")
Back to Journals » Cancer Management and Research » Volume 11
Serum Dickopff 1 as a Novel Biomarker in Hepatocellular Carcinoma Diagnosis and Follow Up After Ablative Therapy
Authors Younis YS, Alegaily HS, Elagawy W, Semeya AA, Abo-Amer YEE , El-Abgeegy M, Mostafa SM, Elsergany HF, Abd-Elsalam S
Received 6 June 2019
Accepted for publication 30 October 2019
Published 17 December 2019 Volume 2019:11 Pages 10555—10562
DOI https://doi.org/10.2147/CMAR.S218532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Yehia Sadek Younis,1 Hatem Samir Alegaily,1 Waleed Elagawy,2 Atteyat Aboelmaged Semeya,3 Yousry Esam-Eldin Abo-Amer,3 Mohamed El-Abgeegy,4 Sahar Mohamed Mostafa,4 Heba Fadl Elsergany,4 Sherief Abd-Elsalam5
1Hepatology, Gastroenterology and Infectious Diseases, Benha Faculty of Medicine, Qalybia, Egypt; 2Department of Tropical Medicine, Faculty of Medicine, Port Said University, Port Fouad, Egypt; 3Hepatology, Gastroenterology and Infectious Diseases, Mahala Hepatology Teaching Hospital, Gharbia, Egypt; 4National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 5Department of Tropical Medicine, Faculty of Medicine, Tanta University, Gharbia, Egypt
Correspondence: Sherief Abd-Elsalam
Department of Tropical Medicine, Faculty of Medicine, Tanta University, El-Geish Street, Tanta, Egypt
Tel +201095159522
Email [email protected]
Background: This study aimed to evaluate the role of Dickopff 1 (DKK1) serum levels as a marker for early detection of hepatocellular carcinoma (HCC) and to compare it with alphafetoprotein (AFP) after non-surgical intervention (microwave ablation, radiofrequency ablation) in HCC.
Patients and methods: This prospective study was conducted in Al-Mahalla hepatology teaching hospital from June 2015 to June 2017. One hundred and twenty patients were included. They were classified into four groups: Group A: 40 patients with chronic liver disease; Group B: 40 patients with HCC which were divided into 2 main sub groups, group Ba which included HCC patients who were not eligible for ablative therapy and group Bb which included HCC patients who were eligible for ablative therapy; Group C: 20 healthy control subjects matched for age and sex; Group D: 20 HCC patients with negative AFP, DKK1 was done for them.
Results: There was a highly significant difference (p < 0.001) between groups regarding serum level of Dickpoff 1 with mean of 1 ng/mL in group A (cirrhotic), 2.38 ng/mL in group B (HCC), and 1.83 ng/mL in group D (AFP negative HCC) in comparison to control group C with mean of 0.54 ng/mL. There was a highly statistically significant difference (p value less =0.01) in the studied groups regarding serum Dickpoff 1 before and after intervention with a mean of 2.38 ng/mL before intervention and mean of 1.37 ng/mL after 1 month of intervention.
Conclusion: Serum Dkk-1 has higher sensitivity, specificity, and accuracy in early diagnosis of HCC than AFP.
Keywords: serum Dickopff 1, aphafeto protein, hepatocellular carcinoma, radiofrequency ablation, microwave ablation, TACE
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer, and the fifth most common cancer allover the world.1 Its allover frequency in Egypt is 2.3% among other types of cancer. HCC has increased two fold in chronic liver disease patients for the last ten years. Liver cirrhosis due to hepatitis C virus contributed to 48% of HCC cases.2–5
Without pathologic confirmation, HCC can be diagnosed using the combination of serum alpha-fetoprotein (AFP) level and imaging procedures, including ultrasonography, dynamic magnetic resonance imaging, and triphasic spiral computerized tomography.6
About 44% of patients are diagnosed at localized disease stage and curative treatment can be done to only 30% of patients with HCC at the time of diagnosis. So early diagnosis must be considered.7
Since AFP was discovered in HCC patients in 1964,8 it has been considered as the most useful marker in these patients9 in spite of its low sensitivity (25–60%),10 and specificity, and its presence in 11–47% of patients with cirrhosis and 15–58% of patients with chronic hepatitis.11
More than 20 serum proteins in addition to AFP have clinical significance in HCC's early diagnosis and several of them are considered to have advantages over AFP. DKK1 belongs to a family of secreted proteins that play an important role in HCC progression through the promotion of cytoplasmic/nuclear accumulation of beta-catenin in HCC cells via the Wnt/beta-catenin signaling pathway.11,12
Shen et al, (2012)12 reported that DKK1 had better diagnostic value in HCC patients than AFP, especially in early stages of HCC with low AFP levels. Combined testing of serum DKK1 and AFP was more accurate than either of them alone.
This study aimed to evaluate the role of Dickopff 1 (DKK1) serum levels as a marker for early detection of hepatocellular carcinoma (HCC) and to compare it with alphafetoprotein (AFP) after non-surgical intervention (microwave ablation, radiofrequency ablation) in HCC.
Patients and Methods
This prospective study was conducted in Al-Mahalla hepatology teaching hospital from June 2015 to June 2017. The study protocol was performed according to the ethical guidelines of Helinski declaration; and the protocol was approved by the ethics committee of Tanta University faculty of medicine. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. A written informed consent was signed by all patients participating in this study.
