")
Back to Journals » Clinical Interventions in Aging » Volume 9
Self-care telephone talks as a health-promotion intervention in urban home-living persons 75+ years of age: a randomized controlled study
Authors Sundsli K , Söderhamn U , Espnes GA, Söderhamn O
Received 14 October 2013
Accepted for publication 13 November 2013
Published 6 January 2014 Volume 2014:9 Pages 95—103
DOI https://doi.org/10.2147/CIA.S55925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Kari Sundsli,1,2 Ulrika Söderhamn,2 Geir Arild Espnes,3 Olle Söderhamn2
1Department of Social Work and Health Science, Faculty of Social Sciences and Technology Management, Norwegian University of Science and Technology, Trondheim, Norway; 2Centre for Caring Research – Southern Norway, University of Agder, Grimstad, Norway; 3Research Centre for Health Promotion and Resources, Department of Social Work and Health Science, Faculty of Social Sciences and Technology Management, Norwegian University of Science and Technology, Trondheim, Norway
Aim: The aim of this study was to evaluate the effects of a telephone-based self-care intervention among urban living individuals 75+ years of age by comparing self-reported perceived health, mental health, sense of coherence, self-care ability, and self-care agency before and after the intervention.
Materials and methods: In a randomized controlled study, 15 persons answered a questionnaire about perceived health, mental health, sense of coherence, self-care ability, and self-care agency. In a sex- and age-matched control group (n=15), the same questions were answered. Data were collected before and after intervention. An open-ended question about experiences of the intervention was included in the last questionnaire. The intervention consisted of a first meeting with health professionals and additional five self-care telephone calls. The control group did not receive any intervention or attention except for the questionnaires. Descriptive statistics were used to describe the study group. To compare the intervention group and control group on nominal and ordinal levels, the McNemar test and the Wilcoxon signed-rank test, respectively, were chosen.
Results: Thirty individuals (14 females and 16 males) participated in the study, ranging in age between 75 and 93 years. A significant difference was obtained in the intervention group regarding mental health. Mental health improved significantly in the intervention group (P=0.037). In the control group, mental health, sense of coherence, self-care ability, and self-care agency showed worse outcome results after the intervention (19 weeks).
Conclusion: Self-care telephone talks improved mental health significantly in our sample, and mental health focus could be understood as a possible condition for health promotion to take place. Structured self-care telephone talks have proved to be successful and a relevant method to use in practice.
Keywords: case-control study, changes, mental health, older people
Introduction
Self-care might be considered a health-promoting activity for the purpose of maintaining, restoring, or improving health and well-being.1–3 Studies on self-care show a health decline in people older than 75 years.4,5 Results from these studies, combined with ongoing research on population aging internationally,6–8 as well as political discussions on future health policy for older people,9–11 highlight the necessity to develop an intervention that promotes self-care in older people that enables them to live their lives in their own homes as long as possible.3,4,12 In a Norwegian context, however, there were no such studies found that encompass the aim of this study.
Aim and hypothesis
The aim of this study was to evaluate the effects of a telephone-based self-care intervention among urban-living individuals 75+ years of age by comparing self-reported perceived health, mental health, sense of coherence, self-care ability, and self-care agency before and after the intervention. The hypothesis was that the effect of such a self-care intervention would bring about a positive outcome.
Background
Self-care is what the person does for himself, by himself, or with help from others, to obtain health and well-being.2 Two important factors promoting self-care in older people 75+ years of age are self-care agency and frequency of physical activity.4 These results accompany studies on the importance of physical activity in older age,13–16 as well as the importance of keeping up with activities for self-care.8,17–19
Three Norwegian studies3,4,12 upon which the current study is based point out significant results concerning self-care among urban-living older people and the ability to live their lives in their own homes.
