")
Back to Journals » Patient Preference and Adherence » Volume 17
Self-Efficacy as Moderator and Mediator Between Medication Beliefs and Adherence in Elderly Patients with Type 2 Diabetes
Authors Wu J, Shen J, Tao Z, Song Z, Chen ZL
Received 27 October 2022
Accepted for publication 7 January 2023
Published 21 January 2023 Volume 2023:17 Pages 217—226
DOI https://doi.org/10.2147/PPA.S382362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jianbo Wu, Jie Shen, Zhujun Tao, Zhongjuan Song, Zhi-Long Chen
Department of Pharmacy, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China
Correspondence: Jie Shen; Zhi-Long Chen, Email [email protected]; [email protected]
Purpose: Poor antidiabetic medication adherence remains a great barrier to effective diabetes self-management among aging adults. This study investigates the mediation and moderation effects of self-efficacy on the relationship between medication beliefs and adherence in elderly patients with type 2 diabetes.
Methods: This cross-sectional study evaluated a sample of 309 hospitalized elderly patients who completed the assessment of medication beliefs, self-efficacy for medication uses and medication adherence in a tertiary hospital in Shanghai, China. A bootstrapping sampling method and hierarchical moderator regression analysis were used to verify the hypothesis of mediation and moderation effects of self-efficacy on the relationship between medication beliefs and adherence.
Results: Self-efficacy for medication use acted as a moderator (B=− 0.063, t=− 2.215, p=0.028) and partial mediator (CItotal effect=4.5– 16.63, p=0.001; CIindirect=1.524– 5.323, p=0.014; CIdirect=2.151– 11.817, p=0.001) on the relationship between general harm medication beliefs and medication adherence. Participants with lower general harm medication beliefs may develop higher self-efficacy, which, in turn, results in a higher level of medication adherence, and higher self-efficacy may attenuate the negative effect of high general harm medication beliefs on medication adherence.
Conclusion: Self-efficacy for medication use not only mediated the relationship between general harm beliefs about medication and medication adherence, but moderated it negatively. The findings of this study indicate an opportunity to improve the prognosis of elderly Chinese patients with type 2 diabetes through improved medication adherence by strengthening factors such as self-efficacy for appropriate medication use and general harm beliefs about medication.
Keywords: self-efficacy, medication adherence, medication belief, mediation effect, moderation effect, elderly patients
Introduction
Effective diabetes self-management (DSM) relies on patients’ essential care abilities, integrating adherence to complicated pharmacotherapy, skillful integration of a healthy diet, regular exercise, and self-monitoring of blood glucose.1 Medication adherence is a critical factor in DSM that contributes to optimal glycemic control, and poor medication adherence is associated with increased risks of hospitalization, mortality, and diabetic complications.2–5 Nevertheless, medication adherence in patients with diabetes appears to be suboptimal compared with patients with other chronic diseases.6–8 As such, nonadherence to antidiabetic regimens remains a great barrier to achieving promising outcomes in patients with diabetes.
Medication self-efficacy, defined as patients’ beliefs in their ability to follow prescribed medication regimens to achieve improved health outcomes, has been associated with patient-reported medication problems and adherence, and considered as an essential component of diabetes education programs.9,10 Studies indicated that self-efficacy is strongly correlated with medication adherence and glycemic control.11–15 As a social cognitive factor, medication self-efficacy was proved to mediate but not to moderate the relationship between numeracy, literacy, and diabetes medication adherence, and is an important mediator in the relationship between socio-demographic characteristics and medication adherence.16,17 Self-efficacy is also regarded as a type of perceived behavioral control, which impacts how an individual performs behaviors based on their perception of the tasks.18
Patients’ attitude and beliefs are regarded as social cognitive factors that influence their self-care behavior.19 In general, patients’ beliefs about medication include the general harm belief (which concerns the potential of medication to harm, and comprises representations of medication as harmful and the belief that people who take medicines should stop their treatment every now and again) and the general overuse belief (the notion that medicines are overprescribed by doctors, who place too much trust in them).20 Patients with more general harm and overuse medication beliefs have been proved to be less likely to adhere to medications.21,22 Stronger medication beliefs have been shown to be twice as likely to lead to high adherence (OR=1.98, p=0.006) and are regarded as a more powerful predictor of reported adherence than clinical and sociodemographic factors.23–28 However, despite the well-studied relationship between medication beliefs and adherence, little research has covered the relationship between medication beliefs and self-efficacy, or interrogated the pathway connecting medication beliefs, self-efficacy, and medication adherence. Testing indirect variable effects (ie, mediation) is important in studies, as these models provide deep insights into a definitive and plausible causal mechanism for designing effective interventions,29 while a moderating effect affects the direction and/or strength of the relationship between independent and dependent variables.30 If medication self-efficacy mediates the relationship between medication beliefs and adherence, then this relationship should become nonsignificant when self-efficacy is controlled. If medication self-efficacy moderates the relationship between medication beliefs and adherence, then this relationship should be attenuated for patients with a poor level of medication beliefs and strengthened for patients with a good level of medication beliefs.
Therefore, this study aimed to broaden our understanding of the impact of medication beliefs on medication adherence by examining the potential mediator and/or moderator effect of medicationself-efficacy. The recognition of such variables is important for the development of interventions that focus on improving patients’ self-care abilities in medication management.
Patients and Methods
Participants
This cross-sectional study, using a face-to-face interview, was conducted at a tertiary hospital in Shanghai, China, from July to December 2020. Participants were patients aged 65 years or older with type 2 diabetes who had been treated with antidiabetic agents for at least 3 months and were admitted to the internal medical unit, including the endocrinology department, nephrology department, respiratory department, gastrology department, neurology department, and cardiology department. Exclusion criteria included the following: patients with type 1 diabetes and other specific types of diabetes, diabetic ketoacidosis, or diabetic coma, and those who could not communicate by themselves or refused to accept the assessment.
