")
Back to Journals » Infection and Drug Resistance » Volume 15
Serum Interleukin-26 is a Potential Biomarker for the Differential Diagnosis of Neurosyphilis and Syphilis at Other Stages
Authors Shen Y, Dong X, Liu J , Lv H, Ge Y
Received 15 March 2022
Accepted for publication 1 July 2022
Published 14 July 2022 Volume 2022:15 Pages 3693—3702
DOI https://doi.org/10.2147/IDR.S366308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yuhuan Shen,1,* Xiaoyan Dong,2,* Jinlin Liu,1 Huoyang Lv,1 Yumei Ge1,3
1Department of Clinical Laboratory, Laboratory Medicine Center, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, People’s Republic of China; 2Department of Clinical Laboratory, Ningbo Blood Centers, Ningbo, Zhejiang, People’s Republic of China; 3Key Laboratory of Biomarkers and in vitro Diagnosis Translation of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Ge, Department of Clinical Laboratory, Laboratory Medicine Center, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), No. 158, Shang-Tang Road, Gong-Shu District, Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel +86-0571-85893264, Email [email protected]
Background: Interleukin-26 (IL-26) is an atypical proinflammatory cytokine due to its binding to circulating double-stranded DNA and direct antibacterial activity. Although IL-26 has been confirmed to be involved in the pathophysiology of cancer, chronic inflammatory diseases and infections, the diagnostic and prognostic values of IL-26 levels in syphilis patients are not clear. This study aimed to investigate IL-26 levels in different stages of syphilis progression.
Methods: A total of 30 healthy controls and 166 patients with syphilis at different stages of disease progression were enrolled. Serum IL-26 levels were quantified in accordance with the protocols of RayBio® Human Interleukin-26 Enzyme Linked Immunosorbent Assay (ELISA) kits. Clinical laboratory diagnostic parameters and blood analysis data were detected and collected according to clinical medical laboratory standards.
Results: The levels of serum IL-26 were significantly higher in neurosyphilis patients than in healthy subjects (6.87 (4.36, 12.14) and 1.67 (0.09, 4.89) pg/μL, respectively; ****p < 0.0001), latent syphilis (1.48 (0.40, 2.05) pg/μL, ****p < 0.0001), seroresistant syphilis (0.81 (0.20, 2.91) pg/μL, ****p < 0.0001) and secondary syphilis (1.66 (0.41, 4.25) pg/μL, ****p < 0.0001) with data presented as the median with interquartile range. The concentration of serum IL-26 was most sensitive to serum low-density lipoprotein concentration (r = − 0.438, **p = 0.004) in latent syphilis, urine epithelial cells (r = 0.459, **p = 0.003) in seroresistant syphilis, and serum creatinine levels (r = 0.463, **p = 0.004) and urea creatinine ratio levels (r = 0.500, **p = 0.008) in secondary syphilis patients. There was no significant correlation with the concentration of IL-26 and toluidine red unheated serum test (TRUST) titers in each type of syphilis patient.
Conclusion: Circulating IL-26 in serum displays diagnostic potential in the progression of neurosyphilis and warrants further evaluation in clinical trials.
Keywords: neurosyphilis, interleukin-26, IL-26, disease progression, biomarker, diagnosis
Introduction
Syphilis is a globally prevalent multisystemic and chronic infection caused by the spirochetal bacterium Treponema pallidum subspecies pallidum (T. pallidum).1 It can be transmitted through blood transfusion and derivatives, unprotected sexual intercourse and maternal-neonatal transmission. Syphilis is still a major public health problem, with estimated 36 million occurrences and 12 million new cases worldwide.2,3 Acquired syphilis is divided into primary, secondary, tertiary, latent, and seroresistant syphilis based on disease progression and clinical characteristics.4–6 Although neurosyphilis is a tertiary syphilis, it is one of the most destructive, concealed, changeable and difficult clinical types of syphilis due to its occurrence at any stage of the infection and its involvement in the CNS with irreversible neurological dysfunction and potentially serious sequelae.7,8
Neurosyphilis is easily overlooked by patients and clinicians because it can be asymptomatic. Moreover, symptomatic neurosyphilis, mainly including meningitis, cerebral gumma, meningovascular syphilis, ocular syphilis, ear syphilis, general paresis and tabes dorsalis, is usually accompanied by deceptive mental symptoms, such as delusional impairment of memory and judgment, depression, hallucinations, seizures, personality changes and psychosis.9,10 It was confirmed that nonspecific symptoms and multifarious performance of neurosyphilis could lead to a clinical misdiagnosis rate as high as 48.3%.11
Currently, the laboratory diagnosis of neurosyphilis is primarily based on abnormalities of cerebrospinal fluid (CSF) with a reactive VDRL or elevated protein (>450 mg/L) or white blood cell (WBC) count (>5 cells/μL). In addition, clinical manifestations, neuroimaging and other diagnostic tests are also useful in the joint diagnosis of neurosyphilis.6 However, there is still no “gold standard” of neurosyphilis diagnosis. Various guidelines have contradictions regarding the identification of clinical symptoms of neurosyphilis, the timing of lumbar puncture and the diagnostic criteria of treponemal and nontreponemal detections in CSF.12 Therefore, specific biomarkers and new diagnostic methods for neurosyphilis are a hot spot in clinical laboratory research.