A quantitative study on ability for self-care in older home-dwelling people in urban areas (n=1044)4 showed that a majority of the respondents perceived themselves as being in good health (87.2%). Most of the participants were in good mental health, as measured by Goldberg’s General Health Questionnaire (GHQ-30). However, some experiences in life can hardly be covered in an instrument. Mental health in old age might be influenced by life changes or losses of former roles, such as being a husband or wife or being gainfully employed, as well as physical or mental changes that occur as people age.3,12
To have good mental health is an important issue in older people’s abilities to handle their everyday lives in their own homes. For the participants 75+ years of age, in the quantitative study on ability for self-care in older home-dwelling people in urban areas, promoting factors for self-care ability were self-care agency, perceived good health, being active, being frequently physically active, and being satisfied with life. Perceived helplessness, being anxious, advanced age, and receiving home nursing were negative factors for self-care ability. One of the strongest factors for lower self-care ability among people 75–84 years of age was reduced mental health, measured by the GHQ-30.4
A study on lived experiences of self-care among older physically active urban-living individuals3 revealed findings of concern for what self-care might bring forth. The participants in that study lived active everyday lives and were frequently physically active. They were part of a supportive, inclusive, and promoting fellowship, and they had the opportunity to travel. They utilized their competence, and experienced making themselves useful. It was a privilege to be part of a family life as a husband, wife, parent, and/or a grandparent. They acknowledged physical and mental limitations, yet they felt that they were in good health.3
In a study on being old and living alone in urban areas, self-care and the meaning of self-care and health on the perception of life situation and identity12 were characterized by strength, temporality, gratitude, autonomy, and natality. These characteristics show the capabilities of older people that society needs to acknowledge to a greater extent in planning for the current and upcoming older generation’s health situation.
Health promotion has been recognized as a key factor in active aging internationally, and is the process of enabling people to increase control over and to improve their health.20 Aron Antonovsky, the creator of the sense of coherence (SOC) concept, claimed that people’s life orientation will have an impact on health,21 where health is understood as a position on a health ease/disease continuum towards the healthy end.22 The SOC concept consists of the three dimensions: manageability, comprehensibility, and meaningfulness. All three dimensions relate to each other, and meaningfulness is the most important component.23 In this respect, along with the fact that SOC is about resources for health and problem solving, it is conceptually and empirically related to self-care.24
In response to population aging,25 and the fact that older people aged 75 years and above should focus on their self-care with the intention of living in their own homes as long as wanted,9,10 an intervention on self-care talks was established.26–28 Self-care talks developed by Teel and Leenerts26 capture some main topics with respect to self-care, ie, practicing healthy habits, building self-esteem, focusing on the positive, communicating, and building meaning. The self-care talks intervention was performed by using telephone calls for the purpose of improving self-care for older adults in caregiving roles. The implementation and testing of the intervention has shown improving results in caregivers’ awareness about self-care practices, as well as the intention to practice better self-care.26
Few studies can be found on phone calls as intervention in older urban home-living persons randomly chosen for the purpose of promoting self-care. On the other hand, there are several studies presenting results from intervention studies using phone calls to promote specific treatments29–31 or to improve health in people with various diseases.32–34
Materials and methods
Design and participants
This self-care intervention study had an experimental design and was based on a model of self-care for health promotion in aging described by Teel and Leenerts.26 The model consists of self-care telephone talk sessions, and was slightly modified and implemented with the purpose of enhancing self-care in an intervention group. The design of the intervention was grounded in the results of the aforementioned three self-care studies.3,4,12
The intervention group and a control group were randomly chosen among respondents from a larger study on self-care and health among older home-dwelling people in urban areas in southern Norway,4 which included 1,044 persons. The inclusion criteria in the current study were respondents living in a specific urban area and being 75+ years of age. A total of 284 persons met the criteria. In the specific urban area, there were two cities: city A and city B. In city A, there were 100 persons, and in city B, 184 persons who met the age criterion. A power analysis showed that 49 individuals were needed in each study group when a P-value of 0.05 was chosen with an effect size of 0.60 and a probability of 70%.
For the intervention group, a sample of 76 persons was randomly chosen from the individuals in city A, and 15 individuals answered a questionnaire at baseline. A group of 150 individuals in city B was randomly chosen from the group of 184 persons, and 64 individuals answered the questionnaire at baseline. The 15 individuals in the intervention group were age- and sex-matched with the individuals in city B (Figure 1).