Prior studies suggested that an adequate sample size for psychometric validations is 10 cases per parameter, and a sample size of 200 is sufficient to perform a path analysis.31,32 Hence, at least 250 patients were recruited for this study to account for loss of questionnaires or incompletely filled in or invalid questionnaires.
Outcome Measures
Medication Adherence
Medication adherence was evaluated using the Adherence to Refills and Medications Scale (ARMS).33 This study used the Chinese edition of ARMS, with permission from Sunil Kripalani, the author of the original ARMS. The measurement has been validated in elderly hospitalized Chinese patients, which indicated that the instrument has good internal consistency (Cronbach’s α=0.731–0.89) and high construct validity.34,35 The ARMS is a four-point Likert scale with 12 items. It contains eight items that assess adherence to taking medication correctly and four items that assess adherence to refilling medications on schedule. The total score on the ARMS ranges from 12 (best) to 48 (worst).
Self-Efficacy for Medication Use
Several measurements are available in clinical practice for evaluating medication self-efficacy, such as the Medication Understanding and Use Self-Efficacy Scale (MUSE),36 the Self-Efficacy for Appropriate Medication Use Scale (SEAMS),13 and the Long-Term Medication Behavior Self-Efficacy Scale (LTMBSES).37 Of these measurements, SEAMS was proposed as a tool to evaluate the medication self-efficacy owing to good evidence of its psychometric properties.38 The scale has been translated and validated in Chinese, Portuguese, and Arabic versions.39–41 The Chinese version of SEAMS has been proved to have good internal consistency (Cronbach’s α=0.768–0.915) and validity in evaluating medication self-efficacy in elderly hospitalized patients.35,39
This study used the Chinese version of SEAMS, with the permission of the scale’s originator, Jessica Risser. The measurement is a three-point Likert scale of 13 items, which evaluate the two dimensions of medication self-efficacy: self-efficacy for taking medications under difficult circumstances and self-efficacy for continuing to take medications when circumstances surrounding medication-taking are uncertain.39 Patients are asked to indicate their level of confidence with respect to taking medications correctly, and total scores range from 13 to 39, with higher scores indicating greater self-efficacy for appropriate medication use.
Patients’ Beliefs About Medicines
The Beliefs about Medication Questionnaire (BMQ) is the most commonly used measurement for evaluating medication beliefs, owing to its sound psychometric properties.20,42 This study adopted the Chinese edition of the Beliefs about Medicines Questionnaire – General (BMQ-G8) as a tool to assess patients’ beliefs on general medications.20 This validated Chinese edition of the BMQ-G8 was obtained from the originator of the scale, Professor Robert Horne. The BMQ-G8 has eight items on two subscales, namely General Overuse and General Harm, measured on a five-point Likert scale, with strongly disagree to strongly agree as the response to each scale item. Higher scores on each subscale represent stronger beliefs about the relevant beliefs about the medicine.
Data Collection
Scale scores and sociodemographic information, including age, gender, education level, health insurance, and the monthly household income, were collected by two qualified clinical pharmacists. All participants were approached and investigated within 24 hours after their admission to the hospital. Questionnaires were issued to the participants by investigators and completed by the participants themselves. One clinical pharmacist distributed the questionnaire, in the order of BMQ-G8, SEAMS, and ARMS, and the other checked the completion of the questionnaire and collected all three questionnaires on the spot. Participants were asked to answer the scales according to their actual medication habits before admission. Assistance was given if participants had difficulties understanding the scale items or giving item answers by themselves.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Ethics approval was obtained from the ethics committees of Huadong Hospital affiliated with Fudan University, China (2018k148). All of the participants gave their written informed consent before taking part in the study. All methods were performed in accordance with the relevant guidelines and regulations.
Statistical Methods
All statistical analyses were performed using AMOS 21.0 and SPSS Statistics 23.0, with an a priori level of 0.05 for statistical significance. Numerical variables are presented as the mean ± standard deviation, and categorical variables are presented as proportions.
Although the most widely used method for testing hypotheses about intervening variable effects is the causal steps approach by Baron and Kenny, MacKinnon and co-workers indicated that the approach is regarded as being among the lowest in power.30,43,44 The Sobel test may be a new analytical approach to inference about intervening variable effects, but it has a major flaw in that it requires the assumption that the sampling distribution of the indirect effect is normal.45,46 Bootstrapping is more powerful than the Sobel test and the causal steps approach to testing intervening variable effects.29 Therefore, bootstrapping for testing the hypothesis about the mediating role of self-efficacy for medication use, and a 95% percentile-based bootstrap confidence interval based on 2000 bootstrap samples, were adopted in this data analysis, as suggested by Hayes.47 The conceptual framework used in this study was adapted from the framework by Bailey et al, which demonstrates the possible relationship among medication beliefs, self-efficacy for medication use, and medication adherence.19
The moderator effect of self-efficacy was tested using hierarchical moderator regression analysis. To reduce the potential effects of multicollinearity, all variables were standardized. The technique of least squares was used, with the main effects in step 1 (general harm beliefs, general overuse beliefs, self-efficacy for medication use) and the interaction and moderators in step 2.
Results
Demographic Characteristics
The study inclusion criteria were met by 309 patients, and all of these patients completed the survey (Table 1). The majority of participants were male (145/309, 46.9%), with a mean age of 73.84±6.93 years. Over half (55.3%, 171/309) of the participants had completed senior high school education or above. The mean time since diabetes was diagnosed was 13.09±9.31 years. On average, the participants took 2.03±0.88 antidiabetic medications, with a mean HbA1c level of 8.09±1.69%. Almost two-thirds of the participants only took oral diabetes medicines (59.9%, 185/309) and 27.8% of the participants (86/309) took both insulin and oral diabetes medicines.
