")
Back to Journals » Infection and Drug Resistance » Volume 14
Serological Evidence of West Nile Virus Infection Among Humans, Horses, and Pigeons in Saudi Arabia
Authors Alkharsah KR , Al-Afaleq AI
Received 16 November 2021
Accepted for publication 14 December 2021
Published 21 December 2021 Volume 2021:14 Pages 5595—5601
DOI https://doi.org/10.2147/IDR.S348648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Khaled R Alkharsah, 1 Adel I Al-Afaleq 2
1Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Kingdom of Saudi Arabia; 2Department of Environmental Health, College of Public Health, Imam Abdulrahman Bin Faisal University (IAU), Dammam, Kingdom of Saudi Arabia
Correspondence: Adel I Al-Afaleq Email [email protected]
Purpose: This study was designed to investigate the seroprevalence of WNV antibodies in humans, horses, and pigeons in the Eastern Province of Saudi Arabia.
Materials and Methods: Blood samples were collected from 323 humans, 147 horses, and 282 pigeons from two regions, Al-Ahsa and Al-Qatif, in East of Saudi Arabia. Serum samples were tested for anti-WNV antibodies by ELISA.
Results: The percentage of anti-WNV antibodies in the human population was found to be 9.6% (3.1% in females and 6.5% in males). This percentage was much higher in horses, as 71.4% (105/147) of the horses had anti-WNV antibodies. However, no statistically significant difference in the anti-WNV antibody prevalence was found among horses from the two regions, Al-Ahsa (73.9%) and Al-Qatif (70.3%) (P value 0.665, 95% CI 0.37– 1.82). No significant difference was found in the frequency of WNV antibodies among different age groups from humans or horses. Noticeably, 72.7% of the horses had detectable anti-WNV antibodies by the age of 1 year. In total, 53.19% (150/282) of the pigeons in the study had anti-WNV antibodies.
Conclusion: Our study provided the first evidence for anti-WNV antibody detection in humans and pigeons. This study further ascertained the high seroprevalence of the virus in horses as reported previously by Hemida et al 2019. Overall data indicates that WNV is endemic in Saudi Arabia. These findings suggest that more attention should be given to the diagnosis and reporting of WNV infections in human and animals and monitoring of virus circulation in the environment.
Keywords: pigeons, horse, Saudi Arabia, West Nile virus, zoonotic disease
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
West Nile virus (WNV) is an enveloped RNA virus that belongs to the family Flaviviridae. This virus was isolated for the first time in 1937 from a feverish patient from the West Nile province of Uganda.1 The main WNV reservoirs of WNV are bird species, in which the virus can cause high levels of viremia that is sufficient to infect mosquito vectors.2 The principal mosquito vector involved in WNV transmission belongs to the Culex species, where they get the virus from a viremic birds.3 Other mosquitoes such as Aedes species and Coquillettidia richiardii also serve as vectors for the transmission of WNV depending on the geographical location.4
The virus thereafter replicates in the gut of the mosquito to the infectious levels and transmit to another bird during hematophagy.3 In this complete cycle, the virus circulates in nature among birds and culex mosquitoes. However, an infected mosquito could also transmit the virus to other vertebrate species including horses and humans, which are considered incidental hosts as they only develop transient and low level of viremia insufficient to infect new mosquitoes.5 Many other vertebrate hosts were reported to be infected with WNV, including sheep, cats, and rodents, but are mostly considered a dead-end infection (incidental host) except for fox squirrels and crocodiles.1 Despite the fact that mosquito bite is the main route of WNV transmission, other routes of transmission were also reported during WNV outbreaks such as blood transfusion and organ transplantation, hypothetical aerosol transmission among laboratory workers and animal handlers, and only one case of mother to child vertical transmission.1
Most human WNV infections are asymptomatic, but when symptomatic, these infections are characterized by mild fever, rash, headache, gastrointestinal problems, arthralgia, and myalgia collectively called as West Nile fever (WNF).6 Less than 1% of the infected individuals may experience more invasive infection called West Nile neuroinvasive disease (WNND), which is manifested by either meningitis or encephalitis, or less frequently poliomyelitis.6
WNV received little attention till the year 1999, when it caused an outbreak in humans and horses with neuroinvasive manifestations.7 Since then, multiple outbreaks in human and animals were reported with increasing incidences of human and equine cases.1,8 Currently, WNV is considered an important zoonotic disease in the USA and other countries.9
Several studies documented the presence of WNV antibodies in humans and animals in the Mediterranean area and the Arabian Peninsula.10–13 A systematic review investigated the prevalence of WNV antibodies in the countries of the Eastern Mediterranean Regional Office of WHO (EMRO). It was found that antibodies against WNV were reported in the general population of 17 out of the 22 countries in the region at variable percentages ranging from 1% to 61%.12 There was no data regarding this from Kuwait, Bahrain, and Oman.12 In a recent study, Dargham et al estimated 10.4% seroprevalence of anti-WNV IgG antibodies in healthy blood donors of multiple nationalities in Qatar.
