")
Back to Journals » Clinical Ophthalmology » Volume 13
Self-monitoring of intraocular pressure using Icare HOME tonometry in clinical practice
Authors Cvenkel B , Atanasovska Velkovska M
Received 19 December 2018
Accepted for publication 4 April 2019
Published 10 May 2019 Volume 2019:13 Pages 841—847
DOI https://doi.org/10.2147/OPTH.S198846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Barbara Cvenkel,1,2 Makedonka Atanasovska Velkovska1
1Department of Ophthalmology, University Medical Centre Ljubljana, Ljubljana, Slovenia; 2Medical Faculty, University of Ljubljana, Ljubljana, Slovenia
Purpose: To determine the value of self-monitoring of diurnal intraocular pressure (IOP) by Icare Home rebound tonometer in patients with glaucoma and ocular hypertension.
Methods: Patients with open-angle glaucoma or ocular hypertension, controlled IOP at office visits, and at least 3 years of follow-up in the glaucoma clinic were included. Progression of glaucoma was based on medical records and defined by documented structural and/or visual field change. Patients were trained to correctly perform self-tonometry and instructed to measure diurnal IOP in a home setting for 3 days. IOP characteristics (mean, peak IOP, fluctuation of IOP as range, and SD of IOP) were documented and compared between the progressive and stable eyes.
Results: Ninety-four patients (50 females) with a mean (SD) age of 57.1 (14.7) years were included. Among the 94 eyes from 94 subjects, 72 (76.6%) eyes had primary open-angle glaucoma, ten (10.6%) had pigmentary glaucoma, four (4.3%) had exfoliative glaucoma, and eight (8.5%) eyes had ocular hypertension. Thirty-six eyes showed progression and 58 eyes were stable. Patients with progression were older than those with stable disease (mean (SD) 65.8 (8.4) years vs 51.7 (15.3) years, P<0.001). The progression group had higher average IOP (mean (SD) 15.8 (4.0) mmHg vs 13.3 (3.7) mmHg, P=0.002), peak IOP (mean (SD) 21.8 (5.8) mmHg vs 18.6 (4.8) mmHg, P=0.01), and greater IOP fluctuation range (mean (SD) 11.6 (4.8) vs 9.1 (3.5) mmHg, P=0.011) compared to non-progression group.
Conclusion: Self-monitoring of IOP using Icare Home tonometry provides more complete data on variability of IOP to assist in the management of glaucoma.
Keywords: glaucoma, intraocular pressure, progression, self-tonometry
Introduction
Intraocular pressure (IOP) is an important factor in the management of glaucoma. Lowering of IOP delays the onset and progression of glaucoma and remains the main treatment to maintain visual function.
IOP is usually monitored using Goldmann applanation tonometer (GAT). In the clinical setting, despite the importance of IOP assessment, the efficacy of IOP-lowering treatment is usually based on a few IOP measurements annually. A substantial proportion of patients show progression in visual field defects at apparently controlled IOP. Studies have shown that IOP fluctuates during the day and over longer periods. In one of the first studies, Drance found that the range of diurnal variation in patients with glaucoma was two to three times that of normal individuals, and emphasized that a single office IOP reading may not be representative of the IOP most of the time.1 Later on, several researchers reported that highest IOPs were measured outside office hours and that pressure peaks and higher diurnal fluctuation in patients with controlled office IOP were associated with progression of visual field.2–6 In the literature, there is no consensus which IOP parameter (mean IOP, peak IOP, fluctuation of IOP) is the most important risk factor for glaucoma progression.7,8 IOP variation over time may be divided into diurnal fluctuation measured on a daily basis, short-term fluctuation occurring over days, and long-term fluctuation occurring over months to years. Also, the definition of fluctuation varies across studies. One definition refers to the difference between highest and lowest IOP value over 24 hours or less, or over a certain period.7,9 Many studies define IOP fluctuation as the SD in IOP over time.10–12 Important randomized clinical trials have shown different results about long-term IOP fluctuation as a risk factor for glaucoma progression.13–15 These studies have different study populations, designs, and definitions of IOP fluctuation. Twenty-four hour monitoring of IOP may provide the most accurate measurements.16 However, it is hospital-based, inconvenient, costly, and it is questionable whether pattern of IOP remains similar over the following days, or over longer periods.17,18 Collecting more IOP readings at home has led to development of self-tonometers and continuous pressure measurement devices. At present, continuous monitoring of IOP is not clinically useful to assess treatment response in glaucoma patients.19 Recently, a novel model of self-tonometer, Icare Home rebound tonometer (Icare Finland Oy), has been commercially available for self-use. Compared to its predecessor, Icare One, Icare Home tonometer has EyeSmart eye recognition and EasyPos alignment feature, both of which improve comfort and ease of handling.20 Icare Home tonometer has shown good agreement with GAT and good-to-excellent repeatability.21,22 Topical anesthesia is not required and no adverse ocular surface changes have been noted.23
The purpose of this study was to evaluate diurnal IOP using self-tonometer in patients with open-angle glaucoma and ocular hypertension with at least 3 years follow-up, and to further assess whether there are any differences in IOP parameters (mean IOP, peak IOP, fluctuation of IOP as range, and as SD of IOP) between progressing and stable eyes.