One hundred and twenty patients were included. They were classified into four groups: Group A: included 40 patients with chronic liver disease according to clinical, laboratory, and ultrasonographical findings divided into 2 sub-groups on basis of child-Pugh score, both AFP and DKK1 were measured, subgroup A (a): 20 cases of CLD child A and B, subgroup A (b): 20 cases of CLD child C.
Group B: included 40 patients with HCC. They were diagnosed by spiral CT. DKK1 was done and the cases were subdivided into group B (a): included patients who were not eligible for non-surgical intervention (MWA and RFA). The exclusion criteria for non-surgical intervention were portal vein thrombosis, hepatic metastasis (secondaries) or abdominal lymph node infiltration, tumors larger than 4 cm in diameter, tumors located within 1 cm of liver hilum, gall bladder or common bile duct, tumors in the dome of liver which may be unreachable percutaneously, platelets less than 60,000 mL, prothrombin concentration less than 60% and Child–Pugh class C patients; Group B (b): included patients who were eligible for non-surgical intervention, AFP and Dkk1 were measured before intervention and one month after intervention; whereas the inclusion criteria for nonsurgical intervention were tumors smaller than 4 cm in diameter, platelets more than 60,000 mL, prothrombin concentration more than 60%, and Child Pugh class A or B.
Group C: included 20 healthy control subjects.
Group D: included 20 HCC patients with negative AFP, DKK1 was done for them.
History was taken. Clinical examination was done. Laboratory investigations including liver functions, viral markers, and AFP and DKK1 estimation by ELISA technique were performed for all subjects.