Only two studies from Saudi Arabia reported the presence of WNV-specific antibodies in the horses.10,13 The first study included 63 horses from Al-Ahsa region in 2014 and reported WNV antibodies by ELISA in 33.3% of the recruited horses.10 A larger study included 200 horses from multiple regions and tested serum samples collected between 2013 and 2015 employing ELISA followed by microneutralization assay for the positive samples.13 The study found that the seroprevalence of WNV was the highest in Al-Jubail (60%) followed by Al-Qatif (55%) then by Al-Ahsa (51%), which are regions from the Eastern Province, while it was lower in Qassim and Riyadh, which are the central regions.13 However, no study has been conducted to investigate the seroprevalence of WNV in human and pigeons. Keeping all this in view, the present study was designed to provide the serological evidence of anti-WNV antibodies in humans, equids, and pigeons from two different regions of the Eastern Province of Saudi Arabia.
Materials and Methods
Study Settings
The Eastern Province, named according to its geographical location (Figure 1) of Saudi Arabia is the largest and the third most populated region comprising about 5 million inhabitants.14 Al-Ahsa is the largest governorate in the Eastern Province (latitude 25.3800° N, 49.5888° E) comprising about a million inhabitants. While Qatif is located to the north of the province (latitude 26.5765° N, 49.9982° E) and comprises about 500,000 inhabitants. Both regions are agricultural regions and are about 170 km apart.
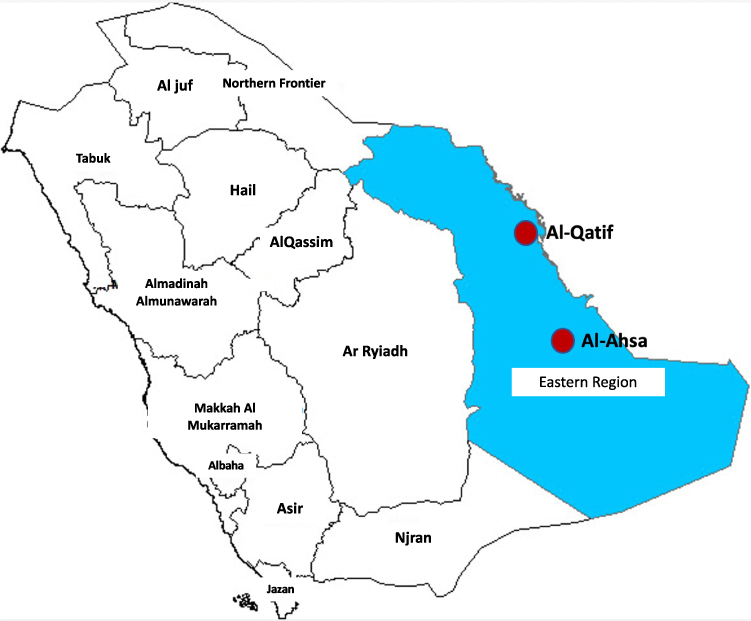 |
Figure 1 Map of Saudi Arabia showing the location of Eastern Province and the regions of Al-Qatif and Al-Ahsa. |
Sample Collection
Horse samples: About 3–5 mL of blood sample was collected from 147 apparently healthy horses from various private farms and stables in Al-Ahsa and Al-Qatif regions from the Eastern Province of Saudi Arabia (Figure 1). Blood samples were obtained from the jugular vein. All horses included in this study were locally bred.