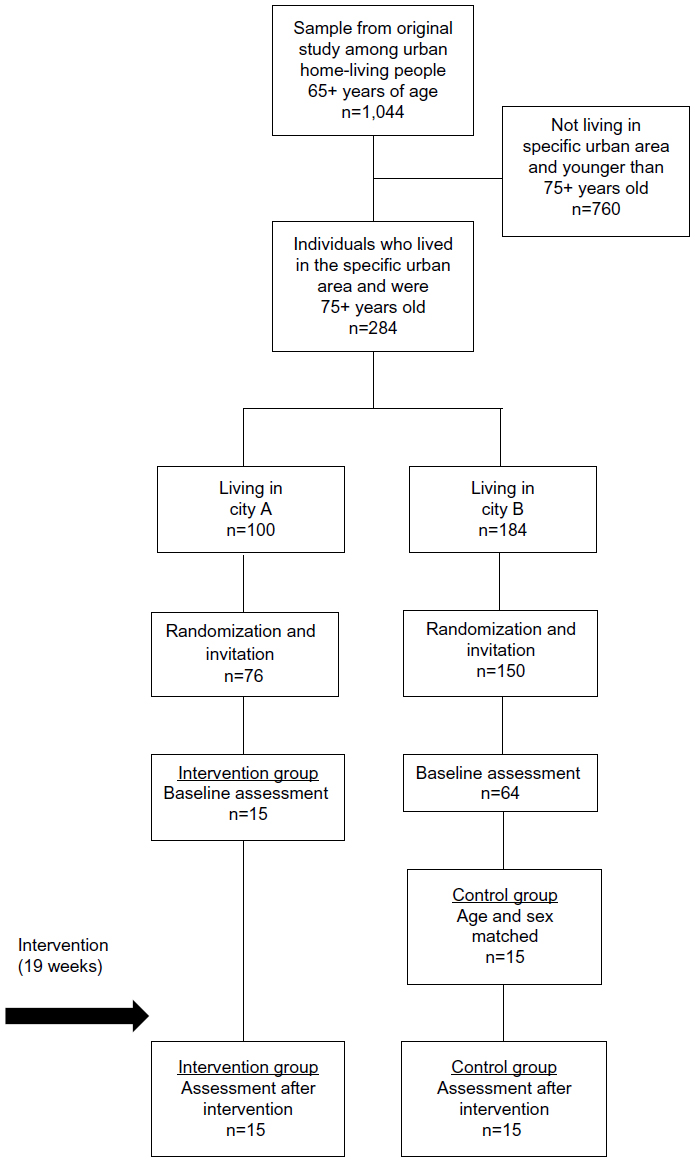 | Figure 1 Flow diagram of design and participants in the intervention study. |
Data collection
The self-report questionnaire used in the study consisted of four instruments, and background variables concerning age, sex, and perceived health. Data were collected at baseline and after the intervention, ie, after 19 weeks. Enclosed in the last questionnaire for the intervention group, an open-ended question about their experiences from the self-care telephone talks was asked: “Could you please narrate your experiences concerning the self-care telephone talks and what they have meant to you?”
The instruments
The Self-Care Ability Scale for the Elderly (SASE) is designed to measure perceived self-care ability, ie, the ability to maintain health and well-being.35,36 It is a 17-item Likert scale based on Pörn’s theory of health adaptedness.37 The items involve subjects/matters that may be of concern to older people, such as activities of daily living, mastery, well-being, volition, determination, loneliness, and dressing. Each item ranges from a score of 1 (“totally disagree”) to 5 (“totally agree”), and the total score ranges between 17 and 85, where a higher value indicates higher perceived self-care ability. A cutoff score ≥71 has been identified, indicating higher self-care ability, and a lower self-care ability for those with a score <71.35 Four items, negatively stated, are reversed in the summary of the scores. The SASE has been tested for reliability and validity,35,36,38,39 and Cronbach’s α-values between 0.68 and 0.89 have been reported.35,36,39
The Appraisal of Self-Care Agency (ASA) scale is a self-reporting instrument for the purpose of reporting the activation of power and engagement in self-care activities, and is based on Orem’s self-care deficit theory of nursing.2 It is a Likert-type scale with 24 items, where each item has five response categories ranging from 1 (“totally disagree”) to 5 (“totally agree”). The total score ranges from 24 to 120, with a higher score indicating greater self-care agency. Nine items are negatively stated and need to be reversed in the summation of the scores. The ASA instrument has been tested according to reliability and validity in several studies internationally.39–42 Among home-dwelling older people, Cronbach’s α-values between 0.72 and 0.86 have been reported,5 as well as 0.77 among older people with health problems.43
The Sense of Coherence (SOC-29) scale22 consists of 29 items measuring three dimensions of health, ie, comprehensibility, manageability, and meaningfulness. The scale is a semantic differential scale on the ordinal level with anchoring phrases, where the scores range from 1 to 7. The total score ranges from 29 to 203, where a higher score indicates a stronger SOC. Eleven items indicate comprehensibility, ten items indicate manageability, and eight items indicate meaningfulness. Thirteen items are negatively stated, and need to be reversed in the summation of the scores. The scale has been found to be a reliable and valid instrument, and has been used in several studies and in different languages.22,44–46 Cronbach’s α-values between 0.82 and 0.95 have been reported.45
Goldberg’s General Health Questionnaire (GHQ-30)47 is a 4-point Likert-type scale consisting of 30 items that aim to assess mental state, where 15 items are positively worded and 15 items are negatively worded. It is a summative scale, where the minimum score is 0 and the maximum score is 90, and where higher scores indicate more severe conditions. The GHQ-30 is widely accepted and a reliable scale for the purpose of establishing minor psychiatric disorders (such as anxiety, depression, social dysfunction, insomnia, lack of energy, inadequate coping, unhappiness, and feelings of incompetence) among general populations.47–49 The GHQ-30 is one of the most used instruments for the assessment of older people. The Norwegian version has been found to be a reliable and valid instrument for assessing the mental state of older home-living people, and has a Cronbach α-value of 0.92–0.93.50,51
Intervention
The organization of the intervention included two parts. The first part consisted of one gathering together with the participants (n=15) and the three health professionals who made the phone calls during the intervention, one co-researcher, and the project leader. The second part consisted of the five phone calls, which each participant received from their personal professional, for the purpose of enhancing self-care ability and self-care action among older persons.
