")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Semaglutide 2.4 Mg for the Management of Overweight and Obesity: Systematic Literature Review and Meta-Analysis
Authors Smith I, Hardy E , Mitchell S, Batson S
Received 13 October 2022
Accepted for publication 1 December 2022
Published 17 December 2022 Volume 2022:15 Pages 3961—3987
DOI https://doi.org/10.2147/DMSO.S392952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Inger Smith,1 Emily Hardy,2 Stephen Mitchell,2 Sarah Batson2
1White Box Health Economics Ltd, Worthing, West Sussex, UK; 2Mtech Access, Bicester, Oxfordshire, UK
Correspondence: Sarah Batson, Mtech Access, 30 Murdock Road, Bicester, Oxfordshire, OX26 4PP, UK, Tel +44 1869 222 490, Email [email protected]
Purpose: Semaglutide has demonstrated safe and effective weight loss for overweight and obesity, including participants with concomitant type 2 diabetes mellitus (T2DM), in randomized placebo-controlled trials (RCTs). We conducted a systematic literature review (SLR) and network meta-analyses (NMA) to compare weekly semaglutide 2.4 mg with pharmacological comparators for weight management in overweight or obesity.
Methods: The SLR was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist. NMAs were performed to compare weight change for semaglutide 2.4 mg with comparators using data identified in the SLR. The populations of interest were total population, normal glucose tolerance, non-T2DM, pre-diabetes, and T2DM. Included outcomes were weight change from baseline (CFB, %) at 52 weeks and proportion of participants losing ≥ 5% baseline fasting body weight at 12 weeks (at full therapeutic dose).
Results: The SLR identified 108 RCTs examining non-surgical interventions, of which 41 were considered for inclusion in the NMAs. In all populations, semaglutide 2.4 mg was associated with a greater percentage weight CFB with 52 weeks of treatment versus all available comparators. In all populations, semaglutide was associated with a higher likelihood of participants losing ≥ 5% of baseline fasting body weight at 12 weeks versus all available comparators.
Conclusion: In NMA, semaglutide 2.4 mg demonstrated effective weight loss (≥ 5%) in the total population and all subpopulations of glucose tolerance versus active comparators. Semaglutide is an effective treatment that may address unmet need in the management of overweight and obesity.
Keywords: network meta-analysis, obesity, semaglutide, systematic literature review
Introduction
Obesity is a major global public health issue; the World Health Organisation estimated that in 2016 there were almost 2 billion adults worldwide with overweight and 650 million with obesity.1 Obesity is associated with the development of serious comorbidities, including type 2 diabetes mellitus (T2DM), cardiovascular disease, obstructive sleep apnea, and osteoarthritis.2–4
Lifestyle interventions, such as improved diet and increased physical activity, are the cornerstone of obesity management.5 However, lifestyle intervention alone may not be a durable management method for overweight and obesity as it does not appear to have a long-term impact on morbidity or mortality, as found in the Look AHEAD study.6,7 Pharmacological options for obesity include orlistat (lipase inhibitor), liraglutide (glucagon-like peptide 1 [GLP-1] agonist), naltrexone/bupropion (opioid antagonist/dual norepinephrine and dopamine reuptake inhibitor), and phentermine/topiramate (adrenergic agonist/gamma-aminobutyric acid receptor modulator). However, despite the substantial burden of obesity, pharmacological therapy has not been widely adopted as a management approach.8 This may be because these therapies only result in modest additional weight loss when used in conjunction with lifestyle intervention.8 In addition, there are safety concerns with some pharmacological weight loss therapies, such as phentermine/topiramate, that have led to negative opinions from regulatory agencies.9 Therefore, newer, more effective, and safer pharmacological interventions are needed to augment lifestyle interventions in overweight and obesity. Newer pharmacological interventions include tirzepatide (glucose-dependent insulinotropic polypeptide and GLP-1 agonist), which has demonstrated efficacy in people with T2DM in the SURPASS-2 trial,10 as well as sodium glucose cotransporter 2 (SGLT-2) inhibitors (eg, dapagliflozin, canagliflozin) that are used to manage T2DM but can also induce clinically significant weight loss.11
Another newer intervention is semaglutide, a long-acting GLP-1 analogue that mimics the effects of native GLP-1, which regulates appetite and blood sugar levels.12,13 Weight loss with semaglutide occurs through a reduction in energy intake, increased satiety and satiation, and reduced hunger, in conjunction with enhanced glycemic control; the latter occurs through semaglutide’s action on GLP-1, which stimulates insulin secretion and suppresses glucagon secretion when blood glucose levels are high.12–14 The safety and efficacy of semaglutide in overweight and obesity has been demonstrated in the Semaglutide Treatment Effect in People with obesity (STEP) clinical trial program. The STEP program (currently comprising STEP 1 to STEP 8) is a collection of Phase 3 trials of 2.4 mg semaglutide administered subcutaneously once weekly in conjunction with different intensities of lifestyle interventions. The STEP study participants have overweight or obesity, with or without T2DM. Compared with placebo, semaglutide 2.4 mg conferred a significantly greater reduction in body weight and a higher proportion of participants achieved ≥5% weight reduction in STEP 1 and STEP 2.12,15 Weight loss with semaglutide 2.4 mg was accompanied by greater improvements in cardiometabolic risk factors (eg, waist circumference, blood pressure, and lipid levels) and physical functioning than placebo.12,15 The most common adverse events with semaglutide were gastrointestinal (nausea, diarrhea) but these were generally mild-to-moderate and transient.12,15
Until the results of STEP 8 (weekly semaglutide 2.4 mg versus daily liraglutide 3.0 mg) were published in 2022,16 all randomized controlled trials (RCTs) in the STEP program have compared semaglutide with placebo; therefore, to compare semaglutide with other active comparators, indirect treatment comparison is required. The objective of this systematic literature review (SLR) and meta-analysis was to compare RCT evidence for weekly semaglutide 2.4 mg with that of relevant pharmacological comparators for weight management in people who have overweight or obesity. The outcomes of interest were weight change from baseline (CFB, %) at 52 weeks and proportion of participants losing ≥5% baseline fasting body weight at 12 weeks at full therapeutic dose (ie, as per the stopping rule for certain weight loss drugs, such as orlistat and liraglutide, when participants fail to achieve ≥5% baseline fasting body weight at 12 weeks at full therapeutic dose).
Materials and Methods
Systematic Literature Review
A systematic literature review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist.17
To identify RCTs reporting on semaglutide 2.4 mg and comparators (to include pharmacological agents, surgical intervention, and diet) in people with overweight or obesity, searches of Medline®, Medline® Epub Ahead of Print (In-Process & Other Non-Indexed Citations), Embase, and EBM Reviews were performed via Ovid on 8th September 2020. The search strategy used to interrogate the EMBASE database is provided in Supplementary Table 1. Additional searches of conference proceedings (from the last 3 years), health technology assessment (HTA) body websites, clinical trial registries (ClinicalTrials.gov and World Health Organization International Clinical Trials Registry Platform), and reference lists of included studies were performed to identify other relevant evidence. Eligibility criteria included RCTs, SLR, and meta-analysis publications reporting efficacy and safety data for semaglutide 2.4 mg and relevant comparators. Full eligibility criteria are presented in Table 1.
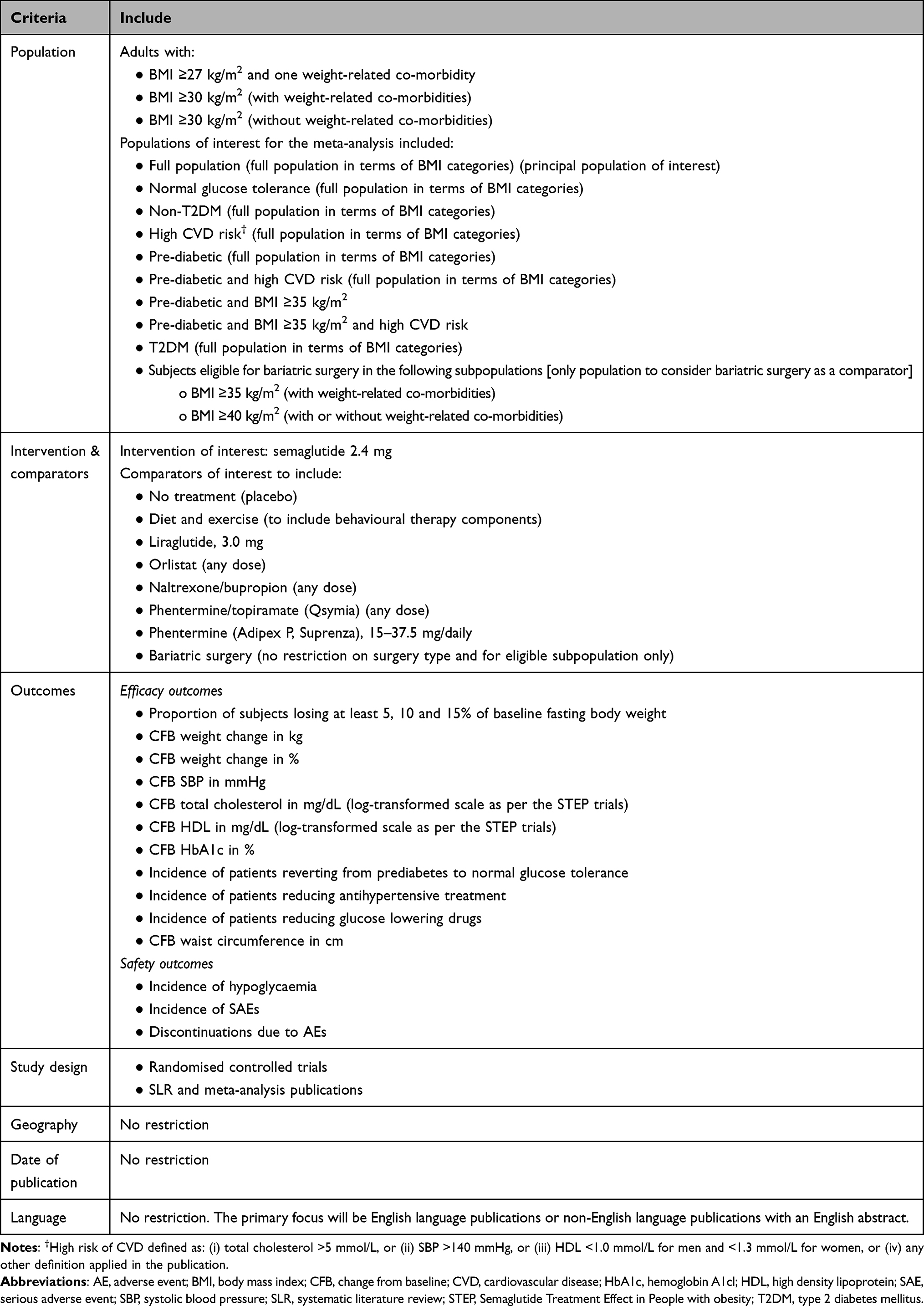 |
Table 1 Eligibility Criteria for the Systematic Literature Review |
Citations of interest were identified by a member of the team (authors EH or SM) and verified by an independent reviewer (authors SB or SM), based on title and abstract. Full publications were obtained for all citations of interest and were assessed by one reviewer and verified by a second reviewer. Any uncertainties were resolved through discussion. Data were extracted into an Excel spreadsheet by one reviewer and checked against the original publication by a second reviewer.
Quality Assessment
Quality (risk of bias) assessment of eligible RCTs was conducted using the criteria provided in the National Institute for Health and Care Excellence (NICE) single technology appraisal user guide.18 This approach is in line with guidance provided by the Centre for Reviews and Dissemination for assessing the quality of studies in SLRs.19
Network Meta-Analysis
A network meta-analysis (NMA) was performed to compare weight change for semaglutide 2.4 mg with comparators. Relevant data were analyzed from publications identified in the SLR (considering total trial population data or subgroup data). The populations of interest were total population, normal glucose tolerance (NGT), non-T2DM, pre-diabetes, and T2DM; separate NMA analyses were conducted for each of these populations.
The outcomes of interest were weight CFB (%) at 52 weeks and proportion of participants losing ≥5% baseline fasting body weight after 12 weeks at full therapeutic dose. The latter outcome included 16-week data for liraglutide, naltrexone/bupropion and phentermine/topiramate (4 weeks titration and 12 weeks at full dose), 12-week data for orlistat (no titration), and 28-week data for semaglutide (16 weeks titration and 12 weeks full dose).
Bayesian framework and Markov Chain Monte Carlo (MCMC) simulation were used for modelling, with the inclusion of vague prior distributions in line with guidance on evidence synthesis from the NICE Decision Support Unit.20–22 All NMA models were fitted using WinBUGS software (MRC Biostatistics Unit, Cambridge, UK); normal likelihood, identity link (CFB weight) and binomial, logit link (proportion of participants losing ≥5% baseline fasting body weight). The models were run with three chains for a burn-in of 50,000 iterations and inferences were based on a further 20,000 iterations. The point estimate of the results represented the median of the posterior distribution with associated 95% credible intervals (CrIs). As there are no closed loops of evidence within the current evidence base (other than loops of evidence comprised multi-arm trials) it was not necessary to assess inconsistency in the networks.
Both fixed effect (FE) and random effect (RE) models were conducted, and model fit compared in terms of deviance information criterion (DIC) and residual deviance; the model with the lowest DIC and residual deviance closest to the number of data points was selected as the model of choice.
