")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 11
Self-management and associated factors among patients with end-stage renal disease undergoing hemodialysis at health facilities in Addis Ababa, Ethiopia
Authors Gela D , Mengistu D
Received 21 August 2018
Accepted for publication 24 October 2018
Published 27 November 2018 Volume 2018:11 Pages 329—336
DOI https://doi.org/10.2147/IJNRD.S184671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Debela Gela, Daniel Mengistu
School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
Introduction: Patients with end-stage renal disease (ESRD) face multifaceted problems arising from complications of the disease and dialysis that require consistent and, effective self-management from the patients’ side, on top of the management offered by health care professionals. However, little is known about the level of self-management and influencing factors among patients with ESRD undergoing hemodialysis in the study area. Therefore, the aim of this study was to assess self-management and associated factors of patients with ESRD undergoing hemodialysis at health facilities in Addis Ababa, Ethiopia.
Methods: An institution-based cross-sectional survey was used to recruit 169 patients with ESRD undergoing hemodialysis from six private health facilities between March and April 2016. Data were collected using an interviewer-administered structured questionnaire inquiring about patients’ self-management and associated factors. Data were entered into EpiData Version 3.1 and analyzed using the descriptive, correlation, and logistic regression using the SPSS Version 22.0 statistical software.
Results: The mean age of the patients was 49.86±15.58 years. The majority of the respondents (69.8%) were male, and 65.7% of them were married. Half of the respondents (50.3%) had diploma and above educational level. The great majority of the respondents (93.5%) were on hemodialysis for less than 5 years, and 53.3% of them underwent dialysis twice a week. More than half (57.4%) of the patients had low levels of self-management. There were statistically significant positive associations between self-management and education (adjusted OR [AOR] =6.25, 95% CI =1.40, 27.85), knowledge (AOR =5.5, 95% CI =2.15, 14.03), and self-efficacy (AOR =4.73, 95% CI =1.95, 11.48), while there were statistically significant negative associations between self-management and anxiety (AOR =3.19, 95% CI =1.28, 7.95) and depression (AOR =2.68, 95% CI =1.01, 7.05, P<0.05).
Conclusion: Patients’ education, knowledge, self-efficacy, anxiety, and depression were found to be independent predictors of self-management.
Keywords: self-management, self-efficacy, knowledge, hemodialysis, end-stage renal disease, Ethiopia
Introduction
End-stage renal disease (ESRD) is a complex chronic disease. Contributing to the mortality associated with ESRD are the comorbidities such as hypertension, diabetes, anemia, and heart failure that accompany this renal disease. It also associated with compromised quality of life and unintended hospitalization with a high burden of disease.1–4 Globally, the number of patients being treated for ESRD was estimated to be more than 2.7 million by the end of 2011 with a 6–7% growth rate. The prevalence of ESRD is the highest in Taiwan, followed by Japan and then USA.5 The lack of working registries in most of the sub-Saharan Africa, including Ethiopia, has resulted in an absence of reliable statistics, but there is a general impression that chronic kidney disease (CKD) is at least three to four times more frequent than developed countries.6,7
Maintenance hemodialysis (MHD) is the most common therapy for ESRD. Globally, of the 2.7 million ESRD patients, approximately above 2 million were undergoing dialysis treatment (hemodialysis or peritoneal dialysis).5 The dialysis treatment rate in Africa ranges from 70 per million population (pmp) in South Africa to 20 pmp in most of sub-Saharan Africa.6
Ethiopia’s health service is structured into a three-tier system: primary, secondary, and tertiary levels of care. The primary level of care includes primary hospitals, health centers, and health posts. The secondary and tertiary levels comprised general and specialized hospitals. Hemodialysis services for patients with ESRD are given at the tertiary level health care (specialized hospital).8,9 In Ethiopia, dialysis as a treatment modality of ESRD is extremely scarce and unaffordable to the majority of the patients. Study on MHD in Ethiopia shows that survival pattern in those on the treatment is less satisfactory. Forty-five percentage of deaths occurred during dialysis treatment, 23% of them died within the first 90 days of starting dialysis, and only 42% of them survived longer than a year. The frequently reported causes of death were septicemia (34%) and cardiovascular complication (29%).10
Patients with ESRD face multifaceted problems arising from the complications of disease and dialysis that require a consistent, effective self-management from the patients’ side. Studies have demonstrated that improving the level of self-management of patients with ESRD undergoing hemodialysis is an effective way to reduce the incidence of mortality and complications and improve the quality of life.1,2,11,12 Self-management is defined as “the ability of individual’s to manage the symptoms, treatment, lifestyle changes and physical and psychosocial consequences of health conditions (particularly chronic diseases).”12,13 Hemodialysis requires essential lifestyle changes such as consistent attendance at a dialysis unit for treatment and restriction of fluid intake and diet and taking medications.2,14 These lifestyle changes are strongly influenced by increasing self-management.