Pigeon samples: Around 1–2 mL blood was collected from 282 local breed and free flying pigeons from Al-Qatif region (Figure 1). Samples were collected from pigeons, which were sacrificed for human consumption.
Human samples: About 3–5 mL blood sample was collected from 323 human subjects residing in the region at least 2 years prior to sampling. One hundred and forty-eight samples were collected from apparently healthy blood donors and 175 samples were collected from diabetic patients and patients with psychiatric disorders who were recruited for other studies. Demographic data were obtained from the medical records.
In all cases, blood sampling was done during the period 2014–2017 and serum was separated and stored at −80°C till the time of analysis.
Detection of Anti-WNV Antibody
Detection of anti-WNV IgG antibodies in the sera obtained from the horses and bird samples was done using the blocking ELISA assay technique, Ingezim WNV Compac kit (Ingenasa, Madrid, Spain). Serum samples were diluted 1:5 in the provided dilution buffer. The diluted serum samples were added to the wells of the 96-well plate, which were coated with WNV antigen, then incubated at room temperature overnight. The wells were washed thereafter with washing buffer and then incubated with anti-WNV antibody conjugated to the enzyme horseradish peroxidase to bind to the free WNV antigen. The substrate (tetra methyl benzidine, TMB) was then added after a washing step. The result was considered positive when the reading was at least 40% or higher than the inhibition percentage. According to the manufacturer’s data, this assay has 100% sensitivity in equine and birds. The assay also showed 98.8% specificity in birds and 96% specificity in horses. For further information see the discussion below.
Detection of WNV antibodies in sera from human samples was done using the Dx Select kit (Focus Diagnostics, Cypress, California, USA). Serum samples were diluted 100-fold with the provided dilution buffer. 100 microliters of this diluted sample was added to the wells of 96-well plate and incubated for 1 hr at room temperature. After 3 washing steps a goat antihuman IgG antibody conjugated to the peroxidase enzyme was added and incubated for 30 min. The 96-well plate was then washed three times and the substrate was added. The change in color was read at 450 nm after 10 min. According to the manufacturer’s information, the clinical sensitivity of this assay is 97.3%, while its agreement with CDC IgG ELISA samples is 100% for the positive samples and 99% for the negative samples. For further information see the discussion below.
Study Ethics
The study was approved by the ethical committee of the Institutional Review Board at Imam Abdulrahman Bin Faisal University (Approval number: IRB-2014‐ 04-268).
Informed consent to participate in the study was obtained from all human participants.
This study was conducted in accordance with the Declaration of Helsinki. Horses and pigeons were treated with the best veterinary care and protocols.
Statistical Analysis
The data were tabulated in the Excel spread sheets and frequencies were calculated. The calculation of the P value was done using the OpenEpi website. A P value of less than 0.05 was considered statistically significant.
Results
In total 323 human samples were included in the study (37.2% females and 62.8% males). The average age of the participants was 45.1 years (range 18–81 years). The percentage of the anti-WNV IgG antibodies found in the human population was 9.6% (3.1% females and 6.5% males) (Table 1). There was no statistically significant difference in the frequency of antibody detection between males and females (P value 0.56, OR 0.78, 95% CI 0.34–1.72).