IL-26 is an atypical proinflammatory cytokine due to its binding to circulating double-stranded DNA and direct antibacterial activity.13,14 IL-26 interacts directly with viral nucleic acids for antiviral defenses and operates independently of the immune system; it belongs to the IL-10 cytokine family and was originally described in virus-transformed human T cells.15 IL-26 was first reported to be increased in chronic inflammatory disorders, including Crohn’s disease and rheumatoid arthritis.14 We searched PubMed with “IL-26 + syphilis” as the keyword, and no relevant research reports were retrieved. After analyzing the levels of IL-26 in healthy controls and patients with different stages of syphilis, including late latent syphilis, seroresistant syphilis, secondary syphilis and neurosyphilis, we unexpectedly found that the serum IL-26 level in neurosyphilis was significantly higher than that in other stages of syphilis. This suggests that the newly discovered biomarker of circulating IL-26 in syphilis may have promising applications in the diagnosis of neurosyphilis.
Methods
Ethics and Subjects
Thirty healthy controls (HCs) who had undergone physical examinations in our hospital and 166 serologically and phenotypically confirmed syphilis patients were enrolled from the clinical diagnostic laboratory of Zhejiang Provincial People’s Hospital (Table 1). Intravenous blood was obtained from syphilis patients and healthy individuals after written informed consent and ethical approval (Ethics Committee of Zhejiang People’s Hospital approval number 2019KY311) for the quantification of IL-26, which was carried out in accordance with the ethical standards of the Declaration of Helsinki. All healthy individuals were serologically negative for human immunodeficiency virus (HIV), syphilis, hepatitis C virus, hepatitis A virus, and hepatitis B virus. Syphilis patients were determined based on epidemiological history; clinical manifestations; physical, neurological and psychiatric symptoms; and signs and laboratory serological and etiological results. The diagnosis and classification of late latent syphilis was determined by the recommendations of the 2020 European guideline on the management of syphilis and was described as positive serological tests for syphilis with no clinical evidence of treponemal infection and one of the following conditions: 1) a negative syphilis serology ≥1 year or an unknown duration of syphilis diagnosis, 2) a fourfold or greater increase in nontreponemal antibody titers ≥1 year or unknown duration of previous testing, or 3) unequivocal evidence that the disease was acquired ≥1 year or an unknown duration (on the basis of clinical signs in patients and partners).6,16 The serofast state was described as we reported previously and was defined as a positive Treponema pallidum particle assay (TPPA) and TRUST, with the TRUST titer declining by less than 4 times in the nontreponemal test compared to previous results after one year of continuous treatment by retrospective analysis and clinical follow-up; neurosyphilis and other organic syphilis infections were excluded.6 According to the neurosyphilis diagnosis published by the health industry standard of the People’s Republic of China in 2018 and 2020 European guidelines on the management of syphilis, neurosyphilis can be classified according to one of the following criteria: (1) CSF-TPPA positive and CSF-TRUST positive, (2) CSF-TPPA positive and CSF-TRUST negative and CSF protein increased (>500 mg/L) or CFS white blood cell count (>10 × 106 cells/L), (3) CSF-TPPA positive, CSF-TRUST negative, and signs or symptoms of neurosyphilis with other clinical causes of such symptoms being excluded. Patients with cancers, injuries, HIV and other viral infections, autoimmune diseases and other irrelevant underlying diseases, medications and antibiotic treatment were excluded, but seroresistant syphilis patients were treated with penicillin.