Methods
Participants
Participants were patients with open-angle glaucoma or ocular hypertension attending the Glaucoma Clinic at the Department of Ophthalmology of the University Medical Centre Ljubljana, Slovenia. Patients were recruited from November 2016 until the end of June 2017. Inclusion criteria were: subjects with open-angle glaucoma or ocular hypertension at baseline, ≥3 years of follow-up and controlled IOP at regular examinations. Controlled IOP is eye-specific target IOP and was based on staging of glaucoma at baseline examination and determined from both a percentage reduction (at least 20% from baseline for ocular hypertension and early glaucoma eyes, 30% for eyes with moderate and advanced disease) and an absolute IOP threshold.24 These examinations included slit-lamp exam, standard automated perimetry, dilated ophthalmoscopy every 6 months, and annual photography of optic nerve head. Exclusion criteria were: visual acuity ≤0.1, corneal anomalies (keratopathies, keratoconus, patients with severe dry eye disease, etc), less than 2 months after refractive surgery and those with tremor, arthritis or other disorders affecting self-handling of tonometer. Progression was defined by documented change of the optic nerve head or retinal nerve fiber layer (eg, thinning of rim, disc hemorrhage, appearance or widening of retinal nerve fiber layer defect) or confirmed significant deterioration of the visual field using EyeSuite™ progression analysis function of the Octopus perimeter. For trend analysis, the last six reliable visual fields were selected. The results of the home tonometry readings were not known to the glaucoma specialists at the time they assessed glaucoma progression.
The study was approved by the National Medical Ethics Committee and adhered to the tenets of the Declaration of Helsinki. All participants signed informed consent after a complete explanation of the study.
Procedure
A certified health care professional explained the tonometer, instructed, trained, and supervised all the participants. The subject was deemed able to obtain reliable self-measurements if the following criteria were satisfied:
- the first of the three Icare Home readings taken by the trainer and subject differed 5 mmHg or less.
- The range of the three readings (max-min) taken by the patient was 7 mmHg or less.
- The positioning of the tonometer was correct during self-use, as determined by the trainer.
- They were able to take three reliable self-measurements of each eye in 30 minutes or less from the start of training.
Subjects had to perform self-measurements several times under observation without any intervention by a health care professional. Then they received the Icare Home kit with the instruction to measure IOP at home from 8 am to 8 pm, every 3 hours for 3 days. The tonometer stores information of each complete measurement including the final IOP, date and time of the measurement, identification of the eye (right or left), and the quality of each measurement. The collected data for each subject were copied to the computer via USB cable and opened in the Icare LINK software.
Statistical analysis
Data collected for all participants included age, gender, diagnosis, progression of disease (previously defined), number of eye drops, best corrected visual acuity, refractive error, central corneal thickness, mean defect (Octopus perimeter), average IOP, peak IOP, and IOP fluctuation. Average IOP was the mean value of all self-measurements and peak IOP was the highest value of IOP taken during 3 days of self-use of the device. IOP fluctuation was defined as the difference between the highest and lowest IOP values and as the SD of diurnal IOPs measured over 3 days. IOP data from a randomly selected eye per subject were included. The randomization was done using random number generator with even numbers indicating right eye and odd numbers indicating left eye for statistical analysis. If only one eye fulfilled the inclusion criteria, the data from this eye were analyzed. Values for continuous variables are presented as mean (±SD). Values of variables were tested for normal distribution using the Kolgomorov-Smirnov test. In the case of normal distribution, an Independent t-test was used to compare means between the two groups (progressing vs non-progressing eyes); otherwise Mann-Whitney U test was performed. For all tests, P<0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 22.0 (IBM Corporation, Armonk, NY, USA).
