")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Self-Care Practice and Associated Factors Among People Living with Type 2 Diabetes in Addis Ababa, Ethiopia: A Facility-Based Cross-Sectional Study
Authors Wolderufael M , Dereje N
Received 6 November 2020
Accepted for publication 4 December 2020
Published 6 January 2021 Volume 2021:14 Pages 1—9
DOI https://doi.org/10.2147/DMSO.S287352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Meklit Wolderufael,1 Nebiyu Dereje2
1Department of Medicine, Myungsung Medical College, Addis Ababa, Ethiopia; 2Department of Public Health, Myungsung Medical College, Addis Ababa, Ethiopia
Correspondence: Nebiyu Dereje
Department of Public Health, Myungsung Medical College, Addis Ababa 14972, Ethiopia
Tel +251978788638
Email [email protected]
Introduction: Diabetes is a global public health threat with a considerably high burden in low- and middle-income countries. The application of self-care practice by people living with diabetes helps to manage diabetes and its complications, and to lengthen their life. However, the level of diabetes self-care practice in Ethiopia is very low.
Methods: A cross-sectional study was conducted among people living with type 2 diabetes who were on follow-up from January 01 to 31, 2019 at Yekatit 12 Hospital. A systematic sampling technique was employed to recruit 354 study participants. A face-to-face interview was administered by trained data collectors using a structured questionnaire. Diabetes self-care practice was assessed by using Summary of Diabetes Self-Care Activities (SDSCA) scale. Multi-variable binary logistic regression analysis was carried out to identify factors associated with diabetes self-care practice.
Results: More than half (52.0%, 95% CI: 49.9% - 57.1%) of the people living with diabetes had poor diabetes self-care practice. Poor self-care practice was associated with being unemployed and retired (AOR= 3.57, 95% CI 1.65– 7.72), having diabetes for ≥ 10 years (AOR= 1.78, 95% CI 1.07– 2.95), having comorbidity (AOR= 2.15, 95% CI 1.35– 3.43), not owning glucometer (AOR= 1.81, 95% CI 1.16– 2.83), not receiving diabetes education (AOR= 1.95, 95% CI 1.20– 3.18) and dissatisfaction with social support (AOR= 4.24, 95% CI 1.25– 14.40).
Conclusion: Poor self-care practice was found to be substantial among people living with diabetes in Addis Ababa, with self-monitoring of blood glucose and regular exercise being the least performed. It is beneficial to focus more on lifestyle modifications and educating about the severity of the disease for better management of blood sugar levels and hindrance of complications.
Keywords: type 2 diabetes, self-care practice, diabetes education, Ethiopia
Background
Diabetes mellitus is a global public health problem with its prevalence rising from 108 million in 1980 to 463 million in 2019, with further rise to 700 million expected by 2045.1 More than three-quarters (79%) of the people with diabetes are living in low and middle income countries (LMICs).1 Diabetes was responsible for 4.2 million deaths and $760 billion dollars of health expenditure by the year 2019.2 In Ethiopia, it is estimated that 1.7 million people were living with diabetes in the year 2019.2
For optimal health outcomes and quality of life, the American Association of Diabetes Educators (AADE) model suggests self-care behaviors consist of an ongoing set of activities such as healthy coping, healthy eating, being active, taking medications, self-monitoring of blood glucose, reducing risk and problem solving.4 These well accepted activities are thought to prevent early occurrence of complications and lengthen the healthy life of people living with diabetes.3–5 However, previously conducted studies indicated that self-care activities vary extensively according to the nature of the activity itself; with exercise frequently falling below recommended levels.6–9
Self-care practice is usually provided by the people living with diabetes, themselves, or their families. It takes their own motivation to eat, exercise, stop smoking, take medication, test glucose levels and maintain a healthy body weight making blood sugar management entirely achieved by them. In a country like Ethiopia where there are limited resources, it would be economical to practice such kind of preventive measures to minimize the burden of the disease and the occurrence of complications. The level of self-care practice among people living with diabetes in Addis Ababa is not well understood. Moreover, factors associated with self-care practice were not well identified in Addis Ababa, Ethiopia. Therefore, this study was conducted with the aim of determining self-care practice and its associated factors among people living with diabetes in Addis Ababa, Ethiopia.
Materials and Methods
Study Setting and Recruitment of the Study Participants
A facility-based cross-sectional study was conducted among people living with type two diabetes who were on follow-up from January 01 to 31, 2019 at the Yekatit 12 Hospital. Yekatit 12 Hospital is one of the prominent public hospitals in Addis Ababa, with separate diabetes and hypertension follow-up clinics. People living with type two diabetes who were on follow-up in the out-patient departments (OPD) of the diabetes clinic during the study period were recruited to the study. Those who were 18 years or older, on diabetes treatment, with time of diagnosis of at least one year and with at least two OPD visits in the past one year, were included while those with hearing difficulty or unable to provide the required information were excluded.