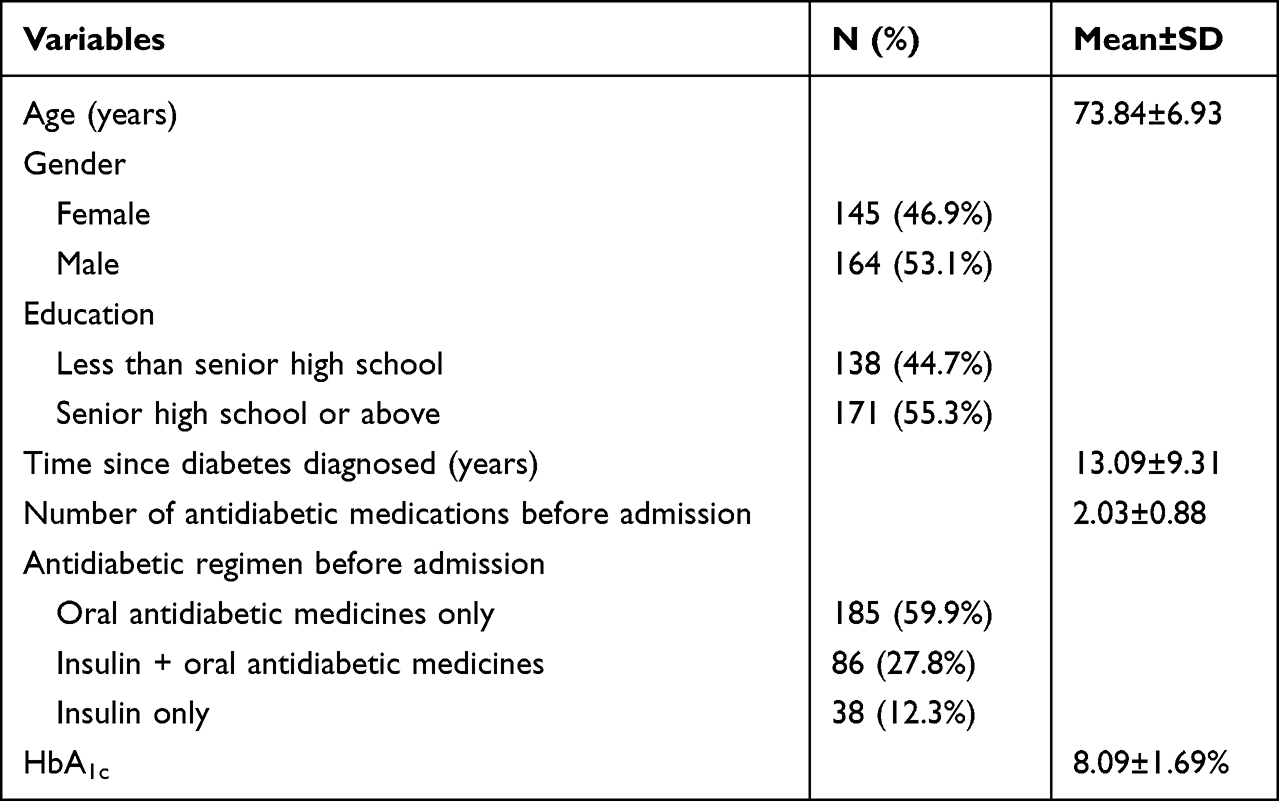 |
Table 1 Participants’ Characteristics (n=309) |
Descriptive Statistics and Correlations Among Variables in the Study
Based on the ARMS, 79.6% (246/309) of the participants reported adequate medication adherence. On average, participants had good self-reported medication adherence (mean=14.68; SD=3.09). Participants also reported moderate self-reported medication general overuse beliefs (mean=2.39; SD=0.54) and general harm beliefs (mean=2.69; SD=0.45), but inadequate self-efficacy for appropriate medication use (192/309, 62.1%). Patients who possessed higher medication self-efficacy had better medication adherence, and lower general medication overuse beliefs and harm beliefs. The participants with higher general medication overuse beliefs and harm beliefs showed lower medication self-efficacy and medication adherence (Table 2).
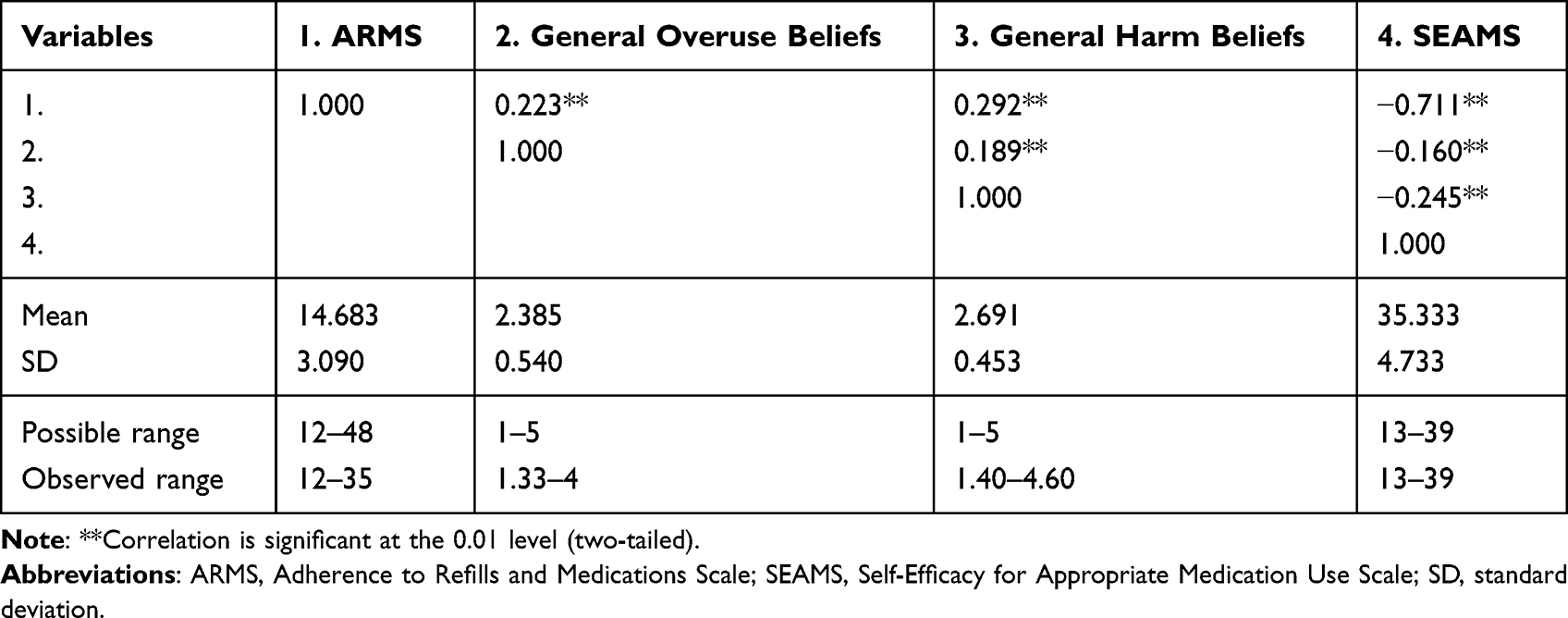 |
Table 2 Descriptive Statistics and Correlations Among Variables in the Study |
Test of the Mediation Effect of Medication Self-Efficacy on the Relationship Between General Overuse/General Harm and Medication Adherence
The total effect of general harm beliefs on medication adherence is significant, in that the effect is not zero with 95% confidence (CI=4.5–16.63, p=0.001), while the general overuse beliefs is not significant (CI=−1.786–1.763, p=0.935) (Table 3). The indirect and direct effects of general harm beliefs on medication adherence through self-efficacy for medication use are also significant (CIindirect=1.524–5.323, p=0.014; CIdirect=2.151–11.817, p=0.001), while the general overuse belief is not (CIindirect=−0.834–0.846, p=0.919; CIdirect=−1.330–1.423, p=0.977). Because both direct and indirect effects of general harm beliefs on medication adherence through self-efficacy for medication use are significant, the self-efficacy for medication use plays a partial mediator role in this relationship. But the mediating role is not presented