")
Back to Journals » Infection and Drug Resistance » Volume 12
Serological evidence of Coxiella burnetii infection in cattle and farm workers: is Q fever an underreported zoonotic disease in Ecuador?
Authors Echeverría G, Reyna-Bello A, Minda-Aluisa E , Celi-Erazo M, Olmedo L , García HA , Garcia-Bereguiain MA , de Waard JH
Received 26 November 2018
Accepted for publication 7 February 2019
Published 9 April 2019 Volume 2019:12 Pages 701—706
DOI https://doi.org/10.2147/IDR.S195940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Gustavo Echeverría,1,2 Armando Reyna-Bello,3 Elizabeth Minda-Aluisa,1 Maritza Celi-Erazo,1 Lisbeth Olmedo,1 Herakles A García,4 Miguel Angel Garcia-Bereguiain,5–7 Jacobus H de Waard,5,8 On behalf of the UNU/BIOLAC network for infectious cattle diseases
1Instituto de Investigación en Salud Publica y Zoonosis (CIZ), Universidad Central del Ecuador, Quito, Ecuador; 2Facultad de Ciencias Veterinarias, Programa de Doctorado, Universidad de Buenos Aires, Buenos Aires, Argentina; 3Departamento de Ciencias de la Vida y la Agricultura, Carrera de Ingeniería en Biotecnología, Universidad de las Fuerzas Armadas ESPE, Santo Domingo, Ecuador; 4Departamento de Parasitologia, Instituto de Ciências Biomédicas, University of São Paulo, São Paulo, Brazil; 5One Health Research Group. Facultad de Ciencias de la Salud, Universidad de Las Américas (UDLA), Quito, Ecuador; 6School of Biological Sciences and Engineering, Yachay Tech, Urcuquí, Ecuador; 7Laboratorio para Investigaciones Biomedicas. Facultad de Ciencias de la Vida, Escuela Superior Politécnica del Litoral, Guayaquil, Ecuador; 8Instituto de Biomedicina Dr. Jacinto Convit, Universidad Central de Venezuela, Caracas, Venezuela
Background: Q fever is an underreported zoonotic disease of cattle and men in most countries of the world. Very little information about the prevalence of Coxiella burnetii infection in animals and humans comes from South and Central America and systematic studies are lacking.
Methods: A seroprevalence survey for Q fever amongst cattle, farm workers and students was conducted in Ecuador using a commercial ELISA kit.
Results: Survey results showed an unexpectedly high prevalence of Coxiella burnetii antibodies in dairy cattle (43%) and in farm workers (34%). In addition, a clinical case in a human of acute Q fever in the convalescent stage was detected.
Conclusion: We conclude that the disease is endemic in Ecuador but is overlooked by medical and laboratory personnel. Q fever should be considered a public health issue in Ecuador and further research into the clinical relevance of this infection is recommended.
Keywords: Q fever, Coxiella burnetii, Ecuador, phase I antibodies, phase II antibodies
Introduction
Q fever caused by Coxiella burnetii is a zoonotic worldwide-distributed infectious disease. Cattle, sheep, and goats are the main reservoirs for the bacterium. Transmission of C. burnetii from animal to animal, or from animal to human, most frequently occurs via inhalation of dust or droplets that contain the microorganisms.1 The importance of ticks in transmission remains controversial, even though many studies have shown that ticks species can carry C. burnetii.2,3 No human to human transmission of C. burnetti has been reported.4
The World Organization for Animal Health (OIE) lists Q fever as notifiable animal disease and the member countries of this organization are encouraged to report the incidence of the disease in livestock.5 In cattle, C. burnetii infection is generally asymptomatic but the infection can result in late stage abortion, stillbirths or delivery of weak offspring.6 Nevertheless, Q fever is not considered to cause significant economic losses and consequently very little effort are made to control this infection.