Results
Systematic Literature Review
The electronic database searches identified a total of 13,287 publications. Following deduplication, 11,352 publications were screened by title and abstract. Of these, 318 articles were deemed potentially relevant and were screened based on the full publication. A further 112 publications were excluded at this stage. Handsearching yielded an additional seven citations, giving a total of 213 publications covering 130 unique studies for inclusion. The flow of studies through the review is summarized in the Preferred Reporting Items for Systematic Reviews and Meta-analysis flow diagram (PRISMA) in the Supplementary Figure 1.
Non-surgical interventions were of primary interest for the NMAs. The potential inclusion of bariatric surgery in the NMA was explored but was not deemed appropriate because the populations included in the bariatric surgery trials (comparing surgery with medical treatment or diet) were highly selective in comparison with the studies investigating pharmacological agents. For example, populations in the surgical RCTs had a higher mean body mass index (BMI), included participants with comorbidities, often required weight loss of ≥5% prior to enrolment, included small numbers of participants, and had issues associated with participant retention. These factors may have biased the trial results in favor of bariatric surgery. Of the trials included in the SLR, 108 RCTs (164 publications) investigated non-surgical interventions. Of these, 67 RCTs (115 publications) were not considered for the meta-analysis for the following reasons: trial duration <9 months (STEP trials reported outcome data at a minimum of 9 months’ follow-up and therefore a trial duration of <9 months did not align with the STEP program and the outcomes considered in the analyses); no appropriate comparator for inclusion in evidence network; no relevant data reported; and