in the relationship between general overuse beliefs and medication adherence. Figure 1 shows the mediation model of self-efficacy for medication use on the relationship between medication beliefs and adherence. As a result, the fit indices indicated that the mediating model fit the data well (χ2/df=1.788, goodness of fit index [GFI]=0.965, comparative fit index [CFI]=0.946, standardized root mean square residual [SRMR]=0.050, and root mean square error of approximation [RMSEA] =0.051]).48 Patients having high general harm beliefs may directly lead to less medication adherence; meanwhile, this can also result in poorer self-efficacy for medication use, which has a negative impact on medication adherence.
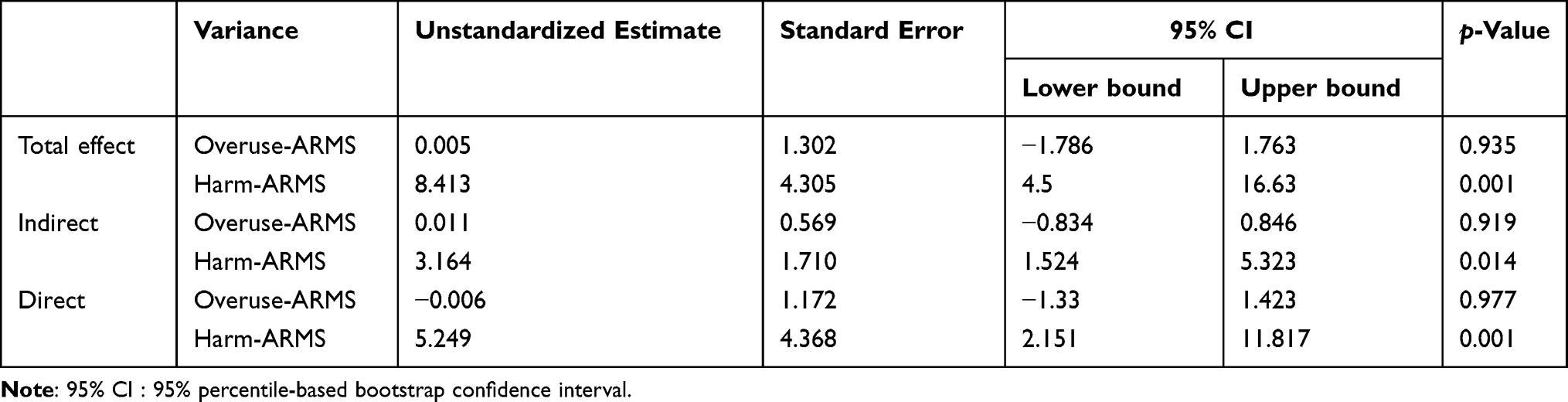 |
Table 3 Mediation Effect of Self-Efficacy on the Relationship Between Medication Adherence and Beliefs |
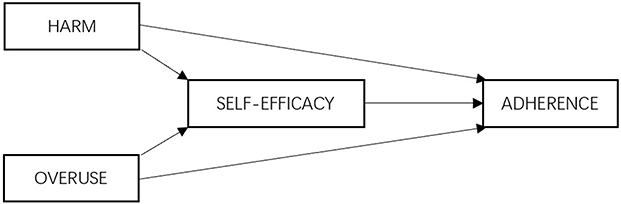 |
Figure 1 Conceptual path diagram of mediation model of self-efficacy for medication use on the relationship between medication beliefs and adherence. Bootstrapping for testing the hypothesis about the mediating role of self-efficacy for medication use, and a 95% percentile-based bootstrap confidence interval based on 2000 bootstrap samples, were adopted in the data analysis. |
Test of the Moderation Effect of Self-Efficacy on the Relationship Between General Overuse/General Harm and Medication Adherence
In the hierarchical moderator analysis, general harm beliefs (HB) (p=0.000), overuse beliefs (OU) (p=0.008), and self-efficacy for medication use (SE) (p=0.000) are significantly associated with medication adherence (MA). The associations are shown to be robust when the full model is specified in step 2 to assess the moderation hypothesis. Specifically, the main effects of HB and OU, as well as the hypothesized interaction term of HB×OU and the moderators of HB×SE, had significant associations with MA, while the moderators of OU×SE had no association with MA (Table 4).