Sample size for the magnitude of self-care practice was determined by using single population proportion by taking 95% confidence interval (CI), 5% margin of error and 52.3% of diabetes self-care practice in Addis Ababa.7 For the analytical component of the study (factors associated with self-care practice), sample size was determined by using two population proportion formula by taking 80% power, 95% CI, one to one ratio, 64% and 37% self-care practice among those with adequate and inadequate knowledge of diabetes, respectively. However, the sample size determined by the single population proportion formula (n = 354) was higher than that was determined by the two population proportion formula (n = 157). Thus, the higher sample size of 354 was used in this study. In the month prior to the study (November, 2018), there were a total of 664 people living with type 2 diabetes in the two OPDs of the hospital. Therefore, a systematic random sampling technique was employed to recruit every other people living with type 2 diabetes (sampling interval (K) = 2) on follow up in both OPDs. The first people living with type 2 diabetes were selected randomly. When the sampled participant did not consent, the next was selected.
Data Collection Procedures
A face to face interview was administered by trained nurses by using a structured questionnaire which was adopted from the Summary of Diabetes Self-Care Activities (SDSCA) diabetes self-care scale10 and diabetes knowledge questionnaire (DKQ).11 The tools are valid, reliable and have been previously used in different studies done in Ethiopia.7,8 The questionnaire has seven parts: socio-demographic characteristics, health status data, diabetes knowledge, health education, social support, diabetes self-care activities and medication adherence. The questionnaire was initially prepared in English then translated into the local language, Amharic. Consistency of the translation was checked by back translation. Ethical approval for the study was obtained from the Institutional Review Board of Myungsung Medical College and permission to conduct the study was obtained from Yekatit 12 Hospital. Prior to the data collection, information about the study was provided to the participants and written consent was obtained. The study was conducted in accordance with the Declaration of Helsinki.
Measurement of Variables
Regular exercise was defined in this study as moderate-intensity aerobic physical activity for at least 30 minutes at least 5 days a week or at least 150 min/week.12 Regular monitoring of blood glucose is defined as monitoring blood glucose at least once every week.9 Healthful eating plan was defined as limiting foods that are high in sugar, eating smaller portions spread out over the day, eating a variety of whole-grain foods, fruits and vegetables every day while consuming less fat and limiting use of alcohol and salt.13 Diabetes self-care practice of participants was assessed using the SDSCA diabetes self-care scale which includes behaviors such as diet plan, exercise, self-blood glucose testing and foot care practiced in the last seven days prior to the study.10 These four domains were used to assess diabetic self-care practices of participants for which frequency of each was measured. Following that, mean was calculated for each domain and categorized as adequate if above or equal to the mean and less adequate if below the mean. Then, overall mean of diabetic self-care practice was computed using the means of each domain dividing it by the number of domains. Accordingly, those who scored ≥3 had good self-care practice while those who scored <3 had poor self-care practice.7,8,14,15 Adequate knowledge of diabetes was defined as participants with correct answer to knowledge-related questions and scored above or equal to 50%.11 Optimal glycemic control was considered when the fasting blood sugar (FBS) was between 70–126mg/dL.9
Data Management and Analysis
The information that was obtained from the filled questionnaires was cleaned and entered in SPSS version 20.0 statistical software for analysis. Descriptive statistics were used to summarize the data by frequency, percentage, mean and standard deviation. The magnitude of poor diabetes self-care practice among the people living with type 2 diabetes was given in percentage and its respective 95% confidence interval. Factors associated with poor self-care practice among people living with type 2 diabetes were first identified by bivariate analysis using chi-square test and binary logistic regression. Those variables with p value <0.25 in the bivariate analysis were considered for further multi-variable binary logistic regression. The magnitude of association between the independent variables and poor diabetes self-care practice was determined by the odds ratio (OR) and 95% confidence interval. The level of statistical significance was set at 5% and p value of <0.05 was used as a cut-off point to ascertain statistically significant associations. Model fitness was checked by the Hosmer–Lemeshow goodness of fit test and no multi-collinearity was observed (VIF and tolerance test).
Results
Socio-Demographic and Clinical Characteristics
The mean age of the study participants was 62.2 years (±8.8 years). As indicated in Table 1, about half (49.4%) of the study participants were females. More than two-thirds (68.6%) of the participants were married and about one-third (33.6%) of the participants had a monthly family income of 1651–3200 ($US50 – 100).