Results
Ninety-four subjects (50 females/44 males) entered the study. The mean age (SD) was 57.1 (14.7) years, range 19–87 years. Females were significantly older than male subjects (mean age (SD) females 63.9 (9.8) years; males 49.3 (15.6) years; P<0.001). Out of the 94 eyes from 94 patients, 72 eyes had primary open-angle glaucoma, ten had pigmentary glaucoma, four had exfoliative glaucoma, and eight eyes had ocular hypertension at baseline. Patients’ characteristics and clinical measurements are presented in Table 1.
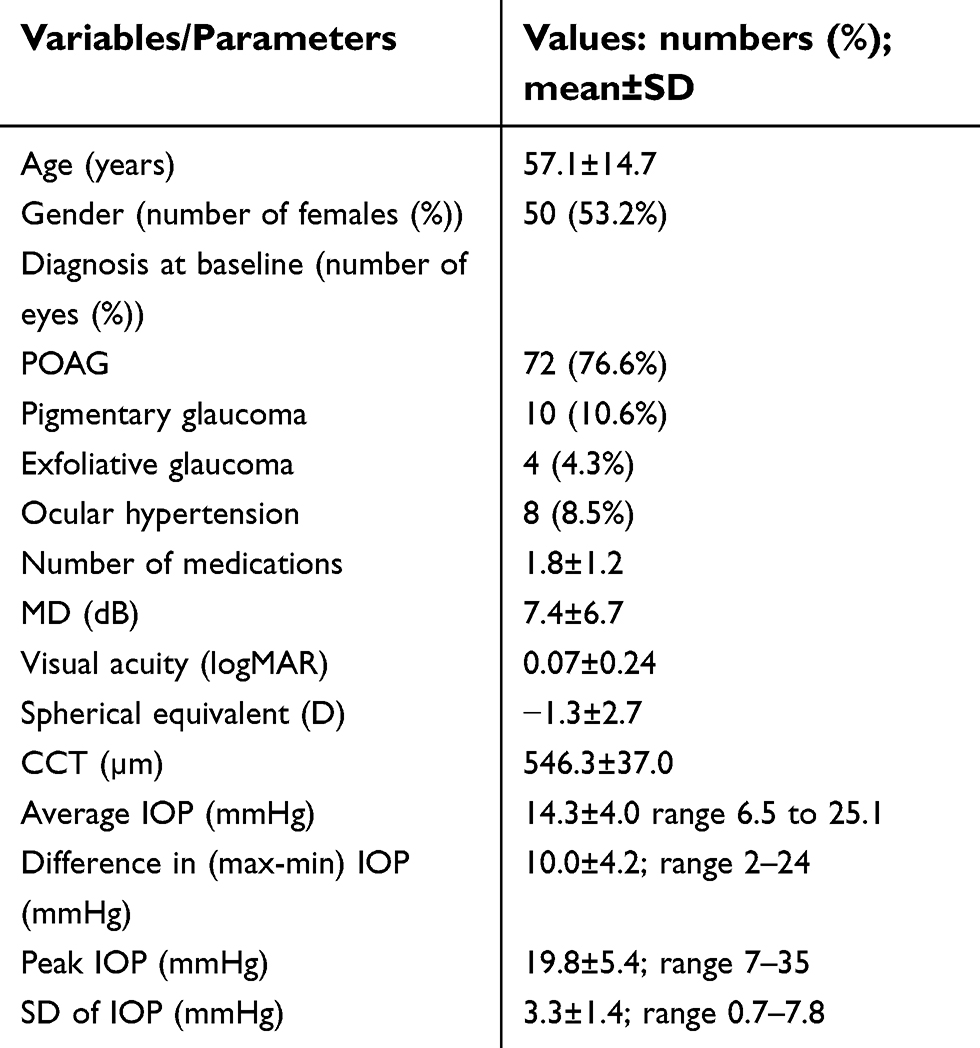 | Table 1 Patients’ characteristics and clinical measurements for 94 eyes from 94 subjects |
Thirty-six eyes showed progression and 58 eyes were stable. Thirty-one out of 72 (43%) eyes progressed in the primary open-angle glaucoma group, two out of ten eyes in the pigmentary glaucoma group, three out of four eyes in the exfoliative glaucoma group, and none of the eight eyes in the ocular hypertension group. Patients with progression were significantly older, with greater proportion of female patients. Eyes that showed progression had significantly higher average IOP, peak IOP, and higher IOP fluctuation expressed as the difference between the highest and lowest IOP value but not as SD of IOP (Table 2).