The gathering
The purpose of this get-together was to provide information about the intervention as well as to meet, talk, and make appointments both with the health professionals and the participants. Materials for use throughout the intervention were handed out, knowledge about aging in general was taught, and results from the study in which they had all participated in 2010 were presented to them. However, meeting the health professionals face to face in advance of the phone call was assumed to improve the relationship between them.26,28
The self-care telephone talks
The three health professionals – two occupational therapists and one physiotherapist – were all well skilled in conversations for the purpose of promoting health in older people living in their own homes. In addition, they were inspired by the intention of motivational interviews,52 ie, a method to enhance personal motivation for change, beginning with the assumption and honoring of personal autonomy, ie, that people make their own behavioral choices, and that such power of choice cannot be appropriated by another.53 These skills were acquired over the years, and not for this intervention in particular.
Both health professionals and participants each received a folder where information and themes of every self-care telephone talk were listed, as well as a question for every theme upon which the participants were encouraged to reflect for the upcoming self-care talk. The themes were: 1) self-care habits, eating habits and nutrition, and physical activity, 2) health promotion, identity, and self-esteem, 3) roles and relationships, 4) communication, and 5) building meaning.26 These five themes were all grounded in the previous research on self-care that emphasized findings of importance: frequency in physical activity,3 eating habits and nutrition,54,55 taking part in supportive, inclusive, and promoting fellowships,3,56 being grateful for friends and family, and life situation, the situation of looking back, remembering earlier days, being grateful and appreciating the day, being forward-looking and being in change, planning for the future, as well as being generous and independent.12
Each self-care telephone talk lasted approximately 30 minutes. Before ending each conversation, the participants and their personal health professional wrote a plan for the next self-care talk. Every new session would start with an evaluation upon the previous theme.
Data analyses
Descriptive statistics were used to describe the study group. Ordinal data that consisted of the total scores of SASE, ASA, SOC-29, and GHQ-30 were presented with medians and interquartile ranges. Health was the only variable on the nominal level and was presented with numbers. To compare the two groups, the intervention group and the control group, on a nominal level, the McNemar test was chosen. For comparing the two groups on an ordinal level, the Wilcoxon signed-rank test was used. Statistical significance was defined as P<0.05. Some data were missing in some questionnaires. That appeared to be completely random, ie, questions were forgotten or not noticed or maybe participants did not want to answer one particular question. When up to five values were missing in the SASE, ASA, or SOC-29 instruments, a neutral score was put in the place of the missing values. For a specific individual, when there were more than five missing values in one scale, that particular scale was not included in the analyses for that individual. The data were analyzed with SPSS Statistics 19 (IBM, Armonk, NY, USA).
In relation to the open-ended question about the experiences on the self-care telephone talks, the participants’ answers were grouped according to their essential content.
Ethical considerations
The study was conducted with the approval of the Regional Committee for Medical Research Ethics in southern Norway (REK Sør-øst A: 2009/1321, REK Sør-øst D: 2011/2588), and was designed and implemented according to the Declaration of Helsinki57 and common principles used in clinical research.57,58 The participants were informed about the study by a written paper in addition to the questionnaire, and their written informed consent was requested. The participants were guaranteed anonymity and confidentiality.57
Results
Participants
Thirty individuals (14 females and 16 males) participated in the study, ranging in age between 75 and 93 years. Mean age in the randomly selected intervention group was 80.73 years (standard deviation 3.24), and in the age- and sex-matched control group was 80.73 years (standard deviation 4.20). There were no significant differences between the intervention group and the control group regarding self-reported perceived health or scores on SASE, ASA, SOC-29, and GHQ-30 at baseline (Table 1).
 | Table 1 Comparison between intervention group and control group at baseline |
Outcome of the intervention
In the intervention group (Table 2), there were no significant differences before and after intervention regarding self-reported health and scores on the SASE, ASA, and SOC-29 instruments. On the GHQ-30, a significant difference was obtained in the intervention group between baseline and intervention. The GHQ-30 score improved from a median of 24 to a median of 20 (P=0.037).