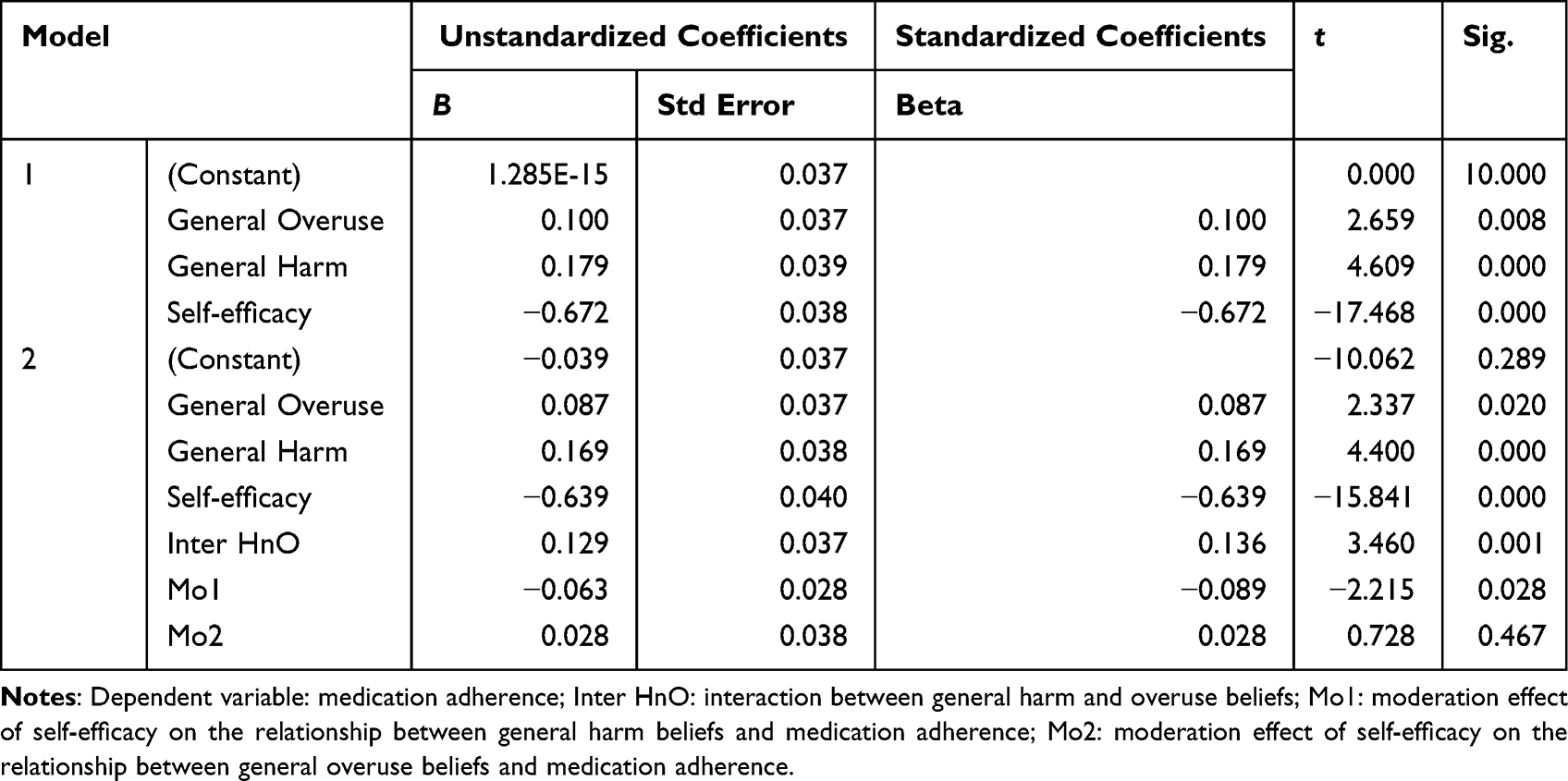 |
Table 4 Results of Hierarchical Moderation Regression Analyses |
The results indicate that SE serves as a (negative) moderator of the HB→MA relationship. The inclusion of the moderator and interaction terms (HB×SE, OU×SE, and HB×OU) in step 2 explained significant variance beyond step 1 (ΔR2=0.025, p<0.01). The fully specified model (ie, including steps 1 and 2) results in R2=0.785 (p<0.01). Overall, the moderation hypothesis was partially supported in the hierarchical regression analysis. Figure 2 shows the moderation model of self-efficacy for medication use on the relationship between medication adherence and beliefs.