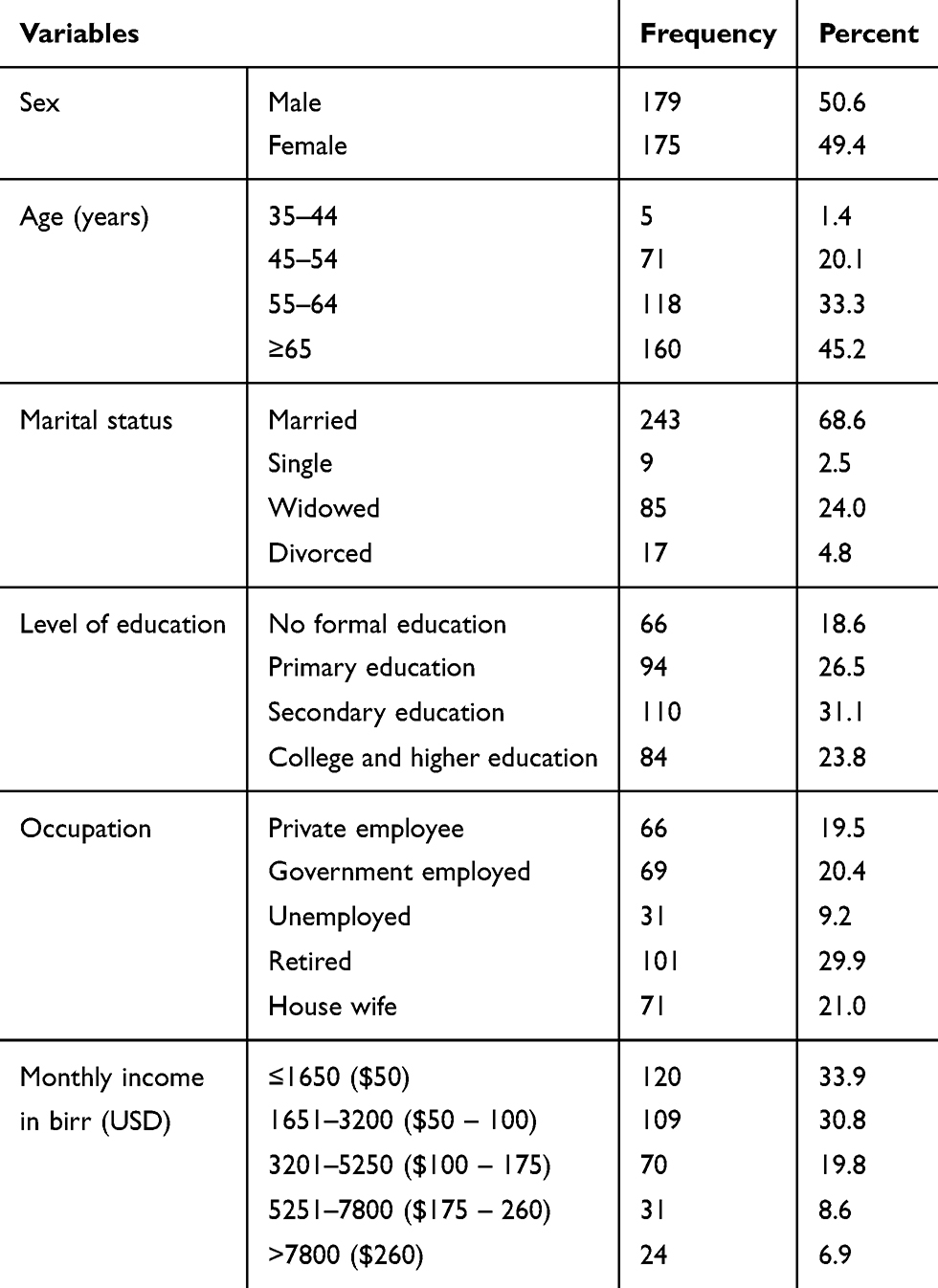 |
Table 1 Socio-Demographic Characteristics of Study Participants on Diabetes Follow-Up at Yekatit 12 Hospital, Addis Ababa, Ethiopia, 2019 (n = 354) |
The mean duration of illness with type 2 diabetes was 8.4 years (±6.3 years). Nearly two-thirds (63.6%) of people living with type two diabetes had comorbidity; of which majority (67.1%) were hypertensive. About a quarter (23.4%) of the participants have a family history of diabetes. As mentioned in Table 2 below, majority of the participants (67.8%) use oral hypoglycemic agents as a mode of diabetes treatment. Majority (94.6%) of the participants had adequate knowledge on diabetes.