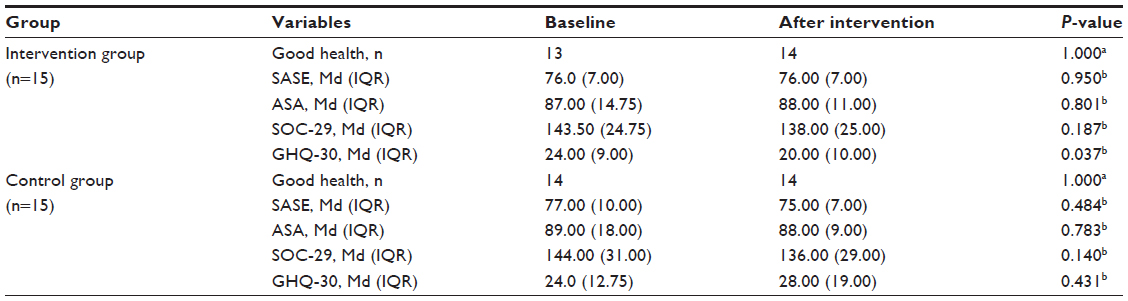 | Table 2 Measured variables in intervention group and control group at baseline and after intervention |
According to the open-ended question about the experience of the self-care telephone talks, all the participants were satisfied, and the majority experienced a change in their attitude and adjustment towards their self-care in everyday life. Through the self-care talks, how they thought about self-care as well as how they managed their daily life was acknowledged. They received support and encouragement for their self-care action.
The participants appreciated the confidentiality and anonymity of the talks, knowing they could talk freely about their concerns. In addition, the predictability of the phone calls was explained, in that every week there would be a nice talk with a health care professional. The participants obtained advice and suggestions about physical activity and food and meals, as well as practical adjustments for the future. The phone calls were described as pleasant and good-humored.
In the control group, no significant differences emerged between baseline and the assessment after intervention. However, all instruments – SASE, ASA, SOC-29, and GHQ-30 – showed worse outcome figures (Table 2).
Discussion
The results of this study show that in this sample, self-care telephone talks improved mental health significantly. These results support research from previous studies that reported mental health as an inevitable factor in older people’s self-care.3,4,59,60 Although this study was meant to have more participants, the results clearly show the importance of good mental health in relation to self-care actions.
Good mental health, measured by the GHQ-30, was one of the strongest factors for higher self-care ability among older people aged 75+ years of age in two previous studies.4,5 It seems that emotional reactions become less strong in older people and that they adapt more easily to changes in the environment than do their younger counterparts. In addition, they are better at adjusting goals and opportunities.59
The promotion of older peoples’ health and well-being should take into account their mental health and adjustment to changes in life. The results might indicate that the first change this intervention puts into effect is related to better mental health, and therefore could be understood as most likely being a condition for health promotion to take place in this study group. Why the control group had worse outcomes after intervention might be questioned. It is reasonable that a more or less natural decrease in self-care has taken place, although the time period was short. Maybe the participants also felt abandoned for not receiving any intervention. However, there were no differences between the groups at baseline, and they belonged to different geographical areas, which should indicate there was no connection between the two groups during intervention.
When testing their self-care talk method, Teel and Leenerts26 found that the participants acknowledged an increased awareness about self-care as the most important factor in promoting self-care practices. These results are in line with the experiences in the present study. The participants were acknowledged on how they thought upon self-care as well as how they managed their everyday life. During the self-care talks, they received support and encouragement on how to handle their coming years. They also experienced changes in their way of thinking about self-care, health, and well-being, and in their opportunity to live independent lives. Maybe it is reasonable to believe that those experiences, together with the contact with the professionals in the intervention, were important mechanisms for improvement in mental health. In addition, the self-care talks introduced suggestions for the participants according to physical activity, food and meals, as well as the importance of social fellowship and interaction. However, it seems that the most important message, according to the effect of self-care telephone talk intervention, is the improvement in the participants’ adjustment to self-care and their experiences of living healthy and good lives overall.