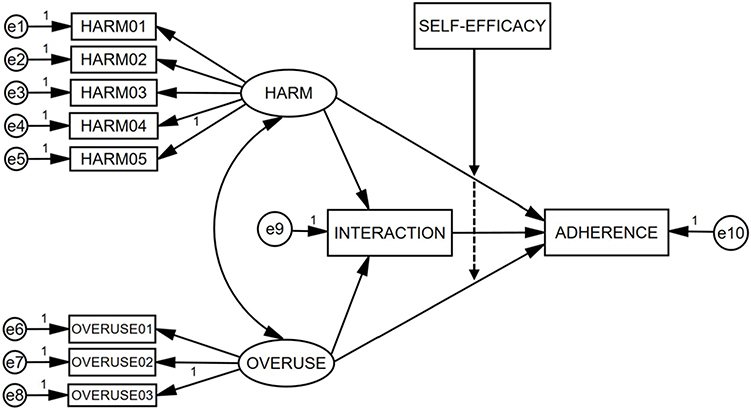 |
Figure 2 A conceptual model of general harm beliefs, general overuse beliefs, and medication adherence in patients’ medication self-management behavior. The moderation effect of patients’ self-efficacy for appropriate medication use was tested using hierarchical moderator regression analysis. SELF- EFFICACY stands for patients’ self-efficacy for appropriate medication use; HARM stands for general harm beliefs; OVERUSE stands for general overuse beliefs. |
Discussion
To our knowledge, this is the first study to illustrate the mediation and moderation effect of self-efficacy for medication use on the relationship between medication beliefs and adherence in elderly patients with type 2 diabetes. This study showed that a patient’s self-efficacy for medication use not only mediates the relationship of general harm beliefs with medication adherence, but moderates them negatively. As previous studies focused on the relationship between specific medication beliefs and medication adherence in China,42 the current study demonstrates that the general harm beliefs of medication are related to the self-efficacy for medication use, which, in turn, affects medication adherence. Moreover, self-efficacy for medication use can negatively moderate the negative impact of general harm beliefs on medication adherence.
As reported in other literature, this study also indicated that general harm beliefs and overuse beliefs about medicines are associated negatively with medication adherence.49–51 A number of studies have shown that medication adherence is negatively associated with general harm beliefs, while a few studies identified the negative association with general overuse beliefs.52,53 Horne et al and Armstrong and Swartzman indicated that cultural background influenced students’ views about the intrinsic nature of allopathic medicines.54,55 Students who identified themselves as Asian in origin were more likely than students with a European origin to perceive medicines as intrinsically harmful, but not so regarding their views about whether medicines are overused by doctors.54 Our study underpinned the hypothesis that the interaction between general harm beliefs and overuse beliefs is negatively associated with medication adherence. Considering that general overuse beliefs are not reported consistently significant with medication adherence, this may indicate that the direct effect of general overuse beliefs on medication adherence may not be predominant in elderly patients. Nevertheless, the establishment of communication and trust should also be an important consideration in healthcare interventions to enhance patients’ general overuse beliefs.
In addition to the relationship between general beliefs about medicines and medication adherence reported in recent studies, the present study reveals the important role of self-efficacy for medication use in the process of diabetes self-management in elderly patients. Self-efficacy refers to the belief or confidence in one’s capability to perform specific behaviors.12 As self-efficacy beliefs operate together with goals, outcome expectations, perceived environmental impediments, and facilitators in the regulation of human motivation, behavior, and well-being, the concept of self-efficacy has been widely used in medication practice and is regarded as a critical component of diabetes care.14,15,56–59 This study indicated that in addition to the mediation effect of general harm beliefs on medication adherence through self-efficacy for medication use, a moderation effect of self-efficacy for medication use on the relationship between general harm beliefs and medication adherence can also be found. This result highlights the need to identify a patient’s level of self-efficacy for medication use when pharmaceutical care is provided to elderly patients, and a tailored intervention should be developed and performed accordingly to maximize the effect on medication adherence. On the one hand, self-efficacy negatively moderates the relationship between general harm beliefs and medication adherence, and the effect of self-efficacy on medication adherence depends on the level of medication beliefs. As the literature reported that patients from Asian cultural backgrounds were significantly more likely to perceive medicines as being intrinsically harmful, it is important that improving self-efficacy for medication use can attenuate the negative effect of general harm beliefs on medication adherence, to a certain extent. On the other hand, self-efficacy for medication use partially mediates the relationship between general harm beliefs and medication adherence. The improvement of self-efficacy for medication use can result in better medication adherence, together with medication education targeting the medication beliefs of elderly patients. As a consequence, self-efficacy for medication use should be regarded as an essential part of any intervention in elderly patients with diabetes.
Limitations
This was a cross-sectional study measuring all variables from a single study visit, and several limitations should be noted in the study. First, we conducted this study from a single tertiary hospital in Shanghai, China. The study findings could have been more generalizable if we had adopted a varied population of diabetes patients and launched the study in more hospitals in China. Future research should involve a more diverse patient population (eg, patients from minority democratic autonomous regions in China and other ethnic populations) to determine whether our findings are applicable. Second, the participants recruited in this study were from the inpatient department; future research should also be implemented among the community residents, who are the basic core of society needing pharmaceutical care. Third, according to the methodological method used in our study, the outcome here may be confined to the population of our research.
Implications for Clinical Practice
The results from this study give a deep insight into the relationship among self-efficacy, medication adherence, and beliefs in elderly patients with type 2 diabetes. Tests on the mediating effect showed that self-efficacy can partially mediate the relationship between general harm beliefs and medication adherence, but the mediation effect is not shown between general overuse beliefs and medication adherence. Similarly, the results of hierarchical moderation regression also indicated that self-efficacy can only moderate the relationship between general harm beliefs and medication adherence negatively. This demonstrates the value of self-efficacy for medication use in improving medication adherence in elderly patients with poor medication beliefs, and the feasibility of implementing educational interventions on self-efficacy, tailored to the needs of these elderly patients.
Conclusion
The current study demonstrated that the general harm beliefs about medication are related to self-efficacy for appropriate medication use, which, in turn, affects medication adherence (mediation effect). Better self-efficacy for appropriate medication use can also strengthen the medication adherence by attenuating the effects of higher general harm beliefs about medication (moderation effect). The findings of this study indicate an opportunity to improve the prognosis of elderly Chinese patients with type 2 diabetes (ie, HbA1c or diabetic complications, etc) through improved medication adherence by strengthening factors such as self-efficacy for appropriate medication use and general harm beliefs about medication.
Funding
This work was financially supported by the China National Key Research and Development program (No. 2020YFC2009000&2020YFC2009001).