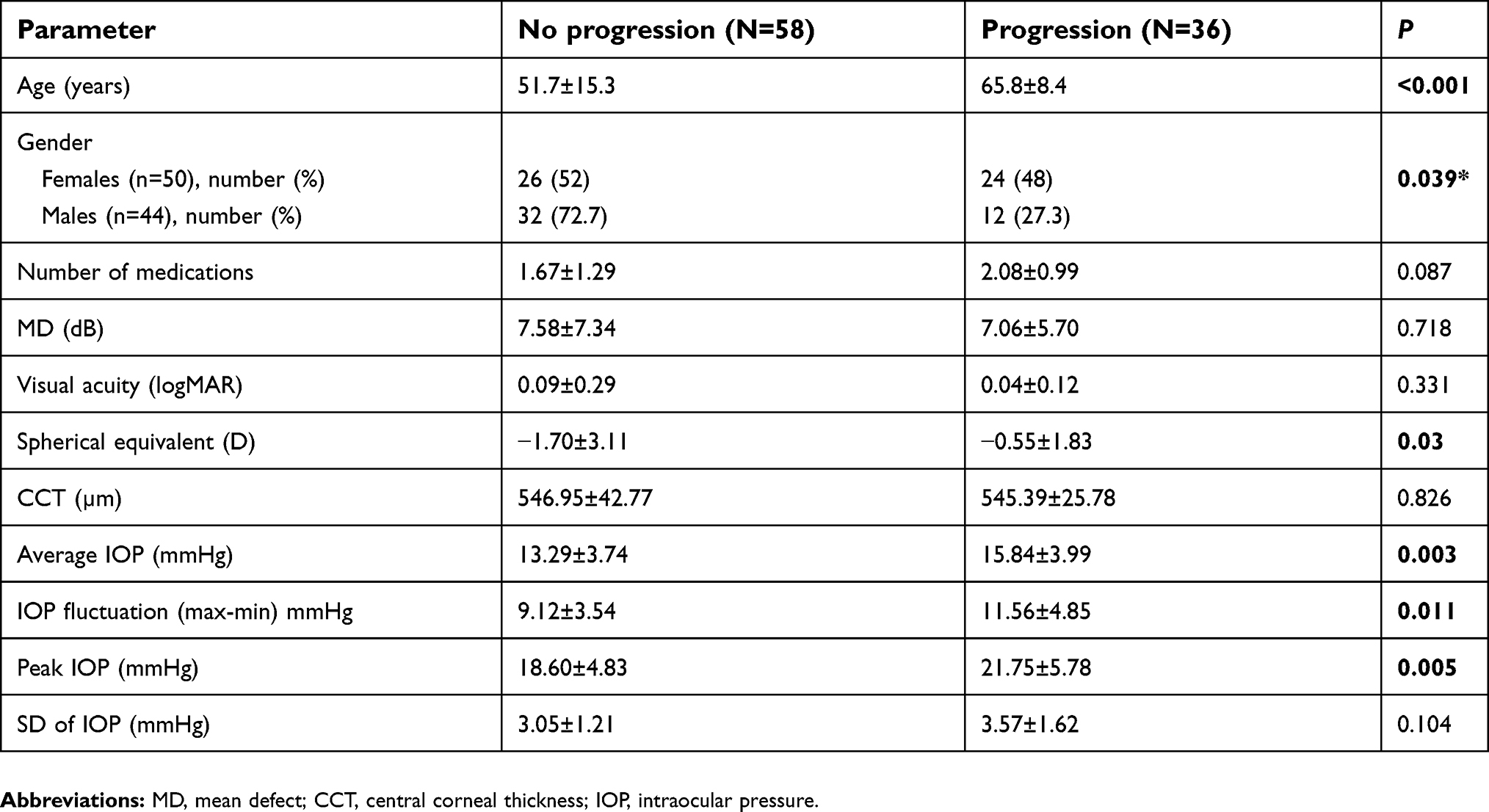 | Table 2 Comparison of stable vs progressing eyes |
Discussion
The current approach is to measure the IOP at routine clinic visits. A single IOP measurement during office visits does not characterize true IOP and many patients progress in this setting. In these patients, 24-hour IOP monitoring, or if not feasible, diurnal IOP curve, can impact glaucoma management. In a busy clinic diurnal phasing is time-consuming and inconvenient for the doctor and the patient.