subpopulation not of interest. The remaining 41 RCTs (49 publications) were considered for the NMAs (Table 2). Table 3 shows the active comparators with available data for each outcome-specific network (placebo/control was the common comparator across all networks) and the evidence networks are presented in Supplementary Figure 1 and Supplementary Figure 2. For the percent weight CFB to 52 weeks, data were available for all comparators in the total, non-T2DM, and T2DM populations. Liraglutide was the only comparator with available data in the NGT population. In the pre-diabetic population, data were available for liraglutide and phentermine/topiramate.
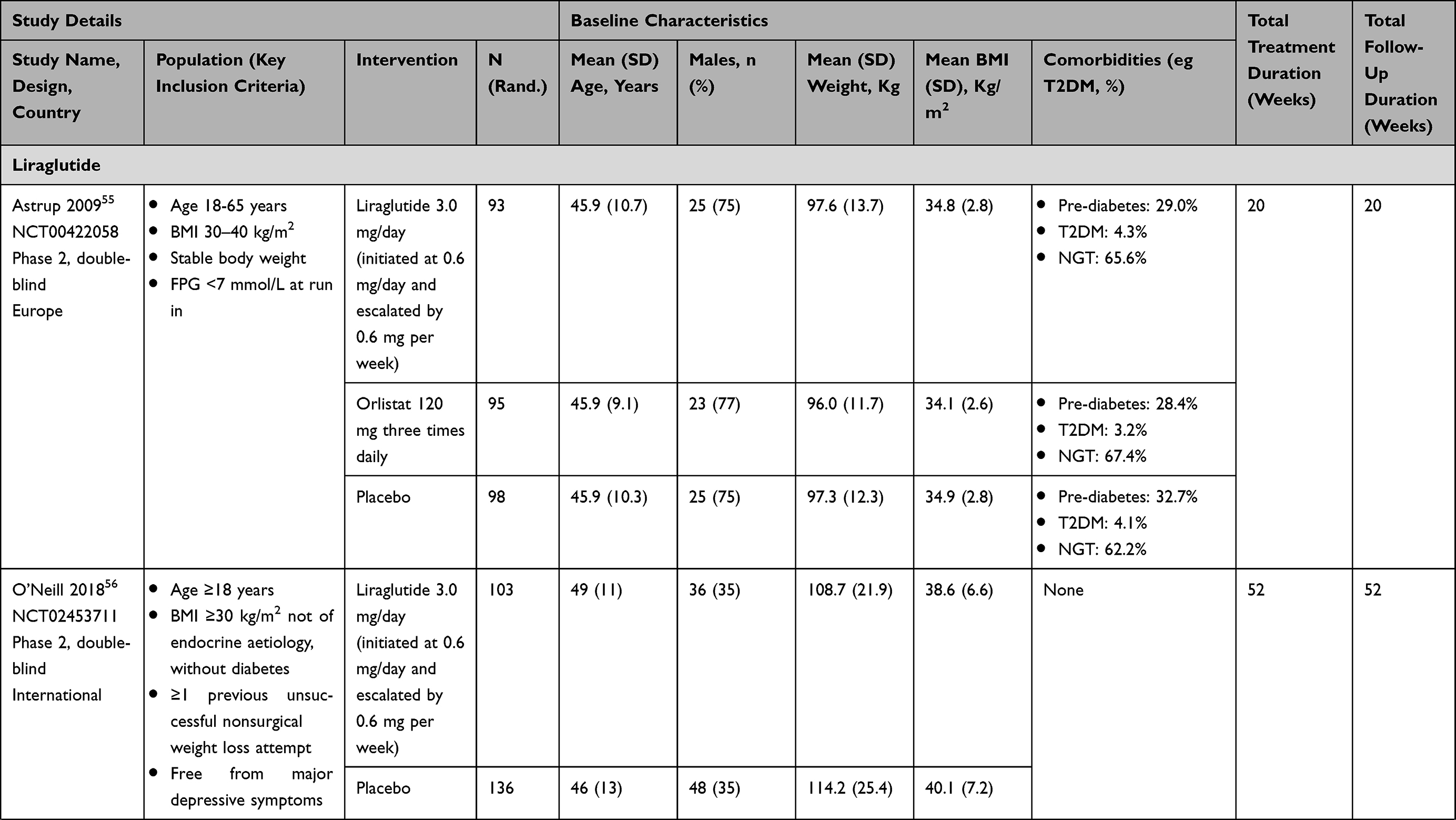 | 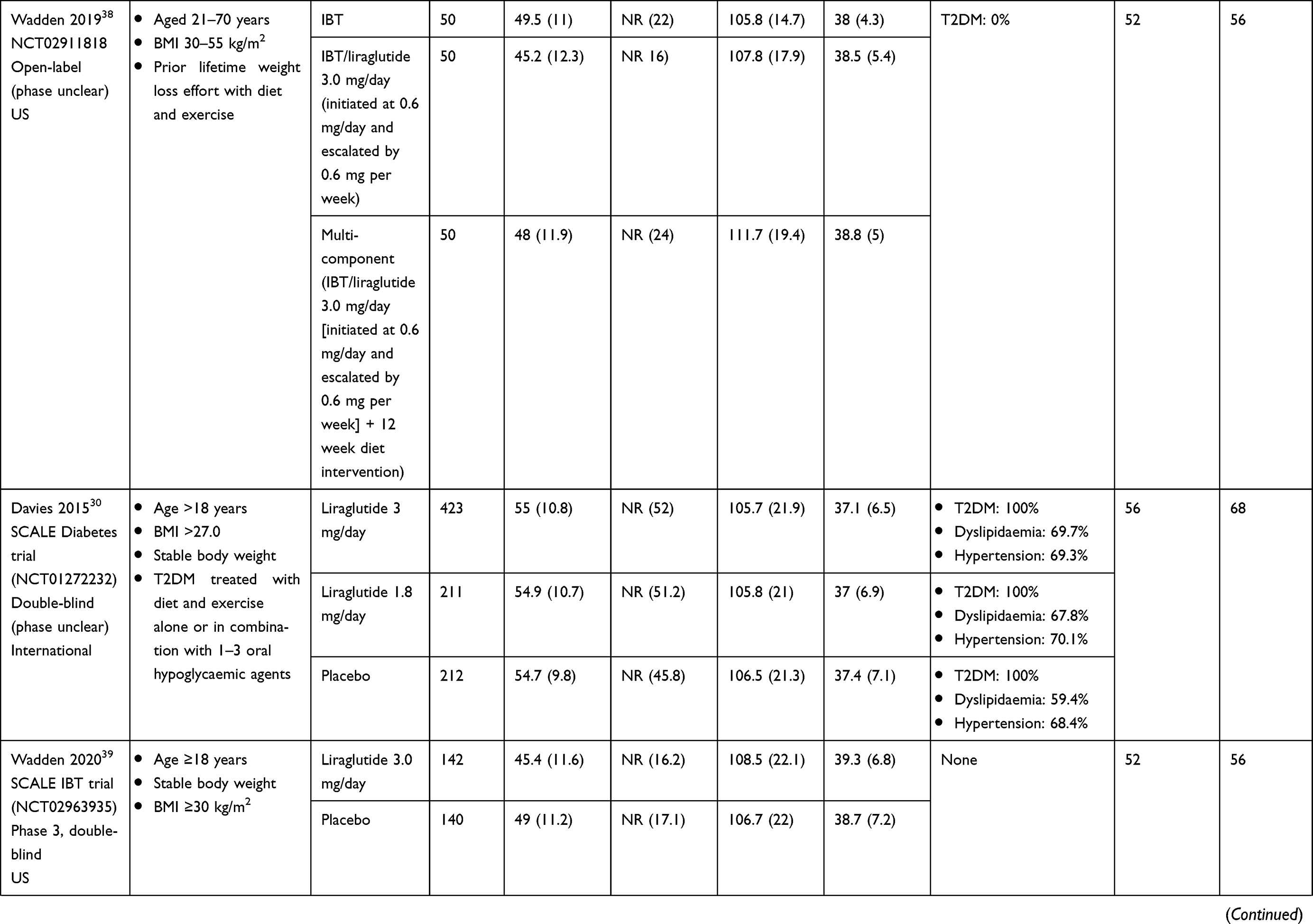 | 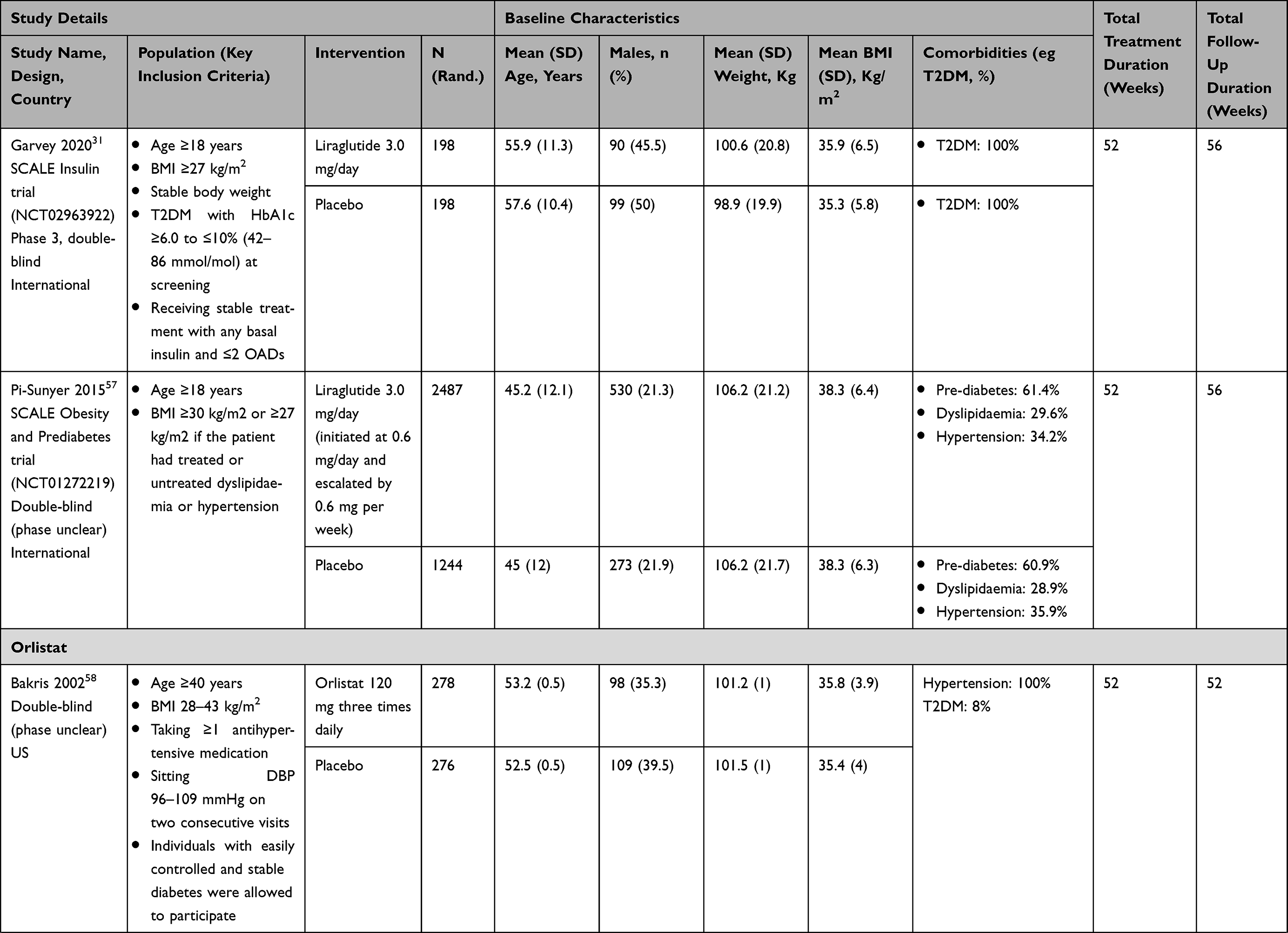 | 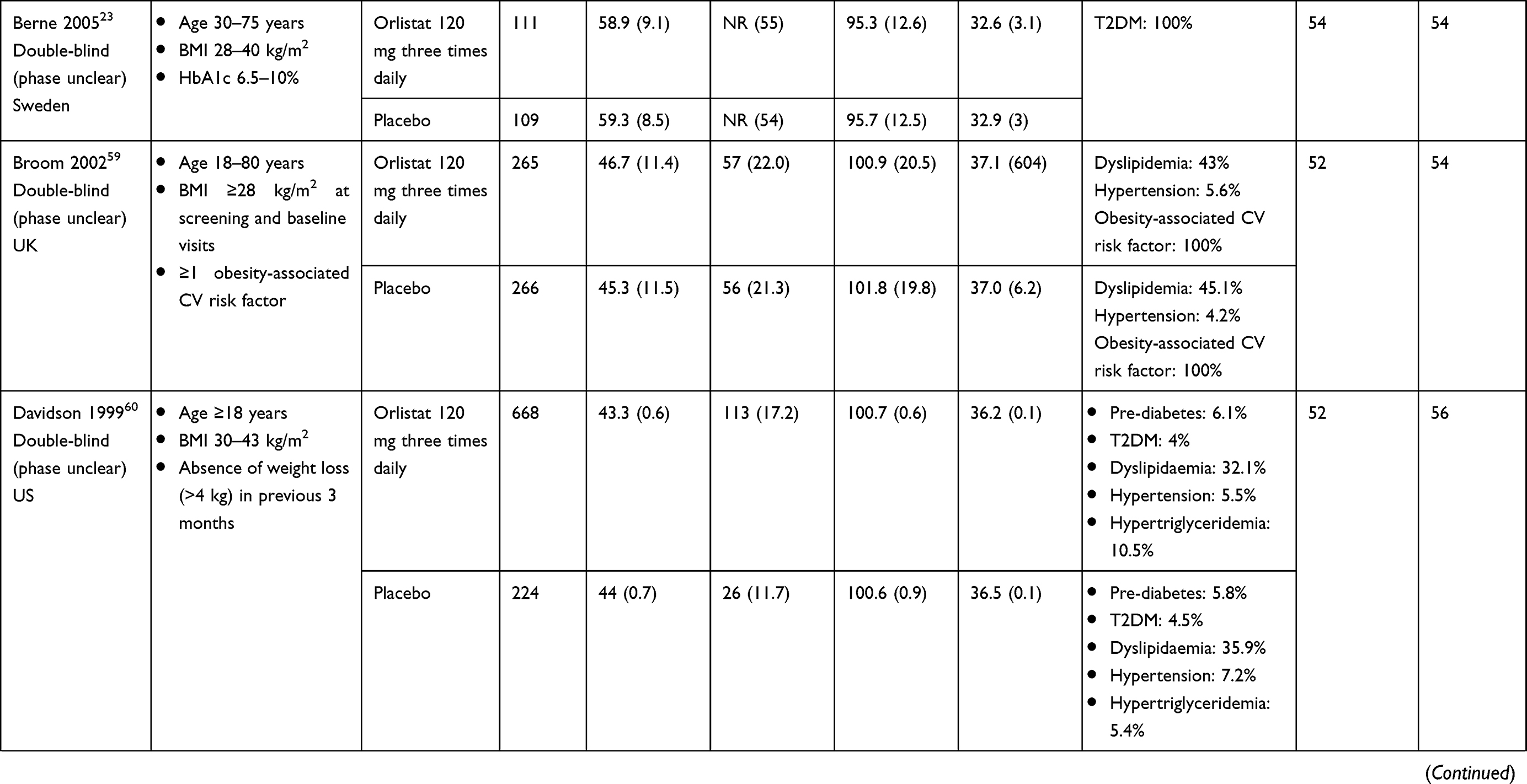 | 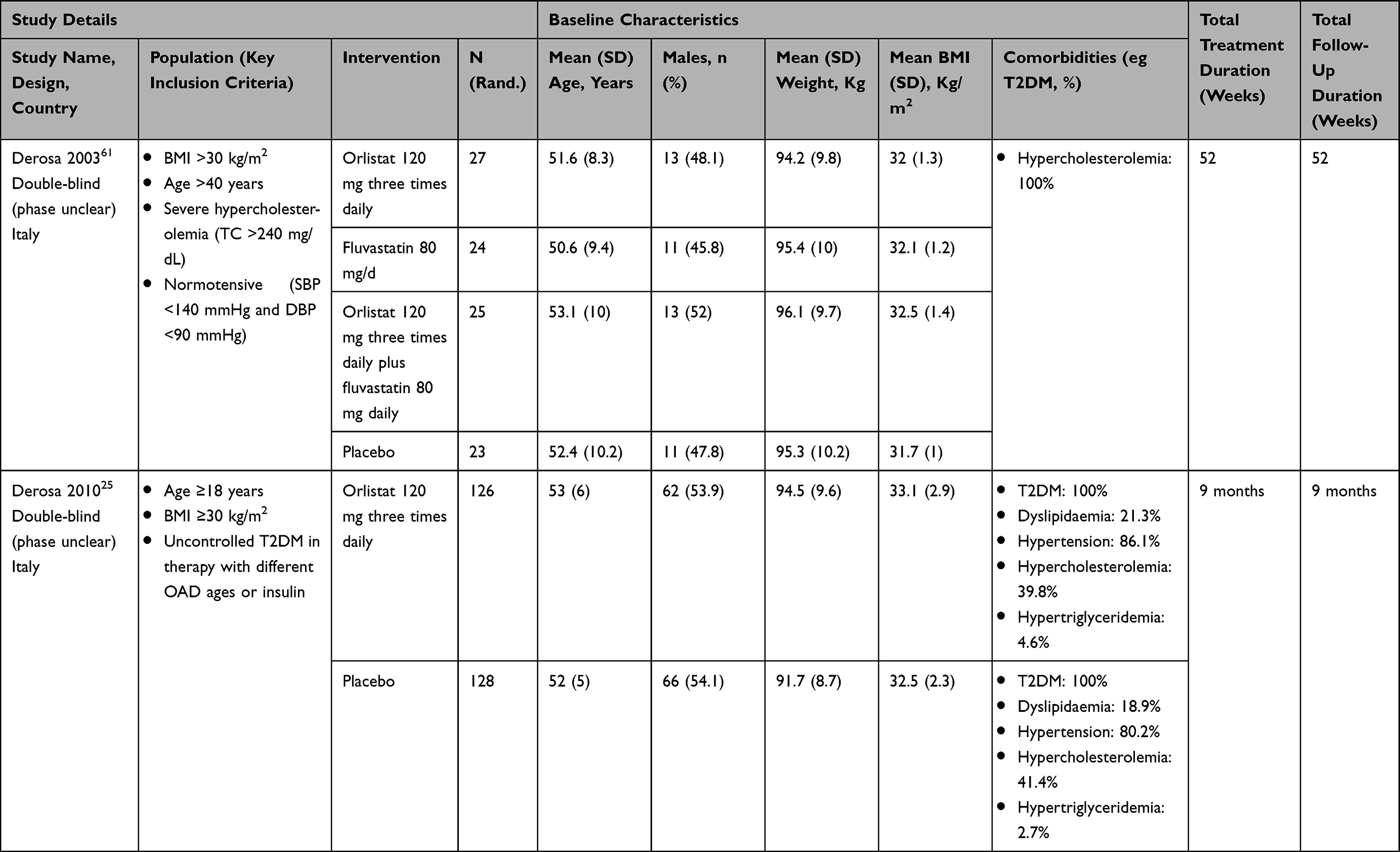 | 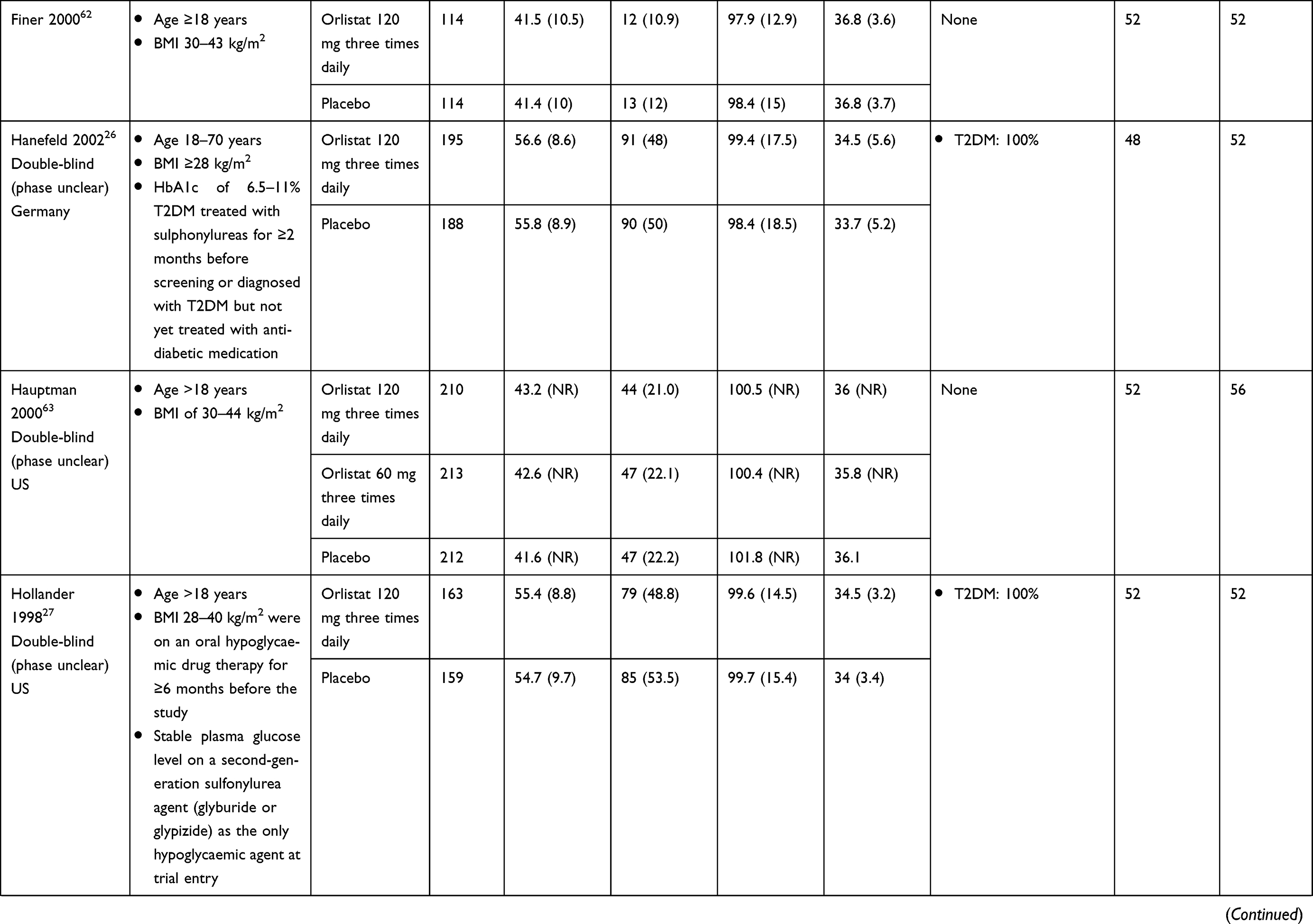 | 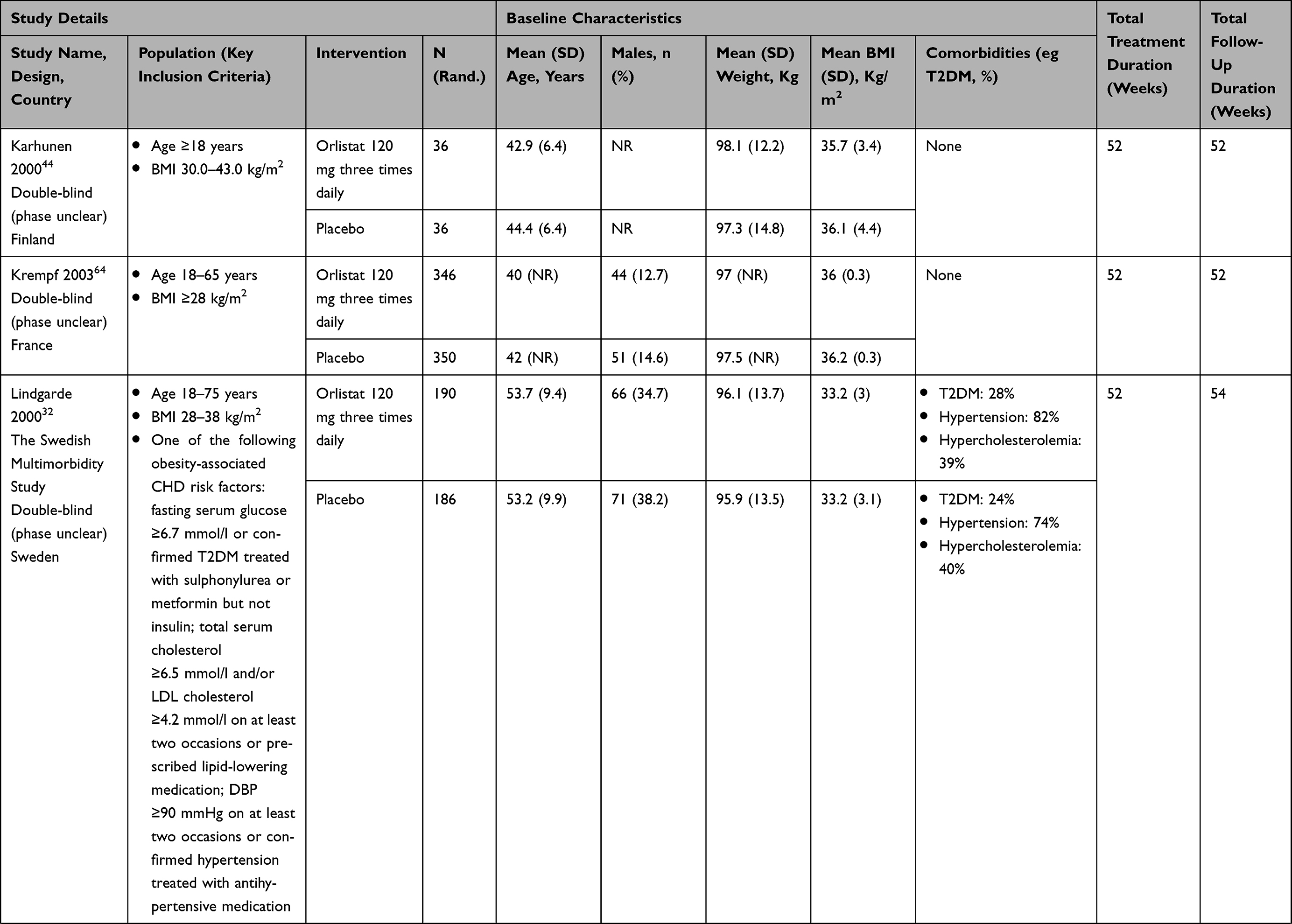 | 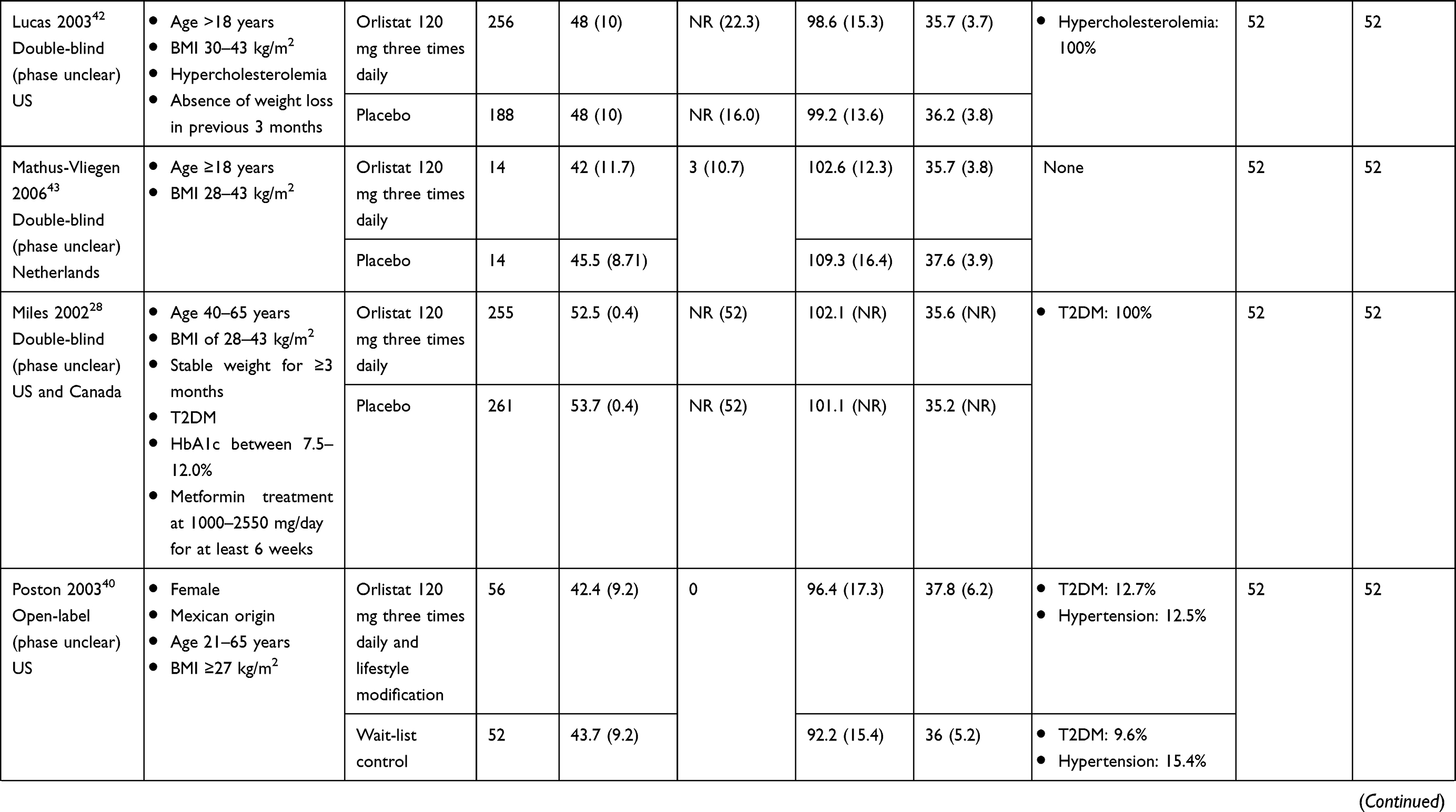 | 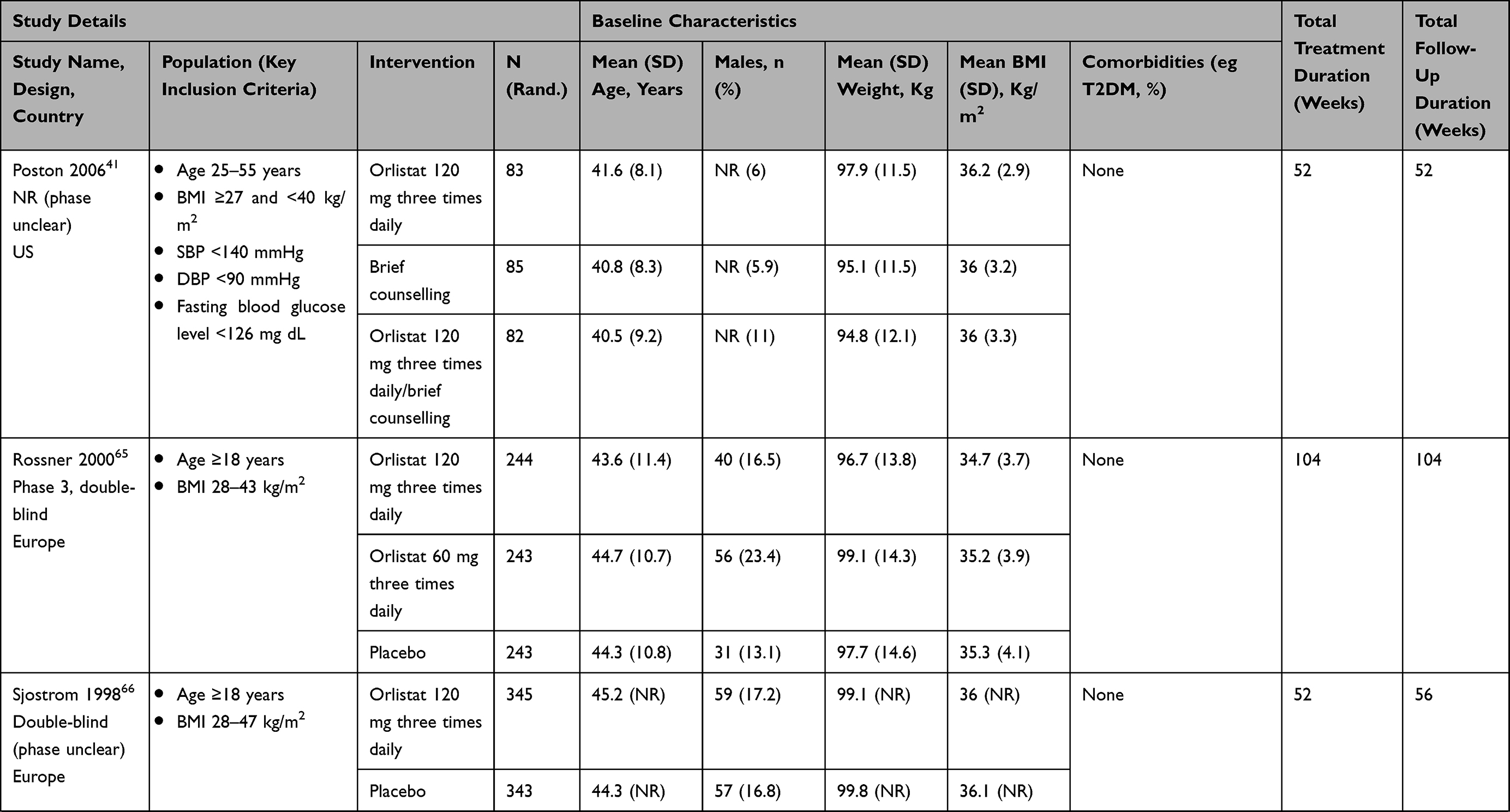 | 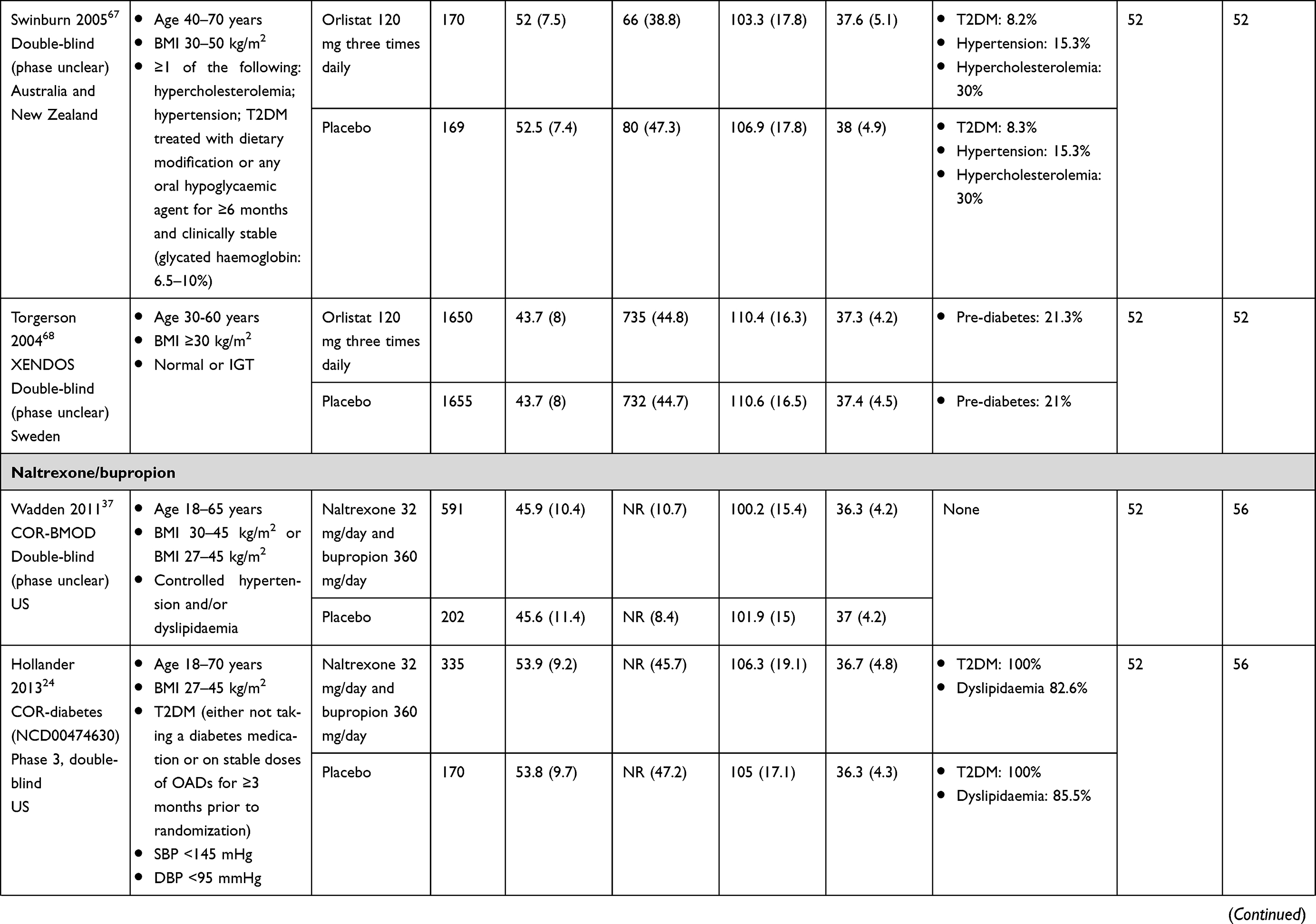 | 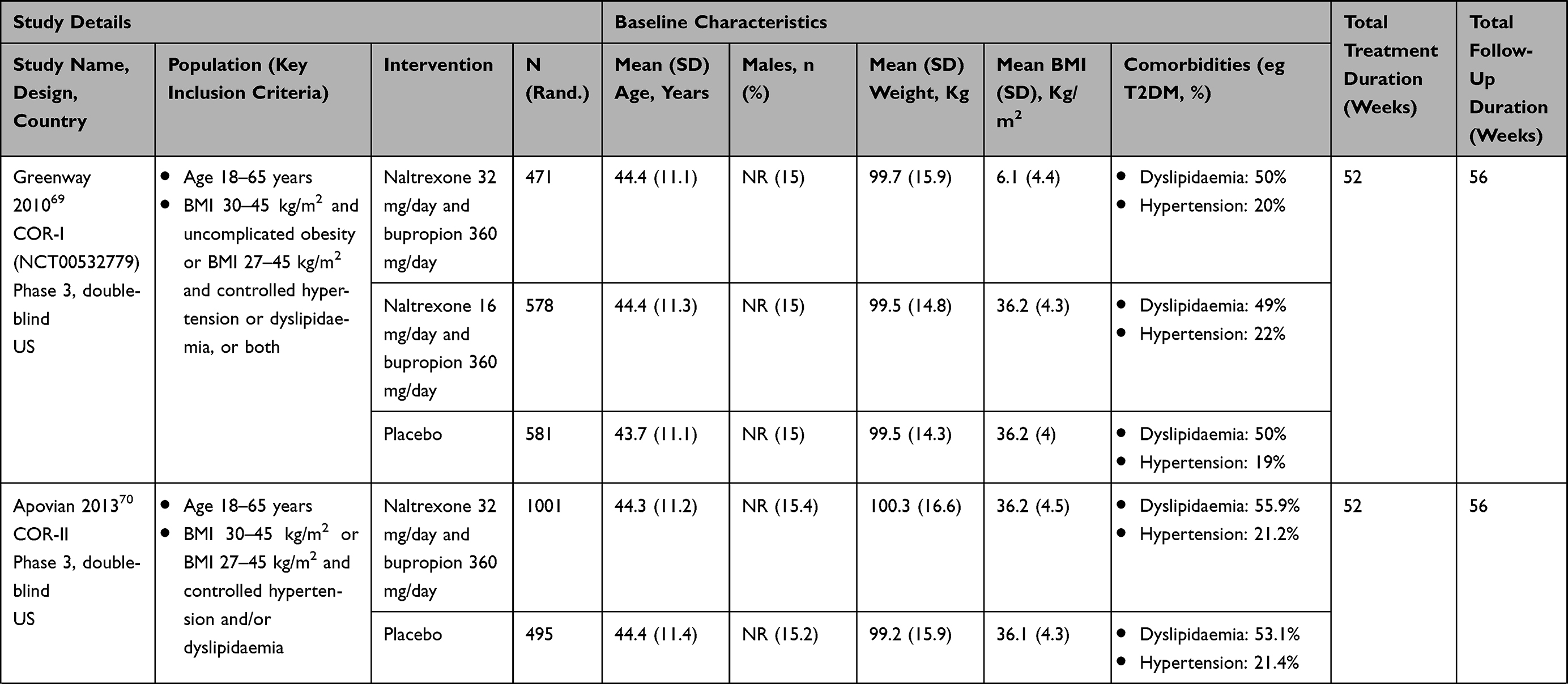 | 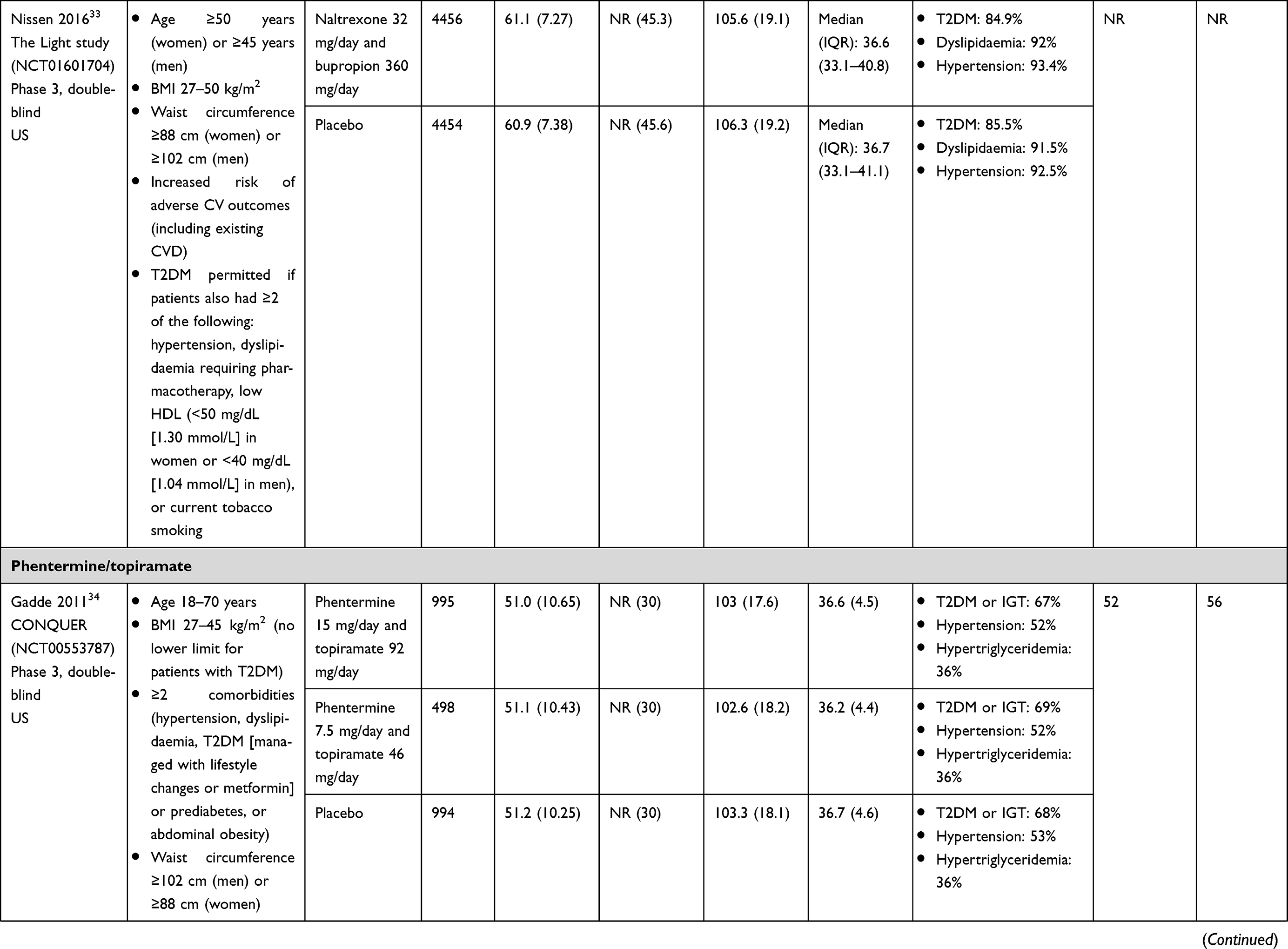 | 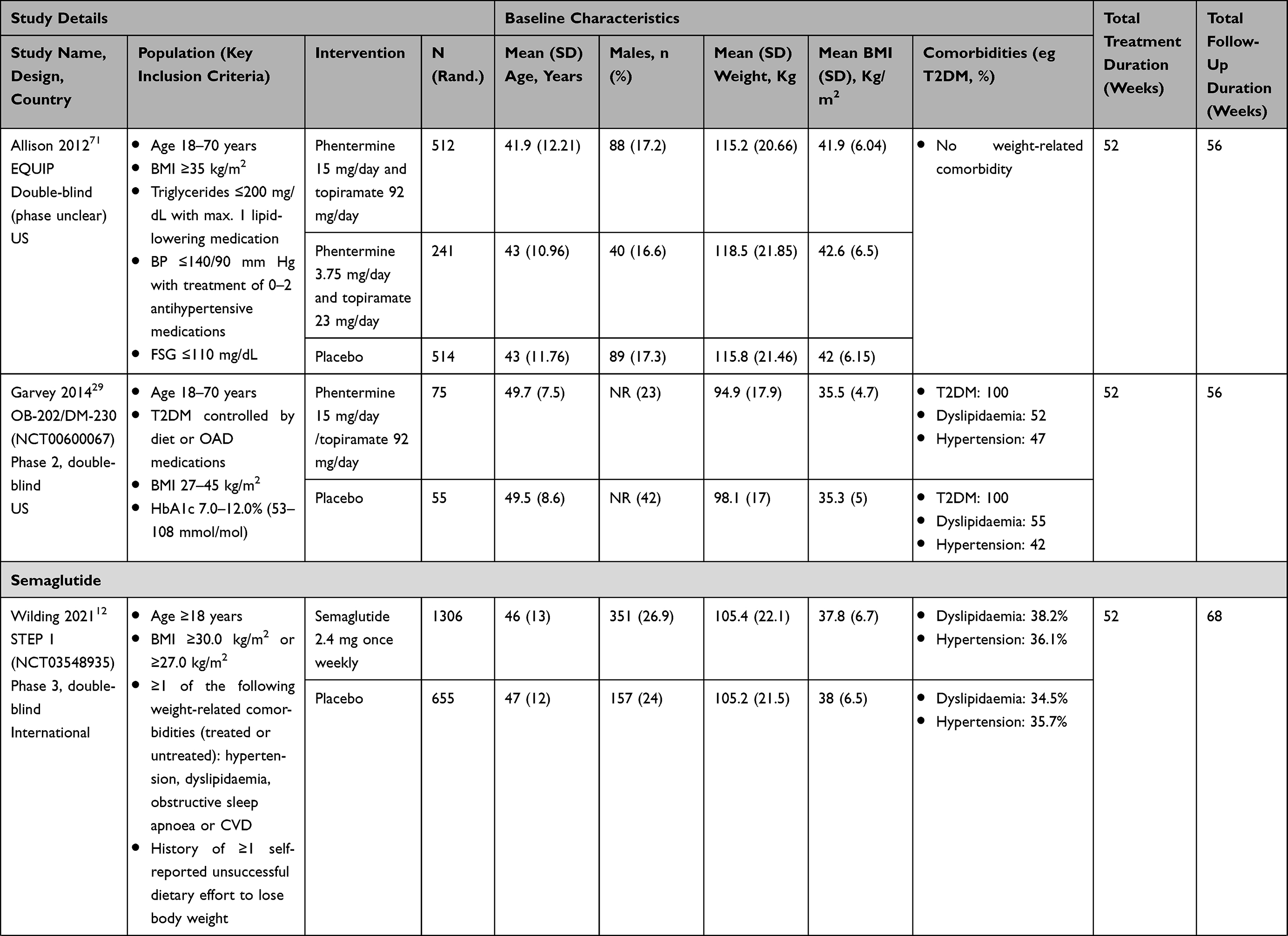 | 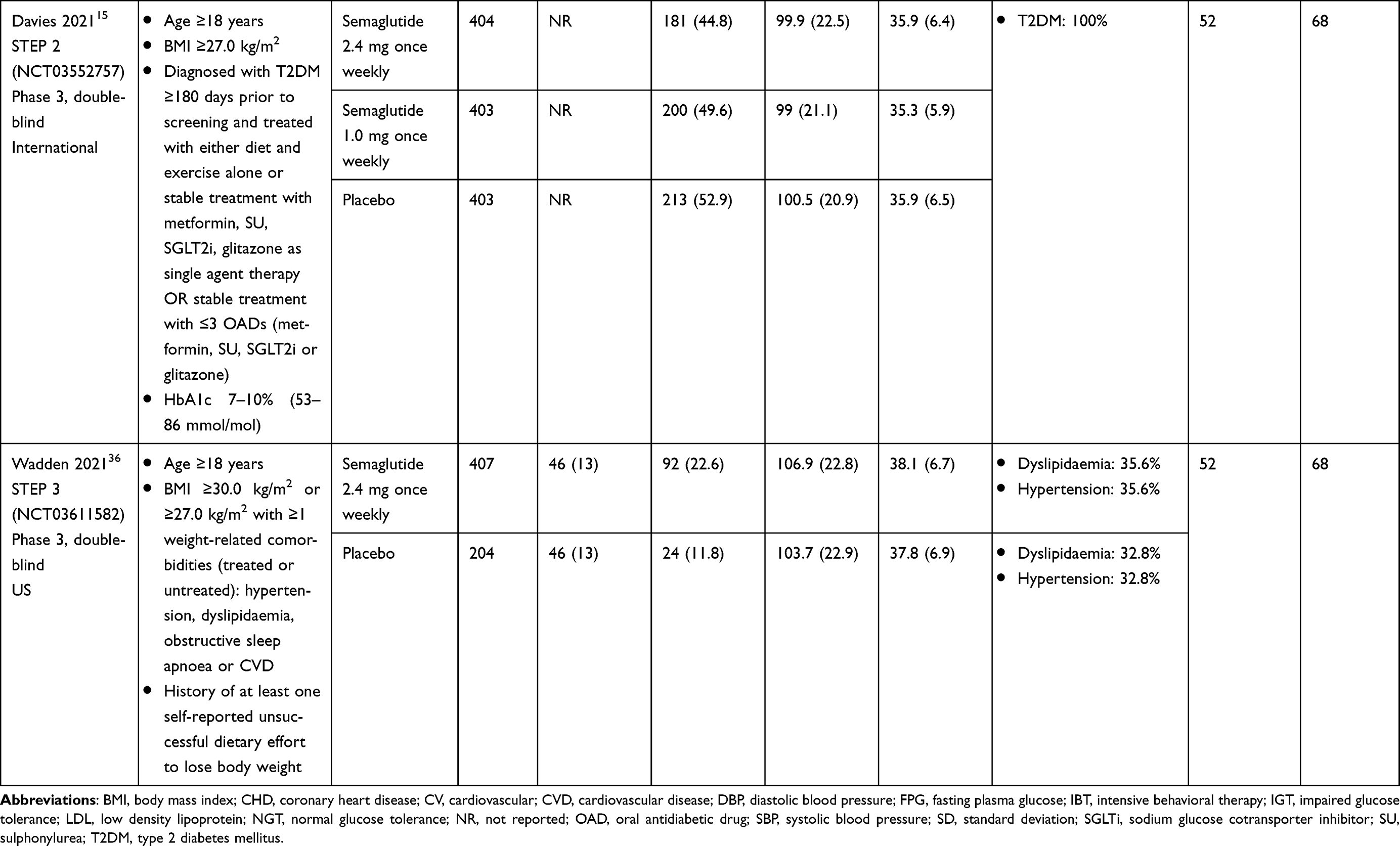 |
Table 2 Summary of Eligible Studies Investigating Pharmacological Agents Identified in Systematic Literature Review |
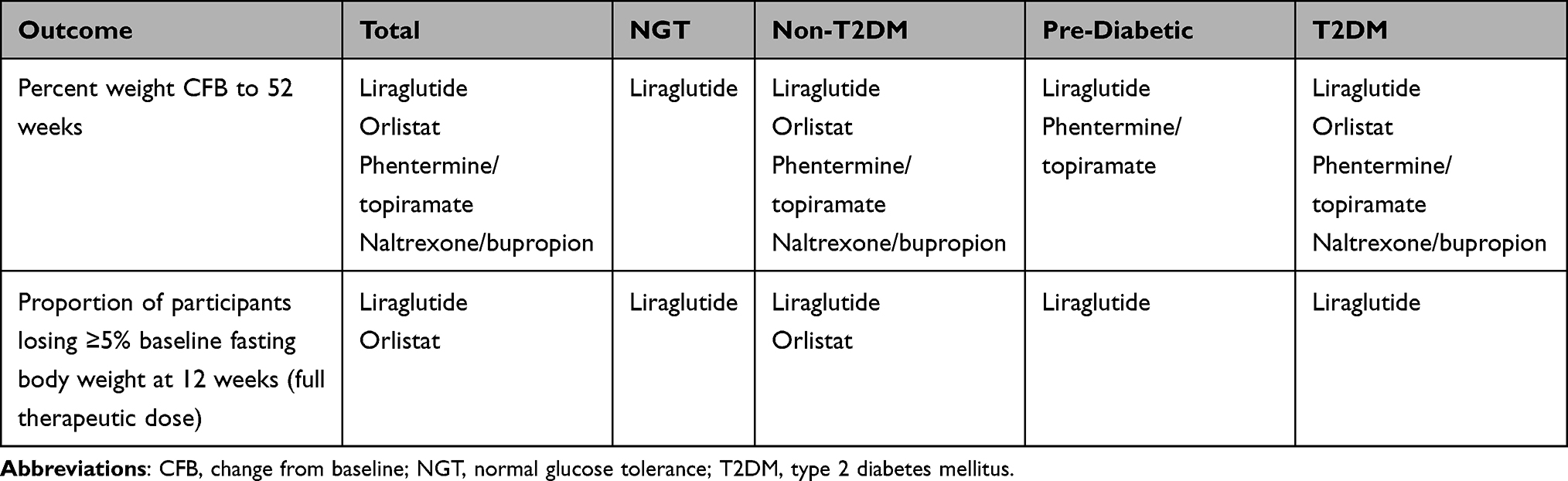 |
Table 3 Comparators for Which Data are Available Across the Populations of Interest |
For the proportion of participants losing ≥5% baseline fasting body weight at 12 weeks of full therapeutic dose, no comparisons were feasible for semaglutide 2.4 mg versus phentermine/topiramate or naltrexone/bupropion. Data on liraglutide and orlistat were available for the total and non-T2DM populations, while liraglutide was the only comparator for the NGT, pre-diabetic and T2DM populations.