C. burnetii infection in cattle has been described for most countries, with New Zealand remaining an exception and the prevalence is highly variable from one country to another. For example, a herd and individual prevalence for C. burnetii antibody of 41% and 13%, respectively, has been reported in Iran.7 A seroprevalence of less than 13% has been reported for cattle from most countries of Africa, with some exception in Western and Middle Africa where seroprevalence up to 18–55% has been reported.8 Several studies in cattle from the USA have shown a relatively low average seroprevalence of 3.4%.9
Few reports concerning this bacterial zoonotic infection come from South and Central America, and systematic studies from this continent are lacking.10 Countries in South America with an considerable cattle population like Argentina, Uruguay, Brazil, and Colombia have no studies published in the English language when searched for in PubMed (January 2019) with the search terms “Q fever, cattle” and the country name. The only study for Central America comes from the State of Nuevo León in Mexico, where apparently 28% of the exanimated dairy cattle and 10% of the beef cattle were diagnosed as seropositive for Q fever infection.11
Concerning Q fever in humans, current epidemiological studies indicate that this zoonosis should be considered a public health problem in many countries, including France, the United Kingdom, Italy, Spain, Germany, Israel, Greece, and Canada, as well as in many countries where Q fever is prevalent but unrecognized because of poor surveillance of the disease.12 However, a lack of surveillance and diagnostics for Q fever limits our knowledge of the true prevalence of this disease in humans, leading to underdiagnosis and consequently mismanagement of cases by the medical physicians. In humans, C. burnetti infection causes highly variable diseases ranging from acute (often self-limited) infection to fatal chronic infection. The most frequent clinical manifestation of acute Q fever is a flu-like and self-limited illness with high and prolonged fever, severe headache, coughing and atypical pneumonia and hepatitis.1,4,10,12 Chronic Q fever occurs in less than 5% of the infected patients and may occur several months or years after the onset of the acute infection.1,4,10,12 Chronic Q fever is accompanied by symptoms such as endocarditis, vasculitis, prosthetic joint arthritis, persistent fatigue and lymphadenitis. Endocarditis and vascular infections caused by Q fever are fatal if untreated.13 The Q fever seroprevalence in humans varies amongst countries and risk groups. Q fever is an occupational hazard for those who live and work in rural settings and those who are in contact with animals. For people working in high-risk occupations such as farmers, veterinarians and abattoir workers the seroprevalence of C. burnetii infection can range from 30% to 70%.14 A recent meta-analysis reports a seroprevalence rate ranging from 4.7% to 91.7% amongst abattoir and slaughterhouse workers.15
In November 2017, we organized a workshop for the diagnosis of infectious cattle diseases, with the participation of 22 veterinarians from 11 countries from Latin America. This course was financed through the United Nations University Program for Biotechnology in Latin America and the Caribbean (UNU/BIOLAC) program.16 During this course, we investigated the health status of four dairy cattle herds searching for zoonotic and production affecting bacterial, viral and parasitic infections including Q fever. The present study aims to document the prevalence of Q fever in this setting and investigates the proportion of cattle, farm workers, and veterinary staff with evidence of exposure or infection to this zoonosis.
Material and methods
Cattle
Four dairy cattle farms from owners who agreed with the study were selected at random. Two dairy cattle farms were located near Quito in a mountainous Andes region (≈3,000 meters above sea level) and two near Santo Domingo de los Tsachilas, in a tropical region in Ecuador (≈300–600 meters above sea level). All dairy farms had over 300 cows. Blood samples of 352 cows were taken by a veterinary from the tail vein in tubes without additives, and transported the same day on ice to the laboratory and processed. After coagulation of the blood, the tubes were centrifuged (2.000 g for 5 mins), and the serum was harvested and stored for a maximum of 3 days at 4 °C before used in the Q fever-ELISA.
Human subjects
Thirty-two cattle farm workers and 22 course participants coming from 11 different countries, all veterinarians, were asked to collaborate and firmed an informed consent before blood was drawn from the right forearm, by a trained professional. Blood was processed in the same way as the cattle blood.
Serology of Q fever
For the diagnosis of Q fever, an indirect multi-species ELISA for the detection of one or both anti-Coxiella burnetii phase I and phase II IgG antibodies in serum was used (ID.vet, Innovative Diagnostics, Grabels, France). According to data provided by the manufacturer this ELISA has a sensitivity of 100% (CI 95%: 89.28–100%) and a specificity of 100% (CI 95%: 97.75–100%). The ELISA was performed according to the manufacturer’s instructions and the manufacturer’s guidelines for the interpretation of results were followed.
Statistical analysis
We performed a Chi-square test and a Fisher’s exact test analysis to compare the prevalence data of Coxiella burnetii infection. In addition, we calculate 95% confidence intervals (CIs). The statistical significance was set at p<0.05. The data were analyzed using SPSS Version 22.0 for Windows.