In our study we evaluated the value of self-tonometry in patients with open angle-glaucoma and ocular hypertension with controlled IOP at office visits for at least 3 years of follow-up. We found that patients with progression were older and had higher diurnal average IOP, peak IOP, and range of IOP fluctuation compared to those with stable disease.
In an early study using a self-tonometer to monitor IOP over several days in patients with glaucoma and controlled office IOP, Wilensky et al2 found that 29% of patients with visual field progression had IOP peaks, compared with 5% of patients with stable visual fields. Later, Asrani et al reported that large diurnal IOP fluctuation detected by self-measurements over 5 days was an independent risk of glaucoma progression in patients with controlled office IOP.5
In studies, short-term IOP characteristics are usually evaluated using 24-hour measurements in a controlled hospital or laboratory environment. Grippo et al25 evaluated 24-hour pattern of IOP in untreated ocular hypertensive (OH) patients in supine position during the night and in sitting and supine position during the day, and showed that OH patients who converted to glaucoma had similar diurnal-to-nocturnal changes in IOP as glaucoma patients, both of which were significantly different from controls. Fogagnolo et al26 evaluated short- and long-term IOP in 52 patients with primary open-angle glaucoma, controlled by topical prostaglandin analogs for at least 1 year. At baseline, 24-hour IOP curve was recorded in hospitalized patients and used to calculate short-term IOP parameters. At follow-up visits, office-hours IOP curves at three office-hours time points were obtained every 6 months for 2 years, and from these 12 IOP measurements, long-term IOP parameters were calculated. Patients with progression in the visual field during the 2-year follow-up, from baseline, showed an increase in the mean IOP, fluctuation of IOP and peak IOP compared to the patients without progression. In the regression analysis, the peak IOP at baseline from the 24-hour phasing was associated with glaucoma progression.
Most studies evaluated IOP parameters over the long term and their impact on progression. Different IOP parameters were associated with visual field progression. Whereas some studies found that eyes with higher IOP fluctuation (SD in IOP) demonstrated greater visual field progression,13,27,28 others reported that mean IOP, but not long-term IOP fluctuation, was associated with glaucoma progression.7,26,29 From a retrospective cohort of 587 eyes of 587 patients, de Moraes et al10 reported that peak IOP was a better predictor of visual field progression than mean IOP or fluctuation.
To address these inconsistencies regarding IOP characteristics as potential factors for glaucoma progression, a reliable method for continuous measurement of IOP is of paramount importance. Such a device should be accurate, reliable, show good agreement with GAT, be safe, user-friendly, and comfortable. Currently, such an ideal device for continuous IOP monitoring is not available. The Sensimed Triggerfish® contact lens sensor is a device designed to provide continuous 24-hour recordings of ocular dimension changes. It does not not measure IOP directly but curvature changes of the limbal cornea which are related to IOP variation and are therefore considered representative of IOP changes.30 Recently, Vitish-Sharma et al31 demonstrated a weak correlation between the Sensimed Triggerfish contact lens sensor data output and IOP measurements taken using the Tonopen XL applanation tonometer.
