")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Self-Reported Skin Sensation by People Who Have Experienced Containment During COVID-19 Pandemic
Authors Kluger N , Le Floc'h C , Niore M, Delvigne V, Le Dantec G , Taieb C
Received 7 September 2020
Accepted for publication 31 October 2020
Published 9 December 2020 Volume 2020:13 Pages 943—947
DOI https://doi.org/10.2147/CCID.S280310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Nicolas Kluger, 1 Caroline Le Floc’h, 2 Margot Niore, 2 Veronique Delvigne, 2 Guénaële Le Dantec, 2 Charles Taieb 3
1Dermatology, Venereology, Allergology, Skin and Allergies Hospital, University of Helsinki and Helsinki University Central Hospital, Helsinki, Finland; 2Direction Scientifique, Laboratoire La Roche Posay, Levallois Perret, France; 3Patients Priority Department, European Market Maintenance Assessment [EMMA], Fontenay Sous Bois, France
Correspondence: Charles Taieb
European Market Maintenance Assessment [EMMA], 18 Rue de la Renardière, 94120, Fontenay Sous Bois, France
Email [email protected]
Efforts to curb the spread of the new coronavirus (SARS-CoV-2) have led to an unprecedented simultaneous containment of almost two-thirds of the world’s population. The excessive use of hand washing and hand disinfection has been associated with an increased incidence of irritant and allergic contact eczema in health care workers.1 Face masks and headgear worn tightly for prolonged hours are also responsible for various cutaneous conditions, such as contact allergies, irritation, friction dermatitis, abrasions and aggravation of chronic dermatoses.2 Some authors also suspect that chilblains (“COVID toes”), which were widely reported in spring 2020, could be related to the containment rather than to direct SARS-CoV-2 infection.3 In addition, sensitive skin is a frequent condition in Western countries, ranging from 26 to 57% of the population, depending on the country.4 Sensitive skin is defined by the occurrence of unpleasant sensations in response to stimuli that should not normally provoke such sensations. The causative factors of skin sensitivity include physical (heat, cold, wind, or ultraviolet radiation), chemical (cleansers, cosmetics, water, or pollutants), psychological (emotional change or stress), or hormonal (menstrual cycle) factors.4,5
Efforts to curb the spread of the new coronavirus (SARS-CoV-2) have led to an unprecedented simultaneous containment of almost two-thirds of the world’s population. The excessive use of hand washing and hand disinfection has been associated with an increased incidence of irritant and allergic contact eczema in health care workers.1 Face masks and headgear worn tightly for prolonged hours are also responsible for various cutaneous conditions, such as contact allergies, irritation, friction dermatitis, abrasions and aggravation of chronic dermatoses.2 Some authors also suspect that chilblains (“COVID toes”), which were widely reported in spring 2020, could be related to the containment rather than to direct SARS-CoV-2 infection.3 In addition, sensitive skin is a frequent condition in Western countries, ranging from 26 to 57% of the population, depending on the country.4 Sensitive skin is defined by the occurrence of unpleasant sensations in response to stimuli that should not normally provoke such sensations. The causative factors of skin sensitivity include physical (heat, cold, wind, or ultraviolet radiation), chemical (cleansers, cosmetics, water, or pollutants), psychological (emotional change or stress), or hormonal (menstrual cycle) factors.4,5
Perceived consequences of containment on skin conditions have not been addressed to date in large-sized populations and in individuals suffering from sensitive skin. We performed an international online survey on a representative sample of people over 18 years of age from five countries (Brazil, France, Russia, China and the United States). The data collection procedure was identical to that in previous studies.6–9 For each country, a representative sample of the adult general population aged ≥18 years was recruited using a stratified proportional sampling with replacement design. Based on a database with the e-mail addresses of Internet users in each country, who agreed to participate in surveys (Megabase, Kantar Health, New York, NY, USA), fixed quotas of subjects fulfilling predefined sociodemographic criteria were decided. These quotas were based on the following aspects: sex, age, socio-professional status and regional distribution, thereby ensuring accurate representation of the sample population. Proportional quota sampling was used to make the study population representative of each country. Each selected participant was contacted by e-mail. If contact was not achieved, another potential participant with the same characteristics was randomly selected. Each participant agreed to complete a digital questionnaire.
A total of 11,100 individuals (2,000 each in Brazil, France and Russia, 3050 in China and 2050 in the United States) participated between April and May 2020.
