")
Back to Journals » Patient Preference and Adherence » Volume 16
Self-Management About Adjuvant Therapy in Breast Cancer Survivors: A Qualitative Study
Received 21 June 2022
Accepted for publication 15 September 2022
Published 23 September 2022 Volume 2022:16 Pages 2663—2681
DOI https://doi.org/10.2147/PPA.S379435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Lingying Jia, Yan Hu
School of Nursing, Fudan University, Shanghai, People’s Republic of China
Correspondence: Yan Hu, School of Nursing, Fudan University, Shanghai, People’s Republic of China, Tel +86 21 6443 1273, Fax +86 21 6416 1784, Email [email protected]
Objective: This study aims to describe the experience and connotations of self-management about adjuvant therapy (AT) in Chinese breast cancer survivors (BCS) and explore possible factors that affect their self-management level.
Methods: Semi-structured interviews were conducted in postoperative BCS undergoing AT using a qualitative description method. The conceptual structure and connotations were extracted after researchers collected and coded interview transcripts.
Results: After interviewing 29 patients, the conceptual framework of self-management in BCS during AT was optimized with three major themes: medical-related, emotion, and role management. Medical-related management includes AT-related adverse reactions; medical cooperation and knowledge acquisition; recovery and protection of affected limb; medical compliance; body image; sexual function and fertility; healthy lifestyle; catheter daily protection; and AT-related financial burdens. Emotion management includes recognition, prevention, and regulation of negative emotions. Role management consists of three aspects: family role, social role, and work role.
Conclusion: The conceptual structure and connotations formed in this study can help researchers to evaluate and intervene in the self-management ability of BCS during AT, so as to formulate the best model of care to improve their quality of life and clinical outcomes.
Keywords: breast neoplasm, adjuvant therapy, self-management, survivorship
Introduction
Breast cancer has replaced lung cancer as the most common cancer type worldwide since 2020, with higher morbidity and survival rates.1–3 According to the latest data, breast cancer will rank first in the proportion of new cancer cases among women both in China (19.5%), and the United States (31.0%) in 2022.3 Adjuvant therapy (AT) after the operation is crucial for breast cancer survivors (BCS) to prolong survival, which includes four methods: chemotherapy, targeted therapy, radiotherapy, and endocrine therapy.
Since cancer has been widely recognized as a regulated chronic disease, the concept of self-management (SM) has also been extended to cancer survivorship.4
In the 1980s, Corbin & Strauss5 originally proposed that SM should include three tasks: (1) medical management, the patient’s ability to manage their own disease symptoms and treatment; (2) life role management, the ability to adapt to the new role and continue a normal life; and (3) psychological management, the ability to face and resolve emotional disturbances caused by illness.6
On this basis, Lorig7 added six major skills of SM to achieve the management tasks: problem-solving, decision-making, resource utilization, building good relationships with healthcare providers, taking action, and self-tailor.
While there are various definitions of SM, Van de Velde’s definition fits better with the content raised by Corbin and Lorig: self-management is a patient’s ability to work with social networks and healthcare providers to internally control medical, role, and emotional changes after the illness.8
Cancer Self-management was first proposed by the National Cancer Survivorship Initiative in 2007.9 In 2009, Coster defined Cancer SM as the conscious and active participation of an individual in the recovery and rehabilitation process of the disease, minimizing the side effects of treatment, improving health status, and improving quality of life.10,11 But so far, the conceptual structure of Cancer SM has not been filled, and the definition is also limited to the symptom level.
In 2017, LL Cheng tried to construct a conceptual structure of Cancer SM, including six management aspects: daily life, symptom, emotion, communication with medical staff, resource utilization ability, and self-efficacy.12 However, the inclusion of self-efficacy as one of these aspects is debatable, since self-efficacy refers to confidence in SM and proves to be an antecedent to SM.13–15 Also, this structure does not clearly define each dimension, which may restrict researchers from using it to guide their research. Moreover, the content of SM may vary for different cancer types. Correspondingly, the conceptual structure needs to be further refined and supplemented.
Since the conceptual structure of cancer SM is still insufficient, our study chose Corbin & Strauss’ SM theoretical framework to conduct research due to its maturity.
For BCS, good SM skills may help improve their quality of life, as well as their sense of self-worth and self-satisfaction.16–19 In particular, SM of symptoms may help improve physiological indicators (such as bone density, body weight, pain, etc.), leading to less dependence on the medical staff and the relief of financial burdens due to frequent medical visits.6,13,14,16,17,20–24
Although research proves that about 80% of BCS can manage themselves safely and efficiently,16 BCS faces many specific SM issues, such as limb dysfunction and lymphedema;24,25 breast loss or scars; sexual dysfunction and fertility preservation, that require assessment, guidance, and professional support.26 A focus group interview shows that SM needs for BCS after treatments mainly include symptoms, emotions, information acquisition, a relationship with healthcare providers, and role adaptation.27 However, due to the characteristics of AT treatment (home/outpatient treatment; long duration; multiple treatment options; various side effects), BCS under AT may require more self-management skills than those after treatment.28
In recent years, SM in BCS has gradually become a hot topic, but there still are some limitations. First, most of the research is not supported by a theoretical framework or does not use the concept of SM.29 Second, although self-management and self-efficacy have been clearly defined, the two are closely related. In language systems other than English, these two concepts are more likely to be confused. In addition, the outcome of SM interventions is usually assessed through depression, self-efficacy, and quality of life, instead of using the SM measurements.30 However, it is vital and necessary to directly assess SM. A direct assessment can help researchers judge whether the intervention matches the patients’ ability well, and help compare the changes in SM ability resulting from the intervention, thereby reducing the bias of the research results. These limitations may be caused by the conceptual structure of SM in BCS not being sorted out. Therefore, clarifying the conceptual structure of SM may help us provide BCS with more efficient and appropriate self-management support and intervention.
As mentioned, AT is a core stage of SM for BCS. There are various methods of AT treatment, and different methods may bring different side effects. Some treatments also require the management of catheters and oral drugs. But we believe these are only a part of medical-related management in SM. There are actually more commonalities of SM between different AT methods, such as medical cooperation, function recovery, lifestyle optimization, role and emotion regulation, etc. And we noticed that some BCS receive multiple AT treatments at the same time or in succession, so it is difficult to divide AT by treatment methods. We believe that using a holistic view to measure SM in BCS during AT may help us dynamically assess the SM changes in individuals with the progress of AT, as well as compare and analyze the SM status of BCS under different AT methods.
Studies found that SM in chronic disease may be related to self-efficacy,13,14,17 information acquisition,13,17,31 motivation,13,32 and social support system,13,14,17 but in BCS, these relationships remain to be verified. For BCS during AT, we believe that AT types, demographic characteristics, disease severity, and treatment effects may also affect their SM ability to a certain extent.
The purposes of our research were to: (1) explore BCS perspectives on SM during AT, including their experiences, behaviors, motivators, and barriers through interviews; (2) explore the conceptual structure and connotations of BCS self-management during AT, in order to provide a basis for further assessments and interventions.
Methods
A qualitative description method was used to explore the connotations and possible factors of self-management of female BCS undergoing postoperative adjuvant therapy.
Participants
The purposive sampling method was used to maximize the sample diversity according to tumor stage, tumor type, surgical approach, therapeutic planning, age, marital status, and education level to ensure the representativeness and comprehensiveness of the participants.