Self-tonometry in a home setting is a suitable way to collect IOP data. Icare Home self-tonometer was found to be safe, reliable, reproducible, usable by the majority of patients, and demonstrated reasonable agreement with the reference standard GAT. Self-monitoring of IOP can provide more information about IOP characteristics and impact glaucoma management. Sood et al32 reported that 24-hour IOP self-monitoring in patients with NTG with progression revealed higher IOP spikes than those identified during office hours. Following IOP phasing using the rebound self-tonometer, a change in management occurred in 56% of patients. Chen et al33 reported that diurnal IOP pattern taken by Icare One or Icare Home differed between consecutive days in 47% of patients with glaucoma, and IOP peaks outside office hours occurred in up to 16% of the study eyes. Therefore, measurements over several days provided valuable data in adjusting glaucoma treatment and can be used to complement the investigation of patients with glaucoma.
When evaluating our results, there are a number of factors that need to be considered. First, patients with controlled IOP at office visits self-measured diurnal IOP over 3 days and progression was defined retrospectively from medical records. The IOP curves over 3 days may not be representative of the IOP pattern in the preceding years during which visual field and/or structural changes may have occurred. Some studies reported that both healthy subjects and glaucoma patients failed to show repeatable diurnal and circadian IOP pattern over a short period of time,17,34,35 whereas others found no significant differences in diurnal IOP fluctuation on 2 consecutive days.36,37 Second, blood pressure, which is associated with IOP, was not monitored.38,39 Third, the patients’ follow-up was ≥3 years, which is a short period to detect glaucoma progression. However, visual field progression in all subjects was defined by linear trend analysis using the last six reliable visual fields. It has been reported that linear trend analysis on a shorter sequence has improved the ability to detect progression compared to longer sequence, in particular when treatment effect may confound the outcome.40
Obtaining IOP measurements at home may be more representative of true IOP than phasing in hospitalized patients. IOP readings were shown to be consistently lower during hospitalization than after discharge from hospital, which has been assigned to the absence of normal activities.41
For the future, improvements of Icare Home tonometer to enable self-use in a supine position would help to detect nocturnal IOP elevation or patterns of IOP as potential risk factors in individuals for disease progression.
Conclusion
In our study, self-monitoring of IOP in patients with glaucoma progression despite apparently adequate IOP control at office visits, detected higher average mean IOP, peak IOP, and range of IOP fluctuation. This indicates that self-monitoring contributes additional information about IOP characteristics which can be useful in supporting treatment decision, as well as in IOP monitoring following treatment change.
Acknowledgments
The abstract of this paper was presented at the 13th EGS Congress of the European Glaucoma Society, May 19–22, 2018, in Florence, Italy. The poster’s abstract was published in the abstract book available online at: https://www.egs2018.org/sites/www.egs2018.org/files/documenti/egs2018-abstract-book.pdf.
Disclosure
Barbara Cvenkel reports nonfinancial support from Icare Finland Oy, and personal fees from Thea, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Drance SM. Diurnal variation of intraocular pressure in treated glaucoma. Significance in patients with chronic simple glaucoma. Arch Ophthalmol. 1963;70:302–311.
2. Wilensky JT, Gieser DK, Mori MT, Langenberg PW, Zeimer RC. Self-tonometry to manage patients with glaucoma and apparently controlled intraocular pressure. Arch Ophthalmol. 1987;105(8):1072–1075.
3. Hughes E, Spry P, Diamond J. 24 hr monitoring of intraocular pressure in glaucoma management: a retrospective review. J Glaucoma. 2003;12(3):232–236. doi:10.1097/00061198-200306000-00009
4. Zeimer RC, Wilensky JT, Gieser DK, Viana MA. Association between intraocular pressure peaks and progression of visual field loss. Ophthalmology. 1991;98(1):64–69.
5. Asrani S, Zeimer R, Wilensky J, Gieser D, Vitale S, Lindenmuth K. Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma. J Glaucoma. 2000;9(2):134–142.
