")
Back to Journals » Patient Preference and Adherence » Volume 16
Self-Care in Patients with Non-Optimal Diabetes Management in Brazilian Rural Areas: A Mixed-Methods Study
Authors Macedo JCL , Soares DA, de Carvalho VCHS , Cortes TBA, Mistro S , Kochergin CN, Rumel D , Oliveira MG
Received 4 May 2022
Accepted for publication 21 July 2022
Published 27 July 2022 Volume 2022:16 Pages 1831—1842
DOI https://doi.org/10.2147/PPA.S373302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jessica Caline Lemos Macedo,1 Daniela Arruda Soares,1 Vivian Carla Honorato dos Santos de Carvalho,2 Taciana Borges Andrade Cortes,1 Sóstenes Mistro,1 Clavdia Nicolaevna Kochergin,2 Davi Rumel,3 Marcio Galvão Oliveira1
1Master’s Program in Collective Health, Multidisciplinary Health Institute, Federal University of Bahia, Vitória da Conquista, Bahia, Brazil; 2Multidisciplinary Health Institute, Federal University of Bahia, Vitória da Conquista, Bahia, Brazil; 3Department of Community Health, School of Medicine of the Municipal University of São Caetano do Sul, São Caetano do Sul, São Paulo, Brazil
Correspondence: Marcio Galvão Oliveira, Multidisciplinary Health Institute, Federal University of Bahia, Rua Hormindo Barros, 58 - Candeias, Vitória da Conquista - BA, Vitória da Conquista, Bahia, 45029-094, Brazil, Tel +55 77 988280954, Email [email protected]
Purpose: This study aims to assess self-care in patients with non-optimal diabetes management (HbA1c > 7.0% for adults and > 8.0 for those aged 60 or over) and the positive and negative experiences associated with it in the rural communities of a Brazilian municipality.
Patient and Methods: This is a cross-sectional mixed-methods study. The data were collected from participants with high HbA1c through focus group discussions, subsequently performing thematic analysis, and through structured questionnaires (socioeconomic characteristics and the Summary of Diabetes Self-Care Activities (SDSCA)).
Results: The mean HbA1c of the 156 study participants was 9.94% (95% confidence interval: 9.70– 10.19%) and most participants (86.54%) had negative self-care behaviors, with an overall SDSCA mean score of 3.55. This mean was not positive for any of the socioeconomic characteristics. The self-care activities with the most satisfactory performance concerned non-smoking and the use of prescribed medications, and the poorest results were observed for the practice of specific physical activities. The qualitative data indicated that the study participants face many difficulties regarding self-care practices, especially those related to an adequate diet.
Conclusion: The self-care assessment revealed unsatisfactory self-care behaviors as well as high HbA1c levels among the study participants and highlighted the various difficulties they encounter. This indicates the need for more attentive health teams to monitor patients, especially regarding actions focused on the non-pharmacological elements of self-care, such as lifestyle changes, which were found to be the dimensions with the most unsatisfactory results.
Keywords: primary care, non-communicable diseases, behaviors, rural communities
Introduction
Diabetes mellitus (DM) is characterized by a deficient action and/or production of insulin and is an important global health problem.1 The number of adults with diabetes in Central and South America is projected to increase to 49 million by 2045, equivalent an increase of 50%.2
In addition to its high prevalence, optimal management of diabetes is still limited worldwide.3 The estimates indicate that approximately 50% of individuals with diabetes do not meet the recommended glycated hemoglobin (HbA1c) target, and, therefore, that of metabolic control.4 Another concerning issue is that most individuals with diabetes do not have access to HbA1c monitoring as recommended,5 and, when the test is requested, there is a significant delay in obtaining the results during the clinical visit of the patient to the health care professional, which causes treatment delays and increases the risk of complications.5
The micro and macrovascular complications of diabetes can result in retinopathy, nephropathy, coronary heart disease, cerebrovascular disease, peripheral arterial disease, and neuropathy, and are important risk factors for amputations. Therefore, this disease has a great impact on morbidity, mortality, and quality of life, as well as an economic impact on health systems. Moreover, it requires patients to make a wide range of decisions.1
Self-care is a lifestyle in which individuals practice activities to ensure a healthy life.6 Diabetes self-management education and support is related to a lower risk of complications, and, consequently, reduction of hospitalizations and costs. Correspond to the process of facilitating the understanding and coping necessary for the patient to adapt to the behaviors for a continuous self-care, addressing and evaluating barriers to optimal diabetes management, such as psychosocial issues, misinformation, diabetes-related distress, fears, medication side effects, and misperceptions.7
In this way, optimal management of diabetes is achieved through adequate pharmacotherapy together with key lifestyle elements, which is a result of self-care behaviors.8 Additionally, the social determinants of health, namely the economic, environmental, political, and social conditions in which individuals live, are highly influential.9
Problems that affect mental health can impair an individual’s ability to effectively practice self-care. The health care workers should promote activities involving emotional support, nutritional support, physical activity, smoking cessation, and other healthy habits.10
Therefore, in rural communities, it becomes even more imperative to strengthen strategies for monitoring patients with diabetes, since this population primarily faces challenges related to expenses and transportation to access care services, given the greater distances to health care units and their greater social vulnerability.11 The objective of this study was to assess self-care in patients with diabetes with off-target glycated hemoglobin levels and the positive and negative experiences associated with it in the rural communities of a Brazilian municipality.