Nevertheless, many patients face challenges in implementing the recommended hemodialysis self-management. A multitude of factors may affect the self-management of patients with ESRD undergoing hemodialysis. These may include sociodemographic factors such as age, sex, marital status, and educational status2,7,15,16 and disease-related factors such as duration and frequency of hemodialysis and complications,2,17 hemodialysis knowledge,2,18–22 self-efficacy,2,17,19,22–24 psychological status (anxiety and depression),2,18–20,25,26 and social support.2,18,26,27 However, little known about the self-management of patients with ESRD undergoing hemodialysis in Ethiopia. Therefore, the aim of this study was to assess self-management and associated factors among patients with ESRD undergoing hemodialysis at health facilities in Addis Ababa, Ethiopia.
This study was informed by the Self-Management Model, which is used as a framework for identifying and explaining patterns among factors that influence the ability of individual’s to manage the symptoms, treatment, lifestyle changes, and physical and psychosocial consequences of health conditions.12 Self-Management Model proposes that demographics, knowledge, self-efficacy, psychological health status, and social support influence individual’s self-management. The association between these variables and self-management of patients with ESRD undergoing hemodialysis was analyzed in this study.
Methods
Study design, setting, and population
This is an institution-based cross-sectional survey conducted among patients with ESRD undergoing hemodialysis from six private health facilities in Addis Ababa, Ethiopia. The total number of patients on hemodialysis served by these health facilities was 178. Since the number of patients in these health facilities was small, all of them were included in the study using census method. Data were collected for a total duration of 1 month from March to April 2016. Ethical approval for the study was obtained from an Institutional Review Board (IRB) of the College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia (protocol number: 094/Nurse). Permission to conduct the research was obtained from the authorities in the study settings, written informed consents were secured from each participant, and the study was conducted in accordance with the Declaration of Helsinki.
Of the 178 patients, 169 patients were consented and recruited from these health facilities making the response rate of 95%. All patients with ESRD undergoing hemodialysis who fulfill the inclusion criteria were included in the study. We included all patients with ESRD undergoing hemodialysis routinely for at least 3 months, aged 18 years or older, and willing to participate. Patients with ESRD undergoing hemodialysis who were reported psychological disorders (acute or chronic psychosis, documented depression) and physical limitations in self-care were excluded from the study, as these factors could potentially affect their self-management.
Data were collected in local languages – Amharic languages using interviewer-administered questionnaire. The interview was taken for 25–30 minutes. Before data collection, we took measures to ensure meaning equivalence between the original English version of the questionnaire and the version in local languages. In this regard, the questionnaire was translated from English to Amharic language by a bilingual translator and then back translated to English by another bilingual translator. Four nurses holding Bachelor of Science degree were involved in data collection under the supervision of a senior nurse professional and were also followed up by the principal investigator in order to ensure the quality of the data collected.
Measurements
Demographic characteristics such as age, sex, marital status, education, and disease-related factors such as duration on hemodialysis, frequency of hemodialysis, and complication were collected using seven structured items. The hemodialysis self-management instrument (HDSMI) was used to measure the level of self-management. The scale contains 20 items, which are divided into the following four subscales: problem solving, emotional management, self-care, and partnership. Participants were asked to give responses to each item on 4-point scale ranging from never (1) to always (4). The scores ranged from 20 to 80, with the higher score above the mean indicating a higher level of self-management. The internal consistency reliability of the scale was 0.81.2 The internal consistency of the measure was 0.81 (a) in this study.