 |
Table 1 Characteristics and Clinical Detection Indices of the Total Study Population |
Clinical Parameters
Indices of blood routine tests were analyzed by an automated blood cell counter (XN-9000, Sysmex, Japan), the blood coagulation indices were measured by a CS-5100 Hemostasis System (Sysmex Corporation, Japan), and the serum biochemical indicators were recorded by commercial kits using an automated chemistry analyzer (Chemistry Analyzer Au5821, Beckman Coulter, Inc., USA). The toluidine red unheated serum test (Rongsheng Biotech, China) was used in combination with treponemal pallidum particle agglutination (FUJIREBIO Inc, Japan) for serological detection of syphilis patients. The clinical laboratory is certified according to the international standards for laboratories 15,189, and internal quality control procedures and external quality assessment schemes were used to guarantee the quality of the data.17
IL-26 Quantification
Five milliliters of peripheral blood was collected in a vacuette blood collection tube for separation gel coagulation and centrifuged at 900 × g for 5 min at room temperature. The quantitative measurement of human IL-26 in serum was performed by an in vitro enzyme-linked immunosorbent assay with the RayBio® Human IL-26 ELISA kit (Cat: ELH-26, Lot: 0103202063, Raybio Inc, USA) according to the manufacturer’s protocol. Standards and samples were pipetted into the wells coated with human IL-26-specific antibody, and IL-26 present in the sample was bound to the wells by the immobilized antibody. The wells were washed, and a biotinylated anti-human IL-26 antibody was added. Then, unbound biotinylated antibody was washed away, and horseradish peroxidase (HRP)-conjugated streptavidin was pipetted into the wells. After washing again, a solution with 3,3’,5,5’-tetramethylbenzidine (TMB) substrate was added to the wells, and the color developed in proportion to the amount of bound IL-26. The stop solution changed the color from blue to yellow, and the intensity of the color was measured at 450 nm (Bio-Rad, iMarkTM Microplate Reader). The mean absorbance for each set of duplicate standards, controls and samples was calculated, and the average zero standard optical density was subtracted. The minimum detectable dose of human IL-26 was determined to be 3.3 pg/mL.
Statistical Analysis
Statistical evaluation was performed using Statistical Product Service Solutions (SPSS) version 24.0 and GraphPad Prism 5.01 software. The Mann–Whitney U-test and Pearson’s correlation coefficient were used for the statistical analysis. The results with values of *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001 and ****p ≤ 0.0001 were rated significant. The smaller the p value is, the greater the number of asterisks is used to represent the greater the correlation and difference. NS indicates not significant. The correlation coefficient R represents the linear correlation between the two variables. When R is greater than 0, the two variables are positively correlated; when R is less than 0, the two variables are negatively correlated. The absolute value of R is between 1 and - 1. The closer the absolute value of R is to 1, the stronger the linear correlation between the two variables. When the absolute value of R is close to 0, there is almost no linear correlation between the two variables. Generally, when the absolute value of R is greater than 0.75, there is considered to be a strong linear correlation between the two variables.
Results
Patient Characteristics
This study included 30 healthy donors (17 males and 13 females) aged 51.70 ± 14.07 years. Among the 166 patients in this study, 43 (25 males and 18 females) had late latent syphilis, 45 (19 males and 26 females) had seroresistant syphilis, 45 (28 males and 17 females) had secondary syphilis and 33 (25 males and 8 females) had neurosyphilis. The mean ages of late latent syphilis, seroresistant syphilis, secondary syphilis and neurosyphilis patients were 55.42 ± 14.91, 56.04 ± 15.46, 48.09 ± 16.38 and 57.15 ± 15.82 years, respectively. In this study, forty-five seroresistant syphilis patients were positive for serological TPPA and serum TRUST titers, with 14 cases of TRUST titers of 1:1, 20 cases of TRUST titers of 1:2, and 11 cases of TRUST titers of 1:4 accounting for 31.1%, 44.4% and 24.4% of patients, respectively. Forty-five secondary syphilis patients were positive for serological TPPA and serum TRUST titers, with 11 cases of TRUST titers of 1:8, 14 cases of TRUST titers of 1:16, 12 cases of TRUST titers of 1:32, 5 cases of TRUST titers of 1:64, and 3 cases of TRUST titers of 1:128, accounting for 24.4%, 31.1%, 26.7%, 11.1% and 6.7% of patients, respectively. Thirty-three neurosyphilis patients were positive for serological TPPA and serum TRUST titers, with 3 cases of TRUST titers of 1:1, 2 cases of TRUST titers of 1:4, 10 cases of TRUST titers of 1:8, 5 cases of TRUST titers of 1:16, 6 cases of TRUST titers of 1:32, 6 cases of TRUST titers of 1:64, and 1 case of a TRUST titer of 1:128, accounting for 9.1%, 6.1%, 33.0%, 15.1%, 18.1%, 18.1%, and 3.0% of patients, respectively. There was no TRUST titer in the serum of any late latent syphilis patient. These data are summarized in Table 1.