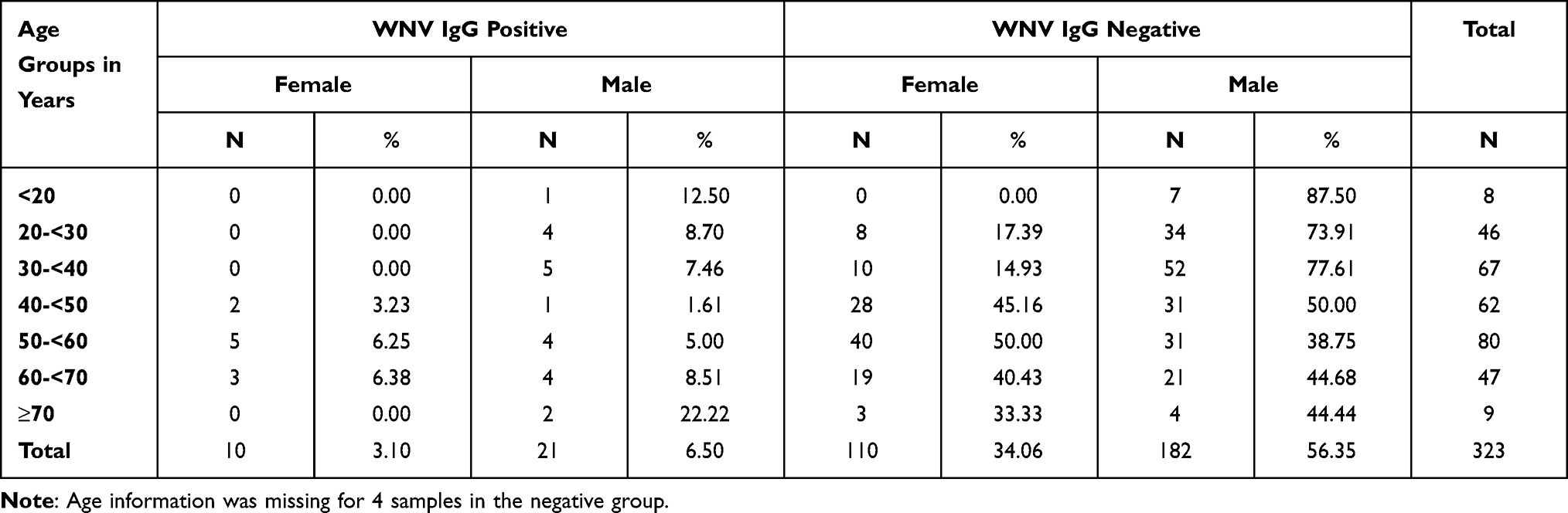 |
Table 1 Frequency of WNV IgG Antibodies Among Human Samples Based on Gender and Age Groups |
Additionally, 147 horses were included in the study, of which 101 (68.7%) horses were from Al-Qatif region and 46 (31.3%) horses were from Al-Ahsa region (Table 2). The prevalence of anti-WNV antibodies among horses in general was found to be 71.4% (105/147). There was no statistically significant difference in the WNV IgG antibody prevalence among horses from the two regions, Al-Ahsa (73.9%) and Al-Qatif (70.3%) (P value 0.665, OR 0.83, 95% CI 0.37–1.82). The prevalence of anti-WNV antibodies was significantly higher (84%, 42/50) among female when compared with the male horses (64.9%, 63/97) (P value 0.015, OR 2.8, 95% CI 1.2–7.1) in general. Additionally, the difference in prevalence between male and female horses was statistically significant in horses from Al-Qatif region (P value 0.025, OR 3.5, 95% CI 1.15–12.89) but not in horses from Al-Ahsa region (P value 0.346, OR 0.5, 95% CI 0.11–2.02). Table 2 shows the frequency of WNV IgG antibodies among horses from the two areas according to age and gender.