Interviews
Cattle workers and participants, seropositive for Q fever, were interviewed and asked if they had experienced the typical symptoms and signs of acute Q fever after having contact with an aborted fetus: flu-like symptoms, lower respiratory tract symptoms, pneumonia and fever, or hepatitis-like symptoms. Chronic Q fever in the seropositive subjects was accessed using the Nijmegen Clinical Screening Instrument (NCSI), a questionnaire to measure the health status of the subject.17 This questionnaire consists of three main domains of functional impairment, symptoms and Quality of Life, divided into eight sub-domains assessing symptoms and signs as fatigue, functional impairment, Health-Related Quality of Life and Satisfaction Relations
Ethical considerations
Permission for the study and ethical approval involving human subjects was obtained from the Ethical Committee of the Universidad San Francisco de Quito. The participant consent was a written signed informed consent, and the study was conducted in accordance with the Declaration of Helsinki. Cattle owners gave a written permission for the diagnostic blood testing of the cattle and all blood drawing was done by veterinarians and free of cost to cattle owners.
Conflicts of interest statement
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Results
Serological testing of cattle and men
Serum samples were obtained from 352 bovines, about 90 serum samples of each farm that participated in the study. See Table 1. One hundred fifty-one serum samples (151 or 42,9%) tested seropositive for C. burnetii antibodies with no significant difference in prevalence amongst the four cattle farms. (Chi-square analysis, p=0,593). Thirty-two cattle farm worker working on three of the four dairy farms visited in this study were tested for the presence of antibodies against Q fever and eleven (34%) were seropositive with no significant difference in seropositivity amongst the three cattle farms. (Chi-square analysis, p=0.340). The 22 course participants of the BIOLAC course were tested and 2/22 (19%) resulted seropositive. Both were participants from Ecuador. No participants of the other countries resulted seropositive. The results of ELISA test are summarized in Table 1.
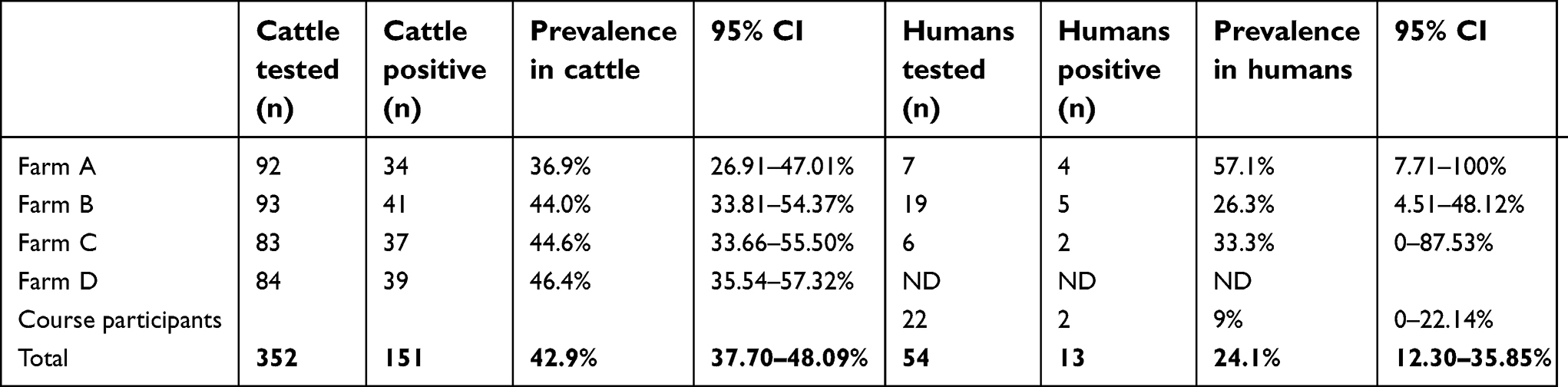 | Table 1 Prevalence with a 95% confidence interval of Q fever infection in cattle and cattle workers on four cattle farms and the participants of the UNU/BIOLAC course. ND in this table means “not determined”. |
Interviews
Interrogation of the eleven seropositive farmer workers and the two Ecuadorian course participants revealed no acute Q fever cases but one of the seropositive veterinarians reported contact with animal abortive material approximately a year before without using special protection or precaution and subsequently a weeklong hospitalization with an atypical pneumonia approximately 3 weeks after this contact. The interviews with the other seropositive subjects did not reveal any symptoms of chronic Q fever such as long-lasting health effects like persistent fatigue, lethargy, depression or incoordination. No further testing of the seropositive subjects for the presence of phase I and phase II antibodies was undertaken because of the lack of serodiagnostic methods for Q fever in Ecuador (see also the discussion).