6. Barkana Y, Anis S, Liebmann J, Tello C, Ritch R. Clinical utility of intraocular pressure monitoring outside of normal office hours in patients with glaucoma. Arch Ophthalmol. 2006;124(6):793–797. doi:10.1001/archopht.124.6.793
7. Bengtsson B, Heijl A. Diurnal IOP fluctuation: not an independent risk factor for glaucomatous visual field loss in high-risk ocular hypertension. Graefe‘S Arch Clin Exp Phthalmol. 2005;243(6):513–518. doi:10.1007/s00417-004-1103-8
8. Kim SH, Lee EJ, Han JC, Sohn SW, Rhee T, Kee C. The effect of diurnal fluctuation in intraocular pressure on the evaluation of risk factors of progression in normal tension glaucoma. PLoS One. 2016;11(10):e0164876. doi:10.1371/journal.pone.0164876
9. Lee PP, Sultan MB, Grunden JW, Cioffi GA, Panel IOPC. Assessing the importance of IOP variables in glaucoma using a modified delphi process. J Glaucoma. 2010;19(5):281–287. doi:10.1097/IJG.0b013e3181b4ca8d
10. De Moraes CG, Juthani VJ, Liebmann JM, et al. Risk factors for visual field progression in treated glaucoma. Arch Ophthalmol. 2011;129(5):562–568. doi:10.1001/archophthalmol.2011.72
11. Jonas JB, Budde WM, Stroux A, Oberacher-Velten IM, Junemann A. Diurnal intraocular pressure profiles and progression of chronic open-angle glaucoma. Eye. 2007;21(7):948–951. doi:10.1038/sj.eye.6702351
12. Fujino Y, Asaoka R, Murata H, et al. Evaluation of glaucoma progression in large-scale clinical data: the Japanese Archive of Multicentral Databases in Glaucoma (JAMDIG). Invest Ophthalmol Vis Sci. 2016;57(4):2012–2020. doi:10.1167/iovs.15-19046
13. Nouri-Mahdavi K, Hoffman D, Coleman AL, et al. Predictive factors for glaucomatous visual field progression in the Advanced Glaucoma Intervention Study. Ophthalmology. 2004;111(9):1627–1635. doi:10.1016/j.ophtha.2004.02.017
14. Bengtsson B, Leske MC, Hyman L, Heijl A. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology. 2007;114(2):205–209. doi:10.1016/j.ophtha.2006.07.060
15. Miglior S, Torri V, Zeyen T, et al. Intercurrent factors associated with the development of open-angle glaucoma in the European glaucoma prevention study. Am J Ophthalmol. 2007;144(2):266–275. doi:10.1016/j.ajo.2007.04.040
16. Fogagnolo P, Orzalesi N, Ferreras A, Rossetti L. The circadian curve of intraocular pressure: can we estimate its characteristics during office hours? Invest Ophthalmol Vis Sci. 2009;50(5):2209–2215. doi:10.1167/iovs.08-2889
17. Realini T, Weinreb RN, Wisniewski S. Short-term repeatability of diurnal intraocular pressure patterns in glaucomatous individuals. Ophthalmology. 2011;118(1):47–51. doi:10.1016/j.ophtha.2010.04.027
18. Hatanaka M, Babic M, Susanna R
19. Hollo G, Kothy P, Vargha P. Evaluation of continuous 24 hr intraocular pressure monitoring for assessment of prostaglandin-induced pressure reduction in glaucoma. J Glaucoma. 2014;23(1):e6–e12. doi:10.1097/IJG.0b013e31829e5635
20. Mihailovic N, Termuhlen J, Alnawaiseh M, Eter N, Dietlein TS, Rosentreter A. Ease of handling of first and second generation rebound tonometers. Ophthalmologe. 2016;113(4):314–320. doi:10.1007/s00347-015-0153-0
21. Pronin S, Brown L, Megaw R, Tatham AJ. Measurement of intraocular pressure by patients with glaucoma. JAMA Ophthalmol. 2017;135:1030. doi:10.1001/jamaophthalmol.2017.3151
22. Noguchi A, Nakakura S, Fujio Y, et al. A pilot evaluation assessing the ease of use and accuracy of the new self/home-tonometer IcareHOME in healthy young subjects. J Glaucoma. 2016;25:835–841. doi:10.1097/IJG.0000000000000457
23. Mudie LI, LaBarre S, Varadaraj V, et al. The Icare HOME (TA022) study: performance of an intraocular pressure measuring device for self-tonometry by glaucoma patients. Ophthalmology. 2016;123:1675–1684. doi:10.1016/j.ophtha.2016.04.044
24. Damji KF, Behki R, Wang L;
25. Grippo TM, Liu JH, Zebardast N, Arnold TB, Moore GH, Weinreb RN. Twenty-four-hour pattern of intraocular pressure in untreated patients with ocular hypertension. Invest Ophthalmol Vis Sci. 2013;54(1):512–517. doi:10.1167/iovs.12-10709
26. Fogagnolo P, Orzalesi N, Centofanti M, Oddone F, Manni G, Rossetti L. Short- and long-term phasing of intraocular pressure in stable and progressive glaucoma. Ophthalmologica J Int D‘Ophtalmologie Int J Ophthalmol Z Augenheilkunde. 2013;230(2):87–92. doi:10.1159/000351647
27. Hong S, Seong GJ, Hong YJ. Long-term intraocular pressure fluctuation and progressive visual field deterioration in patients with glaucoma and low intraocular pressures after a triple procedure. Arch Ophthalmol. 2007;125(8):1010–1013. doi:10.1001/archopht.125.8.1010
28. Rao HL, Addepalli UK, Jonnadula GB, Kumbar T, Senthil S, Garudadri CS. Relationship between intraocular pressure and rate of visual field progression in treated glaucoma. J Glaucoma. 2013;22(9):719–724. doi:10.1097/IJG.0b013e318259b0c2