Participants were all recruited at the outpatient department of comprehensive therapy at Fudan University Shanghai Cancer Center by the interviewer.
The inclusion criteria included: age above 18 years old; the primary tumor was diagnosed as breast tumor by pathology; currently undergoing postoperative AT; voluntary participation in this study.
The sample size was subject to the saturation of thematic information during data analysis, and 2–3 additional participants would be selected for confirmation and supplementation after no further information could be obtained.
Data Collection
We used semi-structured one-to-one interviews for data collection. The interview outline was mainly based on a literature review and was finally formed after pre-interviewing 2–3 participants. According to Corbin & Strauss’s chronic disease SM theoretical framework,5 we asked participants about their self-management methods and experiences from three management aspects: medical-related, emotion, and roles. (The interview outline is shown in Appendix 1).
The interview was conducted by a trained female researcher (LY Jia), who had interview experience and was not staff in the outpatient department.
The interviewer might adjust questions and ask in-depth according to the feedback.
A new outpatient office was selected as the interview site. The interview time for each participant was kept at about 30 minutes. Before the interview, all participants allowed us to record and use their responses anonymously. During the interview, we would not interrupt or induce the participant, and the participant had the right to terminate the interview at any time or ask questions. The verbatim transcription and verification were completed within 72 hours after the interview by the interviewer
Data Analysis
To protect patient privacy, numbers were used in place of the names when recording and organizing. The materials were analyzed and coded using content analysis methodology in Nvivo 12.0 software (QSR International, Melbourne, VIC, Australia) by ways of three-grade coding: Grade 1 coding is the decomposition, conceptualization, and reorganization of the original materials; Grade 2 coding is the formation of core categories; Grade 3 coding is the association and reorganization of categories.
To make the conceptual structure more organized and credible, we refer to Corbin & Strauss’ chronic disease SM theoretical framework5,7 as the theoretical basis when coding the materials.
According to the theory, the concept of self-management of BCS under AT can be divided into three themes: medical-related management, emotion management, and role management.
In the emotion management section, we also refer to the Gross’ emotion regulation process model,33,34 the classic model in emotion psychology, to help organize the original materials and form the core categories. In this model, emotion management consists of antecedent-focused regulation and response-focused regulation. The methods for antecedent-focused emotion regulation include situation selection, cognitive reappraisal, and attentional deployment, whereas response-focused regulation methods include expression suppression and emotion catharsis.33,34 In brief, we can summarize the emotion regulation process in three steps: recognition, prevention, and regulation.
Finally, we conducted a supplementary review based on the coding results and formed a conceptual structure framework after expert argumentation. We invited 15 experts with relevant research or clinical experience. The basic information of experts is shown in Table 1.
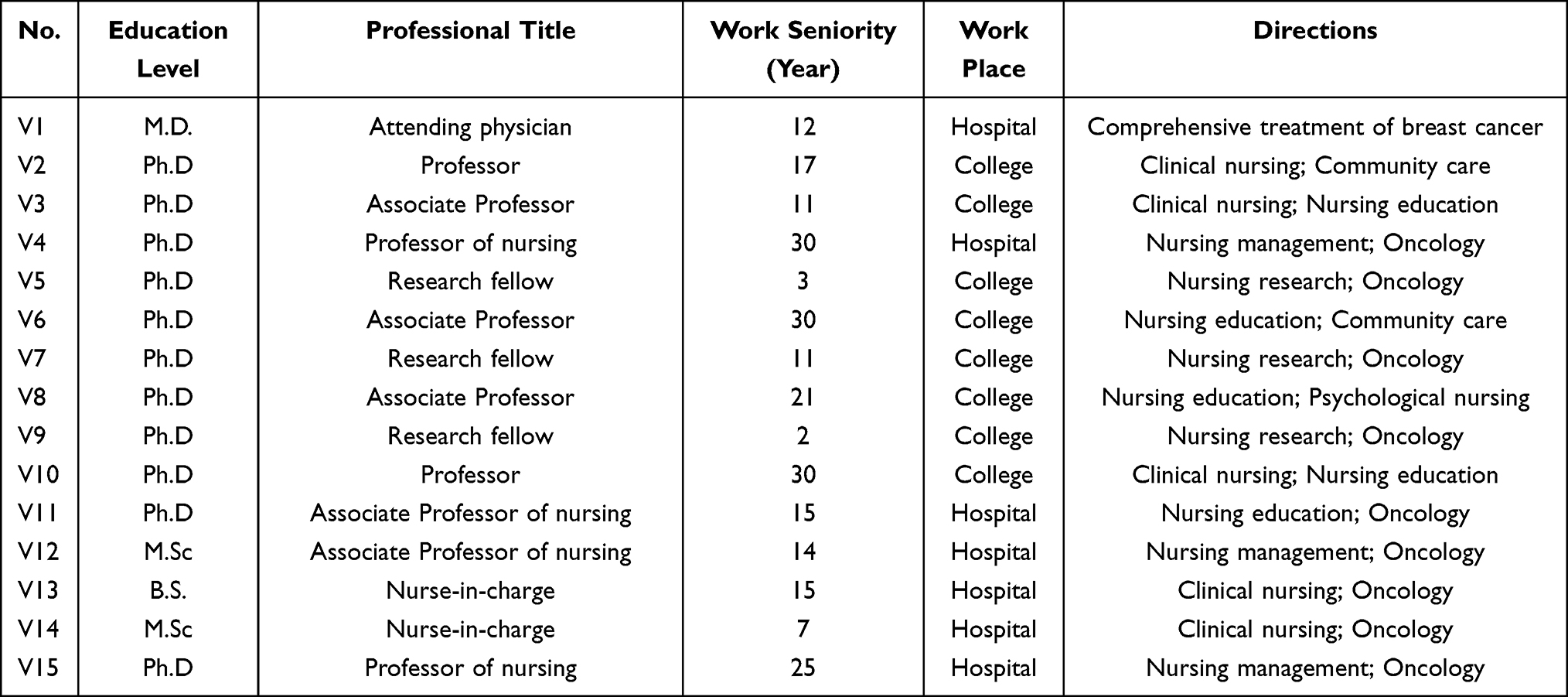 |
Table 1 Basic Information of Experts Involved in the Concept Demonstration (n=15) |
Results
General Information
A total of 29 BCS were selected from December 2021 to January 2022. The average age of participants was 50.7±11.03 years. Approximately 72.4% of them received chemotherapy, 37.9% of them received targeted therapy, 51.7% of them received radiotherapy, and 72.4% of them received endocrine therapy. In addition, molecular classification, TNM staging, surgery type, treatment plans, and demographic data are also considered to ensure maximum differentiation in sample selection. Participants’ information is shown in Table 2.