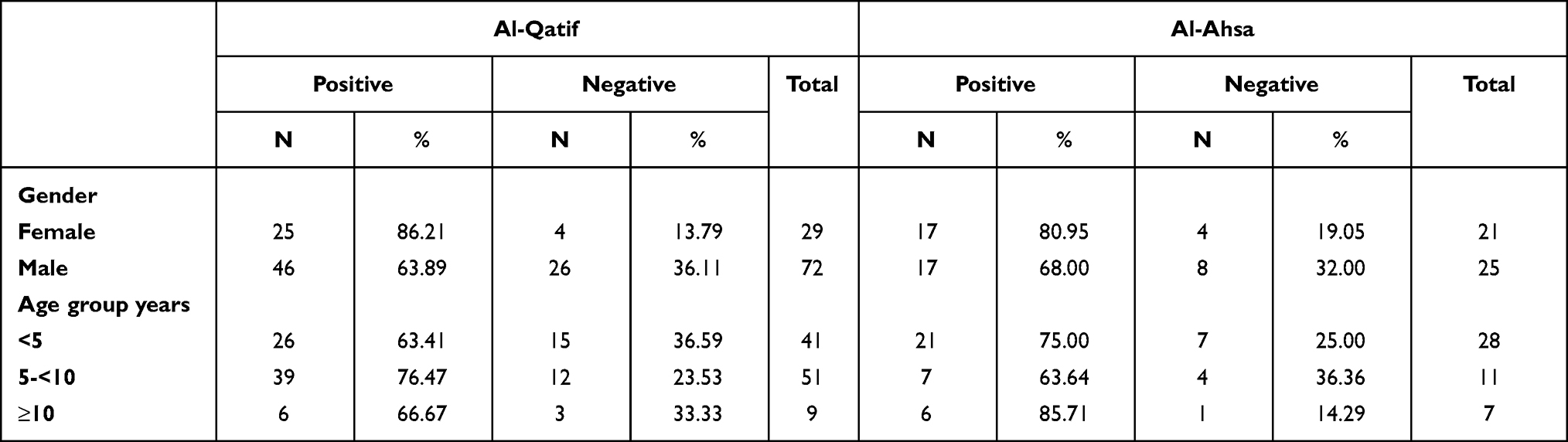 |
Table 2 Frequency of WNV IgG Antibodies Among Horse Samples from Two Areas |
The average age of horses included in the study was 5.68 years (range 1–23 years). 72.7% of the horses already had detectable anti-WNV antibodies by age of 1 year. There was no statistically significant trend in the prevalence of WNV antibodies with different age groups neither from Al-Qatif region (P value 0.491) nor from Al-Ahsa region (P value 0.992) (Table 2).
In total, 53.19% (150/282) of the pigeons included in the study had anti-WNV antibodies.
Discussion
Data on the prevalence of WNV in Saudi Arabia are limited. To the best of our knowledge, this is the first study conducted for the detection of WNV antibodies in humans and pigeons from Saudi Arabia. High frequency of WNV antibodies in the horses from Saudi Arabia observed in our study is in coherence with two other previously published studies.10,13 A survey study conducted on mosquitoes in 2010 found that the mosquitoes of Culex spp, WNV vector, were the most abundant mosquito species in the Eastern Province of Saudi Arabia, constituting more than 66% of all the captured mosquitoes in the region.15 The detection of Culex spp was also reported from other regions of Saudi Arabia.16–19 The abundant presence of the vector and the presence of antibodies in the pigeons, the amplifying vector, and the incidental hosts, humans and horses, indicate that WNV may be endemic in Saudi Arabia.
About 10% of the human population in this study had anti-WNV antibodies indicating a previous exposure to the virus. This finding was similar to a previously reported data on the seroprevalence in the population of Qatar (10.4%), a neighbor country to Saudi Arabia.11 No data is available about seroprevalence of WNV in humans from other neighboring Gulf countries in the Arabian Peninsula. A study from UAE reported no detection of WNV RNA in the blood donors in 2008.20 Since the first outbreak in USA in 1999, WNV has become the most common cause of mosquito-borne virus infections in the USA and the leading cause of viral encephalitis.9,21 During the last two decades, WNV has become a leading infectious cause of human neuroinvasive disease.4 This emphasizes that attention should be paid to diagnose and report such cases from Saudi Arabia.