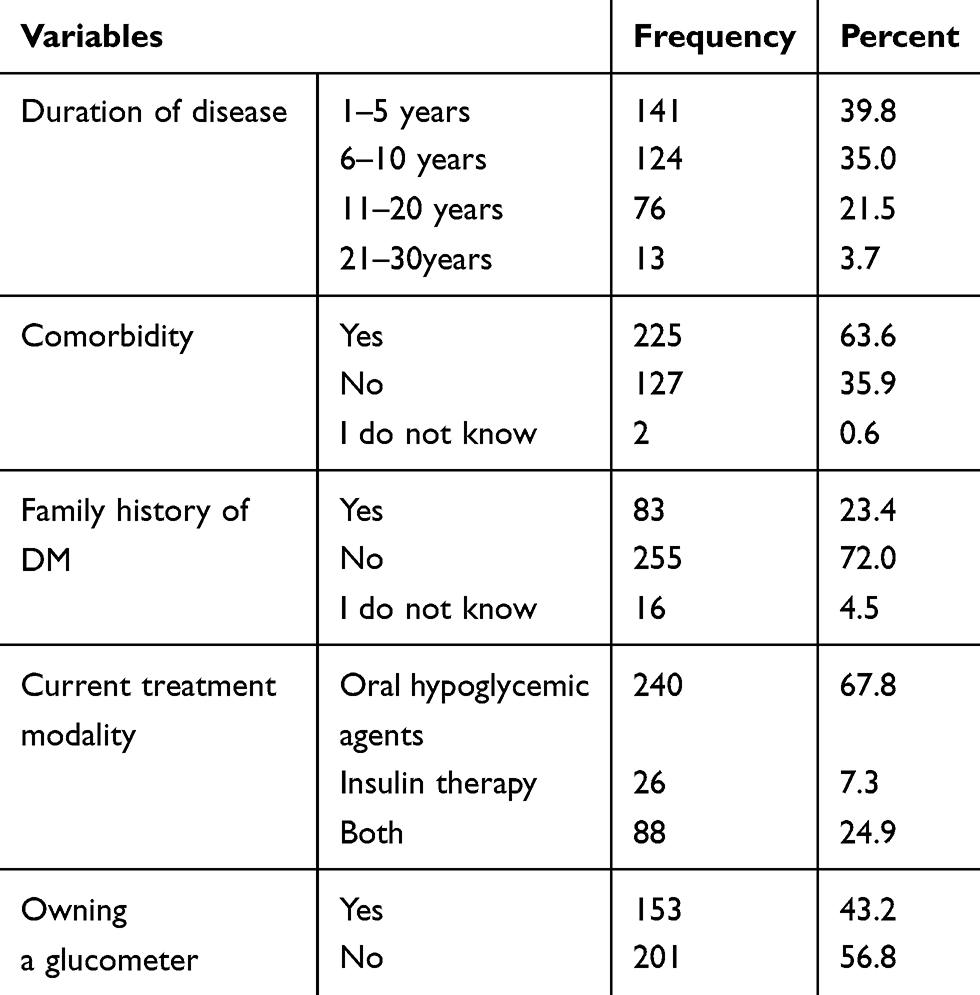 |
Table 2 Disease-Related Characteristics of Study Participants on Diabetes Follow-Up at Yekatit 12 Hospital, Addis Ababa, Ethiopia, 2019 (n = 354) |
Magnitude of Diabetes Self-Care Practice
Overall, more than half (52.0%, 95% CI= 46.9% - 57.1%) of the participants had poor diabetes self-care practice. Foot care being the least (50.8%) practiced (Figure 1).
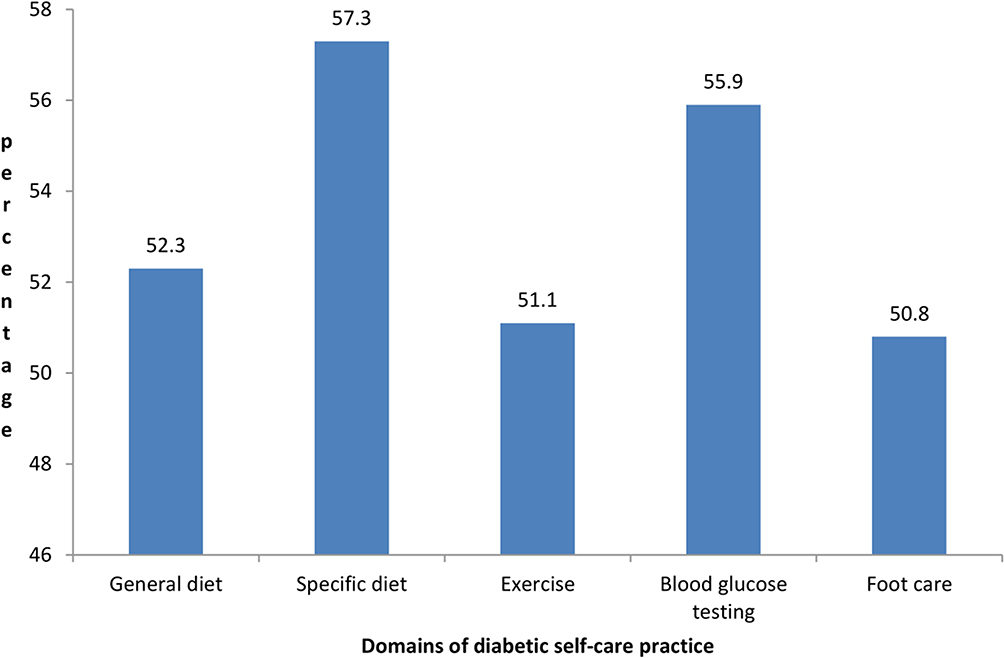 |
Figure 1 Magnitude of diabetes self-care practice domains among study participants at Yekatit 12 Hospital, 2019. |
Mean (standard deviation) score for general diabetic diet in the past seven days was computed to be 3.3±0.5 and about half scored above and equal to the mean as illustrated in Figure 1 below. Moreover, 57.3% of the participants had scores above or equal to the mean for specific diet plan (3.9±0.5). The mean practice of blood glucose testing in the past seven days was 1±0.5 and about 55.9% of the participants scored above and equal to the mean. Furthermore, about half of the participants exercised above or equal to the mean and half also had better foot care practice in the past seven days with mean score being 4.4±0.5. From all the participants, 95.5% did not smoke cigarettes in the seven days before interview.