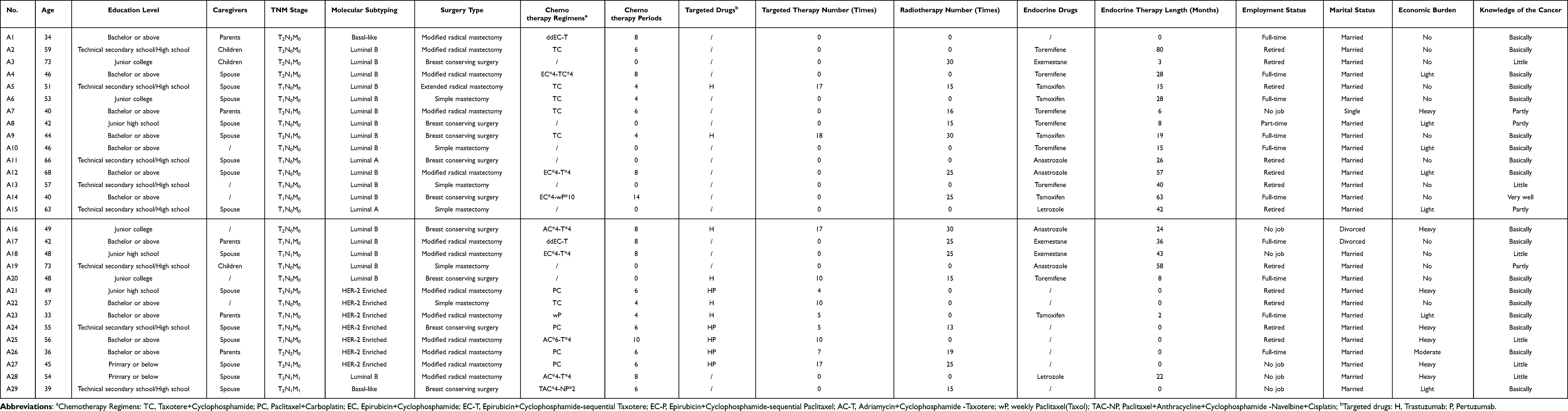 |
Table 2 Demographic Data (n=29) |
Medical-Related Self-Management
AT-Related Adverse Reactions
Although BCS under different AT methods has different types and degrees of adverse reactions, their self-management methods have lots in common.
For acute symptoms such as fever and severe vomiting, they (15/29) usually seek medical attention.
For most chronic problems such as osteoporosis, constipation, and dermatitis, some of them (10/29) prefer taking dietary supplements or over-the-counter drugs such as calcium tablets, multivitamins, and probiotics.
P18: I have been suffering from constipation all the time, so I bought probiotics myself. I think it is better to eat than not.
P3: I occasionally take vitamin B6 for mouth ulcers … and I feel constipation has worsened in the past two years. I tried some cassia seed tea, which seems to have some effect.
For intermittent or paroxysmal pain, they (11/29) may tolerate it and then consider medication after exceeding their tolerance limit, due to their concerns about the side effects of painkillers and sleeping pills.
P18: … the joints all over my body hurt so much that I couldn’t even lift chopsticks. My doctor said I could take painkillers, but I didn’t. I don’t think taking painkillers is good for my body, so I won’t take them when I can tolerate the pain.
TCM culture is popular in Chinese BCS. Some of them (5/29) believe that TCM conditioning can improve their body immunity and alleviate their adverse effects during AT. Especially during chemotherapy, they (3/5) would have Chinese medicinal diets like sea cucumber and finless eel soup to manage myelosuppression.
P5: I asked my attending doctor if I could do TCM conditioning … to improve my immunity, reduce side effects, and improve sleep quality … I think it works.
Recovery and Protection of Affected Limb
Some patients (11/29) reported that their affected limb had dysfunction; axillary web syndrome; edema during adjuvant therapy, but they (7/11) did not know how to manage it.
P24: I feel that my arm is hanging, which is a tingling feeling. Is there a good management method now, or should I just wait for the recovery on its own?
A small number of participants (4/11) tried to help their limbs recover through physiotherapy, massage, and acupuncture.
P22: My arm couldn’t be lifted. I felt that the upper arm was hanging with one tendon at the beginning, and gradually became a bundle at the back. I tried Baduanjin exercise, physical therapy, and acupuncture. Now I can at least straighten my arm.
Knowledge Acquisition
Social networks have become important for young and middle-aged patients to acquire knowledge. Almost all participants (25/29) said that they added online friends with their attending doctors, or followed the official account of the cancer center on WeChat.
Some participants (15/29) also joined the online group chat organized by other patients. In the group chat, they shared information on disease experience, the latest diagnosis/treatment news, and dietary advice.
P24: I am in an online BCS recovery group chat called ‘Roses the rebirth’ … I check group messages every day … they are very enthusiastic and helpful to me … I feel relief every time after browsing their online discussions in this group.
Medical Cooperation
Medical staffs have a solid relationship with patients. But there are barriers to their cooperation. Some participants (4/29) complained of difficulty in making medical appointments and the time limit of each follow-up visit.
P9: … the atmosphere here is too tense, and it’s too difficult to line up.
P13: The registration process is too complicated, and it is also very troublesome to make an appointment. It costs me all day long to see the doctor.
Also, due to cautiousness and introversion, some participants (8/29) confessed that they would not ask questions actively although there is a lack of knowledge.
P9: … the doctor won’t take the initiative to tell me … and I have never thought of asking questions when coming for follow-up.
Besides, many participants (11/29) could not tell the side effects of AT, not knowing where to consult and how to manage symptoms.
P3: I’m not sure if these symptoms are side effects of the drugs ….
P21: I haven’t dealt with these issues … I don’t know whom to look for … there’s nothing I can do.
P26: Do these side effects require treatment? Will it be fine?
Medical Compliance
Participants (18/21) generally had good compliance with chemotherapy, although they had to suffer from severe adverse reactions.
P9: I had severe urticaria at that time, but I still wanted to complete chemotherapy.
While radiotherapy seems more acceptable, there is still one participant who gave up due to fear of radiation hazards.
P11: I think radiotherapy is a bit excessive for me as my physique is not good enough … I’m afraid I cannot bear it ….
Since the participants who received endocrine therapy are all coming for examination or to purchase oral drugs, they can all be considered to have good medication compliance. However, many studies have shown that BCS often has poor AT compliance.35
In addition to oral anti-cancer agents, some participants (8/29) showed poor compliance with non-cancer treatment oral drugs used to alleviate adverse reactions. They were concerned about the extra damage and effects of such medications.
P9: My doctor prescribed painkillers, but I only took them three times (in total) when I failed to sleep because of the pain … I definitely don’t eat it during the daytime.
P22: The doctor suggested taking medicine for nourishing nerves, but I stopped taking it because I thought it was useless … there is also a liver-protecting medicine, but I didn’t insist on ….
Healthy Lifestyle
Participants reported various health problems, they usually relieved those problems and improved their life quality by managing diets, exercise, sleep and rest.
Diets
For high blood lipids, bone loss, and constipation, they (8/29) adjusted their diet structure for self-management.
P2: I was anemic before the operation, but I started taking supplements after chemotherapy, and I started eat more high-protein and high-vitamin foods instead of greasy food. Now even my anemia is cured.
P10: I have a fatty liver problem after AT, then I become a vegan.
Exercise
According to the participants (4/29), the purpose of physical activity and exercise is not only to maintain a healthy physical state but also for functional rehabilitation, the release of emotional problems, and the improvement of fatigue and sleep quality.
P4: Sometimes when I’m in a bad mood, I go for a run or do aerobics at home, then I feel better ….
P17: No matter how tired I am, I will let myself keep moving. I will let myself get out of bed and walk around … I walk around my community every night for hours to exercise. I think it benefits my sleep quality.
Besides daily activities, they usually went jogging, Tai Chi, swimming, etc. The intensity and frequency of activities were self-adjusted according to their endurance.
P26: I plan to practice yoga and swimming after the radiotherapy is over, but I don’t know if there are any yoga moves that I can’t do.
Sleep and Rests
Sleep habit adjustment is also a method for them to deal with fatigue and sleep disturbances. They (2/29) usually set a fixed sleep time, took a nap in the afternoon, etc.