WNV was previously classified in the Japanese encephalitis antigenic complex together with other flaviviruses including Murray Valley encephalitis, Saint Louis encephalitis, Usutu, and other viruses.22 Therefore, a cross reaction may occur due to a recent infection or vaccination with either of these viruses. No vaccine is available for these viruses in humans and none of these viruses were reported to be circulating in the region. An infection with dengue virus was also reported to cause cross reaction with WNV antibody detection.23 Dengue virus is endemic only in the Western Province of Saudi Arabia, which is located about 1200 km away from the Eastern Province.24 There are no reports of dengue fever virus in the Eastern Province. Nonetheless, our results might still be overestimating the seroprevalence of WNV among human population in Saudi Arabia. Multiple studies used the plaque reduction neutralization test (PRNT) as a confirmatory test for the detection of WNV antibodies. However, even PRNT was shown to lack the specificity particularly with the repeated flavivirus exposure.25 Therefore, and with the increasing reports of WNV infections worldwide, there is an urgent need for highly sensitive and specific assays to study the WNV prevalence in the population.
We reported equivalently high prevalence of WNV antibodies in horses from the two-study regions. Two previously published studies on the seroprevalence of WNV in the horses from Saudi Arabia have also reported high seroprevalence of the virus in the horses. The first was published in 2014 including 63 horses from Al-Ahsa region and found that 33.3% of horses have WNV antibodies by ELISA.10 Another study included 200 horse serum samples collected between 2013 and 2015 and employed ELISA followed by microneutralization assay for the positive samples, found that the seroprevalence of WNV from Al-Ahsa and Al-Qatif region was 51% and 55%, respectively.13 The same study also found that the prevalence of WNV antibodies from Al-Jubail, another region in the Eastern Province of Saudi Arabia, was 60% while it was lower in the central regions such as Qassim and Riyadh.13 These reports might indicate an increasing tendency of WNV seroprevalence in the country over time. No WNV virus vaccination is implemented in Saudi Arabia, which precludes the possibility of acquiring the antibodies from the vaccination. We noticed that 72.7% of the horses already had detectable anti-WNV antibodies by age of 1 year supporting the idea of high virus circulation rate in the region based on the serological evidence. Multiple WNV vaccines are available for veterinary use and this high seroprevalence of WNV in the horses suggest that these vaccines should be considered in Saudi Arabia for animal vaccination.
As mentioned above, there is cross antigenicity between members of the Flavivirus genus. Despite the high sensitivity and specificity of ELISA, particularly the one we used (see below), the virus neutralization assay (PRNT or microneutralization assay) has the advantage of targeting multiple viral antigens at the same time. Hemida et al compared the seroprevalence of WNV antibodies in horses using ELISA and microneutralization assay.13 They found that the WNV seroprevalence in regions from the Eastern Province ranged between 45.5% and 80% using ELISA and between 30.4% and 60% using microneutralization assay.13 In some regions, the microneutralization assay gave a higher seroprevalence than ELISA, most probably due to its ability to detect other antigens than these antigens targeted by ELISA.13 However, the detection of high seroprevalence level of WNV antibodies even with microneutralization assay in their study supports the fact that our data reflects a true presence of WNV in the tested population of humans, horses and pigeons.
More than 50% of the tested pigeons had WNV antibodies in our study. We used the blocking ELISA assay technique to test for WNV antibodies in horses and birds. According to the manufacturer’s data, the assay has 100% sensitivity in equine and birds. The assay also showed 98.8% specificity in birds and 96% specificity in horses. The Blocking ELISA assay seems to be more specific than the competition ELISA kit in proficiency testing in terms of cross reaction with tick-borne encephalitis virus (manufacturer’s brochure). It was suggested that infection of birds with Usutu virus produces antibodies that may cause cross reaction with WNV antibody detection in the ELISA-based assays.26 However, this seems to be minimal in the employed blocking ELISA technique (manufacturer’s brochure).
