.1016/j.bbi.2013.04.010
16. Gao Q, Kou T, Zhuang B, Ren Y, Dong X, Wang Q. The association between vitamin D deficiency and sleep disorders: a systematic review and meta-analysis. Nutrients. 2018;10(10):1395. doi:10.3390/nu10101395
17. Chen D, Yin Z, Fang B. Measurements and status of sleep quality in patients with cancers. Support Care Cancer. 2018;26(2):405–414. doi:10.1007/s00520-017-3927-x
18. Andrechuk CR, Ceolim MF. Sleep quality and adverse outcomes for patients with acute myocardial infarction. J Clin Nurs. 2016;25(1–2):223–230. doi:10.1111/jocn.13051
19. O’Connor GT, Lind BK, Lee ET, et al. Variation in symptoms of sleep-disordered breathing with race and ethnicity: the Sleep Heart Health Study. Sleep. 2003;26(1):74–79.
20. Kump K, Whalen C, Tishler PV, et al. Assessment of the validity and utility of a sleep-symptom questionnaire. Am J Respir Crit Care Med. 1994;150(3):735–741. doi:10.1164/ajrccm.150.3.8087345
21. Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
22. American Diabetes A. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care. 2020;43(Supplement 1):S14–S31. doi:10.2337/dc20-S002
23. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
24. Mogire RM, Mutua A, Kimita W, et al. Prevalence of vitamin D deficiency in Africa: a systematic review and meta-analysis. Lancet Glob Health. 2020;8(1):e134–e42. doi:10.1016/S2214-109X(19)30457-7
25. Sun YS, Kao TW, Chang YW, et al. Calf circumference as a novel tool for risk of disability of the elderly population. Sci Rep. 2017;7(1):16359. doi:10.1038/s41598-017-16347-9
26. Lee SWH, Ng KY, Chin WK. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: a systematic review and meta-analysis. Sleep Med Rev. 2017;31:91–101. doi:10.1016/j.smrv.2016.02.001
27. Zheng H, Berthoud HR. Neural systems controlling the drive to eat: mind versus metabolism. Physiology (Bethesda). 2008;23:75–83. doi:10.1152/physiol.00047.2007
28. Barone MT, Menna-Barreto L. Diabetes and sleep: a complex cause-and-effect relationship. Diabetes Res Clin Pract. 2011;91(2):129–137. doi:10.1016/j.diabres.2010.07.011
29. Lo K, Woo B, Wong M, Tam W. Subjective sleep quality, blood pressure, and hypertension: a meta-analysis. J Clin Hypertens (Greenwich). 2018;20(3):592–605. doi:10.1111/jch.13220
30. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
31. Li YC. Vitamin D regulation of the renin-angiotensin system. J Cell Biochem. 2003;88(2):327–331. doi:10.1002/jcb.10343
32. Vaidya A, Williams JS. The relationship between vitamin D and the renin-angiotensin system in the pathophysiology of hypertension, kidney disease, and diabetes. Metabolism. 2012;61(4):450–458. doi:10.1016/j.metabol.2011.09.007
33. Weng S, Sprague JE, Oh J, et al. Vitamin D deficiency induces high blood pressure and accelerates atherosclerosis in mice. PLoS One. 2013;8(1):e54625. doi:10.1371/journal.pone.0054625
34. Wong MS, Delansorne R, Man RY, Svenningsen P, Vanhoutte PM. Chronic treatment with vitamin D lowers arterial blood pressure and reduces endothelium-dependent contractions in the aorta of the spontaneously hypertensive rat. Am J Physiol Heart Circ Physiol. 2010;299(4):H1226–34. doi:10.1152/ajpheart.00288.2010
35. Jin ZN, Wei YX. Meta-analysis of effects of obstructive sleep apnea on the renin-angiotensin-aldosterone system. J Geriatr Cardiol. 2016;13(4):333–343. doi:10.11909/j.issn.1671-5411.2016.03.020
36. Thosar SS, Rueda JF, Berman AM, et al. Separate and interacting effects of the endogenous circadian system and behaviors on plasma aldosterone in humans. Am J Physiol Regul Integr Comp Physiol. 2019;316(2):R157–R64. doi:10.1152/ajpregu.00314.2018
37. Qi D, Nie X, Cai J. The effect of vitamin D supplementation on hypertension in non-CKD populations: a systemic review and meta-analysis. Int J Cardiol. 2017;227:177–186. doi:10.1016/j.ijcard.2016.11.040
38. Majid MS, Ahmad HS, Bizhan H, Hosein HZM, Mohammad A. The effect of vitamin D supplement on the score and quality of sleep in 20–50 year-old people with sleep disorders compared with control group. Nutr Neurosci. 2018;21(7):511–519. doi:10.1080/1028415X.2017.1317395
39. Shu L, Huang K. Effect of vitamin D supplementation on blood pressure parameters in patients with vitamin D deficiency: a systematic review and meta-analysis. J Am Soc Hypertens. 2018;12(7):488–496. doi:10.1016/j.jash.2018.04.009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.