Serum IL-26 Levels Were Higher in Neurosyphilis Patients Than in Healthy Subjects, Late Latent Syphilis Patients, Seroresistant Syphilis Patients and Secondary Syphilis Patients
The levels of serum IL-26 were significantly higher in neurosyphilis patients than in healthy subjects (6.87 (4.36, 12.14) and 1.67 (0.09, 4.89) pg/μL, respectively; ****p < 0.0001), late latent syphilis (1.48 (0.40, 2.05) pg/μL, ****p < 0.0001), seroresistant syphilis (0.81 (0.20, 2.91) pg/μL, ****p < 0.0001) and secondary syphilis (1.66 (0.41, 4.25) pg/μL, ****p < 0.0001) with data presented at the median with interquartile range. No statistically significant difference in IL-26 levels was observed between the non-syphilitic healthy subjects and late latent syphilis patients (p = 0.7271), seroresistant syphilis patients (p = 0.4517), or secondary syphilis patients (p = 0.7771). No statistically significant difference in IL-26 levels was observed between the late latent syphilis patients and seroresistant syphilis patients (p = 0.4371), or secondary syphilis patients (p = 0.1223), and no statistically significant difference in IL-26 levels was observed between the seroresistant syphilis patients and secondary syphilis patients (p = 0.2947) (Figure 1).
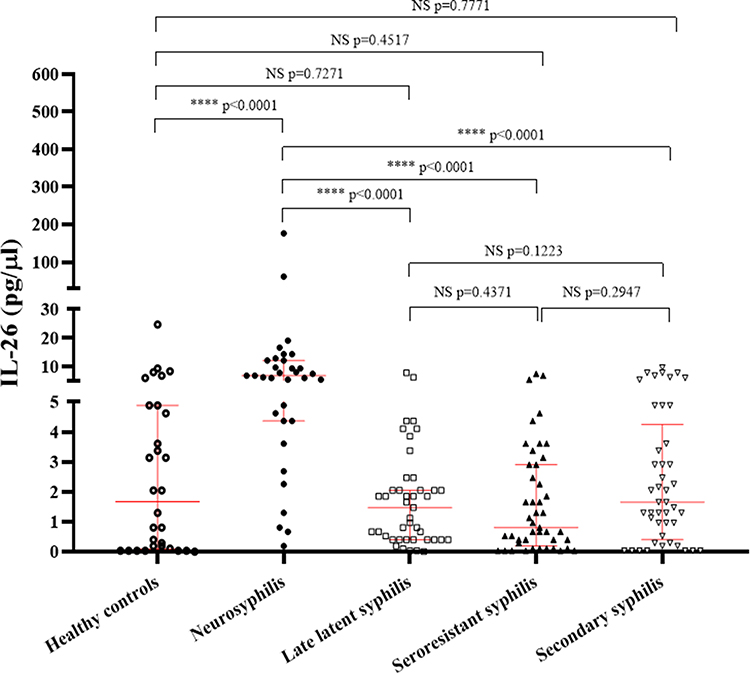 |
Figure 1 The serum concentrations of IL-26 were quantitatively examined by ELISA. Notes: ****p ≤ 0.0001 versus healthy controls or neurosyphilis patients; NS = not significant; and U-Mann–Whitney test. Each data point indicates an individual subject, and error bars and medians with interquartile ranges are displayed by red lines. |
The Concentration of Serum IL-26 Was Most Sensitive to Low-Density Lipoprotein Cholesterol (LDLC) in Late Latent Syphilis, Urine Epithelial Cell Count (SPC) in Seroresistant Syphilis, and Creatinine (CR) and Urea Creatinine Ratio (B:C) in Secondary Syphilis Patients
The serum concentration of IL-26 was not correlated with any of the clinical parameters we detected in healthy subjects. The serum concentration of IL-26 was negatively correlated with serum glutamyltranspeptidase (GGT) level (r = - 0.383, *p = 0.040), platelet distribution width (PDW) level (r = - 0.445, *p = 0.012) and platelet-large cell ratio (p-LCR) (r = - 0.359, *p = 0.047) in the peripheral blood of neurosyphilis patients. The serum concentration of IL-26 was positively correlated with serum total bilirubin (TB) level (r = 0.320, *p = 0.037) and indirect bilirubin (IBIL) level (r = 0.329, *p = 0.031) was correlated with urine protein (uPRO) level (r = 0.347, *p = 0.028) in urine and was significantly negatively correlated with low-density lipoprotein cholesterol (LDLC) level (r = - 0.438, **p = 0.004) in the serum of late latent syphilis patients. The serum concentration of IL-26 was positively correlated with serum glucose (GLU) level (r = 0.325, *p = 0.029) and globulin (GLB) level (r = 0.342, *p = 0.027), platelet (PLT) level (r = 0.297, *p = 0.048) in the peripheral blood, and urinary white blood cell count (uWBC) (r = 0.395, *p = 0.012) in urine and was significantly positively correlated with urine epithelial cell count (SPC) (r = 0.459, **p = 0.003) in urine of seroresistant syphilis patients. The serum concentration of IL-26 was negatively correlated with serum total bilirubin (TB) level (r = - 0.305, *p = 0.050), direct bilirubin (DB) level (r = - 0.342, *p = 0.027), albumin globulin ratio (A:G) (r = - 0.310, *p = 0.045) and monocyte (MO) level (r = - 0.351, *p = 0.018) in the peripheral blood of seroresistant syphilis patients. The serum concentration of IL-26 was significantly positively correlated with serum creatinine (CR) level (r = 0.463, **p = 0.004) and BUN/Cr (B:C) ratio (p = 0.024) in urine and was negatively correlated with PLT level (r = - 0.353, *p = 0.022) in peripheral blood of secondary syphilis patients. All results are shown in Figure 2.