AFP-L3 concentration was determined using AFP-L3 ELISA kit, Catalog No. E1117h, EIAab Science Co, Ltd. The kits used to assay the DKK1 in the sample of serum of human patients and controls uses a double–antibody sandwich enzyme linked immunosorbent assay to assess the level of human DKK1 in serum samples.
Statistical Analysis
Data were analyzed using Statistical Program for Social Science (SPSS) version 20.0 Statistical tests including t-test of significance was used when comparing two means. A one-way analysis of variance (ANOVA) was used when comparing more than two means. Post Hoc test (Tukey’s test) was used for multiple comparisons between more than two means. Receiver operating characteristic (ROC curve) analysis was used to find out the overall predictivity of parameter.
Results
The demographic and clinical data of the studied groups are demonstrated in Table 1. AFP and Dickpoff 1 showed highly significant statistical difference between all groups (p < 0.001) in both. AFP had a mean 11.06± 5.19 ng/mL in Group A (cirrhotic), a mean of 293.43±318.03 ng/mL in group Ba (HCC patients not eligible for intervention), a mean of 815.65± 490.32 ng/mL in group Bb (HCC patients eligible for intervention), a mean of 1.43± 0.43 ng/mL in group C, and mean of 12.33± 3.02 ng/mL in group D (AFP negative group) (Table 2).
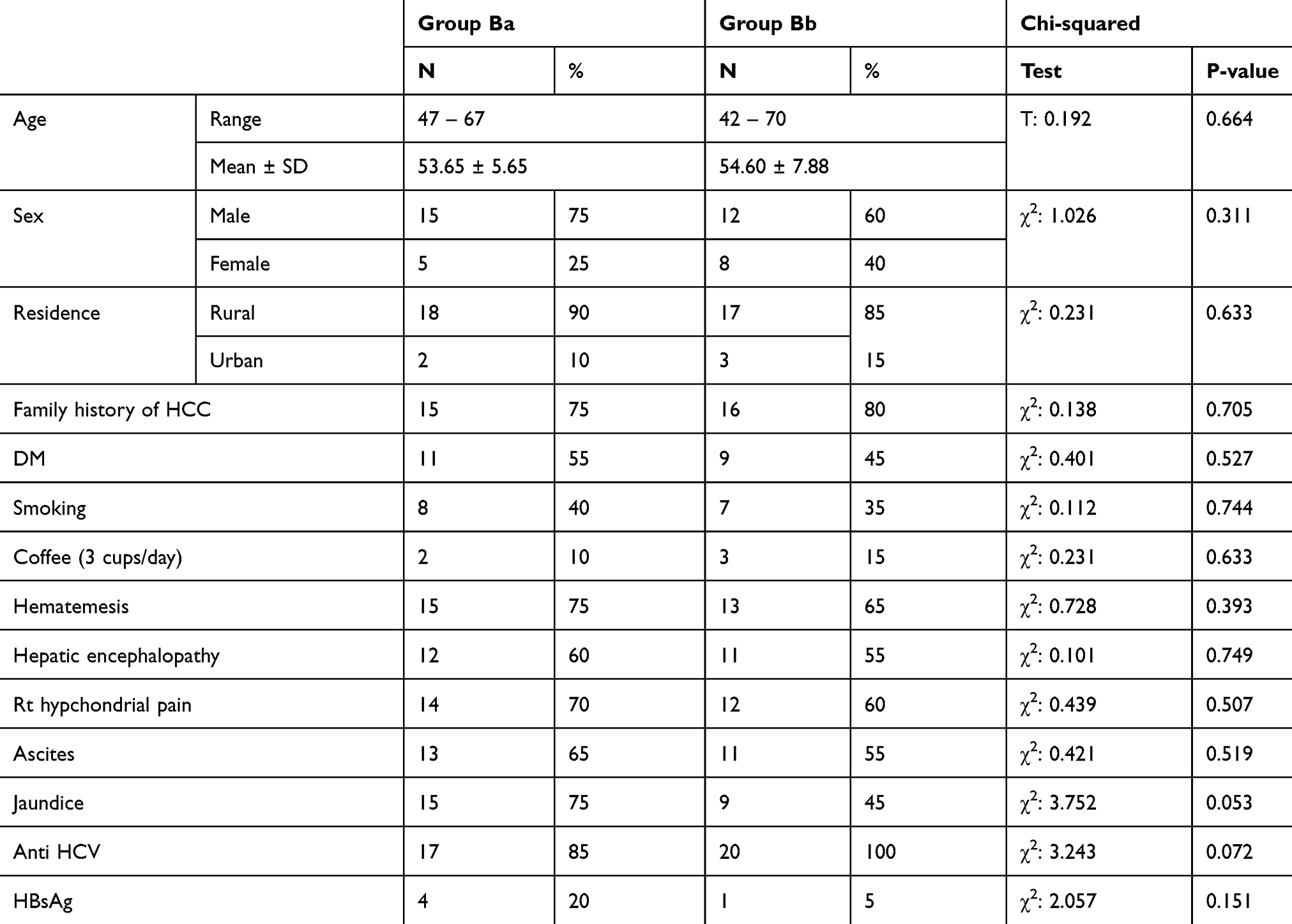 |
Table 1 Demographic and Clinical Data of All Studied Patients |
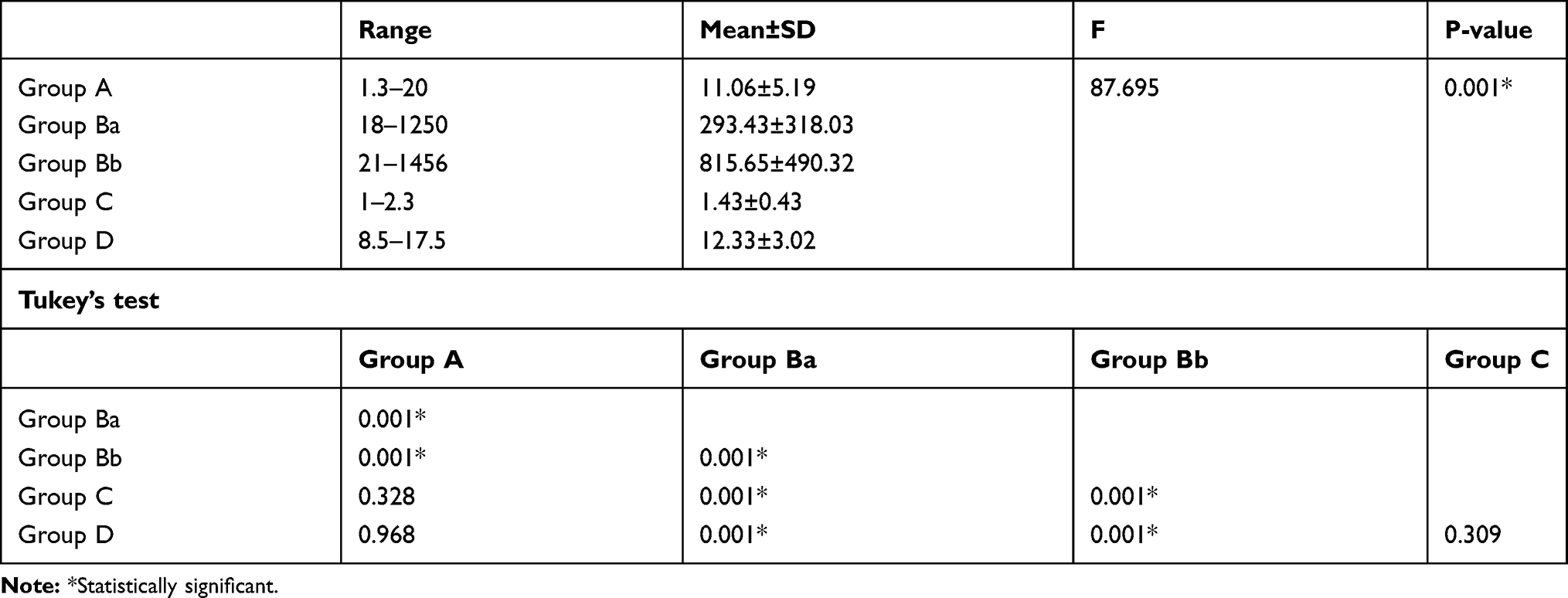 |
Table 2 Comparison Between Different Groups as Regards to Serum Alfa Fetoprotein |
Dickpoff 1 had a mean 1.28±0.1 ng/mL in Group A (cirrhotic), 2.3±0.08 ng/mL in group Ba (HCC patients not eligible for intervention), 2.38± 0.33 ng/mL in group Bb (HCC patients eligible for intervention), 0.73±0.12 ng/mL in group C, and 1.83±0.88 ng/mL in group D (AFP negative group) (Table 3).