The hemodialysis knowledge questionnaire was used to measure the knowledge of hemodialysis. It contains 16 items. Responses were scored correct (1) or incorrect (0). The scores ranged from 0 to 16. Participants who scored above the mean in the hemodialysis knowledge questionnaire were classified as having knowledge about hemodialysis. The version has internal consistency (a=0.77).28 The internal consistency of the measure was 0.74 (a) in this study.
The six-item Chronic Disease Self-Efficacy Scale was used to measure self-efficacy. Participants were asked to give responses to each item on a 10-point scale ranging from not at all confident (1) to totally confident (10). The scores ranged from 10 to 60, with the scores above the mean indicating having self-efficacy. The reported retest reliability estimate was 0.91.29 The internal consistency of the measure was 0.94 (a) in this study.
The Hospital Anxiety and Depression Scale (HADS) was used to measure anxiety and depression.30 The scale has seven anxiety and depression item subscales. Participants were asked to give responses to each item on a 4-point scale ranging from not at all (0) to most of the time (3). The scores range from 0 to 21 for both anxiety and depression, with the scores above the mean indicating the existence of anxiety and depression. The internal consistency of HADS-Anxiety was 0.83, and that of HADS-Depression was 0.82.31 The internal consistency of the HADS-Anxiety was 0.89, and that of HADS-Depression was 0.73 in this study.
The 12-item Multidimensional Scale of Perceived Social Support (MSPSS) was used to measure perceived social support.32 Items were scored on a 5-point Likert scale ranging from strongly disagree (1) to strongly agree (5). The score range is 12–60, with the scores above the mean indicating having social support. In reliability analysis, the internal consistency was 0.78.33 The internal consistency of the measure was 0.93 (a) in this study. We used sociodemographic data, knowledge, self-efficacy, anxiety, depression, and social support as independent variables and self-management as the dependent variable.
Data processing and analysis
Data were entered and cleaned using EpiData Version 3.1 and then transported to SPSS Version 22.0 for analysis. Descriptive statistics was calculated to describe the characteristics of the participants and the measured variables. Mean with SD and percentage were used to present the descriptive statistics. Pearson’s correlation was computed to explore the bivariate correlation between hemodialysis self-management scores and hemodialysis knowledge, self-efficacy, anxiety, depression, and social support scores. In logistic regression analysis, we have dichotomized the HDSMI score as follows: higher level of self-management for a score above the mean and lower level of self-management for a score below the mean. We have also used the same procedure to dichotomize the hemodialysis knowledge, self-efficacy, HADS-Anxiety and -Depression, and MSPSS scores. We have used the dichotomized scores of the HDSMI, the hemodialysis knowledge, self-efficacy, HADS-Anxiety and -Depression, and MSPSS for the logistic regression analysis, with the dichotomization based on their mean values. The mean values were used to dichotomize these variables as data were normally distributed. The sociodemographic variables such as age, sex, marital status, education, and disease-related factors such as duration on hemodialysis, frequency of hemodialysis and complications, knowledge, self-efficacy, anxiety, depression, and social support associations with self-management were analyzed first by using the simple logistic regression model. Then, only those variables with P-value less than or equal to 0.2 were taken as candidate for multiple logistic regression analysis. In both simple and multiple regression models, the statistical significance of associations between variables were determined using ORs with 95% CI and P<0.05.
Results
Participants’ characteristics
Table 1 shows that the participants’ mean age was 49.8±15.58 years, the majority were between 40 and 59 years (n=64, 37.9%), male (n=118, 69.8%), and married (n=111, 65.7%) and had diploma and above educational level (n=85, 50.3%). From the total participants, 158 (93.5%) participants were on hemodialysis for less than 5 years and above half, 90 (53.3%) of them underwent dialysis twice a week. The majority of the patients with ESRD had complications, such as anemia, 138 (81.7%), and heart failure, 126 (74.6%). Table 1 also shows the disaggregated mean scores of the HDSMI.