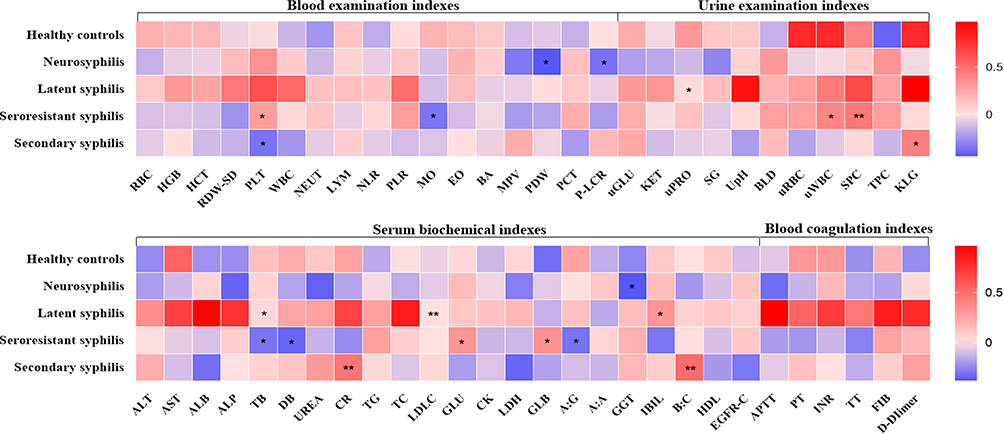 |
Figure 2 The associations between the levels of serum IL-26 and clinical routine hematological and humoral indices in healthy subjects and syphilis patients are presented in the form of a heatmap. Abbreviations: RBC, red blood cell; HGB, hemoglobin concentration; HCT, hematocrit; RDW-SD, red blood cell distribution width; PLT, platelets; WBC, white blood cell; NEUT, neutrophils; LYM, lymphocytes; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MO, monocytes; EO, eosinophils; BA, basophils; MPV, mean platelet volume; PDW, platelet distribution width; PCT, plateletcrit; P-LCR, platelet-large cell ratio; uGLU, urine glucose; KET, urine ketone; uPRO, urine protein; SG, urine specific gravity; UpH, urinary pH; BLD, urinary occult blood; uRBC, urinary red blood cell count; uWBC, urinary white blood cell count; SPC, urine epithelial cell count; TPC, bacterial count; KLG, cast count; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALB, albumin; ALP, alkaline phosphatase; TB, total bilirubin; DB, direct bilirubin; GLB, globulin; Cr, creatinine; TG, triglyceride; TC, total cholesterol; LDLC, low-density lipoprotein cholesterol; Glu, blood glucose; CK, creatine kinase; LDH, lactate dehydrogenase; A:G, albumin globulin ratio; A:A, AST-to-ALT ratio; GGT, glutamyltranspeptidase; IBIL, indirect bilirubin; B:C, BUN/Cr; HDL, high-density lipoprotein; EGFR-C, epidermal growth factor receptor C; APTT, activated partial thromboplastin time; PT, prothrombin time; INR, international normalized ratio; TT, thrombin time; FIB, fibrinogen. Notes: *p ≤ 0.05, **p ≤ 0.01 were considered statistically significant with clinical routine hematological and humoral indices in syphilis patients. Heatmap representation of the correlations between the levels of serum IL-26 and RBC, HGB, HCT, RDW-SD, PLT, WBC, NEUT, LYM, NLR, PLR, MO, EO, BA, MPV, PDW, PCT, p-LCR, uGLU, KET, uPRO, SG, UpH, BLD, uRBC, uWBC, SPC, TPC, KLG, ALT, AST, ALB, ALP, TB, DB, UREA, CR, TG, TC, LDLC, GLU, CK, LDH, GLB, (A)G, (A)A, GGT, IBIL, (B)C, HDL, EGFR-C, APTT, PT, INR, TT, FIB and D-dimer levels in healthy subjects (n = 30, Pearson coefficient), neurosyphilis patients (n = 33, Pearson coefficient), late latent syphilis patients (n = 43, Pearson coefficient), seroresistant syphilis patients (n = 45, Pearson coefficient) and secondary syphilis patients (n = 45, Pearson coefficient). |
There Was No Significant Correlation with the Concentration of Serum IL-26 and TRUST Titers in Each Type of Syphilis Patient