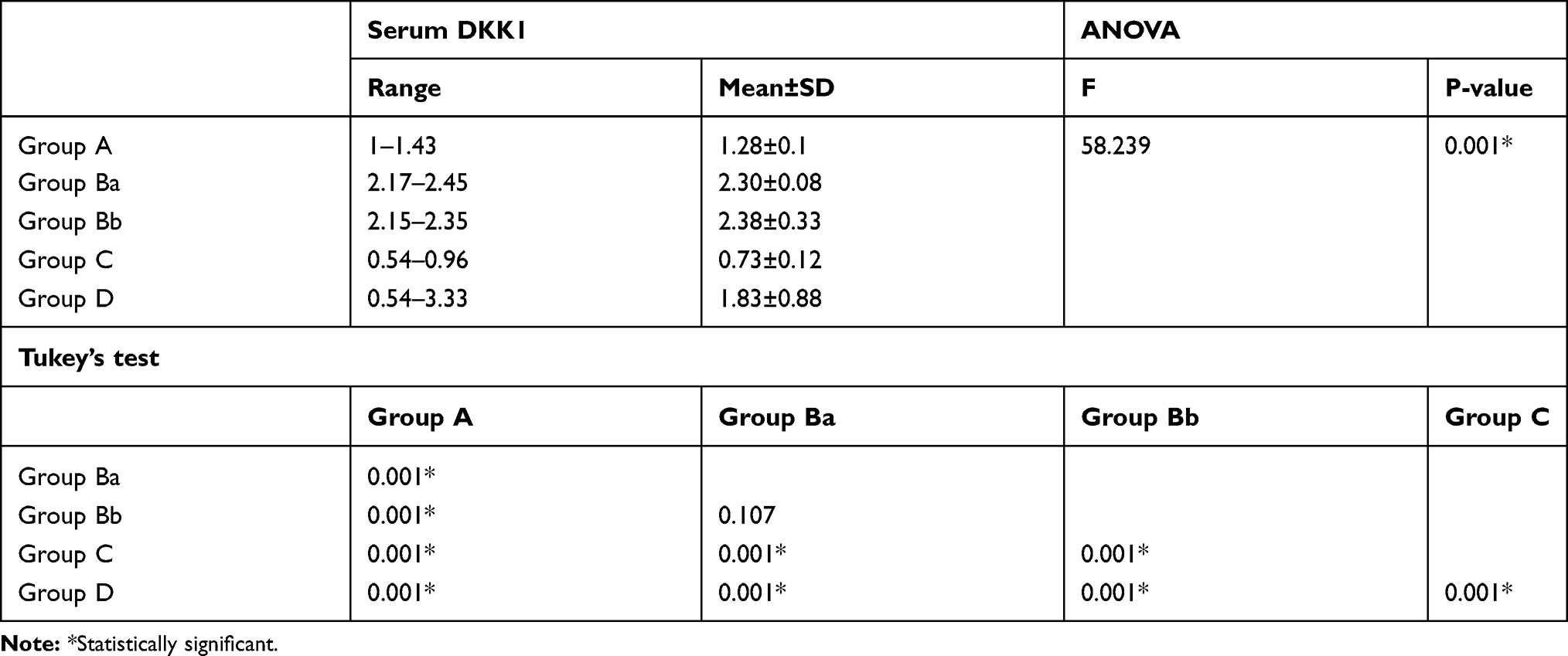 |
Table 3 Comparison Between Different Studied Groups Regarding Serum DKK1 Level |
AFP was significantly lower one month after intervention (RFA and MWA) (332.98 ±444.74 ng/mL) than before intervention (815.65±490.32) (Table 4). Whereas; DKK1 was highly significantly lower one month after intervention (RFA and MWA) (1.37±1.24 ng/mL) than before intervention (2.38±0.33 ng/mL) (Table 5).
 |
Table 4 Comparison Between Serum Level of AFP in Group Bb Before Intervention (MWA and RFA) and One Month After intervention |
 |
Table 5 Comparison in Group Bb of Serum Level of DKK1 Before and After Intervention |
Moreover; DKK1 was highly significantly lower in completely ablated cases (0.68± 0.13 ng/mL) than recurrent cases (3.45± 0.25) (Table 6).
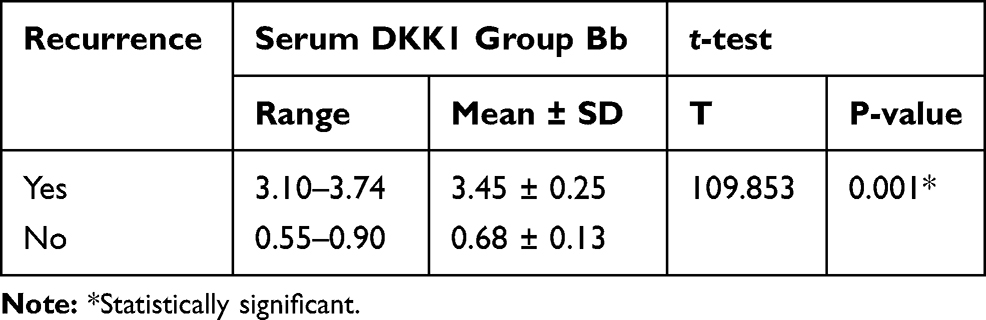 |
Table 6 Serum DKK1 in Both Recurrence and Completely Ablated Cases Group Bb |
Regarding recurrence of HCC one month after ablation; in group Bb 4 cases (20%) were detected as recurrent cases of HCC by serum AFP level, while 5 cases (25%) were detected as recurrent cases of HCC by serum DKK1 (Table 7).