Variability was noted across the trials in terms of the study design and populations (eg, age, sex, weight, and BMI); however, the studies in the evidence networks were considered sufficiently homogenous to combine in NMAs. Potential outlier studies included the Light study, which enrolled women aged ≥50 years and men aged >45 years and included a population with a higher mean age than other trials. The EQUIP trial enrolled people with BMI ≥35 kg/m2 and therefore the study population had a higher mean BMI than other trials. There were also differences in the proportion of participants with comorbidities, particularly T2DM. A total of 13 studies included in the SLR exclusively enrolled people with T2DM23–31 or a proportion of participants with T2DM.32–34 As relative treatment effects may be different in people with or without T2DM, the current analysis considered subpopulations according to glucose tolerance to account for any differences conferred by T2DM.
Intensive behavioral therapy (IBT) is a form of obesity management that aims to change eating and exercise habits.35 Inclusion of IBT as an adjunctive treatment in studies may be disadvantageous to pharmacological therapies; the relative treatment effects versus control may be lower in trials that include IBT than in those that exclude IBT.36 Five trials (COR-BMOD,37 NCT02911818,38 STEP 3,36 SCALE IBT,39 and SCALE Insulin trial)31 specified IBT as a concomitant lifestyle therapy (comprising counselling, dietary advice, and increased physical activity). To account for the potential impact of IBT on the outcomes of the NMA, these five trials were excluded from the networks (although it is noted that participants in the remaining studies in the network may also have received dietary and exercise advice). Thus, up to 20 studies were included in the evidence networks (20 in the total population, nine in the TD2M network, 12 in the non-T2DM network, three in the pre-diabetes network, and two in the NGT network).
Results of the quality assessment are presented in Supplementary Table 2 for all 41 RCTs (49 publications) considered for the NMAs. In general, the trials included in the NMAs were high quality with adequate randomization and concealment of treatment allocation. Across all studies, baseline characteristics were well balanced between treatment groups and all measured outcomes were reported. All trials were blinded except one that was not blinded and the authors acknowledged that this prevented them from determining the independent effect of orlistat.40 In a second study, the extent of blinding was unclear but the potential impact on results was not discussed.41 All studies used an intention-to-treat (ITT) analysis except for two in which this was unclear42,43 and two that did not use an ITT analysis. Of the latter studies, one analyzed completers at 2 years but the impact of the non-ITT analysis was not discussed in the publication.44 The second study was excluded from the NMAs as it included IBT.37
Network Meta-Analysis
Percent Weight CFB to 52 Weeks
In all populations studied, semaglutide 2.4 mg was associated with a greater percentage weight CFB with 52 weeks of treatment versus all available comparators, except for phentermine 15 mg/topiramate 92 mg in the T2DM population.
In the total population, the differences with semaglutide 2.4 mg versus comparators ranged from –0.40% (CrI –4.22, 3.46) for phentermine 15 mg/topiramate 92 mg to –9.36% (CrI –12.06, –6.62) for placebo/control. In the T2DM population, the differences with semaglutide 2.4 mg versus comparators ranged from 0.67% (CrI –6.65, 7.86) for phentermine 15 mg/topiramate 92 mg to –6.22% (CrI –11.29, –1.19) for placebo. In the non-T2DM population, the differences with semaglutide 2.4 mg versus comparators ranged from –3.35% (CrI –5.85, –0.80) with phentermine 15 mg/topiramate 92 mg to –12.43% (CrI –14.51, –10.38) with placebo/control. In the pre-diabetes population, the differences with semaglutide 2.4 mg versus comparators ranged from –3.06% (CrI –4.55, –1.59) with phentermine 15 mg/topiramate 92 mg to –11.26% (–12.52, –10.01) with placebo/control. In the NGT population, data were available for comparison of semaglutide 2.4 mg with placebo/control (difference –13.42% [CrI –14.56, –12.28]) and liraglutide 3.0 mg (–8.13% [CrI –9.47, –6.80]). Full results of the NMAs are shown in Table 4.
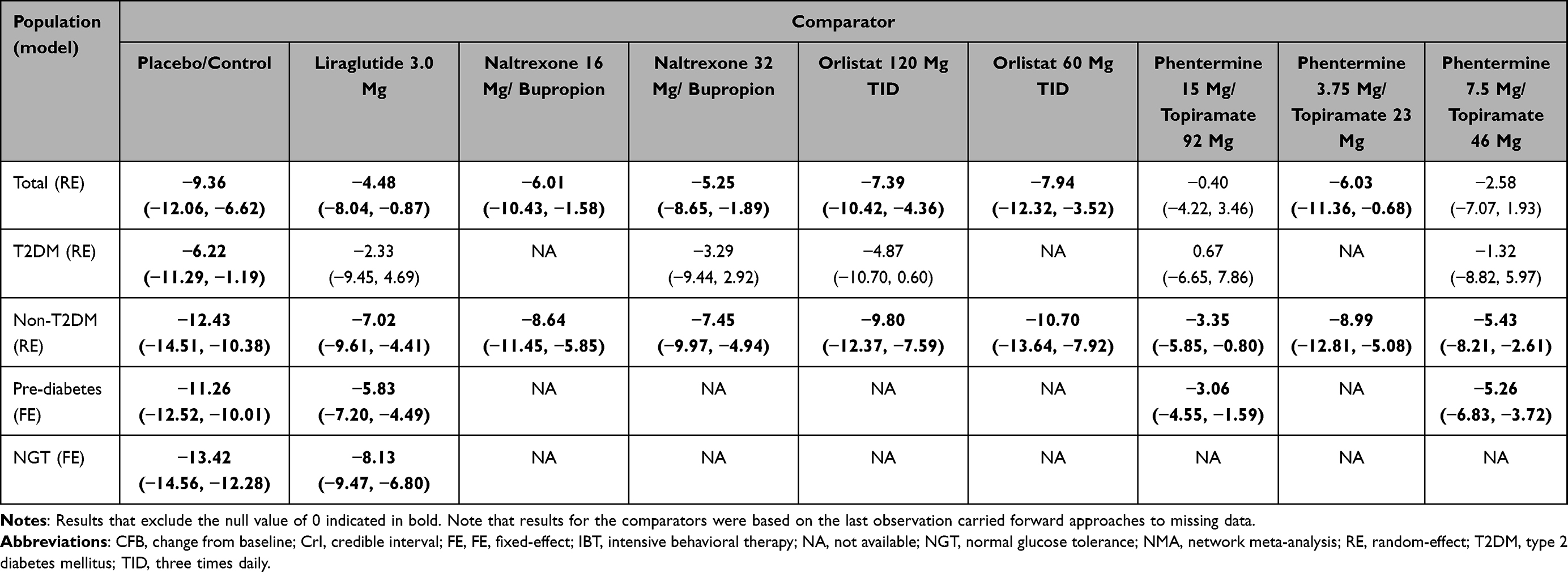 |
Table 4 NMA Results: Estimates of Difference in Percent Weight CFB (Semaglutide versus Comparators, Excluding Trials That Included IBT) |
Proportion of Participants Losing ≥5% Fasting Body Weight at 12 Weeks of Full Therapeutic Dose
In all populations, semaglutide 2.4 mg was associated with a higher likelihood of participants losing ≥5% of baseline fasting body weight at 12 weeks versus all available comparators (liraglutide 3.0 mg and orlistat 120 mg). The ORs for semaglutide versus placebo ranged from 8.86 (95% CI 6.24, 12.00 [T2DM]) to 14.81 (95% CI 11.02, 20.17 [NGT]). When considered against active comparators, semaglutide also increased the likelihood of participants losing ≥5% fasting body weight, with ORs ranging from 1.29 (95% CI 0.70, 2.13 [T2DM]) to 2.17 (95% CI 1.44, 3.27 [NGT]) with liraglutide 3.0 mg and from 6.09 (95% CI 2.86, 11.95 [total population]) to 7.75 (95% CI 5.29, 11.37 [non-T2DM]) with orlistat 120 mg three times daily (TID). Full results of the NMA for this outcome are presented in Table 5.
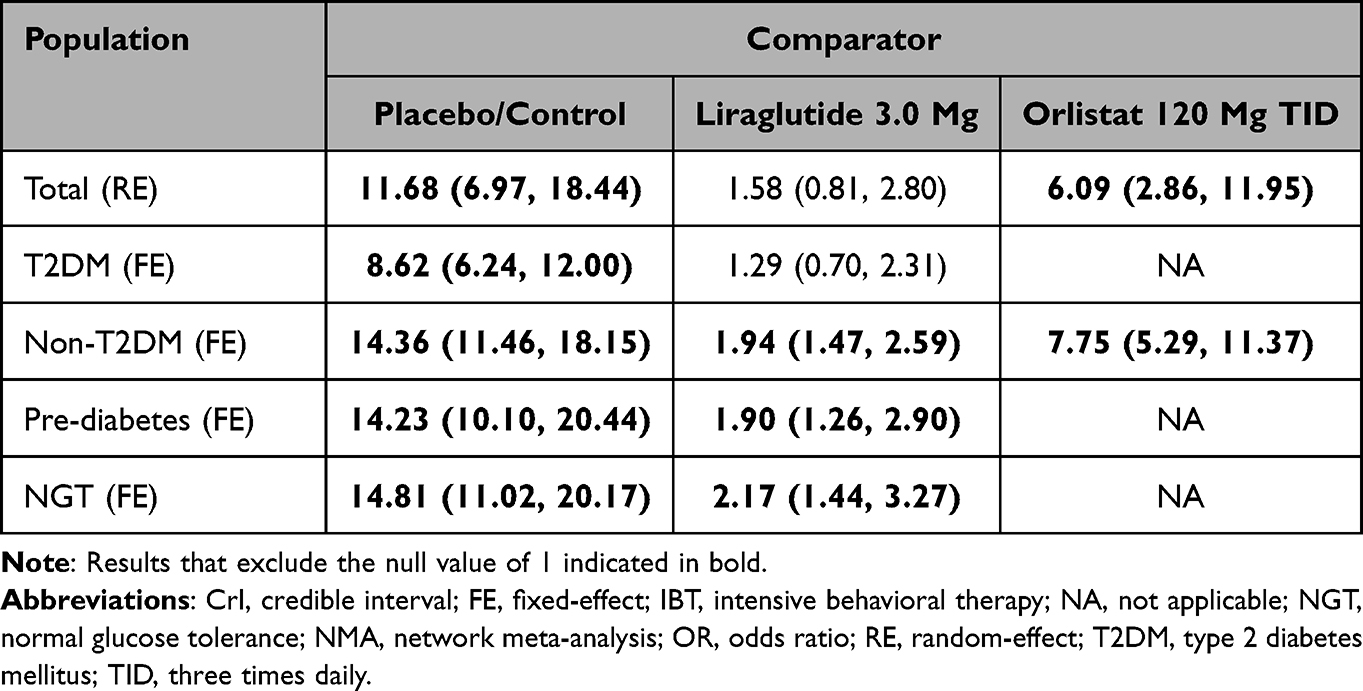 |
Table 5 NMA Results: OR (95% CrI) for Proportion of Participants Losing ≥5% of Baseline Fasting Body Weight at 12 Weeks Full Therapeutic Dose (Semaglutide versus Comparators, Excluding Trials That Included IBT) |
Discussion
Obesity is a substantial clinical and economic burden1 that has grown rapidly in recent decades45 and is expected to continue to increase globally in the coming years.46 Despite overweight and obesity affecting >2 billion people worldwide,1 uptake of pharmacological treatments for the management of these conditions is generally low.8 Low uptake has been attributed to several factors, including only modest additional weight loss with the available therapies, safety concerns, lack of health-care professional experience with such therapies, and expectations that overweight/obesity should be managed with behavioral measures.8,47 There is therefore an unmet need for an effective and safe pharmacological therapy for the management of overweight and obesity.