Disclosure
Dr Jie Shen reports grants from the China National Key R&D Program, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Montague MC, Nichols SA, Dutta AP. Self-management in African American women with diabetes. Diabetes Educ. 2005;31(5):700–711. doi:10.1177/0145721705280414
2. Rhee MK, Slocum W, Ziemer DC, et al. Patient adherence improves glycemic control. Diabetes Educ. 2005;31(2):240–250. doi:10.1177/0145721705274927
3. Nordwall M, Arnqvist HJ, Bojestig M, Ludvigsson J. Good glycemic control remains crucial in prevention of late diabetic complications--the Linkoping diabetes complications study. Pediatr Diabetes. 2009;10(3):168–176. doi:10.1111/j.1399-5448.2008.00472.x
4. Simpson SH, Lin M, Eurich DT. Medication adherence affects risk of new diabetes complications: a cohort study. Ann Pharmacother. 2016;50(9):741–746. doi:10.1177/1060028016653609
5. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med. 2006;166(17):1836–1841. doi:10.1001/archinte.166.17.1836
6. DiMatteo MR. Variations in patients’ adherence to medical recommendations. Med Care. 2004;42(3):200–209. doi:10.1097/01.mlr.0000114908.90348.f9
7. Elsous A, Radwan M, Al-Sharif H, Abu Mustafa A. Medications adherence and associated factors among patients with type 2 diabetes mellitus in the gaza strip, Palestine. Front Endocrinol (Lausanne). 2017;8. doi:10.3389/fendo.2017.00100
8. Joan N, Kalyango EO, Agatha P. Non-adherence to diabetes treatment at Mulago hospital in Uganda. Afr Health Sci. 2008;8(2):67–73.
9. Sleath B, Carpenter DM, Blalock SJ, et al. Development of a new diabetes medication self-efficacy scale and its association with both reported problems in using diabetes medications and self-reported adherence. Patient Prefer Adherence. 2016;10:1003–1010. doi:10.2147/PPA.S101349
10. Al-Khawaldeh OA, Al-Hassan MA, Froelicher ES. Self-efficacy, self-management, and glycemic control in adults with type 2 diabetes mellitus. J Diabetes Complications. 2012;26(1):10–16. doi:10.1016/j.jdiacomp.2011.11.002
11. D’Souza MS, Karkada SN, Parahoo K, Venkatesaperumal R, Achora S, Cayaban ARR. Self-efficacy and self-care behaviours among adults with type 2 diabetes. Appl Nurs Res. 2017;36:25–32. doi:10.1016/j.apnr.2017.05.004
12. Bandura A. The Explanatory and predictive scope of self-efficacy theory. J Soc Clin Psychol. 2011;4(3):359–373. doi:10.1521/jscp.1986.4.3.359
13. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the self-efficacy for appropriate medication use scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Meas. 2007;15(3):203–219. doi:10.1891/106137407783095757
14. McCulley C, Katz P, Trupin L, Yelin EH, Barton JL. Association of medication beliefs, self-efficacy, and adherence in a diverse cohort of adults with rheumatoid arthritis. J Rheumatol. 2018;45(12):1636–1642. doi:10.3899/jrheum.171339
15. Huang YM, Shiyanbola OO, Smith PD. Association of health literacy and medication self-efficacy with medication adherence and diabetes control. Patient Prefer Adherence. 2018;12:793–802. doi:10.2147/PPA.S153312
16. Huang YM, Shiyanbola OO, Chan HY. A path model linking health literacy, medication self-efficacy, medication adherence, and glycemic control. Patient Educ Couns. 2018;101(11):1906–1913. doi:10.1016/j.pec.2018.06.010
17. Xie Z, Liu K, Or C, Chen J, Yan M, Wang H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health. 2020;20(1):1227. doi:10.1186/s12889-020-09274-4
18. Ajzen I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior1. J Appl Soc Psychol. 2002;32(4):665–683. doi:10.1111/j.1559-1816.2002.tb00236.x
19. Bailey SC, Brega AG, Crutchfield TM, et al. Update on health literacy and diabetes. Diabetes Educ. 2014;40(5):581–604. doi:10.1177/0145721714540220
20. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14:1–24. doi:10.1080/08870449908407311
21. Ruksakulpiwat S, Liu Z, Yue S, Fan Y. The association among medication beliefs, perception of illness and medication adherence in ischemic stroke patients: a cross-sectional study in China. Patient Prefer Adherence. 2020;14:235–247. doi:10.2147/PPA.S235107
22. Shahin W, Kennedy GA, Cockshaw W, Stupans I. The effect of acculturation and harm beliefs on medication adherence on middle eastern hypertensive refugees and migrants in Australia. Int J Clin Pharm. 2021;43(5):1283–1292. doi:10.1007/s11096-021-01248-9
23. Al-Noumani H, Wu JR, Barksdale D, Knafl G, AlKhasawneh E, Sherwood G. Health beliefs and medication adherence in omanis with hypertension. J Cardiovasc Nurs. 2018;33(6):518–526. doi:10.1097/JCN.0000000000000511
24. Britten N. Patients’ ideas about medicines: a qualitative study in a general practice population. Br J Gen Pract. 1994;44(387):465–468.