Apparently, further studies are needed to confirm the prevalence of WNV in humans and animals including cases with clinical manifestation. Furthermore, virus isolation from pigeons and mosquitoes and its genotyping should be included in the future studies.
In conclusion, our study provided the first evidence of WNV antibody detection in humans and pigeons and showed that there is high seroprevalence of the virus in horses. This data indicates that WNV is endemic in Saudi Arabia. More attention should be given to the diagnosis and reporting of WNV infections in humans and animals to measure the clinical burden of the virus. Additionally, implementation of WNV vaccine in horses would massively decrease the morbidity. More importantly, monitoring virus circulation in the environment by designing a surveillance program is required as has already been established in several countries. The cross immunity produced between several flaviviruses is of some limitation to our approach due to live virus importation restrictions to the country and should be investigated in humans and birds as already previously done in horses from the same region.13
Study Statement
The study was approved by the ethical committee of the Institutional Review Board at Imam Abdulrahman Bin Faisal University (Approval number: IRB-2014‐ 04-268).
Informed consent to participate in the study was obtained from human participants.
Acknowledgments
The authors would like to thank Mr. Nestor Recella and Mrs. Janaica Yu Logan for their technical help. The authors are grateful for Dr. Abdullah Alobeid for providing the Map of Saudi Arabia. This project was funded by the Deanship of Research at Imam Abdulrahman Bin Faisal University [Project number: 2014336].
Funding
This project was funded by the Deanship of Research at Imam Abdulrahman Bin Faisal University [Project number: 2014336].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Habarugira G, Suen WW, Hobson-Peters J, Hall RA, Bielefeldt-Ohmann H. West Nile virus: an update on pathobiology, epidemiology, diagnostics, control and “One health” implications. Pathogens. 2020;9(7):589. doi:10.3390/pathogens9070589
2. Taieb L, Ludwig A, Ogden NH, et al. Bird species involved in West Nile virus epidemiological cycle in Southern Quebec. Int J Environ Res Public Health. 2020;17(12):4517. doi:10.3390/ijerph17124517
3. Colpitts TM, Conway MJ, Montgomery RR, Fikrig E. West Nile virus: biology, transmission, and human infection. Clin Microbiol Rev. 2012;25(4):635–648. doi:10.1128/CMR.00045-12
4. Fiacre L, Pages N, Albina E, Richardson J, Lecollinet S, Gonzalez G. Molecular determinants of West Nile virus virulence and pathogenesis in vertebrate and invertebrate hosts. Int J Mol Sci. 2020;21(23):9117. doi:10.3390/ijms21239117
5. Petersen LR, Brault AC, Nasci RS. West Nile virus: review of the literature. JAMA. 2013;310(3):308–315. doi:10.1001/jama.2013.8042
6. Byas AD, Ebel GD. Comparative pathology of West Nile virus in humans and non-human animals. Pathogens. 2020;9(1):48. doi:10.3390/pathogens9010048
7. Reisen WK. Ecology of West Nile virus in North America. Viruses. 2013;5(9):2079–2105. doi:10.3390/v5092079
8. Camp JV, Nowotny N. The knowns and unknowns of West Nile virus in Europe: what did we learn from the 2018 outbreak? Expert Rev Anti Infect Ther. 2020;18(2):145–154. doi:10.1080/14787210.2020.1713751
9. Hadfield J, Brito AF, Swetnam DM, et al. Twenty years of West Nile virus spread and evolution in the Americas visualized by nextstrain. PLoS Pathog. 2019;15(10):e1008042. doi:10.1371/journal.ppat.1008042