Materials and Methods
This is a cross-sectional mixed-methods study. The mixed-methods design was employed to allow a more comprehensive understanding of the results. The data was collected from focus groups and through structured questionnaires.
Data collection was conducted in four rural area health units between July 2019 and February 2020. These units were selected based on convenience as they represent various geographical configurations of the rural context, including those that are more difficult to access, those adjacent to the municipality’s main office, those with more vulnerable patient populations, and those with health care workers focused on community engagement.
The focus group participants were selected following referral from the health care workers. For the quantitative stage, participation was solicited through educational groups or health fairs held in the areas catered by the health unit, and home visits with the guidance of community health workers. Since this is a population study, all patients who were approached by the research team were recruited. The inclusion criteria were patients residing in the coverage area of the four health units in the rural area of the study, over 18 years of age, possessing cognitive abilities to answer the questions, and with non-optimal diabetes management (HbA1c>7.0% for adults and >8.0 for those aged 60 or over).9 These are patients followed up by the health units and who, therefore, have a prescription for hypoglycemic drugs.
The focus groups were moderated by an expert in qualitative studies. For the quantitative data collection, the research team was trained to perform the HbA1c tests, as well as to administer the structured questionnaires.
Quantitative Data
The quantitative data were collected via structured questionnaires administered to all study participants with a medical diagnosis of diabetes and HbA1c levels above the therapeutic targets (>7.0% for adults and >8.0 for the elderly).9
Most tests of patients seeking care in the public health system at the municipality level are performed in an advanced public laboratory. The distances from the four health units included in this study to the public laboratory are 6, 11, 12, and 15 km, which had to be covered by the patients in these units when the HbA1c test was requested.
However, the HbA1c levels were measured in this study using the portable Abbott Afinion™ 2 Analyzer, which requires only a drop of blood from a finger for sampling. It is a point-of-care (POC) device, that is, it has analytical systems that allow the test to be performed at the point of care, without the need to be in a physical area of a clinical laboratory.
The patients included in this study were asked about their socioeconomic characteristics, namely gender, age, skin color, marital status, education, income source (none, employed, or retired), number of residents in the household, and the monthly per capita income of the household (considering the total income of the household and the number of residents).
Additionally, the Summary of Diabetes Self-Care Activities (SDSCA) was applied, which includes dimensions on general diet, specific diet, physical activity, glycemic monitoring, foot care, medication use, and smoking. The participants were required to report how often they performed the activities in each dimension in the previous seven days. The responses ranged from 0 to 7, in which 0 is the least desirable situation and 7 is the most favorable, except for the specific diet items regarding the consumption of high-fat foods and sweets;12 the interpretation is the opposite for these specific diet items, that is, it is more favorable when consumption is less frequent. Therefore, to facilitate the analysis, these variables were revised as “Did not eat red meat and/or whole milk products” and “Did not eat sweets” and the responses were reverse coded (7=0, 6=1, 5=2, 4=3, 3=4, 2=5, 1=6, 0=7), as suggested in the revised SDSCA.13 The characterization of good self-care behaviors occurs when the activity is performed for five or more days, that is, the SDSCA overall mean score should be greater than or equal to 5.0 for a classification of good self-care behavior.
The collected data were stored in the Kobo Toolbox®, with subsequent analysis using the Stata® software version 15.0. The sociodemographic variables and the performance of self-care activities by days of the week (0 to 4 or 5 to 7 days) were analyzed using absolute and relative frequencies. Self-care was also presented as a measure of central tendency (mean) and measure of dispersion (standard deviation).
Qualitative Data
A focus group discussion was conducted in July 2019 in each of the four health units in the study, with 10 to 15 participants per group. The scripts used in these groups contained guiding questions that enabled a broad discussion about participants’ health care.
The discussions were in Portuguese and the data transcription was carried out in a non-naturalistic way, that is, while the language used to transcribe the verbal discourse was more polished, the original meaning of the information communicated by the interviewee was maintained.
The focus group data are descriptive and reflect the patients’ subjective experience about diabetes self-care, as well as the underlying positive and negative aspects. The steps of the thematic analysis were based on Braun and Clarke14 and are as follows: Step 1 - The data were transcribed by the researcher or research assistant immediately after collection. The transcripts were read repeatedly to familiarize the researchers with the depth and breadth of the content and to guide subsequent analysis. Step 2 - The researchers divided the text into units of meanings, comprising sentences/paragraphs. The data were further coded for its organization into meaningful groups to fulfil the research objectives. Step 3 - The codes were analyzed, and the analogues were combined into common themes, ultimately resulting in a set of themes and sub-themes, expanding the understanding of quantitative data.
Ethical Considerations
The study was approved by the Human Research Ethics Committee of the Multidisciplinary Health Institute - Federal University of Bahia (Opinion number: 3.357.963). The focus group participants signed informed consent forms (ICF) to authorize the recording and transcription of their testimonies. The participants were not requested to sign an ICF for the administration of the questionnaire in the quantitative stage, since it could not be conducted in practice without a waiver and the risk of this research was only minimal. The Human Research Ethics Committee for the current study has waived the need for informed consent for the participants who were a part of the questionnaire survey. This study complies with the Declaration of Helsinki.