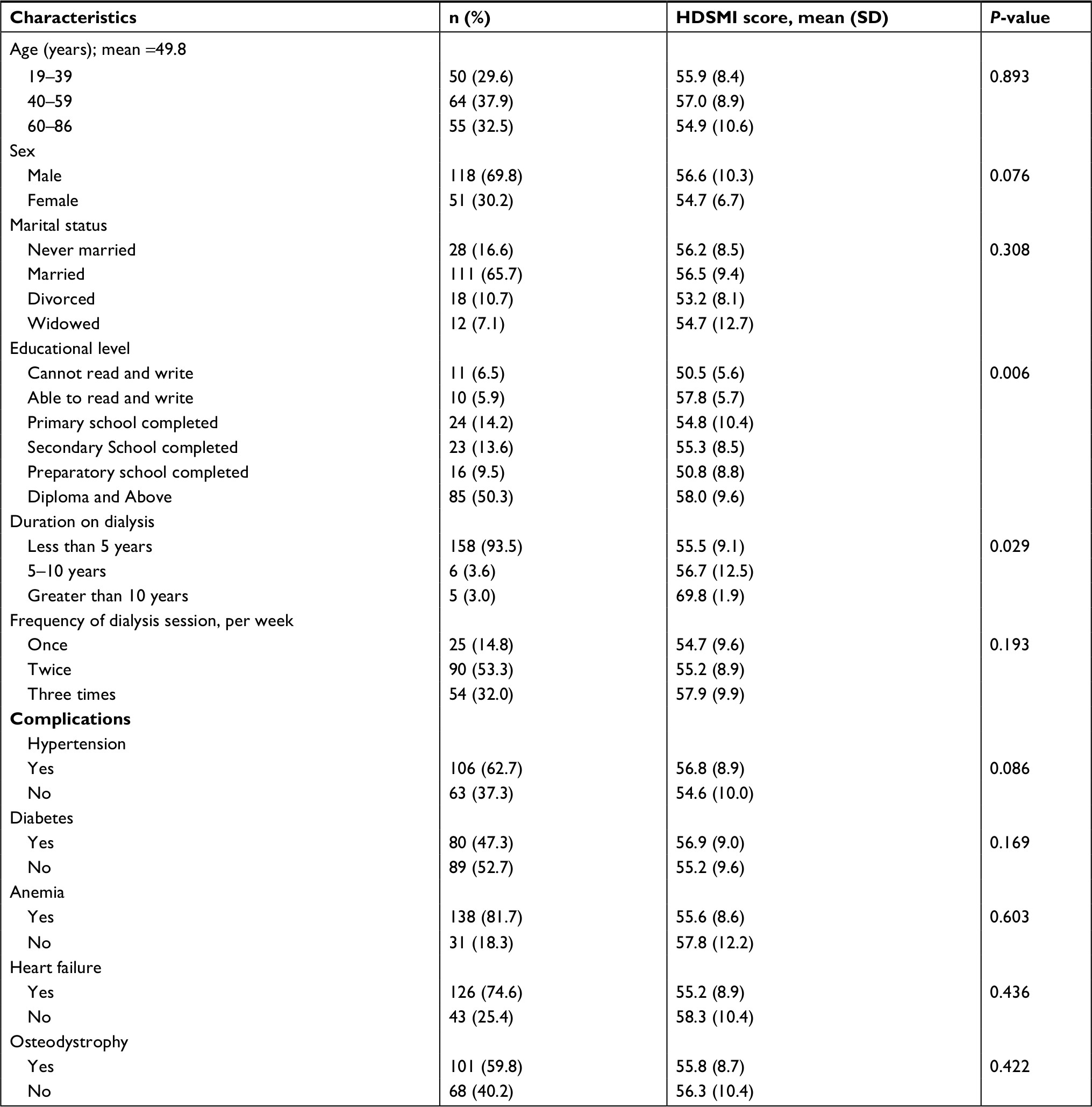 | Table 1 Sociodemographic characteristics of the patients (N=169) Abbreviation: HDSMI, hemodialysis self-management instrument. |
Hemodialysis self-management and correlations
As presented in Table 2, the overall mean score for hemodialysis self-management was 56±9.36. From the total participants, more than half (57.4%) scored below the mean on the HDSMI, indicating lower level of self-management. In contrast, 65.7, 51.5, 52.1, 42.0, and 63.9% scored above the mean on hemodialysis knowledge, self-efficacy, anxiety, depression, and social support scales, respectively.
 | Table 2 Mean scores and correlation coefficients for hemodialysis self-management, hemodialysis knowledge, self-efficacy, anxiety, depression, and social support (N=169) Notes: *P-value <0.05 (two tailed). **P-value <0.01 (two tailed). |
Table 2 also presents the correlation coefficient between hemodialysis self-management and hemodialysis knowledge, self-efficacy, anxiety, depression, and social support. Hemodialysis knowledge, self-efficacy, and social support were positively correlated with hemodialysis self-management (P-value <0.01). However, both anxiety (P-value <0.05) and depression (P-value <0.01) were negatively correlated with hemodialysis self-management.