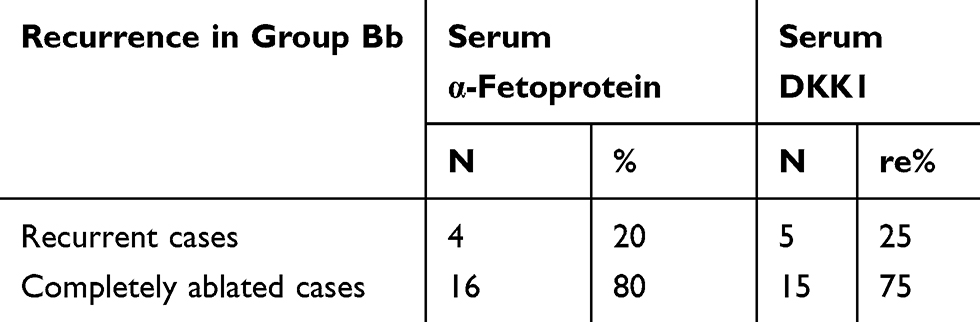 |
Table 7 Serum Level of AFP and DKK1 in Recurrent Cases and Completely Ablated Lesions After One Month in Group Bb (HCC) |
14 cases (70%) were positive for serum DKK1 in AFP negative group (group D) with cut off value more than 2.1 ng/mL (Table 8).
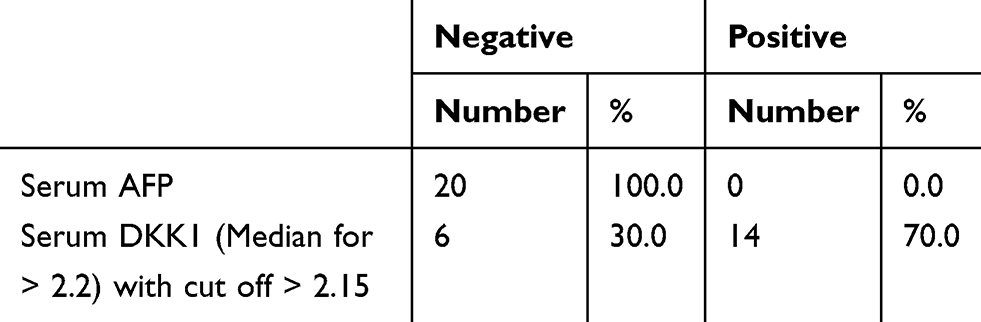 |
Table 8 Level of Serum DKK1 in Group D (AFP Negative Group) |
Regarding the cut off serum level of DKK1 above 2.1 ng/mL in recurrent cases of HCC after ablation, all sensitivity, specificity, positive predictive value, and negative predictive value were 100%, while for AFP at cut off serum level value of more than 400 ng/mL, sensitivity, specificity, positive predictive value, and negative predictive value were 80%, 60%, 67%, and 75% respectively (Table 9).
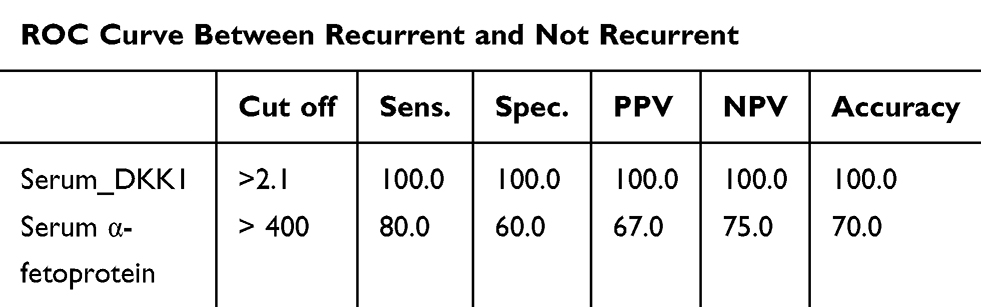 |
Table 9 ROC Curve Between Recurrent and Non-recurrent HCC After Ablation |
Regarding the cut off serum level of DKK1 of 1.4 ng/mL sensitivity, specificity, positive predictive value, and negative predictive value were 90%, 100%, 100%, and 92% respectively (Table 10), while, regarding AFP at cut off serum level value of more than 8.5 ng/mL, sensitivity, specificity, positive predictive value, and negative predictive value were 60%, 70%, 80%, and 45% respectively (Table 11).