Results
Quantitative Analysis
Data obtained from 156 patients with non-optimal diabetes management were included in the quantitative analysis. Most patients included in the study were female (71.79%), aged 60 to 79 years (45.51%), brown (46.15%), married or living with a partner (66.67%), and had a low level of education (with 88.08% illiterate or having incomplete primary education).
Regarding income source, most were retired (49.36%). Although the retirement pension almost constituted minimum wage, when shared among the residents of a given household, it amounted to a monthly per capita income of less than $110 (66.88%).
A mean HbA1c level of 9.94% (95% confidence interval: 9.70–10.19%) was reported, and 17 (10.90%) participants were young adults with values of 7.1–8.0%, 29 (18.59%) participants with HbA1c of 8.1–8.9%, 35 (22.44%) with 9.0–9.9%, and 75 (48.08%) with values greater than 10.0%.
A SDSCA overall mean score of less than 5.0 was observed across all socioeconomic characteristics. Considering the self-care dimensions, the one related to the appropriate use of medication presented a mean above 5.0 for most socioeconomic characteristics, except for participants under the age of 40 (mean=4.14), those with complete primary education (mean=4.00) and incomplete high school education (mean=4.11), and those engaged in a paid activity (mean=4.96). The dimension of glycemic monitoring had a positive result for participants with incomplete high school education (mean=6.42). Participants with an income of less than $55 and those with complete high school education also obtained satisfactory results for the dimension of foot care, with means of 5.00 and 5.63, respectively (Table 1).
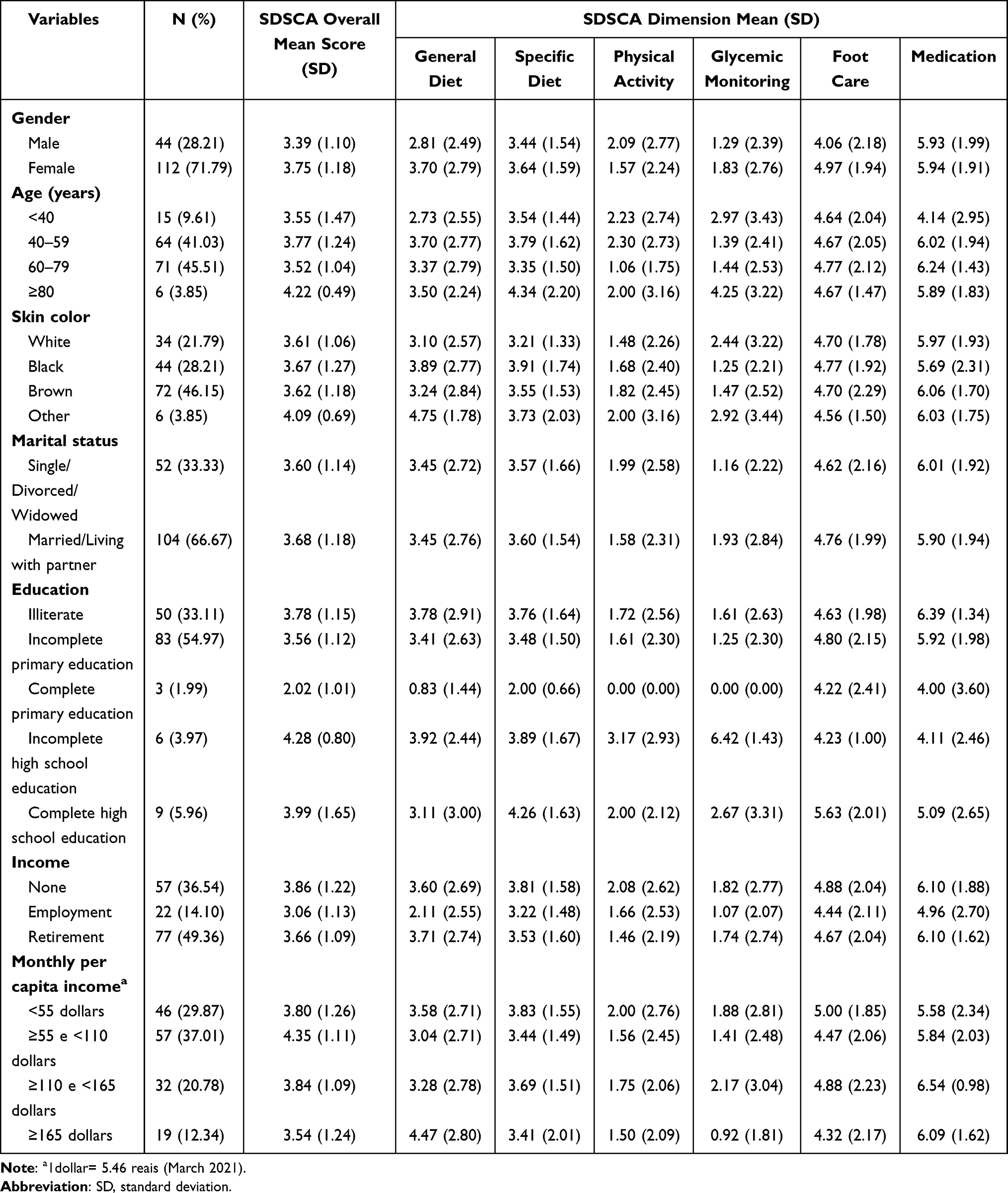 |
Table 1 Sociodemographic Characteristics According to the Means of the Dimensions of the Summary of Diabetes Self-Care Activities (SDSCA) |
Table 2 presents the results regarding the number of days the participants performed the activities according to the general and specific dimensions of self-care. Most participants (86.54%) reported negative self-care behavior, with a SDSCA overall mean score of 3.55.