29. Bengtsson B, Leske MC, Hyman L, Heijl A.
30. Mansouri K, Shaarawy T. Continuous intraocular pressure monitoring with a wireless ocular telemetry sensor: initial clinical experience in patients with open angle glaucoma. Br J Ophthalmol. 2011;95(5):627–629. doi:10.1136/bjo.2010.192922
31. Vitish-Sharma P, Acheson AG, Stead R, et al. Can the SENSIMED Triggerfish((R)) lens data be used as an accurate measure of intraocular pressure? Acta Ophthalmol (Copenh). 2018;96(2):e242–e246. doi:10.1111/aos.13801
32. Sood V, Ramanathan US. Self-monitoring of intraocular pressure outside of normal office hours using rebound tonometry: initial clinical experience in patients with normal tension glaucoma. J Glaucoma. 2016;25:807–811. doi:10.1097/IJG.0000000000000424
33. Chen E, Querat L, Akerstedt C. Self-tonometry as a complement in the investigation of glaucoma patients. Acta Ophthalmol (Copenh). 2016;94(8):788–792. doi:10.1111/aos.13129
34. Song YK, Lee CK, Kim J, Hong S, Kim CY, Seong GJ. Instability of 24 hr intraocular pressure fluctuation in healthy young subjects: a prospective, cross-sectional study. BMC Ophthalmol. 2014;14:127. doi:10.1186/1471-2415-14-127
35. Xu S, Jiao Q, Cheng Y, Sun J, Lu Q, Zhong Y. Short-term reproducibility of twenty-four-hour intraocular pressure curves in untreated patients with primary open-angle glaucoma and ocular hypertension. PLoS One. 2015;10(10):e0140206. doi:10.1371/journal.pone.0140206
36. Ido T, Tomita G, Kitazawa Y. Diurnal variation of intraocular pressure of normal-tension glaucoma. Influence of sleep and arousal. Ophthalmology. 1991;98(3):296–300.
37. Gao Y, Wan B, Li P, Zhang Y, Tang X. Short-term reproducibility of intraocular pressure and ocular perfusion pressure measurements in Chinese volunteers and glaucoma patients. BMC Ophthalmol. 2016;16:145. doi:10.1186/s12886-016-0323-0
38. Fuchsjager-Mayrl G, Wally B, Georgopoulos M, et al. Ocular blood flow and systemic blood pressure in patients with primary open-angle glaucoma and ocular hypertension. Invest Ophthalmol Vis Sci. 2004;45(3):834–839. doi:10.1167/iovs.03-0461
39. Zhao D, Cho J, Kim MH, Guallar E. The association of blood pressure and primary open-angle glaucoma: a meta-analysis. Am J Ophthalmol. 2014;158(3):615–627 e619. doi:10.1016/j.ajo.2014.05.029
40. Gardiner SK, Demirel S, De Moraes CG, et al. Series length used during trend analysis affects sensitivity to changes in progression rate in the ocular hypertension treatment study. Invest Ophthalmol Vis Sci. 2013;54(2):1252–1259. doi:10.1167/iovs.12-10218
41. Hyams SW, Bergman D, Keroub C. The effect of hospitalization on intraocular pressure. Am J Ophthalmol. 1982;94(4):519–521.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.