25. Lorish CD, Richards B, Brown S
26. Conrad P. The meaning of medications: another look at compliance. Soc Sci Med. 1985;20(1):29–37. doi:10.1016/0277-9536(85)90308-9
27. Morgan M, Watkins CJ. Managing hypertension: beliefs and responses to medication among cultural groups. Sociol Health Illn. 1988;10(4):561–578. doi:10.1111/1467-9566.ep10837256
28. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
29. Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7(4):422–445. doi:10.1037/1082-989X.7.4.422
30. Baron MR, Kenny AD. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1171–1182. doi:10.1037/0022-3514.51.6.1173
31. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas. 2013;73(6):913–934. doi:10.1177/0013164413495237
32. Sideridis G, Simos P, Papanicolaou A, Fletcher J. Using structural equation modeling to assess functional connectivity in the brain: power and sample size considerations. Educ Psychol Meas. 2014;74(5):733–758. doi:10.1177/0013164414525397
33. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the Adherence to Refills and Medications Scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118–123. doi:10.1111/j.1524-4733.2008.00400.x
34. Chen YJ, Chang J, Yang SY. Psychometric evaluation of Chinese version of adherence to refills and medications scale (ARMS) and blood-pressure control among elderly with hypertension. Patient Prefer Adherence. 2020;14:213–220. doi:10.2147/PPA.S236268
35. Wu J, Tao Z, Qian C, Song Z, Shen J. Validation and psychometric properties of the adherence to refills and medications scale in elderly Chinese patients. Chin J Pharmacoepidemiol. 2021;30(10):706–712.
36. Cameron KA, Ross EL, Clayman ML, et al. Measuring patients’ self-efficacy in understanding and using prescription medication. Patient Educ Couns. 2010;80(3):372–376. doi:10.1016/j.pec.2010.06.029
37. De Geest S, Abraham I, Gemoets H, Evers G. Development of the long-term medication behaviour self-efficacy scale: qualitative study for item development. J Adv Nurs. 1994;19(2):233–238. doi:10.1111/j.1365-2648.1994.tb01076.x
38. Lamarche L, Tejpal A, Mangin D. Self-efficacy for medication management: a systematic review of instruments. Patient Prefer Adherence. 2018;12:1279–1287. doi:10.2147/PPA.S165749
39. Dong XF, Liu YJ, Wang AX, Lv PH. Psychometric properties of the Chinese version of the self-efficacy for appropriate medication use scale in patients with stroke. Patient Prefer Adherence. 2016;10:321–327. doi:10.2147/PPA.S101844
40. Alhazzani H, AlAmmari G, AlRajhi N, et al. Validation of an Arabic version of the self-efficacy for appropriate medication use scale. Int J Environ Res Public Health. 2021;18:22. doi:10.3390/ijerph182211983
41. Pedrosa RB, Rodrigues RC. Adaptation and evaluation of the measurement properties of the Brazilian version of the self-efficacy for appropriate medication adherence scale. Rev Lat Am Enfermagem. 2016;24:e2692. doi:10.1590/1518-8345.0167.2692
42. Nie B, Chapman SCE, Chen Z, Wang X, Wei L. Utilization of the beliefs about medicine questionnaire and prediction of medication adherence in China: a systematic review and meta-analysis. J Psychosom Res. 2019;122:54–68. doi:10.1016/j.jpsychores.2019.03.184
43. Fritz M, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–239. doi:10.1111/j.1467-9280.2007.01882.x
44. MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi:10.1037/1082-989X.7.1.83
45. Bollen KA, Stine R. Direct and indirect effects: classical and bootstrap estimates of variability. Sociol Methodol. 1990;20:115–140. doi:10.2307/271084
46. Stone C, Sobel M. The robustness of estimates of total indirect effects in covariance structure models estimated by maximum. Psychometrika. 1990;55(2):337–352. doi:10.1007/BF02295291
47. Hayes AF. Beyond baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr. 2009;76(4):408–420. doi:10.1080/03637750903310360
48. Schreiber JB. Core reporting practices in structural equation modeling. Res Social Adm Pharm. 2008;4(2):83–97.
49. Wei L, Champman S, Li X, et al. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: a cross-sectional study in China. BMJ Open. 2017;7(10):e017293. doi:10.1136/bmjopen-2017-017293
50. Sweileh WM, Zyoud H, Abu Nab’a RJ, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14:94. doi:10.1186/1471-2458-14-94
51. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud TJ. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 2018;12:1687–1698. doi:10.2147/PPA.S169236
52. Fischer W, Brandstetter S, Brandl M, et al. Specific, but not general beliefs about medicines are associated with medication adherence in patients with COPD, but not asthma: cohort study in a population of people with chronic pulmonary disease. J Psychosom Res. 2018;107:46–52. doi:10.1016/j.jpsychores.2018.02.004
53. Olorunfemi O, Ojewole F. Medication belief as correlate of medication adherence among patients with diabetes in Edo State, Nigeria. Nursing Open. 2019;6(1):197–202. doi:10.1002/nop2.199
54. Horne R, Graupner L, Frost S, Weinman J, Wright SM, Hankins M. Medicine in a multi-cultural society: the effect of cultural background on beliefs about medications. Soc Sci Med. 2004;59(6):1307–1313. doi:10.1016/j.socscimed.2004.01.009
55. Armstrong TL, Swartzman LC. Asian versus western differences in satisfaction with western medical care: the mediational effects of illness attributions. Psychol Health. 1999;14(3):403–416. doi:10.1080/08870449908407337
56. Cao Y, Chen W, Zhang S, et al. Development and preliminary evaluation of psychometric properties of A tuberculosis self-efficacy scale (TBSES). Patient Prefer Adherence. 2019;13:1817–1827. doi:10.2147/PPA.S208336
57. Du C, Wu S, Liu H, Hu Y, Li J. Correlation of long-term medication behaviour self-efficacy with social support and medication knowledge of kidney transplant recipients. Int J Nurs Sci. 2018;5(4):352–356. doi:10.1016/j.ijnss.2018.09.009
58. Merluzzi TV, Martinez Sanchez MA. Assessment of self-efficacy and coping with cancer: development and validation of the Cancer Behavior Inventory. Health Psychol. 1997;16(2):163–170. doi:10.1037/0278-6133.16.2.163
59. Sleath B, Blalock SJ, Robin A, et al. Development of an instrument to measure glaucoma medication self-efficacy and outcome expectations. Eye. 2010;24(4):624–631. doi:10.1038/eye.2009.174
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.