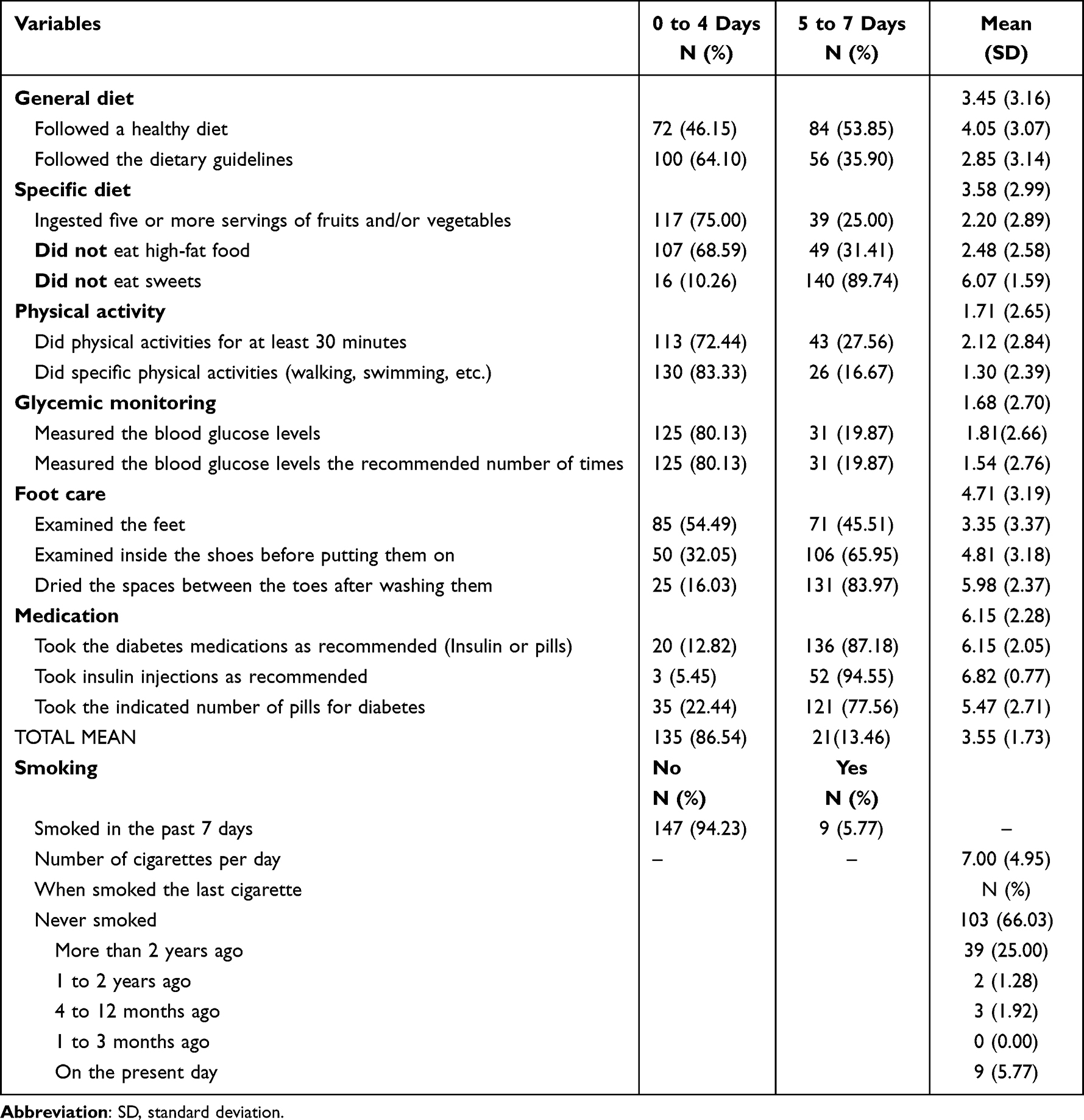 |
Table 2 Number of Days Performing Activities According to the General and Specific Dimensions of Self-Care Among Patients with Diabetes |
As for the “General diet” dimension, more than half of the participants exhibited a desirable behavior for the item on following a healthy diet (53.85%), although only 35.90% responded that they had followed dietary guidelines on 5 days or more. Regarding the items in the “Specific diet” dimension, most participants had five or more servings of fruits and/or vegetables on less than 5 days of the week (75.00%), and 31.41% did not eat high-fat foods for 5 days or more, with a mean of 2.48 days without such consumption, that is, the consumption of high-fat foods occurred every 4.52 days on average. The only item in the “Specific diet” dimension that revealed a desirable result was the consumption of sweets, since 89.74% of the patients reported not eating sweets for 5 or more days, with a mean of 6.07 days without such consumption.
The items of the “Physical activity” dimension revealed undesirable self-care behaviors among the participants, with a mean of 2.12 days for exercising for at least 30 minutes and 1.30 days for specific activities such as walking and swimming.
With regard to the “Glycemic monitoring” dimension, only 19.87% assessed blood glucose levels in 5 or more days and followed the frequency recommended for such monitoring, with a mean of only 1.81 days between glycemic tests.