Randomized controlled trials of semaglutide in conjunction with lifestyle modifications have shown that semaglutide 2.4 mg represents an effective and safe weight loss reduction therapy in people with overweight and obesity with and without T2DM.12,15 Because the trials compared semaglutide with placebo, no head-to-head data were available to compare semaglutide with active treatments used in the management of overweight and obesity. The current SLR and meta-analysis was performed to identify and compare RCT evidence for weekly semaglutide 2.4 mg with that of relevant pharmacological comparators for weight management in overweight or obesity.
The SLR identified 20 RCTs that were ultimately included in the NMA. In the NMA, semaglutide 2.4 mg was associated with a greater percent weight CFB with 52 weeks of treatment versus all available comparators in all populations, except phentermine 15 mg/topiramate 92 mg in the T2DM population. A single study, CONQUER,34 contributed subgroup data to this comparison. It is noteworthy that in the phentermine 15 mg/topiramate 92 mg arm of CONQUER, 192 of 995 participants in the total population discontinued due to adverse events (it was unclear how many of the 664 participants with T2DM in this arm discontinued), which was notably higher than the placebo and phentermine 7.5 mg/topiramate 46 mg treatment arms (89 of 994 and 58 of 498 discontinuations due to adverse events, respectively). The results of this trial confirm the safety concerns associated with phentermine/topiramate. Further, the analyses in this trial were conducted on the ITT sample and applied the last observation carried forward (LOCF) principle which may have biased the trial level results in favor of phentermine 15 mg/topiramate 92 mg. Whilst LOCF was the most commonly used method to address missing data across the trials included in the NMA, LOCF-based statistical approaches are no longer recommended due to concerns regarding the plausibility of the assumptions (ie, body weight would be unaffected by discontinuations for trial participants lost to follow-up) and the potential for bias.48 In contrast, the STEP trials used treatment policy estimands in the primary analyses, which assess all participants who were randomly assigned to treatment regardless of adherence to treatment and regardless of initiation of other therapies; missing data were imputed using a multiple imputation approach. Thus, the use of treatment policy estimands and the difference in approach to addressing missing data in the STEP trials versus the comparator trials in the NMA will have likely biased the treatment effect against semaglutide.
Semaglutide 2.4 mg was also associated with a higher chance of losing ≥5% baseline fasting body weight at 12 weeks (at full therapeutic dose) versus all available comparators. When considering the outcomes associated with semaglutide, it is important to note that semaglutide has a longer dose escalation period (at least 4 weeks) than other therapies (eg, at least one week for liraglutide); therefore, patients receiving semaglutide have a longer treatment exposure duration compared with those receiving other therapies.
While head-to-head comparison data are preferable where available, NMA is a robust statistical approach that facilitates indirect comparison of multiple treatment options when direct comparative data are not available. NMAs are widely used in healthcare decision-making, including in health technology assessment. Compared with head-to-head data from RCTs, in which there is expected to be minimal confounding between the treatment groups, NMA will inevitably be based on data with a degree of heterogeneity between studies. Although the studies in the current evidence networks were sufficiently homogeneous to perform NMAs, some variability was observed between the trials in terms of study designs and patient populations. Differences in the proportion of participants with abnormal glucose tolerance or T2DM were addressed through the analysis of subpopulations according to glucose tolerance. However, other potential effect modifiers were observed, including one study that only included women40 and variation in the age categories included (eg, all participants aged ≥18 years or a narrower age range, such as 25–55 years). It is also important to recognize that publications cover a wide timescale, ranging from 1998 to present. The older studies (which primarily reported on orlistat) had significant amounts of missing outcome data, particularly for adverse events, which may have resulted in reporting bias. Underreporting of adverse events in orlistat trials was also described by Schroll et al who found considerable disparities in adverse event reporting between clinical study protocols, reports, and publications. It was estimated that only 3–33% of all investigator-reported adverse events were eventually presented in the relevant publications, even though most publications claimed that all adverse events were recorded.49
The outcomes reported here were part of a larger analysis that included additional outcomes, such as glucose control, cholesterol, blood pressure and serious adverse events (SAEs). The safety of semaglutide compared with other pharmacological therapies is an important consideration as many of the other therapies have an adverse event profile that contributes to their low uptake.47,50 Although phentermine/topiramate is licensed in the US, it received a negative opinion for the European Committee for Medicinal Products for Human Use (CHMP) due to concerns about the phentermine’s long-term impact on the heart and blood vessels, as well as the potential for psychiatric and cognitive effects.9 The CHMP also noted methodological concerns because the data showed a study dropout rate of approximately 40% and a lost to follow-up rate of more than 10%.9 An NMA conducted for SAEs associated with semaglutide 2.4 mg and comparators showed that semaglutide 2.4 mg was associated with a higher proportion of SAEs than comparators in the populations studied. The exception to this was in the T2DM population where semaglutide 2.4 mg was associated with fewer SAEs than all available comparators, except naltrexone 32 mg/bupropion 360 mg. However, it is important to note that the credible intervals associated with the results were very wide, indicating a high degree of uncertainty. Furthermore, it has been reported elsewhere that the side effects of semaglutide 2.4 mg are mainly nausea, diarrhea, and cholelithiasis, which are typical for this drug class.50 Finally, as described earlier, there is evidence to suggest that adverse events associated with other weight loss drugs, particularly orlistat, are considerably underreported in the published literature.49
Since the current SLR and NMA were conducted, the results of several other studies of semaglutide have been published, as well as a SLR and NMA of pharmacotherapy for overweight and obesity. Published trials include STEP 8, which compared once-weekly subcutaneous semaglutide 2.4 mg with once-daily subcutaneous liraglutide 3.0 mg in conjunction with counselling for diet and physical activity for people with overweight or obesity.16 Semaglutide demonstrated a significantly greater weight CFB compared with liraglutide and participants receiving semaglutide were significantly more likely to achieve ≥10%, ≥15%, and ≥20% weight loss versus those receiving liraglutide at Week 68.16 In STEP 8, the weight CFB reported with semaglutide versus liraglutide was higher than that in the current NMA (–9.4% at Week 68 versus –4.5% at Week 52). Although reported at different timepoints, these data suggest that the NMA results validate (or even somewhat underestimate) the benefits of semaglutide in comparison with liraglutide that have been reported directly in the STEP 8 RCT.16 STEP 8 also showed that the rates of discontinuation due to AEs were lower with semaglutide (3.2%) than with liraglutide (12.6%), with the semaglutide discontinuation rate in line with that of the placebo group (3.5%).16 Additional data from recent reviews and/or meta-analyses show that semaglutide is effective in people with overweight or obesity with or without T2DM.51–53 These findings support those of the present analysis in demonstrating the benefits of semaglutide 2.4 mg versus liraglutide.
Shi et al published the findings of a SLR and NMA of RCTs and pharmacotherapy for adults with overweight and obesity.54 The analysis included data from trials that were inclusive of IBT (whereas they were excluded from the current NMAs) and had a mean follow-up of 24 weeks compared with 12 months in the current analysis. The main analyses by Shi et al included grouped treatment nodes for GLP-1 antagonists and sodium glucose cotransporter inhibitors and the results showed that phentermine/topiramate provided the most effective weight loss; however, it is important to consider this in light of the safety concerns associated with phentermine/topiramate that are reported earlier. The second most effective therapies were GLP-1 receptor agonists, including semaglutide, which was the most effective drug in its class (and versus all other comparators) when sensitivity analyses were conducted. Furthermore, although semaglutide and several other therapies were associated with an increased risk of adverse events, semaglutide showed substantially larger weight loss benefits than other therapies with a similar risk of adverse events.54
Limitations of the current analysis include those that are inherent to indirect treatment comparison and NMA. The creation of evidence networks requires assumptions around study homogeneity with regard to multiple aspects, including study populations and outcome definitions. A heterogeneity assessment and subgroup analyses by glucose tolerance were performed in the current study; however, as noted previously, there was still heterogeneity between studies in factors such as participant age, sex, and BMI. Some of the older studies also had significant amounts of missing data, which limited the analyses that could be conducted and may have resulted in reporting bias. Nevertheless, in the populations for which data were available, semaglutide mainly showed clinical benefits versus the available comparators. Finally, as noted in the methods, trials of bariatric surgery were not included in the NMAs because these trials were highly selective in comparison with studies investigating pharmacological agents. Therefore, the current analysis was limited to pharmacological agents; however, there is potential for future exploration of weight loss indications where a pharmacological agent is used prior to bariatric surgery or following bariatric surgery if weight loss is insufficient.
Conclusion
In summary, high-quality, RCT-based evidence has shown that semaglutide 2.4 mg is an effective weight management therapy in conjunction with lifestyle interventions for overweight and obesity in people with and without T2DM. In NMA, semaglutide 2.4 mg was compared against active comparators, including orlistat and liraglutide, and demonstrated effective weight loss in the total population and nearly all subpopulations of glucose tolerance; this differentiates the present NMA from others conducted previously, which have focused on specific populations of glucose tolerance (eg, only people with T2DM) and shows that semaglutide is effective across different levels of glucose tolerance. The present study also uses longer term data than that of previous studies and excludes IBT to enable more focused comparison between pharmacological therapies. Current pharmacological therapies for obesity have low uptake rates due to limited efficacy but semaglutide represents a new and effective treatment that may address this unmet need.
Abbreviations
BMI, body mass index; CFB, change from baseline; CHMP, European Committee for Medicinal Products for Human Use; DIC, deviance information criterion; FE, fixed effect; GLP-1, glucagon-like peptide 1; IBT, intensive behavioral therapy; ITT, intention-to-treat; LOCF, last observation carried forward; MCMC, Markov Chain Monte Carlo; NGT, normal glucose tolerance; NICE, National Institute for Health and Care Excellence; NMA, network meta-analyses; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; RCT, randomized placebo-controlled trials; RE, random effect; SAE, serious adverse events; SLR, systematic literature review; STEP, Semaglutide Treatment Effect in People with obesity; T2DM, type 2 diabetes mellitus; TID, three times daily.
Data Sharing Statement
All data relevant to the manuscript are presented herein.
Ethics Approval and Informed Consent
This review did not include human or animal participants and therefore ethical approval/informed consent was not required.
Consent for Publication
The authors consent to the publication of all materials submitted with this manuscript, including figures and tables.
Acknowledgments
We thank Helen Lilley (Mtech Access) who provided medical writing services in the preparation of the manuscript, funded by consultancy payments from Novo Nordisk.
Funding
This work (including study design; collection, analysis, and interpretation of data; and preparation of the manuscript) was funded by Novo Nordisk.
Disclosure
Inger Smith is an employee of White Box Health Economics, which received contractor payments from Novo Nordisk for this work. Emily Hardy, Stephen Mitchell, and Sarah Batson are employees of Mtech Access, which received consultancy payments from Novo Nordisk for this work. The authors report no other conflicts of interest in this work.
References
1. World Health Organisation. Obesity and overweight; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
2. Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. 2009;9(1):88. doi:10.1186/1471-2458-9-88
3. Chen X, Pensuksan WC, Lohsoonthorn V, Lertmaharit S, Gelaye B, Williams MA. Obstructive sleep apnea and multiple anthropometric indices of general obesity and abdominal obesity among young adults. Int J Soc Sci Stud. 2014;2(3):89–99. doi:10.11114/ijsss.v2i3.439
4. Pantalone KM, Hobbs TM, Chagin KM, et al. Prevalence and recognition of obesity and its associated comorbidities: cross-sectional analysis of electronic health record data from a large US integrated health system. BMJ Open. 2017;7(11):e017583. doi:10.1136/bmjopen-2017-017583
5. Wilfley DE, Hayes JF, Balantekin KN, Van Buren DJ, Epstein LH. Behavioral interventions for obesity in children and adults: evidence base, novel approaches, and translation into practice. Am Psychol. 2018;73(8):981–993. doi:10.1037/amp0000293
6. Wing RR, Bray GA, Cassidy-Begay M, et al. Effects of intensive lifestyle intervention on all-cause mortality in older adults with type 2 diabetes and overweight/obesity: results from the look AHEAD study. Diabetes Care. 2022;45(5):1252–1259. doi:10.2337/dc21-1805
7. Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145–154.