Discussion
The present study demonstrates the importance of C. burnetii infection amongst cattle and humans, specially in cattle workers in Ecuador and a relatively high seropositivity was found. This is not the first report concerning Q fever in Ecuador and there are two more reports. One report is a study from 2004 with acute undifferentiated febrile illness human patients from the Ecuadorean Amazon basin. Almost 5% of these patients were seropositive for Q fever.18 The origin of the infection with C. burnetti in these febrile patients is unknown as no extensive sheep, goats and cattle are raised in the location of the study. This surveillance study shows a clear need for improvement of our knowledge of the Q fever epidemiology as in this region of Ecuador other wildlife or tick reservoirs could be implicated.2,3 The second publication dates from 2015 and reports a prevalence of C. burnetii seropositivity in dairy and mixed cattle of 12.6% (CI 95%: 11.3–13.9%) with a herd prevalence of 46.9%.19 The present report is the first report that detects the presence of antibodies against C. burnetii in a particular epidemiological setting, cattle, cattle workers and veterinaries, suggesting a possible transmission from cattle to cattle workers.
Concerning a follow-up on the seropositivity in farm workers, we did not determine the presence of antibodies IgG and IgM against the phase I and phase II to define if the infection in our patients is acute or chronic.4 ELISA methods for this determination are not registered and legalized in Ecuador and for this reason are not commercialized. Moreover, a consultation with the main public and private clinical laboratories for human and animal health in Ecuador, in Quito and Guayaquil, disclosed that there are no laboratories in the country diagnosing Q fever in humans or in animals (personal communication to JHdW) and that most of the consulted laboratories were unaware of the disease or its presence in Ecuador. Additionally, interviews conducted with the 22 participants of the course (veterinarians), showed that 95% of the course participants, all veterinaries, was unacquainted with the disease.
Our findings also call for further investigation into the clinical relevance of chronic Q fever in Ecuador. Knowledge about chronic Q fever is limited, but the studies that have been conducted showed that about 5% of the patients who got infected with C. burnetii would develop chronic Q fever. Additional serological and clinical monitoring is recommended for the patients detected in this study to determine if they have high IgG phase I antibody titers, as these patients have been shown to have the highest risk to progress to chronic Q fever.23
Conclusion
We conclude that Q fever is endemic in Ecuador but that reporting only has been done in research studies. More research is necessary in Ecuador to set the human risk groups, to diagnose acute and chronic Q fever and to determine the economic impact of Q fever in the cattle industry. Concerning acute Q fever, we propose the physicians in Ecuador to request testing for acute Q fever in cases of atypical pneumonia in risk groups like cattle farm workers, veterinaries and slaughterhouse workers. C. burnetii is not susceptible to the antimicrobial therapy generally used in the empirical management of febrile patients in resource-poor settings. The antibiotic choice for the treatment of C. burnetii as the etiologic agent of community acquired pneumoniae (CAP) includes doxycycline20 and differentiating acute Q fever from other respiratory infections is not possible without serologic testing.21 We also consider that Ecuador is not ready for an outbreak of acute Q fever as recently has happened in dairy workers in Chile, with 59 suspect cases and 3 confirmed cases in August 2017, of which 82% were livestock workers.22 While there have been no reports of deaths in this Chile outbreak, 18 patients required hospitalization for pneumonia and three of them were connected to mechanical ventilation. The final diagnosis of the acute Q fever cases in Chile was done in the USA, as no diagnostic capacity was present at that time in this country.
Limitations of the study
A limitation of our study is that farms were selected by convenience sampling and therefore are neither representative of the entire cattle population nor the entire farm workers population in Ecuador. Another limitation is the possibility that the seropositive individuals in this study have developed chronic Q fever without being identified with the questionnaire. An objective and precise diagnosis of long-term health effects of Q fever is difficult and serological testing for Phase I and Phase II antibodies can help to better classify the patients. However, this has not been done in our study because the diagnostic kits are not available in Ecuador.