We first inquired about socio-demographics, sensitive skin, and self-reported changes observed during containment (dry skin, skin rash, redness, and itching). The second part addressed facial skin sensitivity. The subjects were requested to rate their skin as “very sensitive,” “sensitive,” “slightly sensitive,” or “not sensitive.” Subjects with “sensitive” or “very sensitive” skin were considered to belong to the “sensitive skin” group, and those having “not very sensitive” or “not sensitive at all” skin belonged to the “non sensitive skin” group, as previously published elsewhere.4,10–12
We did not inquire whether respondents had been diagnosed with COVID-19. As this study did not involve any patient contact and was completely anonymous, approval from the ethical review board was not necessary.
A total of 64% (n=7170) of the respondents reported that they complied with the containment procedures (Table 1), ranging from 39% in China to 85.3% in Brazil (Table 2).
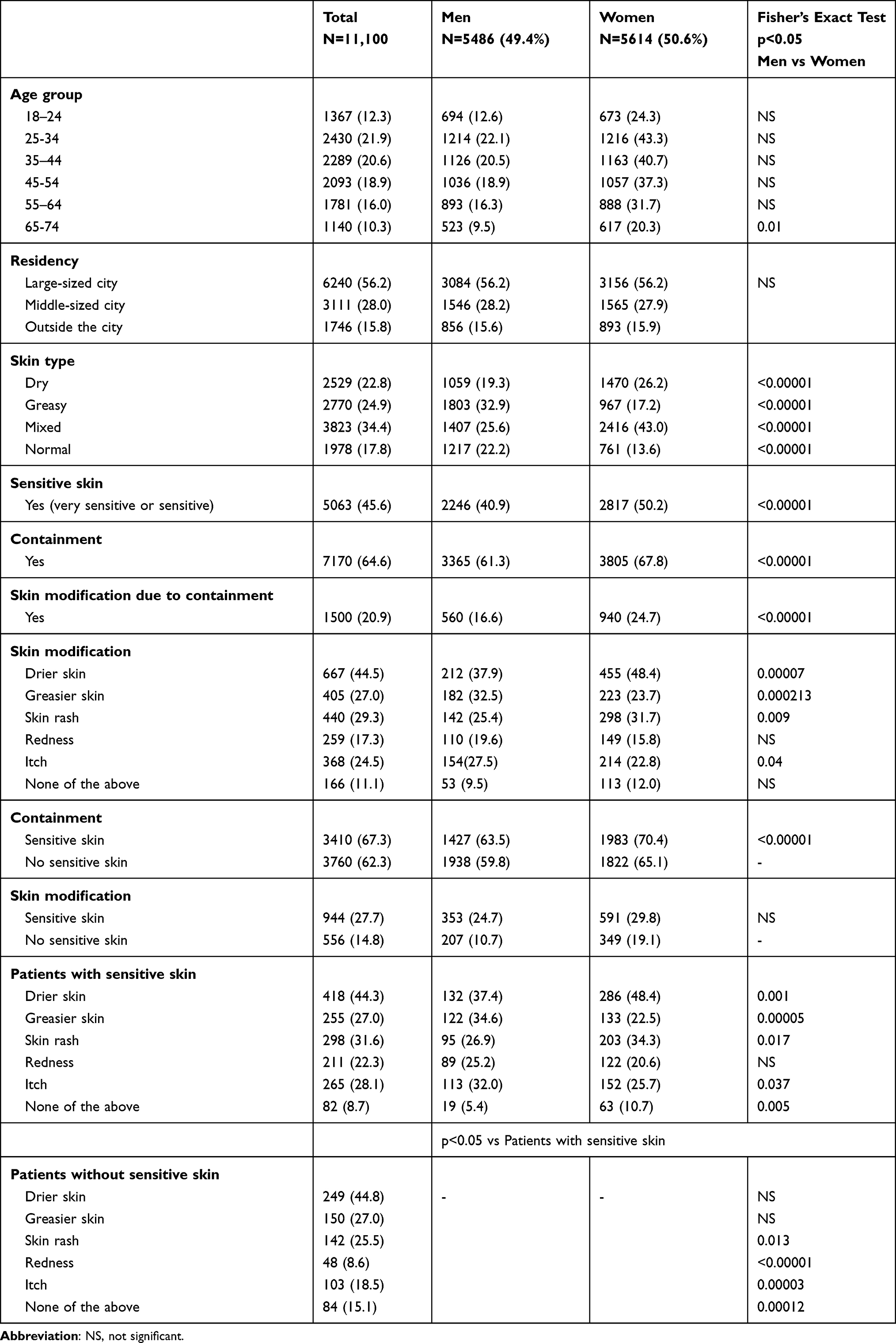 |
Table 1 Characteristics of the Respondents |
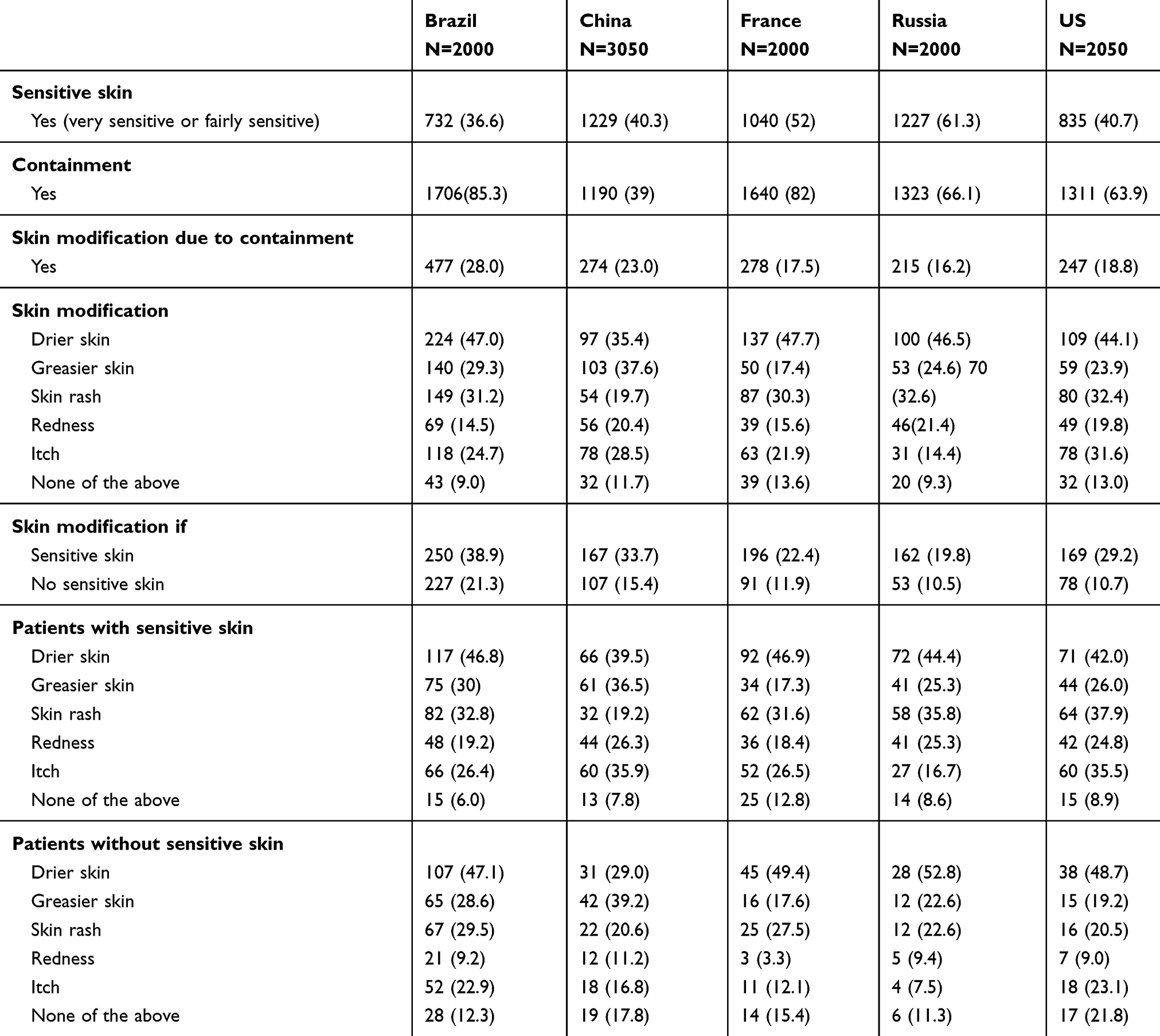 |
Table 2 Detailed Characteristics of the Respondents by Country |
The prevalence of skin changes ranged from 16.2% in Russia to 28% in Brazil. Women were more likely than men to report a change in their skin condition (24.7% vs 16.6%, respectively, p<0.00001). There was a positive correlation between the age and skin complaints (Spearman’s rho r=0.202, p<0.01). Drier skin was the main complaint in all five countries. Overall, the three main reported complaints during containment were drier skin (44.5%), skin rash (29.3%), and greasier skin (27%). Women were more likely than men to report drier skin (48.4% vs 37.9%, respectively, p=0.0007) and skin rash (31.7% vs 25.4%, respectively, p=0.0007).
A total of 40.9% of the men (n=2246) and 50.2% of the women (n=2817) reported having a “sensitive” skin (Table 1). The difference between the 2 sexes was significant (p < 0.001).
Among those, 20.9% (n=1500) reported a modification of their skin in relation to containment.
Patients with sensitive skin were more likely to report skin changes during containment (27.7% vs 14.8%, p<0.00001). The difference was significant for both sexes (p<0.00001). Patients with sensitive skin were more likely to report skin rash, itch and redness (Table 1).