Considering the “Foot care” dimension, 45.51% examined their feet, 65.95% examined inside the shoes before putting them on, and 83.97% dried the interdigital spaces after washing them; thus, the best self-care results were obtained for the last two items.
Most patients presented a desirable behavior for all items of the “Medication” dimension, with a mean of 6.15 days for taking diabetes medications as recommended (insulin or pills), a mean of 6.82 days for using insulin injections as recommended, and a mean of 5.47 days for taking the indicated number of pills for diabetes.
With regard to the “Smoking” dimension, while most patients never smoked (66.03%), 44 (28.20%) were former smokers, and only 9 individuals (5.77%) smoked in the previous 7 days, with a mean of 7 cigarettes per day.
Qualitative Analysis
The themes in this study were grouped into three major categories related to the domains of self-care—diet, physical activity, and medication use—and into subcategories related to each domain. These were then linked to the patients’ positive and negative experiences. The qualitative analysis (Table 3) showed a certain dichotomy between what patients valued in their self-care experience and what constituted an obstacle to its achievement, with the latter standing out.
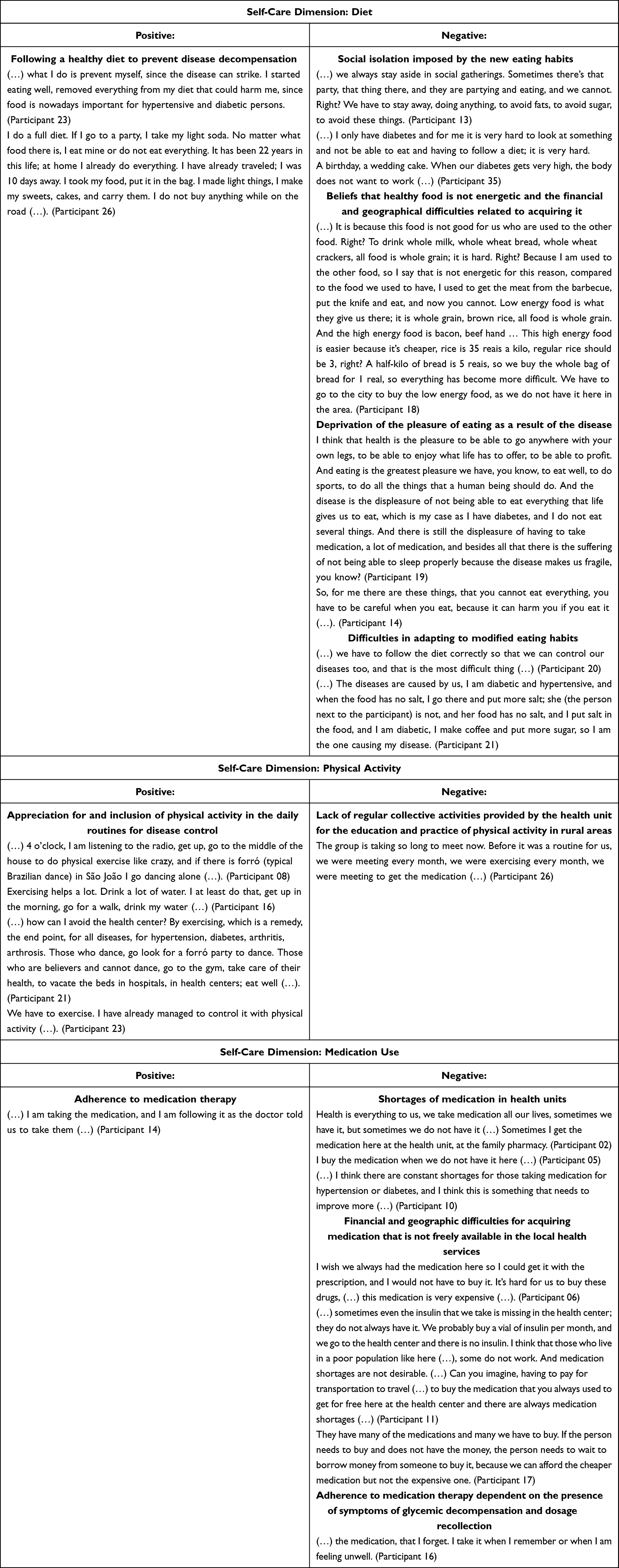 |
Table 3 Positive and Negative Experiences of Patients with Diabetes Related to Self-Care Dimensions |
Regarding diet, although a small number of patients reported making healthy choices, most revealed negative experiences which were related to individual aspects such as distorted beliefs about food, deprivation of the pleasure of eating, difficulty in changing eating habits, as well as social isolation for not being able to eat certain food products and the geographical constraints in acquiring them.
The inclusion of physical activity in daily routines was more significant in patients’ reports. Although collective activities with the community were organized by health units, thereby providing opportunities for socialization and monitoring by a physical educator, these were performed infrequently by the participants, who indicated demotivation to be the reason.
The medication use dimension demonstrated that participants understand the need to follow the recommended pharmacotherapy and consequently, attempt to do so. However, many reported medication shortages in health units, thereby requiring the patients to buy them, which in turn results in an adverse economic impact given the low purchasing power of the population. Adhering to medication therapy depending on the presence of symptoms was also a limiting aspect revealed in the patients’ experiences.