The potential relationship between serum TRUST titer and IL-26 level was examined using SPSS 24.0 and GraphPad Prism 5.01 software. The serum concentration of IL-26 was not correlated with serum TRUST titer in seroresistant syphilis (r = 0.164, p = 0.281), secondary syphilis (r = - 0.126, p = 0.409) or neurosyphilis patients (r = - 0.143, p = 0.428) (Figure 3).
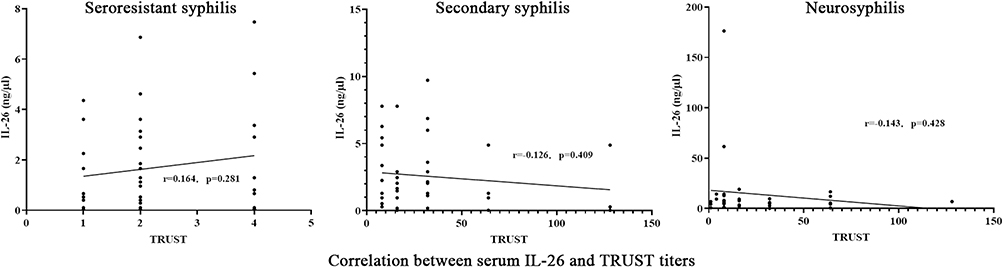 |
Figure 3 Correlation between serum IL-26 and TRUST titers in different stages of syphilis. Notes: The correlation coefficient R represents the linear correlation between serum IL-26 levels and TRUST titers in each experimental group. When the absolute value of R is greater than 0.75 and the p value is ≤0.05, there is considered to be a strong linear correlation. |
Discussion
The symptoms of neurosyphilis are complex and diverse, ranging from local symptoms, such as uveitis, hearing loss and aseptic meningitis, to systematic symptoms, such as personality and behavioral changes and paresis.18 Neurosyphilis can occur at any stage of syphilis, not just in tertiary syphilis, and its clinical manifestations are misleading, generating a high probability of missed detection and misdiagnosis as mental or neurological diseases during the process of initial differential diagnosis.19 In the current diagnostic guidelines, the most important laboratory confirmation standard for neurosyphilis is positive serum syphilis antibody accompanied by cerebrospinal fluid abnormalities of pleocytosis and elevated cerebrospinal fluid protein levels or positive CSF VRDL test results. It also includes signs and symptoms of neurosyphilis with other clinical causes of such manifestations being excluded.18 Based on a review of the literature on the sensitivity and specificity of the diagnostic guidelines used for each stage of syphilis in the past 57 years, it is necessary to reconcile criteria and diagnostics for neurosyphilis.20
The newly reported CSF biomarkers CXCL13,21 neurogranin,22 and the intrathecal synthesis index of specific anti-Treponema IgG23 have been shown to be valuable for the diagnosis of neurosyphilis. However, etiological and serological detection of syphilis in CSF is not commonly performed before the patient shows obvious symptoms of neurosyphilis due to the disadvantages and patient nonacceptance of lumbar puncture, which results in patients missing the opportunity for early antipsychotic treatment. We were inspired by a model study of the prediction of asymptomatic neurosyphilis based on routine blood tests, lymphocyte subsets, serum immunological results and other peripheral blood indicators without using CSF indicators24 and expected to find noninvasive neurosyphilis-specific screening biomarkers.