8. Ryan DH. Drugs for treating obesity. In: Handbook of Experimental Pharmacology. Springer; 2021.
9. CHMP. QSIVA (phentermine/topiramate). 2013; Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/qsiva.
10. Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
11. Pereira MJ, Eriksson JW. Emerging role of SGLT-2 inhibitors for the treatment of obesity. Drugs. 2019;79(3):219–230. doi:10.1007/s40265-019-1057-0
12. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183
13. Müller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metabol. 2019;30:72–130. doi:10.1016/j.molmet.2019.09.010
14. Hinnen D. Glucagon-like peptide 1 receptor agonists for type 2 diabetes. Diabetes Spectr. 2017;30(3):202–210. doi:10.2337/ds16-0026
15. Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971–984. doi:10.1016/S0140-6736(21)00213-0
16. Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA. 2022;327(2):138–150. doi:10.1001/jama.2021.23619
17. PRISMA. PRISMA checklist; 2020. Available from: http://www.prisma-statement.org/PRISMAStatement/Checklist.
18. CRD. CRD’s guidance for undertaking reviews in health care. Centre for Reviews and Dissemination. University of York; 2009. Available from: https://wwwyorkacuk/media/crd/Systematic_Reviewspdf.
19. NICE. Single technology appraisal: user guide for company evidence submission template (PMG24); 2015. Available from: https://wwwniceorguk/process/pmg24/resources/single-technology-appraisal-user-guide-for-company-evidence-submission-template-pdf-72286715419333.
20. Dias S, Welton NJ, Sutton AJ, Ades AE NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials; 2011. Available from: www.nicedsu.org.uk.
21. Dias S, Welton NJ, Sutton AJ, Valdwell DM, Guobing L, Ades AE NICE DSU technical support document 4: inconsistency in networks of evidence based on randomised controlled trials; 2011. Available from: www.nicedsu.org.uk.
22. Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. NICE DSU technical support document 4: inconsistency in networks of evidence based on randomised controlled trials; 2011. Available from: http://www.nicedsu.org.uk.
23. Berne C. A randomized study of orlistat in combination with a weight management programme in obese patients with type 2 diabetes treated with metformin. Diabetic Med. 2005;22(5):612–618. doi:10.1111/j.1464-5491.2004.01474.x
24. Hollander P, Gupta AK, Plodkowski R, et al. Effects of naltrexone sustained-release/bupropion sustained-release combination therapy on body weight and glycemic parameters in overweight and obese patients with type 2 diabetes. Diabetes Care. 2013;36(12):4022–4029. doi:10.2337/dc13-0234
25. Derosa G, Maffioli P, Salvadeo SA, et al. Comparison of orlistat treatment and placebo in obese type 2 diabetic patients. Expert Opin Pharmacother. 2010;11(12):1971–1982. doi:10.1517/14656566.2010.493557
26. Hanefeld M, Sachse G. The effects of orlistat on body weight and glycaemic control in overweight patients with type 2 diabetes: a randomized, placebo-controlled trial. Diabetes Obes Metab. 2002;4(6):415–423. doi:10.1046/j.1463-1326.2002.00237.x
27. Hollander PA, Elbein SC, Hirsch IB, et al. Role of orlistat in the treatment of obese patients with type 2 diabetes. A 1-year randomized double-blind study. Diabetes Care. 1998;21(8):1288–1294. doi:10.2337/diacare.21.8.1288
28. Miles JM, Leiter L, Hollander P, et al. Effect of orlistat in overweight and obese patients with type 2 diabetes treated with metformin. Diabetes Care. 2002;25(7):1123–1128. doi:10.2337/diacare.25.7.1123
29. Garvey WT, Ryan DH, Bohannon NJ, et al. Weight-loss therapy in type 2 diabetes: effects of phentermine and topiramate extended release. Diabetes Care. 2014;37(12):3309–3316. doi:10.2337/dc14-0930
30. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the SCALE diabetes randomized clinical trial. JAMA. 2015;314(7):687–699. doi:10.1001/jama.2015.9676
31. Garvey WT, Birkenfeld AL, Dicker D, et al. Efficacy and safety of liraglutide 3.0 mg in individuals with overweight or obesity and type 2 diabetes treated with basal insulin: the SCALE insulin randomized controlled trial. Diabetes Care. 2020;43(5):1085–1093. doi:10.2337/dc19-1745
32. Lindgärde F. The effect of orlistat on body weight and coronary heart disease risk profile in obese patients: the Swedish Multimorbidity Study. J Intern Med. 2000;248(3):245–254. doi:10.1046/j.1365-2796.2000.00720.x
33. Nissen SE, Wolski KE, Prcela L, et al. Effect of naltrexone-bupropion on major adverse cardiovascular events in overweight and obese patients with cardiovascular risk factors: a randomized clinical trial. JAMA. 2016;315(10):990–1004. doi:10.1001/jama.2016.1558
34. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. 2011;377(9774):1341–1352. doi:10.1016/S0140-6736(11)60205-5
35. Williamson DA. Fifty years of behavioral/lifestyle interventions for overweight and obesity: where have we been and where are we going? Obesity. 2017;25(11):1867–1875. doi:10.1002/oby.21914
36. Wadden TA, Bailey TS, Billings LK, et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive behavioral therapy on body weight in adults with overweight or obesity: the STEP 3 randomized clinical trial. JAMA. 2021;325(14):1403–1413. doi:10.1001/jama.2021.1831
37. Wadden TA, Foreyt JP, Foster GD, et al. Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity. 2011;19(1):110–120. doi:10.1038/oby.2010.147
38. Wadden TA, Walsh OA, Berkowitz RI, et al. Intensive behavioral therapy for obesity combined with liraglutide 3.0 mg: a randomized controlled trial. Obesity. 2019;27(1):75–86. doi:10.1002/oby.22359
39. Wadden TA, Tronieri JS, Sugimoto D, et al. Liraglutide 3.0 mg and Intensive Behavioral Therapy (IBT) for obesity in primary care: the SCALE IBT randomized controlled trial. Obesity. 2020;28(3):529–536. doi:10.1002/oby.22726
40. Poston WS, Reeves RS, Haddock CK, et al. Weight loss in obese Mexican Americans treated for 1-year with orlistat and lifestyle modification. Int J Obes. 2003;27(12):1486–1493. doi:10.1038/sj.ijo.0802439
41. Poston WSC, Haddock CK, Pinkston MM, et al. Evaluation of a primary care-oriented brief counselling intervention for obesity with and without orlistat. J Intern Med. 2006;260(4):388–398. doi:10.1111/j.1365-2796.2006.01702.x
42. Lucas CP, Boldrin MN, Reaven GM. Effect of orlistat added to diet (30% of calories from fat) on plasma lipids, glucose, and insulin in obese patients with hypercholesterolemia. Am J Cardiol. 2003;91(8):961–964. doi:10.1016/S0002-9149(03)00112-7
43. Mathus-Vliegen EMH, van Ierland-van Leeuwen ML, Bennink RJ. Influences of fat restriction and lipase inhibition on gastric emptying in obesity. Int J Obes. 2006;30(8):1203–1210. doi:10.1038/sj.ijo.0803255
44. Karhunen L, Franssila-Kallunki A, Rissanen P, et al. Effect of orlistat treatment on body composition and resting energy expenditure during a two-year weight-reduction programme in obese Finns. Int J Obes Related Metabol Disord. 2000;24(12):1567–1572. doi:10.1038/sj.ijo.0801443
45. Dai H, Alsalhe TA, Chalghaf N, Riccò M, Bragazzi NL, Wu J. The global burden of disease attributable to high body mass index in 195 countries and territories, 1990-2017: an analysis of the Global Burden of Disease Study. PLoS Med. 2020;17(7):e1003198–e1003198. doi:10.1371/journal.pmed.1003198
46. Janssen F, Bardoutsos A, Vidra N. Obesity prevalence in the long-term future in 18 European countries and in the USA. Obes Facts. 2020;13(5):514–527. doi:10.1159/000511023
47. Saxon DR, Iwamoto SJ, Mettenbrink CJ, et al. Antiobesity medication use in 2.2 million adults across eight large health care organizations: 2009–2015. Obesity. 2019;27(12):1975–1981. doi:10.1002/oby.22581
48. Wharton S, Astrup A, Endahl L, et al. Estimating and reporting treatment effects in clinical trials for weight management: using estimands to interpret effects of intercurrent events and missing data. Int J Obes. 2021;45(5):923–933. doi:10.1038/s41366-020-00733-x
49. Schroll JB, Penninga EI, Gøtzsche PC. Assessment of adverse events in protocols, clinical study reports, and published papers of trials of orlistat: a document analysis. PLoS Med. 2016;13(8):e1002101. doi:10.1371/journal.pmed.1002101
50. Cacciottolo TM, Evans K. Research in brief: effective pharmacotherapy for the management of obesity. Clin Med (Northfield Il). 2021;21(5):e517. doi:10.7861/clinmed.2021-0253
51. Gao X, Hua X, Wang X, et al. Efficacy and safety of semaglutide on weight loss in obese or overweight patients without diabetes: a systematic review and meta-analysis of randomized controlled trials. Front Pharmacol. 2022;13. doi:10.3389/fphar.2022.935823
52. Fornes A, Huff J, Pritchard RI, Godfrey M. Once-weekly semaglutide for weight management: a clinical review. J Pharm Technol. 2022;38(4):239–246. doi:10.1177/87551225221092681
53. Li J, He K, Ge J, Li C, Jing Z. Efficacy and safety of the glucagon-like peptide-1 receptor agonist oral semaglutide in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2021;172:108656. doi:10.1016/j.diabres.2021.108656
54. Shi Q, Wang Y, Hao Q, et al. Pharmacotherapy for adults with overweight and obesity: a systematic review and network meta-analysis of randomised controlled trials. Lancet. 2022;399(10321):259–269. doi:10.1016/S0140-6736(21)01640-8
55. Astrup A, Rössner S, Van Gaal L, et al. Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009;374(9701):1606–1616. doi:10.1016/S0140-6736(09)61375-1
56. O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, Phase 2 trial. Lancet. 2018;392(10148):637–649. doi:10.1016/S0140-6736(18)31773-2
57. Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11–22. doi:10.1056/NEJMoa1411892
58. Bakris G, Calhoun D, Egan B, Hellmann C, Dolker M, Kingma I. Orlistat improves blood pressure control in obese subjects with treated but inadequately controlled hypertension. J Hypertens. 2002;20(11):2257–2267. doi:10.1097/00004872-200211000-00026
59. Broom I, Wilding J, Stott P, Myers N. Randomised trial of the effect of orlistat on body weight and cardiovascular disease risk profile in obese patients: UK Multimorbidity Study. Int J Clin Pract. 2002;56(7):494–499.
60. Davidson MH, Hauptman J, DiGirolamo M, et al. Weight control and risk factor reduction in obese subjects treated for 2 years with orlistata randomized controlled trial. JAMA. 1999;281(3):235–242. doi:10.1001/jama.281.3.235
61. Derosa G, Mugellini A, Ciccarelli L, Fogari R. Randomized, double-blind, placebo-controlled comparison of the action of orlistat, fluvastatin, or both an anthropometric measurements, blood pressure, and lipid profile in obese patients with hypercholesterolemia prescribed a standardized diet. Clin Ther. 2003;25(4):1107–1122. doi:10.1016/S0149-2918(03)80070-X
62. Finer N, James WP, Kopelman PG, Lean ME, Williams G. One-year treatment of obesity: a randomized, double-blind, placebo-controlled, multicentre study of orlistat, a gastrointestinal lipase inhibitor. Int J Obes Related Metabol Disord. 2000;24(3):306–313. doi:10.1038/sj.ijo.0801128
63. Hauptman J, Lucas C, Boldrin MN, Collins H, Segal KR. Orlistat in the long-term treatment of obesity in primary care settings. Arch Fam Med. 2000;9(2):160–167. doi:10.1001/archfami.9.2.160
64. Krempf M, Louvet JP, Allanic H, Miloradovich T, Joubert JM, Attali JR. Weight reduction and long-term maintenance after 18 months treatment with orlistat for obesity. Int J Obes. 2003;27(5):591–597. doi:10.1038/sj.ijo.0802281
65. Rössner S, Sjöström L, Noack R, Meinders AE, Noseda G; on behalf of the European Orlistat Obesity Society. Weight loss, weight maintenance, and improved cardiovascular risk factors after 2 years treatment with orlistat for obesity. Obes Res. 2000;8(1):49–61. doi:10.1038/oby.2000.8
66. Sjöström L, Rissanen A, Andersen T, et al. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. Lancet. 1998;352(9123):167–172. doi:10.1016/S0140-6736(97)11509-4
67. Swinburn BA, Carey D, Hills AP, et al. Effect of orlistat on cardiovascular disease risk in obese adults. Diabetes Obes Metab. 2005;7(3):254–262. doi:10.1111/j.1463-1326.2004.00467.x
68. Torgerson JS, Hauptman J, Boldrin MN, Sjöström L. XENical in the Prevention of Diabetes in Obese Subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155–161. doi:10.2337/diacare.27.1.155
69. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595–605. doi:10.1016/S0140-6736(10)60888-4
70. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity. 2013;21(5):935–943. doi:10.1002/oby.20309
71. Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity. 2012;20(2):330–342. doi:10.1038/oby.2011.330
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.