Discussion
The self-care behavior of the study population was classified as poor, given the SDSCA overall mean score of 3.55. In a study in Ethiopia, it was found that 45.5% of patients with diabetes had inadequate self-care practices, while in the present study, were 86.54%. This higher proportion may have occurred because our study was performed only with patients outside the HbA1c target.15 Poor self-care behaviors are associated with poor diabetes management, and the participants of the present study had significantly elevated HbA1c levels, with 69.81% having values greater than or equal to 9.0%. Since there is a direct relationship between the elevated HbA1c levels and the risk of complications,9 it is inferred that the study population was at high risk of suffering from micro and macrovascular events.
It is known that diabetes results from a combination of genetic and environmental factors, and thus, the various social determinants of health, such as employment/occupation, income, level of education, housing conditions, and access to health services, act as risk factors for higher blood glucose levels.9 Therefore, the characteristics of individuals from the rural area selected for this study demonstrate unfavorable risk factors in the study population, contributing to impaired diabetes management.
Optimal diabetes management is ensured through a combination of adequate pharmacotherapy and healthy lifestyle behaviors.8 The health team has an important role in monitoring, supporting, and stimulating the development of the individuals’ autonomy. This may be achieved by understanding them in a comprehensive manner and planning actions together so that the patients are able to perform their self-care activities, and, consequently, improve their clinical outcomes and quality of life.10
The diabetes self-care education includes group and/or individual approaches, with the definition of specific behavioral targets and plan reviews.16 The group method of diabetes self-management education and Support is widespread as it is less expensive, allowing several patients with diabetes to meet and discuss, and is also known to improve clinical outcomes.17
The SDSCA indicates that the self-care activities most satisfactorily performed by the study participants were related to non-smoking and the use of prescribed medications, and the least satisfactory results concerned the practice of specific physical activities. These findings regarding self-care activities performed by patients with diabetes are similar to those found in other studies.18–20
Healthy eating was reported to be performed by 53.85% of the participants with diabetes. In contrast, only 35.90% responded that they followed dietary guidelines for 5 days or more. This difference can indicate that they followed a diet that they considered healthy, but did not receive specific dietary guidance. This may suggest that their eating habits were based on cultural and family guidelines, which constitutes poor objective assessment.
Many participants reported that the greatest difficulty they encountered in diabetes management is related to diet, primarily due to the restrictions on certain types of food that they are culturally accustomed to, that is, the foods that are more easily available in their homes are usually with a higher glycemic index and, therefore, are not considered ideal for diet composition. They believe that diabetes deprives them of the pleasure of eating what they want to eat, especially causing them to withdraw from social gatherings in which other individuals will be eating foods inappropriate for those with diabetes. Some also believe that healthy food is not energetic. Some participants found it harder to acquire healthy foods due to financial and geographical reasons. These perceptions and obstacles contribute to low dietary compliance and are consistent with what is found in the literature.21
Therefore, this study reveals that the most challenging aspect in diabetes self-care is the diet. Ideally, every patient should have nutritional counseling as early as the diagnosis. However, most patients with diabetes have never received formal dietary guidance and even fewer have visited a nutritionist. Considering the improvements resulting from an adequate diet for patients with diabetes, it is thus crucial that all members of the health team provide at least basic dietary guidance.8 The approach of the health team should be based on the perspective of food and nutrition education that considers the cultural and socioeconomic aspects, thereby promoting the autonomy of the individuals to make healthy choices even when they are in different situations, that is, without the need for depriving themselves of social interaction, which is important for mental health and quality of life.
Fresh and minimally processed foods should be preferably consumed; patients should avoid consuming processed and ultra-processed foods as much as possible. The consumption of carbohydrates by patients with diabetes should come mainly from foods such as fruits and vegetables rather than carbohydrate sources with high concentrations of fats, sugars, and sodium.1 However, only 25% of the study participants with diabetes ate five or more servings of fruits and/or vegetables for at least 5 days a week and 68.59% ate high-fat foods for 5 days or more. The only positive self-care behavior related to specific diet was the low consumption of sweets, with a mean consumption of less than 1 day per week (0.93). These results reflect what was pointed out in the qualitative stage, which demonstrates that the participants consider healthy foods to be of low energy and face geographic and economic difficulties in obtaining them. This finding regarding low economic status being a barrier to adequate diet-related self-care is reported in the literature.22
It is recommended that patients with diabetes also practice at least 150 minutes of moderate to vigorous aerobic activity weekly, as it increases glucose uptake in the muscle by up to five times by insulin-independent mechanisms and can improve insulin action by up to 24 to 48 hours.23 Moreover, since type 2 diabetes is a chronic inflammatory disease, exercise leads to improvements for its associated anti-inflammatory and metabolic effects.24 However, 72.44% of the participants with diabetes in this study did not perform physical activity for at least 5 days, and the mean number of days of this practice for at least 30 minutes was 2.12 days per week. However, the analysis of participants’ statements demonstrates a greater appreciation for physical activity, suggesting that the participants practice physical activities but for less than 30 minutes. This could be improved with more regular group activities organized by the health unit for improving awareness and practice of physical activity.17
Glycemic self-monitoring is known to assist in adequate metabolic control, because it increases the individual’s responsibility towards more active self-care performance, facilitates faster recognition of hypoglycemia, and allows for treatment adjustments on the results following visits to the health center.25 However, many individuals do not self-monitor blood glucose levels due to social and economic issues.24 This is observed among the participants in the present study who obtained a mean of 1.81 days of glycemic self-monitoring per week, with less than 20% of the participants assessing their blood glucose levels at home in 5 or more days—a result similar to that found in another study.26
Additionally, individuals with diabetes need to take greater care of their feet, since they have a high risk of developing ulcers, which, associated with wound healing disorders that are common in patients with diabetes, may lead to the drastic consequence of limb amputation, which occurs 10 to 30 times more than in the general population.27 Foot ulcers cause physical, psychological, productivity, and financial losses, drastically worsening the patients’ quality of life. Therefore, it is important to prevent ulcers through health education so that patients are able to properly care for their feet, in addition to conducting clinical examinations with screening for loss of sensation. In this regard, the best prevention outcomes are derived from patients performing self-care and a health system focused on preventive care.1,27 However, the examination of feet in clinical care is still a practice poorly performed worldwide, including Brazil.1
HbA1c levels greater than 9.0% are significantly associated with the development of foot ulcers,28 and, therefore, most participants of this study exhibit this risk factor, as 104 (65.41%) individuals had HbA1c levels above 9.0%. However, the self-care item on examination of the feet by the participants was performed unsatisfactorily (45.51%), although most reported examining inside the shoes before putting them on (65.95%) and drying the spaces between the toes after washing them (83.97%).