Our experimental results showed that not all patients with T. pallidum infection had an elevated serum circulating IL-26 level, but it was higher in neurosyphilis patients than in healthy subjects, late latent syphilis patients, seroresistant syphilis patients and secondary syphilis patients. The neurosyphilis-specific increase in serum IL-26 suggests that circulating IL-26 levels combined with positive syphilis serology may be of considerable potential value in the diagnosis of neurosyphilis. Compared with the laboratory diagnostic method of neurosyphilis widely used in the clinic, evaluating the occurrence of neurosyphilis by detecting serum IL-26 is more convenient because the injury of venous blood collection is very small. Generally, the laboratory tests for neurosyphilis will not be carried out until the symptoms of neurosyphilis appear clinically. Through serological IL-26 screening, the occurrence of neurosyphilis can be found very early, which may significantly improve the detection rate of neurosyphilis. In the clinical laboratory, the excess serum left by the patient after detecting syphilis antibody can be used for the determination of IL-26 level without additional blood drawing. Determination of IL-26 level can provide information on whether doctors should consider the occurrence of neurosyphilis when diagnosing syphilis patients. Since there is no good animal model for syphilis infection to perform the preliminary clinical test, determining the accuracy and feasibility of this diagnostic method will require the accumulation of more clinical data.
Since all participants were from Zhejiang Province, China, this study is limited by geographical and human groups. We look forward to more data from other peers in various countries to verify this conclusion, which will be of great significance in the diagnosis of syphilis, especially neurosyphilis. Moreover, the mechanism of the overexpression and role of circulating IL-26 level in neurosyphilis remain unclear. Although it has been demonstrated that IL-26 mainly originates from activated Th1, Th17, and NK cells and NKp44 innate lymphocytes, induces IL-8 and/or IL-10 production by epithelial cells through a receptor composed of IL-20R1/2 and induces proinflammatory cytokine production by myeloid cells,25,26 the biological function of circulating IL-26 in neurosyphilis is not clearly understood. We intend to further study the internal mechanism of IL-26 elevation in patients with neurosyphilis. In addition, syphilis patients are often coinfected with HIV, hepatitis virus and other viruses, and IL-26 has been reported to increase to varying degrees in patients with HIV, hepatitis virus or other viruses. Although syphilis can be identified through early infectious disease screening in the process of clinical diagnosis, in the case of pathogen coinfections, distinguishing which pathogen is responsible for the presenting signs and symptoms in order to identify a case of neurosyphilis will also be a problem worthy of attention in the process of clinical application. Syphilis patients are often coinfected with hepatitis virus and other viruses, and overexpression of IL-26 to varying degrees has been reported in patients with HBV and/or HCV.14,27 Although syphilis may be identified by early infectious disease screening, distinguishing the cause of the increase in IL-26 level as being other pathogens or neurosyphilis in cases of pathogen coinfection will also be a problem worthy of attention in clinical application.
Conclusion
In conclusion, the circulating IL-26 levels in patients with neurosyphilis were significantly overexpressed compared with those in healthy donors and patients with late latent syphilis, seroresistant syphilis, and secondary syphilis. The neurosyphilis-specific increase in serum IL-26 suggests that circulating IL-26 level may be a potentially significant biomarker in the diagnosis of neurosyphilis among serologically positive syphilis patients.
Summary
Neurosyphilis is one of the most destructive, concealed, changeable and difficult clinical types of syphilis due to its occurrence at any stage of infection and its involvement in the central nervous system (CNS) with irreversible neurological dysfunction and potentially serious sequelae. Currently, the clinical laboratory diagnosis of neurosyphilis mainly relies on the abnormalities of cerebrospinal fluid with reactive venereal disease research laboratory test (VDRL), but collection of cerebrospinal fluid requires lumbar puncture, which is traumatic to patients. Our results found that the serum IL-26 levels in patients with neurosyphilis were significantly higher than those in healthy donors and patients with late latent syphilis, seroresistant syphilis, and secondary syphilis. The serum IL-26 level may be a significant biomarker for the progression of neurosyphilis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beale MA, Marks M, Cole MJ, et al. Global phylogeny of Treponema pallidum lineages reveals recent expansion and spread of contemporary syphilis. Nat Microbiol. 2021;6(12):1549–1560.
2. Xu M, Xie Y, Zheng K, et al. Two Potential Syphilis Vaccine Candidates Inhibit Dissemination of Treponema pallidum. Front Immunol. 2021;12:759474.
3. Knaute DF, Graf N, Lautenschlager S, Weber R, Bosshard PP. Serological response to treatment of syphilis according to disease stage and HIV status. Clin Infect Dis. 2012;55(12):1615–1622.