Factors associated with hemodialysis self-management
In the simple logistic regression analysis, sociodemographic factors (sex and education level), knowledge, self-efficacy, anxiety, depression, and social support had statistically significant association with hemodialysis self-management, while age, duration of dialysis treatment, frequency of dialysis, and comorbidities did not have association with hemodialysis self-management. However, in multiple logistic regression analysis, only education level, knowledge, self-efficacy, anxiety, and depression had statistically significant association with hemodialysis self-management (Table 3). Participants who completed preparatory school were 6.25 more likely to report lower self-management levels compared to those who had diplomas and above (AOR =6.25, 95% CI =1.40, 27.85, P-value <0.05). Participants who did not have knowledge about hemodialysis were 5.5 more likely to report lower self-management levels compared to those who had knowledge (AOR =5.50, 95% CI =2.15, 14.03, P-value<0.001). Participants who did not have self-efficacy were 4.73 more likely to report lower self-management levels compared to those who had self-efficacy (AOR =4.73, 95% CI =1.95, 11.48, P-value<0.001). Finally, participants who had anxiety and depression were 3.19 and 2.68 more likely to report lower self-management levels compared to those who did not have anxiety (AOR =3.19, 95% CI =1.28, 7.95, P-value <0.05) and depression (AOR =2.68, 95% CI =1.01, 7.05, P-value <0.05), respectively.
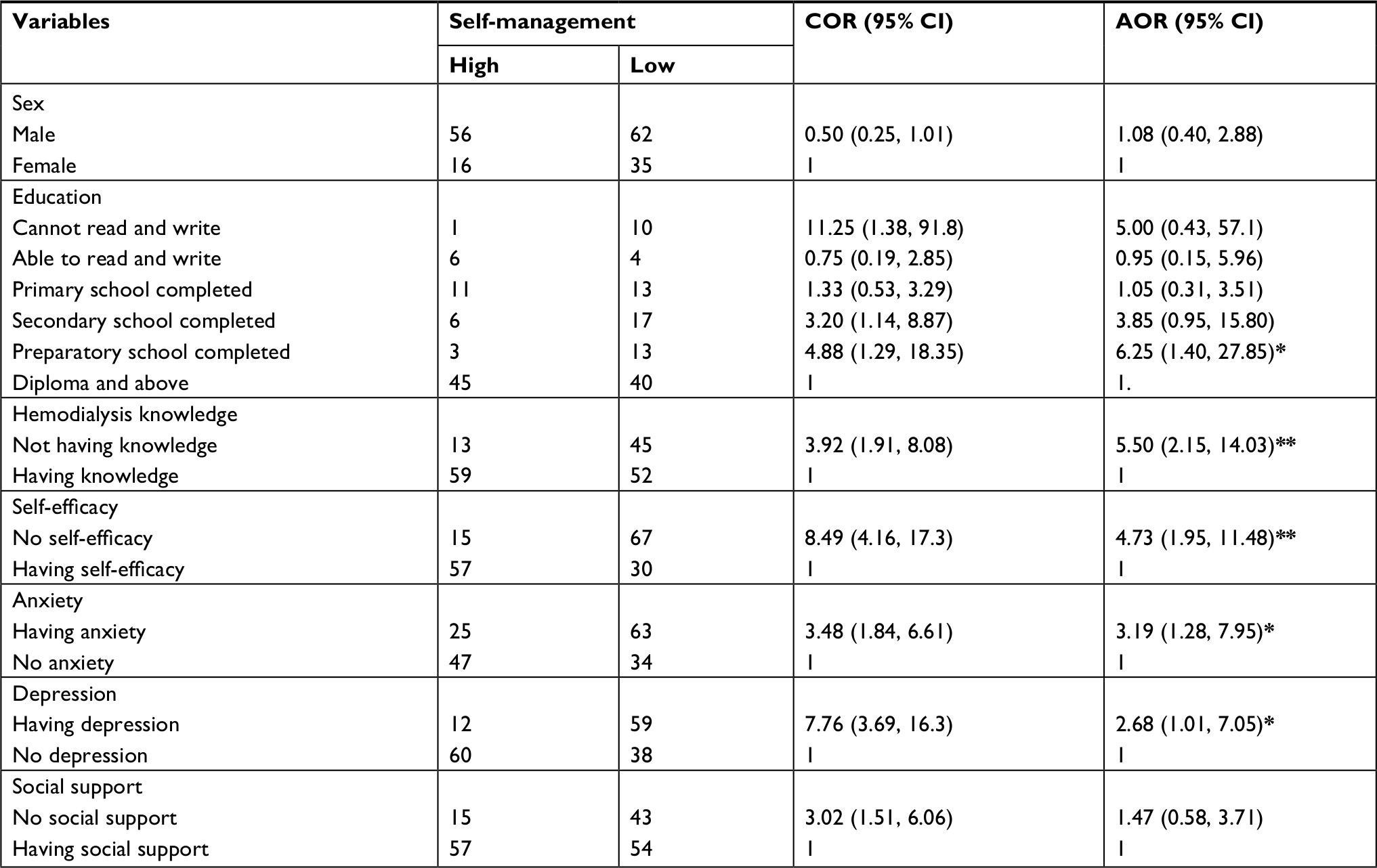 | Table 3 Factors associated with hemodialysis self-management (N=169) Notes: *P-value <0.05. **P-value <0.001. Abbreviations: AOR, adjusted OR; COR, crude OR. |
Discussion
In this study, we explored the level of self-management and associated factors among patients with ESRD undergoing hemodialysis in private health facilities in Addis Ababa, Ethiopia. The mean age of the patients was 49.86±15.58 years. More than half (57.4%) of the patients had low levels of self-management. Majority of the patients (68%) were dialyzed once and twice a week. There was a statistically significant positive association between self-management and education, knowledge, and self-efficacy, but there was a statistically significant negative association between self-management and anxiety and depression.