The prevalence of amputation is also correlated with smoking,29 in addition to being considered a risk factor for the onset of type 2 diabetes, impairing the control of the disease, increasing the incidence of complications such as acute myocardial infarction, peripheral vascular disease, kidney disease, and cancer, and also increasing mortality arising from cardiovascular diseases and overall mortality.1 This risk of overall mortality is reduced by 30% when smoking ceases.1 The present study has a significant number of former smokers (28.20%) and only 5.77% of current smokers, a result below the mean of the Brazilian population (9.3%).30
In combination with a healthy lifestyle, patients with diabetes should properly follow to pharmacological therapy indicated for the clinical profile of each individual.1 Based on the results of the SDSCA in this study, medication adherence was the best performed self-care behavior by the participants, indicating the recognition of the importance of medications, despite the existence of several individual (taking medication when they remember and forgetting the dosage), social (low socioeconomic status and travel difficulties), and procedural (medication shortages and unavailability in local services) constraints. In addition, since the results for the other self-care dimensions related to non-pharmacological therapy were much lower (except for smoking), the greater adherence to pharmacological therapy may indicate that taking medication requires fewer behavioral changes than those linked to lifestyle changes needed for diabetes management.
Since this is a cross-sectional study, it has the limitation of not being able to identify more precise causal links between the variables. Another limitation is that we do not have information on the type of diabetes. The strengths of this study include the novelty of being conducted in a Brazilian rural community setting among patients with decompensated diabetes. Furthermore, it provides insights that promote a more attentive and qualified health team, guiding their actions for diabetes management, thereby enabling better outreach strategies for patients in rural communities.
Conclusion
Considering all the results discussed herein, the self-care assessment of patients with diabetes in this study demonstrated that the participants have a negative self-care score that is related to various difficulties faced by them during self-care and high HbA1c levels. Therefore, as a way of improving diabetes management, family health units should optimize the monitoring of patients with guaranteed access to medication, offer monitoring tests, and assess the need for medication adjustments. Moreover, it is especially important that the health teams continuously conduct awareness and educational activities with a greater focus on the non-pharmacological elements of self-care. This is because lifestyle changes is reported in the literature as being highly difficult, and moreover such dimensions obtained unsatisfactory results in the present study.
Acknowledgments
We are grateful to the Municipal Health Department and the Family Health Teams of the four health units (where the study was conducted) for their support and acceptance of the study’s proposals. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 and Medtronic Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brazilian Society of Diabetes. Guidelines of the Brazilian Society of Diabetes 2019–2020.Editora Clannad São Paulo; 2019.
2. International Diabetes Federation. IDF diabetes atlas, 10th ed. Brussels, Belgium: International Diabetes Federation; 2021. Available from: https://www.diabetesatlas.org.