Factors Associated with Poor Self-Care Practice
In the bivariate analysis (Table 3) factors associated with poor self-care practice were: sex, age, marital status, educational status, occupation, monthly income, duration of the diabetes, comorbidity, current treatment modality, not being a member of diabetes association, dissatisfaction with social service, owning glucometer and receiving diabetes education.
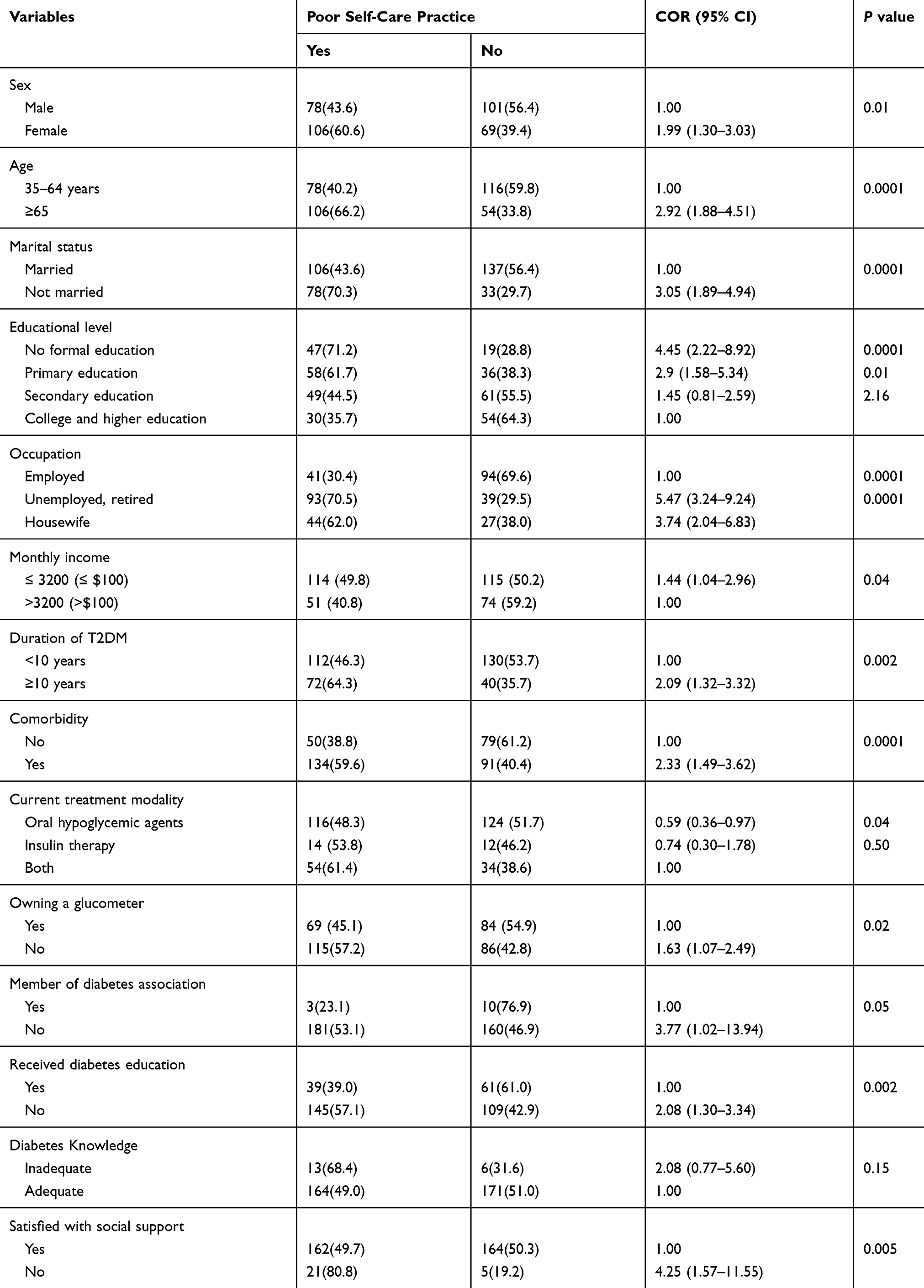 |
Table 3 Bivariate Analysis Showing Factors Associated with Poor Diabetes Self-Care Practice at Yekatit 12 Hospital, 2019 |
In the further multi-variable analysis (Table 4), being unemployed and retired, living with diabetes for ≥10 years, having comorbidity, not owning a glucometer, not receiving diabetes education and dissatisfaction with social support were significantly associated with poor diabetes self-care practice.