This study revealed the percentage of participants those dialyzed once and twice a week was high (68%). This is contrary to the findings of a study conducted in Beijing and Turkey that found about 90% of the participants dialyzed three times a week.2,17 This discrepancy may be linked to the shortage of resources, such as economy and limited access of the health facilities giving hemodialysis services. Of the total participants, 57.4% (n=97) had low level of self-management. This corroborates with a previous study conducted in Beijing and USA that found a low level of self-management among patients undergoing hemodialysis varying from ‘rare’ to ‘sometimes.’2,28 Thus, patients with ESRD undergoing hemodialysis in this country require close attention to improve the level of self-management.
Our study identified that education, knowledge, self-efficacy, anxiety, and depression have strong association with self-management. This study revealed that participants who had completed preparatory school were more likely having lower levels of self-management compared with those who had diplomas and above. This finding was similar to other studies done in Beijing, Iran, and California that found participants with higher education had higher levels of self-management.2,15,16 This might be related to the fact that the participants with higher educational level had better knowledge. In addition, the reason behind this might be that as educational level increases, information was obtained more easily and the obtained information was put into practice, an individual’s awareness increases, and consequently, their interest in their own health were increased. Therefore, participants with the low level of education need special emphasis when designing educational intervention.
Both knowledge and self-efficacy were also important predictors of self-management in this study. Previous studies have also shown that having knowledge2,18–22and self-efficacy2,17,19,22–24 are positively associated with self-management. This implies the need to develop strategies to improve knowledge and self-efficacy in order to enhance hemodialysis self-management. Prospective studies are also needed to determine the effects of knowledge and self-efficacy on hemodialysis self-management.
Psychological factors (anxiety and depression) were also good predictors of self-management in this study. Previous studies done in Beijing, China, Netherland, Colorado, and Turkey have also shown that having anxiety and depression is negatively associated with self-management.2,18-20,25,26 This implies the need to develop strategies to decrease anxiety and depression in order to enhance hemodialysis self-management. Prospective studies are also needed to determine the effects of anxiety and depression on hemodialysis self-management. Our study cannot found association between social support and self-management using the 95% CI. This is contrary to the findings of a study conducted in other settings that found social support having positive association with self-management.2,18,26,27 The discrepancy may be linked to the difference in the study design and sample size.