4. Tong ML, Lin LR, Liu GL, et al. Factors associated with serological cure and the serofast state of HIV-negative patients with primary, secondary, latent, and tertiary syphilis. PLoS One. 2013;8(7):e70102.
5. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187.
6. Janier M, Unemo M, Dupin N, Tiplica GS, Potocnik M, Patel R. 2020 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol. 2021;35(3):574–588.
7. Wu KX, Wang XT, Hu XL, et al. LncRNA-ENST00000421645 Upregulates Kank1 to Inhibit IFN-gamma Expression and Promote T Cell Apoptosis in Neurosyphilis. Front Microbiol. 2021;12:749171.
8. Gonzalez H, Koralnik IJ, Marra CM. Neurosyphilis. Semin Neurol. 2019;39(4):448–455.
9. Skalnaya A, Fominykh V, Ivashchenko R, et al. Neurosyphilis in the modern era: literature review and case series. J Clin Neurosci. 2019;69:67–73.
10. Wong T, Fonseca K, Chernesky MA, Garceau R, Levett PN, Serhir B. Canadian Public Health Laboratory Network laboratory guidelines for the diagnosis of neurosyphilis in Canada. Can J Infect Dis Med Microbiol. 2015;26:18A–22A.
11. Musher DM. Syphilis, neurosyphilis, penicillin, and AIDS. J Infect Dis. 1991;163(6):1201–1206.
12. Qi Y, Jiang Z, Xie D, Lei N, Cai Z. Status epilepticus with focal neurologic deficits: a rare presentation of Neurosyphilis. Int J Infect Dis. 2022;117:345–348.
13. Che KF, Tengvall S, Levanen B, et al. Interleukin-26 in antibacterial host defense of human lungs. Effects on neutrophil mobilization. Am J Respir Crit Care Med. 2014;190(9):1022–1031.
14. Miot C, Beaumont E, Duluc D, et al. IL-26 is overexpressed in chronically HCV-infected patients and enhances TRAIL-mediated cytotoxicity and interferon production by human NK cells. Gut. 2015;64(9):1466–1475.
15. Beaumont E, Larochette V, Preisser L, et al. IL-26 inhibits hepatitis C virus replication in hepatocytes. J Hepatol. 2022;76(4):822–831.
16. Janier M, Hegyi V, Dupin N, et al. 2014 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol. 2014;28(12):1581–1593.
17. Dong X, Zhang J, Yang F, Liu J, Peng Y, Ge Y. CXCL8, CXCL9, and CXCL10 serum levels increase in syphilitic patients with seroresistance. J Clin Lab Anal. 2021;35(11):e24016.
18. Peermohamed S, Kogilwaimath S, Sanche S. Neurosyphilis. CMAJ. 2020;192(29):E844.
19. Chow F. Neurosyphilis. Continuum. 2021;27(4):1018–1039.
20. Tuddenham S, Katz SS, Ghanem KG. Syphilis Laboratory Guidelines: performance Characteristics of Nontreponemal Antibody Tests. Clin Infect Dis. 2020;71(Suppl 1):S21–S42.
21. Gudowska-Sawczuk M, Mroczko B. Chemokine Ligand 13 (CXCL13) in Neuroborreliosis and Neurosyphilis as Selected Spirochetal Neurological Diseases: a Review of Its Diagnostic Significance. Int J Mol Sci. 2020;21:8.
22. Xiang Y, Xin J, Le W, Yang Y. Neurogranin: a Potential Biomarker of Neurological and Mental Diseases. Front Aging Neurosci. 2020;12:584743.
23. Alberto C, Deffert C, Lambeng N, et al. Intrathecal Synthesis Index of Specific Anti-Treponema IgG: a New Tool for the Diagnosis of Neurosyphilis. Microbiol Spectr. 2022;10(1):e0147721.
24. Li W, Han J, Zhao P, et al. Predicting asymptomatic neurosyphilis using peripheral blood indicators. BMC Infect Dis. 2021;21(1):1191.
25. Braum O, Pirzer H, Fickenscher H. Interleukin-26, a highly cationic T-cell cytokine targeting epithelial cells. Antiinflamm Antiallergy Agents Med Chem. 2012;11(3):221–229.
26. Donnelly RP, Sheikh F, Dickensheets H, Savan R, Young HA, Walter MR. Interleukin-26: an IL-10-related cytokine produced by Th17 cells. Cytokine Growth Factor Rev. 2010;21(5):393–401.
27. Luo L, Jiang L, Tian Z, Zhang X. The serum interleukin-26 level is a potential biomarker for chronical hepatitis B. Medicine. 2020;99(1):e18462.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.