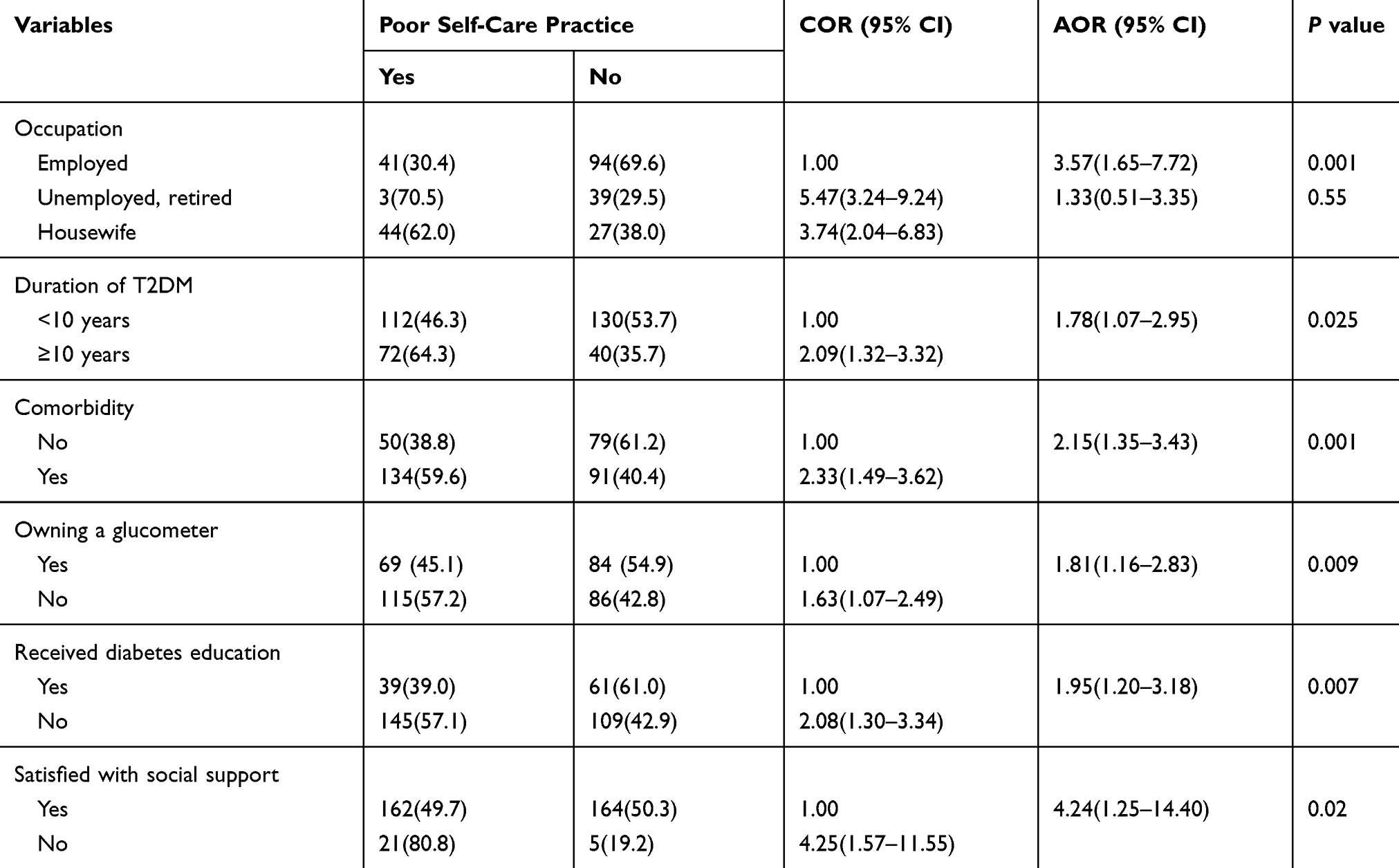 |
Table 4 Multi-Variable Analysis of Diabetes Self-Care Practice with Associated Factors Among Study Participants at Yekatit 12 Hospital, 2019 |
The odds of having poor self-care practice among unemployed and retired participants was 3.6 times higher than those who were employed (AOR: 3.57, 95% CI: 1.65–7.72). The odds of having poor self-care practice was 1.8 times higher in those who have had diabetes for ≥10 years than those who have had it for less than 10 years (AOR: 1.78, 95% CI: 1.07–2.95). Similarly, the odds of having poor self-care practice among those with comorbidity was two times (AOR= 2.15, 95% CI 1.35–3.43) higher than those without any comorbidity. The odds of having poor self-care practice among those who have no glucometer was 1.8 times (AOR= 1.81, 95% CI 1.16–2.83) higher as compared to those who own glucometer. Likewise, the odds of having poor self-care practice among those who did not receive diabetes education was two times (AOR= 1.95, 95% CI 1.20–3.18) higher as compared to those who received diabetes education and four times higher among those who were dissatisfied with social support (AOR= 4.24, 95% CI 1.25–14.40) as compared to those who were satisfied with social support.