Our study shows that women and individuals who reported sensitive skin perceived that containment was responsible for their subjective skin changes. In the current context, dryness of the skin, exacerbation of pruritus and rashes may be attributed to frequent use of soap and/or hydroalcoholic solutions, as well as to the use of facial masks outside of home.13–15 Stress of containment and uncertainty of the global situation, as well as an exacerbation of preexisting dermatoses, cannot be excluded. Geographic and seasonal climatic variations, as well as the way of life, may also have an impact. The limitations of our study include the declarative nature of the responses. In daily practice, dermatologists must integrate the notion of containment in the anamnesis over the next months as a possible clue to cutaneous symptoms.
Funding
Funding source: La Roche Posay.
Disclosure
Caroline Le Floc'h, Margot Niore, Véronique Delvigne, and Guénaële Le Dantec are Employees of La Roche Posay. The authors report no other potential conflicts of interest for this work.
References
1. Guertler A, Moellhoff N, Schenck TL, et al. Onset of occupational hand eczema among healthcare workers during the SARS-CoV-2 pandemic: comparing a single surgical site with a COVID-19 intensive care unit. Contact Dermatitis. 2020;83(2):108–114. doi:10.1111/cod.13618
2. Bhatia R, Sindhuja T, Bhatia S, et al. Iatrogenic dermatitis in times of COVID-19: a pandemic within a pandemic. J Eur Acad Dermatol Venereol. 2020;34(10):e563–e566. doi:10.1111/jdv.16710
3. Herman A, Peeters C, Verroken A, et al. Evaluation of chilblains as a manifestation of the COVID-19 pandemic. JAMA Dermatol. 2020;156(9):998–1003. doi:10.1001/jamadermatol.2020.2368
4. Kim YR, Cheon HI, Misery L, Taieb C, Lee YW. Sensitive skin in Korean population: an epidemiological approach. Skin Res Technol. 2018;24(2):229–234. doi:10.1111/srt.12418
5. Misery L, Jourdan E, Huet F, et al. Sensitive skin in France: a study on prevalence, relationship with age and skin type and impact on quality of life. J Eur Acad Dermatol Venereol. 2018;32(5):791–795. doi:10.1111/jdv.14837
6. Kluger N, Seité S, Taieb C. The prevalence of tattooing and motivations in five major countries over the world. J Eur Acad Dermatol Venereol. 2019;33(12):e484–e486. doi:10.1111/jdv.15808
7. Kluger N, Misery L, Seité S, Taieb C. Tattooing: a national survey in the general population of France. J Am Acad Dermatol. 2019;81:607–610. doi:10.1016/j.jaad.2018.10.059
8. Kluger N, Misery L, Seité S, Taieb C. Body piercing: a national survey in france. Dermatology. 2019;235:71–78. doi:10.1159/000494350
9. Richard MA, Corgibet F, Beylot-Barry M, et al. Sex- and age-adjusted prevalence estimates of five chronic inflammatory skin diseases in France: results of the “OBJECTIFS PEAU” study. J Eur Acad Dermatol Venereol. 2018;32:1967–1971. doi:10.1111/jdv.14959
10. Brenaut E, Misery L, Taieb C. Sensitive skin in the indian population: an epidemiological approach. Front Med (Lausanne). 2019;6:29. doi:10.3389/fmed.2019.00029
11. Kamide R, Misery L, Perez-Cullell N, Sibaud V, Taïeb C. Sensitive skin evaluation in the Japanese population. J Dermatol. 2013;40(3):177–181. doi:10.1111/1346-8138.12027
12. Taieb C, Auges M, Georgescu V, Perez Cullell N, Miséry L. Sensitive skin in Brazil and Russia: an epidemiological and comparative approach. Eur J Dermatol. 2014;24(3):372–376. doi:10.1684/ejd.2014.2367
13. Lan J, Song Z, Miao X, et al. Skin damage among health care workers managing coronavirus disease-2019. J Am Acad Dermatol. 2020;82(5):1215–1216. doi:10.1016/j.jaad.2020.03.014
14. Szepietowski JC, Matusiak Ł, Szepietowska M, Krajewski PK, Białynicki-Birula R. Face mask-induced itch: a self-questionnaire study of 2,315 responders during the COVID-19 Pandemic. Acta Derm Venereol. 2020;100(10):adv00152. doi:10.2340/00015555-3536
15. Choudhary N. Overzealous hand hygiene during the COVID 19 pandemic causing an increased incidence of hand eczema among general population. J Am Acad Dermatol. 2020;83(1):e37–e41. doi:10.1016/j.jaad.2020.04.047
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.