 |
Table 10 Specificity and Sensitivity of Serum DKK1 Cut off Level of 1.4 ng |
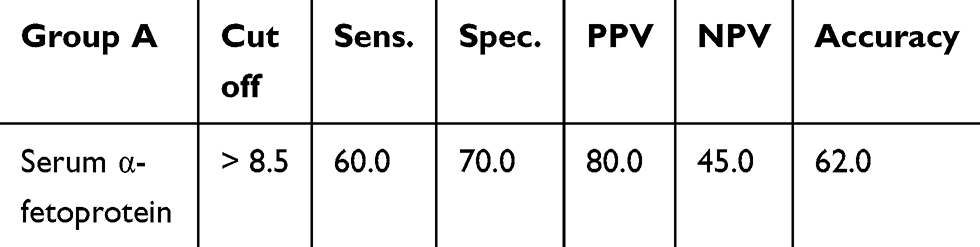 |
Table 11 Specificity and Sensitivity of Serum α-Fetoprotein Cut off Level of > 8.5 ng/mL |
Discussion
This study showed significant AFP elevation in group Bb (HCC patients eligible for intervention), with a mean of 815.65±490.32 ng/mL compared to group Ba (not eligible for intervention), with a mean of 293.43±318.03 ng/mL, group C (healthy controls) with a mean of 1.43±0.43 ng/mL; group D (AFP negative group), with a mean of 12.33 ng/mL and Group A (cirrhotic), with a mean of 11.06±5.19 ng/mL. This was similar to Zahran et al, 2016,13 who found significant AFP elevation in HCC patients with a mean of 2779.74 ± 7928.8 compared to the cirrhotic group with mean of 8.65 ± 7.75. Also, Erdal et al, 2016,14 detected similar AFP findings with a mean of 1466.3±1228.4 and 7.3±1.9 in HCC and cirrhotic patients respectively.
The present study showed DKK1 was significantly higher in group Bb (HCC patients eligible for intervention), (mean 2.38 ng/mL± 0.33ng/mL) than in group Ba (not eligible for intervention), (mean2.3±0.08 ng/mL), group D (AFP negative group), with mean of 1.83 ±0.88 ng/mL, Group A (cirrhotic), (mean 1.28±0.1 ng/mL) and Group C (healthy controls), with a mean of 0.73± 0.12 ng/mL. Also, DKK1 was elevated in group D compared to group A and in group A compared to group C. In agreement with our study, Erdal et al, 2016,14 detected that DKK1 levels were elevated in HCC patients (2.1±0.3 ng) compared to cirrhotic group (1.4±0.08 ng). Also, Zahran et al, 2016,13 detected similar findings in DKK1 levels in HCC patients (mean 1.815 ± 0.625) compared with others.
This study was also similar to that of Shen et al, 2012,12 which reported that serum levels of DKK1 were elevated in HCC patients in comparison to all controls. Also, Zhang et al, 2014,15 showed that DKK1 level was higher in HCC patients than cirrhotic ones, and healthy controls.
Our study results also agree with Prieto and Cha, 2013,16 who reported that DKK1 levels could differentiate between chronic HBV infection, cirrhosis, and HCC. Also, Sharaf et al, 2016,17 detected the significant difference between values of DKK1 in HCC patients (mean 4.97±2.23 ng/mL) compared to liver cirrhosis patients (mean 2.28±0.90 ng/mL).
On the other hand, the current study does not agree with Tung et al, 2011,18 who did not show any significant difference in serum DKK-1 levels between cirrhotic and non-cirrhotic patients, but elevation in HCC group.
Serum DKK1 – in our study – was significantly lower at one month after intervention (RFA and MWA) (1.37 ± 1.24 ng/mL) than before intervention (2.38±0.33 ng/mL) in group Bb (HCC group eligible for non-surgical intervention (RFA and MWA)), which was similar to Sharaf et al's study, 2016,17 which showed decrease in serum DKK1 levels after radiofrequency ablation or alcohol injection of HCC (P<0.001). Also, Yang et al, 2013,19 concluded that high serum Dkk-1 level was associated with poorer overall and relapse-free survival than low Dkk-1. Tung et al, 2011,18 stated the reduction of serum DKK1 levels after liver resection in HCC patients. So, high DKK1 could be a result of over-production of it by tumor cells.
In this study, at one month after ablation in group Bb (HCC patients eligible for non-surgical intervention) 4 cases (20%) were detected as recurrent cases of HCC by serum AFP level; while; 5 cases (25%) were detected as recurrent cases of HCC by serum DKK1. These results were similar to those of Tung et al, 2011,18 who stated that AFP was the most commonly used tumor marker in spite of its low specificity and sensitivity in the primary diagnosis of HCC or diagnosis of recurrence after treatment. Also, Shen et al, 2012,12 concluded that DKK1 was more accurate than AFP in early detection of HCC, which could improve patient survival.
Our study was also similar to that of Zhang et al, 2014,15 whose meta-analysis showed the acceptable accuracy of DKK1 in comparison to AFP in detection of HCC.
Also, Fouad et al, 2016,20 stated that serum DKK1 could be a complementary test to AFP in diagnosis of HCC.
In our study, 14 cases (70%) were positive for serum DKK1 with cut off value more than 2.1 ng/mL, in AFP negative group (group D). This is in agreement with Sharaf et al, 2016,17 who stated that 8 of 13 AFP negative HCC patients, and all AFP-positive patients, had positive DKK1 results. Also, this study concluded that testing for both DKK1 and AFP increased the accuracy of HCC diagnosis. Meanwhile, DKK1 could be used alone with inconclusive AFP.