Discussion
About half of the people living with type two diabetes who were on follow up at Yekatit 12 Hospital in Addis Ababa had poor diabetes self-care practice. In light of this finding, it is important to note that the management of glucose will not be achieved and people living with type two diabetes either suffer because of the complications or die prematurely.9,16 It has also an impact by burdening the health system and the routine clinical practices.17–19 This finding of the study is consistent with previously conducted studies in different parts of Ethiopia such as: Gondar (51.9%)20 and Jimma (49.1%).9 However, the finding of this study was higher than that was reported from a study conducted at Addis Ababa public hospitals (39.7%)7 and Nekemte Hospital (23.2%),15 but lower than a study done at Harari, Eastern Ethiopia (60.8%).14 Inconsistency between results could be because of the differences in the study instruments, source population, educational backgrounds and living status of the participants. This finding of the study underscores the need for strong diabetes education through multiple media and social networking.
From all the domains of diabetes self-care practice, foot care practice and exercise were the least practiced. It is known that diabetes foot complication and subsequent amputation is one of the common problems that people living with type two diabetes encounter.5,11,21 A previously conducted study reported that the risk of amputation due to diabetes foot complications will increase by 13-fold as compared to the general population.21 However, nearly half of the people living with type two diabetes in our study did not practice diabetes foot care. Similarly, regular exercise is also very important to manage blood sugar and prevent further diabetes complications. Exercise makes insulin more sensitive, so that the body can utilize it more effectively. Exercise also improves the glycolipid metabolism which helps to maintain optimal weight and prevent atherosclerosis which may lead to cardiac problems.12 However, about half of the people living with type two diabetes in our study did not do regular exercise. Therefore, it is very critical to provide adequate knowledge towards diabetes foot care practice and regular exercise to people living with type two diabetes in Addis Ababa. Physicians, family members and associations should play a major role in providing adequate information on diabetes foot care practice and regular exercise for the people living with type two diabetes.
Consistent with a study conducted in Bangladesh,22 diabetes poor self-care practice was higher among unemployed or retired individuals than those who were employed. This might be because of several factors such as older age of the individuals, lower socio-economic status, and overall lower health literacy among the unemployed or retired individuals. Poor self-care practice was also higher among those people living with type two diabetes for ≥10 years than their counterparts. This finding of the study indicates that the risk perception will decrease as they live longer with the disease. In a routine clinical practice and diabetes information delivery, this group of people is not usually targeted for health education, as there is a belief that these people might have adequate information on diabetes. Therefore, this study calls for inclusion of all people living with type two diabetes, irrespective of the duration of illness in health education and diabetes sensitization sessions.
In the present study it is indicated that people living with type two diabetes who have comorbidity were less likely to practice diabetes self-care. Consistent to this finding, previously conducted study reported that the amount of time and energy left for diabetes self-care is substantially reduced when comorbid illnesses are co-managed. In addition, having comorbid illnesses can sap the financial resources of people with diabetes by increasing their costs.11
Not owning a glucometer was another factor that was found to be associated with poor diabetic self-care practice. This finding is consistent with the previous study findings from Ethiopia such as studies conducted in Benishagul Gumuz7 and Addis Ababa.8 It is of note that having a glucometer at home will encourage patients to have frequent and regular measurements of blood glucose enabling better management of diabetes. Moreover, consistent with the studies conducted in Harari14 and Addis Ababa,8 diabetes education was found to be one of a strong factor that can affect diabetic self-care practice in our study. Acquiring education about diabetes from experts further encourages patients to know about their disease and act well in taking care of themselves. Furthermore, dissatisfaction with social support is also an important factor that can affect the diabetic self-care practice. Receiving social support is an essential factor in better control of diabetes because having a positive surrounding will better reinforce individuals for better self-care practices. This is supported by studies done at Gondar20 where by the odds of having poor self-care practice was lower by 69% among patient who had strong social support and at Addis Ababa public hospitals8 which showed that those who had social support had 1.59 times better odds of having good diabetic self-care practice.
This study was conducted in one of the public hospitals in Addis Ababa and might not be representative of all the people living with type two diabetes in the city. Moreover, the data collection was based on self-reporting of diabetes self-care practice which could also affect the results of this study. However, the study was conducted using a comprehensive and standardized tool, which allows for international comparison of our findings.
Conclusions
Overall, diabetes self-care practice was minimal among people living with type two diabetes in Addis Ababa. Particularly, diabetes foot care and regular exercise were the least performed. The poor self-care practice was associated with being unemployed and retired, living with diabetes for ≥10 years, having comorbidity, not owning a glucometer, not receiving diabetes education and dissatisfaction with social support. These findings of the study underscores the need for provision of adequate diabetes self-care education by healthcare providers, family members and diabetes associations.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; DKQ, Diabetes Knowledge Questionnaire; OPD, outpatient department; SDSCA, summary of diabetes self-care activities.