Limitations of the study
This study has numerous limitations. First, the use of cross-sectional design does not allow inferring causality. Prospective and experimental studies are warranted. Second is the use of interviewer-administered structured questionnaire for data collection. Using this method to identify self-management and associated factors among patients with ESRD undergoing hemodialysis might involve some risk, though qualitative interviews can let participants to liberally highlight their concerns and obstacles concerning practices of self-management. Finally, some potential influencing factors such as socio-economic and family background such as religious and type of payment and the dialysis modalities (length of dialysis sessions, dialyzers, and vascular access) were not measured in this study.
Conclusion
This study indicated that the level of self-management of patient with ESRD undergoing hemodialysis was low, although more than half of the respondents had knowledge about hemodialysis. Patients’ educational level, hemodialysis knowledge, self-efficacy, anxiety, and depression were found to be independent predictors of the self-management of patients with ESRD undergoing hemodialysis.
Clinical implications of the study
- Most of the patients with ESRD undergoing hemodialysis (57.4%) in this study reported lower self-management levels.
- Being educated and having knowledge about hemodialysis and self-efficacy are related to increased higher self-management levels while having anxiety and depression is related to lower self-management levels.
- Interventions addressing these factors may be effective to enhance hemodialysis self-management of patients with ESRD.
Research implications of the study
- Further studies should be conducted on the association of self-management and the socio-economic and family background, such as religious and type of payment and the dialysis modalities (length of dialysis sessions, dialyzers, and vascular access).
- Further study on large sample size and patients from different areas of the county are warranted.
- An interventional study should be conducted on the effect of educational level, self-efficacy, anxiety, and depression on self-management of patients with ESRD undergoing hemodialysis.
Ethics approval and consent to participate
This study was reviewed and approved by an Institutional Review Board of the College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia (protocol number: 094/Nurse). All subjects provided written informed consent, and the study was conducted in accordance with the Declaration of Helsinki.
Availability of data and materials
Datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We are very grateful to Addis Ababa University for the approval of the ethical clearance and for their financial support. We would like to thank all health facilities included in this study, data collectors, and study participants for their cooperation and assistance. We specifically thank our colleagues as well as our friends who were beside us at the moment we needed encouragement and more support. The study was funded by Addis Ababa University.
Author contributions
Both authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Griva K, Mooppil N, Seet P, Krishnan DSP, James H, Newman SP. The NKF-NUS hemodialysis trial protocol - a randomized controlled trial to determine the effectiveness of a self management intervention for hemodialysis patients. BMC Nephrol. 2011;12(1):1–11. | ||
Li H, Jiang YF, Lin CC. Factors associated with self-management by people undergoing hemodialysis: a descriptive study. Int J Nurs Stud. 2014;51(2):208–216. | ||
Griva K, Jayasena D, Davenport A, Harrison M, Newman SP. Illness and treatment cognitions and health related quality of life in end stage renal disease. Br J Health Psychol. 2009;14(Pt 1):17–34. | ||
Griva K, Stygall J, Hankins M, Davenport A, Harrison M, Newman SP. Cognitive impairment and 7-year mortality in dialysis patients. Am J Kidney Dis. 2010;56(4):693–703. | ||
Scholl LF, Dickenmann M, Hirt-Minkowski P. Outcome of dialysis patients aged seventy years or above a retrospective analysis. Swiss Med Wkly. 2014;144:w13920. | ||
Naicker S. End-stage renal disease in Sub-Saharan Africa. Ethn Dis. 2009;19(1 Suppl 1):S13–S14. | ||
Abd S, Mahmoud A, Selim M, Raouf H. Assessment of Self-Care Practice of Patients on Maintenance Hemodialysis at Cairo University Hospitals. J Educ Pract. 2014;5(39):161–174. | ||