P12: I will keep myself from being too tired and take a nap every day, nothing else can be done.
But more participants (7/29) indicated that they had no effective methods for fatigue and sleep problems, but endure and accept them. Some of them (4/7) said, if the sleep disturbance was severe, they would consider using melatonin and sleeping pills.
P27: It’s difficult to fall asleep … I felt dreaminess all night, which seemed like I was never asleep. It’s torture.
P14: I’m a light sleeper and easy to wake. If I wake up at midnight, it’s hard to fall asleep again. I have been taking melatonin for a while, but unfortunately, it doesn’t help … If I have insomnia for a few days, I will take sleeping pills - at least I can sleep well for a day, which will make me feel better.
Body Image
Most participants (19/29) hid body changes through self-grooming in social or work situations.
P1: I’m losing my hair … instead of sadness, I just think about how to cover it up and make myself look similar to others.
Some (5/29) said that they would refuse unnecessary outings and socializing during AT.
P25: I am much plumper after chemotherapy … So, I rarely go out now; I am afraid people will ask me something ….
For surgery scars and breast loss, elderly participants (6/6) showed an attitude of indifference and acceptance and did not make any modifications.
P19: I’m getting older anyway. It doesn’t matter if I have a (breast) resection.
Young and middle-aged participants were quite the opposite. They preferred breast reconstruction or using wearable artificial breasts. One participant (1/5) indicated that even after breast reconstruction, she could not accept the change psychologically.
P10: The breast was cut off and replaced with a fake one … the shape (of the artificial breast) doesn’t look as comfortable as my real breast.
AT-Related Financial Burden
Except for patients under endocrine therapy or who have retired, participants who are under other AT types may still be in a state of no work and no income (8/29). Therefore, some participants (3/29) were worried about their worsening financial situation because of the long-term and costly AT treatments.
P24: It is a heavy burden on my family’s financial situation. Because my salary is low, and my husband is only a laid-off worker … we can’t afford the treatments with such a low ratio of inter-provincial medical reimbursement. For example, if residents only need to pay one with their local medical insurance, I have to pay ten times.
They (5/29) mainly avoided or reduced AT-related financial burdens by returning to work.
P23: I have to work after targeted therapy, for money to continue the treatments and raise my child.
However, there are still some patients (2/29) with heavy financial burdens who gave up treatments and medical examinations.
P5: As far as I know, some patients will give up targeted therapy because of the expensive out-of-pocket drugs.
P24: I would not do the inspections that I thought were not crucial.
Emotion Management
Recognition of Negative Emotions
Nearly all participants who have not experienced chemotherapy (7/8) reported no major changes in emotional states. On the contrary, most of the participants who had undergone chemotherapy (15/21) recalled that they suffered mood swings or were constantly troubled by negative emotions during that time.
P14: I felt very collapsed. I didn’t believe that my life could return to normal after the treatment. I felt that I could only be in a very sick and weak state forever.
P9: When I first started chemotherapy, I was in a bad mood … I wondered why it was me to suffer this disease ….
P28: Many people told me that once cancer had metastasized, there would be no hope and I would die soon. I felt that I could not pass this barrier. (Patient with pulmonary metastasis).
Most patients (12/15) said that their moods gradually brightened with the end of chemotherapy, but some of them (3/12) still felt fear and anxiety about cancer recurrence.
P12: Since I’m already in this situation, what I can do is take it easy. If cancer still recurred, at least I have tried my best, then there would be no regret.
P26: After the chemotherapy, my body recovers a lot, and my mood is much better. Now I mainly worry about whether it will recur or metastasize. My mood changed from collapse to anxiety. But I think I should face it bravely. I believe that though breast cancer may not be cured, it is not fatal.
Patients under endocrine therapy have fewer negative emotions. However, they (2/21) felt inferior and disappointed sometimes after experiencing limb dysfunction.
P10: Actually, I have been doing all kinds of rehabilitation exercises, but I haven’t practiced the movement of buttoning bras myself. During AT, when I started needing to do this action by myself, I realized that I can’t do it anymore ….
Compared with young patients, elderly patients (6/6) perceive fewer negative emotions.
P11: I feel that breast cancer has no effect on my emotional state at all. I can face the reality very well.
P19: I feel no negative emotions. I think birth; old age; sickness and death are normal. Just let it happen.
Prevention of Negative Emotions
According to Gross,34 people can subconsciously recognize, avoid or modify situations (such as people, objects, places, topics, etc.) that lead to negative emotions, which can help us block the generation of negative emotions. And there is a time lag between when we generate and perceive negative emotions, and when we express these emotions through behavior. During this period, our consciousness will respond to emotional problems first. During the interval, our consciousness responds first to emotional problems.
Situation Selection and Modification
In the interviews, some participants (6/29) indicated that they would not talk about cancer when chatting; one of them (1/6) even said that she would not go in the direction of the hospital when hanging out.
P14: I will neither deliberately hide nor talk about cancer, otherwise I will receive a lot of negative feedback and become very sensitive.
Cognitive Reappraisal
Some participants (8/29) were more inclined to prevent negative emotions by changing their understanding and cognition of breast cancer, regarding it as a challenge or opportunity.
P1: I won’t let myself be in a very anxious state for a long time. I think it’s not good for my condition … I won’t let it become my burden.
P5: God is fair. If God closes the door for you, he will open the window somewhere else.
Attention Allocation
Yet more participants (15/29) tended to pay more attention to work, sports, entertainment, pets, etc., to avoid the occurrence of negative emotions.
P11: I prefer baking now. I feel satisfied and pleased when others received my handmade desserts.
Regulation of Emotional Responses
Psychological Support
Participants (27/29) generally believed that they had good self-management skills on emotions and did not need professional support. Only a small number of young participants (2/29) had willing to seek professional psychological support.
P10: If it turns serious, I will go for psychological counseling … I know the importance of having psychiatrists, but I feel I can dispel the bad moods myself until now.
Expressive Suppression
More than half of the participants (17/29) did not want to add psychological burdens to their relatives and friends, so they usually concealed or suppressed their negative emotional responses.
P1: I won’t show any negative emotions in front of my family. I’m afraid the pressure from my family will be greater … But I will divert my attention in time.
Emotional Catharsis
They (18/29) sometimes vented their emotional stress by crying or confiding in other patients or friends.
P16: I met some patients from other places online, and sometimes I would confide to them when my emotions were indigestible. We would cheer and encourage each other … Sometimes I also hide and cry by myself to release the emotions.
Attention Deployment
Besides, some of them (5/29) exercised, listened to music, or watched movies to decompress and divert attention when the negative emotions could not be released.
P10: I will find ways to dispel my worries … Sometimes I will divert my attention by reading novels and watching TV.
Role Management
Family Role Management
Some participants (7/29) who have given birth said that they frankly told their partner and children about their physical condition. They believed that this would help the adjustment and recovery of their family roles.
P1: I have a 6-year-old child. We told him my situation and why I was losing my hair at the very beginning. I felt he understood it.
The family role functions usually recover after endocrine therapy starts. A majority of patients (19/21) under endocrine therapy continued to assist in raising (grand)children or doing housework as before.
P13: Everything is back to normal. I do laundry and cook. Now I have a little grandson to take care of.
But they also said they would pay more attention to private life after cancer.
P13: I won’t take care of children for a long time. I also have my own recreational activities.