An initial meeting between the participants and the health professionals was important, and included an introduction to self-care telephone talks and conversations about content, as well as appointments being scheduled. Another essential feature was the expertise of the health professionals, comprising their health education and clinical knowledge, as well as practicing in health-promoting conversation, inspired by the idea of motivational interviews.52,53
In this intervention, there were five repeated phone calls. Each self-care telephone call had a special pattern, consisting of themes and goals for the week to come, as well as an evaluation of the last week’s achievements. This pattern might have had a positive influence on the participants, and thus one might assume it made their mental health improve. Both the participants and the health care professionals used the information folder. These guidelines seemed to be easy to use as well as providing a health-promotion attitude.
As previously mentioned, this study was meant to have more participants. Participating in research using self-reported questionnaires, as well as talking on the telephone, might be difficult for older adults with age-related changes in functions, such as vision and hearing losses.61 Using a less comprehensive questionnaire and fewer telephone calls might have increased the number of participants in the intervention group. On the other hand, questionnaires can be too simplistic for capturing the complexity of older persons’ views of a phenomenon.61 However, we believe that our questionnaire revealed important issues regarding the complexity in older persons’ lives. Fewer telephone calls could be required in a later study on self-care talks as a health-promotion intervention.
According to the relationship between the consequences and costs of a study, one might assume that the improvement in mental health in this study was high for a reasonable cost, compared to the control group. No cost–benefit analyses were implemented, but in future studies this would be interesting.
Conclusion
The hypothesis of this study was confirmed in that improved mental health was the effect of the self-care telephone talks. It could be assumed that improved mental health is critical for establishing self-care ability and self-care actions in older home-dwelling people.
The arrangement of the self-care telephone talks has proved to be successful, and a relevant method and tool to use in practice, where it should have an important role in plans for the upcoming older generation’s health and well-being, as well as their ability to live independent lives in their own homes. The next step in developing this intervention should be to identify possible barriers and facilitators, as well as to develop an implementation plan involving a larger group of participants in different counties in Norway. Future research may also include older participants living in sheltered housing facilities, as well as older people being in need of health care services. It is reasonable to assume that this kind of research and interventions are sensitive to local contextual factors, like physical and psychosocial issues in the population in focus.
Acknowledgments
We are grateful to all participants. We are grateful to the three health professionals – occupational therapists Berit Westbye and Grethe Ringdal, and physiotherapist Trygve Waldeland – who performed all of the self-care telephone talks and made the intervention complete. We thank the three municipalities - Grimstad kommune, Arendal kommune and Kristiansand kommune - for their willingness to cooperate. We also thank Cynthia Teel, Professor and Associate Dean, University of Kansas School of Nursing, for her generosity in sharing and making the original work on the self-care telephone talk intervention available to us.
Disclosure
The authors report no conflicts of interest in relation to this paper.
References
Söderhamn O. Potential for Self-Care: Assessing and Describing Self-Care Ability among Elderly People [dissertation]. Linköping, Sweden: Department of Medicine and Care, Division of Nursing Science Faculty of Health Sciences, Linköpings Universitet; 1998. | |
Orem DE. Nursing: Concepts of Practice. 6th ed. St Louis: Mosby; 2001. | |
Sundsli K, Espnes GA, Söderhamn O. Lived experiences of self-care among older physically active urban-living individuals. Clin Interv Aging. 2013;8:123–130. | |
Sundsli K, Söderhamn U, Espnes GA, Söderhamn O. Ability for self-care in urban living older people in southern Norway. J Multidiscip Healthc. 2012;5:85–95. | |
Söderhamn O, Lindencrona C, Ek AC. Ability for self-care among home dwelling elderly people in a health district in Sweden. Int J Nurs Stud. 2000;37(4):361–368. | |