Data Sharing Statement
Data can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board (IRB) of Myungsung Medical College and permissions to conduct this study was obtained from Yekatit 12 Hospital. All participants of the study were informed about the study and they gave their written consent to be included in the study. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
The authors want to acknowledge Myungsung Medical College for funding of this study. The authors are also grateful the participants of the study for their cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Myungsung Medical College. However, the funder has no role on the study design, analysis and interpretation of the findings.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Cho N, Shaw J, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Dall TM, Zhang Y, Chen YJ, Quick WW, Yang WG, Fogli J. The economic burden of diabetes. Health Aff. 2010;29(2):297–303. doi:10.1377/hlthaff.2009.0155
3. Weinger K, Butler HA, Welch GW, La Greca AM. Measuring diabetes self-care: a psychometric analysis of the self-care inventory-revised with adults. Diab Care. 2005;28(6):1346–1352. doi:10.2337/diacare.28.6.1346
4. American Association of Diabetes Educators. An effective model of diabetes care and education: revising the aade7 self-care behaviors®. Diab Educ. 2020;46(2):139–160. doi:10.1177/0145721719894903.
5. Bell RA, Arcury TA, Snively BM, et al. Diabetes foot self-care practices in a rural, triethnic population. Diab Educ. 2005;31(1):75–83. doi:10.1177/0145721704272859
6. Berhe KK, Demissie A, Kahsay AB, Gebru HB. Diabetes self care practices and associated factors among type 2 diabetic patients in Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia-a cross sectional study. Int J Pharm Sci Res. 2012;3(11):4219.
7. Mamo M, Demissie M. Self care practice and its associated factors among diabetic patients in addis ababa public hospitals, cross sectional study. Diab Cholest Metabol 1. 2016;1(1):2–5.
8. Chali SW, Salih MH, Abate AT. Self-care practice and associated factors among diabetes mellitus patients on follow up in benishangul gumuz regional state public hospitals, Western Ethiopia: a cross-sectional study. BMC Res Notes. 2018;11(1):833. doi:10.1186/s13104-018-3939-8
9. Hailu E, Mariam WH, Belachew T, Birhanu Z. Self-care practice and glycaemic control amongst adults with diabetes at the jimma university specialized Hospital in south-west Ethiopia: A cross-sectional study. African j Primary Health Care Family Med. 2012;4:1. doi:10.4102/phcfm.v4i1.311
10. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diab Care. 2000;23(7):943–950.
11. Abdulghani HM, AlRajeh AS, AlSalman BH, et al. Prevalence of diabetic comorbidities and knowledge and practices of foot care among diabetic patients: a cross-sectional study. Diab, Metabolic Syndrome Obesity. 2018;11:417. doi:10.2147/DMSO.S171526
12. WHO W. Global recommendations on physical activity for health. Geneva World Heal Organ. 2010;60.
13. Rohani H, Eslami A, Raei M, Tavakoli Ghouchani H, Afshari A. Psychometric properties of the healthful eating belief scales for type 2 diabetics. J North Khorasan Univ Med Sci. 2014;6(2):319–327. doi:10.29252/jnkums.6.2.319
14. Ayele K, Bisrat Tesfa LA, Tilahun T, Girma E. Self care behavior among patients with diabetes in Harari, Eastern Ethiopia: the health belief model perspective. PLoS One. 2012;7:4. doi:10.1371/journal.pone.0035515
15. Amente T, Belachew T, Hailu E, Berhanu N. Self care practice and its predictors among adults with diabetes mellitus on follow up at Nekemte hospital diabetic clinic, West Ethiopia. World J Med Med Sci. 2014;2(3):1–16.
16. Rubin RR, Peyrot M, Saudek CD. Effect of diabetes education on self-care, metabolic control, and emotional well-being. Diab Care. 1989;12(10):673–679. doi:10.2337/diacare.12.10.673
17. Caspersen CJ, Thomas GD, Boseman LA, Beckles GL, Albright AL. Aging, diabetes, and the public health system in the United States. Am J Public Health. 2012;102(8):1482–1497. doi:10.2105/AJPH.2011.300616
18. Group CM-CTDS. Closing the gap: effect of diabetes case management on glycemic control among low-income ethnic minority populations: the California Medi-Cal type 2 diabetes study. Diab Care. 2004;27(1):95–103. doi:10.2337/diacare.27.1.95
19. Ashwal E, Hadar E, Hod M. Diabetes in low-resourced countries. Best Pract Res Clin Obstet Gynaecol. 2015;29(1):91–101. doi:10.1016/j.bpobgyn.2014.05.009
20. Aschalew AY, Yitayal M, Minyihun A, Bisetegn TA. Self-care practice and associated factors among patients with diabetes mellitus on follow up at University of Gondar Referral Hospital, Gondar, Northwest Ethiopia. BMC Res Notes. 2019;12(1):591. doi:10.1186/s13104-019-4630-4
21. Al-Wahbi AM. Impact of a diabetic foot care education program on lower limb amputation rate. Vasc Health Risk Manag. 2010;6:923. doi:10.2147/VHRM.S13569
22. Saleh F, Mumu SJ, Ara F, Begum HA, Ali L. Knowledge and self-care practices regarding diabetes among newly diagnosed type 2 diabetics in Bangladesh: a cross-sectional study. BMC Public Health. 2012;12(1):1112. doi:10.1186/1471-2458-12-1112
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.