Work Role Management
Although many patients (11/29) changed their jobs or retired early because of the illness, returning to work (RTW) is still an essential way for participants to alleviate the economic burden and divert attention. It also symbolizes the role shift from being a patient to an ordinary person.
An excellent working atmosphere and co-worker relationship can help patients (4/29) relieve emotional stress. Conversely, poor colleague relationship management may exacerbate negative emotions (1/29).
P6: I am no longer in charge of major projects after surgery. After that, my colleagues changed their attitude towards me, which disappointed me a little.
Social Role Management
Some participants (9/29) are sensitive and have a solid ability to perceive discrimination. They fear others’ glances and avoid social occasions.
P11: … my friends asked me out, but I refused … I didn’t tell anyone about this disease. I don’t want others to know because I’m tired of their nonsense behind my back … I would be very disappointed if they don’t want to have contact with me any longer after I tell them I have breast cancer.
P26: I don’t really want others to know that I have breast cancer, I just want to run away and hide my head in the sand.
Some participants (4/29) adjusted their social roles by streamlining or expanding their social circles.
P26: I still keep in touch with my best friends, but I no longer hang out with my normal friends.
P5: During adjuvant therapy, I met many new friends who can share with each other. Now I have a wider social circle.
In the interviews, we also found that COVID-19 had a certain impact on participants’ social function recovery (4/29).
P22: Because I have not been vaccinated due to this disease, and my resistance is poor, I dare not go out when my friend asks me.
P23: Affected by COVID-19, it’s inconvenient to go out now, so I just chat with my friends online.
Discussion
This research provides a deep insight into the perspectives of BCS on self-management (SM) during AT, and we explored the possible factors that may influence the SM ability and behavior of BCS. Based on Corbin & Strauss’ SM theoretical framework and Gross’ emotion regulation process model, the conceptual structure and connotations of SM are also formed in this study. The conceptual structure and the connotations can be found in Figure 1 and Table 3.
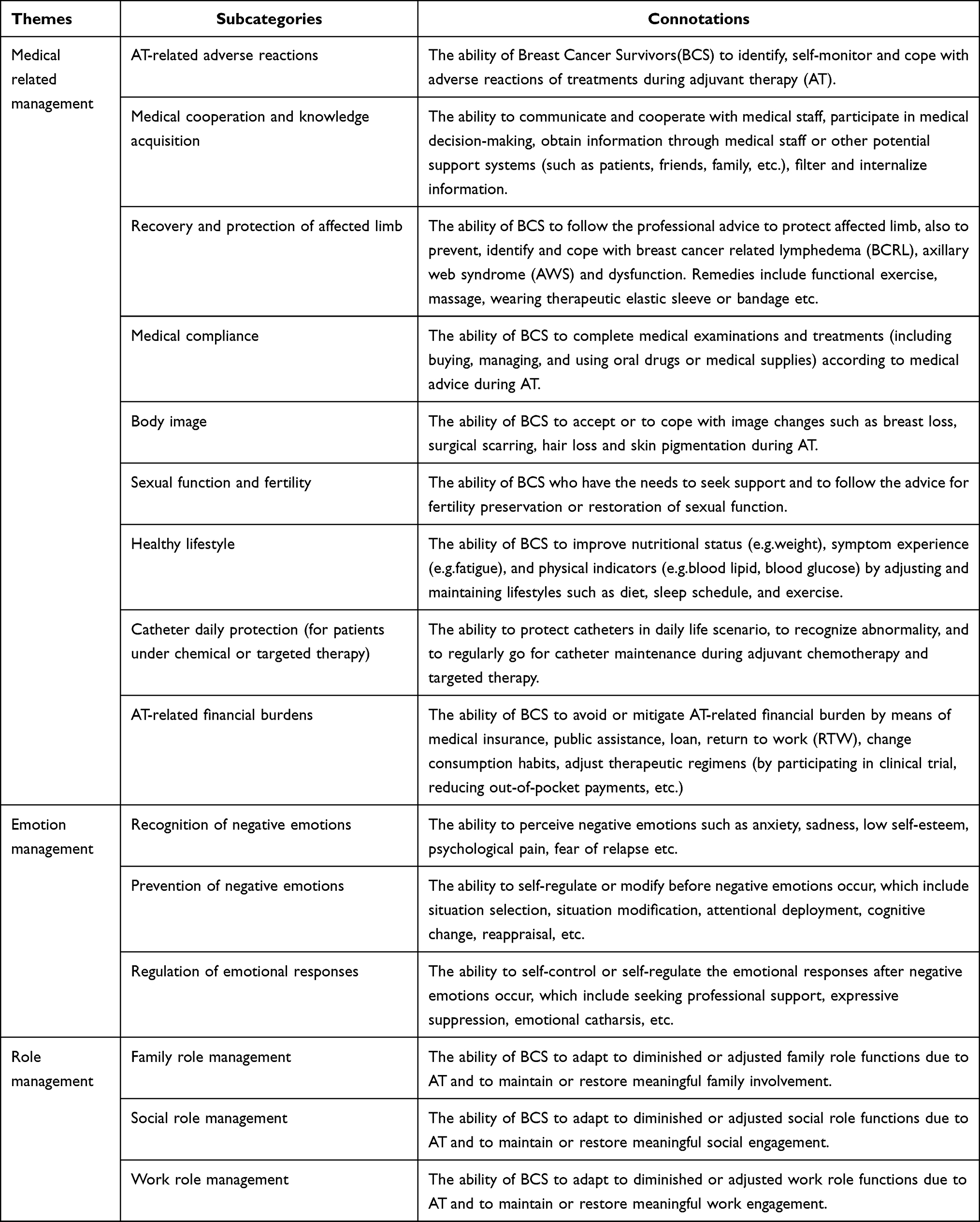 |
Table 3 The Connotation of Self-Management About Adjuvant Therapy in Breast Cancer Survivors |
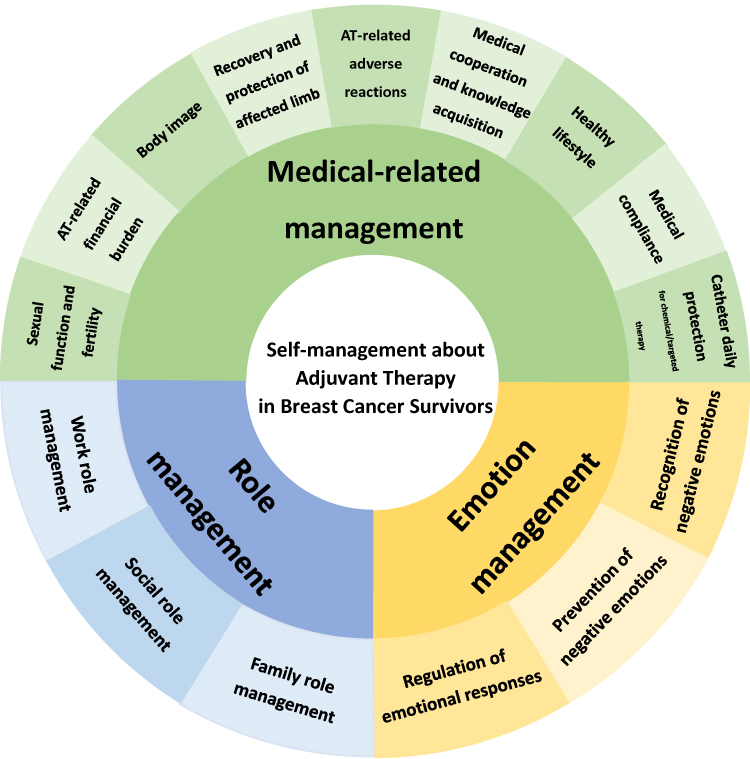 |
Figure 1 The conceptual structure of self-management about adjuvant therapy in breast cancer survivors. |
In the conceptual structure, we integrated SM of BCS under AT into three tasks: medical-related management, emotion management, and role management.5
Medical-Related Management
(1) AT-related adverse reactions; (2) Medical cooperation and knowledge acquisition; (3) Recovery and protection of affected limb; (4) Healthy lifestyle; (5) Body image; (6) Medical Compliance; (7) AT-related financial burden; (8) Sexual function and fertility; (9) Catheter daily protection.