DKK1 could be considered as a promising prognostic marker for follow up of HCC patients who underwent loco-regional treatment. This was also similar to Yang et al, 2013,19 who stated the better sensitivity and accuracy of Dkk-1 than AFP, and that 73.1% of the patients with early HCC and normal AFP could be diagnosed by Dkk-1.
According to Table 8, correlation between size of HCC and serum level of AFP in both groups Ba and Bb was not significant; while, serum DKK1 protein correlated significantly with tumor size.
This was similar to Sharaf et al, 2016,17 who stated that serum DKK1 was more elevated in HCC patients with focal lesions >3 cm than focal lesions <3 cm. This indicated that DKK1 level increases with disease progression from cirrhosis to small focal lesion then large focal mass. Also, these results were similar to Tung et al, 2011,18 who reported a stepwise increase in serum DKK1 from liver cirrhosis to early HCC then to advanced HCC.
Regarding cut off serum level of DKK1 above 2.1 ng/mL in recurrent cases of HCC after ablation, sensitivity, specificity, positive predictive value, and negative predictive value were 100%, while AFP at cut off serum level value of more than 400 ng/mL had sensitivity of 80%, specificity of 60%, positive predictive value of 75%, and negative predictive value of 67%.
This was similar to Zahran et al, 2016,13 who stated that ROC curve showed that Dkk1 had best diagnostic performance compared to AFP in HCC patients. Also, our study was similar to that of Yang et al, 2013,19 who demonstrated larger AUC of DKK1 (0.877) than that of AFP (0.793), (p<0.05); meaning better sensitivity, specificity, and accuracy of DKK1. Also, Beppu et al, 2010,21 stated that the higher the AFP cut-off level, the higher the specificity, and the lower the sensitivity.
On the other hand, the optimum cut off in our study did not agree with Sharaf et al, 2016,17 who concluded that the optimum cut off value of DKK1 for diagnosis of HCC was 4.3 ng/mL (sensitivity 66.7%, specificity 96.6%, AUC 0.89, and P<0.001). While the optimum cut off value for AFP was > 101 ng/mL with sensitivity of 90% and specificity of 75.9% (p<0.001).
Also, our result did not agree with Erdal et al, 2016,14 who found that DKK1 alone had lower sensitivity, specificity, PPV, and NPV than AFP alone when used for comparing HCC patients with cirrhosis patients and healthy controls. So, DKK1 could not be considered alone as a substitute for AFP in screening of HCC. However, DKK1 and AFP together could be considered to improve the accuracy of the screening.
According to Kim et al, 2015,22 the cut off of DKK-1 value was 1.01 ng/mL (AUC=0.829; sensitivity, 90.7%; specificity, 62.0%), AFP cut off value was 7.5 ng/mL (AUC=0.794; sensitivity, 69.3%; specificity, 87.6%). According to Yang et al, 2013,19 AFP cut off value of 20 ng/mL had sensitivity of 28.8%-50% in 2 independent cohorts.
According to Kudo et al, 2010,23 AFP cut off value of 100 ng/mL had sensitivity of 20%-30%.
In the current study, DKK1 at cut off level of 1.4 ng/mL had sensitivity of 90% and specificity of 100% respectively. This was similar to a study by Zahran et al, 2016,13 which showed the same results. On the other hand, it does not agree with Fouad et al, 2016,20 who stated the optimum cut off level was 1.5 ng/mL (sensitivity was 67% and specificity was 89.3%).
Regarding serum AFP in our study, cut off level > 8.5 ng/mL had sensitivity and specificity of 60% and 70% respectively, which agreed with Zhao et al, 2017,24 who stated that AFP had sensitivity of 39–65% and a specificity of 70–94%, but our study does not agree with Chan et al, 2013,25 who reported that the optimal AFP cut-off value was 10 ng/mL (sensitivity of 82.6% and specificity of 70.4%).
The limitation of this study was mainly the small number of patients. So, large sample size and long period of follow up might be needed.
Conclusion
Patients with early HCC, and AFP negative HCC patients have high serum levels of Dkk-1 and sensitivity and specificity were higher than AFP. In addition, serum Dkk-1 decreases after intervention (RF and MWA) and increases again after recurrence with higher accuracy for detection of recurrence than AFP. Serum Dkk-1 alone or in combination with AFP can improve the diagnostic efficacy of early detection of HCC compared to AFP alone.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu AM, Yao TG, Wang W, et al. Circulating miR-15b and miR- 130b in serum as potential markers for detecting hepatocellular carcinoma: a retrospective cohort study. BMJ Open. 2012;2:e000825.