World Health Organization (WHO). Primary health care systems (PRIMASYS): case study from Ethiopia, abridged version; 2017. Available from: http://www.who.int/alliance-hpsr/projects/alliancehpsr_ethiopiaabridgedprimasys.pdf. Accessed October 25, 2018. | ||
Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Development Programme IV, 2010/11 – 2014/15; 2011. Available from: http://www.nationalplanningcycles.org/sites/default/files/country_docs/Ethiopia/ethiopia_hsdp_iv_final_draft_2010-2015.pdf. Accessed October 25, 2018. | ||
Shibiru T, Gudina EK, Habte B, Deribew A, Agonafer T. Survival patterns of patients on maintenance hemodialysis for end stage renal disease in Ethiopia: summary of 91 cases. BMC Nephrol. 2013;14(1):1–6. | ||
Slesnick N, Pienkos S, Sun S, Doss-Mcquitty S, Schiller B. The chronic disease self-management program – A pilot study in patients undergoing hemodialysis. Nephrol News Issues. 2015;29(4):22–32. | ||
Richard AA, Shea K. Delineation of self-care and associated concepts. J Nurs Scholarsh. 2011;43(3):255–264. | ||
Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. | ||
Gallant MP. The influence of social support on chronic illness self-management: a review and directions for research. Health Educ Behav. 2003;30(2):170–195. | ||
Atashpeikar S, Jalilazar T, Heidarzadeh M. Self-care ability in hemodialysis patients. J Caring Sci. 2012;1(1):31–35. | ||
Rockwell JM, Riegel B. Predictors of self-care in persons with heart failure. Heart Lung. 2001;30(1):18–25. | ||
Bağ E, Mollaoğlu M. The evaluation of self-care and self-efficacy in patients undergoing hemodialysis. J Eval Clin Pract. 2010;16(3):605–610. | ||
Smith K, Coston M, Glock K, et al. Patient perspectives on fluid management in chronic hemodialysis. J Ren Nutr. 2010;20(5):334–341. | ||
Luo X, Liu T, Yuan X, et al. Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2015;12(9):11304–11327. | ||
Bayliss EA, Ellis JL, Steiner JF. Barriers to self-management and quality-of-life outcomes in seniors with multimorbidities. Ann Fam Med. 2007;5(5):395–402. | ||
Cavanaugh KL, Wingard RL, Hakim RM, Elasy TA, Ikizler TA. Patient dialysis knowledge is associated with permanent arteriovenous access use in chronic hemodialysis. Clin J Am Soc Nephrol. 2009;4(5):950–956. | ||
Do V, Young L, Barnason S, Tran H. Relationships between activation level, knowledge, self-efficacy, and self-management behavior in heart failure patients discharged from rural hospitals. F1000Res. 2015;4(150):1–11. | ||
Weng LC, Dai YT, Huang HL, Chiang YJ. Self-efficacy, self-care behaviours and quality of life of kidney transplant recipients. J Adv Nurs. 2010;66(4):828–838. | ||
Curtin RB, Walters BA, Schatell D, Pennell P, Wise M, Klicko K. Self-efficacy and self-management behaviors in patients with chronic kidney disease. Adv Chronic Kidney Dis. 2008;15(2):191–205. | ||
Bos-Touwen I, Schuurmans M, Monninkhof EM, et al. Patient and disease characteristics associated with activation for self-management in patients with diabetes, chronic obstructive pulmonary disease, chronic heart failure and chronic renal disease: a cross-sectional survey study. PLoS One. 2015;10(5):e0126400–e0126415. | ||
Mollaoglu M. Perceived social support, anxiety, and self-care among patients receiving hemodialysis. Dial Transplant. 2006;35(3):144–155. | ||
Ahrari S, Moshki M, Bahrami M. The Relationship Between Social Support and Adherence of Dietary and Fluids Restrictions among Hemodialysis Patients in Iran. J Caring Sci. 2014;3(1):11–19. | ||
Curtin RB, Sitter DC, Schatell D, Chewning BA. Self-management, knowledge, and functioning and well-being of patients on hemodialysis. Nephrol Nurs J. 2004;31(4):378396. | ||
Lorig K, Stewart A, Ritter P, González V, Laurent D, Lynch J. Chronic Disease Self-Efficacy Scales. Outcome Measures Health Educ Health Care Interv. 1996;25:2441–2445. | ||
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. | ||
Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. J Psychosom Res. 2002;52(2):69–77. | ||
Zimet GD, Dahlem NW, Zimet SG, Farley GK. The Multidimensional Scale of Perceived Social Support. J Pers Assess. 1988;52(1):30–41. | ||
Mohammad AH, Al Sadat N, Loh SY, Chinna K. Validity and reliability of the hausa version of multidimensional scale of perceived social support index. Iran Red Crescent Med J. 2015;17(2):e18776. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.