Emotion Management
(10) Recognition of negative emotions; (11) Prevention of negative emotions; (12) Recognition of negative emotions.
Role Management
(13) Work role management; (14) Social role management; (15) Family role management.
Similar to previous studies on SM of BCS in other stages, this study shows that adverse reaction management; affected limb rehabilitation; medical cooperation and information acquisition; medical compliance; body image; lifestyle; emotion and role management are also important contents of SM in BCS during AT.12,30,35–38 While our research refined emotion management and role management according to Gross’ emotion regulation process model and different role settings.
Our results also show that the financial burden caused by high-cost AT should also be included. The main reason for the economic burden is the high out-of-pocket expenses.39 The most common solution is to return to work (RTW). Meanwhile, RTW has also been shown to be beneficial for the quality of life, emotion, and role functional recovery, but this is not applicable to the aged as well as patients with severe adverse reactions.40 However, it’s unreasonable to constrain medical staff to answer questions on Medicare coverage and national security policies beyond their area of specialization. Therefore, it is important to improve patients’ health insurance literacy as well as their financial literacy.41 We can also inform patients about access to health care policies and financial assistance when follow-up.
Besides, BCS may have some specific or personalized needs for self-management. For BCS of childbearing age, fertility preservation and sexual function adjustment are quite needed.42–44 Also, we should notice that PICC and PORT are widely used when using intravenous anticancer drugs. Patients with catheters need to manage their catheters during bathing, sleeping, and outdoor activities.45 Therefore, aspects 8 and 9 are added for BCS with specific needs based on expert recommendations and previous studies.
The study indicates that most patients have a lack of knowledge in medical-related self-management, especially in preventive health care and daily life care. Although many patients conducted self-management by adjusting their lifestyles, they were not clear about the scientific methods of diet, exercise, and rest. They also had concerns about the use of TCM and physiotherapy.
Through study results, we can find that SM behaviors of BCS are mainly problem-solving oriented. Their decisions and actions on SM are more likely to be instinctive reactions subconsciously. For tolerable symptoms, such as mild pain, hyperpigmentation, numbness, and menopause-like symptoms, they rarely consult a professional about SM methods. This may be because they have never heard of SM, and there is no consultation channel for SM. So they did not believe that scientific self-management can be carried out with professional support.
Therefore, it’s vital to arouse patients’ subjective consciousness of SM, encourage them to take the initiative in SM, and give them more professional SM support.
However, professional self-management supports are still insufficient.16 Our findings indicated that professionals lack initiative in doctor-patient communication. Moreover, although social support is proved beneficial to patients’ resilience, adherence and quality of life,46,47 there is a certain contradiction in medication belief between professional support and personal social support systems, which makes patients feel at a loss. Quite a few patients in our study had taken dietary supplements or stopped taking oral drugs under the advice of friends and other patients. Despite the low credibility, BCS are more likely to trust personal social support systems because friends, relatives, and other patients are critical components of their lives. Unfortunately, compared with them, professionals have no time and energy to give all SM suggestions and fully explain their views to each patient. Since many medical institutions have begun to create online official accounts through (mini) apps or other social networks, using web-based platforms to promote self-management knowledge may be the general trend, but the findings remain controversial,48 and it’s still difficult for old participants to use complex interactive programs to acquire knowledge. In addition, professionals may also take advantage of the social support system for SM support, as a previous study on BCS peer-led self-management with the aid of both social and professional support systems is proved effective.49
Medical compliance is also a major part of SM during AT. We found that patients under intravenous chemotherapy showed good compliance, not only because of fear and anxiety about cancer recurrence but also because of limited treatment sites and the short treatment period. On the contrary, patients are often resistant to long-term oral drugs due to economic concerns and drug side effects.50,51 For oral drugs, patients need more powerful motivation to insist on taking them. If they cannot feel the immediate therapeutic effect of the drug, or if there are more side effects, they may stop using the drug without authorization.52 While current studies have shown that the use of SMS reminders can improve medical compliance to a certain extent.53
Emotion management of BCS during AT conformed well to the Gross’ emotion regulation process model.34 In this study, negative emotions in patients under chemotherapy were the most significant. With the reduction of adverse reactions and the recovery of role functions, the patients’ emotions gradually brightened. They are more inclined to focus on things other than cancer or change their cognition to reduce the occurrence of negative emotions. Same as past studies, after the occurrence of negative emotions, middle-aged females are more likely to suppress, hide their emotions, or vent their emotions with other patients.54 While young females are more willing to shift their attention to work, sports, or entertainment or seek professional psychological support such as cognitive behavioral therapy and pharmacologic treatments.55
The role function of BCS gradually recovers with the progress of AT. Most patients reported their family role function had completely recovered since endocrine therapy started, whereas their work role was adjusted more or less. Participants thought that their physical strength decreased significantly during AT and they could not undertake high-intensity work, so they took the initiative to adjust their jobs. Consistent with the previous studies, the reduced work engagement and work ability may be due to weakness, fatigue, and AT-related adverse reactions, whereas their work performance and emotions are related to the work environment.56 However, most young survivors still have a positive attitude toward RTW, believing that work is the first step away from the patient role. Because survivors are the primary decision-makers in RTW planning and their wishes must be respected,57 while clinicians are committed to helping them to RTW, interventions remain limited to providing information and psychological support for RTW.56
The social circle and social role function of BCS have also changed. Because of low-esteem and social stigma,58 some of them have reduced their communication with ordinary friends since AT started and prefer to get along with other patients with the same disease experience and similar background. Studies have shown that group therapies, physical activity therapies, as well as cosmetic therapy, can help the recovery of social role function by alleviating cancer stigma and improving their self-esteem.59,60
Agree with previous results, the factors related to SM of BCS during AT mainly include self-efficacy,13,14,17 social support system,13,14,17 motivation,13,32 and information acquisition.13,17,31 In addition, this study concluded that age, education level, and income level were closely related to SM ability. Young patients with high education levels and high income tend to be more determined in self-management because they are usually better at learning and more receptive to new things. Although young survivors may have more body image disturbances and emotional and role management problems, their self-management methods and support systems are much richer.
Emotion and role management are more related to the disease progression, the severity of adverse reactions, and treatment effects. Lack of social support, serious adverse reactions, and poor treatment effects may aggravate BCS’s negative emotions and weaken their role functions as well.
Study Limitations
The interview site for this study was a tertiary A-level cancer center. The participants were limited to the Han-nationality outpatients, and there was a lack of young BCS under 33. Thus, there may be limitations in generalizability to the broader population due to homogeneity of patients’ sources, ethnicity, age, etc.