2. El-Zayadi AR, Badran HM, Barakat EM, et al. Hepato cellular carcinoma in Egypt: a single centre study over a decade. World J Gastroenterol. 2005;11(33):5193–5198. doi:10.3748/wjg.v11.i33.5193
3. Negm O, AbouSaif S, El Gharib M, et al. Role of low-molecular-weight heparins in prevention of thromboembolic complication after transarterial chemoembolization in hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2017;29(3):317–321. doi:10.1097/MEG.0000000000000790
4. Elwan N, Salem ML, Kobtan A, et al. High numbers of myeloid derived suppressor cells in peripheral blood and ascitic fluid of cirrhotic and HCC patients. Immunol Invest. 2018;47(2):169–180. doi:10.1080/08820139.2017.1407787
5. Abdelfattah AAM, Rizk F, Hawash N, et al. Randomized trial of preoperative administration of oral pregabalin for postoperative analgesia in patients scheduled for radiofrequency ablation of focal lesions in the liver. Int J Hyperthermia. 2018;34(8):1367–1371. doi:10.1080/02656736.2018.1424946
6. Aghoram R, Cai P, Dickinson JA. Alpha-foeto protein and/or liver ultrasonography for screening of hepatocellular carcinoma in patients with chronic hepatitis B. Cochrane Database Syst Rev. 2012;9:CD002799.
7. Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002;35:519–524. doi:10.1053/jhep.2002.32089
8. IuS T. Detection of embryo-specific alpha-globulin in the blood serum of a patient with primary liver cancer. Vopr Med Khim. 1964;10:90–91.
9. Zhou L, Liu J, Luo F. Serum tumor markers for detection of hepatocellularcarcinoma. World J Gastroenterol. 2006;12:1175–1181. doi:10.3748/wjg.v12.i8.1175
10. El-Serag HB, Marrero JA, Rudolph L, et al. Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology. 2008;134:1752–1763. doi:10.1053/j.gastro.2008.02.090
11. Yu B, Yang X, Xu Y, et al. Elevated expression of DKK1 is associated with cytoplasmic/nuclear beta-catenin accumulation and poor prognosis in hepatocellular carcinomas. J Hepatol. 2009;50:948–957. doi:10.1016/j.jhep.2008.11.020
12. Shen Q, Fan J, Yang XR, et al. Serum DKK1 as a protein biomarker for the diagnosis of hepatocellular carcinoma: a large-scale, multicentre study. Lancet Oncol. 2102;13:817–826. doi:10.1016/S1470-2045(12)70233-4
13. Zahran F, Barakat L, Radwan N, et al. Comparative study betweeN DKK-1 and AFP FOR diagnosing of hepatocellular carcinoma among Egyptian patients. ejpmr. 2016;3(9):20–27.
14. Erdal H, Utku OG, Karatay E, Celik B, Elbeg S, Doğan I. Combination of DKK1 and AFP improves diagnostic accuracy of hepatocellular carcinoma compared with either marker alone. Turk J Gastroenterol. 2016;27:375–381. doi:10.5152/tjg
15. Zhang J, Zhao Y, Yang Q. Sensitivity and specificity of Dickkopf-1 protein in serum for diagnosing hepatocellular carcinoma: a meta-analysis. Int J Biol Markers. 2014;29(4):
16. Prieto PA, Charles H. DKK1 as a serum biomarker for hepatocellular carcinoma. HepatobiliarySurgNutr. 2013;2(3):127–128.
17. Sharaf A, El-Badrawy EL, Khalifa N, et al. Dickkopf-1: as a diagnostic and prognostic serum marker for hepatocellular carcinoma. Afro-Egypt J Infect Endem Dis. 2016;6(4):156–165.
18. Tung EK, Mak CK, Fatima S, et al. Clinicopathological and prognostic significance of serum and tissue Dickkopf-1 levels in human hepatocellular carcinoma. Liver Int. 2011;31:1494–1504. doi:10.1111/j.1478-3231.2011.02597.x
19. Yang H, Chen GD, Fang F, et al. Dickkopf-1: as a diagnostic and prognostic serum marker for early hepatocellular carcinoma. Int J Biol Markers. 2013;28(3):286297. doi:10.5301/JBM.5000015
20. Fouad YM, Mohamed HI, Kamal EM, et al. Clinical significance and diagnostic value of serum Dickkopf-1 in patients with hepatocellular carcinoma. Scand J Gastroenterol. 2016;51(9):1133–1137. doi:10.3109/00365521.2016.1172337
21. Beppu T, Sugimoto K, Shiraki K, et al. Clinical significance of tumor markers in detection of recurrent hepatocellular carcinoma after radiofrequency ablation. Int J Mol Med. 2010;26(3):425–433.
22. Kim SU, Park JH, Kim HS, et al. Serum Dickkopf-1 as a biomarker for the diagnosis of hepatocellular carcinoma. Yonsei Med J. 2015;56(5):1296–1306. doi:10.3349/ymj.2015.56.5.1296
23. Kudo M. Radiofrequency ablation for hepatocellular carcinoma: updated review in 2010. Oncology. 2010;78(Suppl 1):113–124. doi:10.1159/000315239
24. Zhao Y, Gao Q, Pei L, et al. Currentstatus and future prospects of biomarkers in the diagnosis of hepatocellular carcinoma. Int J Biol Markers. 2017;32(4):e361–e369. doi:10.5301/ijbm.5000299
25. Chan S, Mo F, Philip J, et al. Performance of serum a-fetoprotein levels in the diagnosis of hepatocellular carcinoma in patients with a hepatic mass. HPB. 2014;16:366–367. doi:10.1111/hpb.12146
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.