Bohman DM, van Wyk NC, Ekman SL. South Africans’ experiences of being old and of care and caring in a transitional period. Int J Older People Nurs. 2011;6(3):187–195. | |
Bilotta C, Bowling A, Nicolini P, Casö A, Vergani C. Quality of life in older outpatients living alone in the community in Italy. Health Soc Care Community. 2011;20(1):32–41. | |
Clark F, Jackson J, Carlson M, et al. Effectiveness of a lifestyle intervention in promoting the well-being of independently living older people: results of the Well Elderly 2 randomised controlled trial. J Epidemiol Community Health. 2012;66(9):782–790. | |
Ministry of Health and Care Services. Report no 47 (2008–2009) to the Storting. The Coordination Reform. Oslo: Ministry of Health and Care Services; 2009. | |
Ministry of Health and Care Services. Report no 29 (2012–2013) to the Storting. The Care of Tomorrow. Oslo: Ministry of Health and Care Services; 2013. | |
World Health Organization. Why Urban Health Matters. Geneva: WHO; 2010. Available from: http://apps.who.int/iris/bitstream/10665/70230/1/WHO_WKC_WHD_2010.1_eng.pdf. Accessed January 23, 2013. | |
Sundsli K, Espnes GA, Söderhamn O. Being old and living alone in urban areas: the meaning of self-care and health on the perception of life situation and identity. Psychol Res Behav Manag. 2013;6:21–27. | |
Lohne-Seiler H, Torstveit MK, Anderssen SA. Traditional versus functional strength training: effects on muscle strength and power in the elderly. J Aging Phys Act. 2013;21(1):51–70. | |
Rennemark M, Lindwall M, Halling A, Berglund J. Relationships between physical activity and perceived qualities of life in old age. Results of the SNAC study. Aging Ment Health. 2009;13(1):1–8. | |
Lindwall M, Rennemark M, Berggren T. Movement in mind: the relationship of exercise with cognitive status for older adults in the Swedish National Study on Aging and Care (SNAC). Aging Ment Health. 2008;12(2):212–220. | |
Tse M, Wan V, Ho S. Physical exercise: does it help in relieving pain and increasing mobility among older adults with chronic pain? J Clin Nurs. 2011;20(5–6):635–644. | |
Clark F, Azen SP, Carlson M, et al. Embedding health-promoting changes into the daily lives of independent-living older adults: long-term follow-up of occupational therapy intervention. J Gerontol B Psychol Sci Soc Sci. 2001;56(1):P60–P63. | |
Dale B, Söderhamn U, Söderhamn O. Self-care ability among home-dwelling older people in rural areas in southern Norway. Scand J Caring Sci. 2012;26(1):113–122. | |
Söderhamn U, Dale B, Söderhamn O. The meaning of actualization of self-care resources among a group of older home-dwelling people – a hermeneutic study. Int J Qual Stud Health Well-being. 2013;8:20592. | |
World Health Organization. The Ottawa Charter for Health Promotion. 1986. Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/index1.html.Accessed March 11, 2013. | |
Eriksson M, Lindström B. Antonovsky’s sense of coherence scale and its relation with quality of life: a systematic review. J Epidemiol Community Health. 2007;61(11):938–944. | |
Antonovsky A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well. San Fransisco: Jossey-Bass; 1987. | |
Antonovsky A. Health, Stress and Coping. San Fransisco: Jossey-Bass; 1979. | |
Söderhamn U, Bachrach-Lindström M, Ek AC. Self-care ability and sense of coherence in older nutritional at-risk patients. Eur J Clin Nutr. 2008;62(1):96–103. | |
World Health Organization. Global Age-Friendly Cities: A Guide. Geneva: WHO; 2007. Available from: http://whqlibdoc.who.int/publications/2007/9789241547307_eng.pdf. Accessed October 2, 2013. | |
Teel CS, Leenerts MH. Developing and testing a self-care intervention for older adults in caregiving roles. Nurs Res. 2005;54(3):193–201. | |
Leenerts MH, Teel CS. Relational conversation as method for creating partnerships: pilot study. J Adv Nurs. 2006;54(4):467–476. | |
Leenerts MH, Teel CS, Pendleton MK. Building a model of self-care for health promotion in aging. J Nurs Scholarsh. 2002;34(4):355–361. | |
Zhang JE, Wong FK, You LM, Zheng MC. A qualitative study exploring the nurse telephone follow-up of patients returning home with a colostomy. J Clin Nurs. 2012;21(9–10):1407–1415. | |
Dale J, Caramlau I, Sturt J, Friede T, Walker R. Telephone peer-delivered intervention for diabetes motivation and support: the telecare exploratory RCT. Patient Educ Couns. 2009;75(1):91–98. | |
Smithies M, Bettger-Hahn M, Forchuk C, Brackstone M. Telephone contact intervention in women undergoing treatment for breast cancer. Can Oncol Nurs J. 2009;19(3):122–128. | |
Shearer NBC, Cisar N, Greenberg EA. A telephone-delivered empowerment intervention with patients diagnosed with heart failure. Heart Lung. 2007;36(3):159–169. | |