Conclusion
By constructing the conceptual structure of BCS self-management during AT, we provide deep insights into the directions and contents that self-management support interventions should be offered to BCS during adjuvant therapy. Meanwhile, our study also contributes to the development of SM measurements for BCS, further optimizing SM assessments.
Our results indicate that both professional support and social support are important for BCS to conduct SM, while demographic characteristics and symptom severity are also correlated with SM during AT.
Our study suggests that future self-management interventions should put more emphasis on the motivation of patients’ SM initiative, as well as SM methods for healthy lifestyle, oral drug compliance, financial burden, and role function recovery.
We believe that our results will contribute to the development of SM supportive interventions during adjuvant therapy for breast cancer.
Clinical Implications
Based on the results, we developed a conceptual framework of self-management in BCS under AT. This framework can be used to develop a self-management measurement tool specific to survivors under AT, allowing us to develop the optimal care model, intervention measures, and rehabilitation guidance. These can ultimately help improve survivors’ quality of life, enhance their sense of self-worth, and improve their physiological indicators.6,12,17
Ethics Approval
The research protocol was approved by the Ethics Committee of the School of Nursing, Fudan University (IRB#2021-07-01) and the Fudan University Shanghai Cancer Center (No.2112247-20). This study complied with the Declaration of Helsinki, and all participants gave written informed consent voluntarily with permission to publish their anonymized responses.
Acknowledgments
We would like to express our gratitude to the BCS who participated in this study and to the medical staff in Fudan University Shanghai Cancer Center for their support. We are also very grateful for the funding support given by the Fosun Foundation (FNF202103).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. doi:10.3322/caac.21708
3. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
4. Qian H, Yuan C. Research status and enlightenment of cancer self-management. Chin J Nurs. 2010;45(12):1147–1150. doi:10.3761/j.issn.0254-1769.2010.12.037
5. Corbin JM, Strauss A. Unending Work and Care: Managing Chronic Illness at Home. San Francisco, CA, US: Jossey-Bass; 1988.
6. McCorkle R, Ercolano E, Lazenby M, et al. Self-management: enabling and empowering patients living with cancer as a chronic illness. CA Cancer J Clin. 2011;61(1):50–62. doi:10.3322/caac.20093
7. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
8. Van de Velde D, De Zutter F, Satink T, et al. Delineating the concept of self-management in chronic conditions: a concept analysis. BMJ Open. 2019;9(7):e027775. doi:10.1136/BMJopen-2018-027775
9. Foster C, Brown J, Killen M, Brearley S. The NCRI cancer experiences collaborative: defining self management. Eur J Oncol Nurs. 2007;11(4):295–297. doi:10.1016/j.ejon.2007.08.002
10. Coster S, Norman I. Cochrane reviews of educational and self-management interventions to guide nursing practice: a review. Int J Nurs Stud. 2009;46(4):508–528. doi:10.1016/j.ijnurstu.2008.09.009
11. Coster S, Li Y, Norman IJ. Cochrane reviews of educational and self-management interventions to guide nursing practice: a review. Int J Nurs Stud. 2020;110:103698. doi:10.1016/j.ijnurstu.2020.103698
12. Cheng L, Sun Y. Development and validation of cancer patient self-management assessment scale. Chin J Nurs. 2017;52(9):1082–1087. doi:10.3761/j.issn.0254-1769.2017.09.014
13. Miller WR, Lasiter S, Bartlett Ellis R, Buelow JM. Chronic disease self-management: a hybrid concept analysis. Nurs Outlook. 2015;63(2):154–161. doi:10.1016/j.outlook.2014.07.005
14. Udlis KA. Self-management in chronic illness: concept and dimensional analysis. J Nurs Healthc Chronic Illn. 2011;3(2):130–139. doi:10.1111/j.1752-9824.2011.01085.x
15. Unger WR, Buelow JM. Hybrid concept analysis of self-management in adults newly diagnosed with epilepsy. Epilepsy Behav. 2009;14(1):89–95. doi:10.1016/j.yebeh.2008.09.002
16. Jefford M, Howell D, Li Q, et al. Improved models of care for cancer survivors. Lancet. 2022;399(10334):1551–1560. doi:10.1016/s0140-6736(22)00306-3
17. Matarese M, Lommi M, De Marinis MG, Riegel B. A systematic review and integration of concept analyses of self-care and related concepts. J Nurs Scholarsh. 2018;50(3):296–305. doi:10.1111/jnu.12385
18. Mason M, Harris MR, Greer JA, Jiang Y, Concept A. Analysis of oral anticancer agent self-management. Cancer Nurs. 2022;45(2):E374–e387. doi:10.1097/ncc.0000000000000934
19. Runowicz CD, Leach CR, Henry NL, et al. American Cancer Society/American Society of Clinical Oncology breast cancer survivorship care guideline. CA Cancer J Clin. 2016;66(1):43–73. doi:10.3322/caac.21319
20. Mammen J, Rhee H. Adolescent asthma self-management: a concept analysis and operational definition. Pediatr Allergy Immunol Pulmonol. 2012;25(4):180–189. doi:10.1089/ped.2012.0150
21. Blok AC. A middle-range explanatory theory of self-management behavior for collaborative research and practice. Nurs Forum. 2017;52(2):138–146. doi:10.1111/nuf.12169
22. Balduino AF, Mantovani MF, Lacerda MR, Meier MJ. [Conceptual self-management analysis of hypertensive individuals]. Rev Gaucha Enferm. 2013;34(4):37–44. Portuguese. doi:10.1590/s1983-14472013000400005
23. Ohlendorf JM. Postpartum weight self-management: a concept analysis. Res Theory Nurs Pract. 2013;27(1):35–52. doi:10.1891/1541-6577.27.1.35
24. Paolucci T, Bernetti A, Bai AV, et al. The sequelae of mastectomy and quadrantectomy with respect to the reaching movement in breast cancer survivors: evidence for an integrated rehabilitation protocol during oncological care. Support Care Cancer. 2021;29(2):899–908. doi:10.1007/s00520-020-05567-x
25. Paolucci T, Bernetti A, Bai AV, et al. The recovery of reaching movement in breast cancer survivors: two different rehabilitative protocols in comparison. Eur J Phys Rehabil Med. 2021;57(1):137–147. doi:10.23736/s1973-9087.20.06138-9
26. Kim SH, Choe YH, Cho YU, Park S, Lee MH. Effects of a partnership-based, needs-tailored self-management support intervention for post-treatment breast cancer survivors: a randomized controlled trial. Psychooncology. 2022;31(3):460–469. doi:10.1002/pon.5828
27. Kim SH, Park S, Kim SJ, Hur MH, Lee BG, Han MS. Self-management needs of breast cancer survivors after treatment: results from a focus group interview. Cancer Nurs. 2020;43(1):78–85. doi:10.1097/ncc.0000000000000641
28. National Comprehensive Cancer Network (NCCN). National comprehensive cancer network clinical practice guidelines in oncology, survivorship version 1, 2022 [EB/OL]. National Comprehensive Cancer Network (NCCN); 2022. Available from: http://www.nccn.org.