3. Schnell O, Crocker JB, Weng J. Impact of HbA1c testing at point of care on diabetes management. J Diabetes Sci Technol. 2017;11(3):611–617. doi:10.1177/1932296816678263
4. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic control. Patient Educ Couns. 2016;99(6):926–943. doi:10.1016/j.pec.2015.11.003
5. Egbunike V, Gerard S. The impact of point-of-care A1C testing on provider compliance and A1C levels in a primary setting. Diabetes Educ. 2013;39(1):66–73. doi:10.1177/0145721712465340
6. Abate TW, Dessie G, Workineh Y, et al. Non-adherence to self-care and associated factors among diabetes adult population in Ethiopian: a systemic review with meta-analysis. PLoS One. 2021;16(2):e0245862. doi:10.1371/journal.pone.0245862
7. Powers MA, Bardsley JK, Cypress M, et al. Diabetes self-management education and support in adults with type 2 diabetes: a consensus report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. Diabetes Educ. 2020;46(4):350–369. doi:10.1177/0145721720930959
8. Evert AB, Dennison M, Gardner CD, et al. Nutrition therapy for adults with diabetes or prediabetes: a consensus report. Diabetes Care. 2019;42(5):731–754. doi:10.2337/dci19-0014
9. American Diabetes Association. Standards of Medical Care in Diabetes—2020 abridged for primary care providers. Clin Diabetes. 2020;38(1):10–38. doi:10.2337/cd20-as01
10. American Diabetes Association. 5. Lifestyle management: standards of medical care in diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S46–S60. doi:10.2337/dc19-S005
11. Flor LS, Wilson S, Bhatt P, et al. Community-based interventions for detection and management of diabetes and hypertension in underserved communities: a mixed-methods evaluation in Brazil, India, South Africa and the USA. BMJ Glob Health. 2020;5(6):e001959. doi:10.1136/bmjgh-2019-001959
12. Michels MJ, Coral MHC, Sakae TM, Damas TB, Furlanetto LM. [Questionnaire of Diabetes Self-Care Activities: translation, cross-cultural adaptation and evaluation of psychometric properties] Questionário de Atividades de Autocuidado com o Diabetes: tradução, adaptação e avaliação das propriedades psicométricas. Arq Bras Endocrinol Metabol. 2010;54(7):644–651. doi:10.1590/S0004-27302010000700009
13. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943
14. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
15. Gurmu Y, Gela D, Aga F. Factors associated with self-care practice among adult diabetes patients in West Shoa Zone, Oromia Regional State, Ethiopia. BMC Health Serv Res. 2018;18(1):1–8. doi:10.1186/s12913-018-3448-4
16. Marrero DG, Ard J, Delamater AM, et al. Twenty-first century behavioral medicine: a context for empowering clinicians and patients with diabetes: a consensus report. Diabetes Care. 2013;36(2):463–470. doi:10.2337/dc12-2305
17. Steinsbekk A, Rygg L, Lisulo M, Rise MB, Fretheim A. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv Res. 2012;12(1):213. doi:10.1186/1472-6963-12-213
18. Gomides DDS, Villas-Boas LCG, Coelho ACM, Pace AE. Self-care of people with diabetes mellitus who have lower limb complications. Acta Paulista de Enfermagem. 2013;26(3):289–293.. doi:10.1590/S0103-21002013000300014
19. Nogueira BCM, Souza CA, Manzano RM, et al. Emotional aspects and self-care of patients with Type 2 Diabetes Mellitus in Renal Replacement Therapy. Cadernos Brasileiros de Terapia Ocupacional. 2019;27(1):127–134. doi:10.4322/2526-8910.ctoao1575
20. Veras VS, Santos MA, Rodrigues FFL, Arrelias CCA, Pedersoli TAM, Zanetti ML. Self-care among patients enrolled in a self-monitoring blood glucose program. Rev Gaucha Enferm. 2014;35(4):42–48. doi:10.1590/1983-1447.2014.04.47820
21. Maeyama MA, Pollheim LCF, Wippel M, Machado C, Veiga MV. [Aspects related to the difficulty of glycemic control in patients with type 2 diabetes mellitus in primary health care] Aspectos relacionados à dificuldade do controle glicêmico em pacientes com Diabetes Mellitus tipo 2 na Atenção Básica. Braz J Dev. 2020;6(7):47352–47369. doi:10.34117/bjdv6n7-391
22. Bukhsh A, Goh B-H, Zimbudzi E, et al. Type 2 diabetes patients’ perspectives, experiences, and barriers toward diabetes-related self-care: a qualitative study from Pakistan. Front Endocrinol. 2020;11:534873. doi:10.3389/fendo.2020.534873
23. Colberg SR, Sigal RJ, Yardley JE, et al. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2016;39(11):2065–2079. doi:10.2337/dc16-1728
24. Karstoft K, Pedersen BK. Exercise and type 2 diabetes: focus on metabolism and inflammation. Immunol Cell Biol. 2016;94(2):146–150. doi:10.1038/icb.2015.101
25. de Souza Teixeira CR, Zanetti ML, Landim CAP, et al. Self-monitoring blood glucose at home: integrative literature review Revista Eletrônica de Enfermagem. 2009;11(4):1006–1017. doi:10.5216/ree.v11i4.33257
26. Da Silva NJ, Lima RSC, Dos Santos AP, et al. [Evaluation of self-care in patients with diabetes mellitus in a municipality of east Maranhense] Avaliação do autocuidado em pacientes com diabetes mellitus em um município do leste Maranhense. Braz J Surg Clin Res. 2020;31(2):22–27.
27. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217–228. doi:10.1001/jama.293.2.217
28. Lavery LA, Armstrong DG, Vela SA, Quebedeaux TL, Fleischli JG. Practical criteria for screening patients at high risk for diabetic foot ulceration. Arch Intern Med. 1998;158(2):157–162. doi:10.1001/archinte.158.2.157
29. Jbour A, Jarrah NS, Radaideh AM, et al. Prevalence and predictors of diabetic foot syndrome in type 2 diabetes mellitus in Jordan. Saudi Med J. 2003;24(7):761–764.
30. Ministério da Saúde. [Vigitel Brazil 2018: surveillance of risk and protective factors for chronic diseases by telephone survey: estimates of frequency and sociodemographic distribution of risk and protective factors for chronic diseases in the capitals of the 26 Brazilian states and the Federal District in 2018] Vigitel Brasil 2018: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados brasileiros e no Distrito Federal em 2018. Brasília; 2019.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.