10. Al-Ghamdi GM. Incidence of West Nile virus in Al-Ahsa, Saudi Arabia. Int J Virol. 2014;10(2):163–167. doi:10.3923/ijv.2014.163.167
11. Dargham SR, Al-Sadeq DW, Yassine HM, et al. Seroprevalence of West Nile virus among healthy blood donors from different national populations residing in Qatar. Int J Infect Dis. 2021;103:502–506. doi:10.1016/j.ijid.2020.11.175
12. Eybpoosh S, Fazlalipour M, Baniasadi V, et al. Epidemiology of West Nile virus in the Eastern Mediterranean region: a systematic review. PLoS Negl Trop Dis. 2019;13(1):e0007081. doi:10.1371/journal.pntd.0007081
13. Hemida MG, Perera R, Chu DKW, Ko RLW, Alnaeem AA, Peiris M. West Nile virus infection in horses in Saudi Arabia (in 2013–2015). Zoonoses Public Health. 2019;66(2):248–253. doi:10.1111/zph.12532
14. GASTAT. General Authority of Statistics. Population Characteristics Surveys, Saudi Arabia; 2017:1–51
15. Alahmed AM. Mosquito fauna (Diptera: culicidae) of the Eastern Region of Saudi Arabia and their seasonal abundance. J King Saud Univ Sci. 2012;24:55–62. doi:10.1016/j.jksus.2010.12.001
16. Al-Ali KH, Ayman A EB, Eassa AHA, Al-Juhani AM, Al-Zubiany SF, Ibrahim E-KD. A study on culex species and culex transmitted diseases in Al-Madinah Al-Munawarah, Saudi Arabia. Parasitol United J. 2008;1(2):101–108.
17. Alahmed AM, Al Kuriji MA, Kheir SM, Alahmedi SA, Al Hatabbi MJ, Al Gashmari MA. Mosquito fauna (Diptera: culicidae) and seasonal activity in Makka Al Mukarramah Region, Saudi Arabia. J Egypt Soc Parasitol. 2009;39(3):991–1013.
18. Kheir SM, Alahmed AM, Al Kuriji MA, Al Zubyani SF. Distribution and seasonal activity of mosquitoes in al Madinah Al Munwwrah, Saudi Arabia. J Egypt Soc Parasitol. 2010;40(1):215–227.
19. Alahmed AM, Munawar K, Khalil SMS, Harbach RE. Assessment and an updated list of the mosquitoes of Saudi Arabia. Parasit Vectors. 2019;12(1):356. doi:10.1186/s13071-019-3579-4
20. Alfaresi M, Elkoush A. West Nile virus in the blood donors in UAE. Indian J Med Microbiol. 2008;26(1):92–93. doi:10.4103/0255-0857.38875
21. Centers for Disease C, Prevention. Outbreak of West Nile-like viral encephalitis–New York, 1999. MMWR Morb Mortal Wkly Rep. 1999;48(38):845–849.
22. Calisher CH, Karabatsos N, Dalrymple JM, et al. Antigenic relationships between flaviviruses as determined by cross-neutralization tests with polyclonal antisera. J Gen Virol. 1989;70(Pt 1):37–43. doi:10.1099/0022-1317-70-1-37
23. Papa A, Karabaxoglou D, Kansouzidou A. Acute West Nile virus neuroinvasive infections: cross-reactivity with dengue virus and tick-borne encephalitis virus. J Med Virol. 2011;83(10):1861–1865. doi:10.1002/jmv.22180
24. Ashshi AM. The prevalence of dengue virus serotypes in asymptomatic blood donors reveals the emergence of serotype 4 in Saudi Arabia. Virol J. 2017;14(1):107. doi:10.1186/s12985-017-0768-7
25. Ledermann JP, Lorono-Pino MA, Ellis C, et al. Evaluation of widely used diagnostic tests to detect West Nile virus infections in horses previously infected with St. Louis encephalitis virus or dengue virus type 2. Clin Vaccine Immunol. 2011;18(4):580–587. doi:10.1128/CVI.00201-10
26. Lim SM, Geervliet M, Verhagen JH, et al. Serologic evidence of West Nile virus and Usutu virus infections in Eurasian coots in the Netherlands. Zoonoses Public Health. 2018;65(1):96–102. doi:10.1111/zph.12375
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.