29. Cuthbert CA, Farragher JF, Hemmelgarn BR, Ding Q, McKinnon GP, Cheung WY. Self-management interventions for cancer survivors: a systematic review and evaluation of intervention content and theories. Psychooncology. 2019;28(11):2119–2140. doi:10.1002/pon.5215
30. Kim SH, Kim K, Mayer DK. Self-management intervention for adult cancer survivors after treatment: a systematic review and meta-analysis. Oncol Nurs Forum. 2017;44(6):719–728. doi:10.1188/17.Onf.719-728
31. Rothenberger CD. Chronic illness self-management in prediabetes: a concept analysis. J Nurs Healthc Chronic Illn. 2011;3(2):77–86. doi:10.1111/j.1752-9824.2011.01092.x
32. Schilling LS, Grey M, Knafl KA. The concept of self-management of type 1 diabetes in children and adolescents: an evolutionary concept analysis. J Adv Nurs. 2002;37(1):87–99. doi:10.1046/j.1365-2648.2002.02061.x
33. McRae K, Gross JJ. Emotion regulation. Emotion. 2020;20(1):1–9. doi:10.1037/emo0000703
34. Gross JJ. Emotion and emotion regulation. In: Handbook of Personality: Theory and Research.
35. Clancy C, Lynch J, Dowling M, Dowling M. Breast cancer patients’ experiences of adherence and persistence to oral endocrine therapy: a qualitative evidence synthesis. Eur J Oncol Nurs. 2020;44:101706. doi:10.1016/j.ejon.2019.101706
36. Pierrisnard C, Baciuchka M, Mancini J, Rathelot P, Vanelle P, Montana M. Body image and psychological distress in women with breast cancer: a French online survey on patients’ perceptions and expectations. Breast Cancer. 2018;25(3):303–308. doi:10.1007/s12282-017-0828-2
37. Zhao H, Wu Y, Zhou C, Li W, Li X, Chen L. Breast cancer-related lymphedema patient and healthcare professional experiences in lymphedema self-management: a qualitative study. Support Care Cancer. 2021;29(12):8027–8044. doi:10.1007/s00520-021-06390-8
38. Cheng H, Sit JWH, Cheng KKF. A qualitative insight into self-management experience among Chinese breast cancer survivors. Psychooncology. 2017;26(7):1044–1049. doi:10.1002/pon.4279
39. Longo CJ, Fitch MI, Loree JM, et al. Patient and family financial burden associated with cancer treatment in Canada: a national study. Support Care Cancer. 2021;29(6):3377–3386. doi:10.1007/s00520-020-05907-x
40. Schmidt ME, Scherer S, Wiskemann J, Steindorf K. Return to work after breast cancer: the role of treatment-related side effects and potential impact on quality of life. Eur J Cancer Care. 2019;28(4):e13051. doi:10.1111/ecc.13051
41. Khera N, Zhang N, Hilal T, et al. Association of health insurance literacy with financial hardship in patients with cancer. JAMA Netw Open. 2022;5(7):e2223141. doi:10.1001/jamanetworkopen.2022.23141
42. Burg MA, Adorno G, Lopez ED, et al. Current unmet needs of cancer survivors: analysis of open-ended responses to the American Cancer Society Study of Cancer Survivors II. Cancer. 2015;121(4):623–630. doi:10.1002/cncr.28951
43. Hubbard G, Venning C, Walker A, Scanlon K, Kyle RG. Supportive care needs of women with breast cancer in rural Scotland. Support Care Cancer. 2015;23(6):1523–1532. doi:10.1007/s00520-014-2501-z
44. Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(19):1994–2001. doi:10.1200/jco.2018.78.1914
45. Liu CL, Yan MQ, Lu ZQ. Development and validation of the cancer patients PICC self-management scale. J Nurs Sci. 2012;27(23):1–4. doi:10.3870/hlxzz.2012.23.001
46. Zhang H, Zhao Q, Cao P, Ren G. Resilience and quality of life: exploring the mediator role of social support in patients with breast cancer. Med Sci Monit. 2017;23:5969–5979. doi:10.12659/msm.907730
47. Kroenke CH, Hershman DL, Gomez SL, et al. Personal and clinical social support and adherence to adjuvant endocrine therapy among hormone receptor-positive breast cancer patients in an integrated health care system. Breast Cancer Res Treat. 2018;170(3):623–631. doi:10.1007/s10549-018-4774-2
48. van der Hout A, van Uden-Kraan CF, Holtmaat K, et al. Role of eHealth application Oncokompas in supporting self-management of symptoms and health-related quality of life in cancer survivors: a randomised, controlled trial. Lancet Oncol. 2020;21(1):80–94. doi:10.1016/s1470-2045(19)30675-8
49. Schmidt F, Ribi K, Haslbeck J, Urech C, Holm K, Eicher M. Adapting a peer-led self-management program for breast cancer survivors in Switzerland using a co-creative approach. Patient Educ Couns. 2020;103(9):1780–1789. doi:10.1016/j.pec.2020.03.028
50. Farias AJ, Du XL. Association between out-of-pocket costs, race/ethnicity, and adjuvant endocrine therapy adherence among medicare patients with breast cancer. J Clin Oncol. 2017;35(1):86–95. doi:10.1200/jco.2016.68.2807
51. Neugut AI, Zhong X, Wright JD, Accordino M, Yang J, Hershman DL. Nonadherence to medications for chronic conditions and nonadherence to adjuvant hormonal therapy in women with breast cancer. JAMA Oncol. 2016;2(10):1326–1332. doi:10.1001/jamaoncol.2016.1291
52. Yang J, Neugut AI, Wright JD, Accordino M, Hershman DL. Nonadherence to oral medications for chronic conditions in breast cancer survivors. J Oncol Pract. 2016;12(8):e800–809. doi:10.1200/jop.2016.011742
53. Tan EH, Wong ALA, Tan CC, et al. Improving medication adherence with adjuvant aromatase inhibitor in women with breast cancer: a randomised controlled trial to evaluate the effect of short message service (SMS) reminder. Breast. 2020;53:77–84. doi:10.1016/j.breast.2020.06.012
54. Conley CC, Bishop BT, Andersen BL. Emotions and emotion regulation in breast cancer survivorship. Healthcare. 2016;4(3):56. doi:10.3390/healthcare4030056
55. Yi JC, Syrjala KL. Anxiety and depression in cancer survivors. Med Clin North Am. 2017;101(6):1099–1113. doi:10.1016/j.mcna.2017.06.005
56. Bilodeau K, Tremblay D, Durand MJ. Exploration of return-to-work interventions for breast cancer patients: a scoping review. Support Care Cancer. 2017;25(6):1993–2007. doi:10.1007/s00520-016-3526-2
57. Porro B, Campone M, Moreau P, Roquelaure Y. Supporting the return to work of breast cancer survivors: from a theoretical to a clinical perspective. Int J Environ Res Public Health. 2022;19(9):5124. doi:10.3390/ijerph19095124
58. Kang NE, Kim HY, Kim JY, Kim SR. Relationship between cancer stigma, social support, coping strategies and psychosocial adjustment among breast cancer survivors. J Clin Nurs. 2020;29(21–22):4368–4378. doi:10.1111/jocn.15475
59. Erol Ursavaş F, Karayurt Ö. Effects of a roy’s adaptation model-guided support group intervention on sexual adjustment, body image, and perceived social support in women with breast cancer. Cancer Nurs. 2021;44(6):E382–e394. doi:10.1097/ncc.0000000000000854
60. Morales-Sánchez L, Luque-Ribelles V, Gil-Olarte P, Ruiz-González P, Guil R. Enhancing self-esteem and body image of breast cancer women through interventions: a systematic review. Int J Environ Res Public Health. 2021;18(4):1640. doi:10.3390/ijerph18041640
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.