Acknowledgments
The members of the UNU/BIOLAC Network for Infectious Cattle Diseases can be found on the webpage:
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Angelakis E, Raoult D. Q fever. Vet Microbiol. 2010;140(3–4):297–309. doi:10.1016/j.vetmic.2009.07.016
2. Duron O, Sidi-Boumedine K, Rousset E, Moutailler S, Jourdain E. The importance of ticks in Q fever transmission: what has (and has not) been demonstrated? Trends Parasitol. 2015;31(11):536–552. doi:10.1016/j.pt.2015.06.014
3. Varela-Castro L, Zuddas C, Ortega N, et al. On the possible role of ticks in the eco-epidemiology of Coxiella burnetii in a Mediterranean ecosystem. Ticks Tick Borne Dis. 2018;9(3):687–694. doi:10.1016/j.ttbdis.2018.02.014
4. Eldin C, Mélenotte C, Mediannikov O, et al. From Q fever to coxiella burnetii infection: a paradigm change. Clin Microbiol Rev. 2017;30(1):115–190. doi:10.1128/CMR.00045-16
5. OIE-Listed diseases, infections and infestations in force in 2018. Available from:
6. Agerholm JS. Coxiella burnetii associated reproductive disorders in domestic animals – a critical review. Acta Vet Scand. 2013;55:13. doi:10.1186/1751-0147-55-13
7. Mohabbati Mobarez A, Bagheri Amiri F, Esmaeili S. Seroprevalence of Q fever amongst human and animal in Iran; A systematic review and meta-analysis. PLoS Negl Trop Dis. 2017;11(4):e0005521. doi:10.1371/journal.pntd.0005521
8. Vanderburg S, Rubach MP, Halliday JE, Cleaveland S, Reddy EA, Crump JA. Epidemiology of Coxiella burnetii infection in Africa: a OneHealth systematic review. PLoS Negl Trop Dis. 2014;8(4):e2787. doi:10.1371/journal.pntd.0002787
9. McQuiston JH, Childs JE. Q fever in humans and animals in the United States. Vector Borne Zoonotic Dis. 2002;2(3):179–191. doi:10.1089/15303660260613747
10. Epelboin L, Nacher M, Mahamat A, et al. Q fever in French Guiana: tip of the iceberg or epidemiological exception? PLoS Negl Trop Dis. 2016;10(5):e0004598. doi:10.1371/journal.pntd.0004598
11. Salinas-Meléndez JA, Avalos-Ramírez R, Riojas-Valdez V, Kawas-Garza J, Fimbres-Durazo H, Hernández-Vidal G. Serologic survey in animals of ‘Q’ fever in Nuevo Leon. Rev Latinoam Microbiol. 2002;44(2):75–78.
12. Maurin M, Raoult D. Q fever. Clin Microbiol Rev. 1999;12(4):518–553. Review.
13. Wegdam-Blans MC, Vainas T, van Sambeek MR, et al. Vascular complications of Q-fever infections. Eur J Vasc Endovasc Surg. 2011;42(3):384–392. doi:10.1016/j.ejvs.2011.04.013
14. Aitken ID, Bögel K, Cračea E, et al. Q fever in Europe: current aspects of aetiology, epidemiology, human infection, diagnosis and therapy. Infection. 1987;15(5):323–327. doi:10.1007/BF01647731
15. Woldeyohannes SM, Gilks CF, Baker P, Perkins NR, Reid SA. Seroprevlance of Coxiella burnetii amongst abattoir and slaughterhouse workers: a meta-analysis. One Health. 2018;6:23–28. doi:10.1016/j.onehlt.2018.09.002
16. The United Nations University Biotechnology Programme for Latin America and the Caribbean (UNU-BIOLAC, Caracas, Venezuela). Available from:
17. Peters JB, Daudey L, Heijdra YF, Molema J, Dekhuijzen PN, Vercoulen JH. Development of a battery of instruments for detailed measurement of health status in patients with COPD in routine care: the Nijmegen Clinical Screening Instrument. Qual Life Res. 2009;18(7):901–912. doi:10.1007/s11136-009-9478-y
18. Manock SR, Jacobsen KH, de Bravo NB, et al. Etiology of acute undifferentiated febrile illness in the Amazon basin of Ecuador. Am J Trop Med Hyg. 2009;81(1):146–151.
19. Carbonero A, Guzmán LT, Montaño K, Torralbo A, Arenas-Montes A, Saa LR. Coxiella burnetii seroprevalence and associated risk factors in dairy and mixed cattle farms from Ecuador. Prev Vet Med. 2015;118(4):427–435. doi:10.1016/j.prevetmed.2015.01.007
20. Kersh GJ. Antimicrobial therapies for Q fever. Expert Rev Anti Infect Ther. 2014;11(11):1207–1214. doi:10.1586/14787210.2013.840534
21. Keijmel SP, Krijger E, Delsing CE, Sprong T, Nabuurs-Franssen MH, Bleeker-Rovers CP. Differentiation of acute Q fever from other infections in patients presenting to hospitals, the Netherlands. Emerg Infect Dis. 2015;21(8):1348–1356. doi:10.3201/eid2108.140196
22.
23. Wielders CC, Boerman AW, Schimmer B, et al. Persistent high IgG phase I antibody levels against Coxiella burnetii among veterinarians compared to patients previously diagnosed with acute Q fever after three years of follow-up. PLoS One. 2015;10(1):e0116937. doi:10.1371/journal.pone.0116937
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.