Sperber NR, Bosworth HB, Coffman CJ, et al. Participant evaluation of a telephone-based osteoarthritis self-management program, 2006–2009. Prev Chronic Dis. 2012;9:E73. | |
Walters JA, Cameron-Tucker H, Courtney-Pratt H, et al. Supporting health behaviour change in chronic obstructive pulmonary disease with telephone health-mentoring : insights from a qualitative study. BMC Fam Pract. 2012;13:55. | |
Tomstad ST, Söderhamn U, Espnes GA, Söderhamn O. Testing two self-care-related instruments among older home-dwelling people in Norway. Int J Older People Nurs. 2013;8(3):189–198. | |
Söderhamn O, Ek AC, Pörn I. The Self-Care Ability Scale for the Elderly. Scand J Occup Ther. 1996;3(2):69–78. | |
Pörn I. Health and adaptedness. Theor Med. 1993;14(4):295–303. | |
Söderhamn O. Health and the internal structure of the Self-Care Ability Scale for the Elderly (SASE). Scand J Occup Ther. 2001;8(2):67–71. | |
Söderhamn O, Lindencrona C, Ek AC. Validity of two self-care instruments for the elderly. Scand J Occup Ther. 1996;3:172–179. | |
van Achterberg T, Lorensen M, Isenberg MA, Evers GC, Levin E, Philipsen H. The Norwegian, Danish and Dutch version of the Appraisal of Self-Care Agency Scale; comparing reliability aspects. Scand J Caring Sci. 1991;5(2):101–108. | |
Evers GC, Isenberg MA, Philipsen H, Senten M, Brouns G. Validity testing of the Dutch translation of the appraisal of the self-care agency A.S.A.-scale. Int J Nurs Stud. 1993;30(4):331–342. | |
Lorensen M, Holter IM, Evers GC, Isenberg MA, van Achterberg T. Cross-cultural testing of the “appraisal of self-care agency: ASA scale” in Norway. Int J Nurs Stud. 1993;30(1):15–23. | |
Evers GCM. Appraisal of Self-Care Agency: ASA Scale. Assen, Netherlands: Van Gorcum; 1989. | |
Söderhamn O, Holmgren L. Testing Antonovsky’s sense of coherence (SOC) scale among Swedish physically active older people. Scand J Psychol. 2004;45(3):215–221. | |
Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36(6):725–733. | |
Eriksson M, Lindström B. Validity of Antonovsky’s sense of coherence scale: a systematic review. J Epidemiol Community Health. 2005;59(6):460–466. | |
Goldberg DP, Hillier VF. A scaled version of the General Health Questionnaire. Psychol Med. 1979;9(1):139–145. | |
Caplan RP. Stress, anxiety, and depression in hospital consultants, general practitioners, and senior health service managers. BMJ. 1994;309(6964):1261–1263. | |
Whittington J, Huppert FA. Creating invariant subscales of the GHQ-30. Soc Sci Med. 1998;46(11):1429–1440. | |
Dale B, Sævareid HI, Söderhamn O. Testing and using Goldberg’s General Health Questionnaire: mental health in relation to home nursing, home help, and family care among older, care-dependent individuals. Int J Ment Health Nurs. 2009;18(2):133–143. | |
Dale B, Söderhamn U, Söderhamn O. Psychometric properties of the Norwegian version of the General Health Questionnaire (GHQ-30) among older people living at home. Psychol Res Behav Manag. 2012(5):151–157. | |
Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. New York: Guilford; 2013. | |
Miller WR, Rollnick S. Ten things that motivational interviewing is not. Behav Cogn Psychother. 2009;37(2):129–140. | |
Tomstad ST, Söderhamn U, Espnes GA, Söderhamn O. Lived experiences of self-care among older, home-dwelling individuals identified to be at risk of undernutrition. J Multidiscip Healthc. 2012;5:319–327. | |
Tomstad S, Söderhamn U, Espnes O, Söderhamn O. Living alone, receiving help, helplessness, and inactivity are strongly related to risk of undernutrition among older home-dwelling people. Int J Gen Med. 2012;5:231–240. | |
Dale B, Söderhamn U, Söderhamn O. Life situation and identity among single older home-living people: a phenomenological-hermeneutic study. Int J Qual Stud Health Well-being. 2012;7:1–12. | |
World Medical Association. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. Fortaleza, Brazil: WMA; 2013. Available from: http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed November 4, 2013. | |
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 6th ed. New York: Oxford University Press; 2009. | |
Hansen T, Slagsvold B. [Age and quality of life: older people are satisfied with life – or is it just a figment of their imagination?] Samfunnsspeilet. 2009;23(1):95–99. Norwegian. | |
Kvaal K, McDougall FA, Brayne C, Matthews FE, Dewey ME. Co-occurrence of anxiety and depressive disorders in a community sample of older people: results from the MRC CFAS (Medical Research Council Cognitive Function and Ageing Study). Int J Geriatr Psychiatry. 2008;23(3):229–237. | |
Jacelon CS. Older adults’ participation in research. Nurse Res. 2007; 14(4):64–73. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.